
Abstract
Minimal research has explored the personal experience of burnout in doctors from any medical speciality. Consequently, we aimed to provide a relatable description and understanding of this globally recognised problem. We employed an interpretative phenomenological analysis (IPA) of face-to-face interviews with seven general practitioners (GPs) in Northern Ireland, having selected interviewees best able to speak about burnout. We sought to understand how these GPs understood their burnout experiences. Our participants’ continuous work involved more than their busy weekdays and also working on supposedly off evenings and weekends. In addition, draining intrusive thoughts of work filled most, if not all, of their other waking moments. There was no respite. Work was ‘always there.’ Being constantly busy, they had no time to think or attend to patients as doctors. Instead, participants were going through the motions like GP automatons. Their effectiveness, efficiency, and caring were failing, while their interactions with patients had changed as they tried to conserve their now-drained energy and empathy. There was no time left for their families or themselves. They now “existed” to continuously work rather than “living” their previous, more balanced lives that at one time included enjoying being a doctor. Worryingly, participants were struggling, isolated, and vulnerable, yet unwilling to speak to someone they trusted. We intend our burnout narrative to promote discussion between medical colleagues and assist in its recognition by GPs and other doctors. Our findings warn against working excessively, prioritising work ahead of family and oneself, and self-isolation rather than seeking necessary support.
Keywords
Introduction
Burnout in doctors is important because its widespread, damaging consequences impact not only their physical and mental well-being (Lee et al., 2008; Lheureux et al., 2016) but also their patient care and health-organisation effectiveness and costs (Sinsky et al., 2022; West et al., 2018; Williams et al., 2007). Although considered worryingly common and a “global crisis” (Lancet, 2019), what authors consider “burnout” to be is often unclear (Merriman, 2020) or described without supporting references (Best, 2021). The most common references are to the Maslach Burnout Inventory’s (MBI’s) “emotional exhaustion,” “depersonalisation,” and “reduced personal accomplishment,” a three-part burnout model developed for measurement purposes only (Maslach et al., 1996).
This qualitative research explored the personal burnout experiences of general practitioners (GPs), also referred to as family doctors (FDs) or family physicians (World Organization of Family Doctors, 1972). These doctors uniquely provide personal, generalist, holistic care in a family context (Jamoulle et al., 2017). Our GP research advisors doubted that the MBI’s solely work-related, somewhat impersonal, and non-doctor-specific terminology would be sufficient or even used by medical colleagues to explain and discuss their possibly wide-ranging burnout concerns. All agreed there was a need, as one advisor expressed specifically, for “a description and understanding of burnout from GPs and primarily for GPs in language they would use and understand” (McCammon, 2018, p. 70). Crucially, the large volume of quantitative GP research (Karuna et al., 2022; McCammon et al., 2023) cannot address this need where an in-depth description and understanding requires qualitative exploration (Polit & Beck, 2014).
Qualitative Exploration of the Personal Experience of Burnout in Doctors.
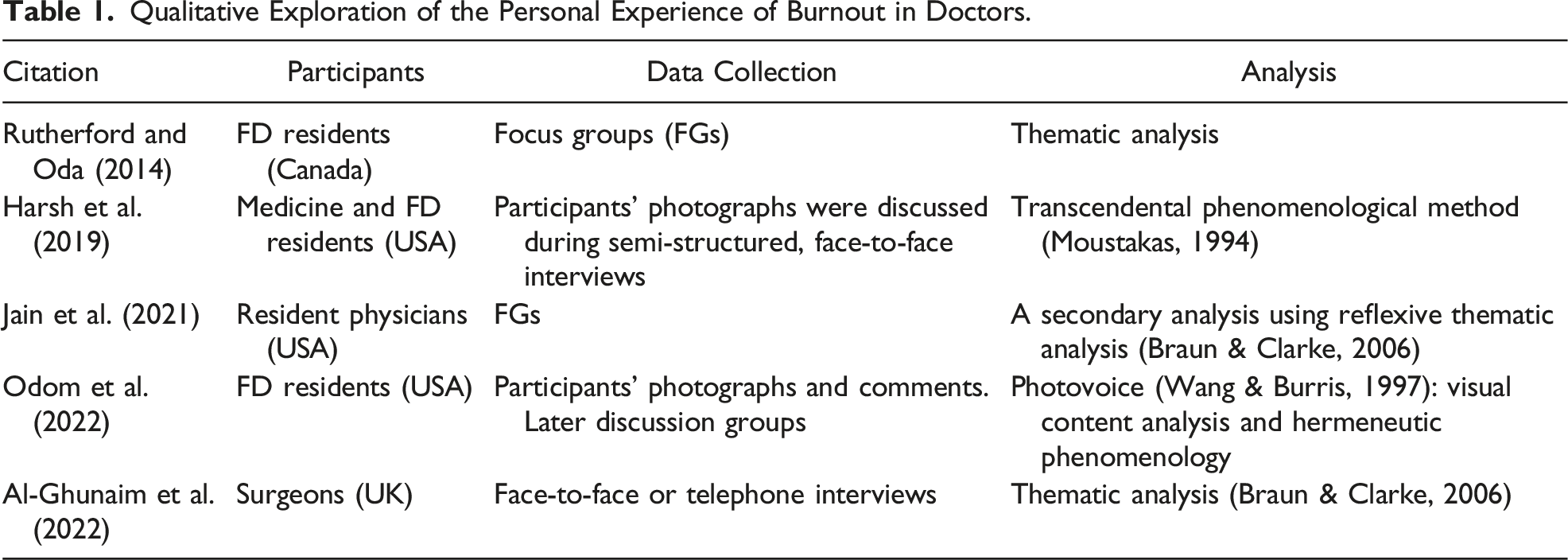
These doctors were overwhelmed by workload and pressure (Odom et al., 2022), with their performance and patient care (Al-Ghunaim et al., 2022) and relationships with patients (Jain et al., 2021) detrimentally impacted. Any enjoyment had gone (Harsh et al., 2019), replaced by exhaustion (Rutherford & Oda, 2014) and sometimes depression (Odom et al., 2022). Furthermore, this pervasive negativity had spread to affect the doctors’ personal and family lives (Al-Ghunaim et al., 2022; Jain et al., 2021). Regarding methodology, three studies explored what was apparent from reading the participants’ accounts rather than seeking deeper access to latent themes through interpretation. Odom et al.’s (2022) Photovoice and Jain et al.’s (2021) Reflexive Thematic Analysis did incorporate interpretation. To select participants, all used convenience sampling without attempting to identify burnout objectively. Personal experience of burnout was a prerequisite for Harsh et al.’s (2019) and Odom et al.’s (2022) interviewees but not for Rutherford and Oda’s (2014) FD residents. However, they shared personal burnout experiences during their focus groups. It is unclear whether Jain et al.’s (2021) or Al-Ghunaim et al.’s (2022) research required burnout self-identification. Notably, three studies involved FD residents and their training, but we did not identify qualitative research involving qualified GPs/FDs.
To address these methodology and knowledge gaps, we qualitatively explored the personal experience of burnout in qualified general practitioners, including what might be beyond the participants’ own understanding. In response to our advisors’ recommendations, we aimed to provide a description and understanding of burnout to which other GPs can relate.
Method
Research Design
We began by choosing a research approach that, because of its epistemological and ontological philosophical assumptions, could provide the type of knowledge required to answer the research question: How do GPs describe and make sense of their personal experience of burnout? Consequently, we employed interpretative phenomenological analysis (IPA) based on its phenomenology, hermeneutics, and idiography foundations (Smith et al., 2009). Researchers familiar with these philosophical foundations produce “more consistent, sophisticated and nuanced analyses” (Smith et al., 2009, p. 5). As a key IPA tenet, the researcher engages in a “double hermeneutic” to make sense of the participants trying to make sense of their experiences. Interpretative phenomenological analysis’ interest is in “understanding how particular experiential phenomena have been understood from the perspective of particular people in a particular context” (Smith et al., 2009, p. 29). Bracketing off preconceptions and prior experiential knowledge was a major challenge because our lead researcher (LMcC) believed he experienced burnout when he was a GP. To address this challenge, our analysis went back and forth between a reductive focus on the participant’s experience and LMcC’s reflexive self-awareness of his own (Finlay, 2008). Consistent with Smith et al.’s (2009, p. 35) description of dynamic “cyclical” bracketing, this back-and-forth provided a means to bracket LMcC’s experiential knowledge while allowing its use on occasions to “sound out” interpretations (Smith et al., 2009, p. 89).
Sampling, Eligibility, and Screening
Qualified GPs who believed they had experienced burnout and worked five or more half days Monday to Friday in general practice were invited to complete Maslach et al.’s (1996) MBI for screening purposes. Our purposive selection seeking those who could speak best about personal burnout required both their subjective belief of having been affected and an objective identification of burnout. However, no evidenced means of burnout diagnosis was available (Korczak et al., 2010). Although also without diagnostic ability (Maslach et al., 2020), the MBI became our preferred screening tool due to being the most commonly used measurement instrument across all professions (Korczak et al., 2010), including GPs (McCammon, 2018). The MBI’s three components are reported separately as high, average, or low. Our interviewee selection criterion was the combined pattern of the components’ score ranges that were individually associated with greater burnout: High Emotional exhaustion (≥27), High Depersonalisation (≥10), and Low Personal Accomplishment (≤33) (Maslach et al., 1996). This article’s “HHL:MBI” abbreviation incorporates the most unfavourable score range “H,” “H,” and “L” capital letters.
Recruitment
Interviewee Characteristics.
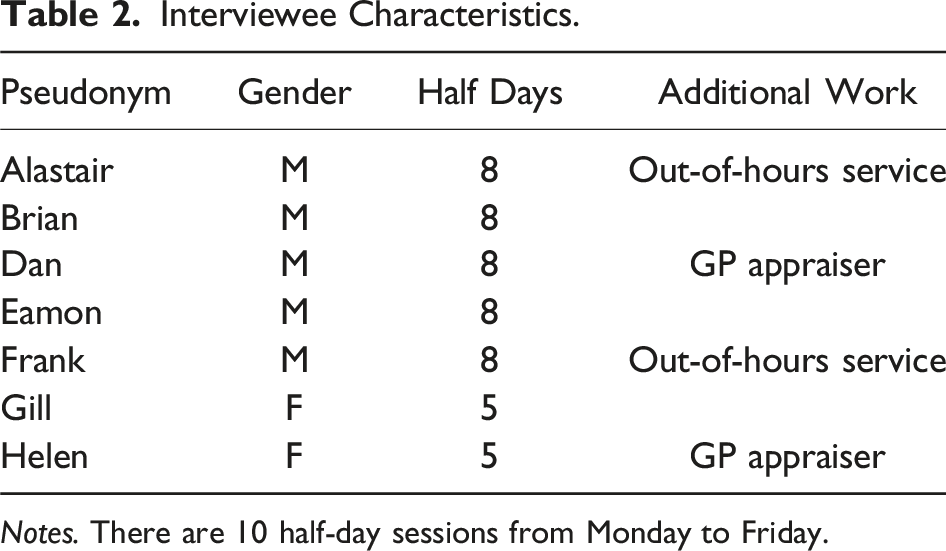
Notes. There are 10 half-day sessions from Monday to Friday.
Ethics and Safety
The Office for Research Ethics Committee Northern Ireland (No. 14/NI/0038) approved our information and support leaflets. It also stipulated our responsibilities should interviewee or patient safety issues emerge during the interviews. To this end, the consent form included permission to contact the interviewee’s employing organisation or nominated doctor for advice if concerns arose. This inability to guarantee anonymity and confidentiality in these circumstances was made clear in the Interviewee Information Sheet. Written, informed, pre-interview consent was obtained by LMcC.
Data Collection
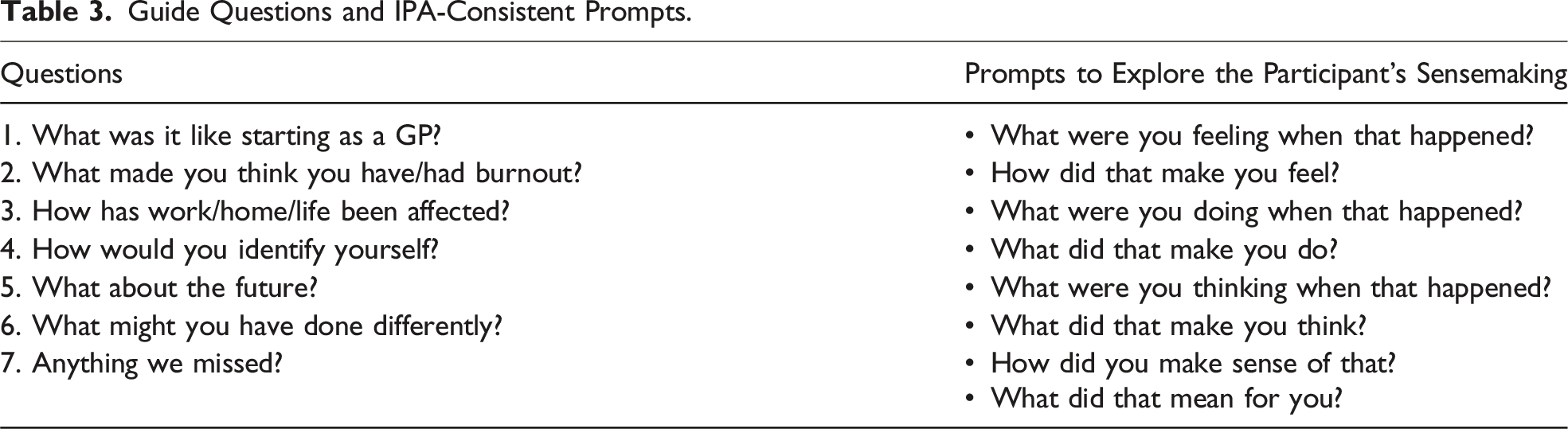
Guide Questions and IPA-Consistent Prompts.
Analysis
Guided by Smith et al.’s (2009) analysis framework, data immersion began with repeated ‘listenings’ to the recording and transcript readings, initially noting anything of interest in a research diary. A word-processor transcript table recorded every detail of the subsequent close, line-by-line exploratory commenting. Each commenting lens was colour-coded for clarity: descriptive (recording what the interviewee made apparent), linguistic (taken from the interviewee’s use of language), and conceptual (interpretative). We likewise differentiated reflexivity comments concerning LMcC’s burnout experience and separate insider knowledge as a GP. This transparent, meticulous computer record of each analysis facilitated demonstrating thoroughness (rigour) and our idiographic commitment at the multiple-case level: the origin of each theme is traceable to a particular word or phrase within individual transcripts (Smith et al., 2009).
The essential psychological substance of these comments was developed into experiential statements and brought together through abstraction and subsumption to become personal experiential themes (PETs). We then constructed a table to illustrate the PET connections for that participant (Smith et al., 2022). Participants did not member check their analysis for validation purposes because the interpretations could have been beyond their understanding of their burnout experience (Cohen & Crabtree, 2008).
We completed each case before moving to the next (Smith et al., 2009), which required additional bracketing of any changes to the previous preconceptions that might have occurred during the preceding case(s). Having concluded with seven individual PET tables, we compared these to create seven group experiential super-ordinate themes (GETs).
The lead researcher (LMcC) undertook all the analyses, but interpretations, themes, PET tables, and GETs were developed with the co-authors. Our IPA advisor later reviewed these analyses to confirm that the interpretations were credible and supported by the data. However, we acknowledge that other credible interpretations were possible in keeping with interpretivist epistemology (Osborn & Smith, 1998). Consequently, we cannot claim the absolute and only truth about GP burnout. Also, thematic saturation is problematic in IPA due to its focus on small samples and its iterative, circular, and potentially unending analysis in pursuit of idiographic detail (Brocki & Wearden, 2006). Rather than saturation, we sought a coherent, persuasive account with nuance (Brocki & Wearden, 2006; Nizza et al., 2021).
Findings
Our findings are presented as a narrative driven by the first super-ordinate theme, Continuously Working, which goes beyond the heavy workloads and long hours that are apparent to others. The unseeable continuing responsibilities, problems, worries, and doubts were perhaps even more exhausting because not even the participants’ thoughts allowed time for anything else but work. Our narrative incorporates the other super-ordinate themes as Continuously Working’s sequelae: Too Busy to Think or Work as a Doctor; Drained Personal Resources; Efforts to Conserve Personal Resources and Protect Themselves; Family and Work, You Can’t Square that Circle; Existing, Not Living; and Isolated and Vulnerable.
Continuously Working
All the participants complained of too much work, insufficient time, and unrelenting pressure. Weekdays began at the surgery before 8:30 a.m. with paperwork and checking results. Patient consultations then commenced at 9:00 a.m. and finished around 11:30 a.m. There was no longer time for coffee or chats with colleagues ahead of house calls. Participants ate sandwiches “on the hoof” (Brian) before returning to the surgery around 2:30 p.m. to repeat the morning cycle, with patient consultations often overrunning to finish after 6:00 p.m. Helen described the lack of respite best using deliberately slow staccato for emphasis: “Your brain hasn’t stopped. It—just—does—not—stop.”
However, even when not on call, work did not end when the surgery finished. You would think that by the end of the day, you would just close your case and drive down the road to the loving wife and kids, not have to worry and say, I have done a good job today. Everything has cleared up. All the books are closed. I’m happy. But that never happens in general practice. (Eamon)
Unfortunately, Eamon never realised his reasonable expectations of some well-earned rest and family time. Instead, he returned home not with satisfaction or contentment but with worries and work still to do. Everyone regularly did paperwork and checked results remotely from home or by returning to the surgery after dinner, on half days and at weekends when supposedly off. Work never seemed to stop, but Eamon’s worries represented another more subtle and possibly even more exhausting form of labour. Draining ruminations concerning work continued even when the participants did not appear to be working. Frank recalled his worries on the several occasions when he broke down in tears at home with his wife because of the amount of work he still had to do. Letters had to be cleared, or the referrals had to be done, or whatever else had to be (done), patient disability claim forms or whatever.
Similarly, Gill described “that Sunday night” apprehension concerning the next day’s work, but her foreboding also regularly occurred midweek. Her distress could only end when she eventually fell asleep, but it was there again the instant she awakened. Alastair was explicit: “(I) just worry and ponder over things and can’t stop thinking about them. […] Just can’t switch off.”
In summary, work for the participants had gone beyond what was done or apparent to patients or colleagues. Silent, invisible, pernicious thoughts of work continued when seeable and tangible work had ceased. Now, there was not even respite inside the participants’ heads. Now, work was always there. Work had become ‘Always.’
Too Busy to Think or Work as a Doctor
Each participant now found it more difficult to get work done. Gill worried that despite her efforts, she was “not fully achieving anywhere,” but everyone had similar concerns. Brian “just couldn’t function effectively,” and Alastair said, “I do get stuff done, but I just don’t think I jump to things as quick.” Eamon explained, “I am much more efficient whenever I am emotionally well […] because I am more confident.” He continued, when you are emotionally tired, you find yourself using all sorts of things to make decisions for you … a full blood count to make sure everything is all right and then I’ll decide what to do. Whereas, when you’re on tune, you find yourself saying, you’ll be all right.
Likewise, when especially busy, Frank’s approach was “to kick it down the road and we’ll come back to it.” However, patient problems, results checking, and decisions were being deferred to when it would still be busy, making future situations even busier. Eamon and Frank had created a burnout-perpetuating cycle where they still had to address the subsequently mounting workload, which was likely to contribute to greater burnout and further work deferral.
Disengagement from their professional roles and responsibilities also affected decision-making, including referrals, which was another issue for Eamon and others. So let’s say a patient with a headache wants referred; you are more likely to refer them for an unnecessary investigation [...] You are more likely to prescribe an antibiotic when you know nothing is wrong. (Eamon) (Dan, to his patients) I don’t think this is a serious thing. Do you want referred? I’ll give my opinion and then ask them what they want done, and I’ll just go along with that.
Both had increased their referrals. Eamon was more readily responding to patient pressure, including for unnecessary antibiotics. Dan, almost as if he had given up, was now leaving patients to decide whether, in effect, to refer themselves to outpatients. Previously, they would have questioned the patient’s complaint, explained their opinion, remained true to it, and then decided on reassurance, medication, or advising referral as indicated. Sadly, both were disengaging from their years of experience, knowledge, and responsibilities to their patients as doctors. Instead, they were now simply writers of often unnecessary referrals and prescribers of unwarranted antibiotics. Mirroring Eamon’s and Dan’s self-deprofessionalisation to become mere technicians, Gill spoke of “going through the motions,” suggesting disinterest, mindless monotony, and weary resignation. This was what general practice had become for her. Like Eamon and Dan, she was no longer giving her best as a doctor. Gill and others were now production-line operatives, GP automatons, mechanical devices running out of steam. Helen’s “just do it” similarly gave the impression of being an automaton, but she provided a worrying additional insight: “You get very little time to reflect on the job which you do. You just do it.” Like other participants, Helen no longer had time to think or engage her doctor’s thought processes as she once did. This interpretation raised the possibility of more poor decisions, misjudgements, mistakes, and quality of care and safety issues.
In summary, the participants were no longer working effectively or efficiently. They were too busy continuously working to use their expertise or properly think and, therefore, too busy to attend to their patients as doctors. They were also losing their previous capacity to care, which is part of the next theme.
Drained Personal Resources
Continuously working had drained the participants’ energy and empathy. All were tired, as evident in Frank describing getting home after a busy week, “I’m wrecked … just knackered, and if you leave me long enough here, I will just fall asleep.” Most had also experienced profound exhaustion like Helen: “Drained … drained. Physically and mentally absolutely drained.” In addition, almost all recognised a reduced capacity to care for their patients. Gill described being “detached emotionally,” and Frank confided, “It is harder to care. It is harder to give one hundred percent the way maybe you used to.” Likewise, Helen said, “I’m not sure I have as much to offer them. I’m not sure I have the reserves anymore.”
Gill, Frank, and Helen had noticed changes in their reserves or maybe even in their desire to care, but Eamon went further. He admitted, “I stopped caring about the patients [said with surprise and guilt]. I didn’t really have empathy for them.” Relying on the fieldnote for a moment, not only did Eamon recognise he had changed, but he was surprised, felt guilty, and appeared concerned that his capacity to care was no longer what it should be. Our analysis reflected on how passionately he had spoken about palliative care earlier in the interview. Consequently, we concurred with the fieldnote’s “surprise and guilt” because it seemed clear that caring was at the heart of being a doctor for Eamon. All the participants held this belief and were also likely to be concerned about their failing empathy.
In summary, energy and empathy reserves were drained, causing participants to be concerned that their capacity or desire to care had diminished. The next theme describes how they tried to conserve these personal resources.
Efforts to Conserve Personal Resources and Protect Themselves
The way all participants viewed and interacted with patients had changed. Gill grumbled, “they’re just a nuisance,” and Alastair had become “nearly callous with people and finding nearly every patient that came in a [… unfinished comment].” A previously very approachable Brian described the change best when he revealed his uncomfortable realisation. To be honest, I didn’t like them. I was probably curt, probably rude […] instead of being friendly and welcoming, I saw them as an intrusion into my life. I saw them as the problem.
“To be honest” suggested an apology, Brian realising and regretting his unfairness to patients justifiably seeking assistance. This depersonalisation of patients by all participants, including Brian seeing them “as the problem,” seemed to be a protection mechanism. It would be easier to conserve their energy and empathy by avoiding giving of themselves if patients were considered “nuisances” rather than sick people needing help. Worryingly, Alastair’s “wanting to get finished and through on to the next one,” and equivalent remarks by the others, warned not only of depersonalisation but also of less time spent with each patient. This again raised questions, as with having less time to think, about the quality and safety of the patients’ medical management.
Helen adopted a different means of protection: “I’m starting to put up barriers because I have to keep myself safe.” Here, she must have felt at risk or even harmed already because of being too close and empathising for too long without thinking of herself. She later described putting on a “front” when emotionally drained, with Gill likewise putting on a “mask” in order to get through her consultations.
In summary, our participants attempted to conserve their personal resources and protect themselves by depersonalising the patients and no longer giving as much of themselves. Due to continuously working, participants also could not give as much of themselves to their families, which leads to the next theme.
Family and Work, You Can’t Square That Circle
Each participant’s family and their own family life were affected by continuously working. If you’re working all the hours that God sends, you’re not spending time with your family. I mean, it is as simple as that. You can’t square that circle. (Brian)
All described their families losing out. Gill admitted, “I find when I’m working, I’m much more irritable and short when I come home.” Even her young child, who often asked, “You had a busy day today mummy?,” was aware of Gill’s brought-home pressure. This pressure also impacted spouses, who were becoming frustrated and angry. Frank said his wife was “fed up with the amount of times I’m out,” and Eamon shared about his wife, she would get annoyed whenever I would go off for a couple of hours to do work whenever the kids are in bed, and she wants to spend time with me.
Eamon’s double “whenever” pointed to him regularly working at home and his wife feeling neglected. Even more troubling, working excessively had contributed to other participants’ significant marriage problems. There seemed a tug-of-war between work and family life, but in reality, there was no contest. I think my family was the most important thing, but when anything turned up with a patient, you would expect your family to take second place. (Dan) I just felt cornered. I was stuck. There were expectations of me from both directions, family on one side and work on the other side, and I just couldn’t please both sides. And work wasn’t going to be sympathetic. Work had to be done. (Frank)
Here and from all the participants’ accounts, we interpreted the needs of patients (Dan) and the demands of work (Frank) as leading to Continuously Working. Both these commitments were non-negotiable, and it seemed the family always had to accept second place and fit in around the GP’s work, including when supposedly off. As with Eamon’s wife after the kids’ bedtime, inevitably, the families lost out.
Participants lost out on family life too, like Helen: I’m looking to retire from medicine to being a grandmother. To take on a nice role and to do all the things that you didn’t do as a mother.
Helen had already been thinking about the many things she missed with her children. Now, she was hoping for a second chance. We reasoned that in looking forward to doing what she had missed, Helen revealed deep regret at previously prioritising work ahead of her family and herself. In contrast, Gill always believed herself a family person “first and foremost,” but all the others shared Helen’s realisation about misplaced priorities and the same regrets. Frank powerfully expressed the depth of his feelings about those years working off-duty evenings and weekends: “stupid times, a waste of family time. It was a misuse of family time.” We further interpreted the participants’ unsettling realisations and regrets as them coming to believe that prioritising being a GP had caused harm to their families and likely themselves, including burnout.
In summary, the regretted prioritisation of work left little time for family life, affecting the participants’ wives, children, and themselves. The next theme explores another “unsquarable circle” involving work and personal well-being.
Existing, Not Living
Continuously working diminished the participants’ well-being and also left little time for a personal life. All were tired or even exhausted. Nearly all felt “down” at times, but Brian had past severe depression with significant suicidal thoughts, and Gill recently resumed antidepressants. Like Frank feeling “cornered” and “stuck,” others anguished over their own work–family dilemmas. However, Alastair’s response when asked about his remaining years in general practice was the darkest: “Sometimes you think, I wish I had cancer just to get out of that [laughs].” His instant “it’s a flippant remark” dismissal and out-of-place laugh suggested he feared being taken literally. Instead, we interpreted an unguarded glimpse of just how very despairing and desperate Alastair could feel at times.
Regarding a personal life and friends, Brian described the underlying problem faced by everyone. You spend all your time working. You lose contact with your friends. This concept of GPs playing golf, I don’t know where people get that idea from.
“Golf” was Brian’s metaphor for time he might spend purely on himself, which he never did. Dan succinctly conveyed the same social isolation and limited personal life that affected all participants: “It was an existence; it wasn’t a life.” In the context of Dan’s comment and for the other participants regarding life generally, “existing” rather than “living” was interpreted as having lost much, maybe even all, of their previous happiness, hopes, and fulfilment expressed elsewhere in their interviews.
Reflecting on work, each participant also described happier times as a GP in the past. Now, across the seven analyses and in keeping with “going through the motions,” the participants’ work-related energy, enthusiasm, job satisfaction, and enjoyment were less or had likewise disappeared. Instead, there was pessimism and a blanketing negativity. Increasingly, work was somewhere the participants did not want to be. Consequently, we considered them as also “existing” in general practice where they once flourished. Gill’s existential doubts, “should I have done medicine at all?,” were in keeping with “existing” rather than “living” as a GP. Paradoxically, despite otherwise “existing” as a GP like Gill, all other participants spoke positively about their vocation in the present tense.
When describing why she studied medicine, Helen said, “very definitely to help people, and I still believe there is no better job for helping people.” Similarly, Brian proudly stated, “we are all trying to do good to people in this job,” but Frank best illustrated this continuing sense of vocation. Overall, it is a super job. It ticks a lot of boxes for job satisfaction and doing something useful and meaningful. Helping your fellow man and stuff like that, and (at a) sort of humanitarian stroke spiritual level, it’s very worthwhile.
Regardless of their miserable times and complaints about burnout’s widespread consequences, these participants did not question their vocation to care for patients, which they still believed was meaningful.
In summary, rather than “living” a life of energy and joy away from work and when working, our participants were merely “existing” in both settings. Continuously Working was now their anaemic, lifeless existence. This existence included isolation and vulnerability, which provides the concluding theme.
Isolated and Vulnerable
Only Brian and Gill had consulted health professionals about their difficulties. When asked about speaking to anyone, Alastair’s extended musical “NnoOOoo” (rather than simply “no”) suggested this was totally unthinkable for him. Likewise, along with other participants, Frank discovered that his practice partner had also completed our questionnaire. Referring to the rigours of daily work, a somewhat surprised Frank was “worried then in a sense about my partner because I thought they were dealing with it well.” Notably, both GPs were concerned enough to complete the questionnaire, but neither seemed willing to share their burnout worries with the other. Eamon was explicit. When he was talking about burnout, being stressed and his practice partners probably feeling the same way, the interviewer asked if they had ever discussed such things together. Eamon quickly replied, “No no,” as if this was again unthinkable, mirroring Alastair above. The lack of openness from Eamon, Frank, and their partners pointed to them hiding their difficulties and being uncertain about seeking support, providing further evidence of self-imposed isolation like Alastair. We considered that this self-isolation was likely to be associated with vulnerability.
In fact, almost all the participants seemed vulnerable in some way. Helen worried about being able to continue practising safely, and Eamon was concerned about his future health. Brian expected another crisis initiated by the employing healthcare organisation that he described as “the enemy,” although nearly everyone complained about being under attack. Alastair colourfully described the spread of criticism best. What always got (me) really angry was when you just thought you were working yourself to the bone […] the public and the papers and the media and the politicians were still shitting on you and saying that you were doing a terrible job.
We interpreted that Alastair and the other participants would have felt professionally vulnerable because their hard work was being attacked rather than appreciated. In addition, their vocation to care for patients as part of their life’s meaning was also under attack, leading to existential vulnerability.
In summary, and to conclude the findings, isolated and vulnerable participants who could have benefited from speaking to a colleague or a medical professional were reluctant to seek support. This is one of the issues for discussion.
Discussion
This in-depth exploration of the personal experience of burnout in general practitioners adds to the small body of qualitative research involving any medical speciality. Our burnout narrative is driven by Continuously Working, which goes beyond being busy on weekdays and on supposedly off evenings and weekends. Work and intrusive thoughts of work filled most, if not all, of the participants’ waking moments. Work was now ‘Always,’ with participants too busy to get work done. They had no time to think or attend to patients as doctors. Instead, they were going through the motions as mere technicians or automatons. Their effectiveness, efficiency, and caring were failing, while their interactions with patients had changed as they tried to conserve their now-drained energy and empathy. Participants faced difficult choices between work and family. However, in reality, there was no contest. Work and their patients always seemed to come first. These GPs now “existed” to continuously work rather than “living” their previous, more balanced lives that at one time included enjoying being a doctor. Worryingly, participants were struggling, isolated, and vulnerable, yet unwilling to seek help.
We interpreted Continuously Working as resulting from the participants’ commitment to care for their patients and their efforts to address the overwhelming workload, which is a principal contributor to burnout in doctors (Bruun et al., 2024; General Medical Council [GMC], 2021). As part of a deteriorating situation, General Medical Council (2023c) research found that 70% of doctors worked beyond their rostered hours (59% in 2021), 68% had difficulty taking breaks (49% in 2021), and 42% felt unable to cope with their work demands (30% in 2021). It is also concerning that 97% of a UK doctor sample believed the National Health Service regarded “excessive stress and workload as the norm” (Dominic et al., 2021, p. 398).
We considered the conceptualisation of work being ‘Always’ particularly thought-provoking. The slightly curious use of a single word in a context where so much has been written about burnout seemed to invite questions surrounding its applicability, leading our GP researcher to reflect again on his previous over-commitment to work and burnout. We hope other doctors might respond similarly to examine whether ‘Always’ is relevant to their work patterns or burnout concerns.
Our interpretations extrapolated doctors continuing to work when work has become ‘Always.’ We concluded that ‘Always’ is likely unsustainable, with consequences including, as found in our research, declining effectiveness and efficiency (West et al., 2018), disengagement from work (Hodkinson et al., 2022), depression and suicidality (Ryan et al., 2023), and a desire to leave general practice (General Medical Council, 2023b). We also concluded that the doctors’ diminished engagement and effectiveness would inevitably impact patient care and the healthcare system (Hodkinson et al., 2022; Lancet, 2019).
Pei et al. (2020) described two definitions of presenteeism in doctors. As in the first, some participants had probably continued to work on occasions when not entirely well, including Gill who recently resumed antidepressants. The second definition of impaired work performance due to illness (Burton et al., 2004) applies to every participant. In addition, some experienced Hodkinson et al.’s (2022) “career disengagement” with productivity loss, job dissatisfaction, and career regret. We offer further disengagement understanding, where other participants were no longer using their listening abilities, clinical expertise, and decision-making skills for the benefit of the patients to the same extent they once did. Instead, they were going through the motions like automatons, operating with disinterest in each consultation’s repetitive production-line ‘sameness,’ whatever the patient’s complaint was. Previously engaged GPs were reduced to being a “cog in the machine” (Harsh et al., 2019).
Previous research has shown that doctors working long hours become drained of energy and empathy (Jain et al., 2021; Prentice et al., 2023; Rutherford & Oda, 2014), which our findings confirm. However, existing literature suggests that doctors with burnout can manage to maintain interpersonal care (Ožvačić Adžić et al., 2013; Willard-Grace et al., 2021) and care quality (Rabatin et al., 2016), although at significant cost to their own well-being (Rabatin et al., 2016; Wallace & Lemaire, 2009). In contrast, our participants were concerned that their capacity to care was failing. Furthermore, we suggested earlier that patients were at risk if, as from our findings, busy doctors did not have enough time to think or were spending less time during each consultation as part of their patient depersonalisation. Therefore, supported by West et al. (2018), Al-Ghunaim et al. (2022), and Hodkinson et al. (2022), we propose that mistakes, safety issues, and diminished care seem eventually inescapable when burnout persists or progresses. Building upon this prior evidence, our findings further highlight the need to protect patients by addressing burnout in doctors.
Participants attempted to protect themselves against further energy and empathy depletion, as can be understood from Hobfoll’s (1989) Conservation of Resources (COR) theory. According to COR theory, burnout may occur when a person’s valued personal resources, such as energy and empathy, become depleted. Therefore, those with burnout concerns seek to maintain these resources (Hobfoll & Freedy, 1993), which supports our explanation of participants depersonalising patients as a defence mechanism.
This research usefully adds to describing and understanding the effects of burnout on GPs’ personal lives and families, given that the related findings in the identified qualitative studies are limited. Our participants lost out on family life, friends, and leisure due to so much time spent working, which Rutherford and Oda (2014) identified as contributing to burnout. We also interpreted a different perspective where participants believed their prioritisation of work had caused harm to their families and themselves, including burnout. More positively, this interpretation offers a personal means to prevent or address these problems through better-considered prioritisation decisions.
Also new, our findings included participants describing their wives as annoyed and fed up with always having to take second place. We interpreted these wives as simultaneously victims and necessary enablers, however reluctantly, of our participants’ Continuously Working. The participants’ extreme work practices would have been impossible without their wives continuing as family and home guardians, who were perhaps also ‘Existing, Not Living.’ Probably unnoticed by them, they too had become cogs in the Continuously Working machine, with little choice but to fit in around the GPs’ work. We acknowledge that this evidence was not first-hand and related only to the wives of male GPs. Future qualitative exploration of the personal experiences of burnout-affected doctors’ spouses and life partners is warranted.
Continuously Working also affected the participants’ happiness and well-being, with most experiencing some degree of depression. Bianchi and Sowden (2022) argued that burnout offers nothing unique to constitute a separate construct and that it is simply work-related depression, which Koutsimani et al.’s (2019) meta-analysis contests. Our findings support an association between the two (Ahola et al., 2005), but contrary to Bianchi and Sowden (2022), our IPA-derived understanding of burnout goes beyond work-related depression alone.
Unrelated to depression, one participant provided a uniquely dark glimpse and perhaps sounded an alarm about just how despairing and desperate GPs with burnout can become. Mirroring the away-from-work aspect of our also stark Existing, Not Living theme, Odom et al. (2022) described family medicine residents missing out on life as it passed them by. However, our interpretation went further to where the participants were now also Existing, Not Living when working as GPs. Surprisingly, despite their burnout misery, vocation was still meaningful for nearly all. We concluded that being driven to attend to patients’ needs was likely related to this sense of vocation playing its part in the participants’ prioritisation of work and being a doctor. Supporting this suggestion, Rimmer (2017) reported Clare Gerada’s view, as medical director of the Practitioner Health Programme, that “the more the vocation, the greater the risk of burnout.”
As part of our Existing, Not Living theme, vulnerability has been proposed as both contributing to burnout (Murphy, 2005) and created by burnout (Al-Ghunaim et al., 2022). We interpreted vulnerability as resulting from feeling attacked and not supported. This combination has implications for both worsening and responding to the current GP recruitment and retention crises (Jefferson & Holmes, 2022), for which Barnett and Holmes (2022) suggested that addressing burnout was part of the solution. Unfortunately, doctors who are vulnerable and most in need of mental health support can tend not to share their concerns (Zaman et al., 2022).
Also part of Existing, Not Living was social isolation (Odom et al., 2022) and our additional ‘self-isolation’ perspective, when participants with burnout were reluctant to seek the support they could have needed. Reported reasons for this reluctance relating to vulnerability include perceived stigma (Clough et al., 2018; Spiers et al., 2017), doctors framing mental illness as a personal failure (Spiers et al., 2017), confidentiality worries (Spiers et al., 2017), and fears that fitness-to-practice concerns may be made known to their employers (Dyrbye et al., 2017), perhaps by a colleague or their own doctor. To counter these unhelpful barriers and encourage those who are struggling, Greenawald (2020) wrote that reaching out for burnout support and professional help “is not a sign of weakness, but rather an expression of wisdom” (p. 22).
Vulnerability issues might also explain our recruitment difficulties, given our explicitly declared inability to guarantee anonymity and confidentiality in all circumstances. As we move to discuss the study’s other limitations, we acknowledge that the most vulnerable GPs may not have participated in our research.
Limitations and Strengths
To the best of our knowledge, our study is the first to qualitatively explore the personal experience of burnout in general practitioner partners.
This research is set apart from the five previous qualitative doctor studies because our interviewee selection required a self-reported experience of burnout and the combined High EE and High DP and Low PA scores on MBI screening. Significantly, in the absence of an evidenced means to diagnose burnout, MBI co-author M. P. Leiter (personal communication, May 5, 2022) supported using this HHL:MBI criterion to best represent burnout as engagement’s furthermost antipode in the engagement–burnout continuum. Consequently, our qualitative findings are the first to relate to this supported MBI specification of burnout in any medical speciality, including GPs. In addition, this research pursued IPA’s idiographic capture of detail and the ‘particularness’ of burnout. While being careful not to claim Husserl’s eidetic “essence” (Smith et al., 2009), we believe that our study is important because we have gone further than previous research towards shedding light on the particularness of what makes GP burnout what it is.
As for limitations, our participants were confined to Northern Ireland and only two were females, although they are now the majority of UK GPs (General Medical Council, 2023a). Also, we did not explore the role of gender or career stage. Data collected from 2014 to 2015 might be considered a limitation, but our original GP advisors concluded that our findings and narrative resonated with current general practice. However, readers will make their own evaluations that will additionally include usefulness and transferability. Transferability to other GPs and doctors could be particularly valuable because there is minimal similar research involving any medical speciality (see Table 1).
As a strength, our findings incorporate and exceed the components of the MBI (Maslach et al., 1996), Oldenburg Burnout Inventory (Demerouti et al., 2003), and Copenhagen Burnout Inventory (Kristensen et al., 2005), the most common burnout conceptualisations measured in quantitative GP research (McCammon et al., 2023). Our evidence includes the impacts on family and wider life that the MBI does not measure (Eckleberry-Hunt et al., 2018), something the other two instruments address only to a limited extent. These holistic findings could assist in developing a more comprehensive and doctor-specific burnout measurement instrument, as called for by Eckleberry-Hunt et al. (2018).
Another strength is that our findings offer meaning to other HHL:MBI-derived prevalence figures for GPs and other doctors, which is currently lacking (McCammon et al., 2023; Rotenstein et al., 2018). Meaningful statistics are essential to debating burnout as a significant problem requiring further resources (McCammon et al., 2023) and when developing improved prevention policies and interventions (Karuna et al., 2022; Rotenstein et al., 2018). Also, Eckleberry-Hunt et al. (2018) explained that the nuances only qualitative research can provide could assist in tailoring those improvements.
Recommendations for Research
Further qualitative research is needed to confirm and add to our GP-burnout findings. Future exploration should include gender, career stage, and burnout in non-partner sessional GPs, trainees, and other medical specialities beyond Northern Ireland. Adding to the body of IPA research may lead researchers closer to GP burnout’s more general but particular features (Smith et al., 2022).
Recommendations for Policy
Government and healthcare organisations must address the workload burden to prevent other GPs from being driven to Continuously Working. Overworked doctors require support rather than feeling unfairly criticised by the public, media, employers, and politicians, with implications for recruitment and retention. Greater system-wide effort is needed to encourage struggling clinicians to seek help, and doing so must become less daunting. Rather than being seen primarily as punitive, it should be clearer that the roles of their employers and the GMC include supporting doctors in keeping themselves well and continuing to care safely for their patients.
Recommendations for Practice
Doctors need to understand the risks associated with Continuously Working and prioritising work and vocation ahead of their families and themselves. Government and healthcare-organisation initiatives to address burnout are welcomed, but they take time to achieve results (Everington & Roland, 2016). This makes it all the more important for doctors to prevent or improve their burnout situations by acting now on whatever is within their own influence, such as re-evaluating their priorities and nurturing a sustainable and happy work–family–life balance.
Conclusion
We aimed to provide a description and understanding of burnout to which other GPs can relate. With this, we hope to encourage discussion between medical colleagues as perhaps their first step towards seeking support and possible burnout recognition. Although much more research is needed, our interviewee selection and IPA’s pursuit of ‘the particular’ has gone further than before towards understanding what makes GP burnout what it is, including the dangers surrounding Continuously Working. We urge readers to reflect on their work behaviour and ensure that work does not become or remain ‘Always,’ a suggestion relevant to both burnout prevention and management. Any acceptance of excessive workloads as “the norm” is a concern. Instead, the government, health service, and doctors must regard the current workload and associated risks to dedicated medical staff as an overwhelming problem requiring urgent corrective action.
Footnotes
Acknowledgments
We are indebted to Professor Marlene Sinclair for her always helpful, critical review of our work and subsequent advice and encouragement. Also, we are grateful for the expertise and patience of the Ulster University library staff and subject librarians Mary Rose Holman and Kelly Coogan. As our Dublin-based IPA consultant, Dr Martina Carrol provided expert guidance and appraisal of our analyses. Most important are the interviewees who shared their burnout experiences. While thankfully there were no problems, major fitness-to-practice concerns could have arisen and created severe difficulties for the already pressured general practitioners. These busy doctors courageously came forward to help their colleagues without seeking anything in return. The profession and individual doctors worldwide owe them their deep gratitude, much more than even we do for the trust they placed in us.
Author Contributions
L.McC.: conceptualisation, research approach, method, data collection, analysis and theme development, writing – original draft preparation, and resources. P.G., D.McL., and W.G.K.: conceptualisation, research approach, method, validation, interpretations and theme development, and writing – reviewing and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.