
Abstract
A 10-year review of the 2008 Council of Australian Governments’ (COAG) Close the Gap Strategy identified the lack of involvement of Indigenous people in developing policies as a key reason health disparities persist. It also posits that disconnection from Country and culture have been crucial factors. Physical and mental health cannot be separated from spiritual health and well-being amongst Indigenous Australians. This article describes the co-development of a cultural enrichment research study with Indigenous Elders, health service leaders, and community members that places culture at the centre of care to augment traditional Western mental health management. The study has been overseen and nurtured from its inception by a governance board of Traditional Custodian Elders and an Advisory Group of Indigenous health workers. Qualitative data were collected through community ‘zoom-yarns’ between an Indigenous research assistant and 44 community members during COVID-19 lockdowns. These yarns were analysed through an innovative, constructivist, multi-perspectival discursive grounded theory method. Findings have led to an Elder-governed adjuvant cultural therapy which is currently being trialled and will be evaluated using the same multi-perspectival discursive grounded theory research methodology. One third of all Indigenous Australians now live in capital cities, so developing models to bring culture and Country into urban health facilities are becoming increasingly important. The Indigenous-led research approach outlined in this paper suggests a model for engaging Indigenous communities that mainly distrust Western research and have been failed by Western mental health care. It has the potential to shape future policy.
Introduction
Indigenous academics around the world have critically re-appraised the Western framing of their research fields, developing an alternative discourse they term ‘Indigenism’ that instead centralises Indigenous ways of knowing and being (Cunsolo Willox et al., 2013; COAG, 2008; Garroutte, 2005; Lavallée, 2009; Martin & Mirraboopa, 2003; Rigney, 1999; Saunders et al., 2010; Simonds & Christopher, 2013; Tuhiwai Smith, 1999; Walters & Simoni, 2002; West et al., 2012). The hope is that through ‘Indigenism’ policy, practice and evaluation might become more socially and culturally informed (Doyle et al., 2017; Drawson et al., 2017; Kite & Davy, 2015; O’Keefe et al., 2022; Pontes et al., 2020; Rix et al., 2019). It is already occurring to some extent (McKendrick et al., 2013), but the health field has been slower to embrace what are perceived to be non-evidence-based approaches from a Western perspective (McGaw, Vance & Uncle Herb Patten, 2022; Vance, McGaw, Winther, & Rayner, 2016). Western lifestyles, medicine, and health care on the other hand have struggled to deliver wellness equitably (Maori Health Authority, 2022; Vance et al., 2022; Vance, McGaw, O’Rorke et al., 2023; Victorian Aboriginal Community Controlled Health Organisation, 2022).
Since Cunningham and Stanley (2003) signalled the urgency of rethinking health from an Indigenous worldview two decades ago, the practice-based literature that advocates for embedding Indigenous ways of knowing, doing, and being in primary health care delivered in communities and brokered by Aboriginal health liaison officers (AHLOs) has grown (Dudgeon et al., 2014). Best practice research guidelines have been developed which emphasise the need to prioritise Indigenous epistemology, ontology, and axiology in Indigenous health research (Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS), 2020; Harfield et al., 2020; National Health and Medical Research Council (NHMRC), 2018). Western models for health continue to drive care, but there are signs of two-way communication between Western and Indigenous paradigms (Vance, McGaw, Winther, Rayner et al., 2016). Binaη Goonj: Bridging Cultures in Aboriginal Health (Eckermann et al., 2010), following Kelly and Sewell (1991), argues that communities, rather than hospitals, are best positioned to create paths for wellness as they offer people space (geographic location), base (space and place where people have economic, social, and political agency), and place (a space where identities and belonging are produced). In addition, there have been a number of local affirmative health programs, led by Aboriginal people for Aboriginal people, which privilege local cultural knowledge and practices (McGaw et al., 2021). Community health models have their obvious advantages. They offer an approach in which power paradigms are inverted and Aboriginal epistemologies and ontologies are normative.
However, the majority of Aboriginal Australians live in major urban centres where health care for serious illnesses continues to be delivered in hospitals. The study Managing Two Worlds Together (Dwyer et al., 2011) recognised that city hospitals are an essential place for delivering health care for Indigenous populations, but they are also an alienating and undesirable destination for many. Patients expressed practical, social, cultural, and spiritual concerns. They also reported perceived systemic racism. Health care professionals’ observations of the experiences of Indigenous patients and their families were similar, although they also identified concerns about compliance to clinical regimes, difficulties gaining consent for treatment, and the importance of AHLOs as advocates and cultural brokers, which they acknowledged is a broad, stressful, and burdensome role. Staff reported occasional recognition of the importance of including Indigenous ways of doing health, noting occasionally Traditional Healers have performed smoking ceremonies to cleanse rooms and move Spirits on as a way of allaying fear and anxiety. But, on the whole, cultural practices are seen as secondary to Western models of care and ignored or excluded if there were perceived conflicts (McGaw, Vance, White et al., 2022).
Like many settler-colonial nations, Australia has dislocated its First Peoples from land and culture. Unlike Canada, the United States of America, and New Zealand, which acknowledged prior sovereignty by brokering treaties with their First Peoples (which were albeit subsequently ignored), Australia was settled under the lie of ‘terra nullius’ – empty land. With the development of a Treaty in Victoria and the legislation of a Voice to parliament in South Australia, changes are underway and a framework for decolonising health care within an urban hospital setting is increasingly important. Hovey et al. (2014) argue that in Canada, health care in hospitals is increasingly ‘culturally sensitive’ but not yet ‘culturally safe’, as medicine continues to be filtered through a Western paradigm that perpetuates colonisation. In New Zealand, efforts to improve cultural safety have resisted cultural awareness education, out of concern regarding ossifying stereotypes, in favour of increasing opportunities for Maori people to lead health care programs (Ellison-Loschmann & Pearce, 2006). Indeed, recently a Māori Health Authority (2022) has been established to support self-determination. Following Kelly and Sewell (1991), such a framework must include new models for care and new ways of providing ‘space, base, and place’ for Aboriginal people within urban hospitals.
Accordingly, in this study, we aim to develop a new model of mental health care to augment traditional Western treatment in urban hospitals that places culture, community, and Country at the centre. The study unfolds in stages. First is the establishment of a Board of Elders and an Advisory Group of Indigenous hospital-based health workers. Second is the completion of community yarns with a representative group of Elders, Healers, and Senior and Junior People involved in health and well-being of the Victorian Indigenous community. The yarns were conducted by an Indigenous research assistant to tease out what culture means for each person and their community, how culture aids and/or maintains health and well-being, who best governs cultural practices in their community, and what practical issues need to be addressed for cultural practices to be put into place at the hospital. Third, we aimed to develop a culturally appropriate method of analysis. Finally, from what we have learned through the community yarns, we aimed to develop an adjuvant model – Elder-governed Cultural Therapy (CT) led by Indigenous health practitioners – to evaluate with young Indigenous participants with mental health conditions referred to an urban hospital outpatient setting.
Study Design
Establishing Indigenous Leadership Following Cultural Protocols
The study is co-led by an Indigenous child and adolescent psychiatrist, within a larger national research program led by a nationally renowned Indigenous academic physician. It is located within, and supported by, an Aboriginal Health Liaison Unit within a major paediatric hospital in an Australian capital city which provides a cultural context. That is, it has dedicated ‘space’ – offices, meeting rooms, small community lounge, kitchen, and a garden – and is also a ‘place’ of safety for Indigenous staff, young people, and their kinship networks to gather within the hospital. ‘Base’ is more difficult to broker within the hospital’s hierarchical structures and complex funding streams, but over the life of the project, the base of this unit has become more secure: there is now recurrent funding (formerly it was financed through annual grants by a philanthropic trust) and there has been a recent agreement to decorate the space with cultural art and redevelop the garden with traditional healing plants.
Following clear socio-cultural protocols, this study has been overseen by a Board of Elders and Senior People since its very beginnings. The central and core role of Elders within Aboriginal community was affirmed: Elders mediate and lead all aspects of communal life, directly and indirectly (Busijia et al., 2020). They advise and govern decisions affecting the community, enable deeper connections between people and with Country, and arbitrate differences of view and interpersonal conflict. Elders hold and keep sacred knowledge for the community and know the ‘old ways’ – cultural practices that emplace and strengthen the community, aiding health and well-being (Flicker et al., 2015; Kennedy et al., 2023). Elder governance of cultural projects is a protocol that is consistent with how Indigenous communities work, nationally and internationally.
An Advisory Group of experienced Indigenous health professionals including AHLOs, a social worker, and a psychologist was established when funding was secured to provide additional guidance on navigating Western health care systems while maintaining cultural authenticity. The project was approved by the Royal Children’s Hospital Human Ethics Committee (2019.207/56941).
The process of seeking Elders’ guidance has been long and involved. Relationships were developed over the course of a previous research project, from 2010 to 2014, led by the co-author (JMcG). A 5-year process of co-development began in 2015 with road trips around the state to meet, lunch, and yarn with Elders recognised in the community for their spirituality, culture wisdom, and concern for health (authors 1 and 2). Co-author (AV) also met with a number of Indigenous leaders of health, welfare, and justice peak bodies for advice and direction. A group of six Elders and Senior People – four women and two men – from different regions around the state of Victoria was consolidated by 2019. They guide the program leads in cultural matters as it continues to unfold. Quarterly board meetings are convened and are supplemented with ad hoc lunches and phone yarns. One has since retired, and another passed away last year. Invitations by remaining Elders have been extended to other Elders to join. The Advisory Group has welcomed a few more Indigenous health professionals while maintaining the initial group membership.
Sampling and Recruitment of Community Members
Participant Characteristics for the 44 Community Needs Assessment Yarns.
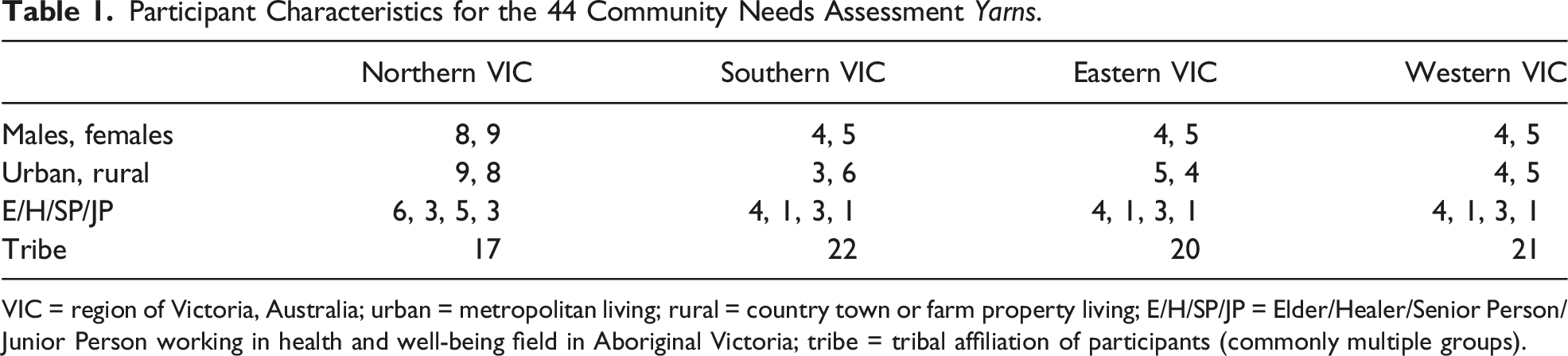
VIC = region of Victoria, Australia; urban = metropolitan living; rural = country town or farm property living; E/H/SP/JP = Elder/Healer/Senior Person/Junior Person working in health and well-being field in Aboriginal Victoria; tribe = tribal affiliation of participants (commonly multiple groups).
Yarning With Community Through COVID-19
The first stage of the project was a consultation with community to co-design the next stage of the project – the development of a CT. Mindful of the inherent Western bias implicit in most research methods, grounded theory was adopted as the overarching research methodology (Bainbridge et al., 2013). Grounded theory commences with open questions, rather than a hypothesis or theory, focuses on social actions and processes, and uses an inductive process to generate theoretical abstractions arising from the participants’ data (Glaser, 1992). The method for the community consultation was yarning.
Yarning is an Indigenous method of making sense of lived experiences with another (Geia et al., 2013). It is a specific, cultural, fluid, and dynamic process and method of knowledge exchange that is culturally safe (Kennedy et al., 2022; Shay, 2021), so sensitive issues and intimate information can emerge through two-way knowledge sharing and so all involved are enriched by the experience. The yarning narrative is circular and goes round and round until the journeying together brings both people to a moment – a point in place and time where shared meanings are conveyed. Bamblett (2013) distinguishes yarning from ‘straight line stories’ that Western settlers tell. He unpacks that Indigenous ways of knowing, doing, and being are rooted in an entirely different epistemology and ontology. Knowledge is situated within a network of human, Ancestral, geographic, and Totemic relationships that are not quantifiable, not measurable, and not individually defined but passed on by ‘mob’ (Aboriginal community defined by connection and belonging to each other and Country) through ‘Storying’. Although language was suppressed on the missions in the colonial era, and contemporary Aboriginal culture is varied as a result of colonisation, contemporary yarning discourse retains many of its traditional characteristics. Bamblett (2013) quotes Gamilaroi teacher Laurie Crawford: “us blackfellas don’t tell stories in a straight line, we go all the way around it.”
Involving a well-known Indigenous community member to lead the yarns was crucial given the known strong insider versus outsider status of Indigenous community membership (Innes, 2009; Merriam et al., 2001). Many Victorian Indigenous community members will not agree to yarn unless with a known and accepted community member. Then, reciprocal kinship connections, obligations, and responsibilities aid the yarning process and smooth the way (Dew et al., 2019). This holds both within Victoria tribal regions and across them.
Four open-ended questions framed the yarns which were circular unfolding narrative journeys:
What does culture mean for you and your mob?
What cultural practices aid and/or maintain health and well-being for you and your mob?
Who best governs cultural practices in your mob?
Any practical issues for cultural practices to be put into place at the hospital? The community yarns were originally envisaged to be group processes to Aboriginal Community Controlled Health Organisations (ACCHOs) in a number of urban and regional destinations, but because of COVID-19 movement restrictions, the team adopted the format of one-on-one ‘zoom-yarns’ between an Indigenous research assistant and a representative sample of Elders, Healers, and Senior and Junior People, involved in health and well-being across the Aboriginal nations in the Victorian Indigenous community (see Table 1). While the social disruption of COVID-19 to the community and project was the primary reason for the change, the method also had its strengths: the zoom-yarns captured a broader variety of perspectives – young and old, working in health and independent community members; they allowed even the quiet voices to be heard – in large gatherings, big personalities can dominate; they were deeply reflective – in fact it seemed they were often a source of solace amidst long durations of social isolation; they were substantial – 45–60 min or 8–10 pages of transcribed conversation on average; and they were easy to record, review by others, and transcribe.
Analysing the Community Yarns to Co-Design an Adjuvant Therapy
The Zoom-yarns were analysed using a multi-perspectival, discursive, constructivist approach to ensure the participants’ experiences drove the findings (Charmaz, 2006; Glaser, 1992). Human ‘coders’ inevitably bring a bias: social, cultural, educational, and disciplinary. To reveal the blind spots that might emerge from the intrinsic interests and disciplinary training of a single coder, a multi-perspectival, discursive approach was adopted. Four coders reviewed all the yarn footage and/or transcripts. Each had a distinct social, cultural, and disciplinary perspective: Two had Aboriginal heritage (but one was more embedded in community than the other) and two were non-Indigenous; one was a former AHLO with education to a year 11 level, one had an undergraduate degree, and two had doctorates; and those with tertiary training straddled diverse disciplines too: mental health (psychiatry), social sciences (anthropology), and the spatial disciplines (architecture and cultural geography). One of the coders was the research assistant who conducted the Zoom-yarns – a participant-researcher. The authors wanted all the emergent perspectives of the yarns to be valued and heard, believing this would best inform the subsequent stage of the project. Luhrmann’s (1986) autopoietic systems theory similarly observes that group processes like this allow for the spontaneous emergence of new ideas, a key ambition of grounded theory.
Initial coding led to focused categorical coding and the formulation of gerunds, which in turn led to theoretical coding as separate stages of the analysis (Charmaz, 2006; Glaser, 1992). Memos were written at every stage to enable the participants’ experiences to be outlined as the coders’ pre-existing ideas and assumptions were defined and questioned so the voices of the participants could be fully heard (Cooper & Burnett, 2006). This discursive reflexivity was crucial to ensure the coder remained mindful of their positionality. Once the individual coding and thematic analysis was complete, the team met, again via Zoom, over four extended sessions, where each coder took it in turns to share what they had ‘discovered’ through each yarn. Sometimes, the group was united in what they believed had emerged from the data. But, at times the dissonance between perspectives was the key finding. Mouffe (1999) coined the term ‘agonistic pluralism’ to describe a process of ‘struggling with’ difference. Consensus, she contends, simply reinforces a dominant discourse. Through multi-perspectival discourse, Western and Indigenist views were equally valued and included in the analysis of the yarns.
Findings
The key themes from the yarns provided by community members are outlined according to the key questions asked: The importance, breadth, and significance of Culture for ongoing health and well-being are explored first. Then, the central role Elders’ play maintaining health and well-being in community and in Country is outlined. The variety of cultural practices and their deep links to particular Country are noted. Finally, the importance of a physical space and an organisational and funding base so a culturally safe place can be created for cultural practices are explored.
Culture Is the Foundation of Health and Well-Being
For our community members, ‘culture’ meant many things to the cohort, but all described something central to their lives. Culture is everything; it is used to make sense of the world; it emerges in community but is also lived individually; it is formative for identity; it is grounded in Country; and it includes values, principles, actions, and behaviours. As participants said: Yeah, culture was our way of life. It was our law, our custom, our governance, our education. The dreaming stories we were taught about values, from food to our marriage system. (Participant 8) Three words – Culture is life. The ability to see people who look like you and sound like you. That’s culture as well. (Participant 23)
Elders Nurture, Facilitate, and Govern Cultural Practices
There was universal support for Elders to govern all aspects of Indigenous cultural practices: They are enabling of Indigenous cultural practices, are knowing about cultural practices that can lead to health and well-being, are emplacing of cultural practices in Country so that they lead to health and well-being, are facilitating of Indigenous cultural practices being passed down the generations, and are governing of the Aboriginal lore so Indigenous cultural practices heal community and Country and make both strong. They also play a pivotal role in ensuring that Indigenous cultural practices are right for particular Country and for particular Indigenous young people and their family/kinship networks. Community members shared: Wominjeka means “to come,” “ask to come.” As an Elder I’m setting you a challenge as you come on country. What is your purpose for coming? My purpose as an Elder for being here is to share my knowledge in the process of being healthy well and wise, particularly so our young people learn. (Participant 2) Elders like me bring people together to learn, celebrate, respect, grow and honour the sacred ground we are all part of. Elders know the lore behind this sacred Place that makes us all whole. This knowledge is part of generations since time began and makes us strong today. (Participant 33) We all need to learn respect for our Elders who govern everything and know what is right for us mob and our Country to be well and healthy. (Participant 41)
Indigenous Cultural Practices Vary and Are Emplaced in Country
There was clear support for a range of Indigenous cultural practices used for health and well-being in community. These included smoking ceremonies, art, music, dance, walking in Country, and connecting with animals. Smoking ceremonies were believed to be particularly important as a protocol of welcome for people from different tribal affiliations and as a way to cleanse the Spirit. Art, music, and dance are all ways of expressing culture. Walking in Country was affirmed to be healing as it keeps the body, mind, and Spirit connected. Animals can be a teacher and guide, especially if they are a Totem. However, there were cultural expressions particular to individuals that were not generalisable. Salt water people, for example, emphasised water ceremonies and totemic sea creatures while the fresh water river aligned tribal groups focused on river creatures. As participants said: Cultural Practices come out of our values and beliefs. Who we are, where we come from. And they are generated by what our family beliefs, our tribal beliefs are, through the generations. (Participant 4) Cultural practices are about the way we live, who we are, where we come from, connection to land, connection to people, place, connection to spirit. For me it’s very much about spirit. And that is rooted in a particular Place. (Participant 29) Cultural practices are living culturally, connected to Spirit that can come in so many different ways – music, dance, art, walking Country, connecting to animals, smoking ceremonies, water ceremonies. I get my cultural strength and connection from my relationship with spirit through cultural practices, my Elders and my family and that connection to my Ancestral country. (Participant 43)
Indigenous Cultural Practices Need the Right Space, a Practical Base, and Culture-Filled Place
The feasibility of implementing Elder-governed Indigenous cultural practices in an urban hospital outpatient setting was an important issue in the yarns, particularly during COVID times. This was also emphasised by the Indigenous Advisory Group. It was agreed they should guide and supervise but not do front-line work. There was also concern that the hospital may need professionally trained workers to do Indigenous cultural practices so seriously unwell children are managed safely. Finally, the location mattered. It was clear that the hospital organisation needs to support these practices in a culturally safe space like an Aboriginal Health Liaison Unit. Further, they needed to happen in a private place away from the public’s gaze. A private, Indigenous-owned location at the hospital offers a base that enables economic, social, and political agency for Indigenous people within the hospital and health system at large which, in turn, facilitates a co-leadership model for Indigenous and Western ways of doing health. A base enables genuine and meaningful dialogue to occur rather than arrangements that merely help Indigenous people to better comply with Western healthcare. Ongoing Elder-governed cultural awareness and safety training for all staff helps maintain genuine Aboriginal and non-Aboriginal dialogue. Finally, the space and a base allow place meaning and place attachment to evolve as community belonging and identity grow (Brearley & Hamm, 2009). As community members shared: Burn out and fatigue happen if cultural practices happen in mainstream without being hidden. A non-Aboriginal person – they work, they go home, it’s fine. An Aboriginal person works but only if it is the right space, Place feels right and not constantly interfered with. (Participant 17) An Uncle told me there is no such thing of a balance for mob, it’s a blend as we cannot counterweight White culture and work structures with our own. The reality is there is never going to be a balance, it’s more of a blend so we can survive. (Participant 30) Funding barriers, bureaucratic barriers, time barriers, no space to do our culture to live it without being poked and prodded and asked question after question like we are at the police station. (Participant 44) We need to empower communities and empower local solutions to teach and share culture with those living on their country so that they can respect and embrace it within the protocols – at the right time in the right way. We need to create spaces that share cultural practices and allow mob just to connect safely and quietly. (Participant 7)
Once the findings emerged from the yarns, a number of meetings were held involving the governing Board of Elders and the Indigenous mental health professionals at the hospital. A model of care – Elder-governed Cultural Therapy – was composed to be at the centre of each young person’s mental health care. It is delivered by Indigenous mental health practitioners (nurses, social workers, psychologists, and psychiatrists) for Indigenous young people and their parent/guardian within a Western tertiary/quaternary hospital setting. It is informed by Indigenist epistemologies and ontologies which affirm that Indigenous people’s worldviews are distinctive and vital for their existence and survival (Dudgeon et al., 2014) and ‘two-eyed seeing’ which seeks the best from both Western and Indigenous models of health (Bartlett et al., 2012). Oversight is provided by a governing board of Elders, and CT is financially supported by a national program grant. Each Indigenous young person and their guardian work with an Indigenous cultural therapist (a mental health professional) under the guidance of the Elders’ board to explore a place-based cultural practice that takes a variety of forms: art, music, dance, animal-assisted therapy, or walking in Country. CT is particular to the therapist and participants, reflecting the different perspectives, skills, roles, and priorities they have. However, the form of CT is generalisable. Reflective, narrative, and dynamic interpersonal processes and mutual co-learning built on respect are its hallmarks. In addition, CT is iterative, fostering internalisation of coping styles and interpersonal skills in Indigenous young people. A crucial element of CT is an invitation to the young person and their guardian to participate in a cultural practice that is integral to the therapist’s own life, so the practice is an authentic and congruent expression of lived epistemologies and ontologies. The cultural therapist, young person, and their guardian engage in CT together as a relational community of Indigenous people. All are expectant of revelations from Country, community, and the spirit world of how to live connected and fulsome lives. Each – therapist, young person, and guardian alike – then share what they have discerned, reflect on the revelations together, and make meaning from it for each young person and their guardian.
CT involves approximately eight hours delivered over six sessions. At the conclusion of CT, agreed themes particular for each young person are inscribed on a message stick, made from sacred sandalwood (Cherry Ballart) prepared according to cultural protocols for the Country from which it comes. This message stick is given in the last session to the young person as a physical summary of the journey they have been on and a tangible reminder of what they have learned.
Discussion
A variety of Elder-governed Indigenous cultural practices were universally affirmed, all emplaced in Country as the Indigenous theme of place particularly relevant for health: Ideally CT takes place in Country rather than within the walls of the hospital. But where Country is not accessible, interestingly, other country becomes available. The location of the hospital where the study is taking place has the good fortune of being located adjacent to a large parkland which is coincidentally (or not) an Ancestral intertribal meeting ground of Kulin nation people.
Country is the term that describes Ancestral lands. It is central for Australian Aboriginal identity – not generalisable or abstract but specific, local, and immediate. Specific landforms and waterways convey evidence of the ongoing action of Creator Spirits (Langton, 2005). The relationship between people and land is one of mutual belonging. Indigenous concepts of Country, which hold that respecting, maintaining, and caring for Country is paramount, are diametrically opposed to the Western paradigm of land as property (Cunningham & Stanley, 2003). Social responsibility to one’s kin is expressed through the rituals enacted in the sacred landscape (Langton, 2005). Colonial laws have displaced Indigenous people from Country and in turn separated people from their kin, totems, and sacred Stories. Indigenous dislocation was arguably greatest in the south eastern states of Australia, although there were no parts of the continent that were left untouched. This is perhaps why any available country is better than none.
This Indigenist approach is founded on the key principle of self-determination for Indigenous young people to achieve and maintain health and well-being (Government of Victoria, 2021). Indigenist research requires Indigenous people to conduct research according to the following principles, enunciated by Martin and Mirraboopa (2003): each people’s worldview is distinctive and vital for their existence and survival; each people’s collective social mores must be honoured as essential processes through which they live, learn, and situate themselves; each people’s contexts are acknowledged as key shapers of their interpretation of past, present, and future experiences; and each people’s voice, experience, and life and their lands are privileged. Authenticity is a primary principle. This approach has meant CT can evolve in many directions, following the different perspectives, skills, roles, and priorities of Indigenous people.
Finally, the Indigenist principles of engagement are relevant. Indigenous young people with mental health conditions and their guardians presenting at the Aboriginal Health Liaison Unit in the hospital are referred by Indigenous staff to participate in CT. If they agree, an informed consent yarning process is completed by our Aboriginal research assistant. Each Indigenous young person and their guardian then meet with the Indigenous cultural therapist (psychiatrist, psychologist, social worker, or nurse) always accompanied by the Aboriginal research assistant. The male cultural therapists see males and the female cultural therapists see females although some young people see a particular cultural therapist because of the nature of the CT offered, be it art, music, dance, animal-assisted therapy, or walking in Country. So far 15 young people have participated in the CT study that places culture at the centre of the young people’s mental health care to augment existing Western health management.
Strengths and Weaknesses
This process for developing the study has had a number of strengths for the Indigenous community (Vance, McGaw, Winther et al., 2023): the leadership by an Indigenous researcher and clinician; governance by Elders; support of an Aboriginal Advisory Group; and consultation through yarning with a representative sample of Elders, Healers, and Senior and Junior People from all regions of Victoria, Australia, who have an interest in culture and health and well-being. Meanwhile, the size of the sample and sophisticated and careful analytic strategy used to explore the themes from the yarns is recognisable to Western qualitative researchers as valid, reliable, and generalisable. The main weaknesses constraining the interpretation of these data include not yarning with community members currently receiving health and well-being care and not being able to yarn with greater numbers given COVID-related restrictions. Future community needs assessments through yarning could address these weaknesses.
Conclusion
Once the study is complete, Elder-governed Cultural Therapy that places culture at the centre of care to augment traditional Western mental health management will be evaluated. The aim is to have 30 randomly selected Indigenous young people with mental health disorders and their families looked after through the Aboriginal Health Liaison Unit where the study is underway. All will continue to receive Western mental health bio-psycho-social management while they receive CT. Pre-therapy, immediate post-therapy, and 3-month follow-up yarns are being conducted with the young person, their guardian, and their therapist. The Indigenous research assistant who accompanies the participants in every therapy session is also writing her own cultural reflections. As with the CT design phase, a multi-perspectival, discursive, constructivist, grounded theory research methodology will be used to analyse these yarns (Charmaz, 2006; Glaser, 1992). In this way, existing urban hospital-based space, place, and base paths for wellness for Indigenous young people and their families will be enhanced through forming an evidence base that supports Elder-governed Cultural Therapy being at the centre of care. This Indigenist research approach outlines a model for engaging Indigenous communities that often distrust Western research and believe Western mental health care is ineffective for their members. It has the potential to shape future culture-centred clinical health service delivery policy for Indigenous young people with mental health conditions.
Footnotes
Author Contributions
AV, JMc, DO’R, SW, and SE conceived and developed the research protocol. AV and JMc wrote the first draft with constructive revisions provided by AV, JMc, DO’R, SW, and SE. All authors contributed to composing the final manuscript and are accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Australian Government Medical Research Future Fund (MRFF) as part of the Million Minds Mental Health Research Mission (MRF1179461). The funder has no role in the study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication.
Ethical Statement
Data Availability Statement
All Indigenous data are under the control of our governing Victorian Traditional Custodian Elder’s Board. Reasonable requests made to the corresponding author will be presented to the Elder’s board and if approved, data will be made available.