
Abstract
The population of transgender and gender diverse (TGD) older adults in the United States may face inequities in the healthcare system due to factors at multiple levels. Research is needed to identify factors that limit and facilitate equitable healthcare delivery for this population. Therefore, researchers conducted a qualitative descriptive study called Shaping Affirming Futures with Elders of all gender experiences (SAFEage) to identify and explore factors that affect health equity for TGD older adults living in the United States. Through purposeful and snowball sampling, researchers enrolled 20 TGD older adults of diverse gender identities and racial and ethnic backgrounds. In Phase 1 of the study, participants discussed their healthcare experiences during semi-structured interviews. In Phase 2, participants reviewed study findings in individual and group sessions. Researchers coded transcripts of interviews and review sessions both deductively and inductively, conducting a thematic analysis informed by the conceptual framework Intersectionality Research for Transgender Health Justice. With participant input, researchers developed six primary themes describing factors that limit (L) and facilitate (F) health equity at (1) structural, (2) systemic, and (3) social levels of influence: (L1) Oppression driving adverse healthcare experiences; (L2) Gaps in healthcare resources and support; (L3) Disadvantages yielding poor health outcomes; (F1) Health justice promoting affirming healthcare experiences; (F2) Catalysts for change in healthcare; and (F3) Assets fostering agency and well-being. Study findings may inform future research, clinical practice changes, and policies that would promote equitable and inclusive healthcare for TGD older adults.
An estimated 1.3 million adults in the United States (U.S.) identify as transgender. Transgender is a term used to describe a person whose gender identity differs from their sex assigned at birth (PFLAG, 2023). Gender diverse is an associated term used to describe gender identities that differ from societal gender norms and are not necessarily aligned with biological sex (Thorne et al., 2019). For the purposes of this study, transgender and gender diverse (TGD) is used as an inclusive term to represent multiple gender identities (Coleman et al., 2022).
More than 170,000 transgender adults in the U.S. are 65 years old and older, and this number likely underestimates the actual population of TGD older adults in the U.S. (Herman et al., 2022). Using the age threshold for Social Security and Medicare eligibility, current estimates only account for the subset of TGD older adults aged 65 years and older. However, age-related health decline may occur as early as 50 years old for some TGD older adults who have experienced stigma, minority stress, and health disparities over the life course (Cortes et al., 2019; Fredriksen-Goldsen et al., 2019; Hughes et al., 2022a).
TGD adults of all ages may encounter limiting factors, such as discrimination, refusal of care, and lack of clinician knowledge about transgender health, that reduce their access to high quality healthcare (James et al., 2024). In the latest report of the U.S. Transgender Survey which collected data from over 92,000 TGD persons aged 16 years and older, nearly 50% of respondents interfacing with the healthcare system reported negative experiences, and nearly 25% delayed seeking medical care due to fear of mistreatment (James et al., 2024). In addition, TGD adults may have limited access to healthcare due to underinsurance or denial of insurance coverage (Bakko & Kattari, 2021; James et al., 2024). These limiting factors may contribute to the elevated risk of morbidity and mortality observed among TGD adults in the U.S., and they may have deleterious consequences for TGD adults as their healthcare needs increase with age, especially for those with disabilities, chronic health conditions, and serious illnesses (Hughes et al., 2021, 2022a, 2022b; Rosa et al., 2023; Smith-Johnson, 2022).
By contrast, facilitating factors, such as anti-discrimination policies and inclusive medical practices, may support health and well-being and promote health equity for TGD adults (Du Bois et al., 2018; Restar et al., 2021). Health equity results from the reduction and eventual elimination of health disparities adversely affecting groups that have been excluded from or marginalized within health systems and society (Braveman et al., 2017). One facilitating factor affecting health equity for TGD adults is gender affirmation, “an interpersonal, interactive process whereby a person receives…recognition and support for their gender identity and expression” (Sevelius, 2013, p. 2). The term doubly refers to medical and legal interventions as well as social acceptance and respect (Dorsen et al., 2022). Gender affirmation is associated with favorable health and wellness outcomes for TGD adults, including resilience, mental well-being, and risk reduction (Crosby et al., 2016; Hughto et al., 2020; Lelutiu-Weinberger et al., 2020; Sevelius, 2013). However, less is known about facilitating factors that may promote health equity for TGD older adults.
Because healthcare for TGD older adults is an emerging area of study, further research is needed to augment the evidence base on limiting and facilitating factors affecting health equity for this population (Fredriksen-Goldsen et al., 2014; Pharr, 2021). Recent research has documented health disparities, such as discrimination in healthcare settings and lack of access to primary and preventative care, which are linked to poor health outcomes among TGD older adults (Cicero, 2020; Pharr, 2021). However, the impact of both limiting and facilitating factors on health equity for TGD older adults warrants further exploration (Catlett et al., 2023; Fredriksen-Goldsen et al., 2014). Additionally, studies are needed that integrate an intersectional lens to explore factors that influence health disparities among TGD older adults of diverse gender identities and racial and ethnic backgrounds (Catlett, 2024; Catlett et al., 2023). Finally, further research on factors that limit and facilitate health equity for TGD older adults is needed to inform the development of interventions that would mitigate these health disparities.
To address the need for research on healthcare for TGD older adults, researchers conducted a qualitative descriptive study called Shaping Affirming Futures with Elders of all gender experiences (SAFEage). Researchers in this study sought to answer the following question: What are the factors that affect health equity for TGD older adults in the U.S.? Thus, the purpose of this study was to identify and explore limiting and facilitating factors that affect health equity for TGD adults aged 50 years and older living in the U.S.
Methods
In this study, researchers used a qualitative descriptive approach, staying close to the data to foreground participant voices (Neergaard et al., 2009; Sandelowski, 2000). This approach was grounded in the transformative paradigm, an epistemological lens focused on issues of “power, social justice, and cultural complexity” (Mertens, 2007, p. 213). Accordingly, study design and analysis were informed by a conceptual framework called Intersectionality Research for Transgender Health Justice, or IRTHJ (Wesp et al., 2019). The IRTHJ framework articulates social justice–oriented actions for researchers working toward health equity for transgender adults (Wesp et al., 2019). IRTHJ actions include centering embodied knowledge, disrupting the status quo, and naming intersecting power relations (Wesp et al., 2019, p. 291). In the process of generating data, researchers centered embodied knowledge by maintaining the primacy and integrity of participant contributions. Additionally, reflexivity allowed researchers to name and mitigate power imbalances common in researcher–participant dynamics. Researchers aimed to disrupt the status quo by prioritizing enrollment of older adults from groups historically underrepresented in health research.
The IRTHJ framework models intersectional causes of health inequities in three layers—structures of domination, institutional systems, and socio-structural processes (Wesp et al., 2019, p. 291). Structures of domination are forms of structural oppression like transphobia, ableism, and ageism, while institutional systems generate anti-transgender policies and regulations. Socio-structural processes refer to social practices or conditions that produce or reinforce health inequities for TGD adults. The three layers of this model informed the conceptualization of themes during data analysis in this study.
Study Ethics
The University of Virginia Institutional Review Board for the Social and Behavioral Sciences approved this study (UVA IRB-SBS#6104). Prior to joining the study, all participants provided informed consent, which was obtained in writing via electronic survey by the principal investigator. Participants also received information and resources related to topics covered during the interviews. After each interview, participants received compensation in recognition of their time and contributions to the study.
Study Design
Researchers addressed study aims in two phases. In Phase 1, the principal investigator conducted interviews to explore factors affecting health equity for TGD older adults. In Phase 2, researchers conducted individual and group sessions to review and expand on Phase 1 findings. The purpose of Phase 1 was to perform a preliminary exploration of individual participant perspectives on healthcare for trans older adults in the U.S., while the purpose of Phase 2 was to engage participants in reviewing and refining the collective representation of Phase 1 findings. Figure 1 details the study design and timeline. Study design and timeline.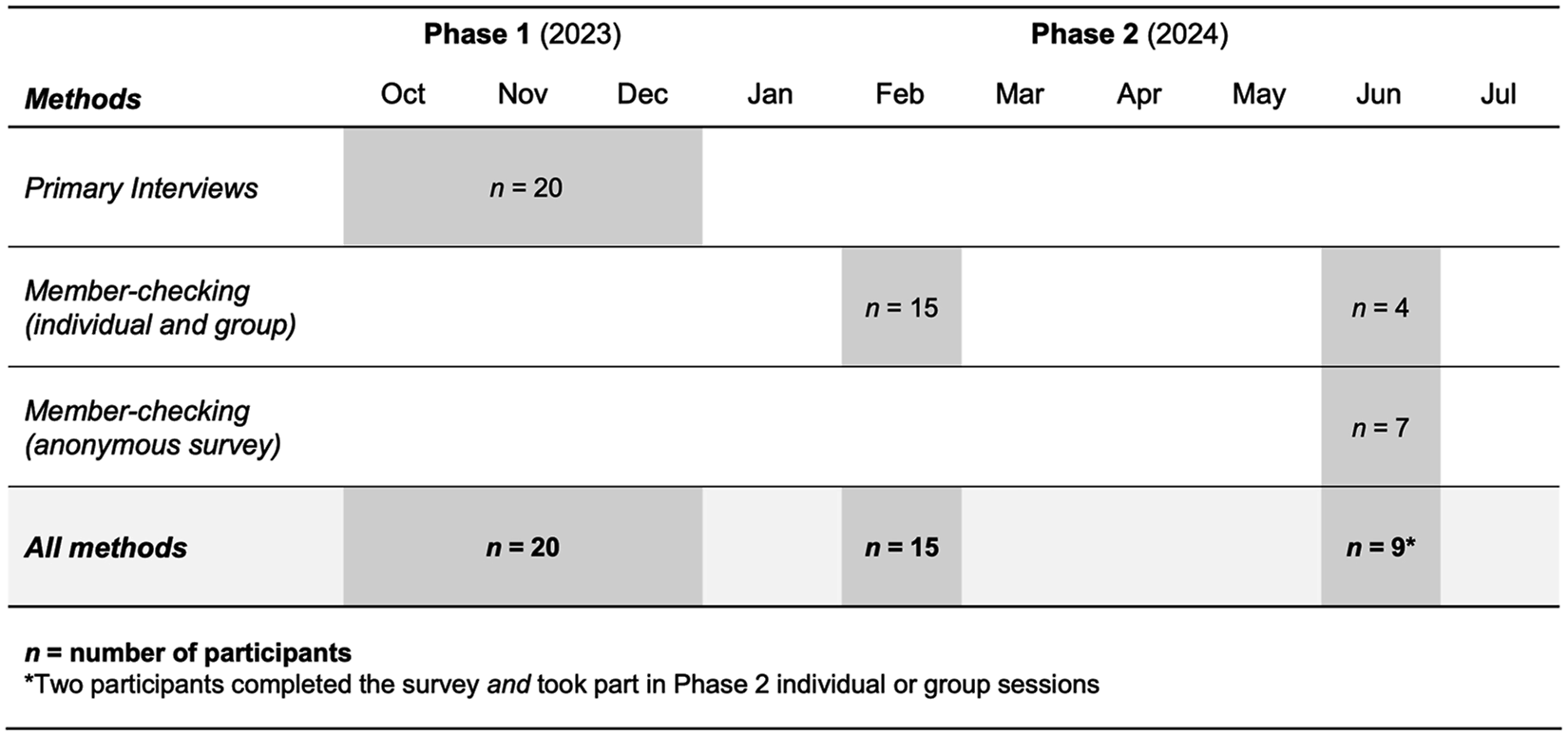
In Phase 1, participants completed an electronic demographic survey and engaged in semi-structured interviews between October and December of 2023. All interviews were audio- and video-recorded with consent from participants, and field notes were recorded after each interview. Interviews lasted between 45 and 90 minutes (65 minutes on average) and were conducted in person, by video call, and by phone to accommodate participants from across the U.S. The principal investigator used a semi-structured interview guide (Supplement 1), which contained open-ended questions about participant experiences seeking healthcare and preparing for future care. Interview questions were informed by multiple scholarly sources as well as the knowledge and lived experiences of researchers and a group of three TGD community advisors who provided guidance during the study (Catlett, 2024; Catlett et al., 2023; Reich et al., 2022).
In Phase 2, participants from Phase 1 who had elected to continue with the study reviewed study findings during individual and group sessions conducted three months and six months after Phase 1 interviews ended. At 3 months, participants discussed preliminary study findings during four group sessions (75–105 minutes each) and four individual sessions (30–65 minutes each) facilitated by the principal investigator. At 6 months, participants provided feedback on the fit between study themes and their own experiences during one group session and two individual sessions (30–60 minutes each) and through an anonymous online survey.
Participant Group Formation
In Phase 1, researchers engaged in purposeful and snowball sampling to form a participant group of TGD adults aged 50 years or older (Onwuegbuzie & Collins, 2007). The principal investigator reached out to prospective participants for Phase 1 via electronic fliers sent to researcher and community advisor contacts, community gatekeepers, and LGBTQ+ organizations for distribution via email and social media. To screen for eligibility, prospective participants completed an electronic form linked in the fliers. Prospective participants were eligible to join the study if they identified as transgender or gender diverse, were 50 years old or older, and had been living in the U.S. for at least 10 years. Fluency in English and capacity to give informed consent were required for this study. Participants who did not have access to the Internet or were not able to participate by video call were eligible for Phase 1 as long as they could meet in person or speak on the phone. All Phase 1 participants were eligible to join Phase 2 if they were able to join group and individual sessions by video call.
Researchers estimated the participant group size for Phase 1 by assessing the “information power” of the evolving dataset (Malterud et al., 2016). Information power is inversely related to the number of participants needed for a study and is influenced by five criteria: study aims, sample specificity, established theory, dialogue quality, and analysis strategy (Malterud et al., 2016). The SAFEage study had narrow study aims, data with high specificity to the research question, and moderately high dialogue quality, indicating high information power in the dataset and the need for a small participant group. However, the use of cross-case analysis and semi-structured integration of the theoretical framework in this study were markers of moderate information power, suggesting the need for a moderate participant group size (Malterud et al., 2016). Researchers considered these factors alongside the need for more participants to enhance group diversity, estimating that a moderate participant group size (15–20 participants) would be needed for adequate information power.
Researchers were intentional about enrolling participants from diverse backgrounds to gain insights into intersectional factors affecting health equity for TGD older adults. Researchers purposefully enrolled participants of diverse racial and ethnic backgrounds, for example, by establishing connections with individuals and organizations serving communities of Black and Latino/a/e TGD adults in the U.S. To ensure that perspectives from different medical, legal, and political landscapes were represented, researchers aimed to enroll no more than half of participants from the state of their home institution (University of Virginia). Researchers and community advisors contacted state and national LGBTQ+ organizations, including one health center recommended by a participant that ended up generating significant interest in the study.
Study Contributors
This study integrates experiences and insights from community advisors, researchers, and participants to build understanding about the factors affecting health equity for TGD older adults. The following sections detail the role of community advisors and researchers in this study, while participant characteristics are detailed in the Analysis section. Initials were used as pseudonyms to represent all study contributors (initials used to name participants are substitutes for their actual initials). Consistent with efforts to mitigate power imbalances in this study, researchers opted not to assign alternate names as pseudonyms out of respect for the agency of community advisors and participants who had already chosen their names as part of their gender transition. Participant ages and self-described gender identities are provided for context alongside their assigned initials in the Analysis section. Researchers also aimed to represent participants as equal co-creators of knowledge in this study by referring to all study contributors (researchers included) in the same grammatical voice (third person).
Community Advisors
Community advisors included three TGD adults—C.B., G.B., and A.S.—with lived experience, scholarship, and community activism relevant to the study. The principal role of these community advisors was to review study materials and early de-identified findings to help researchers conduct a study that would be inclusive and accessible for TGD older adults. Community advisors gave formal written consent to participate and provided their demographic information. Their ages ranged from 53 to 84, and they described their gender identities as “trans man,” “transgender man,” and “female.” One member identified as Black, and two members identified as White. Researchers worked with each advisor during the developmental phases of the study to refine interview guides and participant handouts. Community advisors also reviewed preliminary findings and provided input on materials for participant review. C.B., G.B., and A.S. contributed to this publication as co-authors.
Research Team and Reflexivity
The research team included L.C., principal investigator and nursing PhD student, as well as I.C.W., V.L., and K.D.A., three tenured faculty members at the University of Virginia. L.C. is an asexual, White, nonbinary person; I.C.W. is a straight, Black/African American, cisgender woman; V.L. is a straight, White, cisgender woman; and K.D.A. is a queer, White, cisgender woman. By reflecting on their positionalities, researchers identified points of connection with participants while also illuminating their privilege and potential power imbalances. Researchers did not have established relationships with participants prior to starting the study. To build rapport, L.C. shared their gender identity and pronouns, their professional role, and their motivations for pursuing the research. To equalize power dynamics between participants and researchers, participant perspectives and priorities remained the focal point of discussions and analyses, and researchers maintained humility and gratitude throughout the study.
Data Analysis
Researchers used thematic analysis to develop themes and subthemes describing factors that affect health equity for TGD older adults, structuring the analysis according to guidelines outlined by Braun and Clarke (2022, 2024). L.C. transcribed recordings from Phases 1 and 2 and reviewed transcripts twice to check for errors, inviting participants to review their own transcripts. All transcripts were minimally edited for typographical errors, and filler words were removed as needed to facilitate understanding. L.C. performed initial coding in Dedoose (Version 9.2.012), a web application used for qualitative and mixed-methods data analysis.
L.C. first coded transcripts deductively, applying two codes to differentiate limiting factors from facilitating factors. Subsequently, they performed iterative inductive coding of the dataset to explore limiting and facilitating factors in more depth. Two coders (L.C. and K.D.A.) reviewed the inductive coding schema, and both coders modified the schema until agreement was reached. To form themes and subthemes, L.C. categorized inductive codes manually, grouping interrelated codes and exploring negative cases. The IRTHJ framework informed conceptual refinement of each theme. L.C. juxtaposed findings with excerpts and whole transcripts to assess the fit between themes and the dataset. All co-authors reviewed each theme for alignment with the research question and study purpose.
In alignment with the social justice orientation of this study, researchers employed a form of member-checking to engage participants in collaborative meaning-making and social change (Motulsky, 2021). Fifteen Phase 2 participants engaged in member-checking of study findings during individual and group sessions three months after the end of Phase 1, and nine engaged in member-checking at 6 months. Participants reviewed themes, offering feedback via video call or electronic free-response survey, and researchers modified themes based on participant observations and insights.
Trustworthiness
Researchers applied various methods to promote the trustworthiness of study findings. L.C. produced transcripts of recordings and maintained detailed observation logs during data generation. Engagement in peer debriefing and member-checking strengthened credibility of study findings. Inviting participants to review preliminary themes fostered consistency between study findings and their knowledge and experiences. Researchers enhanced transferability of the findings by recruiting a diverse participant group and building a comprehensive dataset. L.C. performed careful data management and maintained an audit trail of procedural and analytic decisions. As the principal investigator, L.C. kept a reflexive journal in which they assessed the influence of their positionality and assumptions on study processes and findings.
Analysis
Participant Group Demographic Characteristics.
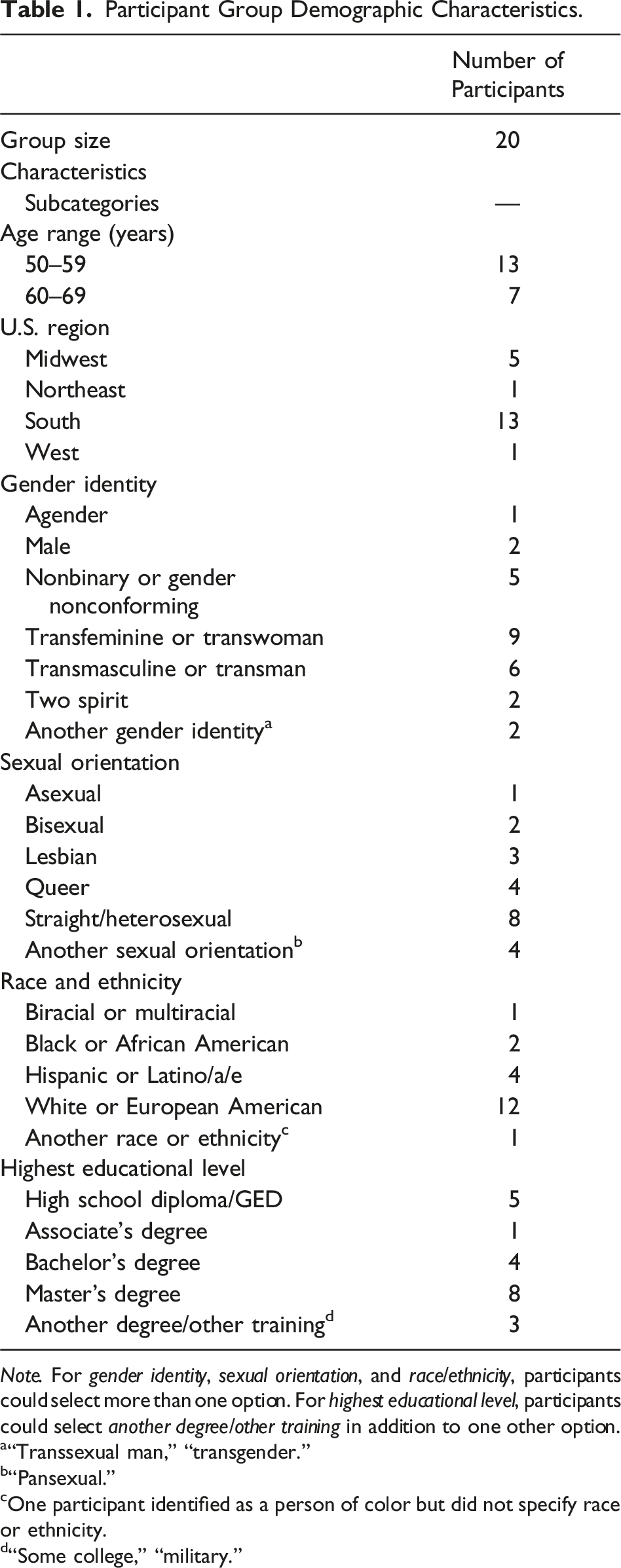
Note. For gender identity, sexual orientation, and race/ethnicity, participants could select more than one option. For highest educational level, participants could select another degree/other training in addition to one other option.
a“Transsexual man,” “transgender.”
b“Pansexual.”
cOne participant identified as a person of color but did not specify race or ethnicity.
d“Some college,” “military.”
From participant insights and narratives, researchers developed a set of six primary themes, each with 2–5 subthemes describing factors that limit (L) and facilitate (F) health equity for TGD older adults at (1) structural, (2) systemic, and (3) social levels of influence. Primary themes were (L1) Oppression driving adverse healthcare experiences; (L2) Gaps in healthcare resources and support; (L3) Disadvantages yielding poor health outcomes; (F1) Health justice promoting affirming healthcare experiences; (F2) Catalysts for change in healthcare; and (F3) Assets fostering agency and well-being. Structural-level factors (L1 and F1) pertain to societal and health system power structures; systems-level factors (L2 and F2) pertain to healthcare procedures, policies, and institutional systems; and social-level factors (L3 and F3) pertain to personal and interpersonal circumstances affecting health and agency within the healthcare system. Featuring data from both study phases, the following sections detail primary themes and subthemes describing limiting and facilitating factors and explore relationships among them at each level. Figure 2 illustrates themes and subthemes in a lock-and-key configuration explained in more detail at the end of the Analysis section. Lock-and-key conceptual model of multilevel factors affecting health equity for transgender and gender diverse older adults.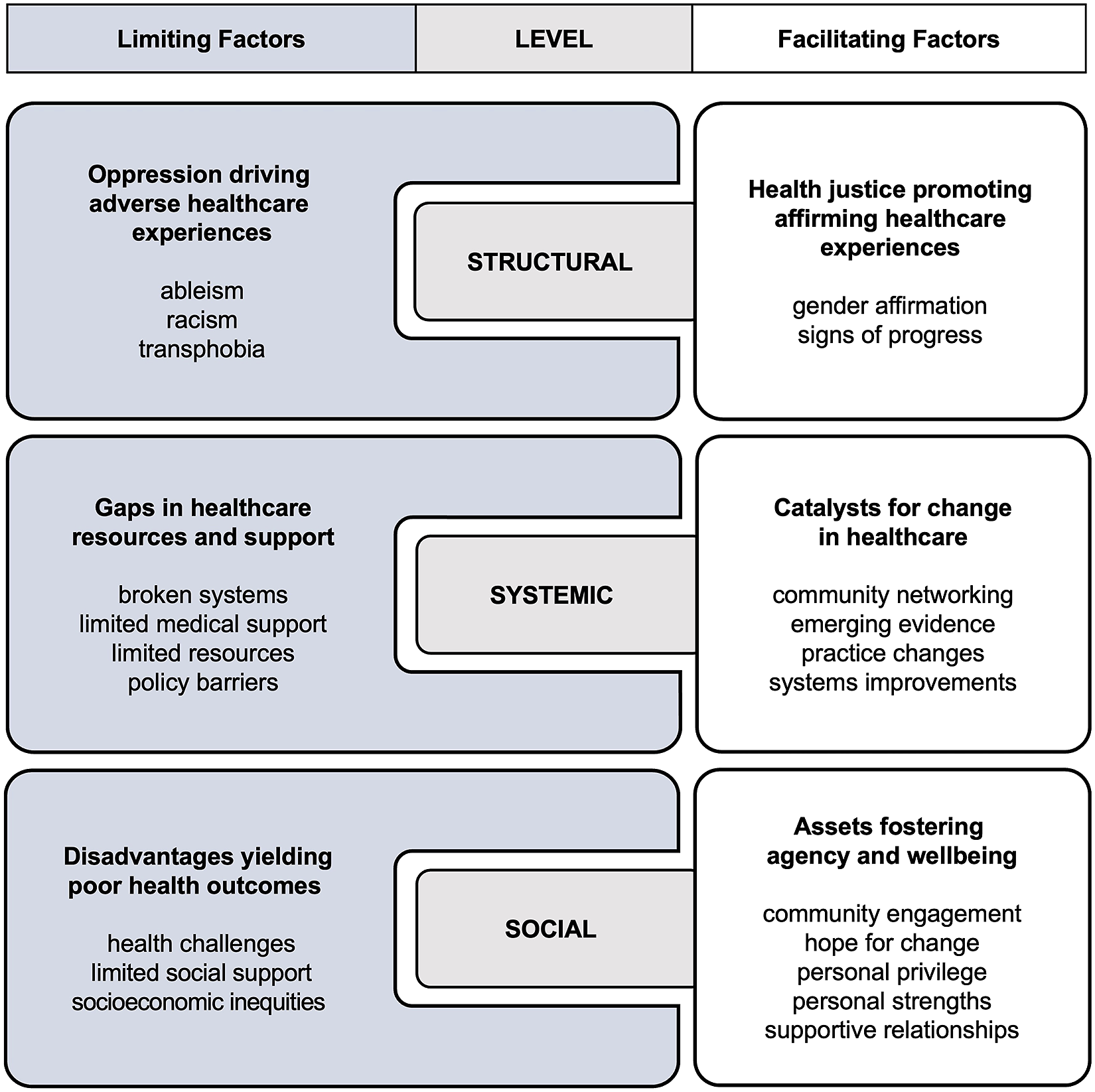
Limiting Factors
(L1) “Transphobia Will Kill You”: Oppression Driving Adverse Healthcare Experiences
Theme L1 refers to attitudes and actions that lead to disrespect, neglect, silencing, othering, abuse, and other forms of structural oppression that participants faced within the U.S. healthcare system. Subthemes include transphobia, racism, and ableism.
Transphobia
Recent incidents of transphobia in healthcare settings were reported explicitly by seven Phase 1 participants, with life-threatening consequences for some. B.H., a 50-year-old trans-identified, genderfluid person, asserted that transphobia is “running rampant” in the healthcare system, citing discriminatory experiences that he and some of his acquaintances had faced, including neglect for their care and lack of respect from healthcare professionals. “Transphobia will kill you,” he said.
Transphobic treatment in healthcare settings was a common experience for participants or members of their social networks. A.T., a 68-year-old trans woman, described the sense of shock she felt hearing a transphobic remark about her genitalia when in the emergency room for a cardiac condition. O.N., a 68-year-old trans woman, remarked that reports of transphobic treatment of TGD adults at a local hospital deterred her and her peers from seeking care at the institution. “I stay out of [Local Hospital X] because they are very anti-transgender,” she said, “And we all stay away from [Local Hospital X], at least those who I know are transgender.”
Racism
Structural racism affected health equity for some TGD participants of color. In general, Phase 1 participants of color reported adverse or mixed healthcare experiences more commonly than White, non-Hispanic participants. Reflecting on the ways in which structural racism has affected his treatment as a person of color within the U.S. healthcare system, B.H. said: It’s built into the structure of healthcare in terms of how it treated different ethnicities and bodies. It’s built in that way … how the healthcare system was built and its viewpoint on Black bodies, bodies of color, anything that was outside of the mainstream.
A.T. also noted the persistence of transphobia and racism in sectors of the healthcare system, calling for healthcare personnel to “give [TGD people of color] the same respect [as] anyone else.”
Ableism
Transphobia and racism also intersected with ableism among participants with disabilities in this study. At least two Phase 1 participants were managing a disability, and two participants shared that they were living with autism. Emphasizing the intersectional stigma affecting TGD older adults with disabilities, J.T., a 57-year-old nonbinary person, explained: If [we]’re going to talk about nonbinary and trans, we need to be having a parallel conversation about autism and about these related physical disabilities … there’s all kinds of content and writing out there about how intersectional those are. And they’re both things that can get you treated like absolute crap … all these things that diminish and minimize what you’re feeling. Those two factors go totally into it, I think.
Highlighting the intersections between transphobia, racism, and ableism that affect health equity for TGD older adults, B.H., as an older person of color with a disability, shared his experiences seeking care for the chronic health conditions he was facing. Quoting from a conversation with his medical provider, he asked, “Why haven’t you recommended that I go to a doctor that knows about folk who have this … condition? Because I’m trans, and you are afraid to address the intersectionalities.”
(L2) “It’s Just a Hairy, Tangled Mess”: Gaps in Healthcare Resources and Support
Theme L2 describes dysfunctional health systems and deficiencies in resources and support that affected healthcare access and quality for participants. Subthemes include policy barriers, broken systems, limited medical support, and limited resources.
Policy Barriers
For some participants, legislative and institutional policy barriers were threatening essential healthcare rights. Since “transgender rights are being pulled in many states” (E.R., a 61-year-old trans man) and some U.S. governing bodies are “trying to legislate away [the] existence [of TGD persons]” (K.P., a 69-year-old trans woman), political actions aiming to limit medical care for TGD older adults were a “major concern” (E.R.) for these participants. Additionally, D.J., a 50-year-old nonbinary trans man, identified institutional policy barriers resulting in “legal documentation and having everything transferred over and the healthcare system not accepting those legal changes that are actually in place.” He expressed concern about the consequences of misgendering in his medical records, especially if he were to lose capacity to advocate for himself due to a serious illness.
Broken Systems
Participants described long-standing systemic gaps in healthcare for TGD older adults which had been exacerbated by circumstances during the COVID-19 pandemic. J.T. remarked that healthcare systems have “just neglected all of us [TGD adults] for so long,” and “we’ve been relying on a bad system for a good decade or more.” Six Phase 1 participants explicitly raised concerns about systemic deficiencies affecting the care and safety of TGD older adults in long-term care settings. L.G., a 58-year-old nonbinary, agender person, remarked, “You hear about people being neglected or abused in nursing homes, but those people are all cis[gender]. So, when you add being trans [gender] on top of that, I just don’t see it being a good situation.”
Systemic factors limited access to care for some participants. For J.T., accessing healthcare had been “just a hairy, tangled mess” They explained, “I feel like I’m being gatekept out of healthcare,” referring to both prohibitive healthcare costs and anti-transgender discrimination in healthcare settings. Q.P., a 56-year-old man beginning his gender transition, struggled to access gender-affirming medical care for his transition due to insurance hurdles, repeated scheduling delays, and the burden of traveling to multiple medical appointments in different locations. For E.R., traveling long distances to access gender-inclusive care had also become burdensome with age. He explained: I’m seeing the doctor 45 minutes away. But it’s like, if this doctor leaves, now I’ll be driving four hours away to [a major city] for healthcare. What is that going to look like five to seven years from now when I don’t want to take the trip, or I can’t physically take the trip?
Limited Medical Support
When they were able to access healthcare, ten Phase 1 participants explicitly reported inadequate medical support due to lack of competency or sensitivity among healthcare professionals involved in their care. T.P., a 52-year-old “post-op” trans woman, shared that she had to disclose and explain her gender identity to a lab technician before a routine prostate cancer screening. Analogously, M.M., a 56-year-old trans man, “had to convince [his physician],” before undergoing a routine colonoscopy, “that [he] was born female and did not have a prostate.” I.H., a 55-year-old trans man, explained the burden that these kinds of interactions impose: “It’s more uncomfortable when you have to tell a healthcare professional [about your gender identity] … More questions get asked … Sometimes I’m just like, I don’t have it in me.” K.P. discussed the need for competent care beyond “a healthcare practice that may deal with gerontology but does not fully comprehend and analyze aging as a transgender [person].”
Nine Phase 1 participants explicitly expressed fears that lack of medical support would result in the withdrawal of gender-affirming treatments in later life. U.T., a 60-year-old, “nonbinary transfemme,” recalled, “I’ve heard horror stories of people de-transitioning, and they had to go back [to their sex assigned at birth].” Contemplating the risk of developing a serious illness later in life, O.N. shared that she would be “absolutely devastated if [she] woke up after three weeks in the hospital … and found out that nobody took care of [her] as a female.”
Limited Resources
Participants lamented the limited availability of gender-inclusive community services and financial resources, and they emphasized the need for more resources to “mitigate [their] current experiences” (B.H.) with health inequities, especially as systemic change unfolds at a slower pace. In particular, they noted the lack of information and research on healthcare for TGD older adults. C.W., a 52-year-old trans man, explained that even available health resources may not meet the nuanced needs of TGD older adults: Regular, heteronormative … resources for things like elder care are going to be framed for a heteronormative population, and … it feels like there’s just a lack of awareness … It’s not just like swapping out a gender … It’s a lot more complicated and layered for us.
With limited health resources and medical support, some participants like R.L., a 56-year-old trans woman, found themselves confronting systemic barriers alone: “I feel like a lot of times we’re just on our own and just navigating through the healthcare system.”
(L3) “If I Get Sick, I’m Pretty Much on My Own”: Disadvantages Yielding Poor Health Outcomes
Theme L3 refers to actual and anticipated socio-structural barriers affecting health outcomes for some participants. Subthemes include limited social support, health challenges, and socioeconomic inequities.
Limited Social Support
Six Phase 1 participants explicitly reported low social support for their care in later life. “My support is slim-to-none,” said D.J., “And by support, I mean, I have support from the medical team, but in terms of family connection, I don’t have that.” Without a strong support network, E.R. worried about finding someone to care for him during a serious illness, stating, “If I get sick, I’m pretty much on my own.” E.R. disclosed that he had faced the reality of his concerns during a recent hospitalization in which he found himself without a relative or friend to transport him home from the hospital. J.T. and U.T. also felt “isolated” without a robust social support system, and one participant had even contemplated suicide fearing that they would have no one to care for them if they experienced a serious illness in later life.
Health Challenges
Eleven Phase 1 participants reported prior hospitalizations for serious illness, and five participants explicitly shared that they had observed or personally faced chronic health conditions, mental illness, and substance use as negative health outcomes affecting their experience of aging. I’m living the life of somebody that’s way older than me actually, and many of us, our bodies are breaking down earlier due to lack of care, denial of care, what-have-you, but our bodies are breaking down earlier. So, things that we expect to see at 60 and 65, we’re seeing way early in us. (B.H.)
J.T. had also observed increasing morbidity and mortality among TGD people at younger ages, stating “It’s a little bleak … talking about real life expectancies as they are right now for trans people.”
Socioeconomic Inequities
For at least six Phase 1 participants, socioeconomic inequities, like financial hardship, lack of insurance, and housing insecurity, had the potential to limit their access to care and compromise their health and well-being. N.G., a 55-year-old person “beginning transition to female,” said that, for TGD older adults in the workforce, the risk of losing employment, and consequently insurance coverage, is “a huge issue” because “[for] a lot of jobs, if you come out [or, express your gender identity] at work, they won’t accept you.” B.H. emphasized the serious health implications of eschewing medical care due to underinsurance and fear of discrimination in healthcare settings: Many of us are aging without insurance. I’m talking about [those of] us, who are now afraid to go to the doctor’s and are choosing not to go to the doctor. When we’re getting to the doctor’s, our conditions are too far gone.
Facilitating Factors
(F1) “The Positive Wins”: Health Justice Promoting Affirming Healthcare Experiences
Theme F1 describes respectful, gender-inclusive treatment in healthcare settings and progress toward health justice for TGD older adults. Subthemes include gender affirmation and signs of progress.
Gender Affirmation
Sixteen Phase 1 participants explicitly shared a desire for affirmation of their gender identity in healthcare settings, and 14 shared examples of respectful, inclusive treatment they received when seeking healthcare. P.T., a 57-year-old trans woman, became tearful recalling a positive interaction with a physician: “In my first appointment … I could tell [the physician] had gone out of her way to make sure everyone knew my name and my pronouns. And just some of the messaging there … was exactly what I needed.” Participants reiterated the value of receiving respectful treatment from clinicians and medical support staff. “It [gender-affirming care] means they [clinicians and staff] respect me as an individual exactly the same as they respect anyone else who comes in,” said K.P.
Signs of Progress
Participants recognized subtle societal shifts, such as greater sociocultural acceptance of TGD people and examples of successful advocacy for transgender rights. S.W., a 64-year-old trans woman, stressed the importance of recognizing incremental progress toward health justice: “I know there’s a lot of negative in the world and in our country right now. That we need to deal with. But you’ve got to focus at least once in a while on the positive wins.” While structural limiting factors may dominate the narrative of healthcare for TGD older adults, the “positive wins” represent emerging signs of progress toward health justice that are allowing more TGD older adults in the U.S. to thrive. However, as K.P. observed when she expressed fears of being “legislated out of existence,” the potential harms of rising anti-transgender policy agendas render such progress precarious and vulnerable to erasure.
(F2) “There’s Been This Sea Change”: Catalysts for Change in Healthcare
Theme F2 details facilitating factors that foster systems changes to improve healthcare for TGD older adults. Subthemes include practice changes, systems improvements, community networking, and emerging evidence. In certain contexts, practice changes and systems improvements may actually limit health equity for TGD older adults when implementation methods and support infrastructure fail to achieve equitable and inclusive outcomes.
Practice Changes
M.M. had witnessed favorable changes in the healthcare system over the preceding decades, noting a shift in awareness of transgender health: “I really do think that the … general level of knowledge and understanding about trans people has changed a lot. So, I have some hope that there’s been kind of this sea change.” Although J.T. had not personally witnessed these changes, they proposed a person-centered strategy to promote further progress: “We need a whole paradigm shift … where we need to flip this on its head, and money is the last concern, and the human aspect is the biggest.”
Without proper support infrastructure, however, practice changes may stall. I.H. described a new mechanism in his healthcare provider’s electronic record system that would “flag” TGD patient accounts, prompting clinicians to use the patient’s correct pronouns. However, he said that the feature had not led to a change in practice because “you still have to educate [clinicians] to do that, because some people are still just going to be like, ‘I don’t care. I don’t believe in that.’” He added that misgendering continued despite efforts to curtail it.
Systems Improvements
Participants noted how gender-inclusive health systems facilitated their access to care and helped them plan for the future. M.M. described promising changes in the electronic health record systems of the medical practices where he sought care, highlighting measures designed to reduce misgendering by healthcare professionals. D.J., E.R., and T.P. praised the quality of care in clinics that specifically address transgender health, and P.T. shared that a transgender health clinic made her gender transition possible. “I don’t know that I would have transitioned if I hadn’t had access to that care,” she said.
Intended improvements may result in disaffirming experiences in some instances. K.P. described her frustration seeing “gender dysphoria” marked repeatedly on her medical forms when the diagnosis was irrelevant to the health condition that prompted her visit. However, she recognized the need for clinicians to have access to this information. “It’s an important thing to be there,” she said, “I just wished in some ways it wasn’t flashing at the top of every page.”
Community Networking
Participants discussed the role of community networking in advancing change for TGD older adults within the U.S. healthcare system. C.W. had observed an increase in access to information about gender-affirming medical care from healthcare institutions, noting that in the past it had been “just the network of us talking to each other, and that’s how we educated ourselves.” O.N. described online platforms that have extended these networks in recent years, providing channels to find information and support and to locate clinicians trained to provide gender-inclusive care. Naming peer networks across the U.S. that could fill the caregiving needs of TGD older adults in later life, F.P., a 57-year-old “transsexual man,” expressed hope that caregiving would be “built in” within “these network communities.”
Emerging Evidence
Noticing the emergence of new studies on healthcare for TGD older adults, some participants were hopeful that ongoing research would lead to more information and resources tailored to their unique healthcare needs. F.P. shared that he was serving on the advisory boards for several research studies in progress centered on LGBTQ+ older adults. “There’s people out there that are starting to research trans people, just the aging population in that community,” said R.L, “And I hope that just keeps going and helps. I’m sure it’s going to help the future generations.”
(F3) “I’m Who I Am Now”: Assets Fostering Agency and Well-Being
Theme F3 captures personal attributes, advantages, and actions that empowered participants to experience healthy aging, embody their true identities, and advocate for their care in later life. Subthemes include personal strengths, personal privilege, supportive relationships, community engagement, and hope for change.
Personal Strengths
Participant stories and insights revealed five key attributes, resilience, resourcefulness, self-advocacy, wisdom, and self-assurance, which allowed participants and their peers to transcend adverse healthcare experiences and find alignment of mind, body, and identity. Highlighting resilience and resourcefulness within TGD communities, R.L. said, “That’s what I like about our community is just, the people are … resilient, and that … when you’re alone, you get creative, you learn something.” D.J. identified his “ability to self-advocate” as a personal strength that had grown substantially since his “younger years.” Recognizing the embodied wisdom of TGD older adults, B.H. said, “We’ve been living in this body. We know what works as well. We have the data that’s stored in us, which [healthcare professionals and researchers] haven’t captured yet.” After years of concealing her identity and surviving a suicide attempt that nearly ended her life, O.N. cultivated self-assurance through her gender transition. When asked about her confidence and renewed energy for life, she replied, “I’m who I am now.”
Personal Privilege
Participants had privileges that benefited their health and facilitated their access to care. With the advantage of being in good health, some participants were taking preventative measures “to not be dependent” (R.L.) in later life and “to continue advocating” (D.J.) for their care. Five Phase 1 participants shared that they had financial assets and insurance coverage to support them in later life. K.P. acknowledged her “place of privilege” financially but clarified that her experience may be “different than most transgender individuals.”
With expanded insurance coverage for gender-affirming medical care, many participants were “very fortunate” (K.P.) to transition in later life, experiencing a sense of inner alignment and improved health and well-being. L.G. marveled at the benefits of gender-affirming care to their health and relationships after spending “forty years just being in a state of mental anguish.” Having endured pressure from family to conceal her gender identity since childhood, H.K., a 65-year-old trans woman, shared that after starting her transition, she “got out of the shower one day, and it was the first time in [her] life that [she] didn’t have dysphoria when [she] looked in the mirror.”
Supportive Relationships
Twelve Phase 1 participants identified social support as a benefit to their well-being or as a source of advocacy in healthcare settings. “I’ve been really lucky and privileged to have a … supportive family and friends and other community supports,” said M.M., adding, “I have a spouse who I know will advocate for me” during a serious illness. A.T. planned to name her niece as her healthcare advocate, and O.N. had appointed friends as executors of her will. S.W. acknowledged the value of her spouse’s support during her gender transition: “I credit her with me coming as far as I have as my authentic self.”
Community Engagement
Engagement in their communities enabled some participants to promote health equity for their peers. “I know everyone. I know the therapists, I know the doctors, the surgeons,” said O.N., describing how she connected members of her local TGD community to healthcare professionals that provide gender-affirming medical and surgical care. Acknowledging her privilege to have access to high quality medical care, S.W. sought opportunities to support her community: “I want to help because my experience has been so positive. And if it’s not positive for everyone, I’d like to be that support if I can.”
Hope for Change
Through adverse healthcare experiences, some participants maintained a sense of hope for change. Imagining the benefits of gender-inclusive healthcare resources and support, R.L. expressed hope in “just having that knowledge that getting older as a trans person doesn’t have to be scary.” Speaking from personal and professional experience in the field of transgender health, M.M. said, “Overall, I’m optimistic, and I think mainly that’s because I’ve really seen a lot of change.”
“Like a Lock to a Key”: Modeling Limiting and Facilitating Factors at Multiple Levels
Participants acknowledged linkages between limiting and facilitating factors. While reviewing themes in Phase 2, F.P. said, “These [themes] don’t strike me as extreme … these themes are more closely linked. It’s like, yes, there’s structural oppression, but … people have figured out how to navigate structures to reduce the oppression.” The complex interplay between limiting and facilitating factors was apparent in the following exchange between two Phase 2 participants, I.H., a Black transmasculine veteran living in the western region of the U.S., and S.W., a White transfeminine veteran living in the northeast: S.W.: [to I.H.] I feel I’m one of the lucky ones. I’m also a veteran. And I’m part of a couple of groups that I’ve heard some pretty horrific stories throughout the country. But where I am in [U.S. state], I have not experienced any of it. I.H.: [to S.W.] I think I fall into one of those categories where it is a little bit different. I am treated a little bit different, and that’s part of life … So, it’s good to hear, I mean, both sides of the story … because I know there’s good and there’s bad in most everything. But categorically, I experienced a lot of the bad.
S.W. and I.H. had contrasting experiences within the same government-run health system, demonstrating regional and possibly race-based influences on the factors affecting health equity for them as TGD older adults. However, they each recognized the validity in the other’s perspective, showing awareness of the complex realities inhabited by a diverse population of TGD older adults seeking healthcare in the U.S. One participant who provided feedback anonymously shared that “coming out and taking control over the quality of my healthcare as a trans person has been rewarding; however, it’s also made me more aware [that] the lack of empathy, discrimination, and daily challenges are widespread concerns.”
During an individual session in Phase 2, E.R. drew parallels between the resourcefulness involved in his work as a locksmith and the resourcefulness required for him to navigate barriers to healthcare access that he had experienced. His narratives prompted a visualization of the limiting and facilitating factors affecting health equity for TGD older adults as locks and keys. Participants who reviewed study findings at the end of Phase 2 endorsed the visualization, rendered in Figure 2. E.R. said, “It fits just like a lock to a key.”
Discussion
Through interviews and member-checking sessions with 20 TGD older adults, researchers developed six themes describing limiting and facilitating factors that affect health equity for TGD older adults at structural, systemic, and social levels. These levels parallel the three layers of the IRTHJ conceptual framework, which “requires researchers to theorize intersecting relations of power at multiple layers of analysis” (Wesp et al., 2019, p. 291). This study extended the IRTHJ framework by including not only factors that cause health inequities but also factors that promote equitable and inclusive healthcare at each level.
As represented in the lock-and-key model, limiting and facilitating factors identified in this study appear to have a dialectical rather than a diametrical relationship with one another, shaping the healthcare experiences of TGD older adults concurrently. Despite criticism of binary barrier–facilitator constructs as decontextualized and overly simplistic, the dialectic between limiting and facilitating factors illustrates the complex state of health (in)equity experienced by TGD older adults in the U.S. healthcare system (Bach-Mortensen & Verboom, 2020). For instance, the degree of influence of factors like limited medical support may determine whether related factors like practice change ultimately limit or facilitate health equity. Moreover, the influence of each factor on health equity seemed to vary based on the social, regional, political, and economic contexts in which participants were situated. For example, participants receiving care within the same health system but in different regions had different experiences of care quality and gender affirmation in those settings. Lastly, paradoxical pairings of limiting and facilitating factors, such as limited social support and supportive relationships; broken systems and systems improvements; and transphobia and gender affirmation, represent simultaneous manifestations of repression and resistance that may occur within communities marginalized by dominant power structures (hooks, 1989).
Findings from the SAFEage study complement emerging evidence reported in recent publications on healthcare within TGD communities. Structural limiting factors identified in this study, such as transphobia, racism, ableism, and (implicitly) ageism as well as systemic factors such as limited resources, have been used in prior research to qualify TGD adults as a population with substantial intersecting vulnerabilities (Baril & Silverman, 2022; Velasco et al., 2023). The SAFEage study augments this research by integrating strengths held by TGD older adults into the conceptualization of transgender vulnerability. The dialectical lens applied in this study suggests that vulnerability and strength can coexist, with space for both precarity and capacity in the experiences of TGD older adults as they navigate the U.S. healthcare system.
Findings coincide with new research that identified barriers to care for TGD adults, such as disrespect and mistreatment in healthcare settings; limited access to care and medical support; socioeconomic disadvantages; and intersectional factors driving health inequities (Berrian et al., 2025; Johnson et al., 2019). Likewise, in a separate study, gender affirmation and peer support facilitated favorable experiences for TGD older adults within behavioral healthcare settings, which is consistent with findings from the SAFEage study (Lampe et al., 2024). However, the SAFEage study also expands on the current body of literature by presenting limiting and facilitating factors jointly, which may aid in the development of policies and interventions that address health inequities with both breadth and nuance.
Research, Practice, and Policy Implications
Findings from this study may inform future research. Focused explorations of individual factors affecting health equity for TGD older adults in future research would cultivate a deeper understanding of each factor. Limiting factors with heightened urgency, such as low social support, housing insecurity, and suicidality among TGD older adults, warrant further study and timely intervention. Researchers may design multi-axis interventions to address factors affecting health equity for TGD older adults at each level of influence. Centering the knowledge of TGD older adults from diverse backgrounds in future research would be essential.
Study findings also have implications for practice and policy. In clinical practice, themes and subthemes from this study may inform educational programs designed to promote clinician competency in the care of TGD older adults. Findings also indicate the need for federal and state policies to protect the rights of TGD older adults. Such policies may secure health insurance coverage; permit preferred gender markers on official documents, such as health records and death certificates; and devote funding to further research on the healthcare needs of TGD older adults (Kinney et al., 2022). Existing programs, such as the LGBTQIA+ Aging Project of the Fenway Institute and SAGE, an organization providing advocacy and services for LGBTQ+ older adults, may serve as models for providing healthcare services for TGD older adults and supporting trans-inclusive policy.
Strengths and Limitations
This study has several limitations. Consistent with its purpose and scope, this study provides a broad view of various factors affecting health equity for TGD older adults; however, in-depth descriptions of each factor require further exploration. Limiting and facilitating factors described in this study are drawn from experiences specific to one participant group, so some factors that affect health equity for the U.S. population of TGD older adults as a whole may not be represented. Due to the complex contextual and temporal variability of barriers and facilitators, factors identified in this study may have limited transferability to contexts that differ from the situations and circumstances described by participants (Bach-Mortensen & Verboom, 2020). However, findings were consistent with existing evidence on healthcare for TGD older adults, reinforcing their applicability to different contexts.
Despite outreach to diverse communities of TGD older adults, this study does not represent the perspectives of Black trans women, Asian TGD older adults, or Indigenous TGD older adults. It also does not represent the perspectives of TGD adults who do not speak English, such as Spanish-speakers and members of the Deaf community. Further, this study lacks representation of TGD older adults aged 70 and over and TGD older adults with cognitive impairment. In future studies, researchers should aim to diversify modes of outreach to ensure that people from the aforementioned racial, ethnic, linguistic, and age groups, as well as TGD adults with serious or terminal illnesses, are represented. Because study participation was limited to U.S. residents, findings may have limited global transferability; however, this study adds to the growing global evidence base on healthcare for TGD older adults (Banerjee & Rao, 2020; Pang et al., 2019; Reisner et al., 2016).
Conclusion
This study developed six themes describing limiting factors (oppression driving adverse healthcare experiences; gaps in healthcare resources and support; and disadvantages yielding poor health outcomes) and facilitating factors (health justice promoting affirming healthcare experiences; catalysts for change in healthcare; and assets fostering agency and well-being) affecting health equity for TGD older adults in the U.S. at structural, systemic, and social levels of influence. They form a dialectic in which limiting and facilitating factors co-occur to varying degrees. Differences in social, regional, political, and economic contexts appear to influence these factors. Filling a gap in the literature, this study augments the body of knowledge on health equity for TGD older adults with implications for future research, clinical practice, and policy change.
Supplemental Material
Supplemental Material - Multilevel Factors Affecting Health Equity for Transgender and Gender Diverse Older Adults
Supplemental Material for Multilevel Factors Affecting Health Equity for Transgender and Gender Diverse Older Adults by Lauren Catlett, Ames Simmons, Ishan C. Williams, Virginia LeBaron, Charley Burton, Gracie M. Barker, and Kimberly D. Acquaviva in Qualitative Health Research
Footnotes
Acknowledgments
The authors thank each study participant for generously sharing their knowledge and experiences during their study. The authors acknowledge the use of the qualitative analytic web application Dedoose (Version 9.2.012) to assist with coding during the study.
Author Contributions
Lauren Catlett: conceptualization, methodology, investigation, formal analysis, validation, writing (original draft), writing (review and editing), visualization, project administration, and funding acquisition; Ames Simmons: conceptualization, resources, and writing (review and editing); Ishan C. Williams: methodology and writing (review and editing); Virginia LeBaron: methodology and writing (review and editing); Charley Burton: conceptualization, resources, and writing (review and editing); Gracie M. Barker: conceptualization, resources, and writing (review and editing); Kimberly D. Acquaviva: conceptualization, methodology, validation, writing (review and editing), and supervision.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ishan C. Williams declares involvement with the HRSA Geriatric Workforce Enhancement Program (U1QHP53069-01-00) and BRIDGE2AI CHoRUS for Equitable AI (OT2OD032701). Dr. Ishan C. Williams did not have access to data in our study and did not conduct analyses of the data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Psychological Foundation Springfield Research Fund Dissertation Fellowship.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.