
Abstract
A co-designed, Aboriginal health practitioner–led dementia risk management program (DAMPAA) was implemented from 2021 to 2024 to address the growing concern of dementia among Aboriginal and Torres Strait Islander peoples in Western Australia. Key features of DAMPAA included group walking and yarning sessions incorporating health and well-being education twice a week, alongside a six-month home program. A theory of change framework guided a parallel process evaluation, co-developed with Aboriginal Community–Controlled Health Services and an Elders Governance Group. The evaluation involved two distinct groups: Elders who participated in the program and staff involved in its design and delivery. Qualitative data were collected through yarning interviews, focusing on the program’s implementation and impact. A brain health program for Elders was highly valued. Through group walking and yarning, the program supported a deeper connection to Country and strengthened community connection enhancing social and emotional well-being for Elders as well as program staff. A key learning was the significance of an Elders-informed health program, delivered by local Aboriginal people at an Aboriginal Community Controlled Health Service, creating a space that strengthens connection and a sense of belonging for Elders. The process evaluation validated the importance of the DAMPAA program. The DAMPAA program and resources have since been integrated into Elders’ health programs across all service partners, demonstrating its relevance and potential for broader application.
Background
It is through our Elders that the spirit of Aboriginal people is kept alive. (Walker, 1993)
Aboriginal and Torres Strait Islander people (hereafter respectfully referred as Aboriginal (Western Australia Department of Health, 2015)) are Australia’s First Peoples, with a rich history marked by resilience and cultural strength safeguarding the oldest continuous culture on Earth (Paradies et al., 2015; Usher et al., 2021). In this manuscript, the term “Elders” is used interchangeably with older Aboriginal people. Elders are revered as knowledge keepers and cultural custodians (Kickett-Tucker et al., 2016), playing a pivotal role in safeguarding and imparting their wisdom to younger generations that guides Aboriginal and non-Aboriginal communities forward (Busija et al., 2020; Royal Commission on Aboriginal Peoples, 1996). It is therefore imperative to ensure that Elders are ageing well and can perform their important roles effectively.
Dementia poses a significant and escalating health and aged care challenge for the broader population in Australia. However, Elders are at increased risk of incident dementia, with age-adjusted dementia prevalence approximately three to five times greater than for the general Australian population (Australian Institute of Health and Welfare, 2024). This disparity reflects the complex interplay of historical, social, and cultural factors that have shaped the health of Aboriginal people (Paradies et al., 2015; Royal Commission on Aboriginal Peoples, 1996; Walker, 1993). These factors include the impacts of colonization, such as the dispossession of land, suppression of culture, forced removals, and intergenerational trauma. They also encompass systemic racism, socioeconomic disadvantage, and limited access to culturally safe and appropriate health services (Paradies et al., 2015; Royal Commission on Aboriginal Peoples, 1996; Walker, 1993). The current strategic direction of the Western Australia Aboriginal Health and Well-being Framework (Western Australia Department of Health, 2015) supports the need to create culturally safe, evidence-based prevention and early intervention initiatives where Elders grow old on Country, maintain culture, and pass on their knowledge and stories. When asked about Elders’ perceptions and priorities of ageing well, they expressed concerns in performing their role due to an array of chronic conditions impacting their physical, cognitive, and mental health (McCausland et al., 2023). Perceptions of dementia in Aboriginal and Torres Strait Islander communities are diverse. In some communities, it may still be seen as a natural part of ageing (Arabena, 2007; Arkles et al., 2010); however, other community perspectives reflect the current evidence (Livingston et al., 2024), including the dementia risk factors of older age, head injury, social isolation (Smith et al., 2011), unhealthy lifestyle, and trauma (Gubhaju et al., 2022). Although awareness is growing, dementia-specific education and knowledge remains a community priority (NHMRC National Institute for Dementia Research, 2020), with fear and denial being additional barriers to accessing related health services (Gubhaju et al., 2022). Nonetheless, strong cultural values around looking after older family members on Country persist in Aboriginal communities (Cox et al., 2019; LoGiudice et al., 2021), with Aboriginal caregivers highlighting the importance of culturally safe, community-based, and community-led dementia care (Smith et al., 2011). Significantly higher prevalence, earlier onset, and increasing incidence of dementia among Elders (Li et al., 2014; Lo Giudice et al., 2016; Radford et al., 2017; Russell et al., 2021; Temple et al., 2022) underscore the urgency of implementing effective strategies.
While some community-based programs, such as the Looma Healthy Lifestyle program, have shown promise in addressing specific risk factors for chronic diseases (Rowley et al., 2000), there remains a need for dementia care and prevention models that are culturally safe and community-based, and incorporate the knowledge and expertise of Elders (Dahlberg et al., 2018; Smith et al., 2011; Wettasinghe et al., 2020). Trauma-informed principles are essential in this context, as they recognize the profound and ongoing impacts of historical, intergenerational, and institutional trauma on Aboriginal communities (Dudgeon, Wright, et al., 2014), and when embedded into practice, they strengthen cultural safety by supporting healing and self-determination (Tujague & Ryan, 2021), both of which are critical to building trust and ensuring respectful, responsive dementia prevention and care for Elders. In collaboration with Aboriginal Community–Controlled Health Services (ACCHSs) and guided by an Aboriginal Elders Governance Group (Smith et al., 2020; University of Western Australia, 2020), a Dementia Risk Management and Prevention Program for Aboriginal Australians (DAMPAA) was co-designed to reduce cognitive decline and functional impairment in Aboriginal Australians aged 45 years and over, and evaluated using a randomized controlled trial (Mateo-Arriero et al., 2023).
Assessing the impact of health interventions, especially in unique contexts like Aboriginal communities, involves a deeper understanding that goes beyond simply assessing program outcomes (Moore et al., 2014). Process evaluation has evolved from focusing solely on the planning phase to a more advanced approach that comprehensively examines program implementation, revealing the mechanisms through which a program achieves its effects, as well as the contextual factors influencing its success (French et al., 2020; Moore et al., 2014; Saunders, 2016). It is therefore a critical tool in understanding program effectiveness and identifying areas for improvement in tailored health interventions like DAMPAA (French et al., 2020; Saunders, 2016). The theory of change (ToC) framework further enhances this process by providing a visual roadmap of the causal pathways through which the intervention is expected to achieve its desired outcomes (De Silva et al., 2014; James, 2011; Vogel, 2012). Application of ToC clarifies the underlying assumptions, activities, and expected outcomes, enabling a comprehensive assessment of program implementation and impact (Breuer et al., 2016; Coryn et al., 2010). While ToC has been used in various contexts, there is a recognized gap in its application within intervention programs and evaluation analysis, particularly in conjunction with randomized controlled trials (Breuer et al., 2016; Coryn et al., 2010; De Silva et al., 2014). This gap was identified and addressed while developing the DAMPAA program and evaluation protocol (Breuer et al., 2016; Mateo-Arriero et al., 2023).
This article presents a detailed process evaluation that was conducted in parallel with the DAMPAA program. The primary objective is to identify and analyze the key enablers and barriers impacting the DAMPAA program and provide recommendations to inform future implementation strategies. Findings from this evaluation will be valuable to researchers as they can apply the ToC framework to develop robust process evaluation protocols for similar tailored interventions and improved resource allocation that address the needs and perspectives of Aboriginal people.
Methods
Study Context and Design
The DAMPAA program involved twice-weekly group sessions that combined walking and yarning with health and well-being education, complemented by a six-month home-based component. A ToC framework underpinned the DAMPAA program protocol and guided a parallel process evaluation assessing its implementation and impact. See Box 1 for a brief description of the DAMPAA protocol (Lalovic et al., 2024). The Dementia Prevention and Risk Management Program for Aboriginal Australians (DAMPAA) study is a co-designed, culturally appropriate, AHP-led, risk management program implemented between 2021 and 2024 (inclusive). Participants were recruited in collaboration with ACCHSs via yarning workshops and community expos, and through a snowballing technique involving recommendations from other participants. People who agreed to participate after meeting initial inclusion criteria provided written informed consent to be in the study. The term “DAMPAA walking and yarning program” is more culturally acceptable than “intervention.” The DAMPAA walking and yarning program comprised two stages, action (1–6 months) and maintenance (7–12 months). During the action stage, participants engaged in twice-weekly group walking and yarning sessions supplemented by a third session at home. Led by trained professionals, sessions included warm-up, walking, strength and balance exercises, stretching, and cool down, lasting up to 90 minutes. Personalized goal setting and health education sessions (brain health, good tucker, physical activity, well-being, falls prevention, and diabetes management) were integrated from week 5 onwards. Medication reviews and adherence monitoring strategies were also implemented. A six-month follow-up assessment concluded the action stage. The maintenance stage involved three weekly sessions, conducted independently or in community spaces, with progress monitored via weekly communication. A final 12-month assessment and process evaluation interviews wrapped up the program. Elders preferred the term “usual care” over “control group.” Participants randomized to the usual care group were followed up with 6- and 12-month assessments. A detailed description of assessments can be found in the study protocol (Lalovic et al., 2024). Participants were sent a general dementia education pamphlet via mail within two weeks of randomization by the AHPs. The pamphlet contained brief information on dementia risk factors for Aboriginal people. Outcome measures were recorded at baseline, 6 months, and 12 months. The primary outcome was cognition, measured by the KICA-Cog (LoGiudice et al., 2006; Smith et al., 2007). Process outcomes were explored through in-depth interviews with project staff and through surveys and/or yarning groups with participants. Other secondary measures included daily function (KICA-Function tool) (LoGiudice et al., 2006), death (follow-up with next of kin), quality of life (GSGL tool) (Smith et al., 2020), cardiovascular risk factors, and number of falls in the previous six months.Box 1. DAMPAA Protocol
Background
Participants and Recruitment

DAMPAA Program
Usual Care
Outcome Measures
The process evaluation, guided by a collaboratively developed ToC framework tailored to this project, aimed to assess program fidelity, identify barriers and facilitators to success, and gather participant feedback to inform future modifications (Breuer et al., 2016; Mateo-Arriero et al., 2023). The ToC diagram developed for DAMPAA (Mateo-Arriero et al., 2023) (see Figure 1) explicitly outlines the program’s intended outcomes (improved daily function, cardiovascular risk management, falls reduction, quality of life, and reduced cognitive decline), the resources and activities required to achieve these outcomes, and a series of 10 underlying assumptions necessary for program success (Mateo-Arriero et al., 2023). These assumptions addressed factors such as the validity of the screening tool, the availability and training of Aboriginal health practitioners (AHPs) and exercise physiologists, participant attendance and engagement, the appropriateness of exercise and education content, medication management, and goal-setting practices (Mateo-Arriero et al., 2023). The ToC framework allowed for the evaluation of both short-term and long-term outcomes of DAMPAA and provided a basis for iterative adaptation and refinement through ongoing evaluation. DAMPAA theory of change diagram developed by Mateo-Arriero et al. (2023). ACCO, Aboriginal Community–Controlled Organization; AHPs, Aboriginal health practitioners; KICA, Kimberley Indigenous Cognitive Assessment tool.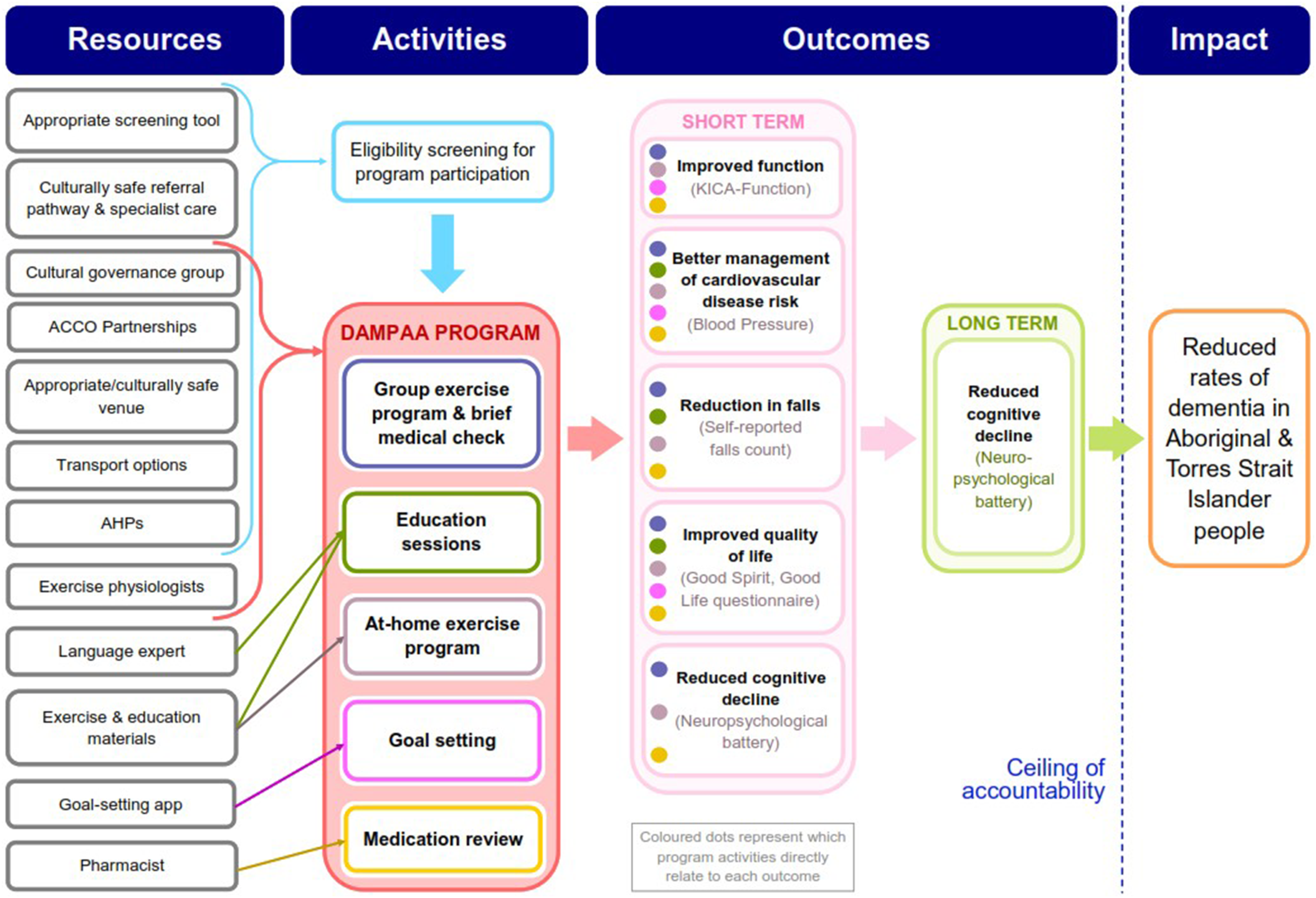
The study employed Indigenous research methodologies (Wilson, 2008), prioritizing the voices, experiences, and recommendations of Elders who were DAMPAA participants, or DAMPAA Elders Governance Group members (Mateo-Arriero et al., 2023). AHPs were employed, and they facilitated yarning circles, a culturally significant and respectful method that encourages storytelling and deep sharing within a culturally safe space (Bessarab & Ng’Andu, 2010; Geia et al., 2013; R. L. Smith et al., 2020). Our continued partnerships with ACCHSs ensured the process evaluation was conducted at trusted and culturally safe spaces for Aboriginal people (Clapham et al., 2024).
Ethics Approval
This study was conducted in accordance with ethical guidelines and received approval from both the Western Australian Aboriginal Health Ethics Committee (#867) and the University of Western Australia Human Research Ethics Committee (RA/4/20/4944).
Participants
Two distinct groups of participants were involved in the process evaluation. The first group included Elders who participated in the DAMPAA program from three program sites across the Perth metropolitan area. Eligibility criteria for Elders are described in Box 1. The age range of 45–90 years was chosen based on the earlier onset of dementia in Aboriginal and Torres Strait Islander peoples, with diagnoses often occurring 10–20 years earlier than in the general population (Li et al., 2014; Lo Giudice et al., 2016; Russell et al., 2021). The second group of participants included staff members involved in the DAMPAA program design and delivery. This included AHPs, an exercise physiologist and trial coordinator, a pharmacist, and a chief investigator (Lalovic et al., 2024).
Researcher Reflexivity
The research team comprised experienced researchers with expertise in collaborative health and well-being research with and for older Aboriginal people. Authors LY (Advanced Certificate in Aboriginal Health, AHP), LM (Bachelor of Science majoring in Exercise and Health), NL (AHP), and AR (PhD in Health Sciences) facilitated yarning circles and interviews with Elders and DAMPAA staff members. LY, a Yamatji Wongi Noongar woman; NL, a Yamatji Noongar woman; and LM, a Bardi woman; were instrumental in providing a safe space for Elders to share their views and stories given their deep understanding of Aboriginal culture and health practices. KS (PhD), a non-Aboriginal researcher with two decades of experience in Aboriginal health research, provided essential methodological and scientific expertise. DB (PhD), a Bard/Yindjibarndi woman and an experienced Aboriginal qualitative researcher and leader in capacity building for Indigenous health research, provided academic and cultural supervision. AR, a non-Aboriginal researcher raised in an Indian cultural context, managed the project under the supervision of KS and DB. AR’s background in qualitative research in Aboriginal community settings, combined with nine years of experience in research project management, provided a strong foundation for the methodological rigor and cultural sensitivity of the study.
Throughout the study, researchers engaged in reflexive practice to critically examine their own assumptions, biases, and positionality in relation to the research process and the communities involved. This included regular team debriefing sessions, journaling, and consultation with the Elders Governance Group to ensure cultural sensitivity and ethical research practices.
Data Collection
Elders participating in the DAMPAA process evaluation engaged in yarning circles, a method rooted in Indigenous knowledge systems. This was used to create a safe and respectful space for Elders to share their insights and experiences, ensuring that Elder’s voices were central to the research process (Bessarab & Ng’Andu, 2010; Geia et al., 2013; Kennedy et al., 2022; R. L. Smith et al., 2020). Yarning circles were facilitated by Aboriginal researchers (LY and NL) and notes taken by a non-Aboriginal researcher (AR). Yarning circles were held at respective program sites as they provided a safe and comfortable space for Elders to share their experiences, perspectives, and recommendations regarding the program. Exit interviews were also conducted with Elders at the conclusion of the program to further explore their individual experiences and perspectives.
Staff members involved in designing and delivering the DAMPAA program participated in yarning interviews every six months throughout the implementation period. These interviews focused on their experiences with program delivery, challenges encountered, and perceived successes in achieving the ToC-defined outcomes. Staff interviews were facilitated by a non-Aboriginal researcher (AR) and were held at a place convenient for staff members.
All yarning circles and yarning interviews were audio-recorded using a digital recording device, with participants’ consent obtained prior to recording. Recordings were securely transferred to a secure university storage site and subsequently deleted from the recording device.
Analysis
Qualitative data from the yarning circles and yarning interviews were transcribed and imported to NVivo software to conduct a reflexive thematic analysis (Braun & Clarke, 2022). Reflexive thematic analysis highlights researchers’ active role in the interpretive process and offers a robust and flexible process guideline to navigate through the data (Braun & Clarke, 2021). In the context of process evaluation, reflexive thematic analysis allowed an inductively oriented experiential analysis prioritizing Elders’ voices while also enabling a critical analysis of staff interviews regarding learning experiences associated with the DAMPAA program implementation. The analysis process involved familiarization with the data that entailed repeatedly reading through the transcripts and listening to audio recordings giving particular attention to the subtleties in the Elders’ narratives, as their voices were prioritized in the analysis. By becoming fully immersed in the data, an initial line-by-line semantic coding was conducted to capture surface meanings of Elders’ experiences and staff’s perspectives of the DAMPAA program. This was followed by an in-depth latent coding to identify conceptual meanings of participants’ experiences and perspectives. Recurring patterns and shared meanings across latent codes were used to generate initial themes. These themes were then refined, defined, and renamed through iterative discussion and review among the research team ensuring deeper understanding, interpretation, and reflexivity of Elders’ and staff’s experiences and perspectives (Braun & Clarke, 2021). Our approach was rigorously evaluated to ensure that Indigenous ways of knowing, being, and doing were respected and remained central to the interpretation.
Results
Process evaluation data were collected from 17 participants (7 staff and 10 Elders) across three program sites. Staff members (two men and five women), including an exercise physiologist and program coordinator, AHPs, a pharmacist, and the chief investigator, participated. Elders (three men and seven women) participated in yarning circles and individual exit interviews. A total of 21 yarning interviews (staff members) and 10 exit interviews (Elders) were conducted between 2022 and 2024, supplemented by two yarning circles with Elders.
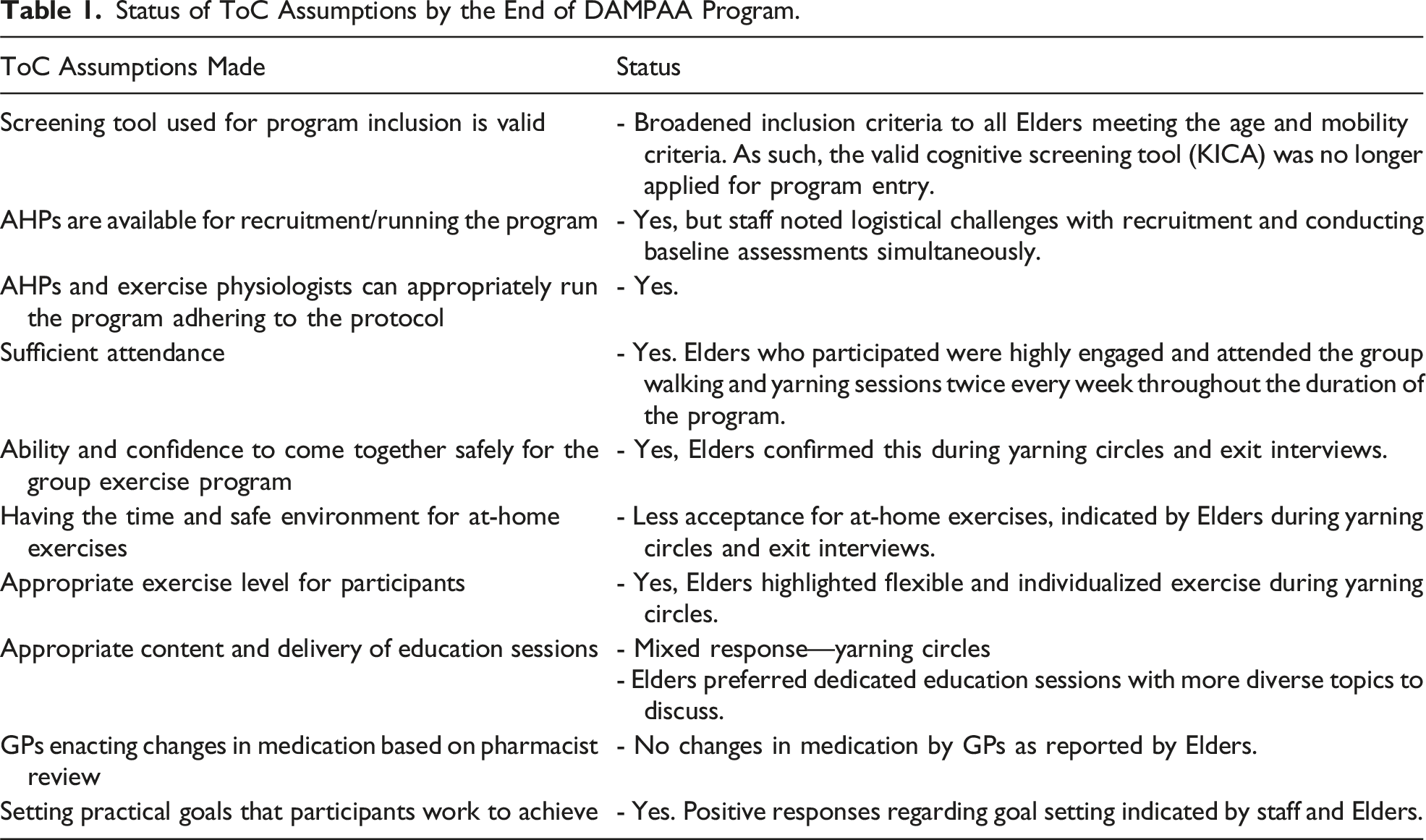
Status of ToC Assumptions by the End of DAMPAA Program.
Brain Health Programs for Elders—An Identified Gap in the Community
Elders expressed their gratitude for the DAMPAA program specifically being designed for them, which incorporated both walking and yarning components. Their appreciation extended to the entire program. I really, really love doing [this program]. The staff is so understanding and very gentle with our exercising, and I enjoyed every bit of it. (Elder, yarning circle) Thanks to everybody that put this program together. (Elder, yarning circle)
Elders highlighted the importance of programs like DAMPAA in promoting social connection and engagement and offering opportunities for cognitive stimulation and physical activity. Elders stated that such initiatives were important in addressing social isolation, and sedentary behaviors common among ageing populations in their community, and in maintaining their physical and mental well-being. And this is why the Elders and that, they need companions, they need to have these similar programs to get them out of their house, to do things, to keep their memories, you know, sharp and stuff. (Elder, yarning circle) But really something that’s really needed in the community because a lot of our old people … when the grandkids not around, they just sit down and don’t do much. (Elder, yarning circle)
Staff members who facilitated the DAMPAA program observed the positive impact of the program on social interaction and community engagement, reinforcing the Elders’ desire for programs that promote connection and combat isolation. The highlights are that the resilience of the people—they still wanna learn. They still wanna do this. And if anything, COVID has highlighted the need to get out and yarn. Get out, mix with people, go walking, reconnect with the land, things like that. That’s really important to them now. And so, that’s a highlight that this program is needed. (Aboriginal health practitioner, female)
The strong demand for brain health programs was also reflected through the positive reception from the partnering organizations. And every organization we’ve gone to and talked to, they’ve said this is such a great initiative. It’s something that’s really needed and they’ve always welcomed us with open arms and been very accommodating. (Research staff, non-Aboriginal, male)
Elders highlighted the importance of making brain health programs accessible to everyone, regardless of age or background, and suggested that starting such programs at a younger age could be beneficial. I think it should be available everywhere, especially for our mob and that should start maybe even younger. (Elder, female, exit interview)
Similarly, staff highlighted the program’s crucial role in raising awareness about dementia, reducing stigma, and empowering Elders and their families with knowledge and understanding. This would be a fantastic program … It’s not as doom and gloom as you think it would be. That’s why I think it’s a program that needs to be done. It needs to get out there. (Aboriginal health practitioner, female)
Elders hoped that brain health programs like DAMPAA would facilitate greater engagement with healthcare providers. We hear about it all the time from the health services that our mob, especially the Elders, they get the lowest access to services, …. but hopefully with this program, we’ll have a lot of people. (Elder, yarning circle)
They also emphasized the need for culturally informed and thorough medication reviews through similar programs that target Elders in the community. A lot of us don’t know what (medication) we’re taking some time, whether it might be affecting our kidneys or something else. (Elder, female, exit interview)
Walking and Yarning—Strengthening Connection and Well-Being
The walking and yarning activities were the most cherished aspect of the DAMPAA program for many Elders. The social element of the program was a primary motivator. Having it in a group and in a community is good because it’s like you got other people motivating you. (Elder, female, exit interview)
The walks and yarning circles provided opportunities for Elders to connect with friends, family, and community members, promoting a sense of belonging and support. I loved being around these guys. I love the walking, the sitting around, sharing and yarning. (Elder, female, exit interview)
Staff members also observed similar engagement and connection while interacting with Elders. The big thing is just learning about the dementia, getting it out to them, is a good thing, giving them more awareness to them about it, and good relationships along the way, good friends, keep in touch with them, that’s really good. Good highlights of this, getting them out. Some of them go through their stuff and when they come and yarn with us, it’s the best feeling, talking. It’s good for us and good for them. (Aboriginal health practitioner, female)
Beyond the social connection, the physical benefits of walking in the context of a supportive group environment were highly valued, underlining the program’s ability to encourage physical activity in a way that feels safe and enjoyable for Elders. As you get older, you know, I couldn’t go jogging around the street on my own. I’d rather be in a group. (Elder, female, exit interview)
The combination of physical activity and social interaction contributed to improved mental and emotional well-being, with many Elders reporting feeling less stressed and more motivated after participating in the program. It gets people activated and talking, instead of sitting at home, I’ll be at home stressing. So, I get out and talk to different people. (Elder, male, exit interview)
Such positive influence was also observed by program staff. But the highlights are watching these people come out of their shells from when we first saw them to now. (Aboriginal health practitioner, female)
Moreover, the yarning component of the program offered a safe and supportive space for Elders to share their stories, experiences, and concerns. And that connection was just even stronger because some of the trauma issues that they were discussing, because they realized, they weren’t the only ones, it made a big difference. (Aboriginal health practitioner, female)
This highlights the therapeutic value of yarning in promoting emotional well-being and reducing feelings of isolation among Elders.
For many Elders, walking and yarning on Country was a deeply meaningful experience. The opportunity to connect with the land, share stories, and pass on cultural knowledge was a source of pride and empowerment for Elders. I think because it’s like a little community base here. So, the venue—and also remember the main venue that we used was the river, so that was really good, scenic, nice in the fresh air. (Elder, female, exit interview)
Staff observed this as a source of joy and upliftment for Elders. They really love it … They really enjoyed that connection to Country aspect and getting outside and walking in the fresh air. (Research staff, non-Aboriginal, male)
A Culturally Safe and Flexible Program Delivery
Elders felt comfortable and respected throughout the program, facilitated by culturally sensitive staff who understood and valued their perspectives. They’re [Aboriginal health practitioners] excellent, yeah. Very friendly. You could actually talk to them about anything … they were concerned about all of us. (Elder, female, exit interview)
This culturally safe environment encouraged open communication and trust. Yeah, well, because (name) and (name) is, you know, Indigenous, as well and I think you sort of automatically just feel comfortable. (Elder, female, exit interview) They make you feel at home when you come here. (Elder, male, exit interview)
Elders commented positively on staff’s proactive approach to addressing their needs, He [exercise physiologist] was very good in that sense that he incorporated exercises to the other participants a little bit older than me. He was really good. (Elder, female, exit interview)
Staff members further elaborated on their participant-centered approach, saying, So, if I have to, I’ll go and do one-on-one sessions with her at home. Not because of the – well, not just because of the program, but because I know it’s gonna help her and we can get her to come back. (Aboriginal health practitioner, female) (Be)cause we can’t go walking or sometimes it’s just the participant’s individual level and there might be an exercise that they’re not comfortable or they struggle to do or whatever, so we have to modify and adapt to them what we sort of do as we’re going and as things come up. (Research staff, non-Aboriginal, male)
The program’s yarning and interactive approach to education facilitated engagement and a two-way knowledge sharing. Staff members actively listened, encouraged participation, and validated the Elders’ wisdom and experiences. They found deep satisfaction and fulfillment in their interactions with the Elders. It’s the sitting and laughing and listening to the stories. That’s my joy. That’s what I take away. (Aboriginal health practitioner, female)
A Need for Dedicated and Diverse Education Sessions
Elders expressed a strong desire for more learning sessions regarding accessible and practical health information specifically focusing brain health and dementia. I mean, the walks are lovely. The walks are really good. I enjoy them because you have a good talk and everything, but yeah. If you threw some other health things in, you know. (Elder, yarning circle) You’ve got to keep the conversation going, the stories. This is very interesting, the one, especially with the brain because we don’t know nothing about the brain. (Elder, female, exit interview)
Staff members responded similarly, indicating the importance of tailoring the educational content to the participants’ unique needs and interests. They emphasized the need for interactive sessions, adaptable to different learning styles and preferences. So, make sure there is that element of flexibility and variability to keep people engaged. So, it’s not going to be repetitive every single time, like you do need some variability. (Research staff, non-Aboriginal, male)
The potential benefits of involving participants in selecting topics for education sessions were highlighted. We should have a core of—or a suite of subjects and ask them what do they want to touch on, what information would they like about heart disease, lung disease, trips, falls, whatever, future exercise programs and things like that. What happens at the end of this? Can we give them more stuff, more information? (Aboriginal health practitioner, female)
Recruitment Hurdles in a Pandemic Research Setting
The COVID-19 pandemic had a profound impact on the program. While the Elders themselves did not directly comment on the pandemic’s influence, its indirect effects were evident in the challenges faced by the staff. They had to adapt to new safety measures, which necessitated revision of the program protocol causing delays and disruptions impacting the flow and implementation of the program. They were going okay but then [COVID] started changing things and even in the protocols that we had in place. (Aboriginal health practitioner, male)
The pandemic also took a toll on staff well-being. The constant changes, uncertainty, and challenges associated with adapting to the new normal created stress and impacted optimism. For a while there with COVID, it was quite depressing because we just didn’t have much good news to share. (Research staff, non-Aboriginal, female)
Public health restrictions and concerns about safety contributed to a decline in participation. So, our confidence was pretty low over that time. And then beginning of this year, we got all our hopes up because all the Elders are starting now to ask [to join the program]. (Research staff, non-Aboriginal, female)
In addition to these challenges, staff members also highlighted the difficulties in finding alternate project sites due to closures and restrictions, as well as the reluctance of some community members to get vaccinated, further complicating program implementation. We actually got good feedback from people that they liked it, you know, they enjoyed it, and they enjoyed it at [service name]. Yeah, after the pandemic, it’s just we couldn’t use the venue anymore, you know, stuff like that. We need to look for somewhere else. Yeah, it took a while. (Aboriginal health practitioner, female)
The concept of randomization, where individuals have an equal chance of being assigned to either the DAMPAA or usual care group, particularly within a community-based setting, was less favored by Elders. An opportunity for the usual care group to join the program at a later stage was provided; however, this was also viewed less favorably by Elders. Elders completing initial assessments without immediate access to the program was perceived as the program being unnecessarily exclusive. I think just that whole process is quite intensive, and then also the fact that participants are told, “You’re gonna go through all this and there’s still a 50% chance you actually won’t be in the program…. It doesn’t always make sense to move on. “Why do I do all this and then I can’t do the program?” (Research staff, non-Aboriginal, male)
The baseline assessment process, which included an array of neuropsychological tests, created a sense of frustration among Elders due to the lack of immediate feedback on test results. What I would’ve liked, though, is the results of that. I would’ve liked to have known where I sat for my age … (Elder, female, exit interview)
This disconnect between data collection and individual health insights can be a source of disengagement, especially when working with Elders who may have different expectations regarding healthcare interactions.
The time commitment required for the assessments and the staggered enrolment process were highlighted as difficulties by staff members particularly in scheduling and coordinating assessments. It’s quite hard to deliver it in that respect because of the staggered interest. (Research staff, non-Aboriginal, male)
The extended time between initial interest and program commencement also led to a loss of momentum and, in some cases, a decline in interest. A lot of them, if you sign them up, you don’t get onto them straight away with your neuropsych and the processes, they lose interest and run. (Aboriginal health practitioner, female)
Elders Caring for Family
Elders’ commitment to their families, particularly in caring for grandchildren or spouses, often took precedence over their participation in the program. A lot of [Elders] are carers for grandkids and so obviously all of those things would come first naturally. (Research staff, non-Aboriginal, male)
The unpredictable nature of family responsibilities made it difficult to maintain consistent attendance, impacting both recruitment and program delivery. Most of the [Elders] have grandchildren they actually look after. So, yeah, that’s another responsibility and how did they make it, like, we’ve got a guy with us now and we haven’t seen him for a few weeks, but he looks after his grandchildren and his wife. (Aboriginal health practitioner, female) I guess, what else with recruiting is consistency in appointments. So when we have someone interested … and if something comes up that they have to reschedule, it just throws our timeline way off. (Research staff, non-Aboriginal, male)
Elders’ own health challenges also emerged as a significant factor affecting their ability to consistently engage in the program. Chronic illnesses, medical appointments, and unexpected health setbacks often led to missed sessions or withdrawal from the program. So, they come in one week then the next week, they’ve got an appointment and then they don’t come in the next week because of their health issues. (Aboriginal health Practitioner, male)
While these care priorities disrupted the program flow, the staff expressed empathy and understanding for the Elders’ priorities, highlighting a culturally sensitive approach. The reality of it, which we can completely understand. And we’ve even had a participant withdraw because their spouse got quite unwell and just became a full-time carer for them. (Research staff, non-Aboriginal, male) Because I’ve noticed lately a lot of deaths have been happening. One of the clients we had on this group, we had a funeral on Tuesday. We got a funeral tomorrow. (Aboriginal health practitioner, female)
Culturally Relevant, Community-Owned Programs Delivered by Local Experts
Elders expressed a clear preference for the program to be based in Aboriginal health services or community-controlled organizations and perceived these locations as safe, welcoming, and culturally relevant. Probably in all of them, especially in the Aboriginal health service. I mean if they could access it there and just have that [in] community organizations. (Elder, female, exit interview)
The physical location itself played a role in participant comfort and engagement. Elders appreciated spaces that were dedicated to their community, offered ample room, and minimized distractions. Because this is more our place. We’re not going into somebody else’s space. (Elder, female, exit interview)
Elders also touched on the historical trauma and the lasting impact it has on their trust in services provided by non-Aboriginal organizations. They highlighted the importance of running programs within Aboriginal community–controlled organizations, where cultural safety and understanding are prioritized. It’s always been an issue with our mob. Because we don’t like to talk about it, but historical contact with non-Aboriginal people, they were very cruel to our people, and they put us down and made us feel like we didn’t know nothing. So that’s why the access to services now, our mobs are cautious about taking it on. They hear about this program, so they all wanna do it there [Aboriginal community–controlled organization]. (Elder, yarning circle)
Program staff strongly advocated for basing the program within community-controlled organizations primarily because they are seen as trusted and familiar spaces for Elders, facilitating a sense of safety and belonging that encourages participation. So, I think being based actually in an Aboriginal community-controlled organization is a good fit because it brings the Elders in. Well, also people feel safe … So, they feel welcome. (Research staff, non-Aboriginal, female) Yeah, because it was there, you know, like in the facility where they go and see doctors and all that stuff. Yeah, it was better, because there was a lot of our people there, you know, Aboriginal people. (Aboriginal health practitioner, female)
The trauma-informed approach taken by the program staff was highlighted in several instances. The presence of culturally aware staff allowed for a deeper understanding and sensitivity toward the Elders’ needs. The shared cultural background and experiences between the staff and the Elders created a safe space where difficult conversations could happen. That was definitely a strength for every one of them, really looking at—and what was also good, one of the team members is to spend a lot of time speaking to Elders who’ve been through some quite traumatic experiences and they did a lot of trauma-informed yarning and really helped a few Elders that hadn’t actually sought support before to get support. (Research staff, non-Aboriginal, female)
In addition to cultural safety, ACCHSs have the potential to enable intergenerational interaction for Elders, a valued eldership role in Aboriginal culture. So, I think being based actually in an Aboriginal community-controlled organization is a good fit because it brings the Elders in. But also, it’s not just to an aged care centre where there’s not much intergenerational exchange, but in a community organization, really, there’s all age groups. (Research staff, non-Aboriginal, female)
Discussion
The process evaluation, underpinned by the ToC framework (De Silva et al., 2014), explored the strengths and learnings during the program implementation phase through reflexive thematic analysis of experiences shared by participating Elders and program staff. The DAMPAA program addressed a critical gap in the community by providing a brain health initiative tailored specifically for Elders. Key components of the program—group walking and yarning—promoted a deeper connection to Country and community to enhance the quality of life and social and emotional well-being of Elders as well as for program staff. Key learnings highlighted the importance of running community-informed health programs within an ACCHS, delivered by local Aboriginal people who understand Elders’ roles and responsibilities. These program elements are crucial for Elders to feel connected and have a sense of place-based belonging. An ACCHS-based program also creates a more comprehensive health and well-being hub for community.
The DAMPAA program was implemented with a strong foundation in trauma-informed principles (Hopper et al., 2010; Substance Abuse and Mental Health Services Administration (SAMHSA), 2017), ensuring cultural safety, empowerment, and trustworthiness throughout the program, creating a supportive and healing environment for Elders, and respect for diversity. Facilitated by local AHPs supported by an ACCHS, the program not only promoted health but also established trust, a key component of trauma-informed approaches, through culturally safe interactions that were sensitive to the historical and intergenerational trauma experienced by Aboriginal communities (Atkinson, 2002; Dudgeon, Milroy, et al., 2014). Furthermore, through Elder-informed flexible delivery of physical activity, the program recognized individual autonomy and provided choices that empowered Elders. This individualized approach promoted and respected diversity and personal agency, which are critical factors in creating an empowering and safe space for Elders. Evidence suggests that trauma-informed care, which emphasizes choice and empowerment, has a positive impact on overall health and well-being, especially in populations with a history of trauma (Harris & Fallot, 2001; Leitch, 2017; Wilson et al., 2017).
Walking and yarning activities were the most cherished and uplifting experiences shared by Elders, signifying the relevance of culturally grounded practices in promoting their well-being. The walking and yarning sessions were not ancillary but formed the core components of the intervention (Lalovic et al., 2024). Elders emphasized that walking outdoors, particularly in natural settings, strengthened their connection to Country, an essential component of Aboriginal health and well-being (Fatima et al., 2023; Thorpe et al., 2023). Similarly, yarning emerged as another key element in the program, contributing significantly to the social and emotional well-being of Elders. The practice of yarning, a culturally accepted way of sharing life experiences and stories, develops trust, a sense of community, and connectedness among participants (Bessarab & Ng’Andu, 2010; Geia et al., 2013). Both Elders and program staff, who were Aboriginal, highlighted the therapeutic nature of yarning circles. Having staff with shared cultural experiences created a culturally safe environment where Elders could express emotions and share stories without judgment. This sense of safety is critical in Aboriginal healthcare, as it encourages open communication and emotional release, leading to improved mental and social well-being (Australian Institute of Health and Welfare, 2023; Garvey et al., 2021). Another important finding from the process evaluation was that the Elders’ family carer role significantly impacted their program enrolment and consistent participation. Family obligations took precedence, even over personal or external commitments, such as participating in structured programs for the health of an individual. By integrating these cultural values and obligations into the program, DAMPAA staff took a culturally sensitive and flexible approach, recognizing and respecting the Elders’ priorities. This approach encourages focusing on the strengths, resilience, and cultural values of Aboriginal people. These findings align with the Good Spirit, Good Life framework (Smith et al., 2020), a culturally centered model which emphasizes the interconnectedness of family and friends, Elder role, community, culture, and Country (and seven other factors) being fundamental to Aboriginal and Torres Strait Islander Elders’ health and well-being (Gilchrist et al., 2023, 2025). The Good Spirit, Good Life framework factors can be applied to strengthen the cultural safety and holistic approach of health and well-being programs for Elders (Gilchrist et al., 2023, 2025; Smith et al., 2020).
The COVID-19 pandemic significantly disrupted the implementation of a group program for a high-risk older population, necessitating frequent adaptations to comply with evolving safety measures and program protocols. These disruptions resulted in delays and negatively affected staff well-being. Conducting a randomized controlled trial in a community setting introduced further complexities, as the rigid structure of the trials often forces additional burdens on Elders. For instance, the concept of randomization and the delay in providing immediate feedback following completion of detailed neurocognitive assessment batteries were less favored by Elders participating in the research (Luke et al., 2023). This response is deeply rooted in a history of mistrust, as many past research efforts involving Aboriginal communities were exploitative, were conducted without regard for their well-being, and failed to provide feedback to communities. This history of disempowering research practices, where Aboriginal people were often misrepresented and excluded from research decision-making, has left lasting scars (Humphery, 2001; Smith, 1999).
The DAMPAA program actively sought to address these concerns. Regular meetings with the Elders Governance Group ensured guidance and advocacy, from the program’s development and design through to program translation. With AHPs as staff, facilitating the program, they ensured that Elders’ voices were heard and respected, while also communicating the complexities of the research setting. This culturally sensitive approach helped to build trust within the community, easing some of the historical apprehension toward research (Smith, 2021). In addition to staff being culturally sensitive and respectful to Elders, provision of adequate training through hands-on experience and reflective practices could enhance staff adaptability and self-efficacy to navigate both external disruptions, such as those caused by the pandemic, and the intrinsic challenges of conducting research in these settings (Maar et al., 2011; Stock et al., 2024).
A key recommendation that emerged from the evaluation was the importance of ACCHSs in delivering programs for Elders and facilitated by local Aboriginal people. ACCHSs provide a culturally safe and familiar setting that strengthens a sense of belonging and ownership among Elders (Clapham et al., 2024), significantly contributing to their overall comfort and well-being. These organizations act as a crucial bridge between the health system and the community, enhancing trust and participation. Although AHPs’ facilitation of the current program was well received and appreciated by Elders, a recognized shortage of AHPs posed challenges to its sustainability and reach (Australian Institute of Health and Welfare & National Indigenous Australians Agency, 2023). Elders highlighted that one strategy to address this is to engage local health workers with strong cultural ties to the community. Aboriginal health workers have an in-depth understanding of community needs and cultural sensitivities (Jeyakumar et al., 2022; Topp et al., 2018). By utilizing the skills and relationships of these local health workers, programs can be effectively delivered, addressing the shortage of AHPs and ensuring continued culturally competent care and support for Elders.
Elders emphasized that the program could be significantly enhanced by incorporating dedicated and diverse educational sessions, particularly more on brain health and support services for dementia. This finding aligns with evidence suggesting that a deeper understanding of dementia risk and protective factors, specific to Aboriginal and Torres Strait Islander peoples, could enhance whole community life course strategies to delay cognitive decline and reduce dementia risk (Nguyen et al., 2024; Smith et al., 2008). Brain health resources were co-designed with Elders and service providers and are now freely available on the Indigenous Ageing Well Research website (University of Western Australia, 2020). Integration of brain health programs within culturally safe and familiar environments, such as ACCHSs, is therefore ideal as they already have an established holistic care framework understanding the historical, social, and cultural experiences of Aboriginal people (Kendall & Barnett, 2015). Locating programs within these health centers creates a supportive structure that not only meets Elders’ health needs but also promotes cultural continuity and well-being, ultimately strengthening the program’s impact and sustainability (Bryant et al., 2021; Davy et al., 2016). For example, the DAMPAA brain health program has been embedded as a community brain health program for Elders at one urban-based ACCHS and integrated into a community heart health program to strengthen brain health and well-being outcomes for participating Elders at two other urban-based ACCHSs (Personal communication with Moortidj Koort Aboriginal Coperation & Derbarl Yerrigan Health Service, 2024).
A key strength of this study is the use of the yarning method for listening to Elders’ and staff’s experiences of the DAMPAA program. Yarning empowers participants (Elders and staff), promoting trust and mutual respect between researchers and participants (Forbes, 2020). Another major strength of this evaluation was the application of the ToC framework, which allowed systematic assessment of the assumptions, resources, and activities needed for a successful program (Breuer et al., 2016; Mateo-Arriero et al., 2023). This evaluation is one of the few studies that provide a detailed account of the practical application of the ToC framework in the context of Aboriginal health research. It is important to note that the findings of this study are specific to the participants and regions included in the research. This is a common consideration in qualitative research, where the focus is on depth of understanding rather than broad generalizability. A major limitation was the gender imbalance among participants, with the majority being female. This may have influenced the range of perspectives and experiences captured, potentially underrepresenting the views of male participants. Identifying and mitigating barriers that prevent men from participating in health research, such as work commitments or cultural perceptions, is crucial for further research and program delivery (Rae et al., 2013).
Conclusion
The process evaluation demonstrated that the DAMPAA program addressed a critical gap by offering a brain health initiative specifically tailored for Elders. Core activities, such as group walking and yarning, supported a deeper connection to Country and community, enhancing the social, emotional, and overall well-being of both Elders and staff. Key insights emphasized the importance of running community-led health programs within ACCHSs, led by local Aboriginal people who understand Elders’ cultural roles and responsibilities, trained in and practice trauma-informed care, and have a relationship with, and insider knowledge of, the community (Clapham et al., 2024). In line with this, we recommend using the Good Spirit, Good Life framework—an Elder-informed model that guided the development of DAMPAA, alongside the DAMPAA facilitator’s guide, and resources to co-design or strengthen health and well-being programs with and for older Aboriginal and Torres Strait Islander peoples. These materials are freely available on the Indigenous Ageing Well Research website (University of Western Australia, 2020). The integration of the DAMPAA program as a community health initiative by locally based ACCHSs and health services validates the significance of localized, culturally informed strategies in improving health outcomes for Elders, ultimately enhancing both the program’s impact and long-term sustainability. Elder-specific programs such as DAMPAA build ACCHSs’ capability as comprehensive health and well-being hubs for the community.
Footnotes
Acknowledgments
We greatly appreciate the support and knowledge shared throughout the study by participants, the Elders Governance Group members—Uncle Charlie Kickett, Aunty Helen Kickett, Aunty Doreen Nelson, Aunty Doris Getta, Aunty Vonita Walley, and Aunty Yvonne Winmar, Moorditj Koort Aboriginal Corporation, Derbarl Yerrigan Health Service, and Geraldton Regional Aboriginal Medical Service.
Author Contributions
Conceptualization: Kate Smith and Leon Flicker. Data collection: Athira Rohit, Lynette Yappo, Aaron Basile, Lesley Markey, and Nakita Little. Formal analysis: Athira Rohit, Lynette Yappo, and Kate Smith. Funding acquisition: Kate Smith, Leon Flicker, Dawn Bessarab, Dina LoGiudice, Kay L. Cox, Osvaldo P. Almeida, Keith D. Hill, Paula Edgill, and Deborah Woods. Writing—original draft: Athira Rohit. Writing—review and editing: Athira Rohit, Lynette Yappo, Alex Lalovic, Glennette Dowden, Lesley Markey, Nakita Little, Aaron Basile, Kay L. Cox, Carmela F. Pestell, Leon Flicker, Sandra C. Thompson, Deborah Woods, Paula Edgill, Keith D. Hill, Dawn Bessarab, Rachel Milte, Christopher Etherton-Beer, Dina LoGiudice, Ivan Lin, Carmel Kickett, Julie Ratcliffe, Osvaldo P. Almeida, Zoë Hyde, and Kate Smith.
Ethical Statement
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Health and Medical Research Council of Australia (grant ID: 1151782). This organization had no role in the design and conduct of this study; in the collection, analysis, and interpretation of data; in the preparation of the manuscript; or in the review or approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
Australian New Zealand Clinical Trials Registry trial registration number: ACTRN12619000656134.