
Abstract
Background
Individuals experiencing and perpetrating intimate partner violence (IPV) are frequently in contact with general health and mental health services. Health service providers, including nurses, thus have a key role in identifying and responding to initial indicators of IPV risk.
Purpose
The present study provides descriptive information about current assessment and intervention practices of health and mental health service providers when patients are presenting with concerns about IPV.
Methods
A secondary data analysis of interviews with general health practitioners (n = 17) were coded and dominant themes analyzed through thematic analysis.
Results
The present study uncovered ways in which IPV-related risks are, and are not, recognized and responded to. A metaphorical visual display in the form of a “domestic violence supply room” depicts the level of access and degree of competency described by practitioners in respective areas of practice. Within reach for all practitioners is the knowledge of factors that increase risk and vulnerability to IPV. Out of reach is a comprehensive understanding of the needs of children and perpetrators as well as the consistent ability to consider intersectionality and be reflexive when working with culturally and linguistically diverse populations. The step ladder to improved IPV response, including formal supports such as training and procedures, is frequently described as lacking.
Conclusions
A consistent and empirically supported approach to IPV assessment and response is rare to find across generalist service provision. Although service providers possess basic knowledge of risk factors, organizational direction is needed to allow providers to address IPV confidently and effectively.
Background and purpose
Intimate partner violence (IPV)–also known as domestic violence–is endemic in Canada. This violent behaviour is perpetrated by a current or former intimate partner and can include physical, verbal, sexual, and psychological abuse. While IPV affects individuals from all demographic and socioeconomic backgrounds, victims are most often women and the violence is commonly perpetrated by men (Conroy, 2021a; Cotter & Savage, 2019). In 2019, IPV-related incidents accounted for 30% of all violent crime reported to the police, with women representing 79% of survivors in these cases (Conroy, 2021a). Given that rates of IPV are underreported to police, these statistics are likely a gross underestimation of the actual population experiencing such violence (Moreau et al., 2020). Furthermore, whereby popular measures for surveying incidences of violence often overlook information surrounding the meaning, context, and consequences of IPV, examination of such variables reveals that women are overrepresented when the violence is most intense (Gurm & Marchbank, 2020). Relative to men, women are four times more likely to be victims of IPV and are at heightened risk of injury and death in intimate contexts (Burczycka, 2018; Conroy, 2021a). At its extreme, IPV can culminate in intimate partner homicide, the murder of intimate partners or family members, with women representing four out of five victims between 2014 and 2019 (Conroy, 2021b; Scott et al., 2020).
The sequelae of IPV are well-documented. Victimization is associated with physical and mental health issues ranging from traumatic brain injury and musculoskeletal injuries to depression, anxiety, suicidality, and traumatic stress (Stewart et al., 2013; Symes et al., 2014; Wathen, 2012). These consequences do not necessarily stop when the violence ends but may persist for years (Delara, 2016). Due to the impact of IPV on health, women who have experienced violence are frequent users of health care services and are regularly in contact with primary care physicians, public health nurses, social workers, and mental health counsellors, among other service providers (Garcia-Moreno et al., 2015a; Sugg, 2015). Perpetrators of IPV have likewise been shown to interact with general mental health providers in the months leading up to major violent events, such as domestic homicides (Oram et al., 2013; Scott et al., 2020). Given that general service providers are likely first among the professional contacts of many victims and perpetrators, they provide a crucial opportunity to identify and intervene in instances of IPV (Stewart et al., 2021).
As general recognition grows and a body of standards and best practices informing general health service responses to IPV continues to evolve, it is essential to examine and understand current service provider practices. Prior research across the United States and Canada suggests that general service responses to IPV vary dramatically (Ahmad et al., 2017; Alshammari et al., 2018; Macy et al., 2009). Interviews with therapists, social workers, nurses, and service users have identified a number of barriers to effective intervention, including a lack of comfort and expertise in the area, insufficient training, a paucity of time and resources, feelings of powerlessness in making a difference or offering a solution, and institutional constraints (Burns et al., 2020; Simmons et al., 2015; Trevillion et al., 2016). Furthermore, individuals seeking services for IPV-related concerns often present with unique individual- and community-level risks that increase the complexity of responding to IPV. In particular, structural violence–such as race-based policies that keep certain groups living under conditions of material deprivation, colonial policies relating to the large-scale removal of children from their families and into state care, policy-enforced poverty, confinement to reserves, cultural erasure, and disproportionate imprisonment–has shaped the health and risk of distinct populations in Canada, including Indigenous communities and immigrant and refugee newcomers (Marchand et al., 2015; Nelson & Wilson, 2018; Varcoe et al., 2014). Such inequities furthermore increase vulnerability for IPV victimization and perpetration (Brownridge et al., 2017; Okeke-Ihejirika et al., 2018). Thus, responding to IPV requires an intersectional framework so that one may appropriately address the needs of individuals who have multilayered identities that intersect with political and socioeconomic realities–realities that often precipitate marginalization, oppression, and discrimination (Lockhart & Mitchell, 2010). General service providers in Canada, interfacing with increasingly diverse populations, must understand such complexities to assess the impact of these identities on risk and access to opportunities and to implement effective risk assessment, management, and safety planning strategies.
The present qualitative study aims to provide descriptive information about the current assessment and intervention practices of general health and mental health service providers when working with men, women, and children in the context of IPV. Such information is critical to identifying gaps in response and ensuring earlier and effective intervention for individuals experiencing and perpetrating IPV. Furthermore, research examining how practitioners attitudinally approach and understand risk and safety will lend support in initiating change in the training and education of general practitioners. Finally, considering the diverse populace of Canada and the unique needs and risks faced by the distinct communities within its borders, exploring these topics within the Canadian context is key for an improved response when working with vulnerable populations. Given the frequency with which victims and perpetrators of IPV present to health settings, nursing professionals may be particularly interested in these data as they are frequently the initial point of contact for patients.
Methods and procedures
The present study involved a secondary data analysis of interviews conducted with participants who worked in mental health, healthcare, and/or addictions sectors.
Data for the present study
This study was conducted as part of the Canadian Domestic Homicide Prevention Initiative for Vulnerable Populations (CDHPIVP). As part of this initiative, 372 interviews were held with participants from various sectors (i.e., violence against women, police, child protection, mental health/healthcare/addictions, and partner assault/corrections) across Canada who interface with victims and/or perpetrators of IPV through their work. This study utilized interviews with participants who worked in mental health, healthcare, and/or addictions (n = 25). From the sample of participants who worked in these sectors, only those interviewees who endorsed not having a specialized IPV role within their organization were selected for this study. That is, since the present study hoped to ascertain perspectives of general frontline professionals, participants who identified as having a specialized IPV role (i.e., nurse on a sexual assault and domestic violence unit, social work manager for domestic violence-related cases, social worker dealing with adult sex offenders) were not included. The final sample for this study included 17 interviews with generalist frontline professionals.
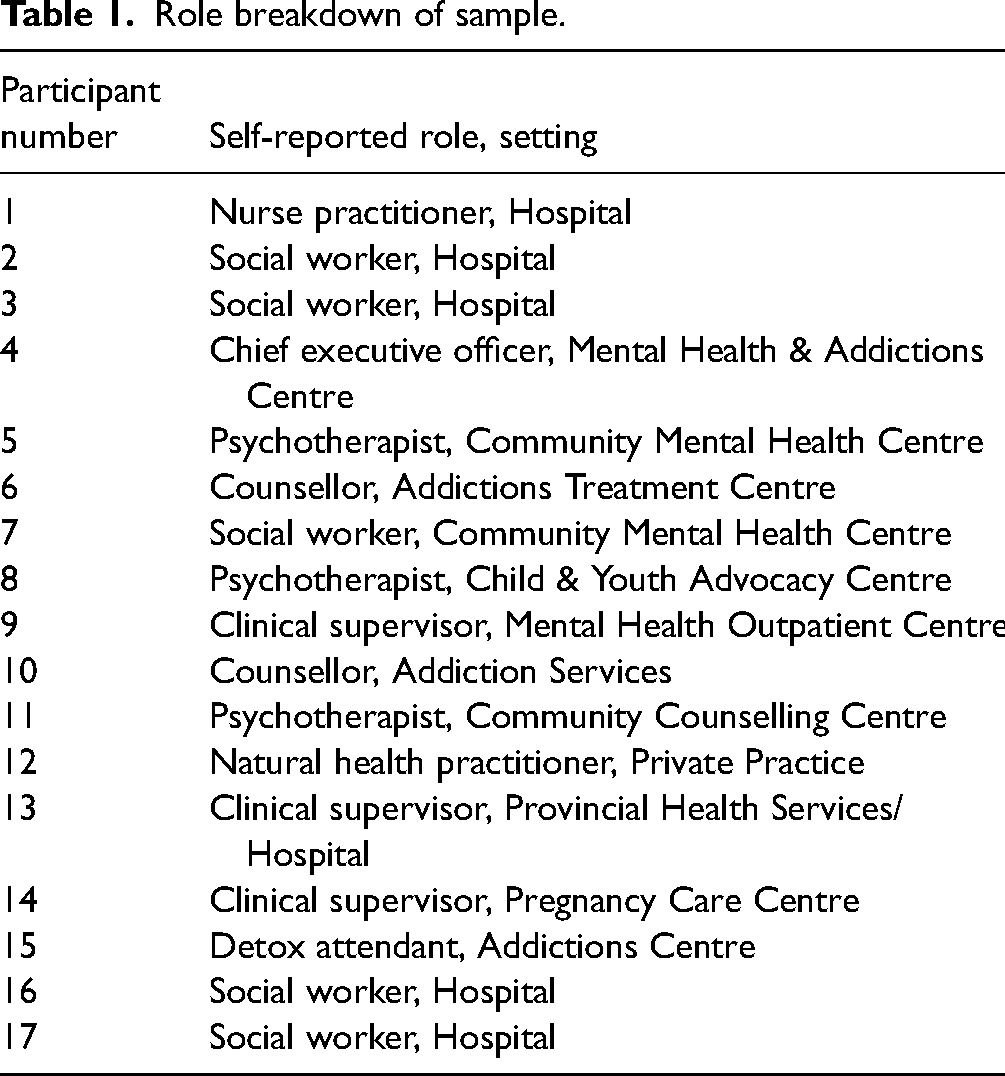
A majority of these participants worked in Ontario (n = 11), with the remainder located in Alberta (n = 3), Saskatchewan (n = 2), and Manitoba (n = 1). Most self-identified as working in community mental health and addictions settings (n = 8), followed by hospitals (n = 6). The remainder worked in other general care settings (n = 7) including private practice and pregnancy care and child, youth, and advocacy centres. Participants furthermore self-identified as social workers (n = 5), clinical supervisors (n = 3), psychotherapists (n = 3), addictions and mental health counsellors (n = 2), nurse and/or natural health practitioners (n = 2), a detox attendant (n = 1), and a chief executive officer (n = 1). Table 1 details the self-reported role and setting for each participant in the final sample.
Role breakdown of sample.
The interviews
After approval from the research ethics review boards at Western University and the University of Guelph–the lead universities for the CDHPIVP–consenting participants were interviewed by graduate students with research or clinical backgrounds related to IPV. Reflecting the intersectional aims of CDHPIVP, approximately 30 interview questions queried across two general areas: experiences with risk assessment, management, and safety planning practices; and challenges, unique risks, and promising practices associated with working with children and Indigenous, newcomer, and rural and/or remote populations. Probes were used to elicit further elaboration. Interviews were completed over telephone between 2017 and 2018 and were audio recorded with participants’ permission. They were subsequently transcribed by research assistants and double checked for accuracy by the original interviewer. Interviews did not include any identifiable information. Transcripts and recordings were stored on encrypted computers.
Data analysis
This study analyzed dominant themes through a qualitative analysis of the content of the interviews. Thematic analysis, as described by Braun and Clarke (2006), was conducted through a multi-step process beginning with an initial familiarization of the interviews. This included a thorough reading and rereading of all the transcripts by the first author. The next step involved the creation of codes which were used to identify the characteristics of the interviews including the topics, patterns, and overall content that they contained. NVivo qualitative coding software (v12.6.0) was used to facilitate the qualitative analysis. A sample of the transcripts (n = 5) were provisionally coded and then collaboratively reviewed with the second author to determine the suitability of the codes. Parent codes were included for each of three major areas discussed in the interviews: risk assessment, management, and safety planning practices; work with children; and work with vulnerable populations. These codes were then broken down into smaller subcodes and this provisional codebook was applied to the remainder of the interviews in a reiterating process of creating and comparing new and existing codes based on emerging themes. Saturation of codes was reached by the completion of all 17 transcripts, suggesting that no new themes were emerging from the addition of more interviews (Hennink et al., 2017). Furthermore, codes were presented to and reviewed by scientist-practitioners immersed in work related to IPV and revised based on their feedback along the way.
It is critical to recognize that the position, experience, and world view of the researcher exerts a substantial influence on the manner in which research questions are framed, methods selected, data collected and analyzed, and results reported (Austin & Sutton, 2014; Flick, 2009). The first author (N.L.) identifies as a white, female graduate student studying in the field of school and clinical child psychology. In addition to completing clinical practica in various settings, this author is afforded knowledge of IPV through involvement in a research lab investigating and aiming to reduce the impact of violence in family relationships.
Results
The present section uses a metaphorical visual display–a “domestic violence supply room”–to depict the current state of practice of responding to IPV (see Figure 1). Several areas of service are represented as boxes on shelves to conceptualize the level of access and degree of competency described by participants with regard to each respective matter. Commonly cited barriers to responding to IPV are visualized as barricades on the door. A step ladder represents aspects of training, experience, and knowledge that promote a more comprehensive and inclusive response–allowing practitioners to “reach” a higher shelf. Finally, a phone represents the described propensity of general health and mental health service providers to “call out” in the form of mandatory reporting and external referrals. Each area is discussed in turn.
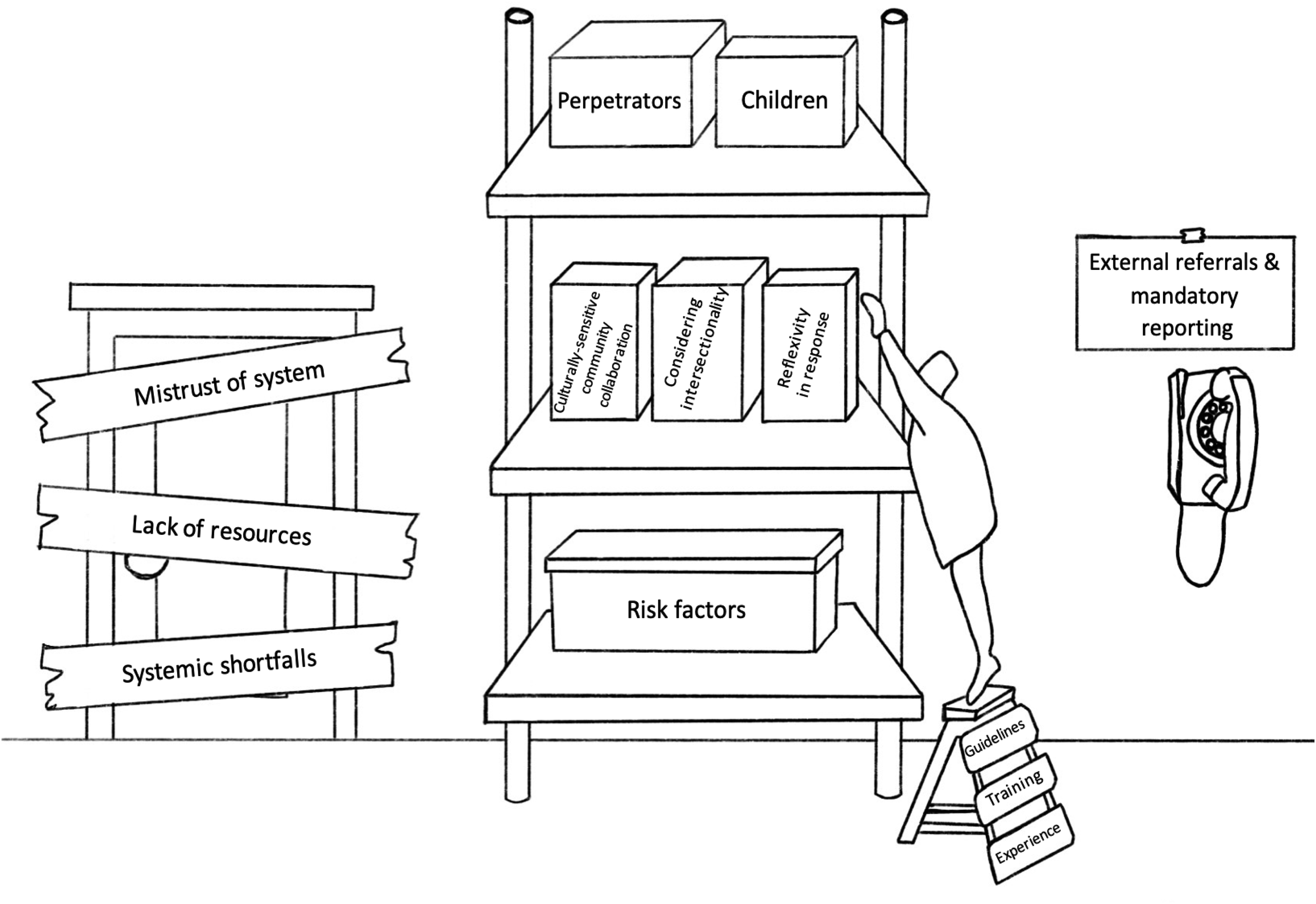
The domestic violence supply room.
Bottom shelf: accessible to general service providers
Items depicted on the bottom shelf of the IPV supply room represent themes that were consistently endorsed in the descriptions of all participants when describing their responses to IPV. That is, the box depicted on the bottom-shelf reflects the aspect of knowledge that is present in the repertoires of all general health and mental health practitioners. In particular, participants described knowing and listening for risk factors that are associated with a higher likelihood of IPV perpetration and victimization. Many provided examples of factors that they consider when determining the presence of specific risks, as indicated by one participant: Is there alcohol involved with her partner? Is she herself judging herself at risk? Where is it that she is living? […] Are there extra vulnerabilities that she has? […] Have there been repeated occurrences of this violence? Has there been repeated separation of the couple? Is he a hunter? […] Where is the guy now; is he awaiting bail? Those are the things I look at (Participant 7).
Participants similarly described exploring risks related to a woman's relationship with the perpetrator of violence, including continued contact, breaches of legal conditions, and concerns around the offender's mental health. Community- and system-level risks that were considered by participants included factors such as poverty, lack of safe housing, and increased isolation from others. Importantly, this knowledge of risk factors included nonverbal signs that a woman might be a victim of violence. For example, one participant described their acuity to subtle postural changes that might suggest injury due to IPV, “Usually, physical abuse is all under your clothes, but there are all sorts of things…like if a woman lowers her center of gravity to below her knees […] that is a sign that she is either torn or very hurt…” (Participant 15).
Lastly, participants demonstrated a knowledge of risk factors that extended beyond those general risks applicable to most women and included risks specific to particular communities. Participants listed several unique risks for immigrant, refugee, and newcomer populations: […] a lack of awareness of how Canadian laws are, a lack of understanding of what their options are, of how our system works…often social isolation, not understanding English makes it really challenging when there is a communication barrier […] their past experiences with police […] many have grown up with certain cultural expectations of gender roles […] if they are a new immigrant, they may have been sponsored by their abuser (Participant 1).
Additional risks for newcomer populations that participants identified included financial barriers, potential prior trauma, and considerations around reputation within their cultural communities, such as shame and embarrassment. Noted risk factors specific to Indigeneity included concurring addiction and mental health concerns, the impact of intergenerational trauma, and the lack of culturally-appropriate and Indigenous-led resources. One participant elaborated: Colonialism can affect people in multiple ways in terms of the fear of engaging services by white community members, in terms of how they are going to be treated, […] sexual abuse in residential schools, physical abuse, mental health issues, substance issues, perhaps isolation if they are living on reserve, disconnection from the land and from their ancestry, from ceremony […] and I see trauma as being a big driver of a lot of mental health [concerns], addictions, violence…so I think this trauma really has a ripple effect (Participant 5).
Many risk factors noted as pertaining to Indigenous communities also overlapped with those of rural, remote, and Northern populations including increased rates of poverty, lack of anonymity, increased isolation and distance from services, and greater access to weapons. Overall, all participants reported a consistent reliance on the knowledge of factors that elevate the risk of harm and violent victimization in their work assessing and responding to IPV.
Top shelf: out of reach for generalist service providers
Contrary to bottom-shelf items, those on the top shelf represent areas of practice that are currently out of the purview–completely out of reach–of the general health practitioner's scope of competency when responding to IPV. Most notably at this level of (in)access are matters related to working with children exposed to violence and perpetrators of violence.
Most participants described children as being rarely–if ever–considered in their work with individuals presenting with concerns of IPV. Children are described as being absent from their considerations of risk and planning around safety: “People forget about the children […] say a woman goes to the hospital because the man beats the hell out of her and nobody in adult mental health or the hospital is asking, ‘Where are the children?’” (Participant 11). Others described children as being forgotten in the process, since general health practitioners are “not trained to consider them” and “don’t have that knowledge” (Participants 6 and 16). Although a few participants maintained that the impact of IPV is profound on children and that youth are often the most vulnerable in situations of IPV, others suggested that the impact of exposure to violence remains to be misunderstood: What I hear in my work is that they didn’t get hurt […] so what is the big deal? They were sleeping, they were in the other room…that minimization about the impact that domestic violence can have on children and on their emotional development, on their physical development (Participant 17).
Still others clarified the target of their service in relation to children: “I don’t worry about anything other than the patient in my bed” (Participant 17). The burden of safety for children, instead, was frequently described as being placed on the mother, with participants “hoping that the mother would be keeping [the children] safe” (Participant 3). Children, thus, are placed on the highest shelf in the IPV supply room, effectively ignored in general service provision targeting IPV.
Likewise, when participants were asked about their work with men and perpetrators of violence, there was an overwhelming consensus that the majority are “not really dealing with the perpetrator” (Participant 3). Even when men are explicitly identified (or heavily suspected) to be perpetrators of violence, participants reported that they neglect to address these concerns. For example: I know I have a perpetrator on my caseload. I will often ask questions on what's happening at home, but that is not within my scope of practice. I don’t do counselling, and I’m not monitoring or supervising the perpetrator (Participant 10).
Instead, the focus of work with men is centred around the specific reasons that brought them to seek services, such as their healthcare needs. Addressing concerns around the safety of his partner and managing his risk to reoffend is otherwise disregarded, even when participants are aware of the importance of involving these men in services: We know the current research is saying we need to make sure that we are thinking about [perpetrators] as well […] I don’t have much information about [what to do with] men (Participant 11).
Overall, work with perpetrators to address concerns of violence is by-and-large omitted from general healthcare provision and thus situated on the top shelf, out of reach for service providers. Participants note a lack of clinical skills and knowledge when addressing perpetrators and agree that there is demand for more programs and organizations that specifically address the needs of men who harm.
Middle shelf: potentially within reach
The middle shelf of the IPV supply room contains the knowledge, attitudes, and skills that participants depicted as being “within reach” for some general service providers but not all. Notably, this level of shelf becomes more accessible with a foundation of particular supports and experiences (described in the subsequent section). Nevertheless, given the idiosyncrasy that exists across organizational processes and individual practitioners’ experiences and training, middle shelf items–that is, one's ability to consider intersectionality and lived experiences when responding to IPV, to initiate culturally-sensitive community collaboration, to be reflexive, and to feel confident in one's capacity to respond–were only reflected in a minority of interviews.
Only a few participants reported working with individuals presenting with concerns of IPV through an intersectional lens that valued the individual's unique identity, experiences, and perspective. These participants described the importance of respecting the distinct history of each individual and emphasized the need to work with people “on their terms,” being open to learning from these individuals, and tailoring their services according each individual's unique needs. Relatedly, these same participants noted their conceptualization of a “woman as expert” in her own life and explained the value of believing the woman when it came to her perceptions of her situation, her safety, and her risk. Key factors that made a difference in fostering trust with women from vulnerable populations were described and included providing services and resources in different languages, hiring clinicians who hail from similar backgrounds as individuals seeking services, and forging relationships with community cultural centres. Finally, one participant highlighted the need to be reflexive in one's work–to question one's attitudes, values, habitual actions, and prejudices as it relates to working with vulnerable populations in particular–as an important piece of competently responding to IPV: You’ve got to process your assumptions and stick them in a jar somewhere and close that jar and work where the patient is and believe that patient. Regardless if they have been here 14 times intoxicated and today they are coming and telling you they were abused, we are believing them and going with what they’re telling us. And I see that as a move forward with staff is that we are a place where [patients] are believed more so than not (Participant 3).
In this way, some participants reflect some degree of access to the items depicted on the middle shelf. However, the prevailing perspective of most participants demonstrated the lack–and occasionally even the opposite–of these same considerations in their work. For example, several participants expressed doubt regarding their ability to consider the multiple and intersecting identities of their patients and specifically to understand “the complexity of the nuances of different circumstances and people's lives and the layers of identities that can contribute to privilege or oppression or marginalization” (Participant 5). Others noted that their own background–often different from that of their patients–made it difficult to understand these intersections. Still others noted some concern in believing a woman's own knowledge of her situation, suggesting instead that women over- or underestimate the risks they are experiencing, thereby making their reports unreliable. Many participant descriptions suggested a lack of awareness of existing cultural centres within their communities, or a continued disconnectedness from those centres that they were aware of: “Again, that's just that all of us in various agencies need to be aware of what one another does. I don’t think we’re very good at that either; I think we’re pretty siloed, all of us” (Participant 11). Finally, interviews with most participants included, to some degree, a recognition of racism, bias, and stigma towards vulnerable populations within their respective organizations and, at times, even revealed participants’ own biases. For example, despite working within Canada's socialised healthcare system, one participant described that their initial reaction to newcomer individuals assumed financial inferiority: “Whenever I hear ‘immigrant’ or ‘refugee,’ […] as soon as I hear that population, I think ‘oh my gosh, they are coming to a hospital and they can’t afford the bill’ regardless of what the issue that they’re coming for” (Participant 8). Other participants stereotypically characterized vulnerable populations through their descriptions, illustrating some vulnerable populations as “always being drunk,” or “relying on honour killings as the right thing to do,” as two examples (Participant 10). These statements reflect the persistence of biased perspectives within generalist care, leaving some participants “worrying that [these biased reasons] are what people blame [intimate partner violence] on, as opposed to actually responding to the violence” (Participant 3). Thus, although some participants are seemingly able to access those items on the middle shelf, they remain out of reach for a majority of providers.
Step ladder: a way to higher shelves
Those items depicted on the step ladder serve as supports that allow some generalist service providers to reach the above-described middle shelf, hereby leading to an overall improved–but often still insufficient, in that the top shelf remains out of reach–response to IPV. These facilitators include accumulated experience in the field, participation in IPV-focused trainings, and the presence of an organizational process to guide the IPV response.
Participants reported learning from prior experiences of addressing IPV as one way to hone their professional judgment and “spidey senses” (Participant 3). The process of becoming more confident and competent in IPV responses was described as one of “learning as they go” and “picking up skills over the years” (Participants 10 and 1) At the same time, many participants described their agencies as relying on a few specific, more experienced individuals to guide the IPV response.
In addition to simply accumulating experience, participating in training activities is a manner by which participants described becoming more competent and confident in their response to IPV. Whereas a few participants noted having received formal courses and refreshers over the years, most learning and training was reported to be completed informally (i.e., supervisory discussions, lunch-and-learns) and largely by choice (i.e., self-education, self-selection into relevant university courses, specialized practica).
Finally, existing IPV processes and procedures described by participants were idiosyncratic, with participants varying with regard to the degree of guidance that they receive from their respective organizations. Of the 17 participants in the present sample, only three were able to convey a clear, well-defined process that is routinely used to guide staff in responding to IPV. Six participants vaguely alluded to the existence of procedures and screening tools at their organization, but were unfamiliar with specifics, unable to provide details about these guidelines, or explicitly noted that they did not refer to those procedures themselves. The remaining eight participants reflected that the extent of any guidelines at their agencies were, at most, one-page pamphlets containing phone numbers for external services and described a desire for additional guidance: “We’ve got to get more structured on this” (Participant 7). Those few participants who did report having a top-down, systemic approach to responding to IPV at their organization, and who were able to explicitly describe the tools or processes they used, generally also endorsed feeling more knowledgeable and confident in their ability to address IPV. Likewise, the existence of guidelines and procedures co-occurred with reports of increased availability of training opportunities. For example, one participant explained the attitude toward IPV education and training at their workplace: [We have a] Violence Against Women Awareness Committee, which is pretty unique to this hospital […] The focus is to continue education for staff in the hospital around violence against women and constantly raising awareness of the issues and constantly training staff to know what to do. You know, with disclosures and suspicions of abuse; just to keep it present as it's an important health care issue. (Participant 3)
Overall, items on the step ladder are described as supports and experiences that promote a more comprehensive response to IPV. Yet, like higher levels of the shelves, even these step ladder items are not ubiquitous across all generalists’ experiences: formal trainings are scarce, with the burden of learning falling on the individual; experience is only accrued with time; and processes are inconsistently available and often nonexistent. Given participant descriptions, it may even be apt to imagine the step ladder in the IPV supply room as being frequently misplaced or missing altogether.
Ring, ring: relying on external referrals and mandatory reporting
When it comes to taking concrete, actionable steps to help men, women, and children in the context of IPV, service providers largely “reach for the phone”. Participants described relying on their ability to get in touch with other organizations, either to refer individuals externally or to follow through with their duty to report. For example, when working with women, all participants endorsed that they attempt to connect women presenting with concerns of violence to external services that may be able to provide them with more specialized support. The degree of involvement when doing so ranged from simply providing women with pamphlets for community organizations to reaching out themselves–with the woman's permission–to ensure a quick connection. Often, participants were able to name specific organizations within their communities to which they might refer women experiencing violence, such as women's shelters, advocacy and sexual assault centres, and victim, police, violence against women, and specialized mental health services.
When participants described potential steps to respond, address, and work with perpetrators around concerns of IPV, the vast majority similarly indicated that they would refer these men to other services. Yet contrary to external referrals for women, they were unlikely to provide the names of specific agencies or organizations. Instead, participants spoke more generally about “encouraging patients to seek treatment,” “directing people towards things and resources,” and “involving other agencies” (Participants 2, 7, and 14). Many agreed that they “need more education and more programs for perpetrators” (Participant 16).
In discussing their work with women who had children, every single participant mentioned, to some degree, their duty to report these cases to child protective services. Some participants described their duty to report as a default plan of action, negating the need to collect additional information or clarify the situation at hand: “We don’t necessarily have to assess the risk in those situations…we just need to have a reasonable suspicion and then we can make the referrals” (Participant 11). In some cases, the decision to report was described as being based on the mother's ability to protect her children, disregarding the fact that she herself was a victim: “If I felt that the mother wasn’t appropriately or unable to–for whatever reason–help protect the kids, then definitely Children's Aid” (Participant 3). Other participants explained that their duty to report, in the context of IPV, is often a “grey zone,” and that they attempt to balance out the risk of reporting to the individual presenting for services, as well as to any children (Participant 2). Nevertheless, reporting to child protection was described as a staple action item for general providers. As one participant put it, “the challenge when you involve CAS is often you’ve alienated the mother, so it becomes this really dicey situation. But, keeping in line, our obligation is to keep the children safe, right?” (Participant 1).
Blocking the door: barriers to an effective domestic violence response
Participants described factors that impede their ability to address concerns of IPV and prevent them from even entering the IPV supply room in the first place. Barriers included a lack of trust (in services, in systems, in helping professionals) by individuals seeking services and providers alike, a lack of resources, and systemic shortfalls.
Numerous participants reported that a lack of trust between patients and clinicians frequently impedes the process of both individuals disclosing, and practitioners addressing, abuse. One participant noted that, even when they suspect IPV, they are often powerless in their response if a woman chooses not to report any concerns: “If the person feels that they are safe, I can’t do anything…assuming that they’re competent” (Participant 1). Additionally, in the context of the initial, isolated, and short visits that typically characterize general care practice, it is difficult to communicate outcomes and build trust between service providers and their patients: One of the issues we had was with asking these questions in an initial interview, because families don’t trust and have not developed a relationship with you. Families don’t want to say these things because it is reportable. (Participant 9)
Over and above mistrust on the part of the patients, participants reported their own lack of trust in the existing systems. The worry is that current systems are neither coordinated nor organized–and therefore inadequate–to help women even if they, as clinicians, attempt to get them help. The difficulty, unease, and lack of clarity in navigating the greater system–not only for women, but for service providers and practitioners–leads to overall cynicism: “I wish they’d make it easier. I need to walk [women] through it [to access services] and have to get higher authorities involved before they can access. It's a brick wall and red tape […] the system is overloaded” (Participant 12). One participant described a situation in which they were unable to help a woman qualify for needed services due to bureaucratic reasons: “The woman herself had charges–she was considered a perpetrator–and was not eligible for service with [community organizations…] she got swapped up in charges that really belong to her husband […] She still remains at risk from him” (Participant 7). On top of mistrust, participants described that their organizations are generally lacking the resources to ensure necessary training and supports: “[We] neither have the expertise, the staff, nor the money” (Participant 4). Even those institutions that “believe in training staff around violence” are described as having difficulty “doing it in the new budgetary way,” resulting in it being more and more “impossible” to continue training nurses and other generalists in responding to IPV (Participant 3).
Finally, participants reported several systemic shortfalls related to the context of their work in a general care setting that get in the way of an effective response to IPV. One participant, speaking from their role in an emergency setting, explained that “it's not that I don’t want to…it's just time” (Participant 17). Another noted that the process of querying and responding to violence would add an extra layer of paperwork that “would be far too much” (Participant 15). Additional systemic barriers centred around the structure of service provision. For example, one participant touched upon the nuances of patient care in a hospital setting, noting, “It's tricky–they have to be a patient of the hospital. We’ve had cases where it's been disclosed that the partner is abusing and they’re there, but we can’t do anything unless they’re a patient” (Participant 3). Overall, general mental health and healthcare was described by participants as a system that often neglects to assess the whole person within the context of their relationships and environment, resulting in mis-appropriated services and an inability to appropriately respond to IPV.
Discussion
This study sought to examine current practices, attitudes, and perspectives of general health and mental health service providers across Canada as they relate to assessing and responding to IPV. An analysis of interviews with 17 participants revealed consistencies–both encouraging trends and glaring absences–in the manner that these professionals understand, talk about, and address risk and safety.
Promising practices
The present study reflected some promising practices in generalists’ understanding of IPV. Participants demonstrated a sufficient knowledge of potential behavioural indicators of abuse, such as increased use of health services, implausibly explained physical injuries, and deference to a partner, as well as specific evidence-based risk factors, such as recent separation, excessive alcohol and/or drug use, financial strain, and prior history of violence. In light of widespread calls over the past decade for broader knowledge about IPV in health and social services (Ontario DVDRC, 2019; WHO, 2013), these are encouraging findings. Consistent with guidelines for generalist service providers (VEGA Project, 2019), many participants also described their capacity to refer community and specialist services for women presenting with concerns of IPV, though referral sources were often only vaguely described.
Gaps in service
The results also revealed gaps in service providers’ knowledge of IPV. Lacking was a comprehensive understanding of the needs of children and perpetrators as well as a consistent application of the nuances of working with diverse populations. While participants frequently referenced mandatory reporting regulations in the context of working with women who had children, there was no mention of child-specific risk assessment and management practices and limited focus on effectively addressing children's needs. This is consistent with prior findings in both generalist and specialist services (Reif et al., 2020). Participants similarly reported that the perpetration of IPV is largely unaddressed in their work, despite the growing literature suggesting high co-occurring rates of mental health problems, violence perpetration, and service use (Scott et al., 2020; Shorey et al., 2012). Furthermore, only a handful of participants endorsed those aspects of response that appreciate intersectionality, involve reflexivity, and allow for a more tailored approach that considers cultural and lived experiences. The present data, along with recent work examining the unmet health needs of distinct populations in Canada, demonstrates the implicit and explicit bias and racism that prevails in general care (Kitching et al., 2020; Marchand et al., 2015; Nelson & Wilson, 2018). Participants, through anecdotal examples, described the stigma and discrimination experienced by individuals who were disadvantaged primarily because of differences in social positioning related to factors of class, gender, and ethnicity which, in turn, influenced the quality of care that generalists provided after disclosures or suspicions of IPV. The impact of these prejudices has the potential to be all the more damaging in the context of IPV given the already heightened risk of Indigenous and newcomer populations in the victimization and perpetration of violence–vulnerabilities that largely exist in the first place because of discrimination, colonialism, and racism (Garcia-Moreno et al., 2015a).
Thus far, this discussion has considered individual-level factors relating to the knowledge, attitudes, and skills of independent general service providers. Yet, perhaps the most relevant and concerning implications of the present study are those related to the systems and structures–those items on the step ladder–that are (or are not) in place to support IPV responses in general care settings. Of greatest significance, the present results suggest that a consistent and empirically supported approach to IPV assessment and response is rare to find across generalist service provision. Most participants were unable to provide any description of well-defined institutional or organizational guidelines governing their response to IPV. This is critical as general service providers, including nurses and mental health clinicians, have elsewhere recognized formal training and standardized procedures as key facilitators to improved IPV practices (Beynon et al., 2012; Burns et al., 2021; Leppakoski et al., 2014; Olive, 2007). In lieu of protocols and training, interviews revealed an overreliance on experience in the field; participants endorsed acquiring IPV knowledge primarily by learning on the job and depending on experienced clinicians to direct IPV follow-up. Prior work has similarly demonstrated that more experienced (and often older) clinicians are more likely to inquire about IPV and report greater comfort when working with women experiencing violence (Beynon et al., 2012). In reality, both formal organizational supports and individual experience are associated with practitioners’ increased feelings of preparedness, self-confidence, and control, as well as decreased feelings of anxiety when responding to IPV (Gutmanis et al., 2007). However, whereas experience is indispensable to improving one's ability to respond, this accumulation of knowledge in generalist provision often relies on a few individuals who possess a combination of many years in practice, prior specialization in IPV-related roles, and personal life experience–all easily undermined by changes in personnel. Training and guidelines, on the other hand, have the potential to be implemented at an organizational level to improve the responses of many providers. These, however, are often contingent on institutional and systemic priorities that may not yet exist (Garcia-Moreno & Watts, 2011; Rutherford et al., 2007).
Implications
Efforts to improve the IPV response in general care have largely focused on individual-level change, using educational campaigns that target service providers’ knowledge and attitudes (Turner et al., 2017; VEGA Project, 2019). The present study likewise highlights a continued need for increased individual knowledge specifically related to working with children and perpetrators. Yet, even more strikingly, these results suggest that further improvement in generalists’ responses to IPV necessitates top-down change at a system-level. Individual practitioners in the present study, for the most part, possess the basic knowledge to identify IPV and ascertain when a more extensive course of action is needed. What is required to guide practice beyond this point is a closer examination of existing organizational practices, as well as the reinforcement of inter-organizational collaboration between generalist and specialist services. In lieu of focusing solely on increasing individual knowledge, organizations–as well as the greater system–must bear the responsibility of ensuring the fundamental conditions that allow providers to confidently respond to IPV. This should include, as several examples, transparent referral networks, clear guidelines and protocols, regular training with feedback mechanisms and established trainers, boundary individuals to bridge connections between services, strong leadership, and the overall prioritization of IPV as a key healthcare issue (Basu & Ratcliffe, 2014; Dowrick et al., 2020; Garcia-Moreno et al., 2015b; Leppakoski et al., 2014). Relatedly, the present study revealed barriers to health equity that were reinforced at the level of both individuals, through racism, and systems, in the form of structural violence. Indeed, shortfalls in institutional policies and priorities are often linked to gaps in individual practice. Addressing such concerns, for example, might involve training that introduces practitioners to equity-oriented and trauma- and violence-informed care. Such a change is reflective of the prioritization of IPV at a system-level such that even the dissemination of knowledge to providers extends beyond individual risk factors and appreciates that violence is strongly related to health inequity, social determinants of health, and social justice (Ford-Gilboe et al., 2018; Varcoe et al., 2014). Overall, improving the IPV response in general service provision will require a broadening of the lens beyond that of the individual practitioner and towards the system at large.
Limitations
This study should be reviewed in the context of its limitations. Inherent to secondary data analysis, the authors were limited to answering the present research questions within the confines of the collected data and existing participant pool. Given the nature of the interview data, certain participant characteristics were difficult to ascertain at times (i.e., gender, age, years of experience). Although all participants hailed from general health and mental health services, there was significant variability in their specific roles, their experiences, and the populations with which they work. Furthermore, the present sample included participants from both health and mental health sectors–settings which may present with inherent differences in barriers, attitudes, and practices. Despite this variability, the present results and discussion attempt to capture the voices of all included participants. Finally, in considering sample selection, it is also important to acknowledge that participants who agreed to participate in this study may have been more motivated to take part in work addressing violence relative to those who did not agree to participate and who may otherwise have lower engagement with the issue of IPV. Most participants also reported working in Ontario, limiting the applicability of these findings to service provision across Canada.
Conclusions
In sum, individuals experiencing and perpetrating IPV are frequently in contact with the general healthcare system, which must be prepared to respond. Shedding light on current practices of general health service in this area reveals that providers are motivated to help individuals experiencing IPV but frequently lack the organizational direction for an effective response. Individual knowledge-building alone will not suffice in improving general service responses to IPV; what is needed is system-level change. It is our hope that greater institutional prioritization of IPV and improved collaboration and integration of generalist and specialist services will result in improved IPV outcomes.
Footnotes
Acknowledgments
Data pertaining to this manuscript was collected as part of the Canadian Domestic Homicide Prevention Initiative with Vulnerable Populations, co-directed by Myrna Dawson and Peter Jaffe.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada, (grant number 895-2015-1025).