
Abstract
The diagnosis of a childhood brain tumor impacts the psychological well-being of parents who experience high levels of post-traumatic stress. To understand the etiology of trauma through this unique healthcare experience, a journey mapping exercise was undertaken with parents of children with brain tumor. Data were collected in an online focus group and by written responses. Framework analysis and research poetry were used to map experiences of traumatization and trauma-informed care across time. Nine mothers mapped their experience of their child’s brain tumor care describing their needs and responses. Findings are presented by eight milestones, supported by research poetry composed of participant quotes titled: “I must be wrong,” “All the fear, no answers,” “Paper Thin,” “Happy but Terrified,” “The Rest of Him,” “Less Than,” and “Into Our Destiny.” Throughout the trajectory of care, parents reported traumatic events and moments of helplessness attributed to the healthcare received, contributing to unrelieved distress. Increased transparency in communication between clinicians and parents fostered increased trust and psychological safety within healthcare services. Understanding the traumatization that occurs across the trajectory of care can inform service improvements and early linkage to specialized support. This study contributes novel understanding of traumatization for parents of children with brain tumor and depth in understanding of emotional components through the presentation of research poetry.
Keywords
The diagnosis and treatment of a child’s brain or central nervous system tumor is a life-changing event that impacts the well-being of both the child and their parents or carers (hereafter referred to collectively as “parents”; Price et al., 2016; van Warmerdam et al., 2019; Young, Cashion, Ekberg, et al., 2023). Parents are impacted by grief for the loss of their child’s imagined future, by distress at their child’s suffering, and by the additional caring role related to their child’s illness, treatment, and long-term effects (Price et al., 2016; van Warmerdam et al., 2019), as well as the increased needs of their other children (Pariseau et al., 2020). A child’s brain tumor diagnosis, treatment, and ongoing effects impact the entire family unit, both practically and emotionally.
A brain tumor diagnosis brings to parents’ minds the possibility of their child’s death or lifelong disability. Brain tumors in children (0–18 years) have the lowest 5-year survival rates of all childhood cancers in Australia (77% compared with up to 97% of children with lymphoblastic leukemia; Australian Childhood Cancer Registry, Cancer Council Queensland, 2023). For survivors, the tumor and treatment impact the developing brain, resulting in late effects that become evident years after treatment and interruptions to normal development (Young, Cashion, Hassall, et al., 2023; Young et al., 2021). Survivors face ongoing complications including seizures, hearing loss, and mobility issues, and a 260% increase in poor neuropsychological outcomes (Young, Cashion, Hassall, et al., 2023). These negative impacts compound over life stages, such that social, cognitive, and physical disabilities caused by the tumor and treatment can affect the child’s relationships, study, and employment opportunities as they become adults (Turner et al., 2009; Young et al., 2021, 2022). The ongoing effects of brain tumor significantly impact the parents’ caring roles and the organization of the family unit, contributing to mental health concerns in the child, their parents, and siblings (Litzelman et al., 2011; Moscato et al., 2022; Young, Cashion, Hassall, et al., 2023).
Following discharge from an intense period of hospitalization related to the diagnosis and initial treatment, parents experience new and continuing stress. These include complex feelings about dislocation from the hospital support system they know, confusion with navigating a new reality as they attempt to return to “usual” activities with their child’s newfound health issues or disability, and difficulty integrating with a social world that is not familiar with their needs (Peikert et al., 2018).
Although distress is an expected experience of a childhood cancer diagnosis, psychological responses range in type, severity, and longevity, with the potential for components to be processed as traumatic. Where an event is processed as traumatic, the individual can experience psychological and physiological responses to reminders or thoughts of the traumatizing event (Kassam-Adams & Butler, 2017; Price et al., 2016). The Integrative Trajectory Model of Pediatric Medical Traumatic Stress (the PMTS model) describes common traumatic stressors and responses for children and their families in the medical system (Kazak et al., 2006; Price et al., 2016). Events such as learning of the diagnosis, exposure to medical interventions (including procedures where parents have to “force” their child to comply; Forsner et al., 2023), witnessing suffering, and reminders of the threat of death can be processed as traumatic (Price et al., 2016).
Traumatic events may subsequently trigger a state of hyper-arousal, re-experiencing the event, and avoidance of reminders (Price et al., 2016). Hyper-arousal includes physical symptoms such as a racing heart, changes in appetite, shaking, and difficulty sleeping and psychological symptoms of hypervigilance and irritability (Miles et al., 2023). Re-experiencing includes re-living the event through intrusive memories and dreams (Prins et al., 2015). Avoidance can be physical, avoiding places or objects associated with the event, or psychological, attempting to detach from thought or emotion related to the event (Kazak et al., 2006; Price et al., 2016; Prins et al., 2015). These clusters of symptoms are categorized as post-traumatic stress symptoms (PTSSs; Kazak et al., 2006; Price et al., 2016). PTSSs are distressing in their own right and are a risk factor for progression to post-traumatic stress disorder (PTSD; Kazak et al., 2006; Price et al., 2016). Indeed, more than half (54%) of parents of children with brain tumors experience PTSD in their lifetime, the highest rate across pediatric cancers (Bruce, 2006).
The PMTS model outlines that an individual’s interpretation of a potentially traumatic event impacts whether PTSSs develop (Kazak et al., 2006; Price et al., 2016). Key components of a potentially traumatic event are the subjective perception that the event is a threat to life or evokes feelings of intense fear, horror, or helplessness, while objective factors such as illness severity and intensity of treatment are not strongly correlated with likelihood of developing PTSSs (Kassam-Adams et al., 2009; Kazak et al., 2006; Price et al., 2016). Importantly, traumatic responses can occur even when symptoms are below the threshold or timeframe for a formalized trauma diagnosis, and PTSSs can be considered on a continuum of the same symptoms that define traumatic stress disorders (Kassam-Adams et al., 2009; Kazak et al., 2006; Price et al., 2016). PTSSs are associated with treatment adherence as well as quality of life (Kassam-Adams & Butler, 2017). Identifying these symptoms early allows preventative measures and early intervention to be enacted.
Understanding healthcare experiences through a lens of trauma-informed care can enable suitable support for parents. Internationally recognized principles for trauma-informed healthcare (Huang et al., 2014) are utilized as guiding principles in trauma-informed cancer research (Davidson et al., 2023). These six principles incorporate (1) consideration of patients’ and families’ feelings of safety; (2) trust and transparency; (3) peer support; (4) collaboration and mutuality; (5) empowerment and choice; and (6) consideration of cultural, historical, and gendered trauma issues (Huang et al., 2014). The sparse literature to date related to parents of children with cancer has focused on their trauma-related needs at a single time point, usually after the completion of their child’s acute treatment (Alderfer et al., 2005; Baenziger et al., 2020; Kazak et al., 2005). A notable gap exists in understanding experiences of trauma-informed care and traumatization throughout the experience of medical care. Better understanding of these experiences enables interventions to mitigate the experience of traumatization. Thus, in this study, we explore parents’ perceptions of experiences of healthcare for their child’s brain tumor over time. The study aims to map common components of the experience to form a combined narrative. The analysis sought to answer two key research questions: (1) What signs of traumatization and PTSSs are experienced, and when? (2) Within the current model of care available, which principles of trauma-informed healthcare are experienced or breached?
This study informs a program of work with the goal to develop resources and interventions that address the needs identified.
Methods
Study Design
To map the healthcare experience of parents of children with brain tumors over time, this study utilized a multi-method qualitative, descriptive design. Qualitative descriptive methodology provides a straightforward, low-inference summary of participant experiences and is commonly used in health research where the goal is to stay close to the data and present findings using the participants’ words (Bradshaw et al., 2017). Multi-method qualitative research is commonly used to enrich the data through opportunities for participants to express opinions individually or in collective situations, and for group discussions to offer deeper contextualization (Lambert & Loiselle, 2008). As the experiences considered in this study were sensitive in nature, respect for individual preferences in recounting emotional experiences was considered when deciding to use a multi-method approach, allowing participants to choose how they contributed to the study.
Here, we outline the qualitative work which informed subsequent co-design processes (Rolfe et al., 2025). As such, the Needs and Aspirations for Design and Innovation model (NADI model; Dijkstra et al., 2015; van der Bijl-Brouwer & Dorst, 2014, 2017) was used as a theoretical framework to design the workshop. The NADI model outlines four deepening levels of understanding, essential for effective design: solutions, scenarios, goals, and themes (Dijkstra et al., 2015; van der Bijl-Brouwer & Dorst, 2014, 2017). In this study, journey mapping was used to understand the deepest level—the “why” which informed the design solutions.
A human-centered design approach (van der Bijl-Brouwer & Dorst, 2017) was taken to compliment the NADI model and the participatory approach of working with individuals with lived experience. This approach recognizes the subjectivity of this research, well suited to the context of understanding the development of an individual’s distress in relation to medical interactions. Authors acknowledge the interpretive nature of this research and have examined their own positionality in relation to this research, highlighted in the Reflexive Statement section to enhance transparency and epistemological rigor.
Participants
Participants were parents of children with benign or malignant brain or central nervous system tumors, who received care between 2019 and 2023 in Brisbane, Australia. The family could be at any stage in their experience of brain tumor, including bereavement.
Recruitment
Participants were recruited through a database of consumers from earlier local research (Young, Cashion, Ekberg, et al., 2023) who elected to receive further correspondence. Recruitment for the earlier study was undertaken using established principles for recruitment in pediatric health (Bradford et al., 2021). At the commencement of the current study, participants were re-contacted via email and asked for their consent to share their contact information with the current research team. The current research team sent the participant information and consent sheet to these parents to consider their participation. After having time to consider, their consent and preference for mode of participation were ascertained via email. Recruitment targets were set at five to eight parent consumers, in line with recommended group sizes for focus groups (Hennink et al., 2019; Krueger, 2015).
Data Collection and Procedures
Journey Mapping Workbook
Journey mapping is a process which utilizes lived experience, incorporating individual stories to produce a “journey map” which summarizes common components of an experience chronologically (Ly et al., 2021; Maddox et al., 2019). Participants were provided with a printed or electronic workbook containing a journey mapping exercise. The workbook presented milestones such as “first symptoms,” “first few weeks of treatment,” “leaving the hospital,” and “home in the community.” Participants were asked to amend these as needed to reflect their own experience and document at each milestone what emotions they experienced, and what emotional and informational support was needed. Participants were asked to complete the journey mapping workbook prior to participating in an online focus group, which was used to explore experiences further. Participants returned their workbooks via email or post, contributing written data.
Focus Group
The focus group was facilitated by co-authors MR, EM, and NB within a human-centered co-design approach (Blomkamp, 2018; Green et al., 2020; van der Bijl-Brouwer, 2016) via online videoconferencing on August 6, 2023. Practical strategies, such as small talk and deliberate openness from the research team, were enacted to help participants feel comfortable, respected as experts in their own experience, and welcome to share ideas (Krueger, 2015). Questions were presented on a shared screen. Participants responded verbally, sharing their experiences and ideas for solutions. Responses were summarized and annotated live onto the shared screen by MR, checking for correct notation as the visual narrative synthesis of the discussion was formed.
The focus group aimed to co-design solutions for the emotional and informational needs identified, and therefore, a design lens permeated the interaction. Journey mapping was the first element in the human-centered design approach, aimed at uncovering the deepest level of the NADI model—the underlying “why” that directs the design process into the “how” and “what” of the eventual products (Dijkstra et al., 2015; van der Bijl-Brouwer, 2016; van der Bijl-Brouwer & Dorst, 2014). After the journey mapping activity, the focus group shifted its focus to solutions and issues that arose in the journey mapping activity. Participants were invited to move from needs to solutions at appropriate moments, with due consideration for emotional impact. The focus group was audio-visually recorded and facilitators debriefed and created field notes immediately following the session. Concepts of trauma-informed care were not explicitly described or discussed with participants during these activities.
Some participants were not able to join the online focus group for reasons described below. Participants who could not attend were asked to contribute by answering questions with free text responses via an online survey hosted in Qualtrics (Version September 2023). Following the workshop, written data from all individual journey mapping exercises were integrated into the workshop’s combined narrative, ensuring individual insights were preserved while enriching the collective output.
Analysis
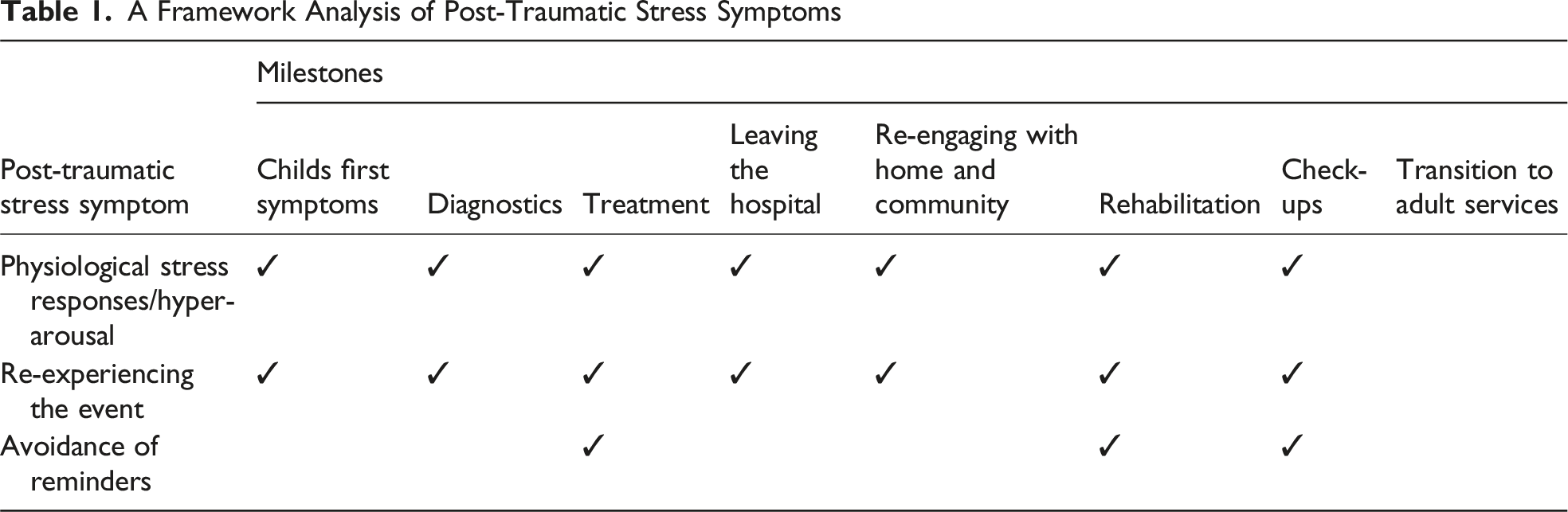
The focus group recording was transcribed verbatim by one author (MR) as part of becoming familiar with the data (Braun & Clarke, 2012; Krueger, 2015). Identification of trauma-related experiences was derived inductively from the narratives. Data from the focus group transcription and journey mapping exercises were subjected to framework analysis (Furber, 2010; Ritchie & Spencer, 1994). Framework analysis is a “codebook” application of thematic analysis where axes in a table are populated with relevant concepts, and the data are sorted categorically (Braun & Clarke, 2019; Braun et al., 2023). Framework analysis was selected for its suitability for comparing qualitative data across participants where common components of phenomena exist (Furber, 2010; Ritchie & Spencer, 1994). In this case, common components were milestones in the trajectory of the brain tumor experience and components of trauma theories. Specifically, the analysis sought to identify at which journey points there was evidence of (1) PTSSs (hyper-arousal, re-experiencing the event, or avoidance of reminders) (Kazak et al., 2006; Price et al., 2016) (2) Provision or breach of principles of trauma-informed care (Huang et al., 2014)
This analysis method allowed identification of trauma-related needs across the trajectory of care. Identification of PTSSs was aligned with the Primary Care PTSD Screen for DSM-5 (Prins et al., 2015), looking for indicators of nightmares or intrusive thoughts (re-experiencing cluster), avoidance of thoughts or external reminders (psychological or physical avoidance), and being “on guard” or easily startled (hyper-arousal cluster; Prins et al., 2015). Evidence of trauma-informed care was identified in recounts of experiences in line with or counter to the six principles of trauma-informed care (patients’ and families’ feelings of safety; trust and transparency; peer support; collaboration and mutuality; empowerment and choice; and consideration of cultural, historical, and gendered trauma issues; Huang et al., 2014), as well as “avoidance of re-traumatization,” one of the four underlying assumptions of trauma-informed care (Huang et al., 2014). This assumption was selected due to its applicability to client-facing service delivery and additional value to the six principles of trauma-informed care. The presence of PTSS clusters was recorded, and aspects of the principles of trauma-informed care were recorded as provided or not.
A critique of coding-based approaches to qualitative analysis is that these can dilute the nuance and richness of discourse (St Pierre & Jackson, 2014). To address this limitation, the arts-based research method of research poetry was used by the first author (MR) to convey participants’ experiences in a concise and emotive way. Research poetry is a form of “found” poetry, where poems or poem-like prose is created from existing text (Lahman et al., 2019; Miller, 2018; Penwarden & Richardson, 2020), in this case the focus group transcripts and journey mapping workbooks. In becoming familiar with the transcript and written data, the first author (MR) compiled salient quotes that particularly conveyed emotion or created an evocative image under the respective milestone. The exact words of participants were used, but the prose was re-arranged in poetic form. Language such as tense or conjunctions were adjusted for consistency, phrases from different speakers were combined, and these were formed into poems. Participants reviewed the poems to ensure they maintained the meaning and authenticity of the original discussion, a method of member-checking to ensure the poetry functions as “both a poem and testimony” (Miller, 2018, p. 18). The resulting research poetry is contextualized within summaries of each milestone, offering readers the opportunity to engage with the authentic lived experience.
Reflexive Statement
Reflexivity is an important component of qualitative research, “acknowledging the partiality of perspective and the effects of different (structural and spatial) locations and power relations between researcher and research” (Kenway & McLeod, 2004, p. 527). In this qualitative research, where humans are interpreting the data, reflexivity is of importance for researchers to examine ways in which their backgrounds and experiences may influence their perspectives. Components of experience which the authors recognize as impacting their viewpoints are delineated here. The first author has shared a more intensive reflection on influences on their positionality elsewhere (Rolfe & Bradford, 2025).
Author 1 (MR) is a current PhD student of the other authors. Author 1 planned and led the focus group with support from Authors 2 (EM) and 5 (NB). Student–supervisor dynamics and professional backgrounds were explained in the focus group. Author 1 has degrees in psychology, oncology, and palliative care and experience supporting young people through cancer in community-based organizations. She identifies as a cisgender white Australian female and has children of similar age to those of the participants. Author 2 has degrees in psychology and marketing management, with expertise in participatory co-design and creative arts approaches across aged, disability, and palliative care. Author 3 (LD) is a dually trained health and clinical psychologist who has worked with oncology patients and their families. She is a cisgendered tauiwi (non-indigenous New Zealander, of European decent) woman and a mother of a child with diffuse intrinsic pontine glioma (a brain cancer). Author 4 (SE) received undergraduate training in psychology and a PhD completed in a psychology department. He has never trained for clinical practice but studies social dimensions of healthcare. He has children of similar ages to the children of study participants. Author 5 has degrees in nursing and public health and clinical background in children’s cancer but was not involved in the care of any participants’ children. As a cisgendered white Australian female, she is of similar demographic profile to some of the included participants.
Ethics
All participants provided informed consent and participation was voluntary. Due to the emotional nature of parents recounting experiences with their child’s brain tumor, special care was given to provide psychologically safe interactions. Participants were assured of their ability to not answer questions or step away from the research at any point and were given details of emotional support services available at multiple points. The project received ethical clearance from the Children’s Health Queensland Human Research Ethics Committee (HREC/19/QCHQ/53816).
Results
Participant Characteristics
Nine participants completed the journey-mapping exercise, with six participating in the video-conferenced focus group, and three contributing only through written responses. Reasons for participation via written responses rather than focus group included scheduling difficulties and one bereaved parent who was cognizant of the difference of their experience to other participants.
Participants were all mothers, whose children had received care through a tertiary children’s hospital, and at least one other medical care provider (general practitioner, pediatrician, regional hospitals, international hospital, community allied health). Four mothers resided in regional areas, four in metropolitan areas, and one had permanently relocated from a regional to a metropolitan location during their child’s treatment. Children were aged between 18 months and 15 years at time of diagnosis and were diagnosed 26 months to 8 years prior to participation in the study. All children had finished intensive treatment, one mother was bereaved, and all other participants were accessing ongoing medical care commonly referred to as check-ups.
Journey Mapping Mothers’ Experiences of Their Child’s Brain Tumor Healthcare
A Framework Analysis of Post-Traumatic Stress Symptoms
A Framework Analysis of Trauma-Informed Care
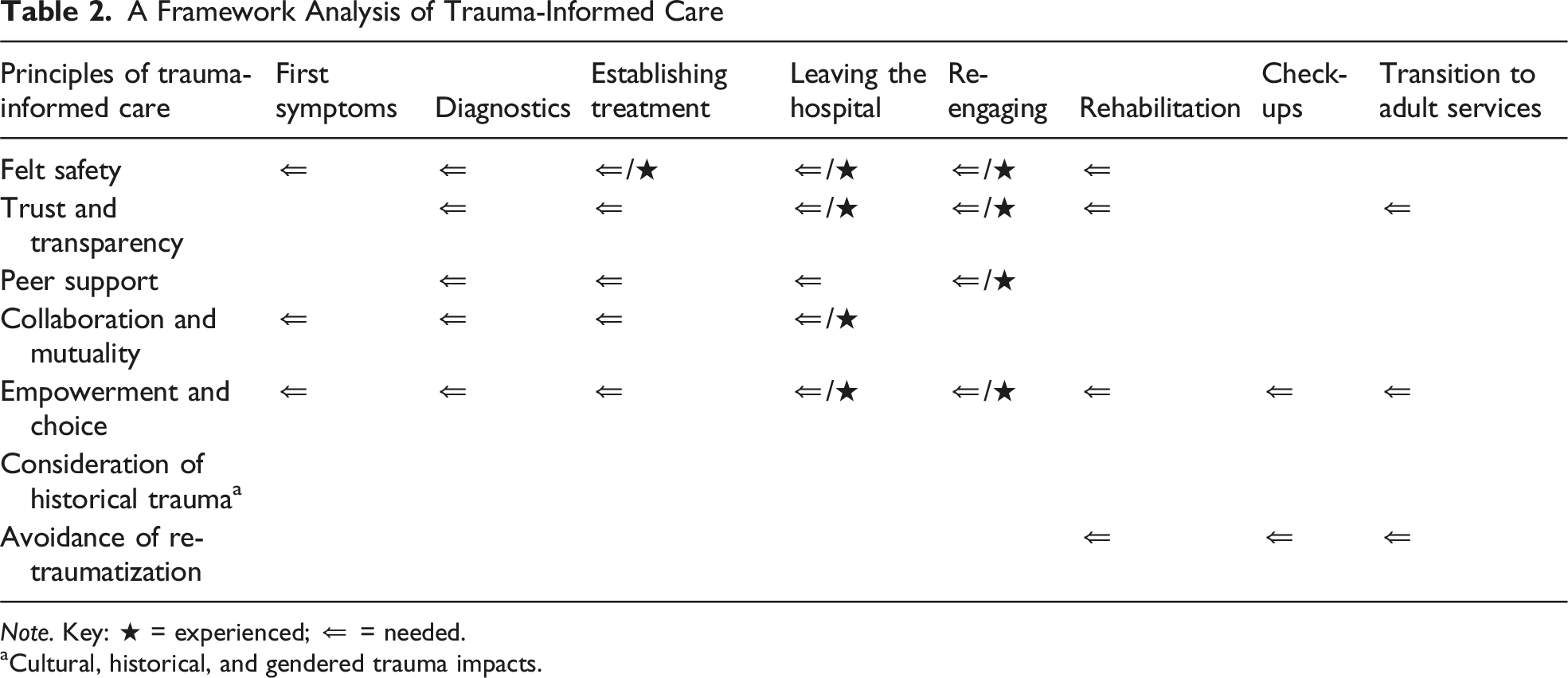
Note. Key: ★ = experienced; ⇐ = needed.
aCultural, historical, and gendered trauma impacts.
Milestone 1: First Noticing Child’s Symptoms and Advocating for Care
The poem “I must be wrong” (Box 1) documents the process of participants transitioning from being a passive recipient of information from medical professionals to becoming “an expert” (P3) in their child’s condition. At the beginning of this journey, participants frequently recounted stories of being dismissed by the health professionals they sought help from and feeling powerless to make them understand the differences they saw in their child’s functioning, an indication of a lack of mutuality in the relationship with the healthcare provider and a breach in trauma-informed care. For example, Participant 2 recounted: I started seeing a bit of a tremor, and him dropping things […] he fell to the ground that day[…] daycare are noticing things […]he’d started dribbling, he had a bit of slurred speech […] [The doctor] didn’t take me seriously […] It was really hard to get across to him that there’s changes in my son. And he just sent us away. (P2) Research Poetry at Milestone 1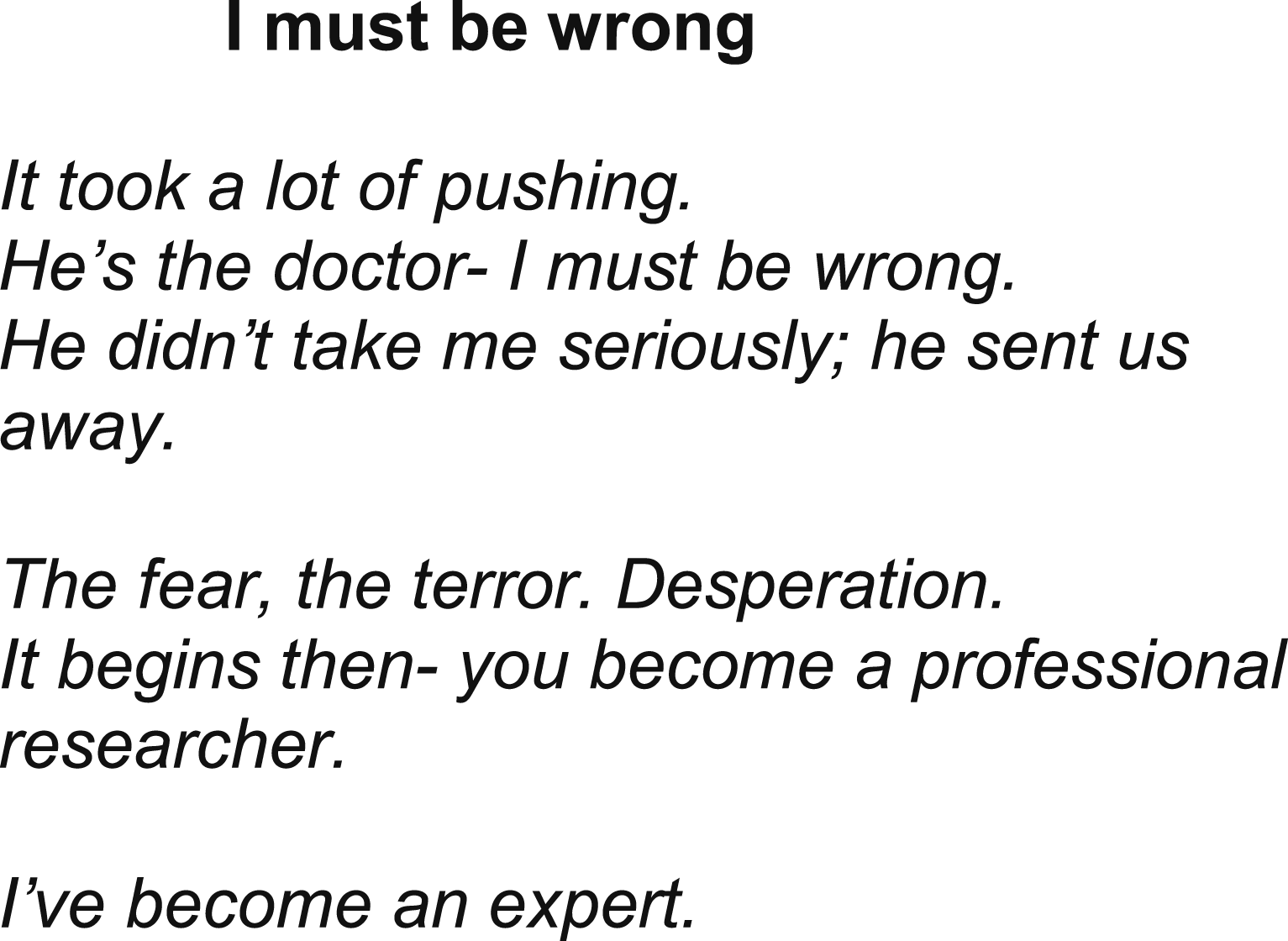
When first noticing symptoms and connecting with the medical profession, parents experienced emotions related to fear and anxiety, self-doubt, “embarrassment” (P4), “guilt” (P2), and worry for imposing on busy professionals. Participant 4 explained the memory of being turned away by doctors still “plays on my mind” and is “a lot of where my trauma is.” The period between first noticing symptoms and receiving help indicates gaps in trauma-informed care, with parents being dismissed or ignored, resulting in feelings of powerlessness and a lack of felt safety, trust, and mutuality in the relationship with their general practitioner or pediatrician.
Milestone 2: The Diagnostic Process
The diagnostic process was divided into two phases: waiting for confirmation of a tumor and waiting for diagnosis of tumor type. These periods varied largely between participants, from 24 hours to several years in one case. Participants named this the “age of anxiety” (P3), marked by intense worry for their child’s future.
In the first phase, while waiting for confirmation there was a tumor, parents reported taking on an advocacy role similar to when they first presented with symptoms. This stage was also accompanied by “emotional fatigue” (P1) related to the wait for answers. One mother (P3), when being told to wait three months and come back to see a doctor, advocated strongly for the urgency of their situation, and this undermined trust in the medical profession: There is a tendency in medical appointments to go with “Well, let’s hope it’s not worst case scenario,” and I would like to say to all those professionals “[Forget] hope—I want certainty, because it has cost my child his childhood.” (P3)
In addition to clinicians’ unwillingness to investigate, unavailability of services also hindered diagnosis. One mother (P1) recounted her story of phoning “every hospital in Australia who would do MRIs on children” to be told there was a 6- to 12-month wait. She eventually secured an appointment, “within a month because I rang the hospital every single day and got lucky that someone cancelled just before I rang.” At that stage, “he probably only had 6 weeks to live […] so if it hadn’t been for me ringing he would have died, 100%.” (P1) Lack of access to neurologists was also reported as a barrier to diagnosis.
When receiving a diagnosis, parents reported emotions of shock, grief, and anxiety. Parents grieved for the health of their sick child, and for their other children, “because suddenly she wasn’t innocent anymore […] suddenly they’re not just kids with no worries” (P4). There were physiological reactions to first hearing of the diagnosis (“jelly legs,” P3), and ongoing issues with sleep and appetite started during this period. Participant 4 recounted that the week between finding out there was a tumor and knowing what the treatment plan was “had the biggest impact on all of our mental health going forward,” and when she reached out to the hospital for support for her own well-being, she was told to access this elsewhere. This milestone is represented in the poem “All the fear, no answers” (Box 2). Research Poetry at Milestone 2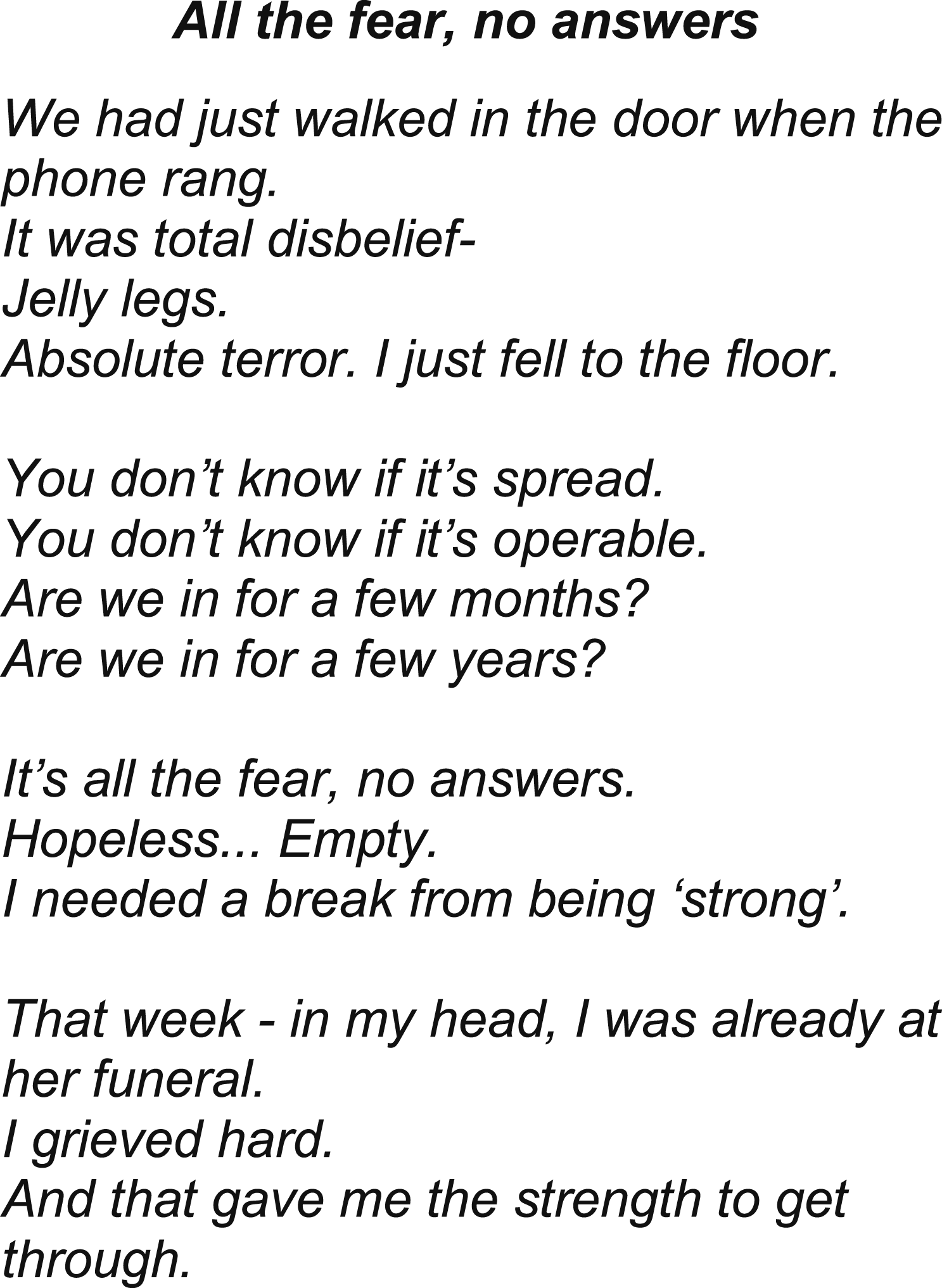
Parents recounted a need for direction and to be “fed and watered” (P5), possibly indicating cognitive impacts related to a dissociative or stress state. Parents had a “need to understand what’s next,” and went “looking for stories” (P5) through online research with a need to connect with families who had similar experiences. Breaches of trauma-informed care in this period related to a lack of felt psychological safety within services, high uncertainty on the possible path ahead, and a lack of connection with peer support.
Milestone 3: Treatment
During the treatment phase, participants described two discrete periods with differing needs: establishing treatment routines and managing treatment once the routine is familiar. In the establishment phase, uncertainty coupled with the need to quickly make important decisions relating to treatment was reported as particularly stressful. These early stressors are highlighted in the poem “Paper Thin” (Box 3). Research Poetry at Milestone 3
Initial concerns regarding “trusting strangers” (P1) and lack of transparency around treatment options undermined trust and psychological safety with some treatment teams. Participant 4 recounted being told of a number of risks with one treatment path, before having to ask “Can we circle back to the first option? You didn’t talk about any risks there.” Her interpretation was that the options were presented to her with the implication “there’s a right and a wrong choice” (P4).
Self-doubt permeated this period in relation to treatment decisions. Participants wanted information on prognosis, support for siblings of the child in hospital, and guidance on what questions to ask. Parents reported feeling “constantly on edge” (P5)—an indication of hyper-arousal—and “a lack of emotion” (P5)—an indication of psychological avoidance or hyper-arousal.
Written responses relating to managing continuing treatment included comments that “we knew we were in good hands” and “in the right place for the best care possible” (P9). The experience of inpatient treatment differed to that of an outpatient, with families who had less inpatient involvement or were discharged to outpatient care reporting feeling “uninteresting” (P3, P6, and P9) to the medical team and “treated differently” (P9). There was a sense of being de-prioritized once treatment changed to the outpatient setting, with parents needing to chase the results of important tests.
Families continued to want more information on “what’s next” (P5), including what to expect from treatment and how they would know if the treatment was working. Many parents reported hearing information on services available to them through other parents and not through hospital staff, which impacted the trust they felt toward staff. Access to hospital-based emotional support for the parents was reported as mixed, with some families indicating they “couldn’t fault” (P1) the support they received for themselves, and others indicating they did not feel any support was offered or received. Participants reported wanting to speak to other mothers who had experienced similar health journeys with their children and recommended family-led social media groups for this purpose, calling one such group “the best resource I have had through this journey” (P4).
Milestone 4: Leaving the Hospital
When leaving the hospital, participants reported mixed emotions. There was simultaneously a relief that treatment was completed, but much fear around handling their child’s needs while losing the “safety of being in hospital” (P5), illustrated in the poem “Happy but Terrified” (Box 4). Research Poetry at Milestone 4
Participants were concerned that without active treatment, there was no way to know that the tumor was “behaving” (P1) and reported thoughts of worst-case scenarios that were hard to switch off, practical concerns regarding infection control or tumor growth while away from hospital, and additional work to find the correct services for their child’s new needs. Some families reported not being given information on what services existed, with resulting impacts on the child’s rehabilitation, functioning, and mental health. They experienced conflicting emotions and overt symptoms of post-traumatic stress (“flashbacks”) at this milestone.
Milestone 5: Rehabilitation
Participants reported mixed experiences of connecting with rehabilitation supports. Some were connected to a hospital-based rehabilitation service while others needed to identify what needs their child had independently, with limited knowledge of what neuro-specific services existed. One mother reported only hearing about neuro-specialty physiotherapy and psychology through participation in research, including the current study. Where connection to rehabilitation was not offered through the hospital, participants felt isolated and “uninteresting” (P3). One participant reported that even though their child’s tumor had significant impacts on his functioning, social interactions, and mental health, support from the hospital was only around the medical components of his recovery, illustrated in the poem “The Rest of Him” (Box 5). Research Poetry at Milestone 5
One participant reported their primary source of support during this period was the use of social media groups for parents of children with cancer because this was a source of “mums and dads who ‘get it’” (P9). A lack of transparency regarding availability of services impacted the trust and psychological safety felt toward the hospital system. Participants reported long waits to access allied health support, especially exacerbated in rural areas where “he’s had none of that … we just do what we can at home” (P1).
Milestone 6: Re-Engaging With School and Community
Families had mixed experiences re-engaging with their communities. Anxiety continued during this phase and extended to concern over infection, recurrence, changes to their child’s abilities (e.g., “he can’t feed himself properly,” P3), cognition, and mental health, and bullying that may arise from this. Participants reported a need to maintain vigilance regarding signs of recurrence or infection. Some families indicated a repeated need to explain to sporting and social groups what the child’s needs were, sometimes in the context of curiosity and sometimes in the face of bullying. Two participants reported sporting groups were lacking in understanding of their child’s disabilities, with experiences where they were laughed at (P2) or people would “roll their eyes when he drops a ball” (P3) despite obvious scars from cranial surgery and attendance at the same club for years. In some instances, bullying had ongoing psychological effects and impacted the child and family’s willingness to engage in the community. These differing perspectives are depicted in the poem “Less Than” (Box 6). Research Poetry at Milestone 6
One participant reported education at their child’s school facilitated by their treating team as a positive element of their care, resulting in the child being treated “like a superstar” (P1) at school. This highlighted the ability to enhance the sense of ongoing psychological safety felt by the family in their home community through clinical education.
Milestones 7: Check-Ups
Returning to the hospital for check-ups was an unexpected and unnoticed period of re-traumatization when it is “hard to switch all of that guilt and anxiety off” (P1). Participant 1 described this time: Everyone else’s life is going on as normal, we’re sitting in waiting rooms a lot […] That’s an aspect of life that is not the same ever again. And it sort of all happens very quietly in the background. And I think—I don’t think people realize how traumatic those appointments can become, and often very unpredictably so. (P1)
Similar to milestone 3 (Treatment Routines), focus group participants emphasized that establishing the check-up routine was a period of higher anxiety than managing established check-ups. The poem “Into our Destiny” (Box 7) highlights the thoughts and stressors associated with these check-ups for participants. Research Poetry at Milestone 7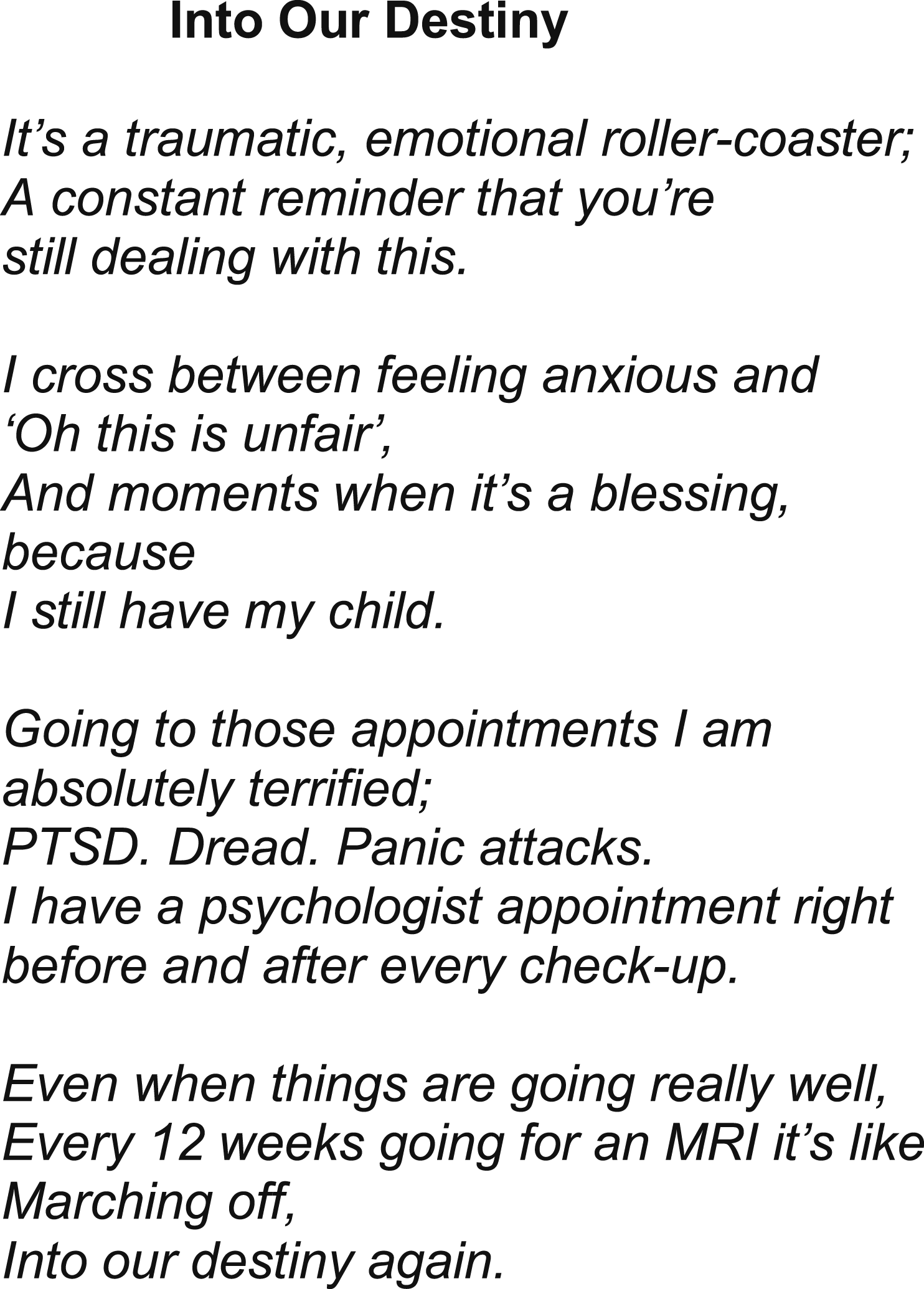
Being “injected back into that environment” (P1), procedural anxiety, waiting for appointments, and witnessing the suffering of others were contributors to re-traumatization. Between appointments, constant monitoring was required for any potential symptoms to report and “scanxiety” (P5; anxiety related to scans and waiting for the results) escalated as appointments came closer. Appointments, even when they resulted in good news, were seen at best as an extension of the monitoring and associated anxiety until the next appointment, with little or no support in between. Check-ups and rehabilitation were viewed as ongoing reminders of abilities their child had lost, and the unfairness of that. Trauma-informed care in this phase was ideally described as understanding the impact of return visits and limiting these through telemedicine and monitoring at local hospitals, and the availability of a nurse to just “ask a quick question” (P3) between appointments, which only some participants had access to. The need to take time off work for trips to the central hospital was identified as an ongoing financial burden.
Other Components
Only two participants had comments on transitioning to adult services (milestone 8); one was in the middle of this transition, and one had this transition approaching but was not cognizant of this until it was discussed in the focus group: “It also just occurred to me […] my son’s 17, are we reaching the end of contact with the children’s hospital?” (P3). These data were analyzed for the presence or absence of trauma-informed care; however, there were not enough data for further analysis.
Although the principles of trauma-informed care highlight gendered and historical components of traumatization (Price et al., 2016), no participant identified these components as relevant to their care. However, there were examples where imbalances existed between male and female protagonists, which displayed traditionally gendered imbalances of power. In one instance, the mother accepted a clinician’s direction that there was no need for concern, before the father insisted the doctor look again. In another instance, a mother reported a male doctor could not be made to understand that the symptoms she was seeing in her son (slurred speech and coordination issues) represented a loss of function.
Needs that persisted across time points include emotional, communication, and behavioral needs of the sick child and of their siblings. For example, Participant 1 reported: The behavioral issues that come out of sitting in hospitals for 3 years as a toddler and being away from family, that’s like a daily thing for us. (P1)
Other issues which persisted across time include financial toxicity and parents’ physiological symptoms such as trouble with eating and sleep. Without being asked, four mothers reported PTSD diagnoses in their family relating to their journey with brain tumor, including two parents from different families, one sibling, and one child patient. Of note, while the hospital system focuses on the acute management of cancer and cancer treatment, for these families the experience of trauma began before their involvement with the hospital and reverberated far beyond the acute phase of diagnosis and treatment.
Discussion
We aimed to map components of the parental experience with childhood brain tumor that may be contributing to trauma-related distress. Our first research question sought to identify indicators of PTSSs across the trajectory of the brain tumor experience. We found evidence of all three PTSS clusters—hyper-arousal, re-experiencing the event, and both physical and psychological avoidance—at various milestones. Hearing the diagnosis and waiting for the start of treatment were reported as exceptionally difficult time points, reflective of research across pediatric cancer types, which indicates diagnosis itself may be a traumatizing event (Christofferson et al., 2020). This contrasts with diagnostic criteria for a PTSD diagnosis, which explicitly articulates that a cancer diagnosis is not a qualifying event for PTSD (American Psychiatric Association, 2022). Some components of psychological avoidance (e.g., feeling “emotionally numb”) were reported during hospitalization. Physical avoidance was evident with families voicing a desire to avoid the hospital after acute hospital treatment had ended. These findings contribute novel knowledge to the field, identifying when in the trajectory of care this group of parents experience symptoms of post-traumatic stress.
In relation to our second research question, we found that trauma-informed care was both received and lacking in different contexts. Positive components of trauma-informed care were provided during hospitalization, transfer home, and re-establishment within the home community. Experiences that are inconsistent with the principles of trauma-informed care, however, were reported across every milestone from the time of their child’s first symptoms through to transition to adult services. Commonly, a lack of felt psychological safety with care providers was evident before engagement with the hospital, ignited by powerlessness in having concerns heard and acted on when symptoms first presented. Families de-prioritized discussing components relating to acute treatment in the focus group, and there were indications across milestones that families had positive relationships with care providers in hospital. Where there was a lack of felt safety and trust with care providers, this was attributed to insufficient transparency around treatment decisions, available services including peer support, and understanding of what to expect. Discussion regarding transition to adult services was relevant to two participants, who both indicated a lack of transparency in this. Our findings indicate the need to enhance trauma-informed care across the trajectory of childhood brain tumor.
The scant research that exists on PTSSs or PTSD in parents of children with brain tumors examines trauma outcomes after the resolution of their child’s treatment (Baenziger et al., 2020; Bruce et al., 2011; Fuemmeler et al., 2001) and calls for research to identify contributing components of the experience (Yalug et al., 2011). Our findings identify components suitable for improvements in trauma-informed care and treatment, highlighting traumatization that occurs before integration with the hospital system. We identified traumatization experienced by parents, siblings, and patients, emphasizing the importance of family-focused care that supports the mental well-being of all family members. Our paper is also one of the first to use the qualitative arts-based research method of research poetry to convey the lived experience of parents, providing deep insight into the world of mothers of children with brain tumors.
Indictors of trauma in this cohort are in line with high rates of traumatization found in previous pediatric brain tumor research. The lifetime prevalence of PTSD for parents of children with all cancers ranges from 27% to 54%, with these rates positively associated with the ongoing disability resulting from the cancer, and the brain tumor cohort being at the highest end of this (54%; Bruce, 2006). This rate contrasts with lifetime prevalence of PTSD ranging to 6.1% in the general population (Kessler et al., 2017), and approximately 30% in Vietnam War veterans (Weiss et al., 1992). These prevalence rates highlight the importance of understanding trauma as a theoretical underpinning for the psychological responses common in parents of children with brain tumors, especially mothers. More contemporary prevalence research is urgently required to better understand this issue.
Parents reported vigilance in monitoring their child for new symptoms or treatment complications in the period following acute treatment. This adaptive vigilance, in the context of trauma, raises questions of whether the attentiveness needed for symptom monitoring impacts mental well-being similarly to hypervigilance, a symptom of PTSD (American Psychiatric Association, 2022), or if there is a causal link between them. Further research should investigate if there is a route between adaptive vigilance and hypervigilance as a clinical symptom, and any impacts of monitoring models on the development of hypervigilance.
Clinical Implications
The findings of the current study highlight trauma-related needs across the continuum of healthcare. This information can inform service-level approaches to address these needs, such as universal trauma screening, universal trauma-informed care, or linkage to trauma treatment early in the trajectory of hospital care for parents. Early screening for trauma would also highlight families entering the system with prior unrelated traumatization, which places them at higher risk for psychological disorders from the current stressor (Yalug et al., 2011). Early and ongoing screening of parental mental health is called for in relevant psychosocial support standards (Kearney et al., 2015; Wiener et al., 2015, 2020); incorporation of trauma-informed care in this component of care could mitigate much distress.
A series of clinical implications can be identified by considering the findings of the current study in relation to existing research. Trauma treatment may be the missing component that is producing low or no impact of parental psychological interventions in pediatric cancer (Muglia Wechsler et al., 2013; Ruiz et al., 2021; Wakefield et al., 2021). Universal trauma treatment could go beyond traditional modalities to ensure sustainability and acceptability to the cohort. Eye movement desensitization and reprocessing (EMDR) therapy involves rapid deliberate eye movements while recounting traumatic events and is recommended by the World Health Organization as one of two therapy types to support trauma processing and trauma-related disorders (Tol et al., 2013). Low-intensity interventions which support the processing of trauma, such as EMDR apps and group EMDR therapy, are effective (Maxfield, 2021) and could be made available universally, soon after entry to the hospital system. Further research should explore the impact of low-intensity trauma interventions in this context, including “gamified” interventions which are being trialled with success in other areas of post-traumatic stress and anxiety (Butler et al., 2020; Hagenaars et al., 2017; Lyadurai et al., 2018) and have been shown to impact brainwaves in similar ways to EMDR therapy (Wang & Yu, 2018). Mobile and low-intensity interventions would suit the needs of families reported in this and previous research (Young, Cashion, Hassall, et al., 2023), which indicates parents’ time and attention are limited resources during treatment.
The lack of transparency and mutuality in the relationship with healthcare systems identified in this research could be remedied through multi-pronged approaches. In the first instance, training for staff in trauma-informed care may underscore the importance of choice and transparency in clinical interactions, especially relating to treatment choices. A key component in the development of PTSSs is a sense of powerlessness (Huang et al., 2014); when families are given transparent information on treatment options without feeling a pressure toward one option, they have the opportunity to be in control of the decision. Where staff understand the impact of full and transparent conversations in the context of trauma, more care may be taken to ensure every family has this experience of their healthcare. Training in trauma-informed care may enable clinicians to identify ways they can provide more certainty regarding the trajectory of care, for example, in providing information on the transition to adult services. A shift in the paradigm toward trauma-informed healthcare has been compared to earlier successful shifts toward family-centered care, needing to be embedded across every interaction and organizational culture (Marsac et al., 2016). Such a shift needs to be supported through organizational focus and training (Marsac et al., 2016), and online training resources are available internationally (Children’s Hospital of Philadelphia, 2021). Additionally, the current study could be used as a template for services to map where in their own setting parents are experiencing or missing components of trauma-informed care.
A second approach to addressing a lack of transparency and mutuality could be empowering parents through resources, particularly where universal information is relevant, such as family-facing handbooks available internationally (Brain Tumour Foundation of Canada, 2011). Issues highlighted in this research relevant for universal dissemination include general information on tumors and treatment, navigating family and sibling communication, availability of services, and signposting of peer support. Facilitation of connections to services and peer support, and guidance on navigation of family communication and the pathway ahead, impacts positively on self-efficacy and mental health, supporting parents’ ability to process potentially traumatizing events (Westgate, 2019). Where information must be more tailored to the family’s situation, communication guides should be provided to empower families to ask questions of their clinical team, such as question (or discussion) prompt lists (Ekberg et al., 2020; Sansoni et al., 2015). Universal provision of information in this regard may foster greater trust with the treating team through increased transparency.
This study also has implications for the broader definition of trauma. Although PTSSs are recognized as significant in their own right within the PMTS model (Price et al., 2016), the most recent edition of the Diagnostic and Statistical Manual for psychological conditions (DSM-V-TR) expressly identifies that a cancer diagnosis in itself, or a death that was not sudden, is not a qualifying event for the diagnosis of PTSD (American Psychiatric Association, 2022). This contrasts with the previous edition (DSM-V), where a cancer diagnosis was not expressly excluded as a qualifying event, and the version prior to this (DSM IV-TR) where a cancer diagnosis that was perceived as a threat to life was a qualifying event (Cordova, 2020; Recklitis et al., 2023). These revisions bring up issues of comparison between earlier and later diagnoses of PTSD in the literature. Relevant to this study, it must be noted that participants reported the period of hearing their child had a brain tumor and waiting to commence treatment had great impact on their mental health years later, with components that are still the target of re-experiencing. The ongoing nature of psychological distress triggered by the diagnosis indicates this is a period worthy of further examination and may indicate that a parent’s trauma in hearing their child could die is in fact an experience that can trigger symptoms of PTSD in parents. The particular shock inherent in a parent hearing that their child may die out of the natural order may need to be considered in future revisions of the DSM, in line with other criticisms that the definition of qualifying events for PTSD diagnoses is unsuitably narrow (Cordova, 2020; Recklitis et al., 2023; Roberts et al., 2012).
Supported by this study, we advocate for recognizing parental well-being as a standalone area of importance in the family-centered care of pediatric brain tumors. Additionally, a parent’s mental health has flow-on effects on family functioning, the child patient’s quality of life (Moscato et al., 2022, 2023, 2024), and the level of care and support a child receives once discharged, highlighting the need to consider parental well-being in the constellation of influences of patient well-being through treatment for a pediatric brain tumor.
Limitations
Some methodological limitations were present in this study. First, as this is a qualitative study with a small sample size from one tertiary healthcare center, it cannot be assumed to represent all experiences of childhood brain tumor. Different children and families may experience varying experiences in addition to the shared experiences described in this study. While recruitment was open to all parents, participants were exclusively mothers and gender differences may significantly alter experiences and interpretations of events and their impacts. While the analysis focused on trauma components, the work is one component of a broader study co-designing solutions; and thus, inferences of traumatization were drawn out from recounts of emotional impacts. This approach may have missed aspects of the experience that were traumatizing but conversely have drawn out components participants may not recognize as traumatizing. Second, the PMTS model is based on a three-cluster model of PTSD, while the latest version of the Diagnostic and Statistical Manual for Mental Disorders (DSM) utilizes a fourth cluster of cognitive symptoms (American Psychiatric Association, 2013). This fourth cluster has taken on some symptoms from the “avoidance” cluster and added symptoms relating to cognition and persistent mood changes (American Psychiatric Association, 2013). Utilizing the three-cluster model aligned with the PMTS model has likely resulted in fewer indications of traumatization than if the four-cluster model was utilized. This work enhances our understanding of malleable contributors to traumatization in the experience of childhood brain tumor, informing the direction of further research.
Conclusions
This work builds on earlier calls for trauma-focused psychological screening (Chaplo et al., 2024) and support for parents to be introduced at diagnosis (Young, Cashion, Hassall, et al., 2023), alongside systemic improvements which foster a sense of psychological safety for parents (Christofferson et al., 2020). Although unchangeable factors such as the threat of death impact the processing of trauma, malleable components such as a felt sense of safety within the care team, recognition of traumatization, and access to trauma-focused psychological support can contribute to reducing the impacts of the potentially traumatizing experience of a child’s brain tumor. The process of trauma-mapping the parental experience of childhood brain tumor is a vital part of providing healthcare that is cognizant of traumatization, in line with the principles of trauma-informed healthcare (Huang et al., 2014). This trauma-mapping methodology could become part of quality improvement initiatives, identifying where in healthcare experiences individual services are falling short of trauma-informed care. Such understandings can inform service improvements and ensure families benefit from early intervention for medical traumatic stress regardless of where in the trajectory of care traumatization occurs.
Footnotes
Acknowledgments
Our gratitude goes to Christine Cashion, who facilitated connection with participants. Our deep gratitude to the mothers who shared their experiences so generously to inform this work.
Ethical Considerations
Our study was approved by the Children’s Health Queensland Human Research Ethics Committee (HREC/19/QCHQ/53816).
Consent to Participate
Participants provided informed consent and were given time to consider their participation.
Author Contributions
Melanie L. Rolfe: conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, and project administration. Evonne Miller: methodology, investigation, resources, writing—review and editing, and supervision. Liesje Donkin: writing—review and editing. Stuart Ekberg: writing—review and editing. Natalie K. Bradford: conceptualization, methodology, investigation, resources, writing—review and editing, and supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is supported by an Australian Government’s Research Training Stipend for Doctor of Philosophy students.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not available publicly due to the small cohort and potentially identifiable content of the participants’ comments.