
Abstract
The philosophy underpinning mental health care has undergone a shift from a biomedical, deficit model to a recovery-oriented, strengths-based approach prioritizing individual abilities, experiences, and skills. Within this context, it is paramount to understand how resilience is experienced by people living with mental distress, and the role it plays in the recovery process. This arts-based qualitative study aims to explore the meanings and experiences of resilience as part of the recovery journey of nine mental health service users from a community day center in Romania. In Romania, the mental health system and research into mental distress and recovery have been traditionally guided by a biomedical approach. This is the first study conducted from the perspective of people living with mental distress in Romania, revealing the experiential and conceptual complexities of resilience in their recovery. Thematic analysis of data generated through ten creative workshops, a focus group, and art-elicited semi-structured interviews revealed four key themes of resilience intertwined with participants’ experiences of recovery: re(dis)covering the authentic self, symbiosis with the day center, navigating conflicts (with self, society, and the psychiatric system), and leaving the past behind. The insights from participants’ verbal contributions triangulated with their artwork provided a deeper understanding of resilience within the cultural context of Romania. The findings add to an increasing body of evidence that informs the reformation of mental health practices in line with the perspectives on resilience held by people experiencing mental distress.
Keywords
Background
Mental health is increasingly understood through a biopsychosocial lens, which recognizes that biological, psychological, and social factors all contribute to mental well-being and distress. Although criticized for lacking meaningful scientific and epistemic content (Roberts, 2002), this integrated model—endorsed by the World Health Organization (WHO, 2022)—has become the foundation for modern mental health policy and practice globally. It moves beyond the limitations of the traditional biomedical model by acknowledging the importance of psychosocial determinants, lived experience, and community support in recovery from mental health challenges (WHO, 2022).
This shift is also reflected in the transition from a deficit-based paradigm focused on diagnosing and treating symptoms to a strengths-based, recovery-oriented approach (Rapp & Goscha, 2012). The deficit model, rooted in the biomedical tradition, views mental health “problems” primarily as pathologies to be “fixed,” often through pharmacological treatment and institutional care. In contrast, the strengths-based model emphasizes individuals’ capabilities, resilience, and potential for personal growth and recovery, even in the face of adversity (Bird et al., 2012).
The transition from a biomedical paradigm to a biopsychosocial, recovery-oriented approach to mental health care varies from country to country. This is a process influenced by unique cultural and socio-political contexts. In Romania and other Eastern European countries, mental health systems have been profoundly influenced by the legacy of communist regimes. Romania inherited a heavily medicalized model of care delivered predominantly in large-scale psychiatric hospitals segregated from community settings (Breemer ter Stege, 1991; Krupchanka & Winkler, 2016; Roberts, 2002). Romania’s mental health services reflect this legacy, with limited investment in psychosocial support and persistent stigma surrounding mental illness (Ciobanu et al., 2022; Sfetcu & Ungureanu, 2020).
The legacy of Nicolae Ceauşescu’s brutal regime, marked by political oppression and human rights abuses, continues to cast a long shadow over Romania’s mental health landscape. The intergenerational trauma inflicted during the communist regime, as reflected in Adler et al.’s (1993) work, has been shaping public attitudes toward mental health, reinforcing stigma and discouraging help-seeking behaviors (Manescu et al., 2023).
In Romania, stigma and stereotypical attitudes toward people with mental health diagnoses reinforce the idea that individuals facing mental health challenges are somehow “less than” others. Stigmatizing, outdated terminology, such as “handicap” or “handicapped,” stemming from a deficit perspective, continues to be used by social and health care professionals, legislators, and policymakers (Briciu & Lupea, 2018). This terminology reduces individuals to their challenges and perpetuates negative perceptions. Furthermore, it frames mental health conditions as inherent flaws rather than as responses to complex trauma and adverse life experiences. The resulting societal attitudes increase pressure on individuals with lived experience of mental distress, undermine social cohesion and collective potential, and perpetuate inequality (Popescu et al., 2017).
This aspect is critical as social connectedness is one of the pillars of current recovery-oriented models alongside hope, identity, meaning in life, and empowerment (Leamy et al., 2011). Such models focus not only on the individual but on the individual within their social context. This contrasts with the deficit models, which emphasize individual limitations and impairments rather than recognizing the broader social and systemic factors that influence recovery (Mathias et al., 2024). In contrast, recovery-oriented approaches foster social inclusion and challenge stigmatizing attitudes (Ness et al., 2021). By doing so, they encourage a shift toward viewing individuals with mental health difficulties as active participants within their communities, capable of contributing meaningfully when supported by an inclusive society.
In the Romanian mental health system, focused on deficits rather than individuals’ abilities to face and adapt to the challenges brought by living with mental distress, resilience and recovery remain under-researched phenomena. By contrast, the concept of resilience has been gaining traction within the international literature on recovery (Shanks et al., 2013). Resilience is generally recognized as a trait that describes how people living with mental distress adapt to adversity (Bark, 2023). International research has increasingly promoted the importance of resilience and individual agency as key psychosocial aspects within recovery processes since the advent of humanistic and positive psychology in the 1960s (Luthar et al., 2014). In a literature review on this subject, Echezarraga et al. (2019) outline the connection between resilience and recovery guided by internal strengths and environmental resources to achieve mental well-being. Drawing on experiential studies, Echezarraga et al. (2019) concluded that individuals who recovered from mental distress showed higher levels of resilience. Furthermore, they recommend researching resilience and recovery as interlinked constructs, pointing out the paucity of studies exploring the role of resilience in recovery, which is an important knowledge gap we aim to address in this article.
However, resilience remains a contested term regarding its meaning, processes, and outcomes. As a result, it is difficult to measure, raising questions about its scientific robustness (Windle et al., 2011). Some scholars have questioned the validity of the concept, arguing that it is fundamentally flawed (Mahdiani & Ungar, 2021). This is often due to the emphasis on individualism and self-reliance, aligned with a neo-liberal ideology leading to reduced societal responsibility, weakened social safety nets, and inadequate community support structures (Fisher & Jones, 2024). Harper and Speed (2012) also warn about the risk of placing the burden of being or becoming “resilient” solely on individuals, which neglects the broader socio-political and cultural context of shared social responsibility.
Therefore, this study adopts a more holistic definition of resilience as a “a dynamic process in which psychological, social, environmental and biological factors interact to enable an individual at any stage of life to develop, maintain, or regain their mental health despite exposure to adversity” (Wathen et al., 2012, p. 10). According to Rutten et al. (2013), resilience may include post-traumatic growth and having a purpose in life as key psychological building blocks. As a result, resilience is conceptualized here as more than simply “bouncing back” to an initial state of wellness. At the same time, we acknowledge that not all individuals—particularly those who have experienced severe or complex trauma—can access or develop resilience without substantial support (Nugent et al., 2014). For this reason, we conducted our research within the theoretical framework of recovery to capture the broader context in which resilience is manifested and understood.
Another domain that warrants attention is the role of creative abilities in developing resilience. The therapeutic benefits of creative arts in supporting recovery among people living with mental distress are well documented (Barnett & Vasiu, 2024; McCaffrey et al., 2021). The literature on the role of art therapy in resilience-building is emerging, with studies showing that art-therapy sessions can enhance resilience in individuals living with mental distress (Collins et al., 2023; Kometiani & Farmer, 2020). Structured group art activities also help develop resilience and contribute to positive mental well-being in young people (Zarobe & Bungay, 2017), people with co-existing health conditions (Gallagher et al., 2024), and across the lifespan in general (McKay et al., 2020). Although this study is not an art-therapy project per se, it capitalizes on the therapeutic potential of arts to facilitate and support resilience. This aligns the arts-based methodology we employed with our aim to investigate the meanings and experiences of resilience within the process of recovery, from the perspective of people living with mental distress in Romania.
Method
Recruitment
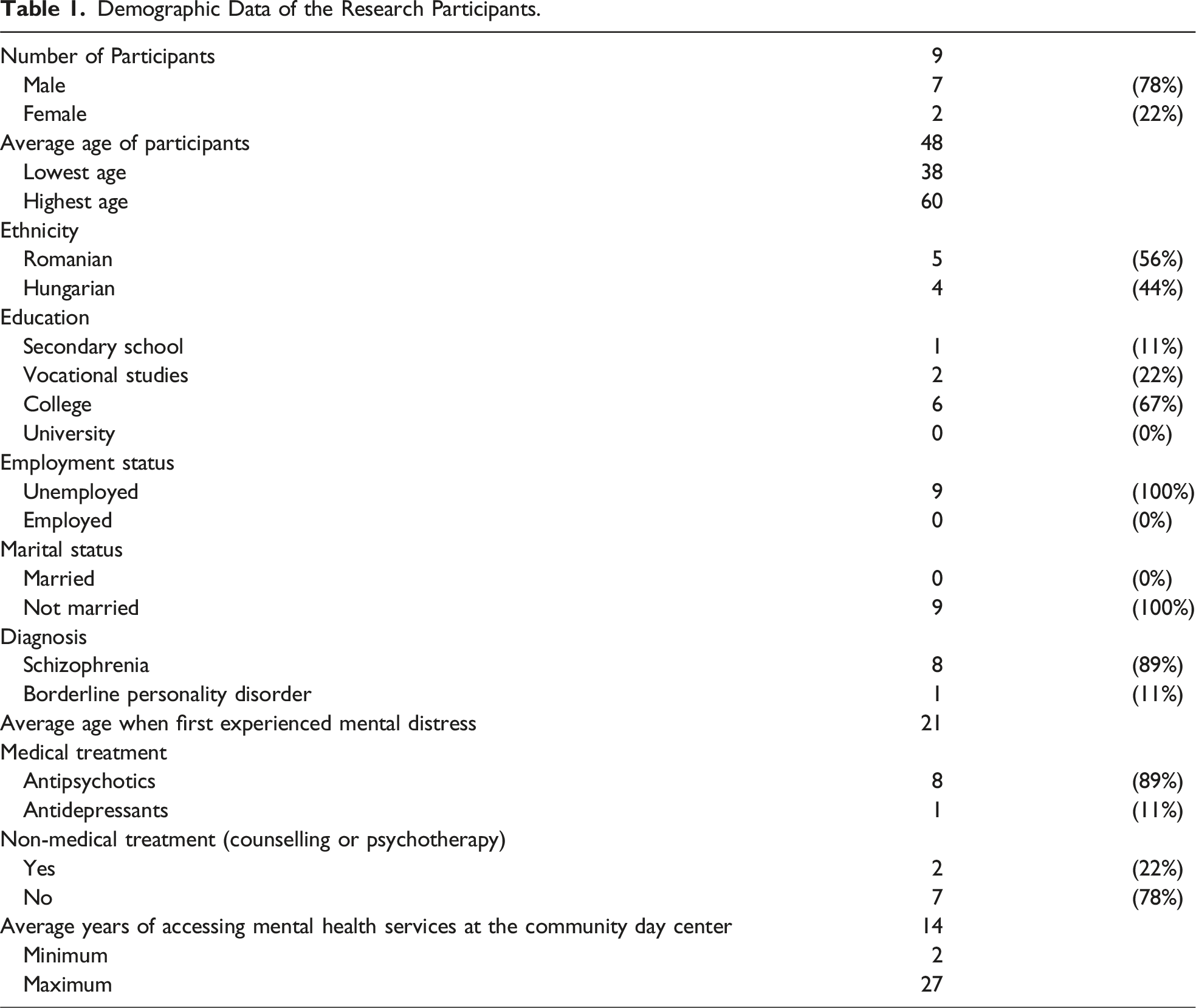
Demographic Data of the Research Participants.
Data Collection
Data collected included verbal contributions from the research participants, alongside their artwork (paintings, drawings, collages, photographs, pieces of creative writing, and clay sculptures). Data collection was structured in three stages: (1) 10 weekly creative workshops (two hours each); (2) one-to-one semi-structured art-elicited interviews (30–45 minutes); and (3) one focus group (one hour) for reflection and feedback, organized at the end of the project. This structure allowed the research participants to socially construct and negotiate meanings of resilience while sharing personal experiences of facing adversity within the creative groups. This design also allowed for capturing individual views and perspectives in one-to-one interviews, adding richness to the insights from the group activities (Lambert & Loiselle, 2008). Additionally, the researchers drew on some aspects of resilience explored freely by participants in the creative workshops, which informed the design of the interview guide. Furthermore, preliminary themes from the creative workshops and interviews were discussed in the art-elicited focus group, which we employed as a member checking activity. In this group activity, the preliminary findings were discussed, elaborated upon, and refined, while misunderstandings and misinterpretations addressed with the research participants (McKim, 2023). The research activities were audio-recorded, transcribed verbatim, and translated from Romanian into English prior to being analyzed.
Participants had a choice of one or multiple artistic media to express their views on resilience based on their lived experience. They were actively involved in planning the activities, including purchasing the tools and materials for the project. The structure of the creative workshops was flexible, comprising a group check-in, planning the artwork for the day, sharing creative ideas and motivating each other, and creating artwork focused on resilience. Finally, a space for discussing the artwork and the meanings behind it was facilitated toward the end of the activity.
A debrief space was available in case the research participants required support in processing distressing thoughts and emotions potentially triggered by the research activities. The debrief was provided by the second author, a qualified mental health professional specialized in psychosocial interventions for individuals experiencing distress. Additionally, the second author facilitated the creative workshops, while the first author conducted the interviews and the focus group. Participants were actively involved in various stages of the research beyond data collection, including the organization of a community exhibition at the end of the project. Their involvement demonstrates alignment with the fundamental principles of participatory arts-based research, such as collaboration and co-creation, empowerment and inclusion, and challenging power dynamics (Nunn, 2022). This claim is supported by the inclusive and empowering data collection methods employed during the project, which prioritized giving participants agency in shaping the research process. By involving participants meaningfully at various stages, the project adhered to the ethos of “nothing about us, without us”—a core principle of the disability rights movement (Charlton, 1998). This underscores the importance of including, and often being led by, the very people the research pertains to. This approach not only ensured the research was genuinely participatory but also highlighted the value of co-creation. Furthermore, the research fostered a sense of ownership and amplified the voices of those who are often marginalized in traditional research paradigms (Shevlin & Rose, 2022).
Data Analysis
This qualitative study subscribes to a constructivist/interpretivist philosophy positing that meanings are generated through social construction and symbolic interaction (Peck & Mummery, 2018). The interpretivist background was complemented by employing art hermeneutics to facilitate reflection, deepen understanding and experiences, and communicate them in a way that is not always possible through words alone (Bergbom & Lepp, 2022). In line with this paradigm, we adopted a reflexive thematic approach to data analysis, capitalizing on “the importance of the researchers’ subjectivity as analytic resource, and their reflexive engagement with theory, data and interpretation” (Braun & Clarke, 2021, p. 330). The analytic process was guided by Braun and Clarke’s (2006) framework: (1) Familiarization with the textual and visual data; (2) Generating initial codes; (3) Clustering codes into themes; (4) Reviewing and refining themes; (5) Interpreting the significance of themes; and (6) Reporting the findings. Attention was given to triangulating textual data with participants’ visual contributions to enhance the credibility and trustworthiness of the findings (Vanner & Kimani, 2017). The researchers decided not to use any specialized qualitative data analysis software, opting instead for a more traditional approach that included a bespoke Microsoft Excel® spreadsheet for coding and organizing data. This approach ensured data accessibility and took into account varying research and digital literacy skills within the research team. Additionally, this method allowed for a more interpretative and human-centered approach to data organization (Bright & O’Connor, 2007).
Authors’ Positionality
The authors brought diverse professional, cultural, and personal perspectives that shaped the study’s design, data collection, and interpretation. The first author, originally from Romania and based in the United Kingdom for nearly two decades, is a qualified mental health social worker, lecturer, and researcher with expertise in participatory and qualitative methods. He led the study design and conducted the interviews and focus group. The second author, a social worker and assistant lecturer in Romania, facilitated the creative workshops. She worked closely with most participants at the community center, which helped create a safe, trusting, and comfortable environment during the study. Her familiarity with participants initially prompted requests for more detailed instructions, which were intentionally limited to avoid bias and preserve the study’s exploratory nature. Both researchers reflected on their conceptualizations of resilience to reduce bias, following Buetow’s (2019) guidance on reflexivity.
During the creative workshops, the second author, bilingual in Romanian and Hungarian, created a culturally and linguistically inclusive environment, although all participants spoke Romanian. The combined expertise of the authors supported a collaborative, participatory approach and ensured accurate translation of participants’ contributions. The first author, fluent in English and Romanian, led the translation of the transcripts, with the second author reviewing them for nuance and accuracy (McKenna, 2022).
Findings
The thematic analysis was conducted on a dataset consisting of 25.5 hours of audio-recordings and 114 artworks created using different artistic media. The process resulted in the identification of four key themes of resilience linked to the recovery journey of the research participants: re (dis)covering for consistency the authentic self, symbiosis with the day center, navigating conflicts, and leaving the past behind. The themes and sub-themes are presented below, supported by verbal contributions and artworks produced by the research participants identified here through pseudonyms.
Re(dis)covering the Authentic Self
Participants’ ability to adapt in the face of adversity is intertwined with the process of re(dis)covering their authentic selves. Although the study was not designed as a narrative approach per se, the research participants explored their recovery journeys from limitations and losses caused by mental distress to developing self-awareness and understanding of their true values, beliefs, strengths, and aspirations.
Losing Oneself
We noted the initial focus of the research participants on the “downs” of their complex recovery trajectories before exploring their “ups” to illustrate strengths and strategies they developed to manage the challenges of mental distress. This aspect provided us with a preliminary understanding of participants’ perspectives on resilience as a positive construct within the process of recovery.
Laura’s narrative, for example, captures a recovery journey that echoed the art-elicited stories of other participants. Laura was an exceptionally talented student who was admitted as one of the top candidates on a competitive art course in her hometown when she was 19 years old. Shortly before the start of the academic year, Laura was diagnosed with schizophrenia, which led to her withdrawal from the course. This was the start of a long journey with distressing and traumatic experiences caused by her illness: I spent one year without leaving the house because of my fear of being filmed. I was convinced that someone brought a snake in my bathroom to make me leave the house […] I cut my hair short, I didn’t shower, I didn’t eat, I was hearing voices. (Laura)
Her experience of hospitalization was equally and, sometimes, even more traumatic: My first interaction with the psychiatric hospital was horrible and traumatic—more traumatic than the illness itself. (Laura)
Shortly after being diagnosed with schizophrenia, Laura was assessed by the local “commission” (i.e., of social welfare) and was classified as having a “severe handicap,” halting her career dreams and personal aspirations.
While keeping her diagnosis secret due to feeling “ashamed” because of the stigma attached to “being schizophrenic,” Laura started her up-and-down journey toward recovery that she symbolized through a conventional sign found in a DIY store (Figure 1). She intentionally misplaced this sign to symbolize a rather strenuous effort to cope with her distress, often in isolation and marked by significant setbacks, including a suicide attempt. My journey symbolized by these steps is extremely difficult at times. It is tiring and this slope feels endless at times. (Laura)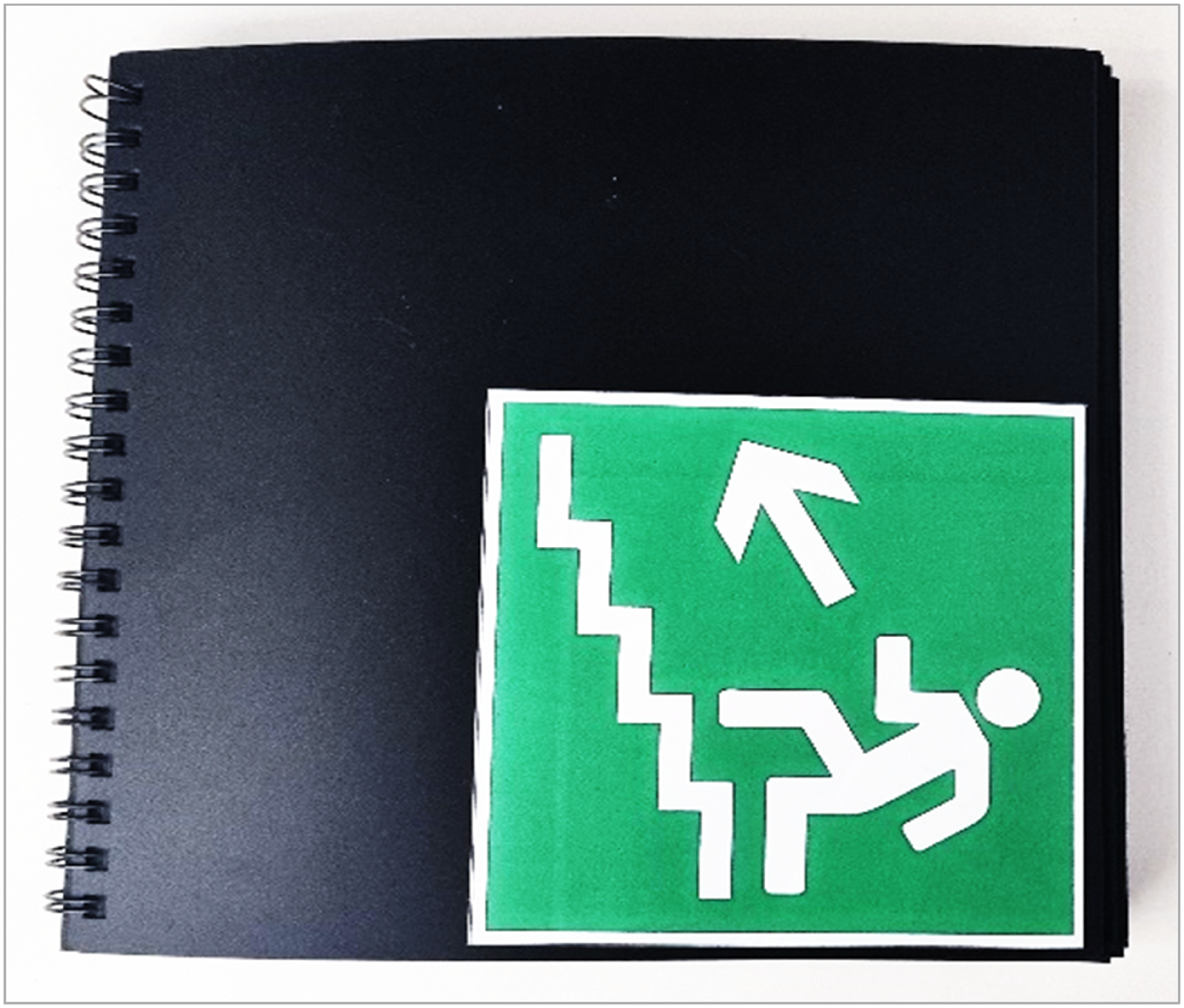
Re(dis)covering Oneself
Paul also elaborated upon the limitations of his diagnosis that resulted in occupational “incapacitation.” This was sealed by “a handicap degree,” i.e., an official evaluation conducted by local authorities in Romania that prioritizes individuals’ deficiencies, activity limitations, and restrictions to social participation: [The diagnosis] has completely changed my life because I used to work, I had my own dreams and desires like every young person. But the illness limited me enormously. (Paul)
Paul compared his resilience with tending to a bonsai tree featured in his artwork. He explained that the metaphor was inspired by the Karate Kid® film which resonated with his idea of “fighting off” the challenges brought by his mental distress: You have to adapt like bonsai trees do. Fate can cut off your branches or place you in a small container. The good thing is that you can trim the tree and arrange it the way you want. It’s all about being malleable, adaptable. (Paul)
Narratives like those of Laura or Paul exemplify the journey from a life shaped by the sudden onset of mental distress and challenges of psychiatric treatments to a process of discovering and embracing their renewed sense of self. Despite sharing some commonalities, this process is instrumentally different for each participant.
For example, Paul and Felix rely on a metaphysical interpretation of their “becoming stronger in the face of mental illness” (Felix) guided by God and the virtues and moral principles of their religion: My meaning in life is to reach eternity through my faith in God. Religion is key to my experience; it’s important to me because everything is ephemeral, life included. We’re simple tourists here on Earth. It [religion] keeps me focused on a well-defined journey. (Paul)
For others, however, resilience centers more on openness and re-connection to the external world than on inner spiritual exploration. In Csilla’s case, the predominant metaphors for reaching the true self through openness to the world were flowers, butterflies, and other fragile representations. As the groups progressed, these were gradually replaced by symbols of endurance and permanence such as trees (Figure 2) and human representations (Figure 2). I painted the tree to express the idea of inner balance and self-confidence I aim for … The woman in the painting is free, independent, powerful. She is a winner … she defeated the fear … the fear of what she carries in her soul. (Csilla)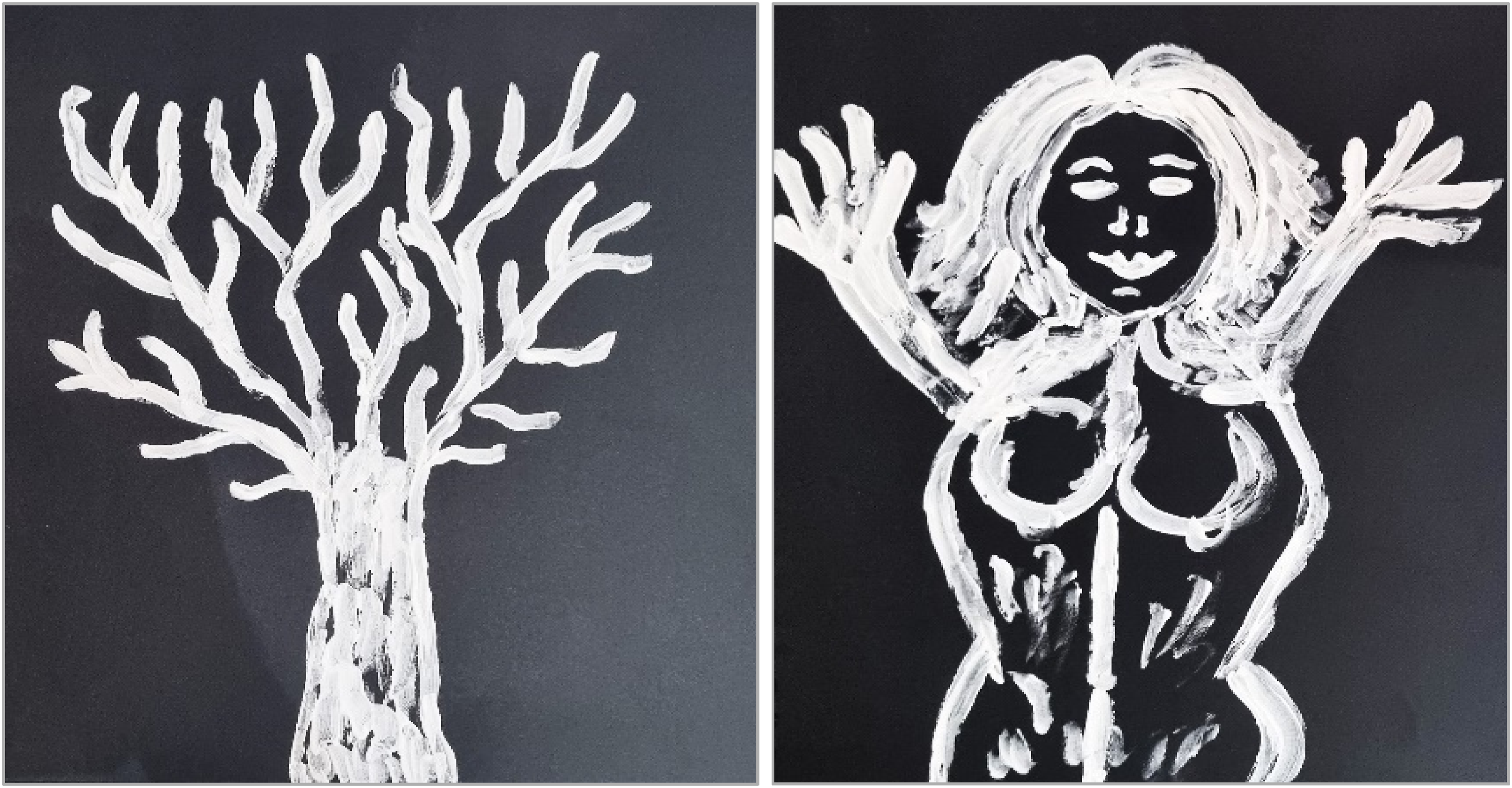
Openness is a key aspect captured in the artwork of other participants for whom art proved to be a powerful tool of self-discovery. This was the case even with those with no prior experience in creative activities, such as Attila (Figure 3). The world is beautiful and colorful, and I am trapped in my own shell. It was a time when I was afraid of people. But I managed to overcome this feeling with treatment, and I opened myself to a world from which I consciously isolated myself. (Attila)
For other participants, discovering their uniqueness was an important milestone in confronting the challenges posed by “mental illness.” This process reflected an awareness of their individuality and “specialness.” It also involved varying degrees of acceptance of their diagnosis and integrating mental distress as part of their identity: Schizophrenia is a posh illness [laughs]. It’s an illness, and it’s part of my personality. Without it, I’d probably not be able to create the way I do now. (Felix)
By developing his artistic abilities and sense of humor, Felix discovered his unique style and talent that became a key tool in his journey to recover from schizophrenia: Art is everything for me. It gives me an occupation, and this is essential for my mental health. For example, I always manage to overcome a negative state of mind when I paint. When I create, I am a different person, I forget about my troubles, my sorrows, I lose track of time. (Felix)
The research participants described their self-discovery through spiritual, artistic, psycho-educational, and other activities. Their creations vibrant with color and radiating energy and appetite for life reflect this journey despite occasional experiences of low mood, anxiety, or other forms of distress (Figure 4).
The research participants captured their experience of re(dis)covering their authentic self, altered by mental distress, through myriad textual and artistic expressions. These contributions enrich the concept of resilience by highlighting the development of self-awareness, improved self-esteem, emotional regulation, and coping strategies, reflecting both inner strength and adaptability. Re(dis)covering their own self also contributes to a clearer sense of purpose and meaning in life, as well as enhanced empowerment and agency, which further supported their ability to face the adversities associated with mental distress. The phoenix bird represents my re-birth from my own ashes. From being a vegetable, restrained to a bed, needing electroshocks to recover my mental capacities, to eventually finding a meaning in life. (Paul)
Symbiosis with the Day Center
Participants’ journeys of self-discovery and narratives of recovery and resilience did not unfold in isolation. The role of family in recovering from mental distress was rarely mentioned by the research participants. In contrast, the day center and its pivotal role in supporting their resilience were discussed at length during the creative workshops.
Participants expressed gratitude for belonging to a safe and supportive community fostered by the day center, often through their artwork. They frequently relied on water-related metaphors, potentially inspired by the name of the day center (Rom. “estuar” / Eng. “estuary”). For example, Felix illustrated his relationship with the day center in a painting depicting a boat secured to the shore by a rope resembling an umbilical cord. Felix explained that the boat symbolized resilience or “staying afloat,” “keeping my head above the water,” and being “anchored in reality,” which he attributed to his engagement with activities at the day center.
Another participant, Robert, conveyed a similar message in a painting abundant with symbols that he and his peers analyzed meticulously (Figure 5). The central piece of his artwork is a lighthouse representing the day center that guided his “turbulent” and “dark” journey through mental distress. Robert illustrated his sense of belonging to the day center by including a chair in his painting. He interpreted the chair as a symbol of the day center’s “stability” and “continuity,” which he felt supported his resilience. The lighthouse was interpreted by other participants as representing “unconditional love” which, along with “kindness” and “patience” of staff and peers, creates a welcoming oasis amidst the many “storms” faced by participants. The lighthouse is Estuar [the name of the day center] beaming tirelessly day and night. (Robert)
Visual representations of the day center as a faithful companion on participants’ journey toward recovery and key factor in building resilience are complemented by verbal explanations, equally optimistic and appreciative: The day centre helped me immensely because I found people with similar problems here, and I always felt accepted. (Paul)
The day center’s perceived healing energy seems to originate in peer support and mutual understanding: Together we can defeat the [mental] illness because we encourage and support each other. (Bogdan)
In participants’ narratives, the day center is more than a physical space. Despite frequent relocations across the city due to financial and organizational instability, it remains a vital resource in their recovery journeys. They consider it an outlet for creation, social integration, and normalization of their life through freedom of expression and empowerment: Through Estuar [the name of the day centre], I can lead a normal life. You can make choices here and [have] the freedom to decide whatever you like. I come here anxious sometimes, but I always leave with a feeling of satisfaction that I achieved something. (Attila)
Overall, the day center plays a crucial role in building resilience and facilitating participants’ recovery. It offers a supportive and nurturing environment where individuals can express themselves freely and find solace. Depicted as a lifeline by many participants, the day center provides a sense of belonging, peer support, acceptance, and understanding. Through creative expression and therapeutic approaches, it fosters emotional recovery and empowerment, enabling participants to navigate mental distress and move toward personal growth and a sense of normalcy.
Navigating Conflicts
Another dimension of resilience as a key process within recovery expressed by the research participants is concerned with navigating internal and external conflicts that add to the challenges of living with mental distress. These conflicts vary in nature depending on individuals’ experiences and are structured around three axes: conflicts with self, with the society, and the psychiatric system.
Navigating Conflicts with Self
The first theme we identified—re(dis)covering the authentic self—reflects the struggles experienced by participants in relation to their self-worth, self-esteem, and identity, following a mental health diagnosis.
While most of the participants expressed some acceptance toward their diagnosis and psychiatric treatment, tensions emerged between their “illness identity,” “diagnosed self,” and broader sense of personhood. For example, Laura described herself as an extrovert. At the same time, she was very reluctant to disclose her diagnosis due to feelings of shame and fear of being “stigmatized” and “labelled,” which caused her to withdraw and isolate herself. Living with this conflict occasionally resulted in frustration. Laura channelled this through art that became a therapeutic outlet and helped her process distressful emotions.
Laura developed awareness of the need to take more responsibility for behaviors she recognized as sometimes non-conformist, and more self-conscious about how these were perceived. This process was described by Attila as “self-censoring,” arising from his ambivalence between a “diagnosed” and “normal” self—an internal conflict that triggered existential reflections: I may seem stable on the surface, but I am tormented by thoughts inside. What is my meaning (in life)? Where should I be heading to? (Attila)
For Felix, this conflict is particularly evident in how he sees himself both as an artist and as someone living with mental distress. On numerous occasions throughout the project, Felix expressed tensions between these two dimensions of “self” he attempted to reconcile. For this reason, and also due to an overt conflict with the idea of psychiatry described in the corresponding sub-theme, Felix decided to focus solely on the aesthetic aspect of art. Consequently, he decided against using his artwork to explore his traumatic past, as he found the process re-traumatizing. As with other participants, becoming aware of such internal conflicts was the first step in attempting to resolve them. He acknowledged the importance of addressing the emotional ambivalence that was detrimental to his mental state and, subsequently, to his recovery.
Navigating the Conflict Between Self and Society
Resilience was understood by some participants as the ability to balance societal attitudes and expectations with personal values, which often conflict due to stigma surrounding psychiatric diagnoses: It took me many years to realize that I’m not schizophrenic; I have schizophrenia. It’s a huge difference. People call me “schizophrenic,” “abnormal,” “defective,” “crazy” … That’s how we end with a label. (Laura)
Some participants also contested societal norms, noting that stigma around psychiatric diagnoses worsened their mental distress and limited their personal, educational, and work opportunities: Society puts a lot of pressure on us. Do this, do that, build a career, have a family, have children … And then they make the distinction between us with mental health problems, and them—the “normal” people. (Laura)
Felix added to this art-elicited debate by highlighting a spectrum of experiences of mental distress that society fails to acknowledge, often leading to social injustice: We have mental capacity, and a conscience that other people might not have. We can reason, while other people cannot. We aren’t dangerous, but others may be. But, at the end of the day, we’re placed in the same boat, and that’s not fair. (Felix)
Attila provides additional insight into this conflict advocating for people with a mental health diagnosis who can meaningfully contribute to the moral foundation of society: Being “crazy” [Rom. “ne-bun” / Eng. “not good”] does not mean you are not “good” at anything. On the contrary, someone called “crazy” can be a model for society. (Attila)
In one of his artworks, Paul introduces the concept of a “mask” as a defense mechanism. It symbolizes how individuals navigate the conflict between self and society by concealing vulnerable thoughts and feelings.
Navigating the tensions between self and society enabled participants to develop self-awareness about their roles, values, and goals. This process involved redefining their aspirations and seeking validation from peers, who served as guides in their recovery journey. These findings indicate that adapting to the challenges posed by mental health difficulties is not purely an internal effort, but also depends on social environments, which are often more obstructive than supportive in building resilience.
Navigating Conflicts with Psychiatry
Although psychiatric care was perceived as beneficial for recovery by some participants, most of them expressed conflicting views about their interactions with the psychiatric system.
One dimension of this conflict revolves around the idea of psychiatric treatments that, in some situations, were abused by the mental health system. This had a detrimental effect on participants’ sense of self and their trust in medication and psychiatrists: I eventually accepted help [from the psychiatric hospital] but they shoved six Levo [Levomepromazin] down my throat in one day, leaving me feeling like a vegetable. (Felix)
Although he had not experienced the same level of overmedication, Rodion described his hospitalization as restrictive and lacking a person-centered approach. This contrasted with his need to participate in life-enriching activities such as arts, sports, and walks in nature, that supported his mental health, an aspect echoed by other participants: In the hospital, I was cut off from anything I’d have liked to do. You are in a hospital “uniform,” like everyone else, and the only freedom we had was to watch a football match on TV. Well, I also read a book. That was it in a month and a half. You get the treatment and that’s it. You cannot make any plans and have any hopes while you are in the hospital. (Rodion)
As a counter-narrative to the isolating, sensory-deprived experience, Rodion brings an abundance of colors into his artwork. By doing so, he reflects the idea of therapeutic spaces which he discovered during his long walks through the city’s botanical gardens (Figure 6). We live in a colorful world, and we cannot deny that. (Rodion)
These vibrant spaces contrast with the monochrome depictions of the psychiatric hospital in Felix’s artwork (Figure 7(a) and (b)), such as a portrait titled “ (a and b) I was restrained in a straitjacket, and I know how it feels. (Felix)Lady in a straightjacket” (Figure 7(a)). He intentionally crossed over the word “lady” to illustrate the degree of dehumanization of degrading psychiatric practices he experienced.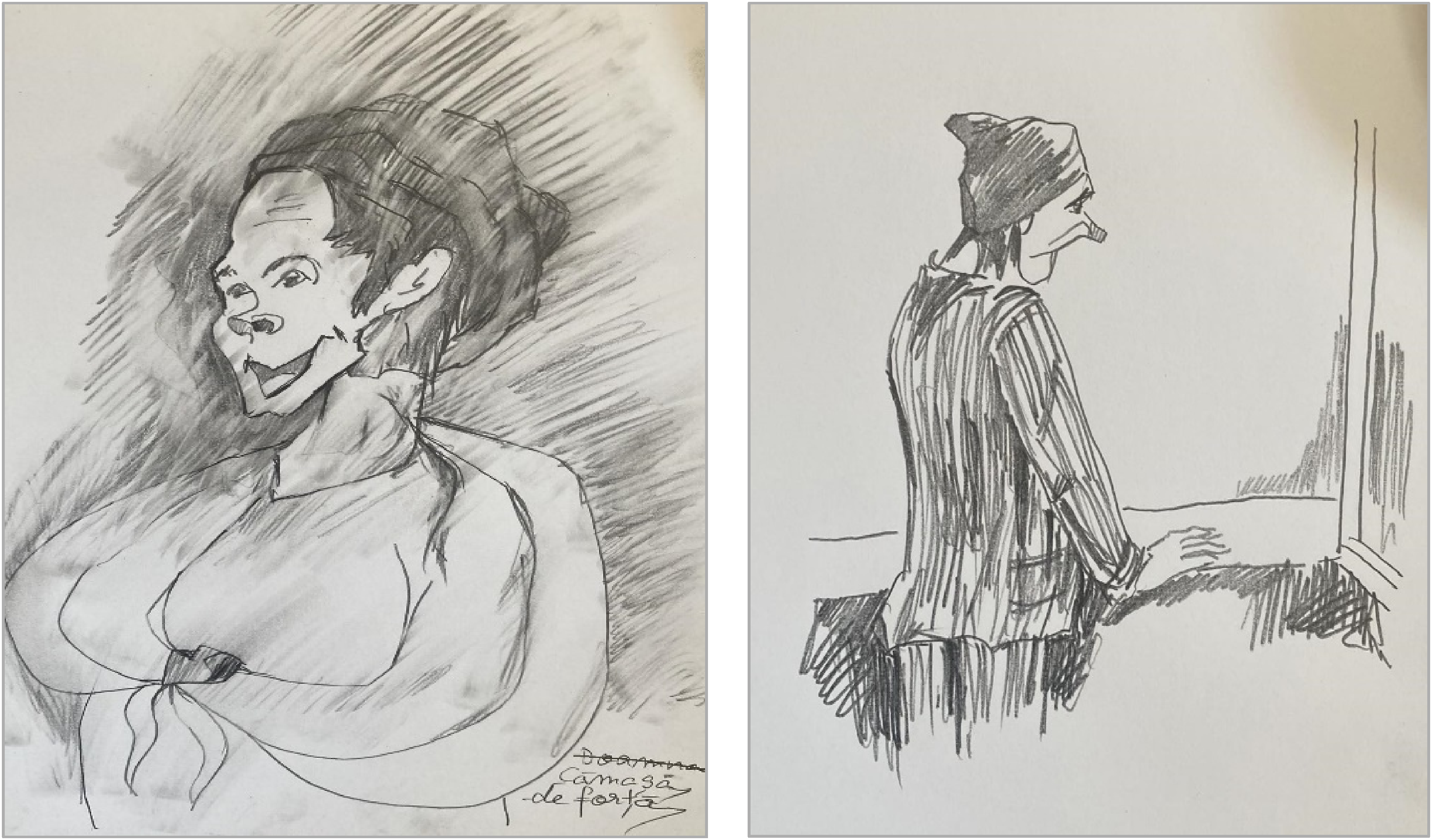
Because revisiting hospital memories and the “side-effects of psychiatry” was triggering early in the project, Felix chose to focus his creativity on the aesthetic aspects of art, rather than using it as a vehicle for exploring past experiences, as some participants did. In his characteristic humorous style, Felix concluded: – I shall focus exclusively on art. – And what about psychiatry? – I paint it all in green. – Why? – It needs ripening. (Felix)
Participants’ narratives of internal and external conflicts experienced during their recovery add another dimension to the concept of resilience understood as more than simply withstanding the direct adversities of mental distress; resilience also means facing collateral challenges stemming from the intersection of individual traits and experiences, and the societal and psychiatric contexts. Through this lens, resilience becomes more than a personal experience; it shows the socio-cultural complexities of this process that offer a more holistic understanding.
Leaving the Past Behind
Another pivotal theme of resilience was guided by participant’s ability to recover from the psychological damage of past traumas, setbacks, and distress. Although most of the participants considered moving beyond these experiences to be an essential aspect of resilience, they illustrated and interpreted this theme in different ways.
A few participants subtly hinted at past family trauma and conflictual relationships. However, most referred to their “past life” as the period of crisis that followed mental distress and the relapses experienced on their journey to recovery. For example, Laura associated her dark past with traumatic experiences of psychiatric hospitalization: Probably the worst thing about being restrained is that you need to go to the toilet and nobody helps you. It’s a horrible feeling. More horrible is when you accept to be restrained, but five people suddenly jump on you. One covers your mouth, another one grabs your throat or your hands, and you end in a straitjacket in like two seconds. Honestly, they were more violent than I was. What could I do? Shut up and endure. Not to mention the electric shocks or being beaten up by another patient … (Laura)
For Laura, leaving the past behind and demonstrating resilience is evident in her ability to avoid compulsory hospital admissions for several years and to find an effective treatment. Her experience is echoed by other participants: It [resilience] means keeping going—taking my medication and living a normal life as much as I can. (Ciprian)
Felix shared an equally traumatic experience in psychiatry in response to another participant’s artwork: When I was admitted in ’95, the doctors told me that I stood no chance of recovering. I lost 15kg while I was in the hospital. I was so bad that my parents almost bought a coffin preparing themselves for the worst-case scenario. But there were also times when I was struggling financially, and I admitted myself [to the hospital] so I can eat something. (Felix)
Other participants referred to their past crises more cryptically, using artistic metaphors such as “storms,” “dark clouds,” and “rain.” For Ciprian, one of the least vocal members of the group, the past is full of “cracks” that he has been trying to mend by doing things he enjoys in life, arts being one of them (Figure 8). That’s how this illness is. With all sorts of scars from the times when we were in crisis. (Laura) (Artwork by Ciprian).
Considering the distressing experiences disclosed by participants, their strong need to suppress memories and flashbacks is not surprising. However, some of them opined that the past remained an integral part of their learning curve to becoming “stronger in face of the adversities brought by mental illness”: My present is the sum of all the decisions I made in the past, and I try to learn from my past mistakes not to repeat them in the future. (Paul)
Similarly, inspired by a painting based on the Yin and Yang symbol, Attila seeks reconciliation with his past self through forgiveness: There are good and bad things in my past. The most important thing is to bring them together in a balanced life. Yes, you can forgive and forget some of them, but some need processing. (Attila)
In contrast, other participants whose past was dominated by feelings of shame expressed a more radical approach: My past is history. I have to erase it and carry on, not to look back ever again. (Felix)
However, they acknowledged that the process can be challenging, as traumatic memories may resurface—sometimes by choice, other times involuntarily.
The idea of moving on away from a past “that does not define me” (Laura) was verbalized by most participants with varying degrees of uncertainty and optimism. One thing their resilience narratives have in common is the importance of finding a meaning in life: I don’t know what to do, I don’t know where I’m heading, but I know I have to embark on this journey and go wherever it takes me. No one tells you which is your way in life. You must find it yourself regardless of whether it’s the right path or not. (Laura)
Rodion provides an ontological interpretation of this theme with reference to periods of hospitalization that some participants hardly remember: We are our memories. If we don’t remember being ill, then we weren’t ill [laughs]. (Rodion)
Another shared meaning with regard to moving on from a traumatic past involves a conscious focus on the present with all it has to offer. However, this may imply a subconscious repression of negative thoughts and memories: I still have some horrible flashbacks, but I try to hide them in a corner of my mind. I believe you can get through this once you bury them deep into your memory. I try to see what’s going on in the present and move on toward the future. (Attila) I’d rather look forward instead of living in the past. Being in the present helps me not to be stuck in the past, and also not to worry about what’s going to be tomorrow. I live in the present, accept it, and continue to fight. (Paul)
The strategies that help participants move on to a more positive future vary from faith and spirituality, hope, self-awareness, and “working with yourself” (Felix), either individually or in therapy. Finding “aspiration and inspiration” and acceptance that “the past cannot be changed, but we can change ourselves” were also added to the repertoire of resilience by Csilla. She sealed her conviction with a line from her favorite song: “All that I lived in the past / I will trade with forgiveness.”
Although the themes in this section were presented separately, participants explored them as interconnected. For example, the day center played a pivotal role in participants’ re(dis)covery of self. It helped them shape their identity positively and allowed them to change their perceptions of self and of a past most of them managed to leave behind. For participants, moving on with their lives often involved resolving internal and external conflicts. This also shaped their sense of self, which they became more aware of partly through involvement in activities at the day center. These links suggest that building resilience is a complex process that requires an exploration of both personal and environmental factors to fully understand the many nuances and meanings attached to this experience.
Discussion
This arts-based qualitative study provides a deeper understanding of the meanings and experiences of mental health resilience within the process of recovery, from the perspective of people living with mental distress in Romania. The knowledge generated addresses a gap in researching lived experiences of mental health in this country, approached through a biopsychosocial lens. More specifically, our interpretation of the findings was guided by Rapp and Goscha’s (2012) recovery-oriented, strengths-based theoretical framework.
The Strengths Model (Rapp & Goscha, 2012) advances five stages of recovery, all of which were reflected in participants’ narratives: (1) moratorium—a time of withdrawal marked by a sense of loss and lacking hope; (2) awareness—the realization that fulfilling a life while living with mental distress is possible; (3) preparation—identifying strengths and addressing weaknesses to support recovery; (4) rebuilding—developing a positive identity along with defining meaningful goals; and (5) growth—living a meaningful life over which the individual has control including the self-management of their condition and resilience-building (Andresen et al., 2006).
Although resilience is featured more prominently at the growth stage of this model, participants’ narratives suggest that it develops throughout all the stages of recovery, following a non-linear trajectory. This aligns with Davydov et al. (2010) who view resilience as a sustainable process that protects against or prevents factors negatively affecting mental well-being. They also describe resilience as a process of recovery from mental distress caused by exposure to adversity and trauma. This latter perspective was especially relevant in our study, given the prolonged and severe mental distress experienced by participants.
Adopting a strengths-based framework is essential given the historical emphasis in mental health research on psychopathology, risk factors, and vulnerability. These approaches align with a deficit model that is increasingly being challenged worldwide, though with varying degrees of success (Mathias et al., 2024). Similarly, the Romanian mental health system remains largely biomedical in its orientation, with limited community-based psychosocial resources available to support people living with mental distress in this country (Ciobanu et al., 2022).
The four themes identified—re(dis)covering the authentic self, symbiosis with the day center, navigating conflicts, and leaving the past behind—highlight the complexity of resilience at both personal and societal levels. These complexities prompted us to question the validity of standardized psychometric resilience scales in mental health research. Such tools often focus on individual traits instead of contextualizing individual experiences of resilience socially and culturally, as suggested by Mesman et al. (2021). Furthermore, Wagnild (2009) warns about the lack of cultural sensitivity in studies using the Resilience Scale (Wagnild & Young, 1993), advocating instead for a more intersectional approach.
Our study addresses this gap by painting a nuanced picture of resilience within the recovery process as understood and experienced by a group of nine people living with mental distress in Romania. We created opportunities for the research participants to tell their own stories of resilience and recovery through art. In Myers and Ziv’s (2016) terms, we facilitated a safe space for participants to regain their autobiographic power often undermined by the dominant discourse of psychiatry.
Our findings allow for comparisons with resilience studies conducted in other cultural contexts, although only a few explore resilience within the broader framework of recovery. For instance, a phenomenological study into the mental health of Syrian refugees (Alachkar, 2023) identified intra- and inter-personal factors, religion, faith, and belief systems as key to resilience-building. Similarly, a multicultural quantitative study of trauma survivors by Raghavan and Sandanapitchai (2019) found that higher resilience scores among Asian populations were correlated with greater use of spirituality as a coping strategy. Although such studies may follow different methodological avenues, they provide similar conclusions to our study. Together, these findings underscore the importance of developing culturally sensitive interventions and adopting a strengths-based recovery approach to support and promote mental health resilience.
In our study, participants associated resilience with maintaining, recovering, or rediscovering their authentic self—a process that often involved confronting and navigating the challenges of an illness identity. This resonates with Identity Resilience Theory developed by Breakwell (2021) from his earlier Identity Process Theory (2015), positing that “a person’s identity configuration is capable of absorbing change while retaining its subjective meaning and value for that person” (p. 574). Undoubtedly, the experience of mental distress with all its detrimental effects on individuals’ personal, social, educational, and occupational domains constitutes a major life disruption, adding further trauma for participants. Many described themselves as “trapped” and “lost” in their struggle to return to the pre-diagnosis version of their lives, a comparison often accompanied by feelings of hopelessness and frustration. A key realization for many was that resilience is more than simply “bouncing back”—an expression criticized by Harrison (2013) for downplaying the more nuanced or “hidden” dimensions of resilience. Such “hidden” aspects, uncovered by our study, suggest that resilience, as with the recovery process with which it is intertwined, is a complex, multifaceted experience. It encompasses not only personal identity but also socio-cultural factors, both within and beyond the day center.
Unsurprisingly, the community mental health day center accessed by the research participants was identified as an important space for identity, recovery, and resilience-building. This underscores the synergistic relationship between the day center, participants, and resilience. Participants’ demographic data revealed that some of them had been accessing services at the day center for over two decades. This raises the question of whether such facilities may inadvertently contribute to re- or trans-institutionalization, i.e., the shifting of mental health service users from one institutional setting such as a psychiatric hospital to another (Priebe et al., 2005). Regardless, the day center remains one of the few therapeutical options available in the local community that is accessible to participants free of charge. This illustrates the limited availability of community-based mental health support in Romania. The contrast between belonging to a safe environment and facing social withdrawal and stigma outside the day center highlights the significance of the day center. This supportive space plays a crucial role in building resilience and facilitating collective recovery through peer support. Robinson et al.’s (2015) study of mental health resilience in men further supports this aspect demonstrating that trusting, informal, and safe social connections, skill-sharing, and peer-to-peer support can significantly enhance resilience.
Similarly, arts-based activities have been widely evidenced in the literature as facilitating recovery through the sharing of creative skills and promoting social connections and inclusion (Goodman-Casanova et al., 2024; Hearst et al., 2023; Macpherson et al., 2016). These findings align with participants’ views of resilience as a process of positive adaptation that extends beyond the personal level and incorporates broader social and cultural contexts. The ecological dimension of resilience has been emphasized by Panter-Brick (2015) and Southwick et al. (2014), who placed it within a genetic, developmental, demographic, cultural, socio-political, and economic ecosystem. This multi-dimensional nature of resilience reflects the complex situatedness and understanding of recovery as a broad, non-linear process that encompasses individual growth, community support, and societal change.
The third theme—navigating conflicts—helps explain why participants view the day center as both a milestone and a vital resource for resilience-building. The center is not only perceived as a haven but also as a source of psychotherapeutic support for processing internal and external conflicts. In some situations, such conflicts are difficult for participants to verbalize, leading them to rely on artistic expression to convey their experiences. Art therapy is widely recognized as a tool for resolving internal conflicts (Goldblatt et al., 2011). However, in this study, the artistic expression was employed primarily as an elicitation method rather than as intentional therapy. Nonetheless, the potential of the arts to alleviate dissonant feelings and thoughts detrimental to individuals’ mental well-being was evidenced in some of the participants’ accounts.
Furthermore, our study adds to the evidence showing the potential of arts to explore conflicts in mental health distress. The nuanced nature of conflicts, such as with self, society, and psychiatry, provides a blueprint for exploring experiences of resilience more holistically. For instance, Crowe et al. (2016) discuss the bidirectional relationship between stigma and resilience, noting that resilience can reduce stigma, while stigma can, in turn, diminish resilience. They also found that help-seeking behavior contributes to increased resilience and reduced stigma. As a result, some researchers have argued the value of anti-stigma interventions in supporting resilience-building (Rometsch et al., 2024).
The conflict emerging between participants’ expectations of person-centered mental health care and their predominantly negative and standardized experiences of psychiatry was notable. Similar concerns are documented in other cultural contexts. For example, Egbe et al. (2014) examined the pervasive issue of psychiatric care, stigma, and discrimination, and their far-reaching consequences including social isolation and marginalization in South Africa. Romania’s mental health system has retained certain elements from the communist era, including outdated facilities and entrenched institutional mentalities. These are reflected in large, understaffed psychiatric hospitals that lack adequate specialization to address the psychosocial dimensions of mental distress. Additionally, the biomedical model, deeply ingrained during the communist period, continues to influence attitudes and practices within the system (Mareci & Tudoricu, 2023; Tataru, 2005). Many participants suggested that psychiatric care is not only inadequate in supporting their sense of “personhood,” but it also hindered their recovery. They recounted additional traumatic experiences such as hospitalization and severe side-effects caused by pharmacological treatments. As a result, some participants considered addressing the “side-effects of psychiatry” as a crucial component of resilience-building. However, a minority held a more favorable view of psychiatric care based on positive experiences with their psychiatrists.
The voices of the research participants challenged a reductionist, labelling, and dehumanizing approach to mental health care often associated with the biomedical model (Deacon, 2013). These findings add to the wider criticism of psychiatry and its underlying philosophy of care documented in the literature (Banner & Thornton, 2007; Stromback, 2021). For example, the persisting reliance on a biomedical model echoes broader critiques of psychiatry’s tendency to pathologize distress while neglecting its social and relational underpinnings, a view central to Lucy Johnstone’s (2021) work. Russo (2023) further critiques the coercive power of diagnosis often resulting in restrictive practices that reinforce the issues of oppression and epistemic injustice in psychiatry. This aspect is evidenced in some participants’ narratives and is increasingly echoed in the literature authored by individuals with lived experience of mental distress (Sharma, 2023; Valliappan, 2015).
Because of the traumatic nature of the events preceding or following their psychiatric diagnoses, most participants expressed the need to suppress their trauma to which they referred to as “past life,” as illustrated by the fourth theme of this study—leaving the past behind. This coping mechanism can be better understood by examining the relationship between psychological trauma and memory control. Hulbert and Anderson (2018) found that individuals with a history of trauma exhibited more suppression-induced behaviors than those who reported experiencing little to no trauma. However, debate remains as to whether this suppression helps or hinders resilience-building (Mary et al., 2020), especially considering recent research on “subjective forgetting” and the repression of traumatic events (Wu et al., 2024). It is also important to acknowledge the trauma endured by some participants resulting from inadequate psychiatric care heavily reliant on medication and restrictive practices (Butterworth et al., 2022). Such narratives reveal trauma-inflicting rather than trauma-informed approaches—an ongoing concern despite improvements in psychiatric hospitals compared to mental health institutions from the past (Cusack et al., 2003).
Through an in-depth exploration of individual experiences and meanings of resilience within participants’ journeys of recovery, this study provides insights that may inform future research in other settings and cultural contexts. In addition to its conceptual contributions, the study introduces an innovative and replicable methodological approach for resilience research. We capitalized on the methodological strengths of arts-based participatory research that allowed the collection of rich textual and visual data, and enhanced the communication of meanings and experiences difficult to verbalize. Moreover, the methodology provided participants with an engaging, creative, and empowering research environment (Chilton & Leavy, 2020; Greenwood, 2019). Finally, the study advocates for the development of community arts-based facilities, which could play a key role in supporting resilience among people living with mental distress.
Limitations
The issue of generalizability continues to be highlighted as a limitation in qualitative research, although continues to be debated in the literature. Carminati (2018) argues that the quantitative concept of generalizability is not entirely appropriate for qualitative research, which prioritizes in-depth understanding and contextual richness over universal applicability. Nonetheless, we acknowledge that conducting this study in an urban community mental health service in Romania may limit the transferability of the findings to other settings such as inpatient facilities or different cultural contexts. Additionally, the sample consisted predominantly of men in their 40s–50s (seven men and two women), which likely introduced some bias, given that perspectives on resilience and recovery can vary according to gender (Sardella et al., 2022). Recovery studies reveal that women tend to be focused on meaning-making in their recovery process, whereas men emphasize symptom control and reinforcing traditional roles such as occupation and independence (Schön, 2010).
Despite initial concerns about the gender imbalance, we were intrigued by a higher response rate from men than women to our invitation to participate in the research. We speculate that a study involving arts-based research methods may have appealed more to men, given the well-documented difficulties in verbally expressing emotions (Chaplin, 2015). Conversely, women are more likely to engage in alternative psychosocial activities relying on verbal communication (Liddon et al., 2017), many of which were available at the day center. Romania’s cultural and historical context of political oppression and a social environment marked by stigma may have created additional challenges to articulating subjective experiences of mental distress. The dominance of a biomedical, deficit-oriented discourse within Romania’s mental health system may also have limited opportunities for participants to express and explore these experiences. Another potential source of bias stems from the creative nature of the research activities that might have been more appealing to participants who regularly attended art workshops at the day center. To minimize this bias, we also included research participants new to artistic expression.
Finally, we encountered linguistic challenges with the term “resilience” (Rom. “reziliență”). Although increasingly used in Romanian psychology and mental health fields, it remains a neologism seldom employed in everyday conversation. To address this, we explained resilience to participants as “the ability to face and overcome the challenges brought by living with mental health problems.” This explanation might have influenced the way resilience was conceptualized by the research participants despite our use of a broad range of open-ended questions and accessible terms, such as “strengths,” to elicit their interpretations. Participants appeared to relate more effectively with the term “recovery,” which allowed them to elaborate freely on their ongoing personal journeys and experiences of mental distress. Employing art metaphors and a qualitative approach helped bridge this linguistic gap through language construction and negotiation. The use of art metaphors allowed participants to express complex emotions and thoughts in a more accessible and relatable manner, addressing potential limitations of conventional language. However, some participants’ voices may not have been fully captured due to limited verbal contributions. This prompted us to reflect on the methodological limitations of relying solely on artistic approaches without integrating textual data for triangulation.
Conclusion
This arts-based participatory study is the first to explore meanings and experiences of resilience within the recovery process, as perceived by Romanian individuals living with mental distress. It draws upon the theoretical shift in mental health care from a deficit model to a strengths-based recovery approach, highlighting individuals’ abilities to navigate and manage the challenges associated with mental distress. The findings underscore the complexity of resilience, challenging traditional definitions that frame it solely as an individual’s ability to return to a prior state of mental health. In addition to internal and person-centered components, the study highlights the critical role of external factors and resources to support resilience-building and recovery. These insights suggest that resilience should not be viewed as a purely individual trait but as a dynamic process that must be nurtured collectively by society and stakeholders within the mental health system, with close attention to the lived experiences and perspectives of those directly affected.
Footnotes
Acknowledgments
We would like to thank the nine research participants from Estuar Foundation (Cluj-Napoca, Romania) without whom this research project would not have been possible. We extend our thanks to Ms. Isabel Turnbull, expert by experience who contributed to shaping and enhancing the research project in line with the lived experience perspective. We are grateful for the support with the project space received from Babeş-Bolyai University in Cluj-Napoca to whom we extend our thanks. Finally, we would like to thank Centrului de Cultură Urbană/Centrul pentru Tineret (Centre for Urban Culture/Youth Centre) in Cluj-Napoca for hosting the community art exhibition at the end of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through the Quality Research and International Partnership schemes at Nottingham Trent University with support from the Centre for Public and Psychosocial Health to which the first author is affiliated.