
Abstract
Eating disorder (ED) recovery narratives provide valuable insights into the recovery process. While existing research identifies key turning points in ED recovery, most studies focus on majority populations, neglecting the experiences of minoritised individuals. This study aimed to explore the turning points in ED recovery among diverse individuals and examine the role of symbolic objects in understanding recovery processes. English-speaking adults with lived experiences of ED who identify as part of underserved groups were recruited for an adapted photovoice study involving individual interviews (n = 11) and two subsequent focus group discussions (n = 4 per group). Participants shared objects symbolising their recovery journeys. Using reflexive thematic analysis, we generated three themes: (1) Up, Down, and Around: Recovery was described as non-linear, with positive and negative turning points; (2) Growing awareness and readiness of recovery; and (3) From feeling disconnected to belonging. The findings show that recovery was often non-linear for these individuals, with social belonging and identity integration being crucial. The study also illuminates how everyday objects can be used as a research method to encapsulate turning points in recovery by representing progress and offering motivation. The findings are also consistent with minority stress theory which shows how one’s mental health intersects with social stressors and marginalisation.
Introduction
Research on mental health recovery stories offers a deeper understanding of personal perspectives on recovery and highlights what is crucial for individuals with lived experiences (van Sambeek et al., 2021). Sharing recovery stories has been shown to benefit the storyteller by fostering coherence, invoking emotional catharsis, and developing a sense of agency (Nurser et al., 2018). It can also be beneficial for recipients, as it can enhance connectedness and validation, foster a better understanding of recovery, and reduce stigma (Rennick-Egglestone et al., 2019).
Turning point in recovery is one of the key characteristics in recovery narratives across different mental health conditions. Llewellyn-Beardsley et al. (2019) systematically reviewed and synthesised a dimensional typology of recovery narratives. One typology was the use of turning points in the narratives, where new understanding about their experiences was gained (Llewellyn-Beardsley et al., 2019). In the area of substance misuse, researchers have found that turning points can be a key facilitator to identity change, when individuals decide to stop using substances due to experiencing identity conflict, and are then able to create a new sense of self and social identity (Brookfield et al., 2019).
In the eating disorder (ED) field, turning points have been identified as one part of recovery stories. Dawson et al. (2014) analysed personal narratives from individuals with enduring anorexia nervosa and identified four phases: (1) unable/unready to change, (2) tipping point of change, (3) active pursuit of recovery, and (4) reflection and rehabilitation. Building on this, other studies have focused on tipping points or turning points (used interchangeably) of change to better understand change during the recovery process. Fogarty and Ramjan (2018) used conventional content analysis to generate themes from survey responses about tipping points of change among females with anorexia nervosa. They defined tipping point as the point at which the illness trajectory is interrupted, shifting towards the pursuit of recovery. Tipping points identified in this study included realising the loss of something valuable, the risk of losing something valuable, and finding something to live for or stay well for. More recently, Watterson et al. (2023) interviewed women with various EDs, reporting three turning points of recovery through structural narrative analysis: finding someone to talk to without fear of being a burden, receiving unconditional acceptance from a therapist, and establishing a motivation for change. Whilst not specifically focusing on turning points, Baudinet et al. (2023, 2024) explored young person and parent/caregiver perceptions of change in single-family and multi-family therapy for anorexia nervosa, reporting themes such as relationships as vehicles for change, awakening, acceptance of the necessity of confronting the disorder, and envisioning life beyond the ED. The theme on awakening, where young people spoke about a point in their treatment where they had a moment of clarity that something was not right, closely resembled the idea of turning points. Complementing these findings, Eaton (2020) conducted a meta-ethnography on ED recovery, highlighting five themes of (1) ED as a life jacket, (2) drowning: recognising consequences, (3) treading the surface: recognising consequences, (4) swimming: the path toward recovery, and (5) reaching recovery: a sense of freedom. The author equated the non-linear process of recovery to learning to swim whilst letting go of the life jacket. Taken together, all these studies allude to recovery being a journey with different phases/stages, where there might be tipping/turning points that move the person from one phase to another in a non-linear manner.
Whilst informative, it is important to acknowledge that the majority of these data are generated from the perspective of Caucasian, able-bodied, and cisgender people, who are overrepresented in clinical practice and research (Hower et al., 2022). Individuals from underserved backgrounds, such as people with lower socioeconomic status, from racially minoritised backgrounds, from a minoritised gender/sexual identity, or from multiple intersecting minoritised-identities, are at higher risk of experiencing an ED and are less likely to access treatment and, if they do, commence treatments at a more severe stage of illness (Burke et al., 2023). Minority stress theory (Meyer, 2003) provides a key framework for understanding the disparity in health outcomes between majority and minority groups due to social stressors faced by the latter group. These stressors include discrimination, stigma, and social exclusion, which can exacerbate physical and mental health issues, including ED (Rodgers et al., 2018). In a recent qualitative study with individuals that identified as part of the LGBTQ+ community, participants described suffering from societal pressure to conform to heteronormative standards, which contributed to their ED (Rawlings et al., 2024). Although research using minority stress theory is primarily conducted within sexual minority populations, research in other minoritised populations such as diverse ethnic groups and people who are neurodiverse is burgeoning (e.g., Botha & Frost, 2020).
What is poorly understood and largely missing from the current literature is the nature of recovery turning points among diverse individuals across different genders, sexual orientations, neurodiversity, (dis)abilities, and ethnicities. Visual methods have been suggested as a way to engage these underserved and marginalised groups (Colucci & Bhui, 2015), as they can effectively capture emotional and relational experiences creatively (Liamputtong & Rumbold, 2008). Objects carrying emotional value can serve memory-bodying and autobiographical functions, which can also help elicit meaningful narratives (Cowan et al., 2019; Yim, 2022). From a sociology and material culture perspective, objects are not simply seen as passive symbol carriers. In addition to the symbolic meaning embedded in the object, objects can carry multiple meanings and have the capacity to affect audience, contributing to the active, dynamic meaning-making process (McDonnell, 2023).
Aims
We aimed to explore turning points in ED recovery among diverse individuals and, as an exploratory analysis, examine the role of objects in understanding one’s recovery process, which will hopefully support the agenda of achieving equitable health outcomes and research representation for diverse individuals.
Method
Participants
Participants were recruited via university circulars, the Beat (ED charity) website, volunteers, supporters, and social media channels, and the research group’s X (formerly known as Twitter) channels. Inclusion criteria included English-speaking adults from diverse backgrounds with lived experiences of an ED and who consider themselves as recovered or significantly improved, and have been discharged from ED services for at least three months. We adopted a broad definition of “diverse,” including identities or intersecting identities of marginalised ethnicity, gender or sexual orientation, (dis)ability, neurodivergence, low socioeconomic status, and being a young carer. The term “diverse” in our study encompasses a wide range of experiences to capture the complexity of marginalised communities. Consulting with individuals with lived experiences, it was decided that embracing heterogeneity is essential for an inclusive approach as marginalised identities are often intersectional. The exclusion criteria concerned people who were at acute physical health or psychiatric risk (e.g., acutely suicidal or experiencing a significant other mental disorder, needing treatment in its own right).
Screening
An adapted version of the Eating Disorder Diagnostic Scale (EDDS, Stice et al., 2000) was used for participant screening to assess eligibility (lifetime occurrence of an ED) following initial expression of interest. The results were used to guide identification of fraudulent participants as reported in other online qualitative studies (Davies et al., 2024). The original scale assesses symptoms during the previous six months. This was adapted to cover lifetime occurrence as the aim was to capture people who considered themselves recovered. The original EDDS has demonstrated excellent psychometric properties (Stice et al., 2000).
Design
An adapted photovoice method (Wang & Burris, 1997) was used in this study. This method was adopted as it is a creative and participatory approach designed to strengthen community and marginalised voices. Wang and Burris (1997), the developers of photovoice method, initially defined photoVOICE as: “Voicing Our Individual Collective Experience.” In the photovoice paradigm, participants are first encouraged to share their experiences, concerns, and ideas through photographs. Participants are then invited to co-construct ideas arising from the photographs in subsequent group-based workshops/focus groups. Many projects are followed by community exhibitions where the photographs and short narratives written by participants are displayed.
Based on previous work by Yim (2022) on Chinese and Vietnamese communities, instead of focusing on photographs, participants were invited to choose an object that relates to their self-perceived turning points of ED recovery. Following the principles of narrative therapy, objects hold affective and memory-embodying values to allow visitors to bear witness to their stories, serving as a communal record and document of collective memories (Yim, 2022). In the current study, participants were encouraged to take a picture of their chosen object for the online display. As part of dissemination, participants could choose to “lend” their physical object, use a replica of the object, or display a photograph of their chosen object. These objects/photos alongside the narratives were then exhibited in an art gallery in London. The article about the dissemination and exhibition is in progress.
Procedure
Ethical approval was obtained prior to the commencement of the study (Health Faculties (Blue) Research Ethics Subcommittee [King’s College London], HR/DP-23/24-39830). Interested participants received an information sheet and consent form. If participants shared photos of the objects for the exhibitions, by UK law, they own the copyright of the images. Therefore, consent was also sought for the research team to use or publish the photos. Informed consent was taken for the following: (1) sharing of their recovery stories, (2) sharing a photo of their object or allowing the research team to take a photo of their chosen object, (3) consenting to the photo or a mock-up object being exhibited, (4) exhibiting their stories, and (5) publicising the photos of the objects and stories online. Informed consent was checked three times throughout the study: prior to the interview, at the interview, and before the exhibition took place. This is to ensure that people could change their mind as the study progressed. The procedure is shown in a written flowchart below (Figure 1). Participants were compensated for their time in the interviews and focus groups (including preparatory work time) via vouchers. Research Study Procedure.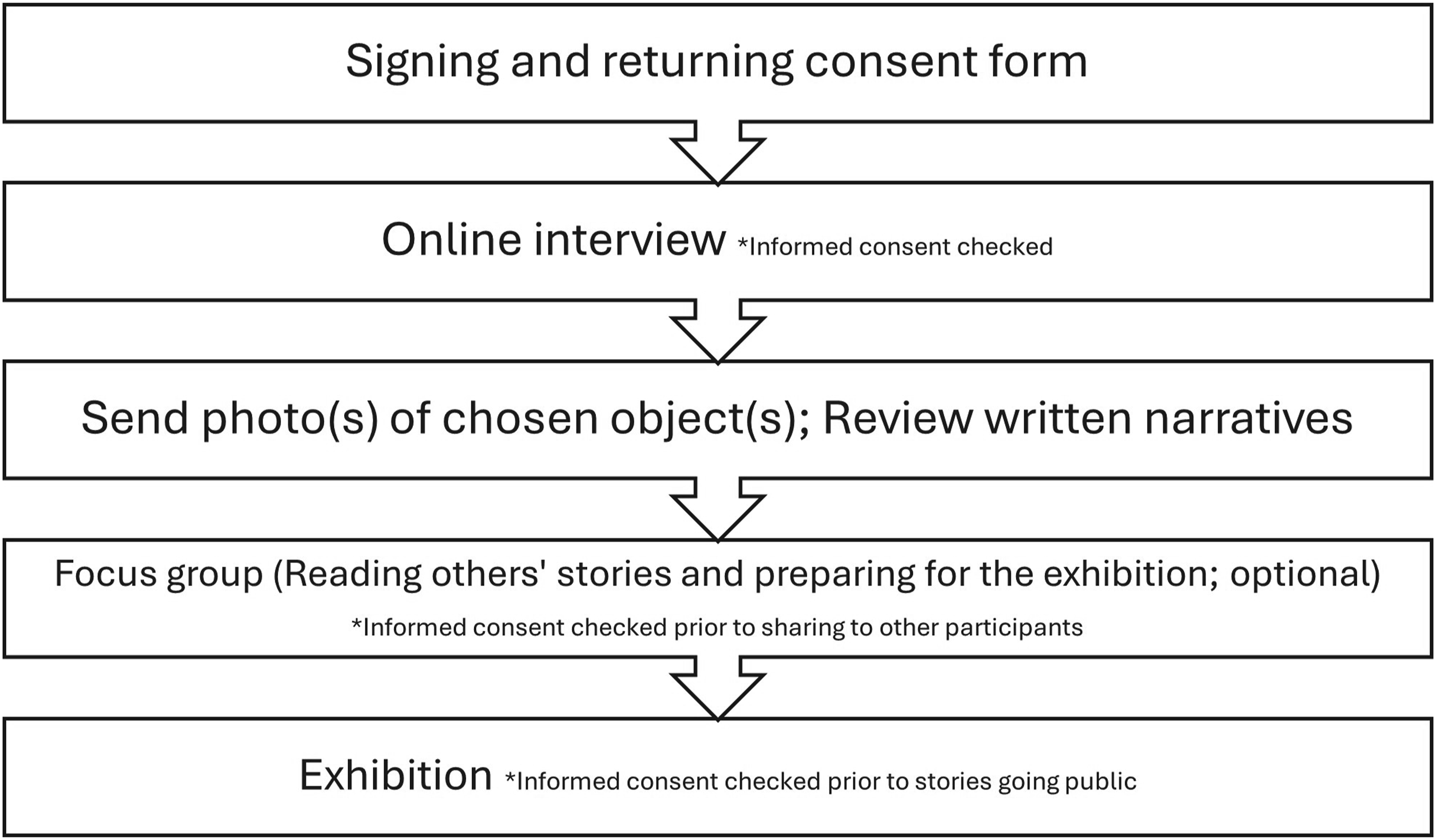
1:1 Interview
Prior to the individual interview, participants received study information including the topic guide that would be explored in the interview. They were also encouraged to identify an object or objects that related to or symbolised their recovery and to bring it/them to the interview, where possible. Semi-structured interviews (see Supplemental Information for the topic guide) took place online using Microsoft Teams for a maximum of one hour. The discussion around marginalised identities during the interviews was informed by minority stress theory. If participants struggled to recall any significant objects, example objects were suggested to stimulate reflection.
After the individual interviews, SHY transcribed the interviews verbatim using the automatically generated Microsoft Teams transcription followed by manual editing against the audio files of the interviews. The transcripts were summarised by SHY, and the edited summary was returned to the participants for review. The revised version of the summaries available on the project website (https://turning-points-eating-disorders.notion.site) and at the exhibition. The narratives and photos of the objects were collated.
Focus Groups
Following the individual interviews, participants who consented to taking part in the follow-up participatory focus groups were invited to collectively co-construct the meanings and common themes across the stories and objects, and plan the subsequent community exhibition. Two focus groups were offered in total, with four people in each group. The focus groups each lasted 1.5 hours. To ensure accessibility and inclusive participation, participants were encouraged to use the text functions or respond to the questions using the anonymised Mentimeter survey (mentimeter.com) if they did not feel comfortable in sharing their responses in front of others.
As people’s stories are fluid and may change according to context, participants were given three opportunities in total to amend their narratives: once after the initial interview, once prior to the focus groups, and once prior to the public exhibition.
In participatory and liberation psychology research, some participants prefer to own their narratives given the potential of photovoice methodology in being emancipatory and effecting social change (Gupta et al., 2019). In those cases, researchers discussed the pros and cons of using their identities and made them aware that they could opt to share their real identities as an informed choice.
Lastly, a preliminary analysis and draft Results section of the manuscript were shared with interested participants for member check. Those who wanted to be involved further were given the opportunity to be co-authors of the paper based on the International Committee of Medical Journal Editors’ authorship criteria.
Analysis
The objects/photos and associated narratives were analysed using reflexive thematic analysis (Braun & Clarke, 2022). Data saturation was not the focus of this methodological approach (Braun & Clarke, 2021). We followed Malterud et al.’s (2016) idea of information power to evaluate the richness of the dataset to ensure that it offers scope to answer our research question. Specific factors that guided our thinking included the characteristics and intersectionality of the participants, theory (minority stress theory), and quality of the dialogue. We reviewed this throughout data collection and analysis process as recommended by Braun and Clarke (2021).
In this study, we adapted the method of photovoice where instead of photos, the choice and the role of objects were analysed. A critical realist approach was used during the analysis process, from which it was assumed that individuals’ experience shape their understanding and experience of the world (Lawani, 2021).
SHY and JB independently familiarised and immersed themselves with the interview data. They coded one interview transcript together inductively; coding was then done separately and discussed on four occasions for one hour each to discuss and refine preliminary themes. The coding process was done by hand as well as on Microsoft Word. The purpose of the meetings was not to ensure reliability but was to discuss our interpretations and enrich them. Reflections were documented during these meetings. A preliminary framework was developed.
In parallel, during the participatory focus groups, the images of the objects chosen and the narratives were discussed. Participants co-analysed the findings in a 90-minute participatory workshop. The research team then shared the preliminary thematic map to get participants’ responses and feedback. SHY and JB discussed the themes that emerged in the focus groups alongside the researcher-generated themes and revised the themes. The themes were then shared with the wider team for discussion. A final thematic map was developed and checked by participants via email for consensus, readability, and whether it was understandable by members of the public and people who are neurodivergent. A final summary of findings was then shared with participants.
Reflexivity
SHY is a clinical psychologist with experience in working in ED across the lifespan and identifies as a woman from a minority ethnic group in the United Kingdom. She has an interest in arts in health approaches and community approaches. JB is a consultant clinical psychologist with 15 years of experience working clinically with people with ED. He is White, is cisgender, and identifies as male. He is interested in working with people to improve their support networks when experiencing difficulties in life. He was able to provide his view as an experienced clinician in ED and as someone who is more independent from the research process in the data analysis. PE identifies as an Indian woman and has a lived experience of anorexia nervosa and bulimia nervosa. EN is a study participant who identifies as a White British female and is a trainee counsellor. She has a lived experience of diagnosed anorexia nervosa and undiagnosed avoidant and restrictive food intake disorder (ARFID), and she also identifies as someone who is neurodiverse and has a physical disability. She uses her lived experience in her work as a trainer, peer support worker, project worker, speaker, and advocate in mental health, EDs, autism, self-harm, suicide, gambling addiction, and neurodiversity. HS is an academic psychologist who is White, cisgender, and female. Her research is focused on risk and protective factors for ED onset and recovery. US is a clinical academic and consultant psychiatrist who is “White European,” cisgender, and female. She is particularly interested in early intervention for EDs. Reflections about the iterative process of analysis and participants’ reflections are included in Supplemental information.
Participant Characteristics
Initially, the team received 44 emails from advertisements on X (formerly known as Twitter). However, those emails were sent within a short space of time with similar subject headings or no subject and typos in the emails. Two of these participants were interviewed and both declined to have their cameras turned on and their accounts of their EDs were inconsistent and seemed inaccurate at times. We excluded their data as these appeared to be imposter participants. This phenomenon has been reported in other studies (Davies et al., 2024), and participants in the present study fitted the fraudster profile identified earlier. Therefore, we changed our recruitment strategy and only accepted participants from trusted channels including University circulars and the Beat charity, where we carefully examined their emails and accounts of their EDs prior to participation. Twelve participants consented to participate; however, one participant did not reply to emails when consent was checked a second time. Her data were therefore not included. The final sample consisted of 11 people.
Demographics of the participants.
Duration of ED.
A Note About the Language Used
In the context of EDs, the definition and conceptualisation of recovery is controversial. Beyond the narrow biomedical definition of recovery as achieving full and lasting remission from the cognitive and behavioral symptoms of ED, recovery may represent something different for different individuals, such as restoring their quality of life, mood, or psychosocial functioning (Bardone-Cone et al., 2018). Whilst the term “recovery” is used here as an inclusion criterion, different participants related to the word differently, and not all used this term to describe their experiences. The intention of the broad definition was to aid recruitment as diverse communities may have different perceptions and definitions of recovery (with the only criterion of the participants having had to be discharged from specialist services for at least three months). We also acknowledge the use of the term minorities which can be misleading as certain ethnic groups are of global majority. There is a risk of homogenising the diverse groups of individuals and communities. We would like to emphasise that the language of minorities is used in the context of the United Kingdom and the societal context of some communities being marginalised.
Results
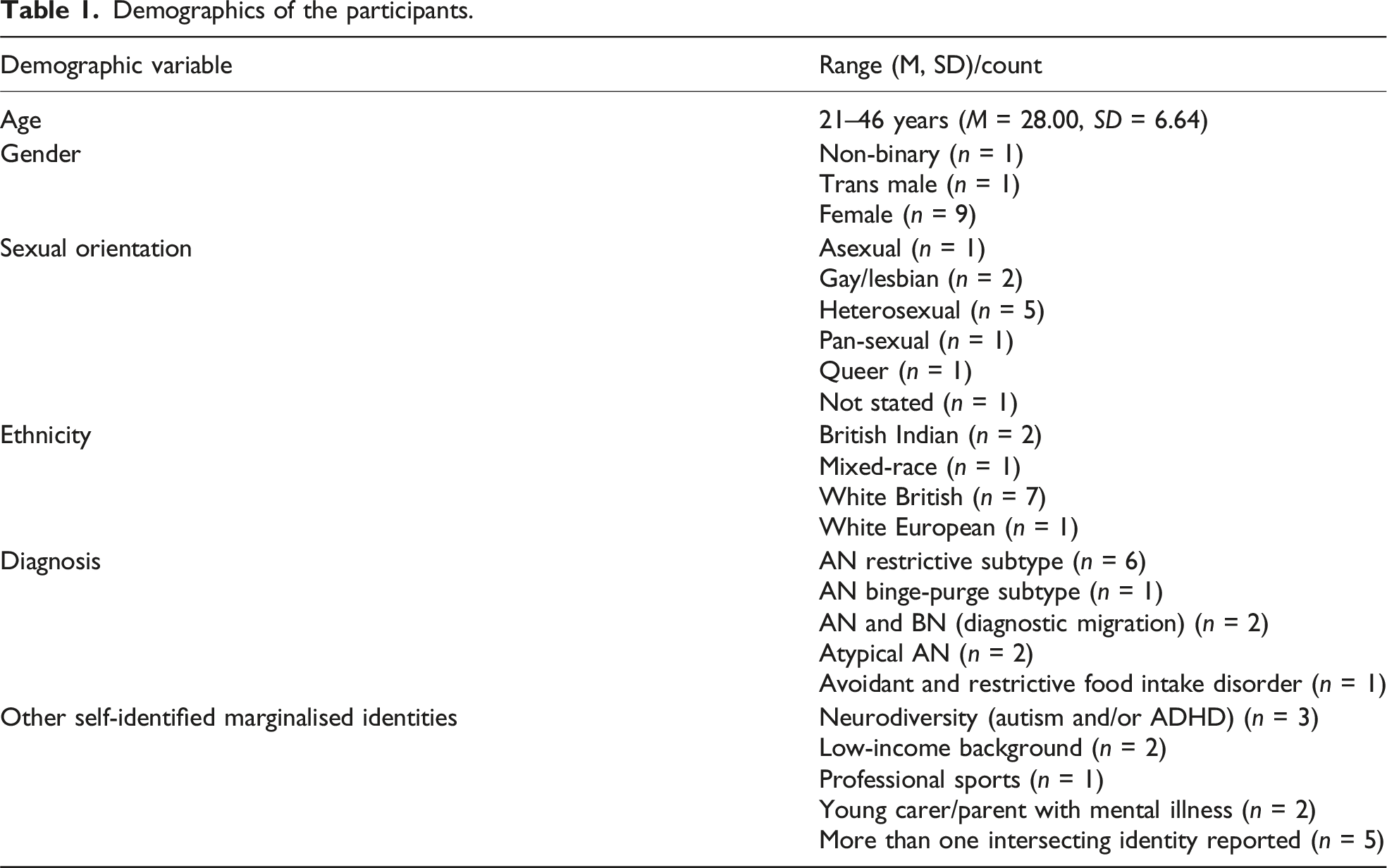
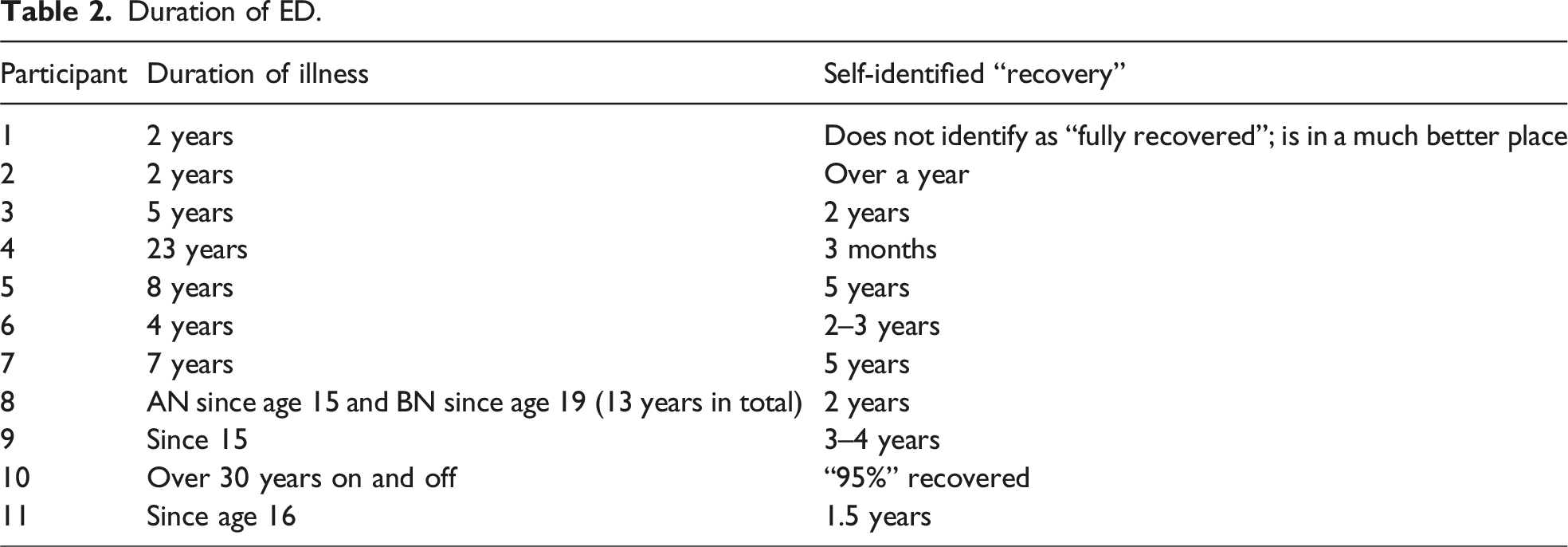
The study included 11 participants aged 21–46 years (M = 28.00, SD = 6.64), primarily female (n = 9), and with one each identifying as non-binary (n = 1) and trans male (n = 1) (Table 1). Sexual orientations included heterosexual (n = 5), gay/lesbian (n = 2), pan-sexual (n = 1), queer (n = 1), asexual (n = 1), and not specified (n = 1). Ethnic backgrounds included White British (n = 7), British Indian (n = 2), and mixed-race or White European (n = 2). Additional identities included neurodivergence (n = 3), low-income backgrounds (n = 2), and other intersecting identities such as being neurodivergent and queer (n = 5). The duration of participants’ EDs ranged from 2 years to over 30 years (Table 2).
Themes and representative objects.
Up, Down, and Around
Across the narratives, it was evident that recovery was seen as a non-linear process. Turning points encompass twists and turns, positive and negative events. Whilst some participants described the process of recovery as a roller coaster, many participants also emphasised the incremental and long-term nature of recovery, describing it as “the babiest of baby steps.” A participant described her journey with an ED that lasted over 20 years: I have called it like a roller coaster journey. So I get the ups I’ve had the downs. I’ve had my little loop, the loops and the middle, and then at the minute it’s kind of the straight on journey and let’s just keeps going and I think for me it’s, you know, because obviously the eating disorder acts as a coping mechanism for underlying emotional distress. (Participant 4)
Therapy or admission to hospital was only described by less than half of the participants as a major turning point. For others, participants described “looping” back and revisiting the therapy materials at a later date, as they initially were not able to engage with psychological therapies. I was in a bad place beyond just like I couldn’t (engage with therapy). I feel like with CBT (cognitive behavioural therapy) sometimes they want you to think your way out of a problem and like there was no way I was going to do that. And I don’t think I was properly able to like reflect on and use that CBT until probably when I was like 24, 25 and like actually start putting into practice as a more well person restarted therapy. (Participant 7)
A few participants mentioned that negative events, whilst challenging, acted as turning points and catalysts for change, such as negative treatment experiences in hospital and deaths of important people. This prompted participants to re-evaluate their situations and commit to recovery.
Participant 11 described the demoralising experience of being admitted to an adult ward, where staff seemed less hopeful about recovery. This became a deterrent for her to go back into the same situation in the future: “I think it felt like the staff (held the view of) they (the inpatients) are not gonna get better anyway …… I don’t ever wanna come back to the ward … this is horrible.”
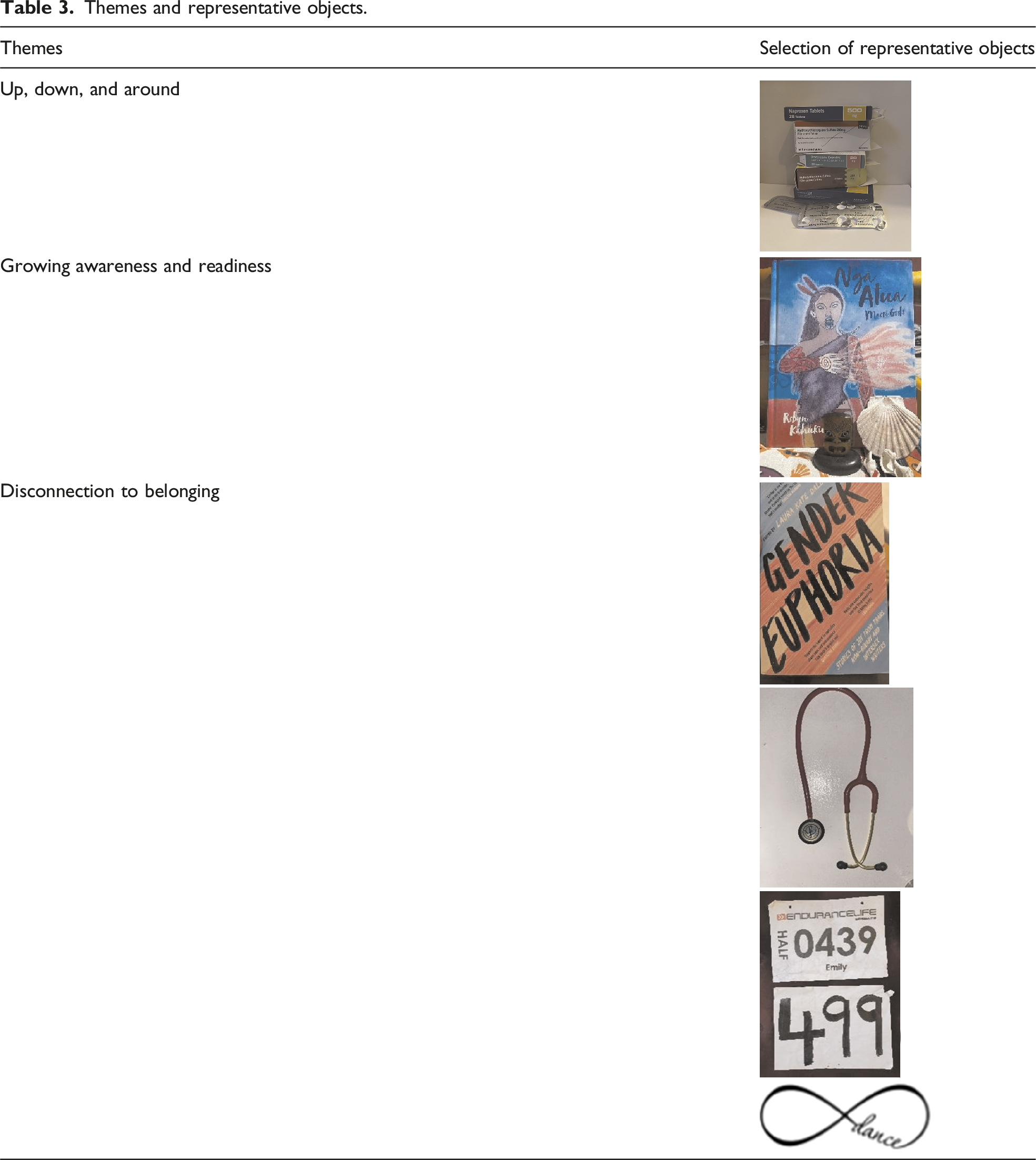
A representative object that captured this theme was contributed by Participant 5, with a picture of all the medications she has taken over the years that captured her ups and downs. She recounted the traumatic experience of being transferred to a secure unit, getting to a low point, which ultimately motivated her to “get herself together” (Table 3).
Growing Awareness and Readiness
Many participants related the first turning points to increasing awareness that “something was not right” and that “this is a serious illness,” which prompted help-seeking in relation to their ED. Whilst these turning points did not directly lead to “recovery,” several participants identified critical moments that made them realise something was wrong or that they needed to change. These moments can be from others telling them the physical consequences of having an ED or from their own realisation that their health is impacted.
Participant 1 recounted an incident of feeling unusually unwell after vaccinations: I had the COVID and the flu vaccine on the same day. And normally I really bounce back. They do not affect me, but I think it knocked me out for like 10 days where I was that actively, really unwell … I remember thinking very clearly … I’m malnourished.
Others described moments of realisation of life outside of an ED contributing to the growing awareness to pursue recovery, such as a desire for independence, or pursuing university/professional studies. For instance, Participant 8 shared her transformative experiences of traveling, which offered glimpses of a hopeful and engaging life: I went on a 14-day Caribbean cruise and then that gave me the bug and I went to Greece. I went to Paris, I went to France. I just did so much solo travelling … I cried for the first day thinking, oh gosh, I’m on my own, but by the end of it, I didn’t want to come home … I did so many amazing things that it just sort of gave me hope … I don’t want my life to be like this anymore.
Participants described how readiness for treatment or lack of it impacted treatment success. Many reported that they did not find their first treatment episode useful or that in hindsight they were not “ready” for it.
Participant 6 expressed initial reluctance when in treatment: When I went at first and with the NHS, I did not want to put on weight. I didn’t want to get better. I thought I was very happy with being extremely underweight with being having an eating disorder. That’s what I wanted. I wanted to have the eating disorder. That’s how I wanted my life. I felt very in control and very powerful.
Similarly, participant 10 highlighted a moment of confrontation with a therapist who “bluntly” questioned her willingness to change. She shared: (The therapist) He asked, “What are you willing to work towards? Because if you’re not willing to put on any weight, then we’re wasting each other’s time.” And I said, I am not willing to. So he said. “That’s fine. Come back if you ever want help” … I think he levelled with me and maybe he just read me properly because I appreciated that.
Representative objects of this theme were the seashells collected by Participant 6 during travels with a friend. Those objects became a fixture in her bedroom which reminded her of freedom (being far away from the United Kingdom and being near the ocean) and the positive impact of relationships. She made a lifelong friendship with someone recovered from an ED, giving her strength and inspiration to recover. Such objects provided tangible reminders of the moment where she realised the possibilities in life after recovery.
Disconnected to Belonging
“Not fitting in” featured prominently throughout the interviews and subsequent focus groups. This theme arises from two aspects: (1) an internal feeling of wanting to fit in and (2) being othered. Turning points occurred when participants moved from a position of feeling disconnected and othered to connecting. This process was both internal, by reconciling and embracing their identities, and external, through connecting with family members and finding like-minded communities based on their intersecting identities. The way in which people experienced disconnection and difference varied depending on participants’ individual characteristics. For example, Participant 5, who identifies as a lesbian, emphasised the desire to be seen as a normal teenager and be part of the mainstream. Participant 10, who identified as mixed-race, shared that striving for thinness was a way to gain social acceptance: I was thinking well, I don’t look white, and if I can’t look right, at least I can be thin … I would have some kind of social kudos.
Examples of othering include the difficulties in growing up in a Christian community where discussions around LGBTQ experience didn’t exist. Participant 8 recounted facing racism at school, creating a conflict between cultural identity and ED behaviors: I was experiencing a fair amount of racism. You don’t want to be associated with the Indian curries or the rice or the naan … but then you’re going home and your family are trying to do this big dinner as it’s the way they show their love. That was really difficult because you’ve got the eating disorder, but then you’ve got the bullying and the racism.
Participants also stressed that not all their marginalised identities intersected with their ED. For example, a participant described that although being asexual made them feel “weird” and isolated at times, they did not think this influenced the development or maintenance of their ED.
There was a strong narrative across stories that the final turning point came from a sense of belonging, internally within their integrated self (that was previously rejected/not accepted/not understood by themselves/others) as well as externally in society. This helped to shift their mindset to make recovery-oriented choices. This was reflected by the choice of object such as the book Gender Euphoria, representing their journey to understanding their sexuality.
Participant 5 discussed the importance of coming to terms with her queer identity and finding solidarity: The final turning point … it was probably when I came out as a lesbian when I was or came out as queer when I was like 21 … Being queer or a lesbian always felt intrinsically bad. Coming out was a massive deal, but it resolved so much for me. Accepting my identity and finding solidarity in the minority community made a huge difference. Many queer people feel like they don’t fit in because society makes us feel like misfits. But I don’t see myself as belonging to a group of misfits; rather, we were made to feel that way by society.
Engaging in meaningful activities and relationships helped mitigate the sense of otherness they experienced, including engaging more authentically with people (Participant 1), feeling supported and connected with the staff in the ward (Participant 11), and meeting a new friend who had an ED during her travels (Participant 6). Participant 7 described how joining a women’s rowing team shifted her focus from body image to strength and teamwork: I joined the women’s rowing team … in a group of women who … all they cared about was like eating or being stronger, being faster on the in the boat and doing that for the team … It was just such a like game changer … it was just so important in like changing the way I thought about things and I probably I think I increased my body weight by almost like 20% and put on muscle … The running (the compulsive exercise in the past) is not fuelling myself properly and ultimately breaking down my body’s ability to do anything. Joining the women’s rowing team is fuelling myself properly and achieving stuff.
Participant 7 chose two sets of race numbers from races they took part in. The object reminded them of the importance of strength and nourishment, embodying the change in their relationship to exercise and their body. As they put it: It (the race/the object) didn’t make everything perfect and recovery was still like elastic and spiralling and everything. But it’s like the one of the like anchors and I can cling on to and know that the food makes my body stronger, and it’s better for me … it kind of symbolises all of the work that I put into that year rowing, and how important all of those women were to me and like changing how I felt about my body.
Another example of a turning point was through significant life roles such as motherhood—providing a new perspective on her body’s capabilities and fostering a sense of pride and belonging within her family. As Participant 10 described her major turning point: My first major turning point I can remember was the day that I was stuck with my son on a lawn in the city where we live, and I was just watching, watching him, playing and thinking God how lucky I am and I just had this lightning bolt of like what on Earth am I doing like this is my life is so good now? Yes I’m still engaging in these restrictive behaviours and obsession and I should just be more present in the moment so that that was a real, and I’ve taken photos talking about that day sitting on this bit of grass and I remember being there and thinking … you don’t need to be doing this anymore. You’ve got everything, it’s wonderful … The family that we’ve made, it’s finally mine and I don’t feel, I don’t feel an outsider or a misfit … I’ve got my place in the world and my family and I’m alright.
This learning was further elaborated by participants who deliberately planned to seek new connections in new environments: Now if I move to a new place and I’ll be there for like a couple months, I’ll join a club or something. (Participant 2)
Over time, the connections made seemed to help divert participants’ attention away from disordered eating thoughts and behaviors, where participants used phrases like “I don’t need the ED anymore” or “the ED thoughts got displaced by the wider life pursuits.” The “breakthrough” could happen after years of being unwell: I made like a lot of friends on my course, more personal, amazing friends. And we went for lunch. And there’s a Subway at Uni. Everyone was like, oh, Iet’s get Subway … So that was the first time without like measuring food or counting calories or anything in like probably 8-9 years. And I just, I don’t know how it how it was like a light switch and it just I just managed it. I didn’t feel guilty afterwards. (Participant 11)
Another type of turning point that related to fostering sense of belonging was through helping others and pursuing careers which aligned with their recovery experiences. For example, several participants worked in healthcare or studied health-related disciplines. Participant 11 decided to become a medical professional and chose the stethoscope bought by her late grandmother as her representative object, symbolising ongoing support and her desire to help others. Another example was from Participant 2 wanting to go abroad for a youth summer camp, assisting other young people with activities. She described needing to be physically fit to get the job, which motivated her to eat more, gain weight, and break her dietary rules of having snacks. One participant chose to pursue a career in lived experience work following on from recovery: I got discharged from the service and I am now the lived experience worker. I can go and meet every person that’s coming in for treatment, help ensure they’re being adapted from lived experience point of view. I am actually now working with a few national services to develop, adapt their services for neurodiversity with eating disorders. I take my job as a turning point because when people come and share that story with you and go, wow, you’ve helped us take this back to our service or actually we’ve known this about you. You’ve given us new ideas and it’s almost like looking back at my younger self going, had this been there when I was going through this, this would have changed, like completely changed.
Participant 4 chose a pillow of her therapy dog that she had during her treatment as her object and noted the additional sensory function the pillow served for her as a neurodivergent person. When I don’t see Alfie (the therapy dog), I kind of remind he’s there and it’s almost like, you know, what would you be doing when I feel like this? And I’d watch a video of us … that’s, you know, my little comfort.
The object encapsulated the shift away from dietary restriction as a coping strategy.
Other participants, whilst not centring their career around their lived experiences, expressed a desire to volunteer and help others with ED as part of their own turning points. Participant 3 was passionate about advocacy about the harm of diet culture and decided to have a recovery symbol tattoo behind her ear, which reminded her of her commitment to recovery. Participant 8 described her life being hindered by the ED as she could not volunteer until she was recovered, which boosted her motivation. Participant 7 described that they were happy that they could make a difference in the world through being able to empathise with the young people who are going through an ED.
Discussion
The findings highlight the various turning points of ED recovery experienced by individuals from marginalised and underserved communities in the United Kingdom. Overall, regardless of the duration of ED, participants noted the non-linear trajectory of recovery, and turning points could result from positive life experiences and challenges. They described the interplay of growing awareness and readiness, as well as feeling connected and a sense of belonging, as important turning points. The findings also show how objects can possibly play a role in reminding people of their recovery.
The themes “up, down, and around” and “growing awareness and readiness” resonate with previous studies that recovery is often non-linear (Eaton, 2020) and involves major shifts in how the individual positions themselves vis-a-vis their illness and in their specific context. The current study adds more visual, contextualised information between the “phases” of recovery (Dawson et al., 2014). In the current study, participants did not move linearly from “tipping point” to “active pursuit of recovery.” There were multiple turning points and people went through ups and downs—“like a rollercoaster” or “babiest of baby steps.” Individuals went through multiple turning points but might only return to the learnings (such as therapy materials) years later. The current study demonstrates that similar moments of awareness and readiness occurred among diverse individuals similar to previous studies (Baudinet et al., 2024; Dawson et al., 2014). Additionally, it provides a more detailed account of how these moments of readiness occurred. For example, some participants shared specific episodic memories such as being with their children on a sunny afternoon in the park or breaking a dietary rule after going out for lunch with course mates, which felt like epiphanies.
One of the most striking findings in this study is the importance of developing a sense of belonging and the integration of parts of self (the minoritised identities) that were once rejected or not understood. Participants emphasised the importance of feeling understood and accepted by themselves and others, whether through family, friends, or like-minded communities. This is consistent with Watterson et al. (2023) finding that a sense of connection with someone who is not judgmental is important in the recovery process. Baudinet et al. (2024) highlighted that recovery is often facilitated when an individual’s life priorities and social roles become more significant than their illness identity. Whilst it has been well-evidenced that finding a new non-AN identity is key to recovery (e.g., Conti et al., 2020; Kiely et al., 2023), in diverse and minoritised individuals, there is an additional layer of sense of disconnection and not feeling belonged that is situated within the broader sociocultural context (Meyer, 2003). This indicates the possible utility of minority stress theory in relation to ED in minoritised social identities including physical disability, neurodiversity, and gender and ethnic minorities. Many participants described developmental histories fraught with feeling different, isolated, discriminated, and othered and an inability to understand parts of themselves or be understood by others. The ED can be seen as an attempt to “fit in” with the dominant and normative culture and standards, and/or to relieve distress and social stress as a result of stigma and being othered. It is also possible that increased stigma-related stress contributes to disordered eating as a coping mechanism. Thus, the turning points toward recovery then involve a process of finding a feeling of belonging in the social world that included their minoritised identities. Similar to the literature in substance misuse, the turning point leads to an identity conflict/change in identity (Brookfield et al., 2019), which displaces/shrinks the ED identity, where participants described they “do not need” the ED anymore. This may include finding like-minded communities and accepting one’s identity. For many, this identity then transformed into a helping identity where they used their lived experiences to help others.
Interestingly, while previous studies (Baudinet et al., 2024; Watterson et al., 2023) have emphasised the importance of therapy/clinical interventions in recovery, participants identified broader turning points and facilitators to recovery in this study. This divergence may be due to the different foci of the studies; where some (Baudinet et al., 2024) concentrated on the process of change within a specific clinical intervention, the current study explored recovery in a broader sense, encompassing individuals, especially minoritised individuals who felt let down by statutory services and sought alternative forms of support.
Another key finding is the role of objects in participants’ recovery journeys. The use of objects in ED recovery is seldom discussed in the literature; it offers rich visual, polytextual, and tangible insights into how individuals can find strength and motivation in everyday items that symbolise their journey. Similar to the observations of Yim (2022), these objects serve a memory-embodying function, acting as tangible anchors in the recovery journey. There is a potential for these objects to help individuals stay connected to their recovery goals. Participants often described cherishing these items, such as placing them inside a drawer with other important objects or having a tattoo as a visible reminder. Additionally, objects are not mere symbols or relics of the past (McDonnell, 2023)—from a material culture perspective, objects carry multiple meanings and are perceived as living. For example, a pillow can be a reminder of the participant’s hospital stay, whilst also providing sensory comfort that supports her present and future challenges.
Strengths and Limitations
This study has several key strengths that enhance its relevance and impact in the field of ED recovery research. A significant strength is the use of a participatory research method. By actively involving participants in the research process, the study ensures that the voices and experiences of those with lived experiences are not only acknowledged but central to the research findings. We carefully considered the power dynamics and ensured the process was not exploitative. For example, we repeated the informed consent process multiple times and checked in terms of the preference for anonymisation. Participants were reimbursed for the interviews and focus groups, and attendance to the exhibition (including transport and potential accommodation expense) was budgeted for in the grant application.
In contrast to other studies that used photovoice, the current study used a novel method where personal objects were used as a tool as well as a study aim. Visual methods, including the use of objects, carry sentimental value and facilitate interactivity with attendees. Attendees described that the personal objects provided powerful and intimate engagement between the lived experience of individuals and attendees (Yim et al., in prep). The tangibility could facilitate the dynamic meaning-making process. This adapted methodology is aligned with the goal of social change (Wang & Burris, 1997). Participants were struck by the everyday nature of the objects chosen when compared to the stereotypical pictures found on the Internet about ED, showing the possibilities of challenging social norm when this collective object archive is being displayed in the public realm.
Another major strength is the study’s focus on marginalised groups, addressing a critical gap in the existing literature, which often overlooks the experiences of these populations. The study contributes to a more inclusive, intersectional narrative and provides insights that are crucial for developing culturally sensitive interventions in clinical practice. In particular, minority stress factors seem to contribute to the maintenance of ED (e.g., not fitting in) (see the Clinical and Research Implications section). Although generalisability was not an aim of the study, it is important to acknowledge that our focus on shared features within a diverse participant group could obscure important within-group differences.
Moreover, the participant size was small and certain ED presentations, such as ARFID and binge ED, were not represented in the sample. Further research is needed to explore recovery experiences in these groups to understand the full spectrum of ED. The study also relied on self-reported recovery of ED rather than using psychometric measures or other behavioral indicators to operationalise recovery. The revised recruitment method, which relied on connections with ED charities and universities, may have inadvertently excluded individuals who are not affiliated with these organisations. Additionally, sufficient English-language skills were required for participation in the study, meaning those from linguistically diverse groups within the United Kingdom were excluded.
Researchers have cautioned regarding the methodology’s transformative and liberatory potential (Liebenberg, 2018). Particularly, researchers have argued that photovoice as a methodology does not automatically mean that any findings from it can reach policy makers or enact policy change. Therefore, it is argued that our project is policy informing rather than policy changing (Johnston, 2016; Liebenberg, 2018). We acknowledge this as a limitation of a small, standalone research project rather than a larger research programme, and therefore, the effect on actual policy change may be limited. We see this project as a starting point and ongoing efforts to understand ED using visual and narrative methods, with a longer-term goal of forming an alternative photo collection on ED to effect social change. In the subsequent exhibition, we invited funders, charity members, and policy makers to attend, in the hope of facilitating ongoing dialogue between stakeholders and people with lived experiences. The exhibition has attracted other interested stakeholders in touring the exhibition (Yim et al., in prep).
Clinical and Research Implications
The findings of this study have several important clinical and research implications. It is important to note that whilst some participants experienced a long and enduring illness history (the recovery journey took more than 10 years), recovery was possible. To further improve treatment effectiveness, clinically, there is a need to explore readiness for recovery within the context of minority stress factors. Regarding facilitating connections and sense of belonging, healthcare providers should receive training to understand the unique stressors (e.g., stigma, discrimination, and pressures of being different) faced by individuals from marginalised groups, as well as to support the person to explore their identities safely and sensitively. Some ED-focused treatments such as Maudsley Model of Anorexia Nervosa Treatment in Adults (MANTRA) include a focus on identity (Schmidt et al., 2023). Clinicians being curious about and facilitating discussion of minoritised identities and minority stress may be useful in clinical assessment, case formulation, and treatment, as the findings suggest that discovering and renegotiating one’s personal and social identity was an important turning point. In addition, fostering a sense of belonging is crucial for supporting recovery. Encouraging the development of peer support networks and community interventions that promote inclusion and belonging may also help address the broader social factors influencing recovery.
Clinicians can also utilise and facilitate the onset of turning points of change in treatment. For example, episodic memories of turning points or imagery of the future without ED may be useful targets to strengthen motivation.
From a research perspective, the study highlights the importance of inclusive research practices. Future studies should take a proactive role to include a diverse range of participants across different genders, sexual orientations, neurodiversity, disabilities, and ethnicities to develop a more comprehensive understanding of recovery processes across various groups. Further exploration of the impact of minority stress on EDs and recovery is also needed to provide deeper insights into the unique challenges faced by marginalised populations. Additionally, the study’s use of visual methods suggests the potential for these tools to be used therapeutically in clinical settings where further research is needed. For example, future research could examine if the reading about/interacting with recovery objects could be useful for people who are in ED recovery.
Supplemental Material
Supplemental Material - Turning Points in Eating Disorders Recovery Among Individuals From Marginalised Communities Using Objects: A Qualitative Study
Supplemental Material for Turning Points in Eating Disorders Recovery Among Individuals From Marginalised Communities Using Objects: A Qualitative Study by See Heng Yim, Julian Baudinet, Priya Ebenezer, Emily Nuttall, Helen Sharpe, and Ulrike Schmidt in Qualitative Health Research
Footnotes
Acknowledgements
We would like to thank the participants for their participation and continued enthusiasm for this study.
Ethical Considerations
Ethical approval was obtained prior to the commencement of the study (Health Faculties (Blue) Research Ethics Subcommittee at King’s College London, HR/DP-23/24-39830).
Consent to Participate
All procedures were performed in compliance with the World Medical Association Declaration of Helsinki on ethical principles for medical research involving human subjects.
Consent for Publication
All participants provided consent for publication.
Author Contributions
SHY: conceptualisation, investigation, project administration, formal analysis, funding acquisition, methodology, writing—original draft, and writing—review and editing. JB: formal analysis and writing—review and editing. PE: formal analysis and writing—review and editing. HS: funding acquisition, supervision, and writing—review and editing. US: funding acquisition, supervision, and writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SHY is supported by a public engagement grant from the Economic and Social Research Council (ESRC) as part of the Festival for Social Sciences. US receives salary support from the National Institute for Health and Care Research (NIHR) Maudsley Biomedical Research Centre (BRC). US and HS are also supported by the Medical Research Council/Arts and Humanities Research Council/Economic and Social Research Council Adolescence, Mental Health and the Developing Mind initiative as part of the EDIFY program, Grant/Award Number: MR/W002418/1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.