
Abstract
People with cancer often experience anxiety and depression following a diagnosis and can face barriers to accessing treatment for their mental health. An increasing number of patients are considering alternative approaches to managing their mental health symptoms, such as the psychedelic, psilocybin. A growing number of clinical trials show significant and enduring improvements in mood and quality of life following psilocybin-assisted therapy (PAT) in this patient group. While the lived experiences of patients undergoing PAT in clinical trials and medical contexts have been explored, the broad decision-making processes, perceptions of societal and self-acceptance of psilocybin, and the impact or otherwise of the legality of psilocybin outside of these settings have not. In this study, qualitative, semi-structured interviews were conducted to explore the attitudes and perceptions of using psilocybin by seven females in the United Kingdom with a current or previous diagnosis of cancer (four who had used psilocybin and three who had considered taking the drug). Data were analysed using Interpretative Phenomenological Analysis (IPA). Three group experiential themes were created: (i) somatic healing needs; (ii) outlawing nature: illegality as both a burden and boundary; and (iii) reconnecting self, nature, and mortality. Participants considered psilocybin a much-needed alternative to traditional treatments for the depression and anxiety they experienced in relation to their cancer diagnosis but felt its legal status was a significant barrier to access. As such, a compassionate access scheme here in the United Kingdom could transform the mental health of people with cancer.
Keywords
Background
In 2022, 20 million new cases of cancer were estimated worldwide, expected to increase to 35.3 million cases by 2050 (Bizuayehu et al., 2024). For one in three, the psychological distress associated with diagnosis, treatment, and post cancer experiences can trigger significant and often enduring bouts of poor mental health (e.g., Logan et al., 2019; Ryan et al., 2005; Salmon et al., 2015; Siegel et al., 2021; Zabora et al., 2001). Mental illness treatments offered to cancer patients are no different to those available to individuals without cancer (e.g., Barre et al., 2018; Compen et al., 2018; Logan et al., 2019). Similarly, the barriers to effective treatment are comparable: extensive waiting times, variable availability, and finding the ‘right’ treatment (McIntyre & Chow, 2020; Mental Health Taskforce, 2016). However, cancer patients often experience additional challenges whereby mental illness and distress triggered by cancer can be treatment resistant (Ostuzzi et al., 2018). For example, there is no clear evidence available for the efficacy of selective serotonin reuptake inhibitors (SSRIs) in treating depression in people with cancer (Okuyama et al., 2017) even though SSRIs are commonly prescribed for this patient group (Smith, 2017). Furthermore, cancer patients’ needs are dynamic and differ markedly from those without cancer due in part to the enduring and typically life-changing clinical treatments they undergo (e.g., Andersen et al., 2007; Bultz & Carlson, 2006; Holland et al., 2007; Spelten et al., 2003).
The psychiatric and psychosocial consequences of cancer for patients and their families are extensive (Caruso & Breitbart, 2020). Irrespective of whether gaining access is proving too lengthy, treatments are ineffective, or individuals are unsure about seeking help in the first instance, it is perhaps unsurprising that some individuals living with cancer might seek non-mainstream alternatives to help manage and/or treat poor mental health (Greenberg, 2004; Mosher et al., 2014). One such alternative is the psychedelic, psilocybin (e.g., Ross, 2018), which can be found in over 100 species of mushrooms. After ingestion, psilocybin interacts with several serotonin receptors in the brain and results in changes in perception and consciousness (McClure-Begley & Roth, 2022). However, in the United Kingdom, psilocybin is a Class A, Schedule 1 drug 1 : an illegal substance deemed to have no medical value.
Nevertheless, psilocybin-assisted therapy (PAT) has demonstrated significant potential in alleviating anxiety, depression, and psychological distress, particularly among individuals with terminal illnesses (Tsang & Roney, 2024). Given these promising results, in combination with the unmet clinical needs of millions of patients, some countries are relaxing their legislation around psilocybin. In the United States, psilocybin is decriminalised in several cities, with the states of Oregon and Colorado allowing supervised use (Marks, 2023). This is not limited to medical use which is the case in several other countries following the demonstration of efficacy in clinical trials. Australia allows psychiatrists with approval to prescribe psilocybin for treatment-resistant depression (TRD) (Dixon Ritchie et al., 2023). In June 2025, the Czech Republic lower house of parliament voted to approve the medical use of psilocybin (Parliament of the Czech Republic, 2025). Even more recently, in July 2025, Germany approved the medical use of psilocybin for TRD under a compassionate access programme (Gründer et al., 2025). Advocacy efforts led by the non-profit organisation TheraPsil were particularly successful in securing access to psilocybin for medical purposes in Canada. Under Section 56(1), TheraPsil helped patients gain legal access to psilocybin, and by December 2021, 47 palliative care and cancer patients had received exemptions (Doll, 2024). Since January 2022, in Canada, a Special Access Program (SAP) allows licensed physicians and nurse practitioners to prescribe psilocybin for individuals suffering from serious or life-threatening conditions, including cancer-related distress, when conventional treatments options have failed, are unsuitable, or are unavailable (de la Salle et al., 2024). In Europe, under a limited access programme, Switzerland has allowed psychedelics, including 3,4-Methylenedioxymethamphetamine (MDMA), for treatment-resistant conditions since 2014; there is evidently a need for this with 100 clinicians authorised to prescribe psychedelics (Liechti et al., 2025). In all of these jurisdictions, compassionate access to psychedelics provides crucial support to patients facing profound existential distress, helping to alleviate mental health symptoms and improve their quality of life. In the United Kingdom, the illegality and scheduling of psilocybin mean legitimate access is severely limited despite evidence showing that this classification hinders research (Howard et al., 2021) and calls for rescheduling to make it more accessible for medical research (Nutt et al., 2024; Rucker, 2024; Rucker et al., 2018). One consequence of this is a lack of insight into the use of psilocybin by cancer patients.
So far, clinical studies have demonstrated significant benefits of psilocybin for individuals living with cancer. One trial, using PAT for 12 participants with advanced-stage cancer-induced anxiety, showed significantly reduced symptoms of anxiety both one and three months after their second dose (Grob et al., 2011). A larger trial of 51 participants with life-threatening cancer diagnoses reported significant reductions in anxiety symptoms both immediately after PAT and six months later (Griffiths et al., 2016). A randomised double-blind control trial conducted by Ross et al. (2016) investigated the combination of psilocybin and psychotherapy for 29 participants with cancer-related anxiety and depression. Anxiety and depression symptoms were significantly reduced for up to 6.5 months following psilocybin plus psychotherapy treatments. Participants received a single psilocybin dosing session (0.3 mg/kg) or one dosing session of an active control (niacin 250 mg), in conjunction with psychotherapy. Psychotherapy followed the psychedelic-assisted psychotherapy framework rooted in the three-phase structure first used by Hoffer and Osmond in the 1950s and later systemised by Stanislav Grof (Grof & Halifax, 1977). This included (i) Preparatory sessions to build the therapeutic alliance, to educate on setting intentions, (ii) Dosing sessions in a clinically monitored, non-directive environment, and (iii) Post-dosing integrative psychotherapy to process the experience, derive meaning, and support lasting behaviour change. Although the crossover design makes it difficult to isolate the clinical effects of psilocybin, the active control, and the psychotherapy, the significant effect does clearly suggest the potential of psilocybin for improving the mental distress experienced by individuals with cancer.
A long-term follow-up was conducted with 15 participants from the Ross et al. (2016) trial three- and four-years post-trial. Both at the first and second follow-up, significant reductions in cancer-related anxiety, depression, and hopelessness were largely sustained. Notably, 71%–100% of participants attributed positive life changes to the PAT experience (Agin-Liebes et al., 2020). Thirteen participants also took part in qualitative interviews, providing their experiential perspectives. Interpretative Phenomenological Analysis (IPA) showed that participants described their psilocybin sessions as immersive experiences, with insights and visions felt as lived experiences. Central themes were reconciliations with death, acknowledgment of cancer’s place in life, and confidence in the face of cancer recurrence. Interestingly, participants noted a sense of meaning and perspective in their lives that was higher than before their cancer diagnosis (Belser et al., 2017; Swift et al., 2017). This newly found confidence and perspective echoes findings of earlier research into strategies for managing illnesses, in which normality and positive thinking were found as important strategies for those living with a chronic disease (Lewis et al., 2016). Additionally, two open-label studies have reported safety with psilocybin-assisted group therapy for participants with cancer-induced depression, also reporting possible efficacy (Agrawal et al., 2024; Lewis et al., 2023).
Despite limited research, small participant numbers, and treatments that also include active controls and psychotherapy, generally positive findings have emerged following treatment with PAT for individuals living with cancer-related mental illness and distress. Multiple clinical trials have demonstrated sustained reductions in depression, anxiety, and existential distress among cancer patients (Bellman, 2024). Combined with wider professional and social narratives centred on the potential application of psilocybin in treating mental health disorders (Daniel & Haberman, 2018) and the emerging social acceptability of PAT (Plourde et al., 2024), there is a need to conduct further research. Currently, understanding of the potentially positive impact of psilocybin per se, both short and long term, and the lived experiences of taking psilocybin in clinical or medical trial contexts has been reported, but little is known about experiences outside of these contexts. Accordingly, there is a clear gap in understanding the journey towards using or not using psilocybin through the lens of individuals who have seemingly overlooked the legal implications of accessing an illegal substance, perhaps feeling they are making a ‘rational choice’ given their current circumstances (Cornish & Clarke, 2002). Lived experiences, broad decision-making processes, perceptions of societal and self-acceptance of psilocybin, and the impact or otherwise of legality and perceptions of using illegal drugs despite reported benefits have yet to be fully explored (Plourde et al., 2024).
A growing interest in PAT to treat existential distress experienced by individuals living with cancer has important public health implications but is hindered by lack of legitimate access to psilocybin and limited access to clinical trials (Plourde et al., 2024). The current study aimed to understand the experiences of cancer patients who have used or who have considered using psilocybin to manage their mental health symptoms.
Method
IPA is a qualitative approach which aims to provide detailed examinations of personal lived experience. Rather than being prescribed by pre-existing theoretical preconceptions, IPA is committed to the exploration of human lived experiences, and accounts of lived experience are presented in their own terms to fully understand how humans make sense of their experiences (Fieldsend & Smith, 2022). This methodology is particularly useful for examining topics which are complex, ambiguous, and emotionally laden (Smith & Osborn, 2015). As such, the research team felt that IPA lent itself to understanding the lived experiences of individuals in relation to their cancer diagnosis and consideration of psilocybin. IPA further enables the researcher to move towards understanding how individual participants make sense of their experience but also the discovery of both patterns, similarities, and any divergences between participants (Fieldsend & Smith, 2022).
Participants
Based on the prevailing literature on IPA, a sample of between six and eight participants was appropriate (Smith et al., 2022). Small sample sizes are desirable in IPA because of its idiographic approach; an in-depth, detailed exploration of individual experiences does not allow for large sample sizes (Smith, 2004; Smith & Osborn, 2015). Participants were eligible to take part if they were over the age of 18 years, had a current or previous (self-reported) cancer diagnosis, felt they had experienced mental health problems in relation to that diagnosis, and had used, or considered using, psilocybin. Purposive and snowballing techniques were used to recruit participants. The study was advertised widely via social media and via contacts of the research team; JCN is an experienced drug science researcher, and potential participants were invited to contact the research team if they were interested in taking part. Further information was provided to anyone who expressed interest in participating in the study. Seven female participants were interviewed. Participants were aged between 35 and 61 years, and all self-reported a current diagnosis of cancer and experiences of poor mental health post-diagnosis. Four of the seven participants reported having taken psilocybin.
Data Collection
Following an expression of interest, a time and date was agreed between the participant and researcher to conduct the interview. A semi-structured interview guide was used to facilitate the interviews; this was developed by the research team to answer the research question and with reference to the existing literature on the topic. The guide included questions around participants’ experiences of mental health post-diagnosis, their knowledge and discovery of psilocybin, exploration of experiences of using or consideration about using psilocybin and its effects (if applicable), and their thoughts about the legality of psychedelics. The guide allowed the interviewer RVD to engage with participants using open-ended questions and prompts that were modified according to responses. All interviews were conducted online via Microsoft Teams or Zoom and were digitally audio recorded. Interviews lasted for up to 1 hour.
Analysis
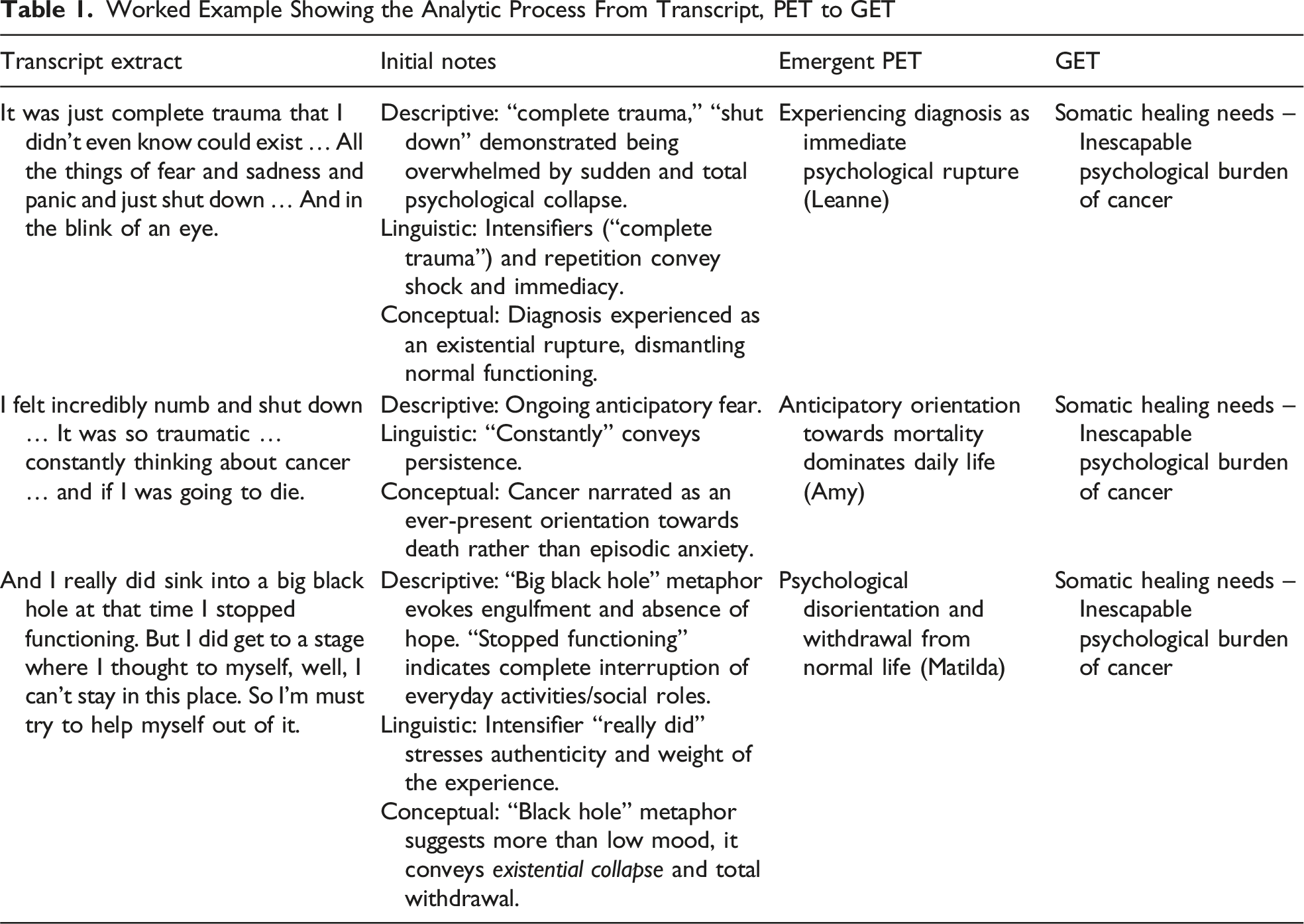
Worked Example Showing the Analytic Process From Transcript, PET to GET
Reflexivity
The authors of this manuscript consist of students with a background in psychology but with no previous experience or knowledge of psychedelics. Two of our team are psychologists: one actively engaged in drug science research, bringing a practical understanding of current research, and the other who has previously conducted qualitative research related to psychedelics. We were also joined by an experienced psychopharmacologist with a particular interest in psychedelic drug policy and research. The primary analyst (ZK) joined the project after data collection had been completed and held no prior relationship with any of the participants. Although IPA traditionally encourages researchers to conduct their own interviews to understand participants’ life worlds, separating the interviewer and primary analyst may offer methodological advantages by providing a distinct and valuable point of entry into the hermeneutic circle, enabling analytical distance and allowing the data to be approached afresh. However, in keeping with IPA’s iterative movement between parts and whole, reflexive engagement was maintained throughout; field notes taken during and after the interviews and dialogue with the wider research team, including the author (RVD) who conducted the interviews, supported interpretation by considering our sense-making of the data to ensure GETs were rooted in the lived experience of participants.
Ethics
Ethical approval for this research was granted by The University of Manchester Ethics Committee (Reference: 2022-13076-22966). All participants were provided with a study information sheet and provided informed consent prior to taking part. Consent was obtained by the interviewer (RVD). Given the legal status of psilocybin, participants were reassured their participation was confidential but advised not to disclose any details of how they had obtained, or potentially would obtain, psilocybin in the future. Any identifying information was removed during transcription to maintain participant confidentiality. A distress protocol was in place to support any participant who became upset during the interview; however, none did. Nevertheless, a debrief form was provided to all participants signposting them to relevant support should they require it at a later date.
Results
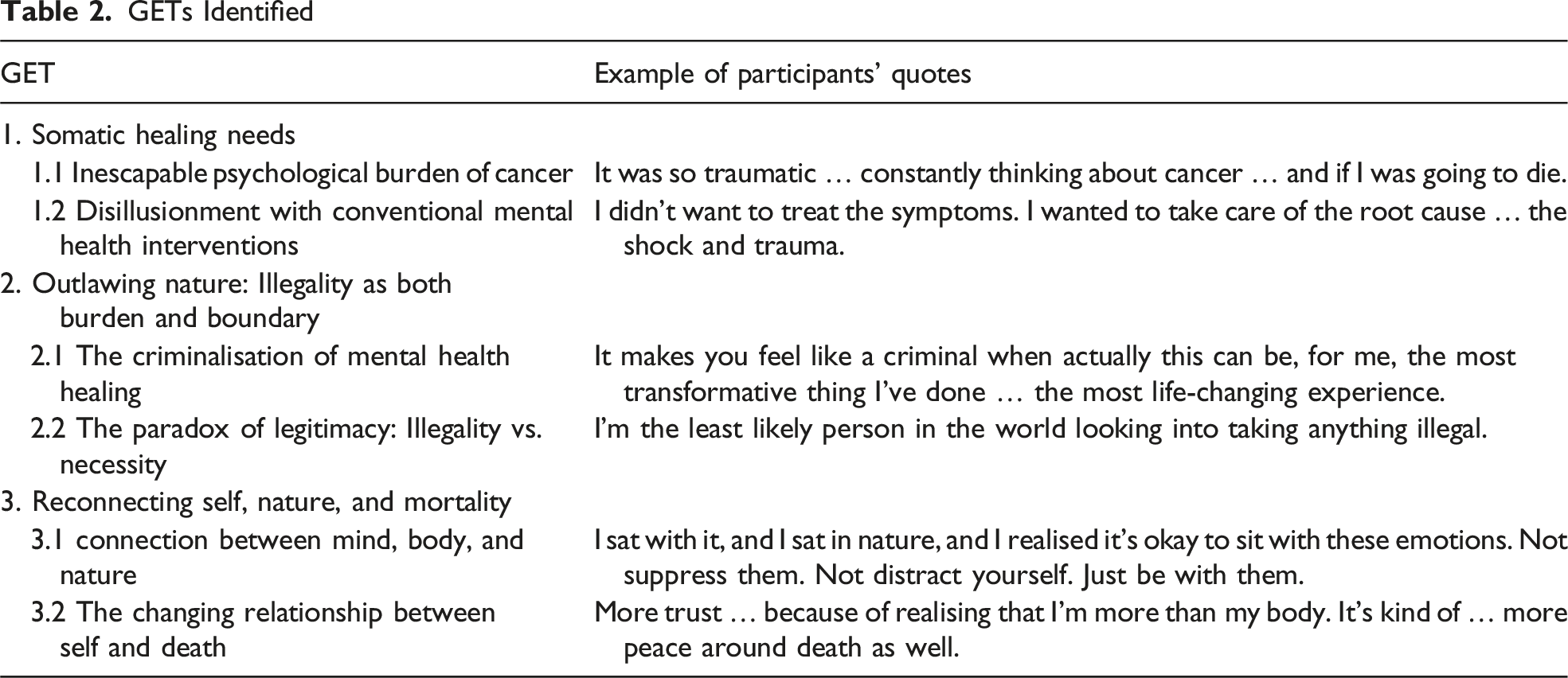
GETs Identified
Somatic Healing Needs
Inescapable Psychological Burden of Cancer
The psychological impact of a cancer diagnosis, particularly in relation to the acceptability of psilocybin as a therapeutic intervention, was identified as a central theme. It explored how participant’s psychological responses to their diagnosis informed their openness to alternative healing approaches, like psilocybin. For some participants, the psychological consequences of receiving a cancer diagnosis were immediate and all-encompassing. Leanne reflected, “It was just complete trauma that I didn’t even know could exist … All the things of fear and sadness and panic and just shut down … And in the blink of an eye.” Unlike mental health conditions stemming from relational or psychosocial stressors, this distress was uniquely anchored in a very real and immediate physiological threat. Like Leanne, Amy referenced a ‘shut down’: “I felt incredibly numb and shut down … It was so traumatic … constantly thinking about cancer … and if I was going to die.” For Amy, the diagnosis triggered what she described as a persistent orientation towards death not just episodic anxiety.
Echoed across participants was a profound sense of psychological disorientation. Matilda reflected, “And I really did sink into a big black hole at that time. I stopped functioning.” This suggests an emotional collapse and her use of metaphor – a black hole – speaks to the void she felt post-diagnosis, the complete psychological withdrawal from her previous life, similar to the ‘shut down’ referenced by Leanne and Amy. Stephanie described post-traumatic stress disorder (PTSD)-like symptoms, saying she was “quite traumatised. I had things like disassociation from my body, that kind of thing. And yes, slightly low mood. So maybe you’d say and I did have some flashbacks. So I guess there was PTSD.” Stephanie suggested it was not the cancer but the uncertainties that surfaced following diagnosis, which distressed her. The use of the term dissociation paints a chaotic picture. Everyday moments, even time with loved ones, became shadowed by thoughts of cancer. Zoe described her fear of emotional intimacy, as though loving too deeply might exacerbate future pain: “I was too scared to love them too much, I suppose, because I was aware of the possible possibility of loss.” For many women, the emotional experience was not merely sadness or anxiety, but a loss of psychological coherence – a fear that the future had evaporated. The cancer diagnosis created a temporal shift; life became divided into ‘before’ and ‘after’, and the ‘after’ was marked by a fundamental destabilisation of the self.
Despite the profound psychological turmoil they faced, several women resisted framing their distress through psychiatric or diagnostic language. Rather than viewing their distress as symptomatic of a mental health condition, they understood their emotions as proportionate responses to the magnitude of their diagnosis. Leanne expressed this insight: They were all just signs that my body were giving me that I want to live and I want to be here … So I wouldn’t necessarily call it mental health issues, I would call it my body just giving me all the emotions that I would expect to face.
She continued, “That’s exactly what my body should have felt at the time. If it didn’t, I would have been worried … I would have been labelled as anxiety and depression, but they’re just labels.” Zoe also rejected psychiatric interpretations of her distress following a cancer diagnosis, saying, she “didn’t think [she] was depressed.” For these women, the emotional suffering was acknowledged as part of what it means to live with cancer and this narrative challenged the medicalisation of distress.
Disillusionment With Conventional Mental Health Interventions
Participants consistently reported that mental healthcare was either absent, tokenistic, or profoundly misaligned with their needs. Amy reflected on the lack of even basic acknowledgement of her distress, saying: Looking back, I kind of can’t believe nobody ever asked me how I was … I got a very brief like, how are you and I walked into the room but I didn’t ever get a proper kind of how are you coping, how is your mental health.
Similarly, Louise recalled being dismissed when she sought psychological support from the palliative care team: But you’re not dying yet. But obviously I have been told I have a terminal illness so I was really anxious about that and I really wanted to talk to someone about that and like what happens. So they said you can talk to somebody about in that six months so yeah. Then what did I do? I think I was just on my own.
These accounts illuminate a system where mental health suffering following a cancer diagnosis is not only deprioritised but, in some cases, actively invalidated.
Conventional psychological support, when accessed by some, was also felt to be misaligned with the depth and urgency of need. Louise described feeling emotionally constrained and unable to authentically express her fears during counselling: “You aren’t allowed to be afraid of dying, you can’t have any of the feelings … It’s amazing how difficult it is to find a place where it is okay to talk about dying … it seems to be a taboo.” Others echoed this, describing short, impersonal sessions and prolonged wait times that clashed with the immediacy of their distress. Stephanie recalled a “three-month waiting list,” while Leanne said she felt “in a worse place after talking.” What set their experiences apart was not only the intensity of distress but the temporality underpinning it. For some participants, slow-progress interventions – long waitlists, trialling therapists, or building rapport – felt like luxuries they could not afford. Zoe explained, “trying to find someone you click with” was not feasible within the time pressures of a cancer diagnosis.
Many women were also disillusioned by the automatic offering of antidepressants, which many perceived as reductive and emotionally invalidating. Zoe expressed frustration at how readily these were prescribed: “[They were] prescribing antidepressants, like Smarties.” This metaphorical comparison of antidepressants to a widely available and easy-to-consume sweet highlights the casualness with which medication was dispensed and stood in stark contrast to the complexity of what participants were navigating. For Louise, this mismatch was particularly stark: “I didn’t want to treat the symptoms. I wanted to take care of the root cause… the shock and trauma.” There was a clear yearning for support to process the experience. Distress was not a disorder to be treated, but a message to be listened to, as Louise summarised: “I am a believer that if your body has symptoms, it’s trying to communicate with you and just sometimes just a bit of space and silence, still attending to those parts of yourself.” Matilda further explained: “I didn’t really want to feel any more numb.”
This rejection of medication was not only philosophical but also practical. Matilda explained that she did not “believe in just taking medicine for medicine’s sake” and Louise shared: “I’m on a shed load of meds… I just get overwhelmed with it.” The term ‘shed-load’ here refers to a large quantity of medications, suggesting that Louise, like Matilda, was already managing multiple treatments and felt overwhelmed by the prospect of adding more to her routine. For some, concerns extended to drug interactions, while others cited personal or vicarious experiences that eroded their trust in pharmaceutical care. Zoe recalled the suicide of a loved one who had been taking antidepressants, saying, “It didn’t seem to be working. In fact, it seemed to be making him feel worse.” These accounts revealed not only a sense of emotional incompatibility but a very real logistical barrier: participants were already navigating polypharmacy, and the thought of additional pharmaceutical drugs added to their distress rather than alleviating it.
Outlawing Nature: Illegality as Both Burden and Boundary
The Criminalisation of Mental Health Healing
The women’s reflections about psilocybin were not limited to its therapeutic potential; they were entangled with frustration over its legal status, especially as a natural substance: “The legalities of natural products is ridiculous. I think it’s unnecessary and I don’t actually know why they would make [psilocybin] illegal.” (Matilda). Matilda’s reflection specifically questioned how something natural could be policed. Leanne articulated that she felt she could be more trusting of psilocybin because it’s a natural substance, saying, “If it’s natural, and it’s grown in the world, it hasn’t been fiddled with… you can definitely be more trusting of it.” Across participants, psilocybin was often contrasted with conventional pharmaceuticals in this regard: “That’s the crazy thing – I can go to my GP and get an SSRI prescribed to me with very little conversation … but something like this, which felt like a more organic solution, is just harder to get.” Her narrative underscores what a contradiction she considered this to be: the system readily offering pharmaceuticals with known side effects but criminalising a naturally occurring substance.
Participants did not describe their interest in psilocybin as oppositional or transgressive; rather, they described it as a considered response to unmet emotional needs. Stephanie encapsulated this tension powerfully: “It makes you feel like a criminal when actually this can be, for me, the most transformative thing I’ve done … the most life-changing experience.” Her words reflect a jarring dissonance between what psilocybin offered her and what the law suggested it was by the nature of it being illegal (i.e., unsafe and untrustworthy). Amy also clarified, “I just have to really know what my intention was and why I was doing it … Not like just recreationally for fun … When I was facing that kind of anxiety, trauma when I was in such a shutdown, say, I would definitely, you know, if there was a legal option, I would have gone with that.”
Some participants drew striking comparisons to highlight the harms of illegality. Stephanie likened the illegality of psilocybin to “backstreet abortions” – a powerful metaphor highlighting how criminalisation pushes people towards hidden, potentially dangerous routes. Others shared this unease, not out of moral conflict but because of the unpredictability and lack of regulation that illegality introduced. Louise described the lingering anxiety that came with accessing something she believed could help: You have some anxiety in the back of your mind that this is not a legal drug … it would be nicer if there wasn’t any of those anxieties, so you could get quality, possibly lab-tested [psilocybin], and not get into trouble with the law.
For her, the concern was not about wrongdoing but safety – the emotional labour of healing was already immense, and the added risk of illegality only compounded this burden.
For many, criminalisation was not just a legal barrier but a philosophical affront, a denial of their right to choose a healing path that felt congruent with their beliefs and needs. Stephanie reflected, “They want to create drugs that people are on for life … antidepressants. But then maybe one, two or three sittings [of psilocybin] can already create changes. It’s almost like it can’t be patented.” These reflections suggest that illegality was not interpreted as protection but as preservation of power, profit, and pharmaceutical orthodoxy. Several participants shared similar thoughts to Stephanie, such as Amy: “I feel really angry. Genuinely, I feel really frustrated … I just think when you’re already facing so much and potentially end of your life, and there’s something that could take away that fear.” Participants were not simply rejecting conventional medicine; they were questioning the authority that defines what healing should look like. In this way, the criminalisation of psilocybin was experienced not only as misinformed but as fundamentally misaligned with their lived experience and what they instinctively trusted to help them heal.
The Paradox of Legitimacy: Illegality Versus Necessity
While psilocybin’s criminalisation provoked frustration, it did little to deter most of the women from seriously considering, or even pursuing, its use, but it did introduce practical and emotional complexities. Louise articulated this, explaining her anxiety was not about criminal consequences but about “not knowing what dose you were getting.” It forced participants to conduct personal research, rely on unverified sources, and navigate their options in isolation. Matilda expressed this sense of disconnection: “I just don’t know anybody in this country. It’s a pretty big thing to do.” Several women sought out lived testimonies rather than scientific literature, placing value on experiential narratives as a way of reclaiming agency in a system they felt had excluded them. Zoe explained, “I suppose I’m more interested, really, to make a decision, in hearing about experiences and effects rather than actually looking at the science.” For her, healing was not a clinical protocol but an embodied, human process, one that required community, not clinical detachment.
The conflict between law and need also created internal moral tension. Zoe, who described herself as “the least likely person in the world looking into taking anything illegal,” acknowledged that the promise of psychological relief outweighed the taboo. Stephanie, who travelled abroad for her experience, echoed this: “I really needed this process to heal.” Women did not describe their consideration of psilocybin as an act of rebellion but as an attempt to address distress that they felt was unmet by existing care routes. Louise, describing her second cancer diagnosis, said, “I had stage four recurrent so I [had] two big hits, so both were really tricky and traumatic, the second one was devastating but at the time I asked for some counselling through the NHS and I was told the waiting list was too long so there wasn’t really anything in the mainstream system I mean there are charities but that’s it.”
Yet, even as participants expressed frustration at psilocybin’s illegality, their hopes for legalisation were tempered by scepticism and in some cases, diverged. For Stephanie, psilocybin should be ‘definitely legalised’ as she felt that keeping it prohibited “kind of creates this backstreet thing which leads to a lot more harm.” Louise expressed a similar concern about the risks created by prohibition, explaining that “it’s absolutely a barrier in terms of sourcing it.” For both women, legalisation represented safety and legitimacy, but for others, such as Amy and Leanne, there were concerns about legalisation, worrying that bringing psilocybin under government regulation and pharmaceutical control would strip it of the very qualities that made it feel safe and sacred. Amy cautioned, “If it goes that way, then it just becomes like a gold rush money kind of space.” Leanne voiced similar unease: “What I worry about if it gets legalised is that they forget about the preparation, the setting, the music, the integration. I don’t think government or big funders should be involved.” Both comments reflected a fear that medical or corporate control could overly-medicalise its therapeutic use and reduce psilocybin to dosages and protocols at the expense of the contextual elements that participants valued. For these women, legalisation was not simply about access, but about preservation of ritual, context, and emotional depth. Although Louise had previously described the need for legalisation, she echoed these reservations, explaining, “Often legalisation can lead to standardisation. Then we can lose some of the good stuff.” Together, these reflections reveal a central tension: while illegality created practical and ethical barriers, legality was also felt to risk diluting the meaning and transformative potential of the experience itself.
Reconnecting Self, Nature, and Mortality
Connection Between Mind, Body, and Nature
Across interviews, most women repeatedly described a need not just for healing but for reconnection with themselves, with nature, and with something larger than their diagnosis. As Leanne put it: I had to go into those emotions rather than avoid them. Because that’s what I’d done my whole life. And it wasn’t working. So I did the complete opposite. And instead of suppressing and repressing even more I was like no … It’s really hard to process them but these emotions will pass.
Her words capture a pattern echoed by others that the trauma of cancer left them seeking ways to bridge a gap between feeling, body, and identity, and participants sought ways to close this gap. Psilocybin, whether through direct experience or anticipated possibility, was understood as a bridge back to wholeness. Amy described this clearly: Psilocybin for me is so powerful that it can help you experience this mystical experience. And within that, there’s so much healing … it was like, one of the top five most meaningful experiences of my life … It’s definitely reduced the fear, reduced the anxiety, all of that. That’s all very much kind of, to the disease. But I think just me as a person is also shifted just how I am in the world … feeling much more connected to nature … like giving much more love and letting myself receive much more love and just being so grateful for being alive.
Even before encountering psilocybin, many women spoke of a deep and often subconscious gravitation towards nature and somatic healing. Sophie explained how her search for physical healing gradually led her into the world of plant medicine: I’d gone to a herbalist and started taking herbal teas and stuff … and then started learning more about plant medicine. And then as you do, you kind of then very quickly get to mushrooms … and then you just, the next step then is to find out, okay, hey, actually, they help with mental health as well.
This pull was not always intentional, but instinctive, a quiet urge towards something that felt safe, trustworthy, and grounding. For others, the shift towards nature was even more subtle, something their body moved towards without them realising. Amy described how walking outside with her brother’s puppy became unexpectedly transformative: “I inherited my brother’s six-month-old puppy that made me just get out and walk every day. And that was really good for me.” Here, the act of walking was not prescribed or planned; it was simply something Amy’s body and mind moved towards, without her needing to name it as healing. These accounts illustrate how reconnection was often sought instinctively through nature and embodied practices long before participants considered psilocybin.
Nature was perceived as a source of wisdom, as sacred, unrefined, and emotionally congruent, a stark contrast to treatments that felt industrialised or emotionally disembodied. Leanne explained, “I trust nature much more than I trust something that’s been made synthetically, that is … mainly for profit.” This foundational trust in nature helped explain participants’ acceptance of psilocybin; Louise reflected on this, stating, “I have a lot more fear around other things … psilocybin makes sense because it’s natural. It just feels like something you can trust.”
Among those who had taken psilocybin, the experience itself was framed not only as clarifying but deeply spiritual, a journey inward that allowed for emotional release and reconnection with self and world. Leanne described her ceremony as a space to fully feel: “The first three hours, I was just crying – a cathartic cry … such a relief.” She went on to explain how this experience allowed her to reframe emotion itself: “I sat with it, and I sat in nature, and I realised it’s okay to sit with these emotions. Not suppress them. Not distract yourself. Just be with them.” Rather than detaching from distress, psilocybin helped these women re-inhabit their own experiences and connect their body and mind through nature. Stephanie described it as “a big sense of peace … almost like an inner peace that all of the things that we kind of worry about faded away.” Louise described moments of acute beauty and emotional restoration: “Where you could see the beauty in the world and feel forgiveness.” The experience offered a kind of clarity and spaciousness: a pause in the chaos, and a felt sense of being whole again.
Even those who had not taken psilocybin, such as Zoe, described an embodied belief in its potential: “I think it’s got immense potential from everything I’ve heard, provided that it’s taken in the right context.” Her hesitation was not rooted in disbelief but in access. Her phrasing of “context” echoed a recurring point: that healing was not just about the substance but about the setting, intention, and meaning that is brought to the experience.
What unites these accounts, both experiential and anticipated, is a shared longing for reconnection. Psilocybin was not perceived as an external fix but as a way to work with the body and the self. Participants felt that their gravitation towards nature was a rational and intuitive response to trauma, a reclamation of agency.
The Changing Relationship Between Self and Death
Those who had taken psilocybin described how it changed their relationship with death: “There is still fear … it doesn’t cripple me” Leanne said. Although the women’s prognosis had not changed, their relationship with the uncertainty had. Amy described the effect of her experience as immediate and liberating: “That huge weight … lifted off me. Not having that crippling fear anymore.” That both Leanne and Amy spoke about the ‘crippling’ nature of the fear is worthy of note; it’s suggestive of how intense this fear was and how their experience with psilocybin softened this. For Stephanie, the experience brought her into a profound state of ease with her body and mortality: “More trust … because of realising that I’m more than my body. It’s kind of … more peace around death as well.” The experience provided a form of transcendence, not in a mystical or escapist sense but as a reordering of perspective. It allowed death to exist without dominating. For those who had not taken psilocybin, the hope was not for transcendence but for the possibility of encountering that same shift: I suppose it seems remarkable that for some people, it only seems to take one experience, one dose to have an effect. And I think it's just really interesting, it’s contrast with … antidepressants, that [they] would numb things and make me feel not me. And that people report having an expanded consciousness and of feeling more at one with everybody else, or with the universe is really quite appealing because of that sort of detachment [that I have]. (Zoe)
With psilocybin, these women seemed to find something that traditional care rarely offered: a space to encounter death spiritually, emotionally, and honestly. These insights were not framed as revelations but as returns to clarity, to calm, and to what participants described as truth. Louise reflected, “You can’t un-experience it … it’s just a mind-opening experience.” This sense of irreversibility was repeated across accounts: what had been gained through psilocybin could not be undone; it had become part of how they understood themselves. Leanne felt strongly that she could “have never been able to get close to the somatic release [she] felt after taking psilocybin] in a lifetime of therapy.” For these women, healing involved sitting with the unspeakable and surviving it.
Discussion
Seven individuals who had a current or previous diagnosis of cancer, who experienced poor mental health in relation to that diagnosis, and who had used or considered using psilocybin participated in qualitative interviews. The interviews aimed to explore participants lived experiences, broad decision-making processes, perceptions of societal and self-acceptance of psilocybin, and the impact of its illegality. IPA resulted in the identification of three overarching GETs: Somatic Healing Needs; Outlawing nature: Illegality as both a burden and boundary; and Reconnecting Self, Nature, and Mortality. These GETs collectively shed light on how participants made sense of their psychological distress in the wake of cancer, why conventional support systems often felt inadequate, and why psilocybin, particularly due to its natural origins, was seen as a compelling alternative. This study makes a novel contribution to the current literature by focusing not on clinical trial participants but on those navigating decisions around psilocybin in real-world, unregulated contexts. Participants described psychological needs that extended far beyond the physical or medical consequences of their cancer diagnosis. Although they encountered substantial distress, including disconnection from their bodies, loss of identity, and fear of death, they frequently reported that these experiences were misunderstood or neglected within existing care pathways. Mental health support was often considered either absent, superficial, or framed in ways that did not align with their lived realities. Participants described an urgent need for healing that was not necessarily about ‘treating’ a disorder but about making sense of their suffering. This aligns with existing literature on existential distress in cancer care, which highlights how psychological suffering among oncology patients often goes unrecognised when it does not fit neatly into diagnostic categories (Boston et al., 2011).
Psilocybin was considered within this context, not as an escape or miracle cure but as a potential avenue for accessing meaning, perspective, and emotional reconnection with traditional mental health treatments, particularly antidepressants, not felt to meet their needs. These views are echoed by existing critiques of SSRIs in oncology, which suggest that they are frequently prescribed with little evidence of effectiveness in managing cancer-related depression or distress (Okuyama et al., 2017). By expressing aversion to conventional antidepressants and emphasising the necessity of alternative, integrative therapies, participants voice the need for treatments that resonate with their complex and dynamic needs (e.g., Andersen et al., 2007; Bultz & Carlson, 2006; Holland et al., 2007; Spelten et al., 2003). This movement away from conventional medicine is a very interesting aspect of our findings which deserves further exploration in subsequent studies. Participants’ accounts call for a reframing of psychological support in cancer care, from an approach that centres symptom reduction to one that validates emotional pain as a rational and even essential response to navigating life under the shadow of illness.
Crucially, participants’ openness to psilocybin appeared to be rooted in this desire for a different kind of healing. Their trust in psilocybin was intimately connected to its perceived naturalness. Participants described a deep-seated belief that, as a natural and historically sacred substance, psilocybin offered something more trustworthy and congruent than synthetic pharmaceuticals. This view resonates with literature on the ‘naturalness bias’, the tendency to view natural remedies as inherently safer, more authentic, and more ethically sound (Blaschke, 2017; Ji et al., 2023; Rozin et al., 2004) Existing literature has argued that such views are not simply irrational beliefs but reflect a deep societal distrust of systems perceived to be driven by profit or industrial interests (Lamberty & Imhoff, 2018; Mao et al., 2022). In this study, participants’ trust in psilocybin emerged from a sense that natural substances were aligned with the body, the earth, and healing, while pharmaceuticals were seen as impersonal, commercial, and emotionally numbing.
Participants described an almost instinctive gravitation towards natural environments, somatic practices, and holistic modalities, before they had encountered psilocybin. This reflected a broader longing for healing that addressed the whole person versus the symptoms. Psilocybin appeared to sit within this framework as a logical extension of a worldview already oriented towards natural and embodied forms of care. Participants expressed a need to experience connection between their bodies (what they were experiencing physically) and minds (thoughts and fears in response to the diagnosis). Fearing their mortality was a key factor in their consideration of psilocybin. For those who took psilocybin, it facilitated emotional catharsis, existential clarity, and a sense of peace in the face of death. This aligns with previous research demonstrating psilocybin’s capacity to reduce death anxiety and foster spiritual or mystical experiences in patients with life-threatening illness (Belser et al., 2017; Griffiths et al., 2016; Malone et al., 2018; Ross et al., 2016). This has been related to the potentially ontological challenging nature of a psychedelic experience. Described as a ‘liminal stage’, a psychedelic experience can be seen as creating a mental state in which established beliefs and identities dissolve, challenging the sense of self and reality and ultimately catalysing transitions in the ways individuals situate themselves within their existential reality (Argyri et al., 2025).
However, the findings illustrate the moral and legal dilemmas faced by participants. Their frustration around the illegality of psilocybin centred around their understanding of the substance as natural and, therefore, trustworthy, but some participants also experienced internal conflict, not wanting to break the law but also feeling they needed mental health treatment. These findings mirror other studies that highlight how prohibition exacerbates the psychological vulnerability of those seeking psychedelic care (Pilecki et al., 2021). Indeed, evidence shows that underground psychedelic use can expose individuals to psychological risks and adverse events due to the absence of screening, supervision, and integration support available in clinical settings (Simonsson et al., 2023). While illegality did not prevent most from considering or using psilocybin, it introduced significant logistical and emotional burdens, including the need to conduct their own research, navigate unregulated spaces, and manage fears around sourcing and safety. Notably, not all participants experienced moral dilemmas regarding the potential breaking of the law and felt that mental health and wellbeing were more important than the legal status of psilocybin. The study demonstrates that, for these individuals, psilocybin was considered a potential treatment, a natural substance offering hope in the face of mental health problems and limited alternatives. This is aligned with the growing body of research and clinical trials demonstrating the efficacy of psilocybin in treating depressive symptoms. Psilocybin has shown positive results in treating both major depressive disorder (MDD) and TRD in Phase II trials, particularly in patients who have not responded to conventional treatments (Aaronson et al., 2025; Davis et al., 2021; Goodwin et al., 2022; Gukasyan et al., 2022; Raison et al., 2023; von Rotz et al., 2022). These results are indeed promising, and larger Phase III trials will be important to confirm clinical efficacy. Indeed, at the present time, psilocybin, LSD, and MDMA are being tested for the treatment of MDD, generalised anxiety disorder, and PTSD, respectively, in Phase III trials (Liechti et al., 2025).
At the same time, in this study, legalisation was not unanimously welcomed with concerns raised about the impact of regulation. Participants discussed the importance of the wider experience when taking psilocybin (e.g., the setting, connection to nature, and music) and worried that this process could be lost. These concerns speak to the importance of ensuring that future models of psychedelic-assisted care remain attentive to preparation, setting, integration, and the values of the people they serve (Noorani, 2021). Further exploration of how distrust in conventional medicine shapes engagement with unregulated psilocybin use is critical for developing safe, equitable, and context-sensitive models of care. In addition, careful monitoring and transparent reporting of adverse events remains essential (Marrocu et al., 2024; Schlag et al., 2022). These perspectives also raise important public health considerations; while participants’ scepticism towards the medicalisation of psychedelics reflects an understandable desire to protect the relational and spiritual integrity of these experiences, research cautions that rejecting regulated frameworks may inadvertently increase psychological and physical risk (Hinkle et al., 2024; Schlag et al., 2022). Rather than advocating for or against legislation, the present findings highlight the need for nuanced frameworks that preserve the relational, contextual, and spiritual dimensions of psychedelic healing while mitigating potential harm in unregulated use (Schlag et al., 2022).
Limitations
This study reports data from a vulnerable and hard to reach population, and so necessarily included both participants who had taken psilocybin as well as those who were seriously considering it. Arguably, the sample would have been more homogenous by including only those who had taken psilocybin. However, we felt the inclusion of those who were also considering taking it was important when exploring the acceptability of the substance to this group of participants and how they made sense of this. Nonetheless, there appeared to be similar attitudes and feelings regarding the use of psilocybin and the illegality of the substance. The sample was also self-selected, and so those who volunteered to take part may have been particularly engaged or positively inclined towards psychedelics and therefore may have had particularly strong opinions that differed from those that did not volunteer. Consequently, the experiences of these participants are not necessarily representative of people more generally who have experienced cancer. We also did not collect information about the psilocybin sessions participants experienced or wider demographic information given our focus was understanding individuals’ experiences. Our study is exploratory in nature, and so future research should seek to explore sub-sections of participant populations and work to engage with individuals with divergent experiences and attitudes towards the use of psilocybin in this context. Future work should also examine how prohibition and limited access shape patterns of underground or self-directed psychedelic use in oncology populations and the potential implications for patient safety and public health.
Conclusions
This qualitative study complements clinical data, reinforcing the argument for further research and policy reforms that could expand access to this promising treatment. Advocacy efforts, such as those led by the non-profit organisation TheraPsil in Canada, have demonstrated the practical feasibility of integrating psilocybin into medical care. TheraPsil secured legal exemptions for palliative care and cancer patients, setting a precedent for compassionate access to psilocybin. Building on these efforts, the federal SAP in Canada now permits licensed healthcare providers to prescribe psilocybin to individuals with serious or life-threatening conditions, including cancer-related distress, when conventional treatments prove ineffective or unavailable (Government of Canada, 2023). Such initiatives highlight the profound impact psilocybin can have on alleviating existential and psychological suffering, improving patients’ quality of life.
The current study provides one of the first qualitative accounts of the lived experiences, broad decision-making processes, and perceptions of psilocybin among individuals with cancer outside of clinical trial contexts. It extends existing literature by illustrating, for the first time, how patients outside clinical trials struggle with their need for healing in a system that does not readily accommodate their needs. Given this population’s evident unmet clinical need, a compassionate access scheme to improve the mental health of people with cancer seems timely.
Footnotes
Acknowledgements
The authors would like to thank the participants in the study for giving up their time and sharing their experiences with them.
Ethical Considerations
The study was approved by The University of Manchester Ethics Committee 5 (approval number 2022-13076-21741).
Consent to Participate
All participants provided written informed consent prior to taking part in the study.
Author Contributions
JCN and VW designed and supervised the study. RVD collected the data and contributed to the interpretation. ZK analysed and interpreted the data. SW prepared the initial draft of the manuscript, and all authors contributed to, read, and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCN is Chair of the Drug Science Medical Psychedelics Working Group, Chair of Trustees at Drug Science, a Trustee for Heroic Hearts UK, and Onaya Science and a scientific advisor for the Centre for Evidence Based Drug Policy. AKS is Head of Research of Drug Science. Drug Science receives an unrestricted educational grant from a consortium of medical psychedelics companies. None of the authors would benefit from the wide prescription of psychedelic medicines in any form.