
Abstract
Because their disease is largely managed in the private environment, people with chronic conditions perform “chronic homework.” The environment with which self-management is coordinated forms a kind of “chronic care infrastructure” in dealing with the disease and, in the case of young adults with chronic conditions (YACCs), is essentially formed by peers. The article investigates how YACCs handle their illness in the context of their peer relationships and how peers see their own role in the context of the YACCs’ self-management. What do chronic homework and chronic care infrastructures look like, if the chronic conditions concern young adults in comparatively unstable and non-committal relationships with their peers? Episodic interviews were conducted with 60 YACCs (with type 1 diabetes, cancer, chronic inflammatory bowel disease, and rare conditions) and 30 peers. The interviews were analyzed using thematic coding. The YACCs’ statements were compared to the peer perspectives on a case-by-case basis. We found that peers differ in the extent to which they seek to monitor or control the YACCs’ self-management. We identified three groups of YACCs: (a) those who focus on their health needs; (b) those who seek to balance their disease management with their need for sociability and belonging; and (c) those who deprioritize their illness in their everyday life in favor of peer acceptance. The multi-perspective approach to YACCs’ and their peers’ experiences with self-management on the one hand and referring to a range of chronic conditions on the other allows to analyze this issue in a complex and comprehensive way.
Background
Chronic conditions are complex, persistent, causally incurable, and associated with functional impairments affecting all areas of life (Whittemore & Dixon, 2008). They are characterized by stable, unstable, and crisis-like phases and accompanied by a variety of coping challenges (Schaeffer & Haslbeck, 2023; Whittemore & Dixon, 2008).
In most cases, the home is the place where people in chronic conditions and their relatives shape their everyday lives and which they often have to adapt for being able to live with the disease permanently and as well as possible (Manderson & Wahlberg, 2020; Wahlberg, 2018). People with chronic conditions and their relatives are trained in the health care system to a certain extent for dealing with their conditions. However, they have to implement the information received during such training courses largely on their own responsibility in everyday life and manage their illness themselves—according to Mattingly et al. (2011), they perform “chronic homework.” Tasks in chronic homework include managing symptoms, treatments, and physical, psychosocial, cultural, and spiritual consequences of the condition, as well as lifestyle changes necessary for living with a chronic disease (cf. Wilkinson & Whitehead, 2009). In addition to these general components of self-management, also disease-specific requirements are associated with the respective chronic diseases (Manderson & Wahlberg, 2020). For example, people with type 1 diabetes need to regularly measure their blood sugar levels, administer insulin, monitor their diet, and engage in physical activity to avoid hypoglycemia or hyperglycemia and (further) serious disease complications (van Vleet & Helgeson, 2020). In general, self-management makes it possible to live with a chronic condition, so it is a basis for “chronic living” understood as: (…) manifold ways in which people attend to, experience, and take care of themselves and their medical conditions often with the indispensable help of loved ones, in differing life conditions and with stratified access to (life-saving) medical treatment and care. (Manderson & Wahlberg, 2020, p. 431)
If chronic conditions are managed at home, it is suggested to establish “chronic care infrastructures” (Langstrup, 2013), which provide a framework for the self-management and the care of the chronically ill and make family care possible in the first place. In this respect, chronic care infrastructures are resources—in the form of certain daily routines, but also medication or in the form of practical care by doctors, nurses, or relatives. The requirements associated with self-management change in the course of the condition. When the disease progresses and there is a threat of a permanent deterioration in quality of life, they become increasingly complex—not only for the patients themselves but also for the care infrastructures (Schaeffer & Haslbeck, 2023; cf. Langstrup, 2013; van Dongen et al., 2020).
Thus, to reconcile the demands of the illness with everyday life represents a particular challenge for many people with chronic conditions. Priorities have to be set, given the limited nature of resources such as time, energy, and support (van Houtum et al., 2015). Just because persons are in chronic conditions does not necessarily mean they will feel “ill,” but symptom-free phases of “conditional health” (Schaeffer & Haslbeck, 2023) can occur. At the same time, the experience of “being ill” becomes familiarized. In that respect, upholding everyday life and its reassuring routines, maintaining contact with peers, and pursuing activities together may be more important than focusing on the condition (van Houtum et al., 2015; see also Arreskov et al., 2021).
As a consequence, living with chronic conditions is characterized by numerous ambivalences and “chronic paradoxes” (Svensson et al., 2020, p. 121) to balance and negotiate as described in studies in medical anthropology. Svensson et al. (2020) have shown in their review that children and adolescents with coronary heart disease often want others to know about their disease but, at the same time, also that they don’t. The children and adolescents thus navigate through a “paradox of (non-)disclosure” (Svensson et al., 2020, p. 127) in order to avoid negative social reactions. For young adults with cystic fibrosis, Knudsen et al. (2018) also illustrate the ambivalence of their participants: The authors describe the young adults in a tension between the constraints imposed on them by their disease and treatment management and their individual striving for “freedom” and autonomous decisions. If ill persons fear that their health will deteriorate in the future despite the strenuous, time-consuming treatment, this can contribute to their desire to live in the here and now and to see friends or work as more important than the treatment. For chronically ill children and adolescents, Bagge-Petersen (2023) shows how they live the ambivalence between “differentness and normality” (p. 192): In interactions with non-ill peers, the children and adolescents try to demonstrate their “normality” and “coolness.” In other situations, for example, when they are with people who are also ill, they focus on their conditions and exchange information about treatment management (Bagge-Petersen, 2023).
Self-Management and Illness Perspectives
The existing research also indicates that self-management is framed by the subjective experience of illness and the meaning(s) attributed to it. The experience of the illness is in turn influenced by illness perspectives, including the individual’s attitudes, beliefs, and values relating to living with the illness (Audulv et al., 2011; Paterson, 2001). Paterson’s “Shifting Perspectives Model” (2001) suggests that every person with a chronic condition has a dominant illness perspective, which may change repeatedly over time (e.g., if the condition worsens or stabilizes for a time). The “illness-in-the-foreground” perspective focuses on aspects of suffering, loss, destructivity, and (illness) burden. Individuals who adopt a “wellness-in-the-foreground” perspective typically succeed in maintaining an emotional distance to their illness that permits them to (re)gain control over their life (Paterson, 2001, p. 23).
In subsequent studies, Paterson’s model was refined, for example, by relating the disease perspectives identified by Paterson (2001) to self-management: Individuals with a “disease-oriented illness perspective” (Audulv et al., 2011, p. 115) focus on symptom management in the sense of adhering to treatment and medication recommendations and adapting their lifestyle. Those with a “life-oriented illness perspective” (Audulv et al., 2011) seek to limit the impact of the illness on their daily life and to remain positive despite the difficulties it causes. Based on Paterson’s model, Robinson (2017) has analyzed how shifting the perspective from “illness” to “wellness”-in-the-foreground works and how the chronically ill develop the skills necessary for such a shift.
Chronic Conditions in Young Adulthood
Chronic conditions can occur at any stage of life. They are increasingly prevalent in childhood, adolescence, and young adulthood (Wilson et al., 2021) with varying challenges. Young adults with chronic conditions (YACCs) face the challenge of taking responsibility for their own disease management, for which their parents had previously been responsible (Lerch & Thrane, 2019; Monaghan et al., 2015). This task comes on top of the many transitions and changes that all young adults have to cope with, for example, moving from school to training or higher education and on to the labor market. This dual burden often proves too much for YACCs and is associated with an elevated risk of complications (Monaghan et al., 2015; Wood et al., 2018).
As Arnett (2024) shows, “emerging adulthood”—the age between 18 and 29—is characterized by restructuring social relationships: Needs for emotional closeness, companionship, and support are less and less satisfied by family members but by friends and romantic partners. Friends are especially important for the well-being of young adults living alone. When close family relationships are absent and young adults have not yet entered into long-term romantic relationships, friends can become a “family of choice” (Takasaki, 2017). However, mutual closeness and support decrease when young adults are married or committed to a romantic partner (Galambos et al., 2018).
If friends or romantic partners are relevant parts of young adults’ social environments, what is their importance in the context of self-management (van Vleet & Helgeson, 2020) and how do they fit into YACCs’ chronic care infrastructures (Langstrup, 2013)?
These questions become even more relevant as—according to Wiebe et al. (2018)—it is unclear whether the effect of involvement of friends in the management of conditions like type 1 diabetes is more positive or negative. Their literature review found that the negative effect of conflictual peer relationships can outweigh the “helpful” effect of support from friends. While friends may offer genuine support in relation to chronic conditions, this may still be experienced negatively by the recipient, for example, if they feel their autonomy is diminished or they fear being a burden on their friends (Kelly & Berg, 2021; Mattacola, 2020; Wright et al., 2021). Peers also influence self-management indirectly. YACCs who orient strongly on peers and their norms (which tends to apply more to young men than young women) may neglect illness-related demands (Raymaekers et al., 2017).
Prior Research on Self-Management in Social Contexts
When studies on self-management and informal support are pursued, they primarily refer to kinship or partnership relationships (Pleschberger et al., 2019). They focus on caregiving relationships in old age or parent–child relationships (Bagge-Petersen, 2023; Bagge-Petersen et al., 2020; Bluebond-Langner, 1996) in chronic conditions, that is, on relationships characterized by dependencies. These studies show that care and nursing activities require a high degree of intimacy and closeness, as well as strong emotional ties (Fihel et al., 2022). How far can these findings be transferred to disease-related self-management in close but informal relationships, for example, peer relationships, which, in young adulthood, are characterized by instability and non-commitment (Nelson, 2021)? Many YACCs fear to lose friends or partners if they confront them with sensitive issues such as illness-related burdens (Rabin, 2019) or if they disclose their support needs, thus violating the implicit expectation of reciprocity of support exchanges in friendships (Bredewold et al., 2020).
When studies address self-management by adolescents or young adults in the context of peer relationships at all, they tend to be quantitative investigations seeking to identify psychological and/or biomedical outcomes (well-being; glycemic control) associated with supportive or conflictual peer relationships (Helgeson et al., 2023; van Vleet & Helgeson, 2020; Wiebe et al., 2018). Questions which remain open in this research are, for example: What does it mean for young adults to manage their disease and to coordinate this management with peers in daily life? How do peers describe themselves in the context of YACCs’ self-management? What do chronic homework and chronic care infrastructures look like, if the chronic conditions concern young adults in comparatively unstable and non-committal relationships with their peers? What might be different from findings concerning older adults in chronic conditions needing care or from children and adolescents involved in close relationships with their caregivers? As many of the studies discussed here focus on one chronic condition (among the few exceptions: Langstrup, 2013), what might a comparative approach to different chronic conditions in everyday life with peers reveal? What is the relevance of peers within chronic (care) infrastructures with a focus not only on “care” but on everyday living with chronic conditions? These questions are addressed in the research reported here.
Materials and Methods
Background and Research Design
Our study began in October 2021 and is funded by the German Research Foundation for 6 years. It seeks to understand how YACCs manage their conditions in the contexts of daily life and peer relationships. It examines both YACCs’ own perspectives and those of their peers (friends and romantic partners). The research builds on theories from medical sociology and nursing science and is based on the theory of social representations (Moscovici, 1973; cf. Flick, 1998). This approach addresses the ways social groups hold differing ideas about a particular topic and how particular circumstances of daily life and sources of knowledge influence these ideas in daily life. In the context of the present article, that would include the ways in which YACCs in differing chronic conditions and their peers develop group-specific ideas about the social and everyday influences and framings underlying self-management and life with chronic conditions.
This article discusses self-management in the context of peer relationships and everyday life which is one of the research questions of our study and addresses the following issues in particular: 1. How do young adults balance the demands of their condition against their everyday needs and social life, and what illness perspectives does this reflect? 2. How do they negotiate their self-management specifically in relation to peer relationships? What roles do peers play, and what functions do they serve in the context of self-management? 3. What role(s) do peers attribute to themselves in the context of YACCs’ disease management? 4. When comparing the YACCs’ statements with those of their peers, which additions, overlaps, or contradictions emerge?
In the first step, we included YACCs in the study, when they mentioned to be affected by one of the following chronic diseases, which were selected to provide breadth and contrast in terms of experiences and needs: • Cancer, for which declining mortality rates are also reported in young adulthood (Close et al., 2019), but this means that there is an intensive treatment period of around 2 years or more, followed by surveillance checks, as there is a risk of relapse and young adults also have to deal with the after-effects of treatment, which can become chronic. • Type 1 diabetes as a lifelong condition that requires constant disease management and can be associated with potentially life-threatening complications (e.g., hypo- or hyperglycemia) (van Vleet & Helgeson, 2020). • Inflammatory bowel disease (ulcerative colitis or Crohn’s disease)—intermittent or permanent inflammatory diseases, primarily of the bowel, that are mainly associated with abdominal pain and diarrhea. Bowel diseases can trigger negative emotions such as fear, shame, anger, and disgust in those affected (Polak et al., 2020). • Complex rare diseases (RDs) with unfavorable and/or unpredictable prognoses, such as cystic fibrosis and terminal renal failure.
For being able to compare and contrast the YACCs’ perspectives with those of their peers, we asked YACCs to suggest a close friend or their romantic partners for being interviewed (see below).
Field Access and Sampling Strategies
The empirical part of the study coincided with the ongoing COVID-19 pandemic. So, we could seek field access only on digital ways for infection protection. We applied several forms of purposive sampling suggested by Patton (2015): The chronic conditions (see above) were selected according to “intensity sampling” (2015, p. 267) referring to the features and more or less severe impact of the conditions on YACCs’ everyday lives. For accessing YACCs with these chronic conditions for interviews, we approached “key informants” (2015, p. 268) and applied convenience sampling within the condition groups. We asked the YACCs to suggest one or more of their peers for being interviewed and thus applied “respondent-driven” and “link-tracing sampling” (2015, p. 299). We tried to contact YACCs via social media. Young adults who blog about their illness experiences were contacted and informed about the study and invited to participate. For attracting young adults to participate in research, online recruitment strategies are suggested (Jong et al., 2023). However, none of the YACCs we contacted via Facebook or Instagram were willing to participate in our study.
Thus, we also searched contact with eligible YACCs through relevant self-help groups, patients’ organizations, advice centers (rehabilitation), clinics, and projects. Relevant decision-makers in these groups and institutions were informed about the study and asked to forward information about the study on their websites or directly (via social media) to YACCs. We also wrote to the student councils at selected universities asking them to circulate information about the study to students.
All in all, we contacted 91 gate keepers from institutions, organizations, and councils of whom 16 informed us that they had forwarded our invitation to potential interviewees. The gate keepers who work in the health care system or self-help organizations have access to young adults with cancer, diabetes, IBD, or RDs and thus cover the range of fields and diseases we wanted to include in our sample. Interested YACCs were individually informed again about the study for clarifying any questions they had.
Sample
Sample-YACCs: Age, Gender, and Condition.
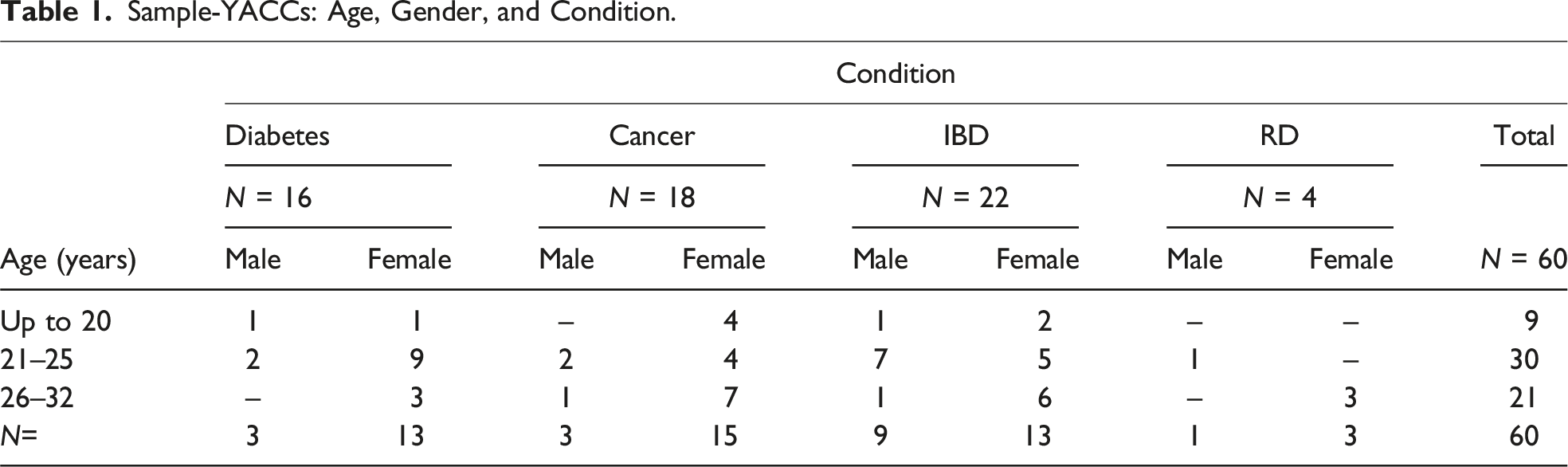
The sample of the YACCs is diverse in two respects: the included chronic conditions and the degrees of severity in the condition. Among the N = 16 young adults with diabetes, N = 12 participants’ disease is well controlled, whereas N = 4 participants mentioned that they suffer from fluctuations in their blood sugar levels and have already experienced severe metabolic derailments. Of the (N = 22) YACCs with IBD, N = 8 participants reported a largely stable course of the disease for a long time. N = 14 YACCs with IBD described frequent severe relapses as well as severe complications of the condition (multiple intestinal obstructions; acute renal failure; sepsis; massive intestinal bleeding; and colectomy). Among the (N = 18) young adults with cancer, N = 5 respondents described their condition as cured with only few remaining complications. N = 13 interviewees referred to severe treatment complications (e.g., limb amputations and chronic pain), suspected recurrence, or the presence of metastases. All YACCs with rare and complex diseases (N = 4) see themselves at risk that their condition might worsen with a potentially fatal outcome. At the time of the interview, more than half the YACCs (N = 37) were university students. Thirteen were working, three were in vocational training, four were unemployed, and three were on permanent sick leave.
Sample-Peers: Age and Gender.
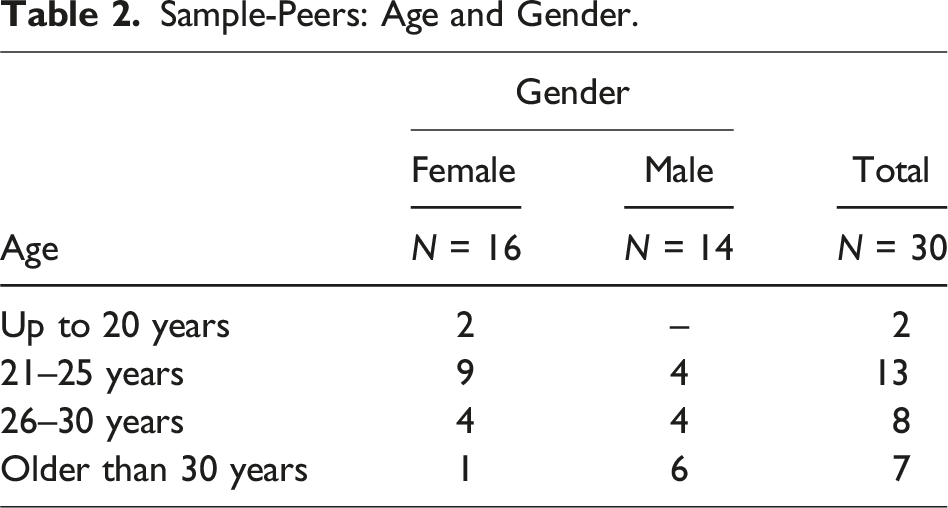
At the time of the interview, many of the peers (N = 24) were studying or had already graduated from university.
Data Gathering
In both groups (YACCs and peers), we collected the data in episodic interviews (Flick, 2022). Here, respondents are invited to recount specific situations (e.g., of learning about their condition being chronic) and asked concrete, directed questions (e.g., “What do you link to the concept of chronic illness?”).
The interviews with YACCs lasted between 51 and 109 min (mean 75 min). The interview guide covers experience of the illness, disclosure, self-management, social support, relationships and the illness, and representations of friendship (see Annex 1 in the Supplemental Material: Selected questions from the interview guide).
The interviews with peers lasted between 23 and 85 min (mean 45 min). The interview guide focused on the peer’s experience and understanding of the condition, its effects on relationships, social support, personal boundaries, prior experience with chronic conditions, and the meaning of friendship.
Most interviews were conducted online using Webex, and a small number of participants preferred to be interviewed by telephone. Online interviewing allowed to extend recruitment and data collection across the whole country. This not only reduced travel costs for the researchers but also saved the interviewees from traveling. Many of them talked about meeting peers online or attending online teaching so that they were familiar with communicating this way.
At the end of each interview, we asked the interviewees how they felt. We asked this question for some kind of ethical care for the participants. We wanted to give them a space to mention any kind of unease with the interview, negative feelings recounting stressful illness, and any memories of critical situations it evoked related to the illness. This might have given us the chance to support the interviewee with active listening and, in case of a (very) emotional response, to reflect together about how to deal with it and perhaps suggest professional support the interviewee could turn to. During the interviews, the young adults only seldom reacted very emotionally. For example, a male interviewee spoke repeatedly and emphatically about his consternation about his former partner having abandoned him because of a severe illness episode some time ago. He also mentioned thinking about suicide at that time, but in the interview, he said that this was no longer the case. The interviewer gave some space for talking about this issue. Some interviewees mentioned cathartic effects (cf. Silverio et al., 2022) and that they could talk about sensitive topics they rarely speak about in their everyday lives. Young adults also mentioned that our questions were ones they had asked themselves anyway, while others said that the interview was the first time they had been confronted with certain questions. They saw this as an opportunity to see the chronic condition with new eyes.
Data Analysis
The interviews were transcribed in full, anonymized, and analyzed with thematic coding (Flick, 2022) supported by MAXQDA software. The interviews with YACCs and peers addressed slightly different questions, leading to differences in the analytic strategies. In this article, we focus on the concept of self-management although YACCs did not use the term “self-management.” Building on Wilkinson and Whitehead’s (2009) definition in our analysis, we identified aspects of self-management when the interviewees described how they dealt with symptoms, treatments, and physical, psychosocial, cultural, or spiritual consequences and which changes in their ways of living resulted. The following statement of one of our interviewees, Wilma, shall illustrate the comprehensive understanding of self-management we use for the current article: (…) I pushed through my studies with some difficulties (…) the better choice, for example, than an apprenticeship (…) because I could arrange my times in a way I could accomplish, at that point I wouldn’t have been able to go to work forty hours. (Wilma,
1
29, IBD, 2008)
Our understanding of “self-management” comprises more than merely disease management aiming at avoiding or treating symptoms. We do not downscale self-management to issues of compliance to regimes of medications or other treatments and thus not to a “good” or “bad” disease management (Franklin et al., 2023).
Analysis of the interviews with YACCs began with case-by-case thematic coding (Flick, 2022) of statements on the above aspects of “self-management.” Comparative dimensions were defined across cases for finding similarities and differences. Cases were grouped along these dimensions and analyzed for specific combinations of features. Contrasting cases allowed comparing the cases in one group for similarities and comparing cases across the groups for differences among them.
In the analysis of interviews with peers, we used the interview guide as a basis for creating more deductive, keyword-style (top-level) categories, to which the interview material was initially assigned. Then open coding was applied oriented on the coding paradigm Strauss (1987, pp. 28–29) and Corbin and Strauss (2008, p. 89) suggested (coding for “conditions,” “interactions/emotions,” “strategies/tactics,” and “consequences”). This involved applying sensitizing questions (How …? Why …? etc.) to the text and creating inductive sub-categories. Then the cases within each sub-category were compared to arrive at a generalizable thematic structure (cf. Flick, 2022). Subsequently, the categories relevant for the present article were analyzed in detail for interpreting the meanings of text passages. Finally, we compared the YACCs’ and peers’ perspectives on self-management in social contexts.
Findings
Self-Management and Relationships
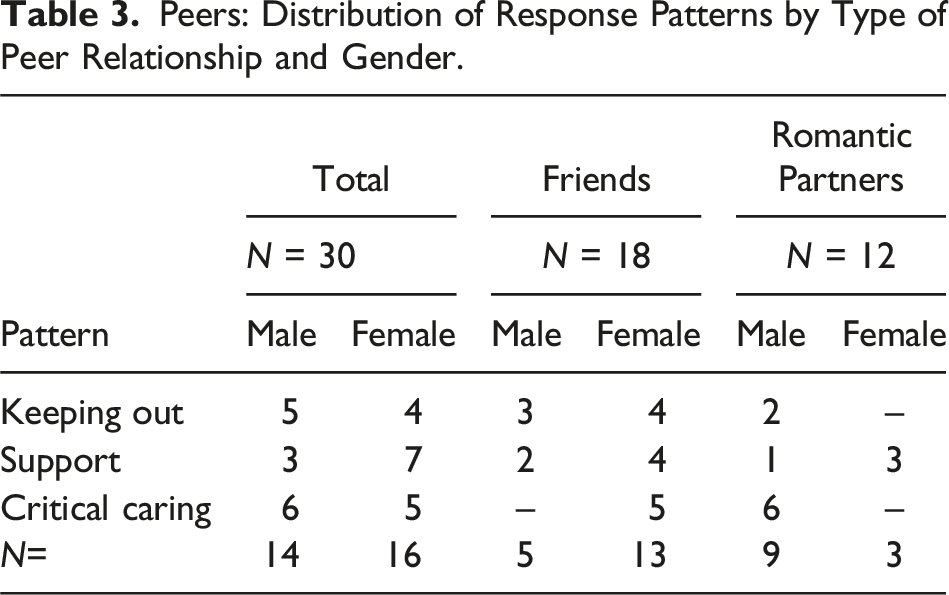
Peers: Distribution of Response Patterns by Type of Peer Relationship and Gender.
Peers’ Perspectives
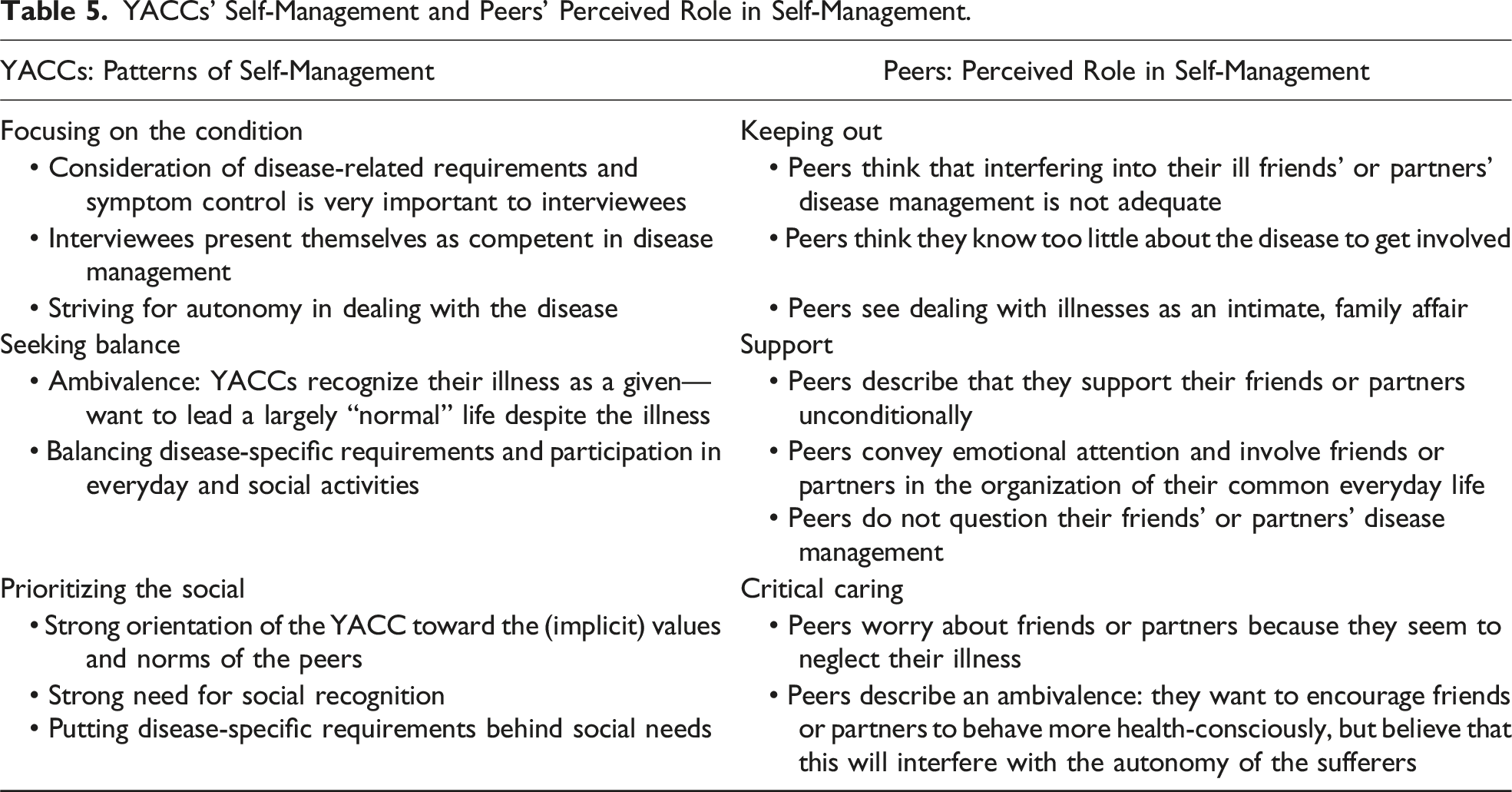
Keeping Out
A first group of peers describe themselves as keeping out of the YACC’s disease management. They do not think they have any right to interfere in the illness. Instead, they regard illness and disease management as very intimate matters that concern nobody but the YACCs and their families. These peers also indicate that they knew relatively little about the illness and therefore felt unqualified to get involved in YACCs’ disease management or to comment on how they handle their illness. They also tend not to comment if they notice that specific therapeutic recommendations are ignored.
Support
Peers in a second group indicate their very close relationship with the YACC and that they support them unconditionally, above all emotionally. These interviewees describe trying to treat the YACC as “normally” as possible. They also include the YACC in their daily lives and routines and feel it is important to show consideration for the YACC’s specific health needs. Spending a lot of time together and seeing themselves as empathetic and attentive, they believe they can understand the YACC very well. These interviewees also indicate that they did not question the other’s disease management but thought that the YACCs were paying close attention to their condition and observing the demands of the illness.
Critical Caring
Peers in the third group also report having a very close relationship with the YACC. They notice the special challenges the chronic condition creates in their daily lives. But these peers also report that the YACCs often neglected their illness-related needs. They reported feeling uncertain how they should react when they felt the disease management was inadequate. These peers—who tend to be mostly male romantic partners—either try to control how the YACCs deal with their condition or they talk to them and convince them to be more considerate of their condition. Trying to persuade YACCs to pay more attention to the demands of the illness comes with fears of endangering the relationship if the peers insisted on particular behaviors.
YACCs’ Perspectives
YACCs: Distribution of Self-Management Patterns by Illness and Gender.
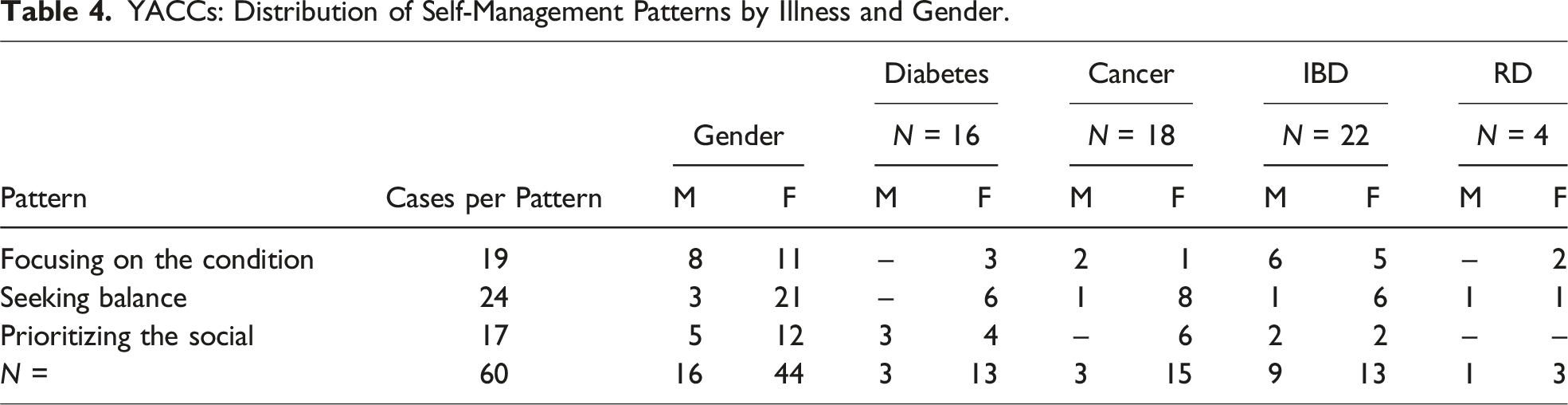
The peers’ self-perceptions discussed above are linked to the patterns of self-management in exemplary cases. These juxtapositions reveal shared and differing social representations of self-management of chronic conditions.
Focusing on the Condition
A first group of YACCs describe how they are intensively concerned with their condition as well as treatment options and therapeutic recommendations. They search for information about their condition on the Internet, read studies on it, and exchange ideas with other YACCs. The interviewees focus on their condition and underline that they are actively involved in the treatment process and try to shape it by making decisions for or against specific therapies. Their descriptions show that they were already confronted with many—prognostic—uncertainties and existential questions during the course of their condition. They appreciate the emotional support of peers who listen in the face of stress and strains. But interviewees such as Leonore, who was born with renal insufficiency and received a kidney transplant as a teenager, also describe that they do not discuss such intimate topics as the finality of their own situation with “healthy” peers but with relatives or peers who are also ill. I sat down with my sister and said, “I’d like to talk to you about what if something happens to me” (…) what do I wish even if I’m gone? For me, these are things that accompany me as a matter of course, and that (…) are often incomprehensible to people my age. (Leonore, 27, terminal renal failure, lifelong)
Leonore and other YACCs who focus on their condition emphasize how important it is for them to take into account disease-specific requirements (e.g., taking medication according to dosage instructions) and needs (e.g., for rest) in everyday life. They tend to prioritize these requirements even when peers try to include them in social activities such as eating out, cinema, game nights, or excursions. Where possible, they try to find compromises in such situations. But they are aware that neglecting the demands of their conditions will lead to an “unnecessary” worsening of symptoms—or even to long-term complications. These interviewees appear to expect their peers to accept their reasons for intermittent absence from social activities or routines. And they do not alter their priorities if peers fail to show understanding. They also resist their peers giving them advice about how to deal with their condition or trying to interfere in their treatments. Fabienne, for example, considers her friend’s self-perception of being an essential source of support to be presumptuous given her cancer’s severity. … so, when I had problems, she [friend] always said “We can manage, we can do it.” But at some point, I noticed,
Fabienne’s view that peers can only provide her with marginal support is formally reflected in the fact that she did not arrange the contact to a peer to interview. In particular, in acute phases of their illness, interviewees focusing on their conditions tend to withdraw from their social networks anyway as they are preoccupied with illness-specific issues. During such acute episodes, they lack the energy to meet peers—but they also assume that their peers would not understand how they are feeling anyway. Instead, they rely only on their parents and their closest peers. There are phases when they are forced to depend on those individuals for their everyday needs (e.g., housework). Such experiences are often associated with shame. When they are being “cared for” by peers, they feel prematurely aged or—as in the case of Elias—that their sense of masculinity is undermined: For example, she [his partner] does all my shopping now. I’m not allowed to lift more than five kilograms, so it’s hard to do the shopping. So now she does it for me, for two years now [laughs]. (Elias, 24, IBD, 2018)
Interviewees like Elias also emphasize that it is a shame for them to accept support from peers who they consider inexperienced in illness-related matters. Although the interviewees in this group appeared not to doubt that their peers were well-meaning when they offer practical assistance or emotional support, they still said it was difficult to reject support; ultimately, they did not want to annoy their peers. By communicating to them that they want to take care of their own affairs as far as possible, they are seeking to retain autonomy and control over their situation.
These YACCs’ peers, who describe themselves as supportive and empathetic, are aware of the YACCs’ conflict between wanting to maintain autonomy and needing help. These peers are trying to leave the “solution” of this conflict to the YACCs. Elias’ partner Luna, for example, also clarifies that for her there are situations in which the support of her partner is absolutely necessary. In any case, I know that he wants to do a lot of things on his own and doesn’t want to be pitied, but when I see that he somehow needs help or, yes, doesn’t look so good physically, then I intervene at the latest. (Luna, 24)
As Luna explains later in the interview, her “intervention” means to arrange a hospital treatment for Elias. That the boundaries between support and a more directive “critical care” described by peers can be blurred has been repeatedly elucidated in our interviews. YACCs, who present themselves as very focused on their condition and as self-responsible in their self-management, can reject such care. In the following example, Greta, after describing the exact system of controlling blood glucose she has developed during her life with diabetes, illustrates what she sees as a patronizing attempt by her partner to control her diabetes management: My boyfriend does such nice things as packing my blueberry portions deep into pots so I don’t finish the whole package at once (…) where I say “Yes, I know that I’m eating too much right now” (…) then, at first, he somehow says again something like “Are you sure?” And if I look at him badly enough, then he lets me do it. Because then I said, “I'm big enough myself. I have to make the decision myself.” (Greta, 30, diabetes, 1996)
When interviewees like Greta reject their partners’ attempts to support them, the partners may perceive this as hurtful and embarrassing. In order to deal with feeling rejected and to defuse the situation, Dominik, Greta’s partner, describes how he tries to objectify the negotiation of diabetes management without going to the personal level. Then I somehow get very clear feedback like, “It’s nice that you’re thinking along, but now it’s not time to think” (…) but then I can also frame it like this and say: Okay, that’s a hypoglycemia, it has nothing to do with me personally, but the body is running on an emergency program. (Dominik, 35)
All in all, the YACCs focusing on their condition feel it is important to have their condition as far as possible under control. In their everyday dealings with it, they rely above all on themselves. They see themselves as experts for their own health matters who know best what is good for them. Among these YACCs, we find a comparatively high proportion of male respondents. Some of them are rather critical about their peers’ roles. The peers mentioned or quoted here can be assigned to the various groups of peers’ perspectives mentioned above.
Seeking Balance
YACCs in the second group also acquired knowledge about their condition that fed into confidence-building routines. They describe themselves in an ambivalence between wanting to maintain control about the course of their conditions and at the same time to lead widely “normal” lives like “healthy” peers. They know how they need to act and what they need to pay attention to if they want to stay (more or less) well. Therefore, from their point of view, dealing with their condition no longer takes up much space. They relativize the subjective importance of it to a point where it “… just follows me through life like a little extra bit of me. It was a much bigger thing at the beginning of course” (Jana, 23, diabetes, 2008).
When interviewees like Jana think that they are hardly affected by the disease anymore because they have lived with it since childhood, they implicitly convey this view to their peers as well. Klara, for example, clarifies in the interview how she can calmly stay out of her friend Jana’s disease management, since Jana seems to know how to deal with diabetes. She’s super independent. She knows her stuff very well. And I don’t need any help from me. (Klara, 23)
YACCs who, like Jana just mentioned, are looking for a balance, describe in the interview that their everyday life is mainly filled with studies, training, or even their first job. They feel it is important to be able to keep up in that context despite their condition. Even during phases of escalation, they often try to use the moments when they feel better to participate, for example, to attend lectures. As Zoe illustrates, these interviewees see such efforts as proof that they are not giving up despite the seriousness of their condition: They generate structure and orientation, supply emotional support, and strengthen their confidence that there is a “normal” life outside of their illness: When I was lying in bed and listening to a lecture … sometimes I was in so much pain … then I couldn’t listen any more. That gave me some kind of motivation, helped me through it a bit, because I knew life will go on … once the chemo is over. (Zoe, 26, Hodgkin’s lymphoma, 2020)
Zoe and other YACCs in this group see their efforts of balancing the demands of their condition with their everyday activities and social life as also characterizing their peer relationships. They underline how important it is that their peers acknowledge their special health needs. They feel noticed and appreciated when peers include them in the planning of leisure activities and insist on taking their current health status into account. But they also want to be treated by their peers as if they were not seriously ill at all, especially in more stable phases. In particular, if they have been confronted with many complications during their long course of illness like Claudia, they tend to avoid mentioning the illness to peers at all: We don’t make it the main topic at every meeting and then just sit around sadly on the bed. (Claudia, 18, IBD, 2009)
Claudia and other interviewees seeking balance try to keep the effects of their condition on leisure time spent with peers to a minimum. This may involve temporarily neglecting specific needs linked to their condition, testing their own limits, and their willingness to bear physical discomfort. With acting in such a way, these YACCs also achieve that peers, such as Claudia’s friend Vera, stay out of disease management and limit themselves to providing distraction and emotional support. An outsider doesn’t know one-to-one how the other person feels, what exactly they have to go through now. And at the end of the day, it’s always like, “Yes, it will work out again.” (Vera, 18)
However, the aforementioned Claudia and other YACCs seeking balance also show that they carefully ponder the risks of neglecting therapeutic recommendations for a short time. They want to avoid any uncontrolled escalation of their illness.
Peers affected by the same condition play an ambivalent role for the YACCs, as in the case of Katharina. She has been hospitalized many times and is now confronted with the fact that she should receive an ostomy. She mentions that she feels better understood by people who are also ill than by other peers, but also says she worried that relationships with other YACCs could define her as marginal and different. She describes how she was reduced to her illness by her “healthy” peers and gradually lost contact with them: So really you just want to be as normal as the others, but at the same time you aren’t. You see, that’s the stupid discrepancy you have to live with. Of course, it’s also important to have people who can understand that, but somehow you don’t want to hang around with people who have the same problem all the time. (Katharina, 23, IBD, 2011)
YACCs describe ambivalences not only when weighing up disease-specific requirements against everyday obligations or social needs but also when dealing with possible treatment alternatives. Seriously ill YACCs like Katharina or Friederike emphasize that they want to be actively involved in medical decisions about their further treatment and are potentially prepared to reject planned therapies. In the interviews, they mention that they are aware of the negative consequences of their treatment decisions. If, facing a possible unfavorable prognosis, Friederike considers not undergoing chemotherapy again, she would be choosing a path from which she hopes to preserve her autonomy and dignity. If I were to get sick again, I wouldn’t know if I would get treatment again (…) I would have to rethink in any case (…) it gave me back a lot of security at the time, when I realized that it is still my body and I can decide whether to do it or not. (Friederike, 24, ovarian cancer, 2017)
In the interview, peers mention strong uncertainty when they are confronted with existential decisions of the YACCs, such as the possible rejection of treatment. Inka, who as a friend sees a supportive role for herself in Friederike’s self-management, describes incomprehension, sadness, and helplessness in the face of the idea of ultimately having to accept Friederike’s treatment decision. What pushes me to the limit is when she says something like “Yes, if this happens again, I won’t do chemotherapy anymore” (…) you can’t force her, but somehow you want to force her, you don’t want her to just give up, so to speak, and ultimately die. (Inka, 23)
The YACCs in this group acknowledge their illness and the associated demands as relevant to their behavior. But they also seek to participate fully in everyday activities and social life. Among the balance-seeking YACCs, we find a relatively high proportion of female participants in the study. Their peers react in different ways—by keeping out, as Vera, or ambivalent and unsettled, as Inka.
Prioritizing the Social
Different from the aforementioned groups, for the YACCs in the third group, peer recognition comes first. To that end, they participate in social activities, describe themselves as engaged and dependable, and thus signalize their feeling of belonging to the peer networks. What is necessary for their conditions appears secondary or even negligible. Indeed, ignoring them can serve to demonstrate personal commitment to the group. For example, Justus says: … at handball. I knew I should never have done sports, [blood sugar] level: disaster. But I, as the only goalkeeper, said: “Okay, no, there’s no other way. I’ll put myself in goal anyway ….” (Justus, 21, diabetes, 2005)
Another reason for Justus and other interviewees who prioritize social issues to ignore their condition is to avoid being a burden on their peers. They consider it as disproportionate to expect peers to be considerate for them for their condition. By taking a step back for the sake of their friends, the YACCs in turn demonstrate how social they are and can thus expect recognition in turn.
Some YACCs were ashamed of their condition and only discussed it with their very closest friends. They described their implicit fear that friendships could suffer or even end if they were to focus on their condition in their daily life. Also, because they do not want to be seen as different by peers and reduced to their illness, these YACCs refrain from making use of social support. In the following example, Ina illustrates how, especially in the presence of peers, she tends to disregard disease-specific requirements such as certain diets. Sometimes I have days or phases (…) when I think I don’t want this illness having anything to do with me (…) and if people say “Well, can we do anything special for you?”, sometimes, I think then “Nah, I just don’t want to be treated differently at all and now I’d just like a great big slice of cake or a plate of greasy chips.” (Ina, 25, IBD, 2018)
Ina and other YACCs who prioritize social relations highlight that they rarely deal with their condition. Some find it hard to acknowledge that it is chronical at all. Instead of making timely medical appointments, they accept the complications caused by postponing these. A few also relied on homeopathic remedies and tried to treat their symptoms independently without therapeutic guidance.
Peers often describe incomprehension when they find out that the YACCs seem to neglect their health needs. When peers are close to the YACCs, like Jenny is to her friend Ina, they try to convey to them that they stand by them, even or in particular when they are (especially) unwell. Jenny emphasizes that through her emotional attention, she hopes to encourage Ina to be more mindful of her illness and to no longer hide illness-related needs. That’s something I try to make very clear to her, that she’s allowed to complain, that she’s allowed to talk about it, that it’s just stupid sometimes and that she’s not doing well and that she doesn’t always have to be a fighter. (Jenny, 26)
YACCs prioritizing social issues often seemed to rely on health information shared by others or coming from lay and popular sources. In this context, they (unknowingly) take risks that their condition becomes worse, as the example of Jonah shows, who has only been suffering from Crohn’s disease for less than a year at the time of the interview. Whisky-Cola also helps, I notice, or whisky in general. You often hear that it is supposed to be good for digestion in the short term, because it has this corrosive quality again (…) then I just drink something like that. (Jonah, 20, IBD, 2021)
Some YACCs prioritizing social issues over their conditions demonstrate an altruistic attitude in relationships with peers as well as family members by playing down their own needs. This applied more to women, and specifically female cancer patients. They tend to feel that they are less affected by their condition than their closest contacts (family or peers). Isabell demonstrates how concern for friends and family can become (in some respects) a greater burden than the condition itself: I’ve always tried not to make it so difficult for my parents (…) I didn’t think it was so bad to be sick, but I thought, “How bad must it be for parents to be afraid for their own child?” (Isabell, 29, Hodgkin’s lymphoma, 2016)
If interviewees like Isabell have peers who are also in a chronic condition, they seem less likely to expect to benefit themselves from the exchange with those peers. Rather, it seems important to them, as well as to their partners with whom they “get through” the condition, to share experiences in order to support those who are facing similar challenges in the process. Oskar, Isabell’s partner, mentions: (…) that she was very happy with how her family and how I dealt with her during that time. Maybe you can convey that to others who are going through something similar. (Oskar, 31)
To sum up, the YACCs in this group prioritize social life over the demands of the illness. As the interviews show, this is often driven by a strong orientation on their peers’ expectations, values, and (implicit) norms. The YACCs present themselves as “normal,” for example, by honoring their commitments (such as training or university) despite their chronic condition. Their peers (those we interviewed or the YACCs talked about) sometimes react with incomprehension or—if they are ill themselves—with a special form of understanding.
Comparing YACCs’ and Peers’ Views of Self-Management and Relationships
YACCs’ Self-Management and Peers’ Perceived Role in Self-Management.
Discussion
We studied how YACCs try to manage their condition in everyday life and what challenges they face when trying to do the “chronic homework” (Mattingly et al., 2011) with their peers that results from considering disease-specific requirements. Our study also explored on how peers perceive disease management and what role(s) they attribute to themselves.
How YACCs describe their self-management can be ordered as a continuum (cf. Kjærulff et al., 2024), extending from prioritization of disease management, through attempts to balance it with everyday commitments, to neglect of health concerns in favor of social needs. In particular, YACCs who attempt to reconcile disease-specific requirements with everyday obligations and social needs describe a number of paradoxes and ambivalences that have also been found in comparable studies (Bagge-Petersen, 2023; Knudsen et al., 2018; Svensson et al., 2020). For example, they assume that peers with chronic conditions have more understanding for them than non-sick people, but at the same time, they fear being reduced to their illness through relationships with other YACCs. The contrasting expectation that peers recognize (former or ongoing) disease-related stress experience, but at the same time treat the YACC like anyone else, is found primarily in cancer patients (cf. Andrés-Jensen et al., 2020), but also in young adults with one of the other diseases included in our study. YACCs also show ambivalences with regard to therapy decisions. In addition to their own ambivalences, there may be those of peers who want to persuade YACCs to undergo certain treatments but suspect that they are interfering in their personal decisions.
Our results show that peers are an essential part of the YACCs’ “chronic care infrastructure” (Langstrup, 2013) and deal with their illness, albeit with varying intensity. In acute phases of the condition as well as in very personal issues, YACCs above all exchange ideas with very close peers with a chronic condition as well and whose support they accept. Similar to studies with chronically ill children and adolescents (Bagge-Petersen et al., 2020; Bluebond-Langner, 1996) or with the elderly in need of care (Fihel et al., 2022), we found that support and care take place within relationships determined by great closeness and also dependence. However, YACCs also emphasize that, if the disease is stable, they are generally supported by peers who offer distraction, for example, by playing games and watching TV together. In the interviews, both YACCs and peers also show that the boundaries between supporting self-management and paternalism are often fluid, differ from situation to situation, and therefore have to be negotiated.
The patterns of self-management we identified in our study also tell us about the YACCs’ perspectives on their conditions. Here, we can refer to considerations of older people illness perspectives first formulated by Paterson (2001), with the aspect of self-management later added by others (Audulv et al., 2011; Dunne et al., 2019; Robinson, 2017):
The YACCs who focus on their chronic conditions exhibit an “illness-in-the-foreground” perspective (Paterson, 2001). They tend to care little for “wellness.” This group often keeps (less close) friends—who appear to understand little about chronic conditions—out of their self-management (cf. Audulv et al., 2011). This allows them to preserve their autonomy in dealing with the condition and to demonstrate their (self-)competence; these strategies have also been found in other studies (Kelly & Berg, 2021; Mattacola, 2020). Young adults with IBD in particular—a condition that is socially taboo (Polak et al., 2020)—try to manage their disease largely on their own.
In contrast, the illness perspective of YACCs who prioritize the social and tend to neglect their illness prefers “wellness” over “illness” (Audulv et al., 2011; cf. Paterson, 2001). These interviewees attempt to not attribute (too much) importance to their illness. Among them, we mainly find young adults with diabetes who think that their disease is well controlled and/or comparatively “harmless.” If “wellness” is a priority for young adults with cancer, they focus on making their environment feel as good as possible, or they try to forget about their illness—temporarily—and focus on aspects of short-term well-being.
In addition, we also found interviewees whose illness perspectives were non-binary in the sense of orientating equally on aspects of “illness” and “wellness.” This finding augments the model proposed by Paterson (2001), who assumes that illness perspectives will focus either on illness or on wellness (even if they may change over time) (cf. also Audulv et al., 2011; similar Dunne et al., 2019; Robinson, 2017). The interviewees who exhibited a non-binary perspective, mainly young adults with cancer, attempted to reconcile the demands of the illness with everyday activities and social life (including training, university, and work). Weighing long-term health against short-term well-being is particularly characteristic in this context. Peers function as a resource, offering emotional support and supplying positivity that “nourishes” the YACCs.
Of course, this study has its limitations, so what are limits of our study? Participants are well educated (university or professional training), so that we cannot say much about how self-management and peer relationships in social precarity. Existing findings (Boucher et al., 2022; van Houtum et al., 2015) on the impact of insecure housing or low income on disease management are contradictory.
Our study is cross-sectional with retrospective data and cannot say anything about whether YACCs and peers succeed over time in managing the condition in a way that enables a “good life” (Dunne et al., 2019; cf. Robinson, 2017). Of the participating 60 YACCs, only 24 have conveyed one or several peers. YACCs with IBD did so more often than those with other conditions. Those who focus on their condition did so more seldom than those in the other two groups. One explanation can be that “focusing” YACCs emphasized in the interview that peers are often not the person to talk to about the condition. None of the YACCs explicitly refused conveying a peer, so we can only speculate why this did not work in 36 YACCs.
However, with its specific qualitative approach, our study makes as contributions to the existing literature: The multi-perspective approach to YACCs’ and their peers’ experiences with self-management on the one hand and referring to a range of chronic conditions on the other allows to analyze this issue in a more complex and comprehensive way than in existing research. The perspective on peers allows to analyze support and self-management beyond the family and in a context highly relevant for young adults facing chronic conditions. The qualitative approach allows to explore what is relevant for YACCs and for their peers in their own perspective and a deeper understanding of both parties’ experiences and views. Further studies should focus not only on the individual view of YACCs and peers on self-management but also on their attempts to coordinate more closely in dealing with the condition.
We used Lincoln and Guba’s (1985) criteria for establishing credibility such as triangulating the perspectives of the YACCs with those of their peers, in order to systematically expand the perspectives on the phenomenon of self-management on the context of peer relationships. Including many different voices (in the form of quotes) also contributes to trustworthiness by allowing the reader to create their own impression of the congruence between the (researchers’) interpretation and the original quotes. Purposive sampling (Patton, 2015) contributes to generalizability by comparing several chronic conditions. Recruiting participants with different conditions expands the data by bringing in a wider range of illness-related experiences (Lincoln & Guba, 1985).
Supplemental Material
Supplemental Material - Self-Management and Relationships: Perspectives of Young Adults With Chronic Conditions and Their Peers
Supplemental Material for Self-Management and Relationships: Perspectives of Young Adults With Chronic Conditions and Their Peers by Uwe Flick and Gundula Röhnsch in Qualitative Health Research
Footnotes
Acknowledgments
The authors thank the interviewees who shared their time and their experiences. The authors thank the German Research Foundation for the financial support of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded from 10/2021 to 9/2027 by the Deutsche Forschungsgemeinschaft (German Research Foundation), grant no: FL 245/12-1; FL 245/12-2. Open Access Funding is provided by the Freie Universität Berlin.
Ethical Statement
Data Availability Statement
The data are not publicly available due to them containing information that could compromise research participants’ privacy and consent.
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.