
Abstract
Mobile health (mHealth) interventions are increasingly used to address the challenges of living with HIV and engaging with antiretroviral therapy. A wealth of evidence supports the efficacy of mHealth in supporting living with HIV. Yet, there is a dearth of evidence on how mHealth improves outcomes, which features are effective, and why these work in a particular setting. This study uses stakeholder views, including patients, providers, peer supporters, counsellors, and program directors, to conceptualize how specific mHealth features could interact with contexts of living with HIV and mechanisms that shape engagement with treatment. The study is part of an ongoing research project on engagement with HIV care in Iran. We draw on the perspectives of recently diagnosed and more treatment-experienced patients and their providers, using purposive sampling, conducting 9 focus group discussions with a total of 66 participants, in addition to 17 interviews. Our findings suggest that mHealth designs that feature provider connection, proactive care, and privacy and personalization are expected to dilute the harsh contexts of living with HIV. We build on previously identified socioecological pathways that disrupt antiretroviral therapy in Iran and find that mHealth can enhance the relation between the health system and patients. Our findings suggest that personalized mHealth features and provisions can partially mitigate the compounded impacts of harsh socioecological pathways that impede treatment success in Iran. Our social constructivist study was augmented with realist-informed analysis and could have transferability to similar contexts that trigger similar mechanisms of treatment disruption.
Introduction
Consistent engagement with antiretroviral therapy is crucial for ending AIDS (UNAIDS, 2022). Despite having a national policy of universal antiretroviral therapy, only 67% of Iranians who are aware of their HIV status are consistently retained on treatment (UNAIDS, 2021), suggesting that for the estimated 45 thousand Iranians living with HIV, engagement with treatment is beset by structural and psychosocial challenges (Ameli, Taj, et al., 2021; Ameli, Haberer, et al., 2021). For example, internalized stigma, which is a key predictor of treatment disengagement, is reported by 96.9% of Iranians living with HIV, a proportion that is substantially higher than any country in the world (UNAIDS, 2022).
Globally, HIV stigmatization can negatively impact mental well-being and motivation for treatment (Earnshaw et al., 2013; Lee et al., 2002), thereby jeopardizing the course of treatment initiation and retention (Kalichman et al., 2019; Katz et al., 2013). People living with HIV experience a disproportionate burden of mental ill health, such as depression and anxiety that can interfere with consistent engagement with HIV care (Gonzalez et al., 2011; Uthman et al., 2014). Even at sub-clinical levels, depression has been shown to trigger disengagement from care and disruption of treatment, while cumulative clinical depression has been shown to accelerate disease progression and elevate the risk of mortality (Gonzalez et al., 2011; Mills et al., 2019). Internalizing beliefs about oneself such as internalizing stigma and shame are the key contributing factors to mental ill health among people living with HIV, jeopardizing health-seeking behaviors and self-care (Brown et al., 2010; Onono et al., 2020), and in some cases increasing the risk of suicide following diagnosis (Ferlatte et al., 2017; Tsai et al., 2023). More generally, illness-related self-discrepancy occurs when the currently ill “actual” self is perceived to be inconsistent with the conceptualized “ideal” self (Higgins, 1987), increasing the likelihood of experiencing mental ill health, such as anxiety and depression (Higgins, 1989). While the discrepancy between the “actual” and “ideal” self appears to be an intra-personal belief, emanating from inside one’s mind, recent research shows that internalization of stigma and self-limiting beliefs have interpersonal and socio-structural roots and must be tackled at the social and structural levels (Pantelic et al., 2017, 2019). In other words, the internalization of stigma is triggered by external socioecological factors that shape living with HIV (Pantelic et al., 2017; Rich et al., 2022).
HIV Stigmatization in Iran
At the outset of the HIV epidemic in Iran, a series of reports indicated that the majority of people living with HIV were committing suicide (Behrouzan, 2010). These reports suggested that suicide, rather than AIDS-related causes, appeared to have become the primary cause of death among Iranians diagnosed with HIV in the 1990s. The heavy burden of stigma, especially in border cities and among the more conservative ethnic minorities, contributed to family disownment, severe isolation, internalized shame, and ultimately suicide (Karamouzian et al., 2014). In response, there was a need for programs that could mitigate the consequences of HIV stigma through intervening at the family and community levels, by providing education and counselling (Rosenberg, 2010a, 2010b). Iran’s health system had a history of community-delivered healthcare, thereby the medical community mobilized community resources to provide culturally sensitive support and counselling to HIV-affected families (Rosenberg et al., 2011). This work was followed by the development of triangular clinics, which provided treatment for drug use, HIV, and other sexually transmitted diseases; a model that diffused stigma by avoiding direct reference to HIV/AIDS, resulting in a higher acceptance of HIV services and uptake of treatment (Mokri & Schottenfeld, 2008). This model, which received a best practice achievement award by the World Health Organization (WHO) in 2004, facilitated delivery of HIV care by intervening at the community and family levels and by targeting the microsystem through a medicalized approach (Rahnama et al., 2014). Evidently the high rates of suicide were reduced as engagement with treatment and support increased, but this medicalized approach simultaneously side-lined efforts that could raise public awareness of HIV and tackle stigma at the macroscale (Behrouzan, 2010).
As a consequence of limited public debates regarding HIV, enacted and internalized stigma associated with HIV in Iran remains high (Rasoolinajad et al., 2018). Iranian society has a collectivist culture, resulting in the experience of collective shame and concerns about family honor. Simultaneously, modern Iranian society has rapidly transitioned toward more individualistic value systems and lifestyles, as a result of increasing access to education, modernization of the workforce, and an expanding middle class (before the past decade of sanctions and chronic inflation pushing people into poverty) (Harris, 2017; Salehi-Isfahani, 2020). For instance, women make up more than 50% of university students; the percentage is even higher for female students in science and technology degrees, which is significant given that Iran is one of the countries with the highest per capita number of engineering graduates (Dobbs et al., 2016). Yet, these statistics are occurring in parallel to emerging and evolving modern transitions that remain embedded within a traditional value system and conservative social norms regarding gender, sexuality, drug use, and consequently HIV (Ferdows, 1983; Mir-Hosseini, 1999; Shahrokni, 2020).
According to the stigma index surveys (2018–2021), the highest percentage of reports on the experience of enacted stigma and discrimination in community and healthcare settings was from Iran, which is the underlying trigger for the 96.9% of Iranians living with HIV who have internalized HIV-related shame (UNAIDS, 2022). Our previous research corroborated these quantitative findings by advancing a more nuanced understanding (see Figure 1). Our findings show that HIV-related stigma, discrimination, lack of societal awareness, and sociocultural factors introduce multiple layers of complexity into the contexts of lifelong engagement with treatment and lead to individual level reasonings and (re)actions of denial, fear, and despair that result in disruptions of daily treatment and disengagement from HIV care pathways (Ameli, Taj, et al., 2021). Recognizing the need to raise public awareness, Iran has now joined a global partnership to escalate efforts that can address stigma and discrimination by establishing formal processes to seek redress and via providing legal assistance to key populations affected by HIV and victims of discrimination (UNAIDS, 2022). Building on such necessities and potentials, this paper aims to conceptualize an intervention to counter the socioecological pathways that lead to treatment disruption among Iranians living with HIV (as displayed in Figure 1). Pathways from social and ecological contexts to individual reactions and reasonings that disrupt antiretroviral therapy in Iran, based on findings from a previously published study (Ameli, Taj, et al., 2021).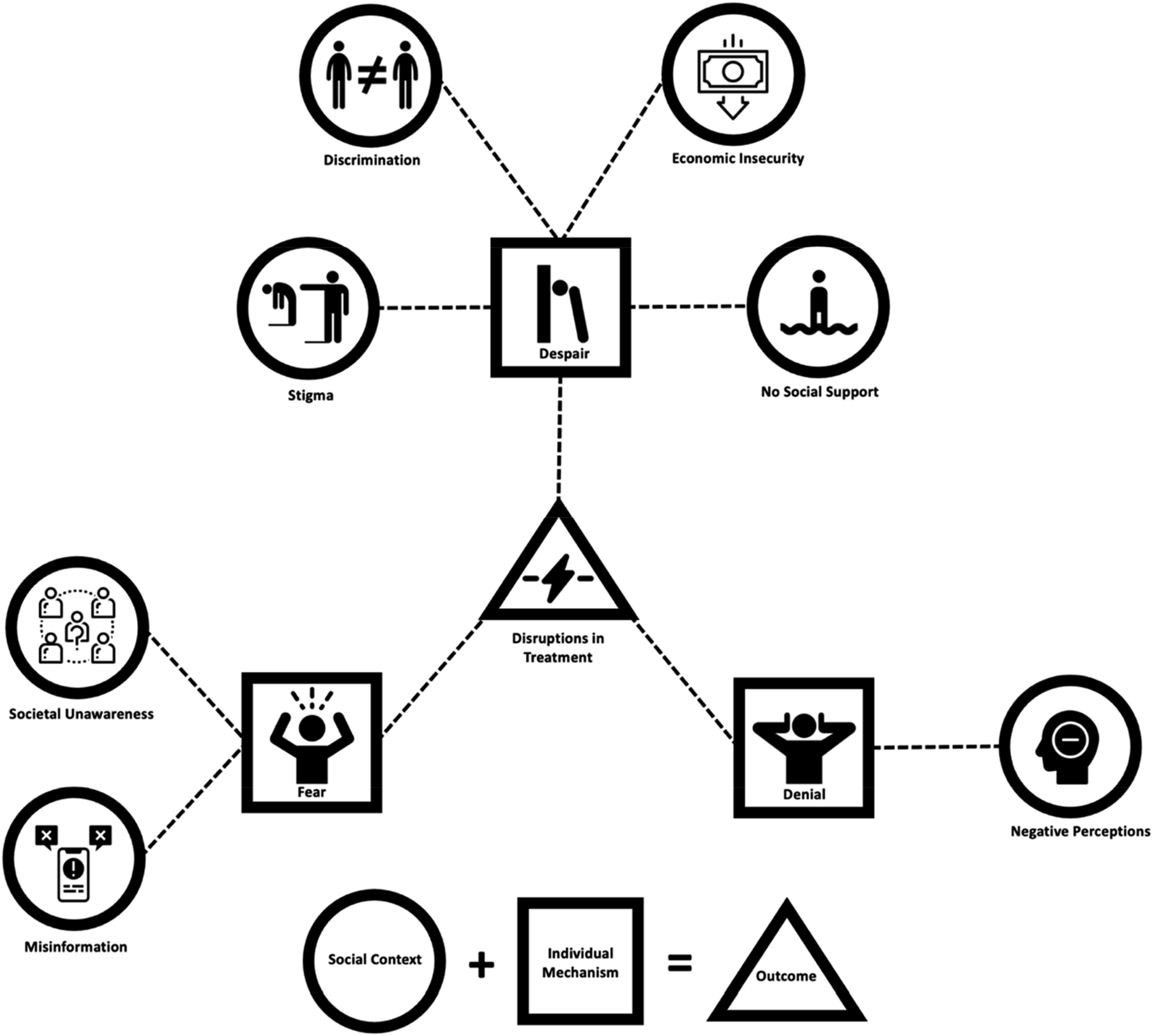
Mobile Health for HIV Care
The WHO has endorsed the use of mobile phones for supporting people living with HIV through tailored and differentiated models of care delivery (World Health Organization, 2016), highlighting the potential of mobile health (mHealth) for health system strengthening (World Health Organization, 2019). In recent years, mobile messaging has been the key mHealth feature used in interventions to deliver a combination of reminders, support, and information to improve treatment linkage, retention, and adherence (Haberer, Sabin, et al., 2017; Sabin et al., 2018; Ware et al., 2016). Across mobile messaging intervention designs, patients can be either passive recipients or active partakers depending on the use of one- or two-way messaging, respectively. The appeal of mobile messaging programs is that they are easy to use, are affordable, are offered through a variety of platforms (such as basic SMS, WhatsApp, iMessage, and other applications), and can offer a personalized array of support components (Campbell & Haberer, 2015; Finitsis et al., 2014; Haberer et al., 2016; Haberer, Sabin, et al., 2017). Importantly, any combination of components must be carefully chosen to match the context into which an intervention is being implemented.
The simplicity, flexibility, and adaptability of mobile messaging provide a powerfully dynamic programmatic tool that can address multiple barriers to treatment; however, this flexibility adds a layer of complexity to the standardization of mobile messaging intervention designs. Moreover, just as with most technological interventions, mobile messaging programs can recursively change (and be changed by) the very social setting and relations into which they are introduced (Abimbola et al., 2019; Greenhalgh et al., 2021; Pawson et al., 2005). Dynamic interactions, material exchanges, and nascent connections enabled by mobile messaging between patients and providers can change the relational contexts in which people living with HIV engage with treatment. Nevertheless, these changes remain understudied within the larger body of experimental mHealth research that are predominantly underpinned by technological determinism, which assumes technology X will have impact Y that is measurable (Greenhalgh & Swinglehurst, 2011; Greenhalgh et al., 2011). This research orientation and its deterministic suppositions largely produce studies that evaluate the impact of mobile messaging on a set of pre-defined outcomes. As a result, a wealth of evidence supports the efficacy of mobile messaging in improving adherence to antiretroviral therapy (Finitsis et al., 2014; Haberer, Musinguzi, et al., 2017; King et al., 2017; Lester et al., 2010; Purnomo et al., 2018; Rotheram et al., 2019; Sabin et al., 2015; Westergaard et al., 2017), but a dearth of evidence can demonstrate how mobile messaging changes the contexts of treatment delivery and why it is suited to a particular context of living with HIV. Randomized controlled trials can evaluate the efficacy of programs, but real-world effectiveness of complex interventions needs to also consider the interactive contextual effects. For example, research is needed to investigate how the local perceptions and actions of Iranians living with HIV, as well as the selected features and designs of an mHealth program, are shaped and constrained by wider socioecological influences and how, in turn, such perceptions, actions, and design features can feed back into and change the wider socioecological settings (Greenhalgh & Abimbola, 2019; Greenhalgh & Swinglehurst, 2011; Greenhalgh et al., 2017).
To evaluate complex interventions, Pawson and Tilley 1997 proposed the scientific realist method, arguing that researchers must look for social mechanisms at the level of human reasonings and reactions, building on the key concept of generative mechanisms expounded by Bhaskar (1978) in A Realist Theory of Science. In realist research and evaluation, interventions are not conceptualized as causing outcomes themselves; rather, people’s reactions to what interventions offer can cause outcomes. For instance, an mHealth program may provide useful information and a new connection that makes people feel cared for, so that they better engage with their treatment and care. Their subjective reasoning, followed by a decision to act or not, will depend on the context. As such, an mHealth program is designed to change the context in such a way to induce the desired mechanism(s) and in turn generate the intended outcome(s). Such data is best collected qualitatively to enable researchers to engage with the reasoning of participants (which is interpretive and socially constructed). This approach helps to view mHealth as a complex intervention that has a recursive relationship with its socially constructed contexts (Greenhalgh et al., 2017; Pawson, 2013).
As a country that has a policy of universal antiretroviral therapy for HIV, Iran constitutes a useful case study for investigating how mHealth could address the socioecological, relational, and programmatic perils that undermine the promises of universal access to treatment. This study is part of a larger research project that is the first to investigate the psychosocial challenges that undermine engagement with and adherence to antiretroviral therapy in Iran. Here, we conceptualize how an mHealth program can change the contexts of living with HIV in Iran. Despite being specific to the Iranian setting, the findings may produce lessons that are transferrable to other contexts that share similar characteristics (e.g., majority Muslim countries in the Middle East and North Africa region or the Asia and Pacific region). This qualitative study, involving stakeholder views, uses a social constructivist approach and thematic analysis, augmented with further realist-informed analysis, to investigate the effect of adding an mHealth program to the contexts of living with HIV and engaging with antiretroviral therapy in Iran.
Methods
Design and Setting
The study is part of a three-staged, ongoing research project to understand and improve use of antiretroviral therapy by Iranians living with HIV. In the first stage, we have investigated the socioecological contexts of living with HIV in Iran and the mechanisms that disrupt engagement with treatment (Ameli, Taj, et al., 2021). The current study comprises the second stage of the larger project and aims to conceptualize how mHealth may be used to change the contexts of engagement with antiretroviral therapy in Iran and to optimize an mHealth design that suits these contexts, based on stakeholder views. In the final stage of the larger research project, we hope to evaluate the effectiveness of the mHealth intervention that is conceptualized here in terms of reducing disruptions to treatment as part of a randomized controlled pilot and a nested realist evaluation (Ameli, Haberer, et al., 2021).
This current study builds on earlier findings from the first stage of the ongoing project (depicted in Figure 1), showing that the cognitive and affective mechanisms of fear, denial, and despair are triggered in response to a societal lack of awareness, misinformation, and negative perceptions regarding HIV, profound levels of stigma and discrimination against HIV, a lack of social support, and economic insecurity fuelled by inflation and sanctions. The research questions for the current study were as follows: (i) What are user preferences with regard to features of an mHealth intervention that uses mobile messaging? (ii) How might these features of an mHealth intervention impact antiretroviral use within the contexts of living with HIV in Iran? We draw on the perspectives of both recently diagnosed and more experienced antiretroviral users, their care providers, counsellors, peer supporters, and program directors to explore their preferences and views regarding how a mobile connection can address some of the psychosocial and ecological factors (such as those depicted in Figure 1) that disrupt antiretroviral use in Iran.
A social constructivist approach was used to explore subjective participant reasonings and inform the design of an evidence-based mHealth intervention for the contexts of living with HIV in Iran. Rather than seeking to generate characterizations of a statistically representative sample, the social constructivist approach aimed to answer the research question through an in-depth exploration of the subjective ways stakeholders in this setting interpreted the role of a mobile connection in changing the contexts of HIV treatment and relational aspects to care. A realist-informed analytical framework was then used to help hypothesize how the intervention design might change the contexts of HIV care and treatment in Iran (that were previously developed and presented here in Figure 1). Within the realist research paradigm, mechanisms and contexts interact to produce outcomes, and the relationship is expressed as Context + Mechanism → Outcome (Pawson, 2013; Pawson & Tilley, 1997). Thus, when introducing interventions, it is important to recognize which aspects of a context are changed by the intervention and how that change, in turn, alters mechanisms and resulting outcomes. By combining a social constructivist data collection phase with a realist-informed data analysis phase, the findings on the shared realities produced here are accessed via the socially constructed understandings and interpretations of interviewed stakeholders, while the realist-informed lens provided us with additional concepts (i.e., context and mechanisms) to further unpack the empirical data we collected to produce an understanding of when and how possible mHealth design features may be useful.
Sampling and Data Collection
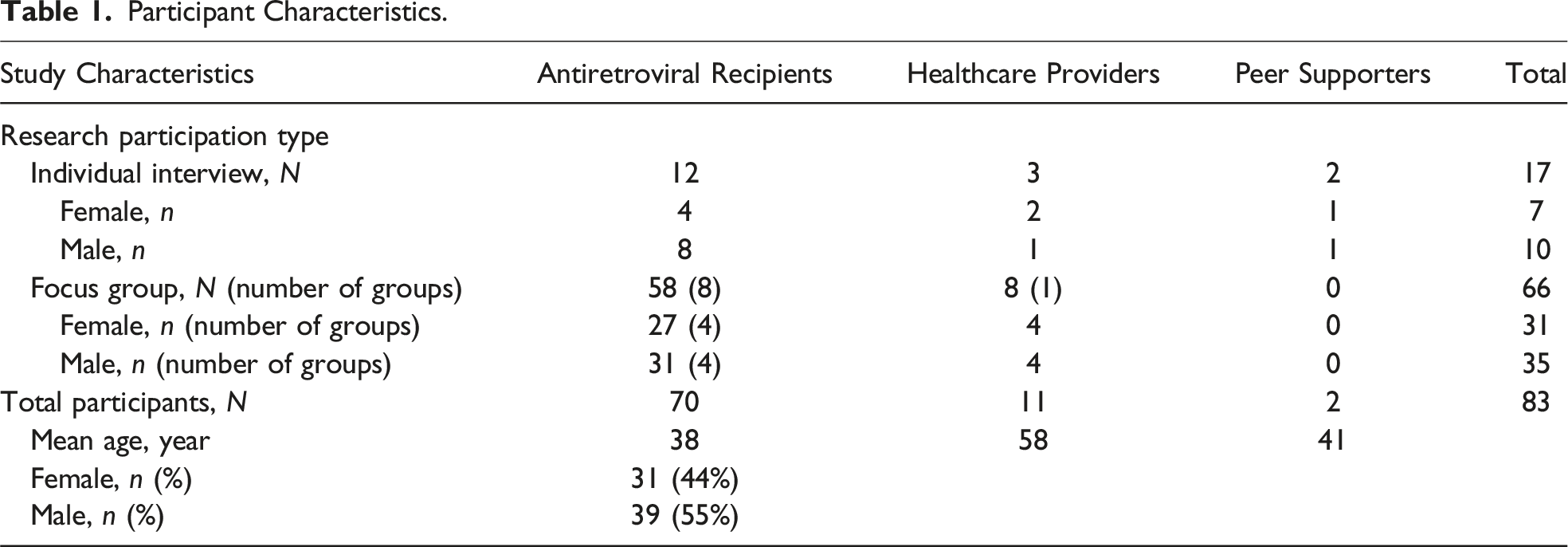
Purposive sampling was used to recruit participants with a range of experience in terms of adherence to antiretroviral therapy, based on information in clinic records of people living with HIV receiving antiretroviral therapy (Palinkas et al., 2015), using the following criteria: (1) antiretroviral recipients diagnosed within the past year, (2) antiretroviral recipients diagnosed more than 1 year ago, (3) antiretroviral recipients who experienced disruptions in care and adherence, and (4) antiretroviral recipients who had to change more than one treatment regimen due to drug resistance. All participants were currently engaged in care. For each of the selection criteria, men and women were sampled separately based on data from clinical records. Further, peer supporters and healthcare workers were invited from the central hospital complex, a central medical university, and a central peer support positive club.
The data collection for this study was conducted from August 2018 to January 2019 at one of the peer support positive clubs for people living with HIV in Tehran, Iran. The research method involved interviews and focus group discussions (FGDs). Considering the social constructivist approach, the former only involved the interactions and conversations of the interviewer and interviewee, while the latter included more in-depth discussions and group interactions. Participants were invited to choose the most comfortable interview or FGD slot, both in terms of time availability and confidentiality concerns. Given that the Positive Club was perceived as a safe and empowering space, run by peers who were living with HIV, and that this unit was located at the site where antiretroviral therapy was received and delivered, confidentiality concerns were minimal. The FGDs were conducted separately for men and women to explore any differences between genders in terms of the reactions and views of participants about adding mobile messaging communication regarding HIV to their lives. Semi-structured topic guides (see Appendix) focused on which mHealth features were perceived by participants to act as facilitators of engagement with antiretroviral therapy. More specifically, the focus was on how and why mHealth features could impact daily adherence in the contexts of living with HIV in Iran (topic guides also focused on what the socioecological barriers and facilitators to antiretroviral therapy adherence were; however, the responses to these are published elsewhere). Ethical issues related to the use of mobile messaging communication with individuals who may be living with an undisclosed condition were also discussed. These discussions were not limited to considering unintended disclosure but also focused on understanding how potential feelings of surveillance and “being watched” could be avoided and how the intervention could be a useful rather than a cumbersome addition to patient lives. Interviews were conducted by the lead researcher, a native Persian speaker, and audio-recorded with permission from the participants.
Ethical Considerations
Participants were contacted by telephone by research staff, who were trained in informed consent processes and introduced to the research project. An overview of information included in the consent forms was provided in terms of the study purpose and design, in addition to details regarding the length and location for the qualitative interviews and topics for discussion. Participants who expressed an interest were offered possible dates for participation. A reminder phone call was made one day prior to the scheduled date. On the day of the interview, participants were given information sheets to read carefully before signing the consent form.
FGDs and interviews were recorded with the consent of participants, who chose their own nicknames to be used during the recording. Following transcription, the audio-recorded files of participants’ voices were deleted, and no information with personal identifiers was stored or accessible. Ethical approval was granted by the local ethics committee, authors’ university ethics committees, and institutional review boards (names not provided to retain anonymity). Written and informed consent was obtained from all research participants with the agreement that their identities would not be revealed.
Data Analysis
These recordings were subsequently transcribed in Persian and imported into MAXQDA, a qualitative analysis software package, for organizing and coding the text segments with descriptive headings. A codebook was developed and organized around the research aims and questions of the ongoing project. Two researchers coded the data independently in Persian and reviewed the codes at two intervals, after coding 20 and 80% of the transcripts, by discussing differences in coding to reach an agreement on the assigned meanings to each code. The developed themes on key mHealth features, to be used in the delivered intervention, were discussed between the local research directors, a research assistant, a peer supporter, a person living with HIV, and a psychosocial support provider. These themes were translated into English and informed the mHealth intervention that was developed for the context of Iran, named HamRaah (in Persian meaning together-in-path), the pilot trial, and the nested realist intervention, which were conducted in collaboration with international research directors. The protocol for this trial and intervention is published elsewhere (Ameli, Haberer, et al., 2021).
Thematic network analysis was used to summarize the main themes that were developed from user preferences on mHealth design features and their views on how these features could have an effect in the contexts of engagement with antiretroviral therapy in Iran. Following the prescribed steps for thematic network analysis (Attride-Stirling, 2001), the transcribed texts were first coded with a basic code and then clustered into higher order themes. Useful mHealth provisions and relational changes to care (such as information, support, motivation, patient initiative, and agency) were identified as basic themes. The basic themes were then grouped into organizing themes by the identified design features (provider connection, proactive care, and privacy and personalization) that comprise the sub-sections of the Results section. Once the thematic analysis was completed, a realist-informed analysis of the themes was conducted. The purpose of the additional analysis was to explore whether using the realist concept of context–mechanism–outcome configurations might help us conceptualize how the mHealth intervention features might contribute to the contexts of living with HIV in Iran (as depicted in Figure 2). These results were used to inform a mobile messaging intervention (HamRaah) that is suited for the Iranian context and the protocol for which is reported elsewhere (Ameli, Haberer, et al., 2021). Two-way mHealth features (blue), introduced into the contexts of living with HIV in Iran.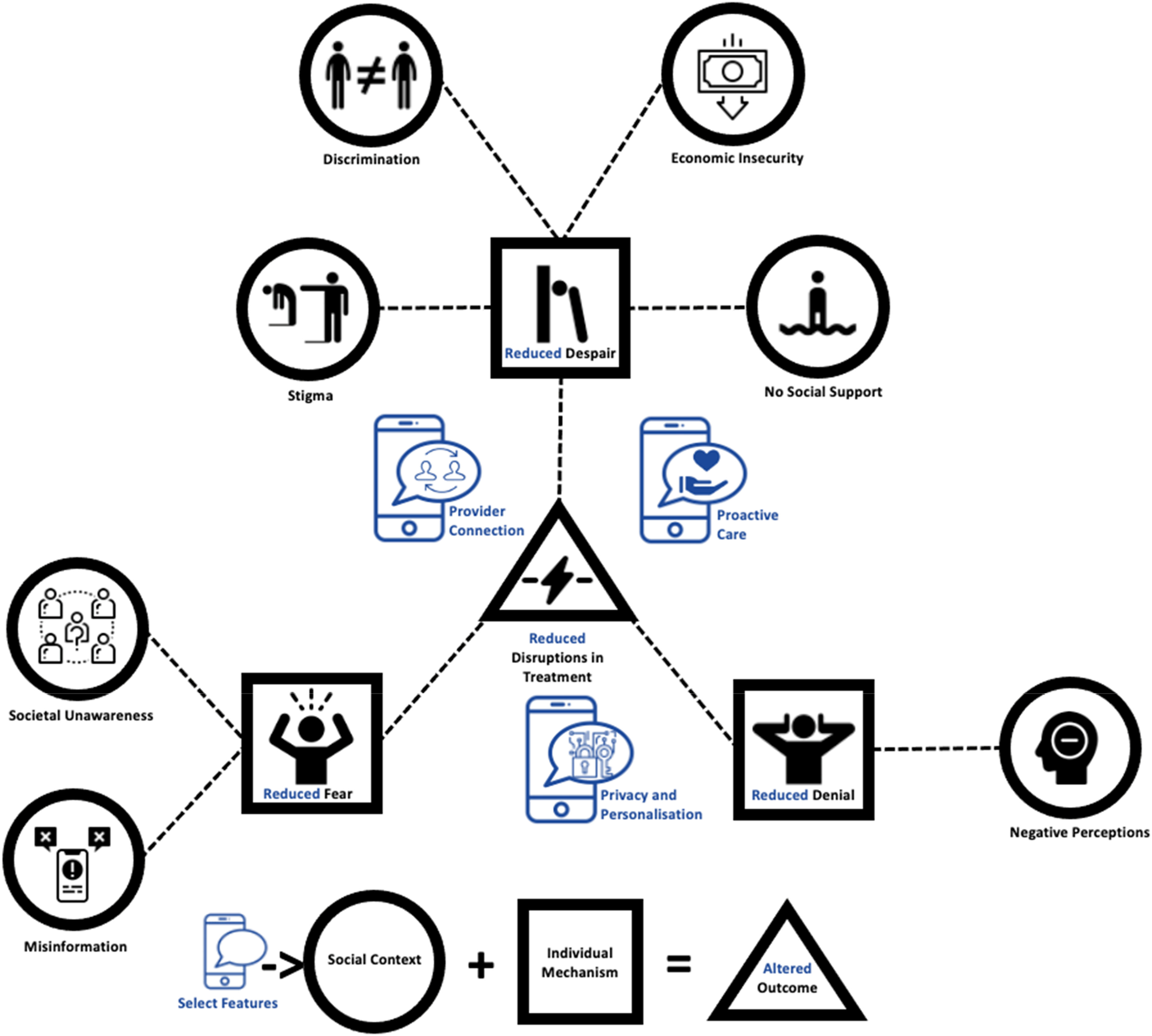
Results
Participant Characteristics.
The findings of our study suggest that mHealth interventions can change the relationship of people living with HIV with the health system in terms of information, support, motivation, initiative, and agency to engage with treatment (basic themes) via three overarching design features (organizing themes): (i) provider connection, (ii) proactive care, and (iii) privacy and personalization. This section presents the three proposed mHealth design features and how these produce their effects. A modified conceptual pathway is then presented in the final section, and depicted graphically in Figure 2, conceptualizing how these design features of the intervention can influence the previously identified socioecological contexts of living with HIV in Iran.
Provider Connection
The ability to communicate with providers more readily through mobile messaging was identified by participants as an essential design element of mHealth that was perceived to be useful, rather than cumbersome, in the contexts of living with HIV in Iran. Emphasis was placed on the ability to directly message a provider who can offer reliable information and support. Some participants suggested that such support can counteract feelings of despair and dilute the harsh realities of living with HIV in Iran: The benefit of texting with a provider is that you can be connected to someone who can give you useful support and maybe a backing when you are faced with the harshness coming from society and the difficulties of everyday life with HIV. The utility of mobile messaging can be a connection to support that can dilute the harshness of life. (Male patient, focus group 7)
When given the choice between receiving one- or two-way messages, participants chose the latter because it provided them with the option of communicating with someone. They highlighted the value of a personalized approach that is open-ended and can accommodate unique patient needs. One physician described how having healthcare staff help patients with their unique needs had been useful in her private clinic. Our patients could really benefit from a personalized approach, because each of them have unique needs and so they would need unique support. But we provide this kind of support to my patients in the private clinic, and we see that each person’s needs are completely different, and that having one person who helps them through this process makes a big difference. (Doctor, focus group healthcare providers)
Another patient explained, “One-way text-messages without the option to respond feels very mechanized and without having the chance for an open conversation these messages will become monotonous and lose their effect” (male patient, focus group 5).
One of the elements emphasized regarding the value of the mobile messaging was its role in providing patients with a reminder about the support available, more than a specific reminder about taking their medication: “Reminders for taking pills are good, but I guess they depend on the person. For me, I prefer to get more support” (female patient, focus group 4). This helps because we will know that there is some support on the other line that comes to you every week. It can make a world of difference and really gives hope. Reminders [to take medicine] will act just like an alarm. If you are in a hopeless place no alarm can help you. (Male patient, focus group 3)
Some participants referred to the importance of having access to a person providing trust-worthy information, especially when there is significant misinformation: “Although we can ask things on the internet or telegram, this way [direct mobile messaging with the provider] we know who is responding. This is a good way to get information that we can trust” (male patient, interview 9). Sometimes you really need to ask a question, especially in the beginning when there is so much confusion and contradictory information. We have the hotline but having one person who you know will answer your questions every week is very useful. (Female patient, focus group 4)
Overall, participants appeared to value having a two-way connection to providers for the possibility of receiving material support and needed information. As opposed to receiving one-way information or reminders, they prioritized having the option to ask individual questions and seek support as they saw fit and as problems arose that impacted their ability to adhere to treatment.
Proactive Care
The interview data also suggests that participants would value the proactive demonstration of care (i.e., by checking up on them) on the part of the clinic. It was suggested that this would help them to feel cared for, reminded them to value themselves, and was a source of motivation in terms of staying on track with their treatment:
One participant described how the proactive check-up initiated by the clinic felt like a service that was delivered to their home: “This is great because it is like having a home-clinic once a week. Instead of you having to go all the way there they come to you and take the initiative to make sure you are doing okay” (male patient, focus group 5).
Another patient described how the proactive messaging could help him feel uplifted: For me I go through these waves of time that I hate myself. I isolate myself in a corner and lose motivation for continuing life tasks. At that moment I can feel uplifted if I get a message. It could give me motivation to keep going and continue my treatment too. (Male patient, focus group 7)
Another interviewee stressed that the caring that is demonstrated by the weekly texting motivates them to value themselves: As patients we become very depressed and isolated sometimes. We retreat within ourselves sometimes. But someone reaching out to us can give happiness. It’s like someone is looking after us even though we are not caring for ourselves. It makes you think that if someone else values you this much, why are you not valuing yourself, why are you neglecting your treatment. (Female patient, interview 2)
On the other hand, patients and peer supporters living with HIV described how a mobile messaging connection can provide patients with a pathway for taking the initiative, thus having more agency, to ask questions when they need help: “Having someone to text your problems to encourages you to think about your problems and take the initiative of contacting the clinic as it’s much easier through texting” (female patient, focus group 4). A peer supporter commented: “I think regular mobile messaging by itself can make patients better at acting and taking initiative for getting the medication and staying on track” (peer supporter).
Overall, the participants appeared to value receiving messages from the clinic, in addition to being able to respond to the messages. Such follow-up demonstrated care and helped reinforce an internal sense of self-worth and self-care, which in turn enhanced motivation for treatment and care, and enhanced agency and initiative on the part of the patient.
Privacy and Personalization
We asked stakeholders about the features of the mobile messaging intervention that they found to be important in terms of its acceptability in their daily lives and the minimization of harms, such as unintended disclosure of HIV status. High levels of privacy, low frequency of text messages, and a personalized approach were emphasized by most stakeholders because such features were perceived to help patients to trust the communication channels, thereby encouraging them to take more initiatives in terms of seeking care and treatment. I would be interested in getting this kind of messaging support, but then again it is important to keep it confidential and not mention HIV, because for me other than my wife no one else in the family knows that I have HIV. (Male patient, focus group 7) As long as it is discrete, I do like to get the text-messages for support, but I prefer not getting direct references to HIV. I think receiving a check-up message once a week is sufficient to give help. (Female patient, focus group 4)
Healthcare providers emphasized the value of a program that would increase contact with patients who are not typically aware of the resources available within the healthcare setting and described the value of a tailored personalized approach over a uniform and unidirectional approach. For example, a counsellor mentioned, “Different patients have different needs and rather than deciding on patient’s behalf it would be more useful to let patients tell us their needs so we can guide and direct them accordingly” (counsellor, interview 1). An infectious diseases doctor suggested: In Iran we do have a lot of services available, by far more than other countries in our region we provide harm reduction, peer support, social support, and access to free counselling. The problem we have is that a lot of patients aren’t aware of these services. If you have a program that reaches patients who are not using the resources, especially in the first year of their diagnosis when they are not familiar with the system, that can change their treatment outlook completely. (Doctor, interview 2)
The overarching importance of maintaining patient privacy and keeping message contents discrete was evident through all discussions. Further, the significance of having personalized communication that addressed individual needs of patients appeared as a key opportunity for providing information and support to more patients, by enabling them to take advantage of the already-existing but under-utilized support services. Such a personalized approach was perceived to improve patient agency to take initiatives toward an improved treatment outlook and better trajectory of retention in care.
Conceptual Model
In this section, we apply the overarching themes that were presented above to conceptualize how the preferred mHealth features could reduce disruptions in treatment. We build on our previous findings (Ameli, Taj, et al., 2021) that demonstrated misinformation, societal unawareness, negative perceptions, lack of social support, economic insecurity, stigma, and discrimination, for individuals living with HIV in Iran appear to trigger despair, denial, and fear, which act as mechanisms that can disrupt treatment (Figure 1). The pathway in Figure 1 is used as a backdrop for the additional realist analysis that was done to hypothesize how the proposed mHealth design features will introduce relational changes within the contexts of living with HIV to reduce the negative outcomes and experiences. Details about where these potential relational changes in design features may have an impact are illustrated in blue within Figure 2. The findings presented in Figures 1 and 2 are based on the FGDs and interviews (guides provided in Appendix) that were conducted to, first, understand the context of engaging with and adhering to antiretroviral therapy and, second, how mHealth can be useful for these contexts. The findings of the former were presented in a separate paper (Ameli, Taj, et al., 2021). The findings of the latter, that include the realist-informed conceptualization of how mHealth suits the socioecological contexts of living with HIV and engaging with antiretroviral therapy in Iran, are presented here.
Participants viewed the most useful aspect of mHealth to be relational by connecting them to providers and improving access to support, especially within the contexts of feeling despair and lacking social support. Misinformation regarding HIV in Iran was shown to trigger fear, which acted as a mechanism driving patients away from treatment and the health system in general. Therefore, having access to information and support from trusted providers who offer proactive care, and the opportunity to ask questions through a private and personalized communication channel could counteract fear as a mechanism that disengages and drives patients away from treatment. Societal stigma against HIV in Iran appears to lead to internalized stigma and a self-defeating feeling of despair, which acts as a mechanism that reduces the motivation to continue treatment. Participants explained that when clinics demonstrate proactive care, the check-in messages acted as an “antidote” to internalized stigma, reinstating feelings of self-worth and motivation for engagement with treatment and adherence to daily medications. Denial in response to negative perception of HIV in Iran appears to act as a mechanism that keeps patients away from existing resources. By providing private and personalized communication links, patients can learn about and access health system resources more seamlessly, have more agency to seek support, and be more informed to take the initiatives needed to engage with treatment, overcoming the state of denial less challengingly.
Discussion
The findings of this study delineate the potentially useful features of mHealth that can change how people living with HIV relate to treatment and care in Iran—namely, by offering provider connection, proactive care, and privacy and personalization in communication. These mHealth features could support Iranians living with HIV to stay engaged with antiretroviral therapy, especially early on after diagnosis, addressing Iran’s significant gap in treatment retention. It is also possible that our realist-informed analysis has developed knowledge that may be of value in other similar settings, such as where HIV is highly stigmatized and affects marginalized populations, thus remaining hidden from public attention and absent in public debates. Iran sits at the border of two UNAIDS designated regions: the Middle East and North Africa, and Asia and the Pacific. The hidden HIV epidemic shares characteristics with countries in both regions, in which the prevalence of HIV is low, but new HIV infections and AIDS-related mortality are high because the enactment and internalization of stigma are high, undermining engagement with antiretroviral therapy, despite free and universal access (UNAIDS, 2022). Therefore, approaches specific to such settings are needed to address the gap between treatment supply and demand, by focusing on the barriers to treatment uptake and adherence through providing services that improve continuity of care, and promote mental and physical well-being of marginalized populations and people living with HIV (Byng et al., 2023; Hajebi et al., 2022; Rasoolinajad et al., 2018).
Being connected to a provider is hypothesized to be the most valued aspect of mHealth and expected to improve access to information and support. Proactive demonstration of care offered through regular text-message check-ins is expected to provide motivation for self-care and continuing treatment. Privacy and personalization in communication is expected to facilitate access to existing HIV care and support services. These findings resonate with previous evidence on mHealth interventions that use two-way messaging, showing that this approach can improve adherence to treatment, particularly for newly diagnosed patients (Gross et al., 2019; Lester et al., 2010). Importantly, here we conceptualize how these outcomes can be impacted through specific mHealth features, using stakeholder views in the seldom-studied setting of living with HIV in Iran. Previously, we reported that the socioecological contexts of living with HIV in Iran are characterized by stigma and discrimination, negative perceptions, misinformation, and low awareness regarding HIV, amidst economic insecurity that is fuelled by financial sanctions and economic inflation (Ameli, Taj, et al., 2021). Our findings here suggest that select mHealth features and personalized provisions can partially minimize the confluence of the detrimental socioecological impacts on treatment outcomes by enhancing information, support, motivation, and initiative for treatment.
Globally, WelTel Kenya was the first study to provide weekly text-message check-ins to people living with HIV who were initiating treatment (Lester et al., 2010). Other quantitative studies have shown that mobile messaging could be effective in promoting adherence, monitoring, and viral load suppression, the outcomes that have most frequently been examined using experimental methods (Badawy et al., 2017; Devi et al., 2015; Hall et al., 2015). Previous qualitative studies have shown that mobile messaging can reduce feelings of loneliness and isolation, while enhancing feelings of being supported by the health system (Sabin et al., 2018; Venables et al., 2019; Ware et al., 2016). We have also seen in other settings that mHealth designs, and mobile messaging interventions in particular, can increase support, not just by making people living with HIV feel cared for and supported but also by linking patients to under-utilized existing support services, including counselling and mental health support, and accessing harm reduction, medical support, or other existing resources when needed. However, few studies have provided detail with regard to the role of context in the potential causal pathways that may explain the impact of mobile messaging on adherence behavior (Glasziou et al., 2014; Nittas et al., 2020; Sutcliffe et al., 2015).
Methodologically, as the body of effectiveness studies on mHealth grows (Lee & Valerius, 2020; Marcolino et al., 2018), it is important to bear in mind that mHealth does not work in a uniform way for all participants and in all settings, thereby bearing means-based results potentially misleading. Mobile messaging is a simple yet flexible and dynamic communication tool, one that can change the social relations and the contexts into which it is introduced. Moreover, reception toward mobile messaging varies depending on the burden of use across countries. In Iran, SMS use is adopted for a wide variety of purposes, from public alerts to banking and advertisements, but stakeholders in this study indicated there is more trust in WhatsApp and Telegram messaging when it comes to private communication options. Thus, it is important to qualitatively investigate and understand what critical features of mHealth are needed for any given context, and how these features could change patient–provider relations and the contexts in which programs will be implemented. Such approaches can be conducted through frameworks that study the recursive relationship of technology interventions with contexts (Abimbola et al., 2019; Aranda-Jan et al., 2014; James et al., 2021). The realist-informed lens in this study provided us with additional concepts (i.e., context and mechanisms) to further unpack the empirical data we collected and produce transferable findings. Concretely, merging two research paradigms: social constructivism with realism, allowed conceptualizing intervention effects based on reasoning that may be socially constructed, but is rooted in a shared reality and an understanding of causation (i.e., through mechanism), which may produce transferable lessons for similar contexts (Bogna et al., 2020).
Stakeholders in this study described how a two-way private and personalized communication, proactive care, and provider connection could increase information, support, motivation, and patient initiative, that could ultimately contribute to improved engagement with care and treatment. These findings echo the constructs highlighted by the widely applied Information, Motivation, and Behavioral skills (IMB) model, which posits that HIV services are successful at the level of individuals when providing information regarding HIV, motivation to practice, and necessary behavioral skills (Fisher & Fisher, 2000). The IMB model is often used as a guide to identify the content of interventions, by specifying specific informational, motivational, and skills factors that are needed in each setting (Aliabadi et al., 2015). However, the model has often been viewed as simplistic for dynamic behavioral contexts, requiring attention to multiple aspects of context that influences individual decisions and behaviors (Rivet Amico, 2011). In line with these critical perspectives, our findings suggest that instead of identifying intervention content that can be delivered uniformly across a population or within a setting, selecting specific mHealth design features––that by their very nature are more personalized––can be more responsive to the informational, motivational, and behavioral exigencies across socioecological settings and structural systems. Future research is now needed to study the ways in which mobile phones can change the contexts of relating to treatment, care, and providers. Through a realist lens, the research focus on the efficacy of specific interventions can be expanded to answer more questions on when, how, and why mHealth with its various provisions can be incorporated in scale and sustained (Greenhalgh & Manzano, 2021). Investigating how certain mechanisms are triggered within specific contexts can unpack causal pathways and produce reusable concepts that can enhance the design and implementation of future interventions.
Policy and Programming Context in Iran
Programmatically, in addition to universal antiretroviral therapy, Iran offers peer support (positive) clubs that provide psychosocial support to people living with HIV, along with voluntary counselling and widespread harm reduction programs (Ghiabi, 2019). Our previous findings suggested that in the face of adversities linked to living with HIV, competent healthcare providers and peers can have a positive impact in helping people living with HIV overcome difficulties in making sense of their experiences and negotiating support. Rewarding and positive relationships with healthcare staff and peer supporters can enable Iranians living with HIV to gain optimal benefits from existing healthcare resources, especially those that are designed to offer sensitive services for people living with HIV. These services exist in a decentralized system across providences, each providing uniform services through triangular voluntary and counselling clinics and peer support network. Access to caring support appears to dilute the experiences of stigma and discrimination from the wider society (and the wider general health system). Existing online and offline support networks in which patients interact with providers and give and receive supportive information to other patients appear to be particularly valued. Thus, the mHealth intervention conceptualized in this study can provide a more streamlined approach by building on existing opportunities, connecting patients to providers more routinely. Crucially, the program conceptualized here can offer support for people who are recently diagnosed with HIV to receive support before multiple episodes of disengagement and before their adherence declines beyond durations that increase the risk of viral rebound (Haberer et al., 2015).
On the policy front, the decriminalization of personal drug possession, medicalization of drug use, recognition of transsexual rights, and provision of sex-change surgeries have certainly reduced the perceived threat of seeking care and treatment for people living with and those at risk of HIV. In spite of this progress, it is suggested that in settings where human rights approaches can be met with resistance, efforts to change “bad” laws can have counterproductive effects, thereby making it more productive to instead build on good policies and programs (El Feki, 2022). When legal reform is met with hindrances, it is important to take advantage of progress that can be made within the economic, medical, and technological realms.
Economic policies and social protection measures have expanded in Iran, with cash transfer policies targeting the bottom deciles of the households, that include key populations that are affected by HIV, more progressively to protect against the economic insecurity that has been identified to lead to despair, treatment disengagement, and thoughts of suicide (Ameli, Taj, et al., 2021; Ameli, Haberer, et al., 2021). Unfortunately, these progressive measures continue to lose their potency in the face of rising inflation and economic sanctions that produce added inflationary pressures (Ameli, 2023; Salehi-Isfahani, 2020). However, medical progress has made positive impacts on the lives of Iranians living with HIV as the uptake of the latest medical guidelines has been met with little resistance within the policy context of Iran, making Iran one of the countries that has adopted most medical policy recommendations, such as PrEP and dolutegravir, for improved HIV prevention and treatment (HIV Policy Lab, 2021). The medical community holds significant societal authority and political power, while including progressive members who have tirelessly fought for progressive change, including the well-being of the HIV community in Iran (Samarasekera, 2021). As such, technological approaches when combined with medical goals have the highest potential to achieve change and implement progress. The Iranian government is highly keen to move toward “smart” provisions of public services to confront challenges that range from fighting corruption to expanding universal health coverage. While such policy prioritizations are combined with an overly optimistic view of technologies, they do open a realm of possibility to deliver services more equitably, including to marginalized populations, by adopting programs such as the mHealth intervention conceptualized here.
Strengths and Limitations
Augmenting the constructivist paradigm with a realist-informed conceptualization enhanced understanding of the value and locations where specific design features have their impacts and potentially produced transferable context-specific findings. A key strength of this study was the co-conceptualization of how mHealth can be useful with and for people with lived experiences of (dis)engagement with antiretroviral therapy in Iran. The findings are deepened because of engagement with the socially constructed realities of living with HIV in Iran, engaging and interacting with stakeholder views, while producing transferable findings for a shared reality in which an mHealth intervention can be implemented and empirically tested. Thus, the advantage of adding the realist analysis to the social constructivist study is that while engaging with subjective realities, were able to produce findings that can be transferable to similar settings through the realist ontological lens (Greenhalgh & Manzano, 2021).
The conceptualized mHealth intervention here can be useful where there is a need for increasing treatment demand and continuity and where treatment supply is not a barrier to successful treatment, but profound stigma, discrimination, and low awareness regarding HIV continue to pose challenges to treatment success. However, this study is only hypothesis generating, through which we attempted to theorize and understand the impacts of specific proposed mHealth design features on living with HIV in Iran or similar contexts. By conducting the study through a social constructivist lens, we acknowledge the subjective nature of the knowledge produced and possibilities for the role of the interviewer to have influenced the findings through their interactions and conversations with the participants. Similarly, we acknowledge that realist evaluations begin with an initial program theory and end with a more refined version of the said theory. By siting at the cross-roads of a social constructionist and realist research paradigms, the findings here cannot be interpreted in “full” realist terms because the data collection processes were not informed by an initial program theory (instead conducted through a social constructivist lens) and as such not meant to be interpreted through a “full” realist logic.
Future Directions
Future research can study the ways in which mobile phones can change the context of living with HIV and relating to treatment, care, and providers. Through a realist lens, the research focus on the efficacy of specific interventions can be expanded to answer more questions on where, how, when, why, for whom, and to what extent mHealth with its various affordances can be incorporated in scale and sustained. Future studies can also explore the contextual dimensions that a specific intervention can address. Investigating how certain mechanisms are triggered within specific contexts can unpack causal pathways and produce transferable concepts that can enhance the design and implementation of future interventions.
Conclusion
This study used local stakeholder interviews to conceptualize how selecting specific mHealth features of offering provider connection, proactive care, and privacy and personalization in communication could mitigate disruptions in treatment within identified adversarial contexts of living with HIV in Iran. Importantly, this study is hypothesis generating, in that we attempted to conceptualize and understand the impacts of specific proposed mHealth design features on living with HIV in Iran. The data on the shared realities discussed were accessed via the socially constructed understandings of interviewed stakeholders. The realist concepts of “context” and “mechanism” enabled unpacking the collected data. Thus, the strength of our findings lies in the contextualized conceptualization, based on stakeholder views, of the role that mHealth could play to prevent treatment disruption in similar settings where universal antiretroviral therapy supply is offered.
Footnotes
Acknowledgments
We acknowledge the members of the Iranian Research Centre for HIV/AIDS (IRCHA), the Voluntarily, Counselling and Testing Centre at Imam Khomeini Hospital, and the Positive Club at Imam Khomeini Hospital. Mitra Sheikhan, Zahra Bayat Jozani, and Nasrin Kordi Ardakani provided invaluable contributions in informing and facilitating this study.
Author Contributions
The lead author (VA) is a female native Persian speaker, who conducted the interviews and is trained in qualitative and quantitative research methods and has received research ethics training as part of her MPH degree at Boston University School of Public Health and as part of her PhD training at the University of Oxford. The lead author’s PhD supervisory team (GW, JB, and FM) contributed to the methodological design of this study and provided constructive comments on the submitted manuscript. GW had the most significant methodological input, especially related to the realist-informed analysis. The local research partner and director (MM), who is an infectious diseases specialist and the founder and director of IRCHA, received the funding and participated in the discussion of emerging themes and contributed constructive feedback on this manuscript. International research partners, who are academic and clinical experts on HIV and mHealth (JH and LS), contributed to the design of the study and to the discussion on the key mHealth features, while contributing constructively to final drafts of this manuscript. LT, who is a trained general physician and HIV researcher, coded the interview transcripts and contributed to the analysis. The analysis of themes and key mHealth features were discussed between the local research directors (MM and VA), a research assistant (LT), a peer supporter (AB), and a psychosocial support provider (TA), who all contributed to the design of the study. The selected design features were then shared with international partners for discussion and feedback (JB, JH, FM, LS, and GW).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded as part of a grant from Tehran University of Medical Sciences and Health Services (97-02-55-38693), Ministry of Health and Medical Education, Tehran, Iran.
Ethical Statement
Data Availability Statement
Data are available on reasonable request. Transcripts from interviews and focus group discussions are available upon reasonable request from the corresponding author. All transcripts are saved in the original language of respondents.
Appendix
The following are the main questions which will be discussed in this qualitative study: