
Abstract
This study feeds into ongoing discussions on the metaphors used by cancer patients. Its aim is to explore how women living with a history of breast cancer use metaphors to express and interpret the experience of cancer remission. Data were collected in interviews designed to capture a rich and metaphorical description of participants’ experiences with breast cancer and what these experiences mean to them. Ten participants were recruited. An interpretative phenomenological analysis of the participants’ narratives highlighted a central metaphor: the cancer trace in one’s life. The participants had to adapt to four specific traces of cancer: (1) the identity trace, (2) the existential trace, (3) the bodily trace, and (4) the narrative trace. We discuss how cancer challenges one’s sense of biographical continuity and initiates a search for a new way of being. We also discuss how the metaphor of the trace differs from the metaphor of the cancer hero living without any trace of cancer.
Keywords
Introduction
The present study feeds into ongoing discussions on the metaphors used by cancer patients. Contemporary Western medicine is imbued with warlike imagery and presents itself as a potent curative activity, aiming to counteract diseases (Marin, 2013; Parsi, 2016). This is evident through metaphors such as fighting cancer and winning the war against cancer. By promoting beliefs and values emphasizing the use of force and dominance, the war metaphor may reflect more of a societal approach to illness and death rather than an attitude specific to individuals experiencing cancer (Marin, 2008). Nevertheless, its combative logic remains a cultural imperative, requiring individuals to position themselves in relation to it (Willig, 2011). It has become the prevailing way to interpret cancer, sidelining emotions and narratives that do not align with it and, consequently, do not fit into the public discussion of cancer (Nie et al., 2016; Surh, 2021; Tate & Pearleman, 2016).
Surviving Breast Cancer: A Winning Battle?
The war metaphor appears to be particularly problematic for women in remission from breast cancer. Indeed, breast cancer is the most frequently diagnosed cancer among women in Western countries, accounting for approximately 25% of all new cancer cases in women (Canadian Cancer Society, 2022). Conversely, this type of cancer boasts the highest survival rate, with a 5-year survival rate surpassing 85% in high-income countries (World Health Organization [WHO], 2023). Consequently, there are a considerable number of women in remission from breast cancer, and they are prominently featured in public discourse about cancer, which portrays them as heroes, survivors, and triumphant fighters (Haines et al., 2010; Nielsen, 2019). However, the “cancer survivor” metaphor, rooted in the combative logic, falls short for many women who fail to see how it accurately represents their new life following cancer, which is characterized by ambiguity in relation to concepts like normalcy and health (Kaiser, 2008; Saraga et al., 2018; Williams & Jeanetta, 2015). As Sontag (1978) argues, it is vital for patients to move beyond the metaphors present in popular discourse to avoid alienating themselves from a meaning that does not correspond to their singular lived experiences.
Qualitative research has shown that being free of a tumor does not mean the end of the illness experience. Concluding cancer treatment does not equate to forgetting about the disease or returning to a state of normality (Koutri & Avdi, 2016; Mino & Lefève, 2016; Rees, 2018). A life-threatening illness like breast cancer can bring about substantial physical and existential suffering, encompassing challenges such as undermined identity, altered relationships with oneself and others, loss of physical security, diminished agency, reduced energy, and search for meaning (Hvidt, 2017; Knox, 2020; Rosedale & Fu, 2010; Trachtenberg et al., 2019). Among women in remission from breast cancer, fear of recurrence emerges as one of the most frequent causes of suffering (Martinez Arroyo et al., 2019; Simard et al., 2013) and seems to underlie the apprehension of mortality and the perception of vulnerability (Almeida et al., 2019; Thewes et al., 2016). On the other hand, some women in remission from breast cancer perceive their lives as changed, forming a deeper connection with the meaning of life and displaying increased concern for themselves and others (Drageset et al., 2016; Pascal & Endacott, 2010). More generally, it seems the women surviving breast cancer need to integrate the enduring effects of the disease into their daily lives and personal narratives (Smit et al., 2019). As Le Boutillier et al. (2019) suggest, “living with and beyond cancer is an experience that disrupts implicit assumptions about life and forces people to reconstruct their perspectives on self and future.” (p. 952).
Cancer Metaphors: The War and Beyond
The growing body of work on the use of metaphors in oncology is mainly composed of editorial and theoretical articles, which reveals a lack of empirical research on cancer patients’ personal metaphors. Indeed, most studies that have proposed or discussed cancer patients’ metaphors were rarely inductive research based on patients’ experiences of cancer. According to literature on this topic, cancer discourses abound with military metaphors, but they also contain other metaphors that conflict with the former and warrant special attention (Harrington, 2012; Parsi, 2016; Surh, 2021; Tate & Pearleman, 2016). Although the war metaphor presupposes a misleading sense of action for some patients, it remains ambiguous as it invokes empowerment for others (Bodd et al., 2023; Semino et al., 2017). Some women affected by breast cancer appropriate the war metaphor to reverse its meaning, revealing how their bodies, through treatment, have become a “medical battlefield” that threatens their human integrity (Guité-Verret & Vachon, 2021, 2023; Hulse et al., 2024). Some women employ other metaphors such as “cancer life as a puzzle,” “unveiling” cancer-related suffering, or “cancer as an imprisonment” (Appleton & Flynn, 2014; Gibbs & Franks, 2002; Guité-Verret & Vachon, 2021; Hommerberg et al., 2020). Also common, the journey metaphor could foster a more holistic and existential view of illness, prompting reflections on self-narrative, life changes, and death (Guité-Verret & Vachon, 2023; Harrington, 2012; Hvidt, 2017).
Objective
The paucity of inductive research on cancer patients’ metaphors, and cancer survivors’ metaphors in particular, has led to an incomplete understanding of their complex language and experiences. The present study aims to better understand the experiences of women living with a history of breast cancer by analyzing the metaphors they employ to describe their experiences.
Methods
Theoretical and Methodological Framework
This study was conducted within a constructivist framework (Ponterotto, 2005) and employed an interpretative phenomenological approach (IPA) (Smith et al., 2009). We reference Ponterotto’s (2005) description of constructivism as a research paradigm consistent with IPA (Smith et al., 2009). It is important to note that when we mention interpretative phenomenology, we are emphasizing its premise that discovering the essence of a phenomenon is impossible due to the inherent nature of interpretation. This position aligns with the hermeneutic tradition of phenomenology. While our focus as researchers was on capturing the manifestation of each participant’s experience, we recognized that our interpretation played a role, contributing to the understanding of the phenomenon. As constructivist researchers, we adhere to a relativist position that acknowledges multiple and equally valid realities (Ponterotto, 2005). We argue that meaning emerges from the interactive dialogue between researchers and participants (Ponterotto, 2005).
IPA aims to capture how people interpret their lived experiences, with a focus on personal meaning in a particular context (Smith et al., 2009). As IPA is strongly influenced by hermeneutic versions of phenomenology, it rejects the idea of producing a pure description of a phenomenon (Tuffour, 2017). IPA stipulates that researchers always interpret the phenomenon they study, referring to a “double hermeneutic” in which the researcher interprets the way an individual interprets their experiences (Smith et al., 2009). From this perspective, our research started “from connection instead of detachment” (van Wijngaarden et al., 2017, p. 1740). IPA is a process of openness to participants’ experiences, which is made possible by the acknowledgment and limitation of our pre-understandings of these experiences (Smith et al., 2009). We pursue our inquiry on the basis of our experiential and theoretical sources of knowledge, while being reflexively aware of our methodological and ontological assumptions (Willig, 2012).
IPA is consistent with metaphorical analysis (Shinebourne & Smith, 2010). Metaphors are integral to how we understand the world (Lakoff & Johnson, 1980). According to the hermeneutic phenomenology philosophers Ricoeur (1978) and Gadamer (1989), metaphors are considered habits of language. Human beings have the great capacity to interpret their experiences by creating metaphors because they need to understand the meaning of what they experience (Ricoeur, 1978). Metaphors are a vivid source of meaning, producing a deviation from the usual use of words and thus enabling a redescription of reality (Ricoeur, 1978). In other words, the creation of metaphors is the emergence of a new way of questioning and living in the world. From this perspective, the creation of metaphors enables us to go beyond the resources of ordinary or scientific language. The creation of metaphors is particularly interesting when a person is affected by an illness, as their medical journey is at first highly associated with a scientific objectification of their experiences. Metaphors are an integral part of the subjectivation process that underpins the interpretation and integration of suffering and changes. Metaphors can be used to clarify experiences as well as to elaborate understandings and provide new healing narratives (Finlay, 2015).
Metaphorical mental representations can also reflect embodiment, that is, one’s feeling, sensing, and relating. According to the phenomenological theory that explores embodied metaphors (Finlay, 2015), language reflects a way of being in the world, including our embodied intersubjective experiencing and our embodied capacities to take on self-movements, activities, and projects.
Participants
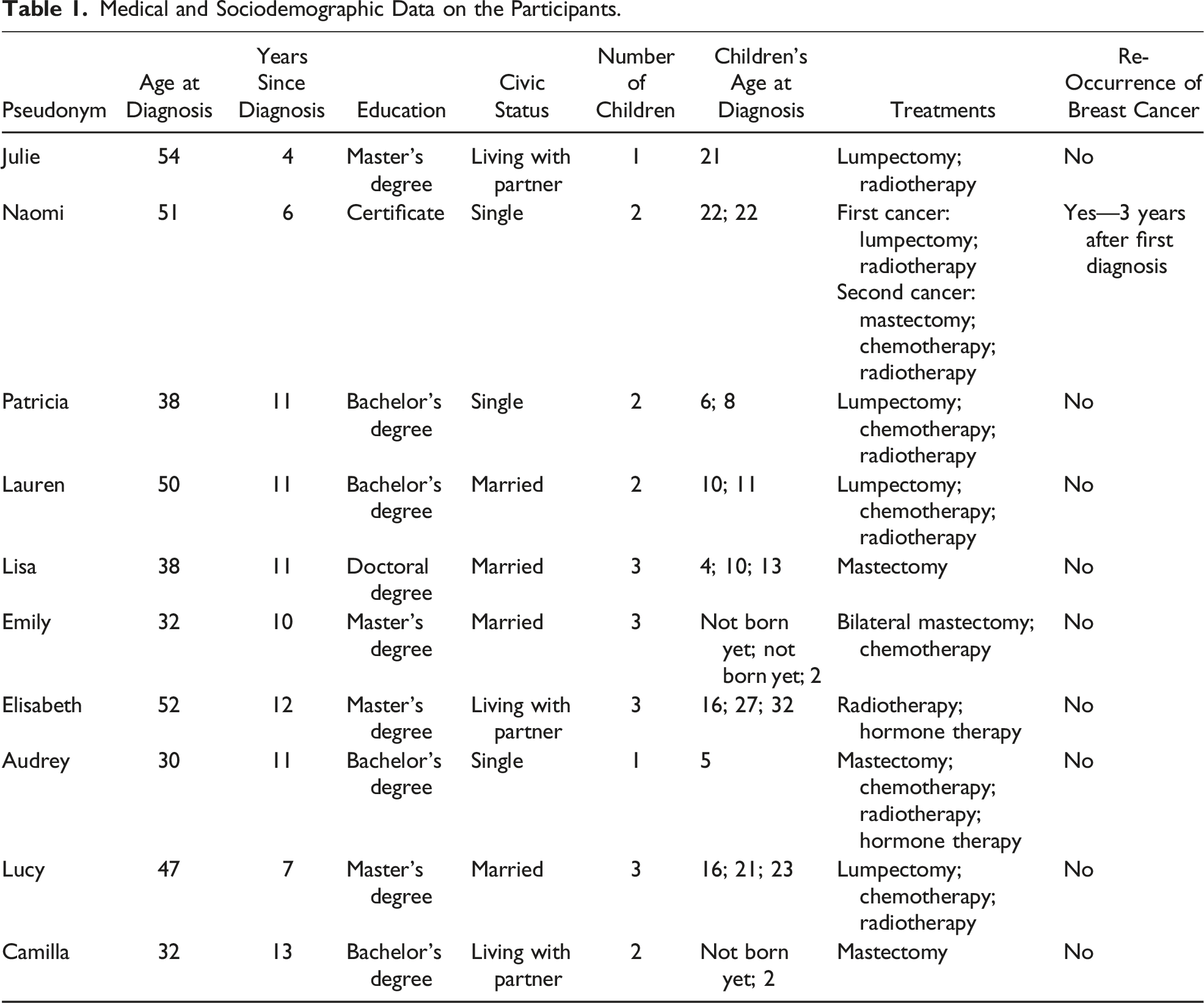
Purposive sampling was used as recommended for IPA studies (Smith et al., 2009). We intentionally selected participants with unique experiences who could provide rich insight into our research question. The recruitment of 10 participants was carried out via social media (researchers’ professional network, breast cancer group pages) and local cancer organizations. The inclusion criteria were (a) having a breast cancer diagnosis and being at least 1 year post-treatment; (b) being over 18 years old; and (c) being proficient in French. The choice of a 1-year post-cancer period as the primary inclusion criterion, as opposed to 5-years post-cancer, was deliberate. While the latter aligns with medical criteria for cancer remission, “remission” is a medical label that is not necessarily meaningful for women, and many women begin to feel isolated as they enter the 1-year post-cancer period due to the assumption that cancer is a past ordeal (Powers et al., 2016). To avoid perpetuating the isolation felt by women within the 1- to 5-years post-cancer timeframe and to maintain a non-medical approach, we included women who were at least 1-year post-treatment.
Medical and Sociodemographic Data on the Participants.
Data Collection
Qualitative data were collected in the form of personal narratives. Individual interviews were carried out by the first author between November 2021 and January 2022, each lasting between 60 and 180 min (M = 94). The interviews were conducted in the province of Quebec, Canada, at the locations chosen by the participants (house, workplace, and café) (n = 7) or virtually using an online platform (n = 3). We adhered to public health recommendations relating to the COVID-19 pandemic.
Each interview began with the following introductory statement: “Please tell me about your motivation to participate in this research study.” After, participants were encouraged to elaborate on their stories using the following question: “Can you tell me what has happened to you from the time you first suspected cancer until now?” As part of the hermeneutic dialogue, prompting questions were also asked to help each participant deepen their understanding: “What do you mean by this? Do you have an image to describe this? How did it happen? How do you feel about this?”
Throughout the interviews, we did not ask about cancer metaphors, nor did we tell participants that we were paying particular attention to the metaphors they employed. We assumed that metaphors appear spontaneously in the process of making sense of lived experiences and that individuals are not always aware that they are speaking metaphorically (Ricœur, 1978). These assumptions allowed us to adopt an inductive approach, as we did not impose metaphors on the participants or artificially create them. We encouraged participants to develop a sense of their experiences and fostered their language creativity.
Ethics
This study obtained approval from the local ethics committee (Université du Québec à Montréal, no. 4615, approved on March 3, 2021). All participants provided verbal and written informed consent to the first author prior to data collection. We extended our ethical considerations to the interpretation of human suffering in qualitative research, prioritizing a posture of humility with the participants and acknowledging the universality of finitude on which we could build a more reciprocal relationship with participants during data collection and data analysis (Bourgeois-Guérin & Beaudoin, 2016).
Data Analysis
IPA is a flexible and creative process rather than a rigid and linear method (Smith et al., 2009). The “hermeneutic circle” is perhaps the most resonant idea of it: the process of interpretation happens through thinking, digging, and connecting (Smith, 2007). IPA allows to go beyond initial themes and uncover latent meanings, enabling an interpretative understanding of the data (Smith et al., 2009). In conformity with the IPA idea of “double hermeneutic,” we interpreted how each participant construed the experience of breast cancer. This interpretation was based on the themes and metaphors that each participant spontaneously expressed during the interviews. We assumed that the first hermeneutic involved engaging with the metaphors created by the participants. The second hermeneutic consisted of interpreting the meaning of these metaphors in relation to their individual experience of breast cancer. Considering this, we adapt the steps of IPA to metaphorical analysis as follows: (1) Immersing in the data by reading the first case while taking reflexive notes; (2) Developing emergent themes (“meaning units” and metaphors) and associating them to participants’ quotes; (3) Identifying connections among the emergent metaphorical themes; (4) Repeating steps 1 to 3 for each case; (5) Looking for patterns across cases; and (6) Presenting a general meaning structure through the interconnected metaphorical themes.
It should be noted that the data collection, analysis, and writing of the article were carried out in French. The article, including the participants’ quotes, was translated into English at the end of the research process. Translating the metaphors into English did not pose any problems, as the two languages are culturally close and share a world of representations and expressions (on the equivalence of English metaphors to French metaphors, refer to Metaphors we live by by Lakoff and Johnson, 1980, and its French translation).
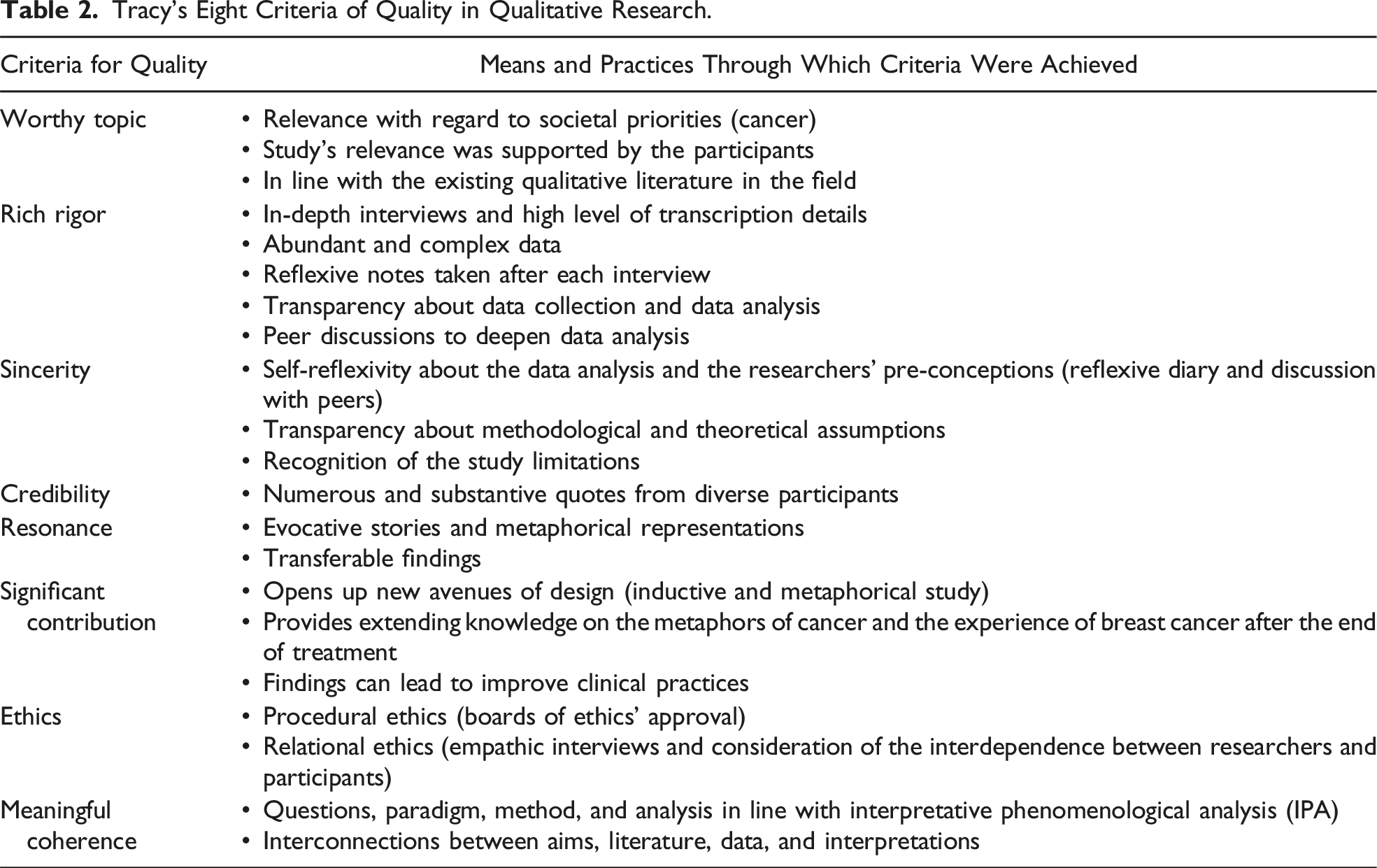
Rigor
Tracy’s Eight Criteria of Quality in Qualitative Research.
Results
The analysis highlighted a central metaphor describing the experiences of women living beyond breast cancer: the cancer trace in one’s life. The women we met had to adapt to four specific traces of cancer: (1) the identity trace, (2) the existential trace, (3) the bodily trace, and (4) the narrative trace.
The Identity Trace
The analysis revealed that coming face to face with a serious illness can lead to an identity rupture: the self is no longer a given and one’s sense of self changes. When reflecting on the time of diagnosis, all participants employed underlying metaphors like shock, rupture, and fall, which represented a personal collapse. They felt an urgency to know more about who they were and who they became: At that time [the diagnosis], I begin to see a glimpse of who I am. Because I don’t know who I am … And when you have cancer and you don’t know who you are, it’s an incredible blow. So before I die .... I want to know who I am. It’s a whole life, I mean, it’s not easy. Nobody really knows who they are. (Julie)
In retrospect, most participants considered themselves a “pillar” before cancer happened—they felt quite strong and psychologically sound. Yet, breast cancer was experienced as the collapse of the pillar they once embodied. Metaphorically, they felt a shift from a sense of solidity to one of vulnerability and personal instability.
All participants spoke specifically about the central meaning of motherhood in their identity and suffered from the rupture that cancer had caused in this maternal identity. Before cancer, they had seen themselves as the “pillar of the family”—the ones who provide support to their children, are present, and take care of the domestic home, offering both material and emotional security. The collapse of the pillar of the family represented a threat to their ability to fulfill their role and responsibility: What has been hard is that for a child, you know, parents are indestructible. They will be there all the time. They are present. And when you have cancer, you’re kind of distressed. It becomes an obsession. (Camilla) Life had changed ... I was the pillar of the family. I was dynamic, I was fit, I was healthy, I ate well, I didn’t drink much, I exercised, so ... I didn’t expect cancer. I saw it as … as a failure. And I was very concerned that I would have to live long enough for my daughter to be an adult because … It was mostly me who paid the bills, and it was my house. And I didn’t want my daughter to live with someone who wasn’t smiling anymore. (Elizabeth)
Most participants recounted how their cancer diagnosis sparked a fear of disrupting their children’s lives and their relationship with them. This was reflected in a profound fear of dying, that is, of leaving their children behind thus failing radically. Experiencing and remembering one’s collapse often implied self-deception, powerlessness, and even guilt: I left my son aside [during treatment] [her voice breaks]. I didn’t have the energy to take care of him, to be attentive. At the beginning, I was very focused on my relationship with my son. I wanted to rebuild it. I wanted to remind him that I’m there for him and that I’m not going to disappear. I think the relationship is back now ... But I’m sure it left a trace. (Camilla)
All participants also expressed great efforts to maintain their image with their children. They needed to shield their children from suffering in order to remain a pillar as much as possible. They tended to suppress part of their emotions in front of their children, avoiding revealing their suffering self. Many participants also needed to limit their children’s assistance to prevent a reversal of roles, which would have confused their identity: Some women received a lot from their children, you know. I couldn’t say that. I rejected all that. Rightly or wrongly ... Sometimes people would tell me to take care of myself. Forget about it! It wasn’t what my heart or my head or my body was telling me. It was all my children. So I probably ignored certain needs I might have had, at times, to rest or let out anger ... But I didn’t enter that zone. (Lucy)
We see there is a metaphorical “zone” that is at risk to enter, emotionally heavy and potentially dangerous for maintaining one’s identity. It is possible that the effort to remain the same strong person in the eyes of their children could give them a sense of their former self and so temporally reduce the identify gap.
Experiencing personal collapse prompted reflections on how to navigate their roles as mothers in the presence of cancer and how to serve as models of resilience for their children. They sought to pass on a way of living and overcoming the collapse, to be a pillar again. This transmission could contribute to rebuild their identity: I told myself that, as a mother, I had a dream opportunity to show my children what it’s like when life slaps you in the face. I said to myself: “I must be brave.” I was educating them. I told myself that someday they, or their partner, or their children, would have to face this. That’s life. I told myself that they’d remember. I strived to live through it in a way that they could learn from and apply to their own lives. My children will draw a lesson of courage from my experience. (Lucy)
The metaphor “when life slaps you in the face” echoes the violence of human life, which strikes without warning. However, it was possible to draw something from this harsh reality. Through transmission, the fallible self could be magnified and serve the children’s personal growth, allowing one to reconnect with the person they want to be.
The Existential Trace
For all participants, an important trace of cancer was an awareness of their own finitude: their mortality, their limits, their uncertainties, the loss of confidence in their failing bodies, the loss of a sense of security, and hypervigilance. Many participants interpreted this awareness as an existential knowledge that must be woven in the fabric of life: Death is part of life from then on. Because before, you knew you were going to die one day ... But now, I know the cancer could come back ... I’ve noticed that it’s not the same trace as at the beginning. It’s not as strong as in the early years. (Elisabeth) Everything is urgent. Even today. My unconscious knows that I have a sword of Damocles hanging over my head. I’d better do what I have to do. Cancer makes you take action. (Lauren)
The metaphor of the “sword over one’s head” shows how death can cast a weighty shadow over existence, propelling one forward while keeping one’s mortality in sight. This heightened awareness of finitude is most intensely felt in the early stages, gaining a more meaningful or nuanced connotation over time.
The analysis also reveals that the existential trace of cancer can be violent periodically. Cancer resurfaces vividly at medical appointments, while waiting for test results, or on important dates such as cancer anniversary. These experiences represented distressing reminders for the participants, reflecting the potential for cancer recurrence and their own vulnerability. The overwhelming emotions in the following quote suggest that the secure envelope of the self can be rebuilt over time but remains fragile due to the existential trace of cancer: You always seem to have reminders ... You have your appointment for this, your appointment for that. You’re anxious about making your appointment, so you don’t call the clinic. At some point, you lose your nerve and call to make an appointment. You’ve got your appointment and you’re anxious! You’re about to have a mammogram and you’re anxious! Did the doctor have a funny look on her face when she looked at the screen? Did she do it again because you moved? You interpret everything! (Patricia)
More generally, it seems the post-treatment period gave way to a new relationship with oneself and the world, since cancer experience led to new foundations: I don’t know many women who say “I’m a survivor.” In fact, we’re still alive. I’m more alive than ever because, you know, cancer brought about a journey: to be closer to myself, to know my roots better. (Audrey) I feel like cancer is a layer of my life and I walk on it every day. With cancer, I feel like I’m always a bit on alert for the next one. In that sense, I feel like it’s a layer that’s been added to my life, that I have to deal with. Today, I’m walking on that floor, and it can be fine. Sometimes it’s not easy. Cancer is certainly not behind me ... It’s not next to me, it’s inside me, and under me. (Lucy)
The metaphor of “walking on a different floor/layer of life” evokes the omnipresence of cancer in one’s life. We can imagine that this floor is normally what the body leans on, providing the individual with support on a daily basis—physically as well as psychologically, in line with Winnicott’s (1971) concept of “holding,” reflecting a fundamental sense of security in the world. Several participants mentioned feeling more “grounded” since breast cancer, more present in their bodies and connected to the meaning of life. However, this metaphorical ground is fragile, as if it could crack at any moment. Such ground is therefore paradoxical: it forms the basis of life’s support, yet it also poses a threat to life’s stability. As a floor or ground, cancer is a layer of meaning that is impossible to forget, as it is central to one’s sense of existence. The metaphor of “the layer” also evokes the idea that cancer leads one to feel and understand a deeper layer of human existence, as if one’s floor/ground was less on the surface than before. The metaphor of the “tree’s roots” also alludes to this depth.
The Bodily Trace
The trace metaphor goes beyond representation to deliver elements of embodiment. The bodily trace pertained to how the participants engaged with their body in the world, as well as their sensations and perceptions of themselves. Participants recounted how they no longer perceived themselves as the same since the end of treatment, attributing this shift to the tangible trace left by cancer on their daily lives and their bodies. Cancer altered participants’ self-perception and embodiment, leading to the potential erosion of their self-recognition due to a sense of unfamiliarity. The following quote gives access to a personal metamorphosis that implies a loss of connection to oneself: Every morning, I get up, and it’s a reminder that I no longer have eyebrows. My eyebrows fell out and grew back, but they’re not the same as before. It’s the same with my hair. I’ve regained my hair, and it’s grown back, but I used to have red hair. I had curly hair, and I’ve got this now! It’s no longer red, and it’s no longer curly! It’s not ugly, but it’s not me. It’s not me anymore. It’s very strange. (Emily)
Many participants expressed disappointment with medical interventions’ late effects, if not a strong sense of injustice. The trace of cancer on one’s body acted as a continual reminder of the lack of one’s freedom with regard to the oncological treatments and more fundamentally with regard to cancer. The stigma of radiotherapy tattoos or scars could be linked to feelings of anger, shame, and powerlessness, as the following quote indicates: Consider the tattoos used in radiotherapy! It’s a big gray mark! I’ve got lots of them, you don’t just get one ... Every day of my life, I see the trace of cancer. I see it all the time. It’s a huge mistake to tattoo women. It’s like having cancer for life. You’ll never forget it. It’s a scar ... See, I’m just talking about this, and it makes me want to cry. How could anyone mark me? I was in no condition to make important decisions. (Julie)
For many participants, dealing with chronic pain was also a taxing daily reminder of cancer. It appears that enduring chronic pain resulting from breast cancer treatments was felt as a sacrifice necessary to remain alive. But the loss of one’s healthy body implied powerlessness, depletion, and resignation: I have neuropathy, and I’ve developed severe food intolerances to lactose and gluten, so I don’t feel well on a daily basis. It’s likely because of the chemotherapy. And lately, I’ve had an autoimmune skin disease. You think it all comes to an end after the last treatment! But after that, it goes on and on. It’s one shock after the other. Each time, I try to tell myself: I’m alive, I don’t have cancer anymore, I haven’t had a relapse. But with the accumulation, it’s exhausting. (Audrey) I no longer have pleasant sensations in my breasts. I only have unpleasant sensations, because I have neuropathy. (…) I tell myself it’s a small price to pay. (Emily)
In the first quote, the metaphor “it’s one shock after the other” echoes Merleau-Ponty’s (2013) concept of “I cannot” body. The participants’ narratives revealed an accumulation of obstacles which limited their actions and overwhelmed their consciousness. The second quote points to an “I cannot feel” body—an area of sensitivity and meaning had been lost and is missed. The bodily trace means a possible alteration of a way of sensing.
The Narrative Trace
Participants said that cancer was part of their history and identity. Many expressed discomfort with the concepts of “remission” and “survival,” which fail to recognize the important traces cancer has left in their lives. I don’t feel in remission. It’s living with what is, with what remains, with what’s there. Post-cancer is about everything that cancer destroys in the process. (Audrey) I think you just learn to live with it. I’m living with cancer ... Am I living with breast cancer, or did I get it? It’s never after. Yes, the cancer is no longer in my body, I’ve had treatments, I’ve been followed up once a year ... But it’s still in my head. I feel like it’s never going to go away! I can’t go a week without thinking about it. (Patricia)
The violence associated with cancer inhabits the mind—it is “in” the head. The “destruction” that has taken place turns representations and thinking upside down. It is not always easy to place cancer in the chronology of one’s life because of its ambivalent “location”: cancer is not in the physical body, but it is present in daily life in the form of fear, pain, grief, powerlessness, a sense of urgency, and a sense of intimacy.
Participants seemed to need to integrate cancer into their life story, to include it among the other ordeals and joys of life. Many kept a trace of cancer in very concrete objects that symbolized it and preserved its memory (e.g., photo album, wig, and medical guides). In a way, these objects prove that cancer happened: I had made a photo album to document this journey. It’s not very big. I just needed a kind of transition, not a transition ... a trace! Of all that. I don’t look at it very often. But my kids do. It’s in the bookcase downstairs, with the other photo albums. (Emily)
It appeared important for participants to share with us how their relation with cancer has evolved over time: Every morning, when I put my prosthesis on, I’m in contact with cancer, and every evening when I take it off, there’s a trace ... I’d say it’s a lot more integrated than it was in the first 2–3 years, when I was very distressed to see my scar ... And I remember that during my psychotherapy, I realized with the psychologist that I was still talking about my “wound.” It had been 5 years, and I was saying “my wound hurts.” I no longer had a wound! It was over: it was a scar. But I kept saying “my wound”! And I became very moved and said to myself: It’s still open, for me, as an experience. Over time, it went from “wound” to “scar,” then finally to “trace.” (Lisa)
The metaphor of “the open wound” suggests the importance to gradually “close the wound” and learn to recognize it as a “trace.”
It is worth adding that most participants expressed regret over the lack of information they had received about remission or post-treatment effects during their medical trajectory. Many expressed feelings of powerlessness, surprise, and even betrayal regarding this issue. Helping other women to be more aware and prepared for the post-treatment period was the participants’ primary motivation for taking part in this research.
Discussion
The trace metaphor suggests that cancer is not an ancient story for women who have been treated for breast cancer. In this study, the women were deeply aware of their relationship with cancer and how this relationship persists but also evolves over time. They thought about cancer in relation to their past (Who I was before cancer? What could I do before?), present (Who I am? What can I do today?), and future (What I can hope for the future? What can I transmit?). Our results revealed that the relationship between the self and cancer remains strong years after diagnosis and extends beyond medical issues, coming to consciousness even though the cancer (the cancerous tumor) is absent.
The trace metaphor clarifies how living with and beyond cancer necessitates the restructuring of one’s identity to sustain meaning and continuity within existence (Le Boutillier et al., 2019; Marin, 2008). Cancer is a life-changing process that opens up a path of existential insight and transformation (Hvidt, 2017; Sekse et al., 2009). This process is a search for a new way of being, that is to say, a search for a new agency through the creation of a new basis and new norms (Holmberg, 2019). Living with and beyond breast cancer means taking part in a journey of reconciliation with life, striving to give meaning to the traces that cancer has left in one’s existence. Speaking in terms of trace reveals an effort to subjectivize cancer experience and the underlying existential shock. From “wound” to “scar,” then finally to “trace,” we observe an evolution in the way participants sense the presence of cancer in their bodies and daily lives. The trace represents a soothed mark, unlike the open wound, as if the passage of time and the subjective integration of suffering allowed for this evolution. In this regard, it is worth noting the fundamental ontological distinction between the subjective body as one experiences it and the objective body as it has been scientifically investigated by clinicians (cf. Merleau-Ponty, 2013). The trace metaphor captures the way in which participants found themselves in the world and feel themselves, once again engaging in projects, relationships, and activities, acting on their new possibilities and limits. In this perspective, we can conclude that the women we have met shared stories consistent with a common trajectory reported in previous qualitative research on the cancer experience: from the shock of diagnosis and the disruption of the self to the integration of the disease into one’s own identity. Our study adds complexity to this trajectory by describing metaphorically how women can live with the traces of cancer.
Our study contributes to ongoing discussions on the metaphors used by cancer patients by describing the trace metaphors, which were spontaneously created by women affected by breast cancer. Our study therefore proposes an alternative to the war metaphor that is widespread and deeply embedded in the discourse on breast cancer. The women we met had to contend with the numerous traces left by cancer—they had figured out or were still trying to figure out how cancer traces would be integrated into their daily lives and life narratives. Their challenge was not to deny or fight against cancer, as if the cancer traces could simply be erased, or as if the cancer had not occurred. In this regard, integrating the traces of cancer in one’s life is not consistent with the war metaphor which implies winning against and overcoming cancer. Indeed, integrating the reality of breast cancer means living it as a part of one’s being rather than engaging in a battle against it. The participants’ attitude was not combative. During interviews, all participants openly discussed their personal experiences of collapse and the suffering they had endured or were still enduring. They also reflected on how they could transmit to others (especially to their children) a way of living with dignity through this ordeal. When participants wanted to regain a sense of solidity and empowerment, they used the metaphor of the pillar, readily relating it to their maternal role. It is also clear that the image of cancer as an outside intruder puts into question the image of a trace that portrays cancer as an inside and embodied phenomenon. It is precisely as a trace that breast cancer persists as an experience and requires ongoing, iterative personal examination over time. Furthermore, the war metaphor involves binary oppositions such as good–bad, illness–health, normal–pathological, triumph–failure (Laranjeira, 2013). However, the participants’ narratives were ambivalent and therefore more aligned with other metaphors such as “cancer as a journey” and “cancer life as a puzzle,” as found in previous empirical studies (Bodd et al., 2023; Gibbs & Franks, 2002; Guité-Verret & Vachon, 2023).
In modern societies, we expect medicine to fight against cancer, completely cure us of diseases, and restore us to our previous state (Bachler, 2020). However, this belief is an illusion that can ultimately lead patients to experience disappointment or hold unrealistic expectations about remission (Marin, 2008). As Canguilhem (1991) argued, healing refers to one’s ability to establish new standards for living. In the case of cancer, this implies the pursuit of a “new normal” instead of reverting back to the previous normal or societal norms (Appleton & Flynn, 2014). Our results suggest that women living beyond breast cancer set new goals, reshape their identity, and discover new ranges of possibilities and limits. These profound life transformations are accompanied by suffering, particularly within the context of chronic pain, but they also yield valuable insights that aid in living and fostering a more authentic existence. In this sense, the concepts of survival and remission may not be precise enough to describe the participants’ experiences. The concept of transformation might be more accurate, as it seems that women found a new way of living in the world, establishing a new approach to life and experiencing with a new way of being oneself. The concept of transformation also accommodates various types of change and the possibility of experiencing well-being despite changes. In this regard, it is possible that resistance to adaptation to the multiple traces of cancer contributes to deeper suffering, such as when the individual seeks to return to their previous state, fights against change, or deals with loved ones who expect a return to the previous state.
As Ricoeur (1992) argued, the manner in which human beings interpret their experiences and construct narratives about their lives is influenced by collective narratives. For this study, it seemed difficult for many participants to deviate from collective narratives that promote a fighting and positive attitude toward cancer (Rosedale, 2009; Trusson et al., 2016; Willig, 2011). They shared stories in which we perceived a certain fear of revealing the suffering associated with cancer and its late effects. This fear appears to be related to their identity as mothers (i.e., avoiding frightening their children or imposing a care role on them) and as human beings (i.e., remaining the same person, remaining a pillar).
Our study also emphasizes that the maternal role holds particular significance within the trajectory of breast cancer, as any alteration to it poses a threat to one’s identity. We found that breast cancer can introduce a novel way of being inhabited by motherhood because being a mother affected by cancer can lead to a unique way of thinking about oneself and relating to others. Other research has shown that cancer disrupts an individual’s ability to fulfill their familial role (Hansen et al., 2019; Park et al., 2017; Semple & McCance, 2010). In addition, while some feminist research has highlighted that the experience of breast cancer challenges hegemonic discourses of femininity, often resulting in women’s bodies being seen as having diminished value in terms of beauty standards (Parton et al., 2016), our study sheds light on other facets of women’s reality: human responsibility and parental transmission. Our study opens up a new avenue by highlighting the importance of passing on to children an inspiring way of overcoming illness and by remaining a pillar for them. It is important to say that the pillar they wanted to continue to be was different from the initial pillar they have embodied because the way they were living included a new fragility and meaningful, often painful traces. Our study also highlights the fact that breast cancer impacts mothers throughout their life course, not just when they are young mothers, this age group being the focus of most studies on the experience of parenthood in breast cancer patients (Di Mattei et al., 2023; Faccio et al., 2020). It is worth noting that maternal identity emerged in our data despite the absence of interview questions specifically addressing this issue, underscoring the importance and relevance of further investigation, particularly considering that, statistically, the majority of women have at least one child in Canada. Future research should continue to explore how cancer impacts parental identity and its implications for cancer remission, irrespective of cancer type.
Clinical Implications
This study may be useful for healthcare professionals in their interactions with women who have a history of breast cancer, helping them to validate suffering at the identity, existential, and bodily levels and to support the construction of narrative identity, even many years after the end of treatment. The trace metaphor may represent the experience of being cured but not completely healed. It captures the liminal nature of post-treatment life for women who are deemed biomedically cured but who continue to suffer the bodily and psychological effects of cancer. In this respect, the trace metaphor challenges the meaning of common words such as survivorship and remission, which imply that cancer is in the past. In fact, after treatment, cancer remains present in certain ways and brings forth other challenges. Therefore, in practice, terms such as “survivor” or “fighter” should be used with caution, depending on the meaning women attribute to cancer in their life. For women in remission from breast cancer, the end of treatment often implies a cessation of medical care and a decrease in social support, even though the end of treatment does not mean the end of the cancer experience (Powers et al., 2016; Ueland et al., 2021). This study supports the development of person-centered models of care aimed at improving the long-term quality of life and the support of women in remission from breast cancer. To this end, the application of palliative care principles to survivorship seems relevant (MacDonald et al., 2021). Palliative care principles could be used to establish an interdisciplinary approach to “healing” women who need presence and understanding but do not need to be cured, either because the tumor has disappeared or because they cannot be cured due to chronic pain.
This study also highlights the need for more informed consent from women diagnosed with breast cancer. Research shows that many women with a history of breast cancer faced the unexpected, unaware that they would have to endure lingering symptoms and self-rupture (Holmberg, 2019; Knox, 2020; Rosedale & Fu, 2010). In this study, participants expressed being unprepared for post-cancer life. The gap between expectations and actual recovery raises ethical questions about patient communication. Research emphasizes the pressing need to improve methods of information dissemination at all stages of the cancer trajectory, from diagnosis to survivorship (Boundouki et al., 2021; Tariman et al., 2014). From a psychological point of view, patients’ perception of a lack of information and consent can lead to anger, regrets, misunderstandings, or even a sense of betrayal, making it more difficult to overcome the losses they have faced, such as the loss of pleasant sensations due to surgery and treatment, the loss of activities and relationships, and the loss of a sense of security. By targeting four specific traces, this study can contribute to better informing women affected by breast cancer. Being attentive to patients’ metaphors appears relevant to better understand their realities and foster their understanding through open dialogue.
Strengths and Limits
The results of this interpretative phenomenological study are to be appreciated in light of the meaning that emerges from the description of participants’ metaphors (van Wijngaarden et al., 2017). The rich details we have obtained from IPA can inform clinicians on how to communicate with women living beyond breast cancer in order to better support them. It can be beneficial for clinicians to pave the road with metaphors for serious, ethical conversations with patients (Casarett et al., 2010; Hui et al., 2018; Southall, 2013).
The main methodological strength of this study is its inductive approach, which reveals the metaphors participants spontaneously used to describe their experience. This study shows the relevance of studying metaphors by conducting interviews whose content depends on the participants who spontaneously produce metaphors, as they tell their stories and make sense of their experiences. We also hope this empirical inductive research on cancer patients’ personal metaphors sheds light on the role of war metaphors in the experience of breast cancer. Our study reveals the near absence of the war metaphor in the participants’ narratives and the importance of alternative metaphors. An exhaustive enumeration of participants’ metaphors would also have provided value by offering access to a categorization of all metaphors. In the present study, we chose to highlight a structuring metaphor to illuminate the studied phenomenon, although other metaphors and meanings could have been extracted from the data. It is to be understood that IPA findings are continuously open to new insights and reinterpretation because participants’ experiences are never completely explored and described by researchers (Smith et al., 2009). Another methodological strength of this study is that it gives access to long-term experiences of breast cancer (from 4 to 13 years after breast cancer diagnosis). Our inclusion criteria allowed for an exploration of the enduring impact and profound meaning of cancer long after treatment.
The homogeneity of our sample ensured rigor from a phenomenological standpoint, as it allowed for a more in-depth exploration of the meaning of a particular phenomenon experienced by a specific group of individuals (Smith et al., 2009). But the sample’s homogeneity and the sampling strategy are also limits to generalization. Participants were all mothers and lived in advantaged socioeconomic conditions in Canada, which influences the way they lived and understood breast cancer. In addition, despite the homogeneity of the sample, participants were at different points in the cancer trajectory, one of whom was not in remission according to medical criteria.
Conclusion
This study contributes to ongoing discussions of metaphors used by cancer patients. It describes the trace metaphor as a central representation of the experience of life after breast cancer. The trace metaphor indicates that the cancer experience is a significant part of one’s life course and that its long-lasting effects impact one’s agency and identity. This study fills the gap in the current literature on breast cancer metaphors, allowing for a wider perspective on the different existing metaphors in oncology and the implicit, deep meaning of the intimate experience of breast cancer they reveal.
Footnotes
Acknowledgments
The authors would like to thank Jessica Boivin and Nicole Simard for their help in translating the manuscript.
Author Contributions
AGV and MV conceived and designed the study. AGV collected the data, performed the analysis, and wrote the paper. MV helped deepen the analysis and reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.