
Abstract
Intimate partner violence (IPV) is associated with a wide range of mental and physical health concerns. Research suggests that many physicians lack knowledge and skills to adequately respond to patients experiencing IPV. In order to better integrate physicians’ contributions into intersectoral responses to IPV, we asked stakeholders with expertise and experience related to IPV about the knowledge, skills, attitudes, and behaviors they wanted them to have. Guided by principles of interpretive description, and using a key informant method, we conducted unstructured interviews with 18 stakeholders in IPV-related frontline, managerial, or policy roles in Ontario, Canada. Data collection and analysis proceeded iteratively through 2022; “thoughtful practitioners” outside the research team were recruited at key junctures to provide feedback on formative findings. Stakeholders suggested that “attending to power” should be a core principle for medical practice related to IPV. Attending to power encompassed understanding interactional, organizational, and structural power dynamics related to IPV and purposefully engaging with power, by taking action to empower people subjected to violence. Specific recommendations for practice concerned four focal contexts: relationships between partners, between patients and providers, between providers, and in social systems and structures. Strengthening physicians’ capacity to attend to power dynamics relevant to their IPV practice is an important step in both improving medical care for people experiencing IPV and integrating physician contributions into other services and supports.
Introduction
Intimate partner violence (IPV) is a pervasive form of gendered violence with profound and enduring implications for health and well-being. People who are made subject to IPV are disproportionately cisgender women, transgender women, and other transgender and gender non-conforming people (Peitzmeier et al., 2020; Sardinha et al., 2022). They suffer from physical injuries and mental distress that are directly attributable to violence, but also from chronic mental and physical health conditions related to stress, coping strategies with deleterious health effects, and denied or delayed access to care (Bacchus et al., 2018; Oram et al., 2022; Potter et al., 2021). As the body of literature elucidating these harms to health has grown, so too has consensus that physicians have both an obligation and unique opportunity to address IPV with their patients (American Medical Association, 2019; Dichter et al., 2021; Tarzia et al., 2020). In this context, the last 20 years have seen a marked proliferation of training initiatives related to IPV for physicians and medical trainees (Ghaith et al., 2022).
Despite this, those directly affected by IPV report reluctance to disclose their experiences with IPV to healthcare providers, citing past unsupportive responses as well as fears about the removal of their children from their care and retaliation from violent partners (Heron & Eisma, 2021; Robinson et al., 2021; Tarzia et al., 2020). Moreover, research with people who have disclosed their IPV experiences to a healthcare provider suggests that many practitioners still lack necessary knowledge and skill to respond to these disclosures with requisite sensitivity (Morse et al., 2012). Further work is needed to ensure physicians are well-prepared to address the needs of people they serve who experience IPV.
The IPV-related work that physicians perform has impacts beyond encounters with individual patients and includes contributions. It is important to better understand and integrate the contributions that physicians make within the broader landscape of services and supports that address IPV. Although intersectoral collaboration is widely regarded as vital to efforts to meet the needs of individuals and families affected by IPV (Colombini et al., 2017; Laing et al., 2018; Lalande et al., 2024), medical education scholarship related to IPV has largely centered perspectives from medical trainees and practitioners without including input from those outside of the medical profession and whose work related to IPV interfaces with that of physicians. For instance, although providing patients who disclose IPV with referrals to appropriate community supports is widely recommended in guidance for physicians (Feder et al., 2013; World Health Organization [WHO], 2013), input from the community service providers on the receiving end of these referrals has often been absent from research that shapes medical education practice and policy. Understanding perspectives from stakeholders doing work related to IPV outside of medicine may reveal opportunities to better integrate the contributions of physicians into an intersectoral response to IPV. With this in mind, we asked key informants with expertise and experience related to IPV about their priorities for physician knowledge, skills, attitudes, and behaviors related to IPV.
Methods
Study Design
We used interpretive description (ID) to guide our study design. ID is a flexible methodological approach to conducting applied qualitative health research (Hunt, 2009; Thorne, 2016). Developed by nursing scholars (Thorne et al., 1997), ID blends constructivist and interpretivist paradigms to produce tentative truth claims that represent and interpret phenomena of clinical interest (Hunt, 2009). ID frames informing clinical practice as the primary objective for developing and deepening insight into human experience. With this study, our objective was to generate recommendations to enhance physicians’ clinical practice related to IPV by drawing on expertise of stakeholders outside of medicine. Our research team included a medical student, clinicians with expertise in family violence, and researchers with expertise in health professions education.
Participants and Sample
We used key informant technique to identify participants with insight into our research topic. Key informants are members of a community or field of practice with unique access and understanding of a phenomenon of research interest (Marshall, 1996; Pahwa et al., 2023; Tremblay, 1957). For the purpose of this study, key informants were defined as stakeholders with professional experience related to IPV, working in a field outside of medicine in a frontline, managerial, or policy-oriented role. We excluded physicians and medical trainees. We did not explicitly seek to recruit participants who had personally experienced IPV, but neither did we exclude them. Instead, our aim was to identify participants with informed perspectives from professional and/or advocacy experience related to IPV. Additional inclusion criteria included the ability to participate in an interview in English and working in Ontario, Canada.
Key informants with a wide range of expertise related to IPV were purposively identified through quota and theoretical sampling strategies. We devised a sampling matrix based on sector (including IPV-specific services, healthcare, education, social services, government, the criminal-legal system, and advocacy) and role (frontline, managerial, or policy-focused) (Appendix 1). Members of the research team populated the sampling matrix, drawing on their professional networks to identify prospective participants with relevant insights. Once interviews began, we engaged in snowball sampling, asking participants to recommend other prospective key informants, particularly those with informed perspectives that differed from their own. As data collection and analysis progressed, we used theoretical sampling to recruit stakeholders with expertise relevant to developing areas of interest in our analysis.
Data Collection
Key informants participated in 45- to 60-min in-depth interviews conducted over Zoom by AC, the lead investigator, or an undergraduate research assistant. Permission was obtained to audio-record interviews and to recontact participants in the future if clarification of any data was necessary. Interviews were structured using an iterating interview framework that included three sections intended to (1) situate the participant’s expertise related to IPV; (2) understand their perceptions of medical care available to people affected by IPV; and (3) elicit their recommendations to improve professional training and medical care. In lieu of a standardized demographic form, participants were asked to reflect on aspects of their identity that they felt were relevant to their perspectives.
Data Analysis
Data collection and analysis proceeded concurrently. Constant comparative analysis was used to identify and subsequently develop “interpretive possibilities” in the data (Thorne et al., 2004). NVivo qualitative data analysis software was used to organize data, and coding took place through iterative stages: the lead investigator immersed herself in the data, listening to audio recordings, reviewing transcripts, and annotating field notes. Next, she identified overarching themes that were present in this data, asking for input and clarification from participants in subsequent interviews through a process of interim member-checking. She subsequently developed a thematic coding template which was applied to new interviews and iteratively refined through comparative synthesis. Data collection was stopped when members of our research team were in agreement that our findings were credible, recurred across interviews, and could be used to generate recommendations for future training related to IPV. Data collection began in January 2022 and concluded in May 2022. Strategies to ensure the rigor of our analysis and the quality of our research findings included reflexive memoing and use of interim member-checking. We also incorporated input from “thoughtful clinicians” (Thompson Burdine et al., 2021) with expertise related to IPV who provided feedback on applications and resonance of the focal concepts, themes, and recommendations developed in analysis. Mirroring the interview prompts provided to study participants, both study investigators and thoughtful clinicians were invited to reflect and share, as they were comfortable, about how their understanding of the data was shaped by their respective identities and experiences.
Ethics
Research ethics approval for this study was provided by the Hamilton Integrated Research Ethics Board (Project #13770). All participants provided written informed consent.
Results
Overview of Participant Roles.
Participants described a range of ways they wanted to see physicians better understand, wield, and yield social power in their work related to IPV. One cross-cutting theme related to the importance stakeholders ascribed to physicians’ ability to understand and engage with different ways power shaped their professional practice. We called this “attending to power.” The analysis that follows first describes different participants’ understandings of power before turning to explicate our conception of what it means for physicians to attend to power. It concludes with recommendations from participants about opportunities for physicians to attend to power in four focal contexts—between partners in relationships in which IPV occurs, between patients and providers, between providers, and in social systems and structures. Participant quotes are identified with the professional role descriptor chosen by each participant.
Conceptualizing Power
In describing power dynamics they saw as relevant to physicians’ work related to IPV, stakeholders provided examples that resonated with three theoretical conceptions of power: (1) interactional power in social relationships; (2) organizational power in institutions; and (3) structural power in society. Interactional power is conceptualized as an individual’s capacity to exert influence over the actions of others (Vanstone & Grierson, 2022). Reflecting on hesitation patients might feel when asked about IPV, one participant framed fear of a violent partner as a facet of interactional power that deters disclosure: Definitely she will say no […]. She’s going back home with the same abuser […]. If she stayed by herself [in the doctor’s office] for a long time, they’re suspicious, like “What were you saying? What did you say?” (Program coordinator, culturally specific social service provider)
Organizational power, by contrast, describes ways in which institutional hierarchies, infrastructure, and policies organize and shape actions and interactions of individuals operating in their confines (Moon, 2019). Organizational power is reflected in barriers to interprofessional collaboration that one participant described at the post-secondary institution they worked at: There’s just a few layers horizontally between the folks who work in health centres, and then staff who do student services. Not that there’s not overlap [in our work], just that those are distinct positions in the [post-secondary institution’s] system. (Service provider, post-secondary sexual violence support service)
Finally, structural power operates at a discursive level to produce knowledge and value systems that circulate through society, shaping how people interact, institutions are organized, and resources are distributed (McHoul & Grace, 1993; Warren, 1992). Reflecting on the evolution of language used in their work addressing violence in relationships—terms including “domestic violence,” “woman abuse,” “gender-based violence,” and “violence against women”—several participants connected changing language to political machinations: “It is women, it is folks from the 2SLGBTQIA+ community [that disproportionately experience IPV], right? But if [policymakers] don’t use those terms then […] it’s not as specific. You’re not held to account” (gender-based violence service provider).
Attending to Power
Attending to power in the context of physicians’ work related to IPV refers to understanding how power operates and purposefully engaging with power for the purpose of empowering people experiencing IPV. Virtually, all of the stakeholders consulted in this project stressed the importance of physicians’ understanding power in relationships affected by IPV, but also described other contexts in which they thought physicians should understand the mechanics of power at work. For instance, participants wanted physicians to understand how their own personal identities and professional power in healthcare spaces shaped their interactions with patients and other providers. Simply understanding the dimensions of power was marked as insufficient. Stakeholders also underscored the importance of translating knowledge into action: “It’s not just recognizing that violence against women exists, but I think it’s also recognizing how [physicians] can intervene and some of the challenges of intervening” (Director of programs and services, women’s shelter). Attending to power therefore encompasses connected imperatives to understand and to respond to power dynamics.
Attending to Power Between Partners
In more concrete terms, participants offered wide-ranging recommendations for how they wanted to see physicians attend to power in their work related to IPV (summarized in Table 2). All of the stakeholders interviewed in this study agreed on the importance of physicians understanding how power operates between partners in relationships where IPV occurs. This included being aware of varied forms and tactics of violence and control used to exert interactional power over a partner. It also included recognizing ways structural power inequities connect IPV and other forms of violence and oppression. To attend to these mechanics of power, participants wanted to see physicians cultivate their capacity to recognize patients experiencing different forms of IPV and provide ongoing support. In doing so, however, stakeholders stressed that physicians must temper their expectations about the impacts their actions might have: I guess I would like [physicians] to appreciate the long game where it’s not just like, they’re going see someone, be like, “Oh I’m more attuned to the fact that you’re experiencing IPV, I’m going to tell you about this woman shelter, you’re going to leave and everything’s going be fine.” Because we haven’t even gotten to all the problems with like, availability and access to resources. (Service provider, post-secondary sexual violence support service) Summary of Recommendations for Practitioners.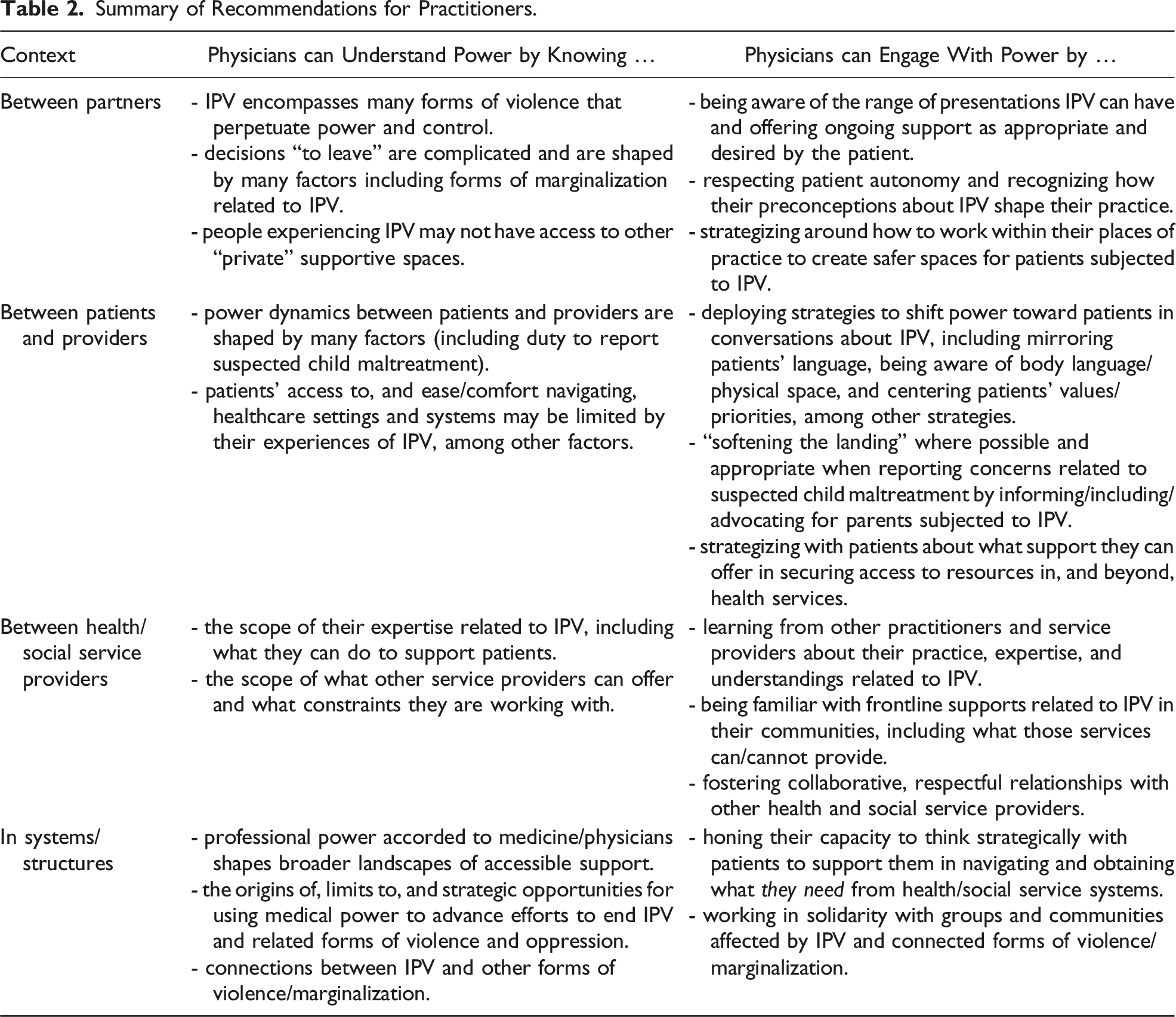
Despite these cautions, stakeholders still expressed optimism about opportunities for physicians to attend to power dynamics between partners by capitalizing on organizational power afforded to them in healthcare settings. One way they could do this was by facilitating safer spaces within their clinical practice. Suggestions included making it routine practice to speak to all patients without their partner present and offering patients known to be experiencing IPV the option of meeting with other support services under the guise of medical appointments. Contextualizing these recommendations in terms of the challenges people experiencing violence face in connecting with services, one participant explained, “[medical appointments are just] such a rare point of contact with victims of domestic violence while they’re in the domestic violence” (former child protection worker/civil litigator).
Attending to Power Between Patients and Providers
In order to be effective in caring for patients experiencing IPV, however, stakeholders also stressed that physicians must work to understand and engage with mechanics of power that shape their patient–provider interactions. Several participants described how interactional power imbalances between patients and providers could evoke the imbalance between partners in a violent relationship: [As a patient], you walk into a physician’s office, [and the doctor] already has tremendous authority in the space, over your body. And if you’ve experienced abuse, […] it can replicate the traumatic experiences. (Senior manager, violence against women (VAW) service provider)
Other participants connected this imbalance to physicians’ mandated reporting obligations related to suspected child maltreatment, noting how structural forms of oppression amplify marginalized parents’ concerns about disclosing IPV: This system is so racist, particularly in the way [it] judges whether people are eligible or capable to take care of their children […]. [People experiencing IPV] really worry that any report of that violence will lead to losing their children. (Organizer, migrant sex worker advocacy group)
To aid in attending to these power imbalances, stakeholders urged physicians to adapt their behavior to mitigate fear and shift the balance of power toward patients. Suggestions included engaging in ongoing informed consent discussions with patients in all aspects of their care, clearly explaining limitations to doctor–patient confidentiality, and mirroring language patients used when talking about their experiences. Stakeholders also stressed close attentiveness to patients’ body language when talking about IPV and allowing patients to direct conversations about IPV in keeping with what feels “safe” to them. Participants acknowledged the way that organizational factors—the physical layout of clinical spaces, the limited availability of interpretation services, and institutional policies related to documentation—constrained medical practice but urged physicians to work “creatively” with their patients within systems to provide person-centered care. One stakeholder explained, Yes [physicians] have an obligation to interact with Children’s Aid [child protective services] but there are ways to connect with helping resources or supportive resources that maybe can offer a softer landing […]. What is the language that you use to describe the situation that was relayed to you? Is this your perception or is this what was said to you? How do you prepare the person that you’re working with for the possibility of you having to contact [Children’s Aid]? What are the mechanisms that you’re offering or attempting to create bridges with so that that person can be supported while they’re going through that process? (Trauma counsellor, service provider for criminalized people)
This active formulation of attending to power in patient–provider interactions reflects the importance participants ascribed to physicians working with patients to support them in navigating fractured health and social service systems, as opposed to simply making referrals or reports in isolation.
Attending to Power Between Providers
Outside of the immediacy of patient–provider relationships, many of the participating stakeholders also described power dynamics between physicians and other providers. These observations were most prominent in interviews with stakeholders whose professional work interfaced directly with physicians. Participants described feelings of interprofessional tension as well as examples of constructive and respectful collaboration. Feelings of frustration were particularly acute among stakeholders with experience in the child welfare system who characterized many of the physicians they dealt with as reticent to share information, even when mandated by law. Three participants with training as social workers described structural power dynamics reflected in the weight accorded to testimony from physicians versus social work perspectives in legal proceedings: “It’s annoying, because [the] courts will ask us for ‘expert evidence’ and if the courts are asking for expert evidence, apparently being a social worker doesn’t count” (child protection worker). Stressing the multi-faceted needs of people subjected to IPV, other stakeholders reflected on the importance of physicians understanding their own scope of practice related to IPV relative to what other service providers can offer. These participants noted how structural power dynamics fostered barriers to connection between those working in different organizations or systems. Reflecting on challenges bridging workers in the health sector with those providing homelessness and violence against women services, one participant noted that “by funding alone, the services are siloed,” hampering collaboration (Director of programs and services, women’s shelter). To attend to these power dynamics, several participants encouraged physicians to get involved with community efforts to coordinate IPV services across sectors: If you have physicians at those coordinating tables, their understanding of the experiences of [patients and service providers] dealing with IPV may grow. Like there might be points where we’re missing this communication, right? […] Sitting at coordinating tables allows you to understand other systems better […]: how you could be delivering services differently or [be] more responsive or aware. (Senior manager, VAW service provider)
Fostering relationships between physicians and service providers working in other sectors was perceived as both an opportunity for education and a gateway to partnership.
Attending to Power in Social Systems and Structures
The final power dynamic that stakeholders addressed relates to how power operates in social systems at a structural level to entrench IPV as a pervasive form of violence. Every single participant in this study wanted physicians to understand how work related to IPV connected to oppression and marginalization. One participant framed this as putting that context into the discussion around IPV, [similar to] when people say that being Indigenous is a “risk factor” for diabetes […]. It’s not really being Indigenous, it’s the history of colonization, and socio-economic factors and all those other things that have been imposed on us. (Education leader, post-secondary institution)
Several participants also suggested physicians could attend to power through political mobilization around IPV, reflecting on credibility afforded to physicians by virtue of their profession: I would love for [medical associations] to use any of their clout to get better services. I mean, really, for anything, for any social welfare state stuff, but specifically for domestic violence. […] Ongoing counseling for the kids, ongoing counseling for the women. Those pieces that the doctor can’t do but could advocate for. (Former child protection worker/civil litigator)
Some participants offered caveats to this encouragement, however, stressing that physicians should reflect critically about their roles in collective action: Any kind of advocacy should be bottom up, right? We have an amazing doctor, they know what is happening from their perspective, but what is actually happening from [the perspective of] the people using [the services]? (Organizer, migrant sex worker advocacy group)
For these stakeholders, attending to power in advocacy work required the cultivation of critical reflexivity around the limitations of physicians’ situated perspectives.
Discussion
Combining ID and key informant method, this study elicited recommendations from stakeholders with expertise related to IPV about the knowledge, skills, attitudes, and behaviors that enable physicians to provide effective care to people affected by IPV. Across these interviews, power was an organically recurring central theme. Participants wanted physicians to understand different forms of power that were relevant to their practice, and to work to address those forms of power in order to empower people experiencing IPV. We developed the concept of “attending to power” to reflect this dual imperative and consolidated participants’ recommendations for physicians around four focal contexts. In the context of relationships where IPV was occurring, participants wanted physicians to understand how power and control operated between partners and to strategize around how they might facilitate safer spaces for patients in their medical practice. In the context of relationships between providers and patients, participants stressed the importance of understanding the many permutations of power that shape patient–provider interactions. They identified practical strategies for physicians seeking to empower patients navigating health and social service systems. In the context of relationships between health and social service providers working in different fields, participants wanted physicians to understand the scope of practice and constraints other service providers worked within and to foster collaborative relationships. Finally, in the context of the broader systems that structure what supports are accessible to people experiencing IPV, participants wanted physicians to understand connections between IPV and other forms of marginalization and to work strategically in solidarity with affected communities to end violence.
Findings from this analysis help to illustrate some of the ways that interpersonal, organizational, and structural forms of power give shape to physicians’ professional roles, including those related to IPV. This resonates with accounts of social power as multi-faceted and ever-present in practices of medicine and medical education (Kuper et al., 2017; Vanstone & Grierson, 2022). It also fits within a broader canon of feminist research that foregrounds issues of power and oppression as key to understanding, addressing, and preventing IPV (Cannon et al., 2015; Goodmark, 2018). Medical education has long been understood as a process of acculturation, with professional training inculcating new physicians with shared professional values, attitudes, and ideas. With this lens, the power dynamics that participants in this study described can be understood, at least in part, as products of the formal, informal, and hidden curricula that constitute how doctors learn about IPV (Hafferty, 1998). These power dynamics can also be problematized as challenges in which the medical education community has a clear stake in trying to address. Although established clinical practice guidelines and education materials related to IPV describe “empowerment” as a key feature for structured therapeutic interventions (WHO, 2013), and include formal curricula addressing gendered inequality (WHO, 2013), our findings illustrate the need to understand and attend to power dynamics beyond violent relationships or the immediacy of the clinical encounter (Tarzia et al., 2020). In order to reshape how physicians learn to think about IPV and their related professional roles, our findings suggest that professional training programs can—and should—support physicians in strengthening their analysis of the ways that power shapes health, illness, and the practice of medicine in the context of IPV and beyond.
Implications for Educators
In urging physicians to attend to power within their professional practice, our intent is not to imply that physicians are unilaterally powerful or can definitively redress power inequities related to IPV. Feelings of powerlessness and moral distress have been identified as factors in burnout for healthcare providers (Beck et al., 2020; Dzeng & Wachter, 2020), and participants in this study agreed that IPV was a problem that physicians could not address alone. Instead, we conceptualize attending to power as an opportunity to forge alliances and solidarity between patients and care providers, between service providers working in different sectors, and between providers and the communities they serve. Indeed, participating in collective action—one strategy for attending to unjust structural power dynamics—is one possible answer to feelings of distress that arise when caring for people who are suffering in an unjust society (Andrews et al., 2019; Coutinho & Dakis, 2017). In lieu of formalized advocacy training, however, we suggest that medical educators wishing to integrate “attending to power” into medical education focus on honing trainees’ capacity to understand how power shapes the health of their patients, to critically reflect upon their own nascent power as providers, and to engage with people they serve with empowerment as a core principle for practice (Cavanagh et al., 2019; Ng et al., 2019).
The rich expertise and wide-ranging professional experiences related to IPV that participants share in their interviews are focal strengths of our analysis; so is the clearly established process we followed while identifying key informants. In keeping with principles of ID, the process of iterative feedback through which our analysis progressed was rigorous. Recognizing that members of our research team and key informants both came to this study with their own investments and attachments to power, we incorporated opportunities for reflexive discussion throughout study design, data collection, and analysis. Our strategy of asking key informants to qualify their positionality in their own words (instead of using a standardized demographic form) may be useful to other qualitative researchers hoping to engage participants in reflexive interviews.
Limitations of our study relate to constraints of our sample. To narrow the scope of our recruitment efforts, we limited our sample to the province of Ontario and our analysis reflects the experiences of people working within one landscape of IPV resources and support. As well, the majority of social workers in our sample is also notable. This reflects the predominance of social workers employed in positions that are related to IPV, but future inquiry developing the concept of attending to power should further probe nuances of power between providers by including service providers working in other roles, and from advocates working outside of regulated health and social service professions. Finally, although we did not ask participants about their personal experiences with IPV, more than half of the individuals we interviewed disclosed having experienced IPV at some point in their lives. Even so, these results should not be interpreted as an account of survivor preferences or patients’ priorities for their medical care. Research examining the perspectives of people subjected to IPV on the strategies for attending to power described in this paper represents a critical next step for this work.
In conclusion, this study has examined the manifold permutations of social power that shape medical practice related to IPV across a range of contexts. In integrating insights and recommendations from stakeholders addressing IPV while working in diverse sectors, we developed the concept of “attending to power” as a cross-cutting principle for physicians seeking to support their patients experiencing IPV. Medical educators and policymakers seeking to strengthen physicians’ response to IPV should explore opportunities within medical training to bolster physicians’ capacity to understand and engage with power in service of supporting their patients.
Footnotes
Blank Sampling Matrix
Frontline
Managerial
Policy-Focused
IPV-specific services
Healthcare
Education
Social services
Government
Criminal-legal system
Advocacy
Acknowledgments
The authors wish to thank Katrina Shen for her support with data collection; Anita Acai, Ilana Allice, Gina Dimitropoulos, and Meg Laupacis for their thoughtful input during analysis; and Cara Evans for her feedback on a formative draft of this work.
Authors’ Contributions
A.C. conceptualized the study and drafted the protocol with input from M.V., H.L.M., M.K., and S.A.R. A.C. led data collection and collaborated on analysis with M.V.; H.L.M., M.K., and S.A.R. contributed formative and final feedback. A.C. drafted the manuscript, and all authors made revisions. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Physician Services Incorporated and the Canadian Institutes of Health Research.