
Abstract
While the cancer advocacy community has been pivotal in progressing oncology care, supporting young adults with advanced cancer transitioning to palliative care continues to be a complex challenge. Palliative care services may not be offered by healthcare providers or engaged by young people themselves. This is in the face of the recognized value that palliative care can provide young people and their families. The purpose of this study was to explore what cancer advocates can do to support young adults (18–39 years of age) with advanced cancer in their transition to palliative care. A community-based research perspective supported engagement with members of the #AYACSM (Adolescent and Young Adult Cancer Societal Movement) from the United States and Canada through social media. Analysis was guided by a reflexive thematic analysis approach to articulate four action-oriented themes: advocate for advances in the delivery of care; support healthcare provider education; mobilize knowledge and share stories; and leverage technology for advocacy efforts. Young adult cancer advocacy must span the continuum of cancer care from prevention to end-of-life. There exist gaps in advocacy efforts surrounding support for young people in their transition to and the integration of palliative care services. Creative and innovative advocacy approaches are needed. This study also showed opportunities for conducting qualitative research through an existing online community as an approach conducive to community-based research.
A cancer diagnosis during the span of adolescence to young adulthood (15–39 years of age) foreseeably comes at a time of critical social, emotional, and physical development (Canadian Partnership Against Cancer, 2017; Perez et al., 2020; Zebrack et al., 2016). The results of which may be unique psychosocial challenges necessitating age-appropriate, patient-centered care that takes an inclusive biopsychosocial approach (Zebrack et al., 2016). In addition, it is recognized that adolescents and young adults (AYAs) often present to health systems with advanced disease, having received delayed diagnoses (Canadian Partnership Against Cancer, 2017; Tricoli et al., 2016; Zebrack, 2009).
Palliative care services have the potential to help AYAs and their families in the face of advanced cancer by providing holistic, interdisciplinary support (Canadian Partnership Against Cancer, 2017; Foster et al., 2019; Rosenberg & Wolfe, 2011). Yet, despite the recognized importance of palliative for AYAs, there are many unanswered questions, as shown in a recent scoping review (Drake et al., 2021, 2023). In particular, there is limited research attending to the perspectives of young adults (YAs; 18–39 years of age) living with advanced cancer as well as community members (e.g., non-profit organizers, researchers, advocates, partners, and policymakers) involved in their care (Canadian Partnership Against Cancer, 2017; Drake et al., 2021, 2023). The focus of this study is to engage with the latter, the contemporary perspectives of AYA cancer community members.
AYA and YA Cancer Community Members
Historically, the recognition of YA cancer patients as a unique oncology population was propelled forward in the 2000s due to pivotal publications, including the National Institutes of Health and National Cancer Institute’s report from the Adolescent and Young Adult Oncology Progress Review Group, which was co-developed with the Livestrong™ Young Adult Alliance (Canadian Cancer Society, 2009; Mick, 2008; National Cancer Institute, 2006). This report largely resulted from the efforts of the collaboration of multiple AYA community members, including advocates for the YA cancer population (National Cancer Institute, 2006). YA advocates have long had awareness of the unique needs of YAs with cancer (e.g., oncofertility; education and employment challenges) and have made strides in the development of guidelines, programs, and other resources for them (Stupid Cancer, 2021; Young Adult Cancer Canada, 2024). However, it would seem that advocacy is still needed to advance healthcare professionals’ and policymakers’ understandings of YA palliative care (Rosenberg & Wolfe, 2011). It would, therefore, make sense to return to the perspectives of AYA community members (Drake et al., 2023; Rosenberg & Wolfe, 2011). Social media is one possible venue with its own opportunities and challenges for exploring such perspectives.
Social media is confronting the hierarchies of academic medicine, research communities, and other institutions by fostering online discussions that mitigate traditional power imbalances (Katz et al., 2019). However, while social media may afford the perspectives of communities of individuals, it can also be limiting. For example, not everyone has access to social media, is interested in participating in online discussions, nor necessarily feels comfortable sharing their opinions in this way. More so, social media may inadvertently amplify certain perspectives, not only by virtue of bringing together people of shared interests and common perspectives but also as a consequence of the various artificial intelligence technologies that work in the background to mediate such interactions (Coeckelbergh, 2024). And it should be acknowledged that social media can be a source of misinformation. That said, disease-specific hashtags used on the X (formerly Twitter) platform have the capacity to unite community members and facilitate conversation and networking over shared healthcare interests across geographic distances and other barriers (Feliciano et al., 2020).
#AYACSM
#AYACSM (Adolescent and Young Adult Cancer Societal Movement) is a hashtag and volunteer-led initiative that our first author (E.K.D.) co-founded in 2013 with Billy Paymaster, formerly of the organization Hope for Young Adults with Cancer, and Maureen Sweet, formerly of the organization Stupid Cancer (2021), to unite AYA advocates around the world on X (Perales et al., 2016). In November of 2013, #AYACSM was filed and officially recognized with Symplur (n.d.), as part of their healthcare hashtag project. Symplur Signals analytics program is an independent platform that is known for its specialization in healthcare and proprietary algorithm and is home to the cancer ontology tag project, a list of formal cancer hashtags used around the world (Salmi et al., 2020; Symplur, 2024).
Like several other disease-specific hashtags, #AYACSM conducts regular tweet chats, which are live public discussions that take place between X users (Furlan et al., 2021; Perales et al., 2016; Salmi et al., 2020). #AYACSM tweet chats began in July of 2014 and, thereafter, have been held monthly. The discussions are conducted by a moderator(s) who welcomes people to the chat and posts a schedule of questions to support conversation. The chats have covered a variety of topics that are relevant to the YA cancer movement, including oncofertility, patient engagement in research, research priorities, and social media engagement. The discussions allow those who identify as AYA advocates to respond live to tweets in plain, everyday language, in a conversation using #AYACSM. Advocates are defined as anyone who speaks, writes, or in other ways actively supports the AYA cancer movement. Participation varies each month, but most conversations involve those who conduct AYA research (including trainees), non-profit organizers, healthcare professionals, caregivers, and patient advocates. These international conversations negate some of the need and resources required to conduct in-person meetings (Furlan et al., 2021). Tweet chats have been used by other oncology X communities including #BTSM (Brain Tumor Social Media) to conduct qualitative research (Cutshall et al., 2020; Salmi et al., 2020) and have proved useful for studying community members’ unique perspectives on palliative care (Salmi et al., 2020). Cutshall et al. (2020) used X to explore barriers to advance care planning through #BTSM community members. While #AYACSM has been used to conduct previous palliative, end-of-life, and advanced cancer conversations, the chat has never been conducted for research purposes. The purpose of this qualitative study was to explore perceptions of what AYA cancer advocates can do to support YAs transitioning to palliative care.
Methodology
This reflexive thematic analysis study was guided by a community-based research perspective (Braun & Clarke, 2021; Collins et al., 2018). A community-based perspective supported the engagement of patient and caregiver #AYACSM partners on our research team, following principles of the Patient-Centered Outcomes Research Institute’s guidelines (PCORI [Patient-Centered Outcomes Research Institute], 2015). Our research question was co-developed and informed by previous research engaging community partners (Drake et al., 2023) and stems from the social justice imperative of seeking equity in care for young people living with cancer. Specifically, North American clinical guidelines for AYAs recommend that they receive early integration of palliative care with their standard care in oncology (Abdelaal et al., 2021); however, research has found that not all eligible AYAs receive palliative care referrals (Lockwood et al., 2021). The use of the term “transition” throughout this study was inclusive of the aim to integrate these services alongside oncological care. Imperative to our reflexive study was the acknowledgement of the power and privilege that our study team holds in society, as the experiences and views of our team are integrated with the community participants throughout the conduct of this study and the analysis process. Our research team identifies as white, and some of our members are part of the queer and disabled communities. From a community perspective, our first author (E.K.D.) has long-standing commitment to the AYA cancer community, supporting engaging with #AYACSM through the X platform. Three of our study team members (E.K.D., D.T., and I.R.) have participated in the #AYACSM community for several years.
Participants
Participants in the study were identified as those using the #AYACSM hashtag and interacting with the discussion on X (i.e., participants were self-identifying as AYA advocates). As a community, #AYACSM defines advocates as anyone who speaks, writes, or in other ways actively supports the AYA cancer movement. Historically, those who participate in the chat do so to varying degrees, from liking a tweet, being tagged in a tweet, and/or retweeting one, to being an active participant in the conversation. The chat was advertised on X, Facebook, LinkedIn, and Instagram using the #AYACSM promotional image. Thirty advocates and broader community members were personally and privately contacted to let them know about the chat and/or promote it. This recruitment approach was consistent with how the chat is normally communicated within the #AYACSM and the larger AYA cancer community.
Ethical Considerations
#AYACSM Tweet Chat Script.
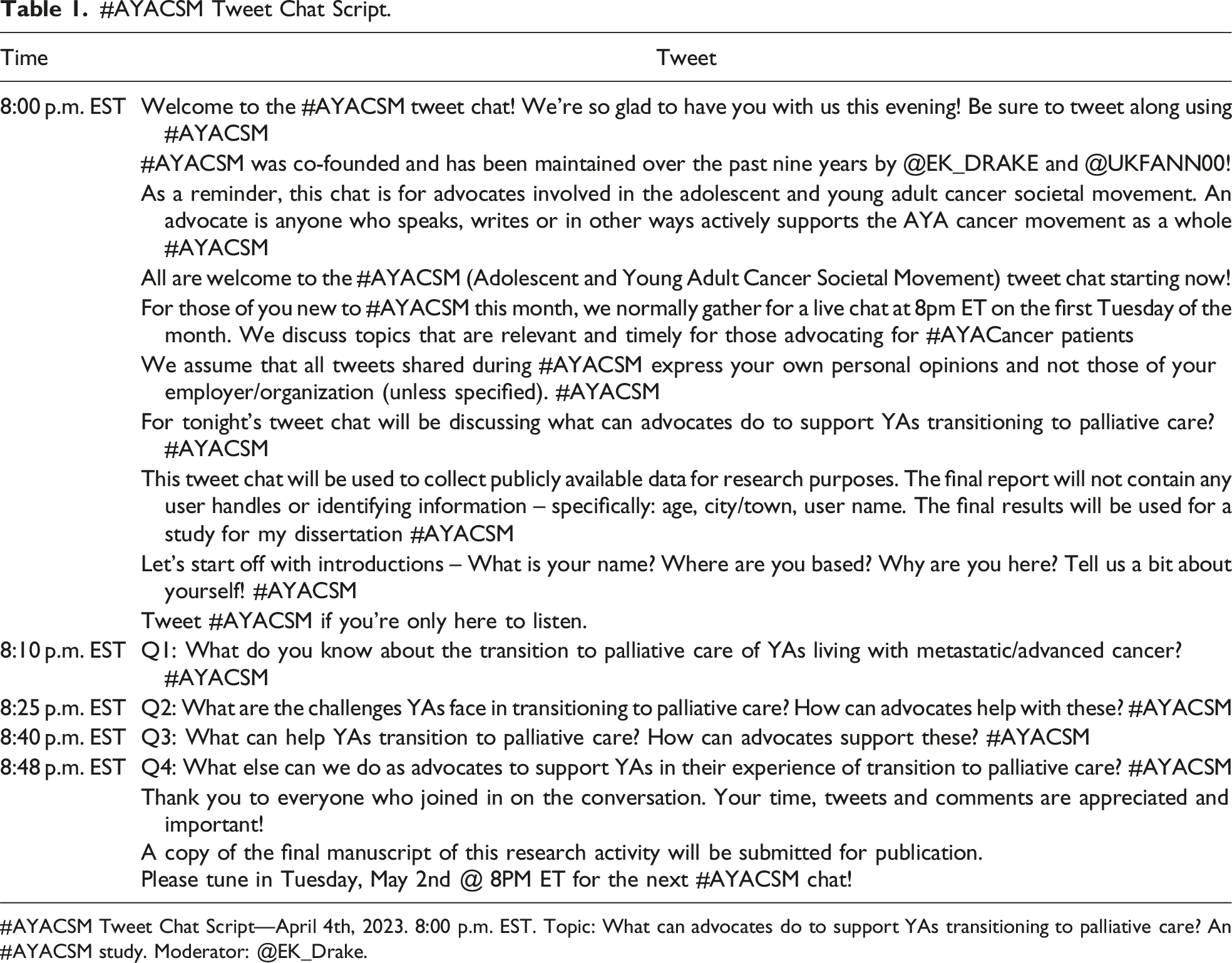
#AYACSM Tweet Chat Script—April 4th, 2023. 8:00 p.m. EST. Topic: What can advocates do to support YAs transitioning to palliative care? An #AYACSM study. Moderator: @EK_Drake.
Data Generation
The #AYACSM tweet chat took place on April 4, 2023, at 8 p.m. EST during the 2023 Global Adolescent and Young Adult Cancer Awareness Week. A central question was posed in a promotional graphic for the event: What can advocates do to support YAs transitioning to palliative care? This question prompted exchanges both in direct response to the question (i.e., answering the question) as well as to topics related to the question (e.g., current deficiencies in access to palliative care). A semi-standardized script guided the conversation (see Table 1). Members of the #AYACSM community on our research team (D.T. and I.R.) provided input into this script, in addition to other aspects of the research protocol in advance of the tweet chat. This served as an activity of piloting for understandability and significance. Our first author (E.K.D.) moderated the official conversation which took place in English over an hour in duration. Members of our research team who are also #AYACSM community members (D.T. and I.R.) helped to promote the conversation. Aligning with community-based research practice, they also participated in the conversation. Following, the conversation continued on its own for an additional hour and 15 min with people using the hashtag to reply to comments and ideas that were shared during the moderated hour-long conversation. While the chat was open to any X users, only those who included “#AYACSM” at the end of their tweets and interacted with the conversation were included in the discussion. The tweet chat’s data were collected from 8:00 p.m. EST to when the discussion came to a close as people stopped actively engaging with the discussion’s content at 10:15 p.m. EST.
Data Analysis
Descriptive X #AYACSM analytics were accessed from Symplur Signals Dashboard (Salmi et al., 2020; Symplur, n.d.; Symplur, 2024). This data helped to contextualize the reach of the chat’s tweets to X users and measure engagement with the discussion. The measures included were impressions (number of times the hashtag is seen [X Help Center, 2024]), tweets, participants, countries represented, and average tweets per participant. Symplur (n.d.) analytics was also used to group the participants. While this software categorizes individual accounts into specific categories, many participants identify with more than one (e.g., patient advocates who are also healthcare providers).
Reflexive thematic analysis allowed us to explore meaning patterns across the X data. The tweet chat transcript was then entered into and managed in NVivo (2024).The first author (E.K.D.) took reflexive notes on her initial reactions after completing the moderation for the tweet chat and continued these efforts throughout the analysis process. This reflexive journal supported returning to varied analytic interpretations of the qualitative material throughout the project.
Initial coding of the qualitative material was completed by the first author (E.K.D.). This involved immersion with the qualitative material through reading, re-reading, and making notes. Following, codes were generated to explicate important features of the data that were perceived to be relevant to the research question. These were then organized under preliminary draft thematic statements. In comparison, theme development was a collaborative process between the first author and authors (L.E.W. and M.V.M.). Drafts of the thematic statements, accompanying analytic narrative texts, and data extracts were shared. This afforded dialogue around different possible interpretations. In this way, through sharing of writing and rewriting, the analysis was developed through group writerly and readerly engagement (Braun & Clarke, 2021). The inductive analysis aimed to go beyond the explicit or surface meaning of the text (semantic meaning) to also explicate hidden meanings or underlying assumptions, implicit ideas, etc. (latent meaning [Braun et al., 2016]). We organized our text around the semantic themes and tried to explicate latent meaning in each paragraph. Preliminary drafts of the analysis were circulated to the remaining authors and team members, including those from the #AYACSM community (D.T., I.R., and J.C.) for their thoughts and insights, which helped to further refine the themes. In this way, the input from the larger team supported a more nuanced and richer interpretation (Braun & Clarke, 2021). We chose to write the analysis in third person to reflect the varied perspectives of our research team which were informed by our unique life experiences and positionalities. For example, not all of us identify as members of the #AYACSM community, and we felt it would be disingenuous to write as if we were. Overall, we found a third person voice supported collaborative dialogue around the tweets, a focus on the tweets, and reflected our team members’ contributions to the manuscript.
We recognize that reflexive thematic analysis has become a common approach to qualitative research, and that researchers at times deviate from its epistemological and methodological foundations. We refer the reader to contemporary writings by Braun and Clarke on epistemological grounding, methodological coherence, and reflexive openness (2023a, 2023b, 2024). For the purpose of this study, we understand validity as relating to the strength of our interpretation as one possible interpretation of the qualitative material we worked with. Following from Braun and Clarke, we hope the reader will read the data extracts as providing the “foundational validation” for our analytic claims (2021, p. 131). We aimed to preserve the integrity of each tweet by refraining from editing the material recognizing the medium of X yields material that is different than the kind afforded by engaging in one-on-one interviews where meaning can be explored through dialogue. We point the reader toward recently published guidelines by Braun and Clarke (2024) to judge the validity of our work.
Analysis
Twenty-four users from the United States and Canada participated in the tweet chat to varying degrees. Participants tweeted an average of 15 tweets each, resulting in 360 tweets shared during the discussion. Tweets were retweeted 143 times during the data collection period, and the tweet chat garnered 1.5 million impressions. Among the participants and those mentioned in the discussion, Symplur Signals (Symplur, n.d.) detailed participants as patient advocates, healthcare providers, advocacy organizations, doctors, provider organizations, researchers/academics, individuals who work in other areas of health care, journalists/media, investigator, media organization, and those not categorized.
We developed our analysis around the following action-oriented themes regarding how YA cancer advocates can focus their efforts to improving access to/integration of palliative care for YA patients and their families:
Advocate for Advances in the Delivery of Care
Underlying the #AYACSM tweet chat was the shared belief that deficiencies exist in the care of YAs: timeliness in referral to services, lack of continuity in care, and failures in integration of palliative supports. YA advocates valued the role and expertise of palliative care services, and they identified their role in pushing to ensure best practices are utilized to support timely and equitable transitions in care.
As one participant tweeted, From the work that I’ve done with #AYAs & #PalliativeCare, I’ve learned that it might be helpful to integrate palliative care supports earlier in the disease trajectory … to help with symptom management, illness understanding, to explore goals/wishes for care. (P5)
However, palliative care is not as easily accessible at some institutions as one participant noted: I think the transition in Canada varies by province. From a few friends that I’ve had go through it in Manitoba, it has been very slow and unable to continue maintenance chemo when there is no chance of cure and pain needed to be controlled. Very bad. (P10)
Across the discussion seemed to be an implicit recognition that more needs to be done to ensure that YAs have access to palliative care services. Two of the key initiatives highlighted by many of the participants in the discussion included the need for advocates to push for patient navigators (also referred to as care coordinators) and auto-referrals (automatic referrals to palliative care). Patient navigators can support the individualization of an adult system to the unique needs of YAs. In comparison, auto-referrals support timely involvement of individuals with this expertise, such as palliative care specialists: The larger the care team, the more complex the burden of treatment management by the patient. More people, more information, more to keep track of. Advocates can push for care coordinators to serve as the main point of contact when things get confusing. (P15)
Introducing palliative care early can also help with identifying the goals of care in addition to bringing in the valued knowledge and skills of other team members: Introduced early in treatment, palliative care can be key to bringing in specialists that you may not otherwise connect with—e.g., dieticians, pain management specialists, mental health experts—which could lead to much more comfort and support during the cancer experience. (P20)
However, systems are complex, and in order for health systems to fully adopt this practice, advocates need to focus efforts around supporting healthcare providers by ensuring they have the resources needed to provide appropriate levels of care. One participant tweeted: Advocacy action has to be loud enough for hospital policymakers and insurers to hear. I believe that would take analysis proving significant overall savings for them in patients engaged in palliative care. (P20)
Participants expressed the need to lobby to government and other related parties to ensure there are enough providers and other human/material resources for YA patients and their families.
Support Healthcare Provider Education
Advocates’ tweets commonly seemed to express a belief that healthcare providers are lacking in their understanding of the needs and preferences of YAs. Following, they identified a need to develop, mobilize, and implement inclusive education initiatives that teach healthcare providers about unique YA cancer issues and also intersecting social justice issues. Throughout the chat, some participants expressed sentiments that some providers may be keeping patients from receiving palliative care services due to a lack of such understanding. One participant highlighted: From the clinician perspective, I know this isn’t always done well. Sometimes clinicians are hesitant to talk about #PalliativeCare with #AYAs as they worry about taking away hope or causing distress … But by not talking about it, we can end up depriving patients & their loved ones the opportunity to access supports. This can leave people feeling alone & unprepared. (P5)
Many of the YA advocates identified that education is pertinent for the delivery of age-appropriate, person-centered specialist care. One participant explained that providers need to have this education in order to adopt needed changes in practice so that services can meet the unique needs of YAs: Palliative care clinicians also need to be aware of AYA needs which is different from other adults and support these needs. We had to change our practice when we started special supportive care clinic for AYA to meet the needs of our patients … Classical palliative care teachings suggest introducing difficult care decisions in the first visit. This may not work well for most young adults. Listen to young adult and understand their concerns. Make the first visit totally about addressing YA concerns (P7)
Other providers need to be aware and motivated to refer their patients to formal palliative care services, as one participant tweeted: Too often gets lumped in with icky language like “giving up” or withdraw of care”—which sucks! It’s another level of care and often an essential one. In practice (most commonly I would see this in heme settings), I would experience clinicians gatekeeping—“not yet”. (P13)
Throughout the X conversation, participants’ comments made clear their perceptions that how palliative care education is offered and healthcare providers supported varies across institutions. Without a supportive and informed care environment, YAs may be missing out on care that could improve their quality of life. The early introduction of palliative care from the healthcare team could be facilitated by supporting and informing these providers, as one participant tweeted: I think there is still significant shame, stigma, and fear here!! From inside and outside of the care team. And often not enough space to take these conversations at a slow and focused pace. Would love to see the language introduced at diagnosis. (P13)
To effect this change, advocates can work to support education initiatives that share with providers patients’ and caregivers’ experiences with these services and equip them with what is known in the extant evidence concerning YA care.
There was a shared understanding that YA cancer advocates have responsibility to effect change for young people living with cancer who are marginalized. Traditionally, YAs are considered marginalized because they often do not receive age-appropriate care. Moving forward and in helping young people with their transition to palliative care, it is imperative that advocacy education efforts be mindful of the multiple ways YAs may be facing discrimination and that advocacy work is considerate of how these intersect. As one advocate tweeted, “It’s hard enough just being an AYA and always fighting to be believed. Then add the layer of being Black or POC and it gets even more difficult because we’re often dealing with bias and microaggressions.” (P21). YA advocacy efforts that are intended to educate for the purposes of equality must not exclude other marginalized populations, as one participant tweeted, “Plus, we must think about the LGBTQIA community. How often are they told about #PalliativeCare and would they be treated with compassion and respect for how they identify?” (P21). In addition to creating anti-racist efforts that are inclusive of all sexual orientations, it is important to recognize that YA cancer is rare and as one participant tweeted, “We know many AYA s receive care outside of big medical centers.” (P24), and efforts must take into consideration their needs in their home communities.
Mobilize Knowledge and Share Stories
Accessing the adult healthcare system requires a great deal of self-advocacy that differs from what is needed for patients who access family-centered pediatric health systems. Underlying the tweets seemed to be a common belief that patients and their caregivers/families are unprepared to advocate for and access palliative care services due to the misinformation and stigma that exists in society surrounding this specialized care. Not knowing what palliative care entails can be distressing to patients who are referred for these services, as one participant tweeted, “Post-cancer, I was diagnosed with #Fibromyalgia and severe #neuropathy. My rheumatologist recommended it AND calmed me down when I initially freaked out thinking it was hospice” (P21). Knowing what palliative care provides can educate and empower patients/families to advocate for these services themselves, but this information is often missing, as one participant stated, “I think many don’t fully understand the difference between palliative care and hospice. Plus, when to even ask for it” (P21). In order for patients to self-advocate for these services, they need to have an understanding of what benefit they would provide and what exists in their area. In general, efforts to normalize talking about palliative care are important, as one patient tweeted, I think just bringing it up is important. I think it’s sometimes the elephant in the room- clinicians can be hesitant to bring it up because they feel patients will think they are giving up and it’s a scary topic. So normalizing pal med services is so vital. (P24)
By mobilizing credible information and creating opportunities for YA community members to discuss palliative care and what it entails, people will become educated on what it is and, in turn, how this normalization will help to destigmatize these services.
While a couple of advocates pointed out that palliative care is not end-of-life care, others emphasized that palliative care can include end-of-life care and efforts to help young people in their transition to these services should be inclusive of the continuum of its care. Sentiments around not focusing on its capability to support patients at end-of-life were rebutted in particular by one participant who tweeted, We also spend a lot of time talking palliative care away from dying but it is a big part of the work! While it is more than dying-deathphobia in our culture is baked in. It leaves us unprepared until we are at our most vulnerable chapter. Talk about death!!!!. (P13)
Another advocate added to this by stating that we should “Provide the opportunities in our personal lives and advocacy lives for AYAs to know that talking about death does not mean it is going to happen sooner” (P2).
Participants commonly voiced throughout the conversation that information for patients/families can be mobilized in a number of ways including at cancer conferences and through other types of knowledge translation activities, sharing sentiments that these efforts should involve co-creation with patients and engagement with a wide public audience. Creative entertainment mediums should also be considered, as one participant tweeted that a podcast could help to spread credible information and another suggested a play: perhaps a funny play written by and for AYAs with cancer about how to discuss palliative care and end-of-life care with themselves and their parents or care partners presented at AYA cancer conferences would help ease this conversation for all involved. (P2)
Whether for the patient or supporters, peer support through sharing experiential stories was commonly noted by participants throughout the conversation as something that could be beneficial to YAs. To better understand which means would be most effective for our advocacy efforts, advocates can push for further research on this YA topic, as one participant tweeted, “I think we need more research on how #AYAs would like this info presented & how we can better support the transition” (P5).
Leverage Technology for Advocacy Efforts
Implicit to the #AYACSM tweet chat seemed to be a valuing of the promise of technologies as tools for both care delivery and advocacy use. In the context of an ongoing global pandemic, many advocates and healthcare providers have had to shift some of their efforts online to continue serving the YA population and addressing their needs, as one participant shared, In many ways, #covid19 forced us to adopt #virtualcare & #telehealth in ways we’d never done before. There are considerations to ensure we don’t exacerbate existing disparities in care but this could be one way to help, especially for people in rural/remote areas. (P5)
Moving forward, advocates should leverage available technology where possible to facilitate the mobilization of credible resources and support efforts, and to address some of the aforementioned socioeconomic barriers. Technology can be used as a medium to deliver pertinent information in a multitude of interactive ways. In fact, the #AYACSM tweet chat is in and of itself a virtual community conversation that would not be possible without leveraging the X platform, as one participant stated, “I think talking about it in forums like this, advocating for more #PalliativeCare supports throughout the illness/treatment trajectory, advocating for ways to improve access & equity (virtual care), sharing stories…” (P5).
One of the new and emerging technological innovations that was referred to several times throughout our conversation was artificial intelligence (AI) and the need for advocates to explore how it can be used to support advocacy efforts. One participant shared, I also think we might see some very slick AI opportunities supporting advocates, patients, partners/parents online support…The data exists. A validated/sponsored AI chat bot can help provide the resources and recommend potential options. Particularly for those not in close proximity for the live bodies in a larger cancer centre. (P9)
An important point for advocates to consider when developing palliative care advocacy efforts for YAs is how technology in and of itself may enable some people to receive information and the support they otherwise would not, but in turn, it can also present barriers for others. As one participant noted, “Nothing like going to the rural library to get computer time to attend cancer Zoom. Access barriers exist in strange & inequitable ways, but I do agree that tech has a big role to play here…” (P15). Of importance to note, throughout the conversation some participants echoed sentiments related to the need of advocates to find balance between using technology to assist patients in their cancer journey and the burden that comes when patients need to rely too much on it to support them in their receipt of care and support.
Discussion
Our community-based research study adds to the tapestry of understanding that the global AYA cancer community is working on to better define what equitable care looks like for young people living with cancer. In particular, our study contributes advocates’ understandings to address the integration of palliative care, an area in the cancer care continuum that is often ignored (Drake et al., 2023; Lockwood et al., 2021). Overall, these themes echo concerns and calls for action in the broader AYA oncology landscape (Canadian Partnership Against Cancer, 2017; Drake et al., 2023; Teplinsky et al., 2022), as well as the need for YA efforts to be inclusive of intersecting social justice issues (Cheung et al., 2021). Our study contributes novel insight into specific areas where advocates can create action for this provision of care in the cancer care continuum.
It is important to explicate that these findings are situated within the sociocultural historical context during which the #AYACSM discussion took place. This event occurred during a global pandemic (World Health Organization, 2024) during which health systems have had to re-strategize and innovate to meet an ever-changing care delivery and patient support landscape (Herzlinger et al., 2023). These events have intersected with other health care-related crises, including both housing and inflation (DeLaire, 2023). These all influence how people speak publicly about important issues related to life and death. Our participants’ perspectives have also been shaped and informed by these events, generating themes that are relevant and reflective of our current healthcare context in North America and the challenges people have recently faced. However, our findings may be timely as we are on the cusp of evaluating how these pandemic-related changes in health care can be sustained moving forward (Herzlinger et al., 2023).
AYAs fall between pediatric and adult health systems, where many YAs are treated alongside patients who are much younger or older than them (Canadian Partnership Against Cancer, 2017). The achievement of important developmental milestones during this period may be impeded, or not realized, due to cancer and the interventions used to treat it (Arnett, 2000; Perez et al., 2020; Zebrack et al., 2016). These challenges all support the need for access to palliative care for this population (Johnston & Rosenberg, 2024), a service our findings highlight is valued by advocates in the YA cancer field. While AYA research has found that palliative care is not consistently integrated into oncology care for AYA patients (Johnston & Rosenberg, 2024), our findings may provide some of the groundwork for a global advocacy strategy to address these gaps in care. Findings from this study contribute to recommendations put forth by Johnston and Rosenberg (2024) who identified ways to support transitions of care as an important research priority in the AYA cancer and palliative care field.
There was contention during our conversation and afterward, as to whether or not advocates should explicitly address in their advocacy efforts how palliative care can be inclusive of end-of-life care. Notably, the provision of palliative care services can include end-of-life care, which provides comfort services to those who are approaching the end of their lives (Marie Curie, 2022). There exist major gaps in research efforts surrounding support for young people in their transition to, and the integration of, palliative care services (Drake et al., 2023), and one could argue that there is even less related to addressing end-of-life for these young people. Therefore, it is imperative, as our findings highlighted, that YA cancer advocacy spans the continuum of cancer care from prevention to end-of-life. Our findings highlight how creative and innovative advocacy approaches could help to address these issues (i.e., through podcasts, plays). Advocates need to work to create action that is anti-racist and inclusive of intersecting social justice issues with our cancer population (Cheung et al., 2021). By not putting forth advocacy efforts that address end-of-life for YAs, advocates may fail to support these people and render our advocacy efforts not inclusive of the entire YA population.
From a community-based research perspective, the act of producing and participating in a tweet chat is community action. The chat offers a time to mobilize credible resources and share thoughts and opinions on unique AYA cancer topics, while also spreading awareness of the unique needs of this cancer population and the challenges that they face. Methodologically, social media comments have been shown to provide rich datasets for reflexive thematic analysis (Braun & Clarke, 2021). The X platform allowed us the opportunity to conduct a chat in a manner that has similar tenets to a focus group. However, probing participants with follow-up questions was different and more challenging, in the sense that tweets could be missed or not responded to in the same way that a focus group discussion would allow. It is also important to highlight the possibility for threads of parallel, intersecting, and diverging discussions to occur on this medium such that this platform requires unique considerations with respect to moderation.
X allows the possibility to conduct community-based research on its platform by its ability for users to share and interact with publicly posted messages in real time. The data collection and engagement of the community with this project has shown the feasibility of using a tweet chat for community-based research. Dynamic #AYACSM conversations can currently take place on X due to users’ ability to search the hashtag and follow the latest posts using it. Our project was possible because our first author co-created and has maintained this community for a number of years, and community members were interested in serving as study team members and/or participants. Academics should consider how they contribute and support communities that they want to work with rather than just accessing them for research purposes. It is unclear whether or not the X platform will continue to exist due to challenges faced by the platform in recent years.
It is important to acknowledge that the content shared during this tweet chat was limited to those who use social media (Cutshall et al., 2020) and presumably felt comfortable participating in a public X conversation about how advocates can support YAs transitioning to palliative care. Having a public conversation is very different from having a private one, and the perceptions people share during online conversations may reflect only what they were comfortable with others knowing so intimately. While the study highlights minimal demographics from those who participated due to the nature of the data collection, it outlines the countries of the community members who participated in the study. Perceptions shared during the conversation may be different from others in differing geographic locations and with varying experiences. However, there may be similar tenets to the themes that were generated not just by other AYA advocates but by advocates of other young terminally ill populations. As the X platform evolves, the language used to explain activity within the platform is gradually changing. The language used in this paper reflects the current terms being used to explain activity on the platform.
Health equity is pertinent to health system quality improvement (Nundy et al., 2022), and in order to enact change, health systems should look at how they can apply innovation to adapt existing resources to support this population. When palliative care teams are involved, AYAs often receive less intensive end-of-life treatments and are less likely to die in intensive care units than those who do not receive palliative care services (Snaman et al., 2017). Yet, the literature has identified that young people may not be offered these services (Lockwood et al., 2021). Through highlighting areas where advocacy efforts are needed to improve care, our study identifies some of the barriers that exist for young people in receiving age-appropriate, person-centered specialized palliative care services from the perspective of a diverse group of YA advocacy community members. When creating equitable and sustainable health care systems, healthcare providers should appreciate the value in engaging and listening to advocates as part of the quintuple aim for healthcare (Nundy et al., 2022; Tyndall, 2023), for their ability to contribute to vital understandings related to health system disparities. It is important to acknowledge, as was mentioned throughout our chat, that advocacy efforts are largely unpaid efforts of those who volunteer their time because they are committed to creating change for YAs. In order for healthcare systems to be sustainable and equitable, gaps in care need to be addressed and not reliant on volunteer work, an unsustainable workforce. Future research in this area can explore and further define what these themes will look like in practice and the barriers/enablers to sustaining these efforts. While our study does not identify individual advocates’ backgrounds and ties to the YA cancer community, this choice may have made it unclear how individuals’ unique backgrounds contributed to our conversation and their own specific advocacy efforts. Further understanding of community members’ experiences with palliative care and YAs who have engaged with these services, could provide more in-depth information that can contribute to our tapestry of understanding around these issues.
Footnotes
Acknowledgments
This original study will contribute toward Emily K. Drake’s doctoral degree. The authors would like to thank members of the #AYACSM community for their support of and participation in this community-based research study.
Author Contributions
This original study will contribute toward Emily K. Drake’s doctoral degree. She contributed to the conception of the study, the development of the study protocol, the development and maintenance of #AYACSM, chat moderation, data collection, and data analysis and led the preparation of the article. L.E.W., M.V.M., D.T., I.R., and J.C. contributed to the conception of the study and the study protocol. All authors provided feedback on the interpretation of the findings and read and approved the final article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Emily Drake owns and operates a consultancy (EmilyDrake.ca). Michael van Manen is a Deputy Editor of Qualitative Health Research. He was not involved in any part of the peer-review process, and the manuscript was subject to the same standard of peer-review as others submitted to the journal. This includes the input of two or more independent peer-reviewers who were blinded to the author’s editorial association with Qualitative Health Research. All other authors report no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Emily K. Drake was supported in this study by doctoral funding from the Killam Trust, the Nova Scotia Research and Innovation Graduate Scholarship, the Canadian Cancer Society, Dalhousie University, and the Beatrice Hunter Cancer Research Institute, with funds provided by the QEII Foundation [grant numbers not applicable].