
Abstract
Rare diseases constitute a group of conditions that are individually rare, but in aggregate impact between 3 and 6% of the world population. Many of these conditions present during infancy and involve substantial caregiving responsibilities, often assessed via quantitative measurements. However, few qualitative analyses examine lived experiences of parent-caregivers during the early period of their child’s life. The purpose of this study was to examine the meaning that rare disease parent-caregivers apply to the postpartum year using data collected from a semi-structured interview exploring significant experiences over the course of their affected child’s life. We utilized an interpretative phenomenological analysis (IPA) approach to analyze 22 interview transcripts from caregivers to children with several inherited metabolic and mitochondrial disorders, as well as an undiagnosed disease. Our analysis yielded three superordinate themes: Reckoning With the Parent-Caregiver Role, Familial Transition, and Adaptation and Adjustment. Subordinate themes expanded upon these concepts and included distinctions between the parent and caregiving identity, communal coping and shifting of family dynamics, as well as meaning applied to child milestones, anticipatory grief, and parental perception of a new normal. Exploration of these themes in relation to existing literature, as well as future research directions for qualitative research on rare disease caregivers, is discussed. Overall, this work contributes to a growing body of literature exploring the parental experience of rare disease across several condition contexts.
Introduction
Rare, Pediatric-Onset Genetic Disease
There are over 300 million people living with one or more rare inherited diseases, in aggregate affecting 3–6% of the worldwide population with approximately two-thirds of these rare conditions affecting children (Nguengang Wakap et al., 2020). Pediatric rare diseases account for 35% of deaths in the first year of life, and a third of those affected by a rare disease will die before reaching the age of 5 years (Wright et al., 2018). While some rare diseases that affect children are identified through newborn screening, many families experience a lengthy and difficult diagnostic odyssey that does not always result in a disease diagnosis (de Ru et al., 2012).
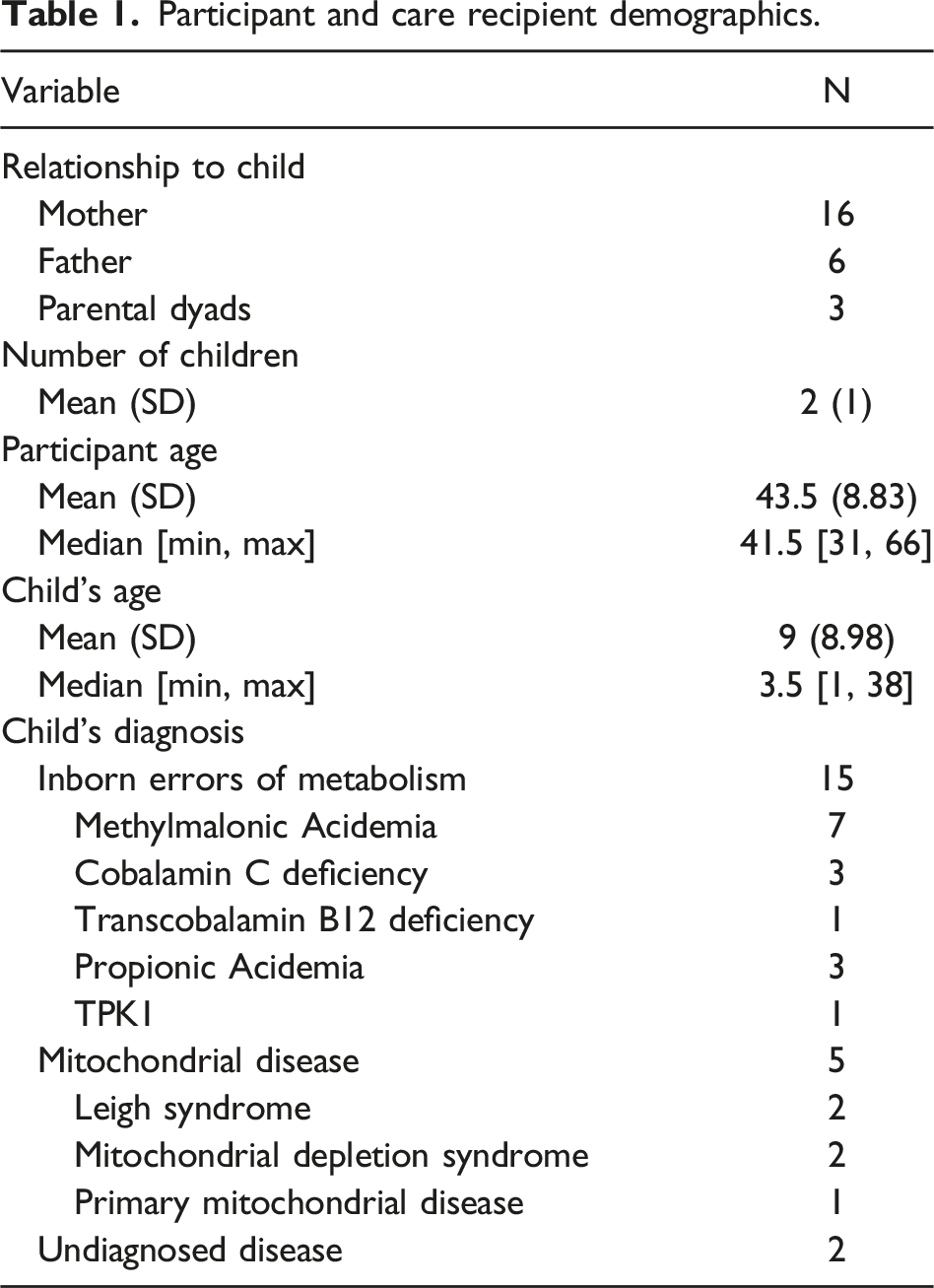
Clinical features, prognoses, and the potential for treatment vary across rare, pediatric-onset diseases. This project, which includes parent-caregivers to children with inherited metabolic conditions, mitochondrial disorders, and a family whose child is undiagnosed, elected to focus on children whose symptoms and conditions resulted in medical complexity within early life. Inherited metabolic conditions, also known as inborn errors of metabolism, represent a class of genetic conditions whose alterations disrupt metabolic processes within the body. When left untreated, they can result in a host of early life symptoms, ranging from stroke, lethargy, poor feeding leading to failure to thrive, and hypotonia (Enns & Packman, 2001). Although certain inborn errors of metabolism, like Propionic Acidemia, are well-characterized and, with proper dietary intervention, lessen the risk for long-term adverse outcomes such as intellectual disability or developmental delay, proper follow-up and identification of all known inborn errors of metabolism is not perfected (Unsal et al., 2022). As a result, infants with inborn errors of metabolism may only be diagnosed after a major crisis event (Waters et al., 2018). Such experiences with metabolic disorders invite considerable medical and prognostic uncertainty, even in the face of a significantly improved prognosis over the past few decades.
Mitochondrial disorders, also a deficit of energy systems in the body, both converge and diverge from metabolic disorders. Similarly heterogenous in nature, several conditions under this umbrella—particularly those included in our analysis—present in infancy, with similar symptoms of neurological findings, including seizures or stroke, as well as muscle weakness, lethargy, and feeding difficulties (Davison & Rahman, 2017). There are no known cures for mitochondrial diseases, and many children facing these conditions continue to worsen or regress substantially as they age. For this reason, we focus on the critical areas of convergence for these families: the postpartum year or year after their child’s birth.
In some cases, the diagnostic odyssey may yield few, if any, answers. The result is that a child is “undiagnosed” but remains medically complex. Although the undiagnosed disease caregivers’ trajectory may differ from diagnosed families due to the liminality and uncertainty of being diagnosed, parents and their children may experience points in their trajectory that dovetail with other condition-specific experiences. Recognizing these convergences is valuable, as undiagnosed caregivers are reported to experience greater levels of isolation in their diagnostic journey. Therefore, understanding communities that these families may be able to connect with to combat that isolation provides valuable theoretical and applied insights (Martinussen et al., 2022; McConkie-Rosell et al., 2018).
The Postpartum Year in Pediatric-Onset Genetic Disease
Despite its often clinically critical nature, the developmental period of postpartum and the early period of a child’s life are under-characterized within rare disease caregiving research. Prior research has characterized the challenges of rare disease parenting across several periods of life, including early-to-middle childhood and adolescence (Siddiq et al., 2016) and future concerns (Weng et al., 2012). Across these accounts, rare disease caregivers report significant burden and challenges, including time constraints, stress, and isolation (Bilginsoy et al., 2005; Eijgelshoven et al., 2013) as well as challenges specific to the parent-caregiver role (Wu et al., 2020). In this early stage of parenting, parent-caregivers of children with rare diseases must balance both the normal adjustment that accompanies the birth of any child with the additional stressors and uncertainty of a medically complex child (Cardinali et al., 2019). Thus, when rare diseases are identified early in life, the stresses of caring for a medically complex child overlap with the transition into parenthood (Buultjens et al., 2013; Cardinali et al., 2019). Research on the diagnostic odyssey, or the journey from onset of symptoms through correct diagnosis and effective treatment, occasionally acknowledges the experiences of parent-caregivers. However, this work is largely focused on the barriers and challenges to receiving a diagnosis (Bush et al., 2022) and offers little on parents’ ascribed meanings to a diagnosis or its process. Carpenter et al.’s work on the early life experiences of parents with children living with phenylketonuria (PKU), a rare inherited metabolic disorder, is one of a few accounts which shed light on parents’ processes in these early months and indicates that there is substantial depth and complexity to how parents navigate the first year of their child’s life when faced with a rare genetic disease (Carpenter et al., 2018).
Using data collected from a life history interview with rare disease parent-caregivers, we examine the postpartum experiences of parent-caregivers of children with several rare genetic diseases, including several inborn errors of metabolism (IEM), mitochondrial disorders, and one case of undiagnosed disease. Interpretative phenomenological analysis (IPA) was selected as the analytical approach because it seeks to explore how participants make sense of their personal and social world (Smith & Osborn, 2003). Our project aimed to better understand how parent-caregivers of children with rare disease construct meaning from their experiences during the first year postpartum, how these meanings overlap across several rare disease contexts, and what their insights might teach us about parent-caregivers’ experiences of their child’s early life.
Methods
Procedures and Participants
Participant and care recipient demographics.
Statement of Ethics
All procedures were approved by the IRB (12-HG-0022). Names and other identifying information were removed following transcription to protect confidentiality of the participants and other individuals noted in the interview.
Analysis
This project utilized IPA framework informed by Smith and Osborn (2003) to analyze parents’ life history interview accounts. An analytical workflow can be seen in Figure 1. Memos were generated for each participant’s interview. Authors designed a memo template that included information relevant to the research questions (topics and information collected in the memos can be seen in Supplemental Table 1). The memo template was initially checked with the senior author (LK) before use and then piloted on two participants. Two authors (HD and SG) then compared their completed memos and provided feedback before continuing to complete memos for each of the interviews. MZ completed memos for several interviewees in which a third perspective felt useful to help clarify insights that were seen by HD and SG. The use of memos within an interpretative phenomenological analysis was intended to capitalize on the immersive process of memo generation (Chenail, 2012). Analytical workflow for manuscript.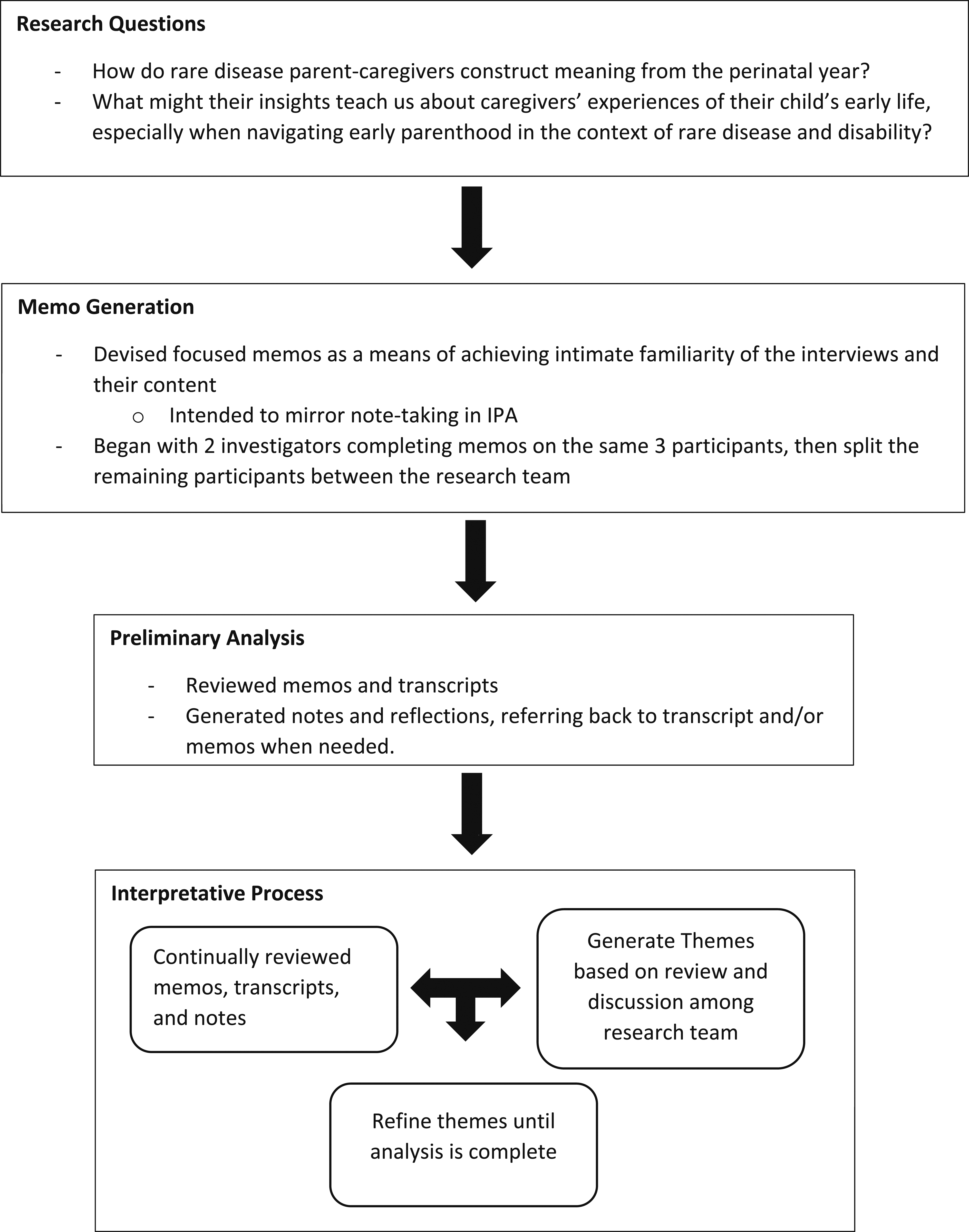
Following a final review of the memos, the authors HD, SG, and MZ entered the interpretative portion of the analysis, which consisted of several iterations of reading/reviewing the memos, transcripts, and personal notes for mention of events and experiences that were related to pregnancy, birth, and postpartum. Themes along these three events were first generated at the participant-level utilizing memos and then compared across participants for convergence and divergence in experience. Through this process, it became clear that the richest interpretative material was found in parental accounts of the postpartum period—events following their child’s birth up to first year—and so our thematic refinement was narrowed to this period of time. Subsequently, authors revisited the data to explore the question of postpartum meanings and to determine if additional themes needed to be captured, condensed, or reorganized. We then began a write-up of our themes which adhered to qualities of IPA described in Nizza et al. (2021).
Reflexive Positioning
Interviews were collected by various members of the team, including a licensed counselor, a licensed social worker, and research fellows associated with the study team. The authors of this manuscript represent several backgrounds, including psychology (MZ, KK, and LK), anthropology (HD and SG), and genetic counseling (HD). Emergent themes were checked with the interviewers as analysis was completed.
Results
Three superordinate themes (identity shift, familial transition, and adjustment and adaptation) were identified. In some cases, quotations are shortened with ellipses (…) for brevity. All quotes are presented with several parental characteristics, including relationship to the child (mother/father), child’s condition, and child’s age. Superordinate themes reflect thematic content that was seen in a majority (over half) of participants’ accounts, while divergence and convergence of these superordinate themes in caregivers’ accounts are described through subordinate themes.
“Having Kids Changes Everything”: Reckoning With the Parent-Caregiver Role
The birth of a child can evoke an identity shift, regardless of a child’s health status. Indeed, parents in our sample remarked on this commonality in their descriptions of their children’s early months. However, what unfolded in their accounts was a narrative inter-woven with conventional ways of “being” a parent in the postpartum period alongside ways of engaging with parenthood that was distinctive to the caregiving role. Thus, parents in our sample not only faced identity shifts reflective of reckoning with a parental identity; they also describe finding their way to “becoming” a caregiver vis-à-vis the early days and months of caring for their children.
Parental Intuition
Several parents made reference to ways of “sensing” and “intuiting” things about their children within the early stages of postpartum. Based on a parent’s subjective understanding of their child, this lay appraisal was distinguished from medical and clinical assessments of a child. However, as aptly described by one parent, intuition was fundamentally in conversation with such assessments as it sometimes provided the initial signal to parents that something was wrong with their child: … [W]e went home on a Friday, so the health unit … said they’d come on Monday to help with the breastfeeding, and latching, and all that, and said to do—it would be fine until then. But my gut said that something wasn’t right, and I honestly didn’t know where to take her. (Mother, Methylmalonic Acidemia, 12 years old) It kind of calmed down a little bit until him bottle feeding and noticing that he was having a hard time, he would choke a lot on it ... and [I] started just kind of noticing some things on his left side that weren’t like the right side. I started thinking like, alright, something’s not right. This isn’t like the other kids. (Father, undiagnosed disease, 3 years old)
Here, both this mother’s and father’s “gut” instincts that “something wasn’t right” is powerful enough to challenge clinical reassurance. Even though this mother felt uncertain of how to act, the process of sensing that something may be wrong with her baby was one way of gathering early data to rebut medical assertions and seek answers to support her child. For this father of an undiagnosed child with medical complexity, comparing his child against his other children and their development signaled that something was amiss and required further attention.
This quote also captures another aspect brought up by several parents: the discordance between a gut instinct and having the tools and resources in this early time to know how to respond to such an instinct. Below, a mother to a daughter with Cobalamin C deficiency shares a similar tension between intuition and despair in the early days of her daughter’s life: I felt like, as a mother ... when you know something—I just felt like something is going on, like something’s wrong, I don’t get it. And when they finally told me that, you know [child had condition], I was just like, “My goodness, like, why couldn’t it, why couldn’t I just,” I felt like It was kind of like my fault. Just, everything, overall. I felt like I could have maybe, I don’t know, eat better or checked up, get checked up more often or something. Or just would’ve noticed her throwing up, you know, that few, first few days or whatever, I should’ve just took her to the hospital—I feel I should’ve did more, as a mom, I should’ve just did more ... (Mother, Cobalamin C deficiency, 3 years old)
Like other parents, she describes a sense of “something … going on” that, after receiving a diagnosis and thus an answer for her daughter’s symptoms, prompts a sense of guilt for being unable to draw connections between her own “data” on her daughter and the clinical insights. In this sense, intuition was understood both as an expanding and a limiting tool for the parents in our sample in regard to their dual parent-caregiving identities.
Micro-Encounters in the Clinic
Each participant described the profound personal impact of early communication about their child’s condition or health status. These encounters took various forms with our participants, including newborn screening follow-up encounters, acute neonatal intensive care admissions, and protracted medical follow-up in the first few months of life after leaving the hospital.
Many participants referenced specific conversations or exchanges—which we deemed “micro-encounters”—with clinicians that often reverberated well past their child’s hospital stay and clinical follow-up. Such encounters stayed with parents particularly when or if grim prospects were offered and operated as signals to parents that their child was not okay. One mother, whose daughter was diagnosed with Methylmalonic Acidemia in infancy, highlights this concept in describing her daughter’s admission to the critical care unit: An event that’s always stood out is when she was admitted to the … pediatric critical care unit—and a nurse told me to go home and get my camera so that I could get one last picture of my daughter. I’ll never forget that nurse, ever [...] [T]hat’s when I was like, “Oh, we might not make it.” I think maybe, that was the moment. And maybe that’s why I remember it so well, because it was like, it’s getting real, right? (Mother, Methylmalonic Acidemia, 12 years old)
For this mother, this single exchange operates as a fulcrum from which she arcs from territory of normalcy into that of having a sick child. These remarks, when held on to in hindsight, signal the start of divergence that will follow these parents, and their children, throughout their child’s lifetime.
Contending With Info-Glut
In most cases within our sample, a diagnosis might be shared with parents during these encounters. Even when a diagnosis wasn’t shared, parents often had to develop the expertise of navigating, integrating, and understanding the medical system and medical guidance within a short period of time. This deluge of information is necessary to contend with, as proper comprehension and understanding of their child’s condition, or alternately, the medical infrastructure, is vital to effectively make decisions regarding their child’s care. In the words of one parent, “… we had a whirlwind of information thrown at us” (mother, Methylmalonic Acidemia, 2 years old).
Such a steep learning curve in the early days, weeks, and months of their child’s life regarding medical information furthered parents’ realizations that parenting their child would be different than anticipated. However, it was also distressing. As illustrated by one parent, who adopted a son that was shortly thereafter diagnosed with Cobalamin C deficiency: … We started trying to look up [condition] and—you know we were finding stuff that was outdated ... but I saw something—there was something that was 80 percent survival rate by age 2, which means 20 percent of those kids are dead. And I just was like, we just got him. That was the phrase I just kept thinking. We just got him. They can’t take him, we just got him ... Even though we found out, you know, very shortly after that that was not the expected lifespan at all. It just echoes. (Mother, Cobalamin C deficiency, 2 years old)
Uniting the deluge of medical information and the micro-encounters with clinicians is the reverberation of prognostic information through time. Such information, as illustrated in this account, has the potential to leave an impact on parents and their narrative of their child’s early life and expectations for their child.
In some cases, parents described medical teams who were sensitive to this information deluge, wherein providers attempted to curb the amount of initial information provided to them at an early onset. However, these approaches varied in their success and value to parents. As illustrated in this interviewee’s account: … the first doctor on the phone, she didn’t want to tell us what she tested positive for. She said no, I’m not going to give you the name, otherwise you’re going to Google it. It’s my decision if I want to Google it. It’s my daughter’s health. So, we actually went first to the pediatrician and then to the geneticist ... without even knowing what she tested for. (Mother, Methylmalonic Acidemia with homocystinuria, 3 years old)
Although an admirable attempt by a provider to not overwhelm a new parent, this overly paternalistic approach highlights a core tension intersected with the info-glut: that parents may be overwhelmed by information yet yearn for control amidst a challenging medical process.
Loss of Freedom
For many, parenthood alters priorities and, notably, the availability of free time. Parents also described a loss of freedom and shifting daily priorities after the birth of their children. Sometimes these feelings were described in association with the normative process of caring for children and the transition to parenthood in general; as one parent remarked, “Having kids changes everything … I think, you know, you just don’t have as much freedom to go do what you used to” (mother, Propionic Acidemia, 2 years old). The concept of losing freedom was also a site of speculation for our participants: parents in our analysis actively grappled with whether their understanding of altered freedom was “normal,” or whether it was amplified due to the complexity of their child’s condition. In some cases, the changes to freedom felt highly distinct for our parents. Seen through one mother’s account of caring for her son: We had an early childhood team evaluate and train us and I basically had to leave my job. And, you know, be a full-time mom …. My sister and my mom and everybody said you have to leave your job if you want [child] to be a normal kid. Because everything is delayed. His speech, his walking, his crawling, everything was impacted … (Mother, Methylmalonic Acidemia, 9 years old)
This mother’s remark illustrates how the loss or alteration of freedom to rare disease parent-caregivers is fundamentally entangled with other complex elements of caregiving. For this mother, the labor of addressing her son’s various disabilities usurped her ability to work outside the home. Alongside her own revelations of how her son’s abilities impact her own mobility is the social projections of family members. These family members’ ideas of parenting values are laid bare in their ideas of how normalcy can be enacted in the case of this child’s life.
Stepping Into the Advocacy Role
By necessity, many of the parents in our sample must find their own ways of effectively digesting medical information and come to terms with the realities of their child’s conditions. In retrospect, many of the parents in our sample describe early gestures toward the necessary role and responsibility of advocating for their child. This is in part distinguished by a sense of mastery over the logistical and medical demands of their child’s condition, as well as a sense of persistence related to getting their child the care and support they need. In effect, advocacy reflects a developing form of caregiver intuition that is often the result of engaging with the medical system under the unique circumstances of receiving care for their child and trying to seek answers: So, going from prior to having my son, where we just, you know, whatever the doctor said was what it was. And then, just how we have changed as parents and moving to, question everything, and advocating, and not just taking an answer from a professional because they're a professional. (Mother, Methylmalonic Acidemia, 2 years old)
In this mother’s reflection, she clearly delineates between what her prior experiences were with medical providers—an attitude of “whatever the doctor said”—to a more critical perspective surrounding medical expertise and guidance. In contrast, other parents in our sample experienced advocacy as a collaboration between them and their child’s care team, often when they found a particular research team, individual pediatrician or other care provider, or hospital system where they felt confident that their child was getting high quality care. In both instances, the demands on parents exceeded “taking an answer from a professional,” instead requiring substantial time, effort, and engagement on the part of parents as an active member in their child’s care.
“The Whole Family Grew Up”: Familial Transition
A child’s illness in early life can reverberate beyond the child and parents themselves to impact the entire family. Caregivers discussed varied impact of early events on the entire family unit during this first year of their child’s life. Parental perception of the impact on the family units and familial transitions manifested in two themes: communally caring for the child as family members accepted caregiving roles and a shift in family relationships and dynamics, often focused on emotional and behavioral reactions.
Communally Coping With Caregiving
Many participants described the process of the family unit communally adjusting to the caregiving experience. Such accounts involved the concept that a family may “come together” in various constellations to help the parents make sense of, or manage care for, their child’s diagnosis and altered life trajectory. This “coming together” took on many forms, including caregiving as a focus of the entire family unit, individuals stepping into new care roles and providing support, and instances of misguided help while navigating caregiving.
In several families, this communal care reflected physically showing up for parent-caregivers and the affected child. The familial support led to descriptions of communal adjustment, cohesion, and positive experiences as the family unit responded to the novelty of, and ultimately learned to manage their child’s illness in the early period of caregiving. Said one parent: So, I think it’s good, I mean, the whole family grew up. Like, it made us stronger, you see. It’s not easy but, as I said, it’s a very big mixture of feelings. (Mother, Propionic Acidemia, 21 years old)
Family members were described as often providing instrumental and logistical support in order to ease the cognitive burden on families. In one participant’s account, the stress of caring for her twins with Propionic Acidemia brought her mother and another relative to her side to provide necessary relief: I remember getting to the point where I called my mom and, I just kind of started talking, and then I lost it, and she immediately came over and started helping. And [family relative] was another person that—everybody did, but [family relative] also came over to help through the night, to kind of help out with the feeds until we got everything taken care of. They helped a lot with [affected child’s sibling] … And that let me kind of get some sleep a little bit ... it just also made me very thankful for my family and [family relative] and my mom and dad, and just everybody that has just, without even asking, they’re, like, there (laughs) to help. (Mother, Propionic Acidemia, child age 2)
In this mother’s account, the flexibility and willingness for her family to help with nightly feeds and caring for siblings—material and instrumental aspects of early caregiving—was an integral part of her early experience caring for her children. Their support offered both necessary time for this mother to rest and return to the demands of caregiving, as well as a reassurance that she was not alone in the process of caring for her children and navigating these new demands.
Although many examples of communal coping within caregiving were positive, some participants discussed examples of misdirected helping in this caregiving support experience. For example, one participant described the experience saying: And my in laws were doing the best they can helping us at great lengths, but that was actually, you know, hampering more. It was, you know, making it more delayed in everything that [child] can do and cannot do. (Mother, Methylmalonic Acidemia, 9 years old)
In cases like these, communal support could effectively crowd out the hopes and preferences of parent-caregivers and, as described by this parent, result in downstream implications for the affected child. An added complexity, illustrated in this account, is the recognition by parents that such communal support is often provided with the best intentions—her in-laws, as she shared, were “doing the best they can,” yet inadvertently posing more challenges to this mother.
Shifting Family Dynamics
Just as the birth of a medically complex child prompted role transition for parents, the dynamics and roles of various familial relationships and connections were also described by several participants in our interviews. These altered dynamics manifested in romantic relationships, larger family contexts, and parent–child relationships and were often described in relation to familial navigation of emotions regarding these early life experiences. However, amongst our sample, the range of impact varied considerably. At its most extreme end, as shared by one parent, “The family dynamics was kind of, I don’t want to use the word shattered, but it was in a way” (mother, Methylmalonic Acidemia, 22 years old).
However, relational changes were also described by some participants in positive ways. Participants described the experience of a sense of spousal or familial cohesion, as well as feelings of gratitude for their spouses in the face of early stressors. As described by one mother: And my husband was very supportive, I mean, he, instead of bringing us apart, it brought us more bonded, because we were helping each other. For our marriage, it wasn’t such a struggle at that, concerning our marriage. Because we really supported each other. (Mother, Propionic Acidemia, 21 years old)
In contrast, participants also shared that spousal dynamics could also be upended by the stressors of caring for a child with a genetic condition. For some participants, this resulted in conflict. For others, like the parent below, individual parents responded with distinct coping strategies to the stress, which in result produced a discordance in response to a child’s illness: And something that marks be a lot about my wife is that she was so strong and wondering immediately what this meant for [our son], and what it meant if one day if he needs us, and we get old and die and he still needs us because of his condition. And still to this day, I can’t believe how strong she was and how those were her only concerns. Where I, in contrast, was thinking so much about, like, selfishly more. Like how did this happen to me or us? Like, oh my God, this is crazy … And so that that whole time was obviously a huge—you know, we had to quickly come to terms, but it was hard. (Father, Methylmalonic Acidemia, 3 years old)
Although shifting family dynamics were described within many different configurations of family members, our sample frequently described how the birth of a medically complex child impacted the child’s siblings in cases where siblings were present. Often, the impact was described negatively, particularly during the proximate days and months of their affected child’s early life. Such cases are reflected by the participant referenced above, on the perceived experiences of her other children: I mean, I think if you talked to my son and my daughter, they would say—it’s not that they felt abandoned at all, but they felt kind of jealous. Every kid works in a different way and feels in a different way, but definitely they felt something was wrong. It wasn’t good for them too, so, it was our main feeling at that point, yes. (Mother, Propionic Acidemia, 21 years old)
In addition to complex emotional terrain associated with this shift in dynamics—jealousy and concern are noted—there is also the active parental awareness that the needs of children are varied and will undoubtedly result in a varied response to a stressful event like the birth of a medically complex child. Similar to this account, many of the parents in our sample who reflected on the impact to their other children acknowledged complex emotional and relational impacts to their children from this early period.
“This Is the Life We’re Going to Lead”: Adjustment and Adaptation
Throughout our interviews, it was clear that each parent experienced the early days and months of their child’s life as a profound, and critical, period of adjustment for which the only way to respond was to adapt. Adaptation took on several forms amongst the parents our research team spoke with. For most parents, early adjustments to expectations manifested in language around a child’s milestones; for parents in our sample whose children’s diagnoses also prompted altered life expectancy, the early months of their child’s life invited early anticipation of grief and losing their child. Finally, regardless of a child’s prognosis, many parents in our sample described events and feelings of “creating a new normal” in their lives that included life with a medically complex child.
Meaning Around Milestones
In the first year of a child’s life, milestones are benchmarks that parents use to track the progression of their child’s development. For children with genetic conditions, particularly those covered in our analysis, developmental milestones are a contested site of experience: children within each of the condition categories included in this analysis may experience developmental delay or regression in milestones. In the case of undiagnosed children, delayed milestones or regression may be one of the first signs to seek medical attention. Such granularity was a key theme in our parents’ accounts of their child’s early life. Their accounts extended this understanding of milestones to also include the consideration of emotional sense-making or speculative thinking. For instance, several parents described the experience of certain milestones as an experience where parents were exposed to the possibility or potential of how a normal child might develop: … we had that brief little window of really good steps, and then we had the decline, and that was really hard, and I know that some families that happen by this disease have kids who typically develop for years, right? And they're walking and talking, et cetera, et cetera, and then their decline starts, and I feel so much tremendous empathy for families who experience that much of a decline. And again, kind of a weird sense of gratitude …. If he had said my name, then stopped being able to say my name, I don’t know if I would survive that. (Mother, Primary Mitochondrial Disease, 3 years old)
For this mother, her own son’s altered trajectory of milestones—described in terms of “steps”—prompted reflection on how other parents navigate such trajectories. Here, she makes sense of her son’s own regression by anchoring his severity in relation to more severe cases. Such anchoring allows her to feel a sense of gratitude, that perhaps it could be worse were she to experience a sharper contrast in regression.
Delay or failure in reaching milestones could also serve as a signal to parents, both of the reality of their situation and as a prompt to adjust their own expectations for their child. Especially since these early milestones may reflect some of the first critical points of recalibration for parents, they were described as especially critical junctures in early parenting. One parent, following a seizure her son had in his first year of life, reflects the following: But after that, he really just lost a lot of his gains that he had been making—and so … he doesn’t reach for things or grab things anymore; really isn’t able to eat anything by mouth, you know, and he is slowly working his way back up and making progress …. So, that was a really hard one because it was just a time when ... we kind of thought things were going okay, and then it just kind of all came crashing down… (Mother, Leigh syndrome, 4 years old)
The story of her son’s seizure and its impact on her family is told through milestones commonly associated with early life. Evident in her account is the notion that, as her son accumulated skills, thereby hitting milestones conventional for a small child, a sense of hope was present that his trajectory may be the exception. However, her assertion that “it just kind of all came crashing down” illustrates a critical revisioning that had to happen regarding her expectations for her child’s developmental trajectory.
In several cases, the experience of hitting an age-appropriate developmental milestone in early childhood was characterized by parents as a powerful triumph or revision on prior expectations. In the words of one parent: … how every milestone, that every parent gets excited about, how—it's amazing how much more excited that you can actually get. That you just can’t understand that. Until you’re there. (Mother, Methylmalonic Acidemia, 2 years old)
Such a remark illustrates how parents in our sample were sometimes highly perceptive of these permutations in their child’s development, paying careful attention to their child’s trajectory and indicators of growth. In another example, a parent explicitly referenced insight provided by a professional and the triumph she experienced: His mobility improvement from the very beginning when all of our physio tests were saying well, he, you know, he needs a lot of work, he doesn’t even get off his belly. To the point where the physio told us, like, we really don’t need to see you much anymore. Like, he’s doing everything that a child his age is supposed to do … was, like, a really nice positive. (Father, Cobalamin C deficiency, 2 years old)
Anticipatory Grieving
Parenting a medically complex child invites profound existential questions surrounding a child’s mortality. For many of our participants, existential reckoning of their child’s fragility invited varying degrees of anticipatory grief. Even in cases where a child’s prognosis might be improved due to medical advancement or improved care management practices—in our sample, this was often parents to children with metabolic conditions—early medical crises or information about a condition prompted some parents to wrestle with the possibility that a crisis could result in the loss of their child: I saw something—there was something that was 80 percent survival rate by age 2, which means 20 percent of those kids are dead. And I just was like, we just got him. That was the phrase I just kept thinking. We just got him. They can’t take him, we just got him. I mean not they but, you know—he can’t go away. So, there’s still I think a little of that. Even though we found out, you know, very shortly after that that was not the expected lifespan at all. It just echoes. (Mother, Cobalamin C deficiency, 2 years old)
In contrast to the episodic awareness of an affected child’s mortality described by parents to children with metabolic disorders, parents to children with life-limiting conditions in our sample faced an early, often ever-present awareness of their limited time with their child. In the words of one parent: … honestly, if you ever Google [condition], it’s like, “Boy, your kid’s going to die real fast.” That’s the message. And so, for me, it didn’t feel like I had to think about a caregiving situation. It was, “You need to prepare yourself for the death of your child.” That was what was out there. (Mother, Leigh syndrome, child age 4)
How parents grappled with this anticipatory grief, and what resources proved most helpful or relevant, could manifest in several forms. Several parents in our sample described a profound sense of emotional reckoning with their child’s mortality. Within these parents’ accounts, an odyssey of feelings are described, often beginning with challenging emotions that, through time, are able to be critically reframed toward a sense of hope or acceptance: Where part of my brain wants to get really riled up and nervous and stressed, and then another fear just comes across and just says, like, it doesn’t matter. Like, is he happy? Is he warm? Is he loved? And so it’s nice … because that sort of seeps its way into the rest of my life, to the rest of my professional life, and everything else, and sort of softens the edges a bit. (Father, Methylmalonic Acidemia, 1 year old) And there—through all of that is the river of bittersweetness that I think every parent experiences, but there was definitely a little bit of bittersweetness of like, is this the only birthday we’ll ever get? That happened every year, but the bittersweetness is not the predominant emotion. The predominant emotion is just gratitude and happiness. (Mother, Primary Mitochondrial Disease, child age 3)
Some of the parents in our sample grappled with the threats to their child’s mortality by turning to instrumental strategies, including the use of palliative care and other forms of long-term planning that incorporate the possibility of losing their child. Later in her interview, the mother referenced above discusses the impact of a palliative care referral as part of her son’s care experience in infancy: … we received a palliative care referral for [child] when he was about seven months old, kind of in between the seizures and the vision issues and the feeding issues, and that was really difficult. At the time, I was very resistant to that and very saddened to be at that point so early in his life ... then we eventually met with the palliative care team and learned more about what palliative care was, and it ultimately became a really critical part of our caregiving. Definitely thinking about how we want to support [child] over the long term, and what quality of life looks like for him, and looks like for us, and how we have those critical conversations. (Mother, Primary Mitochondrial Disease, child age 3)
Anticipatory planning and resources could, as illustrated by this mother’s account, weave into the fabric of everyday caregiving. In other cases, parents acknowledged that keying into these considerations brought them away from the powerful emotions of anticipatory grief, instead providing an opportunity for them to still retain some control in an uncontrollable scenario.
Creating a New Normal
Rare disease families inherently challenge normative family structures surrounding health and resource allocation (Clarke et al., 2020). Such understandings were reflected consistently in our parents’ self and familial conceptualizations. Within our analysis, normalcy had a significant temporal component: in the early period of their child’s life, parents often reflected on reaching a “moment” of settling into routine or “sense” of normalcy in caregiving. Reflection on this early period of time thus highlighted the period of adjustment to caring for and adjusting their lives to meet their child’s needs—thereby highlighting the creation of a “new normal” as a family defined as the period where care for their child became well-integrated into their day-to-day life and overall lifestyle.
Parents recognized this inflection point in different ways. For some, a more abstract sense of reflection on this transition was how they described the adjustment, such as the remarks shared by this parent: I think it really did shift my views on caregiving and my husband’s views on caregiving to, okay, we’re going to be parenting a medically complex child. There had been so many questions marks around that for the first several months, like, which way is this going to go? I think this was really the time that it was like, okay, it’s going to be complex. He’s going to be disabled. This is the life we’re going to lead. (Mother, Primary Mitochondrial Disease, child age 3)
For many other participants, this temporal point of transition was defined via concrete events in the first year of a child’s life that might involve considerable logistic or medical preparation; as a result, their ability to meet these demands placed a “new normal” into view. One participant described a family vacation taken when their child was a few months old as this sort of opportunity: It was great. We went and, just—everything was positive. He was happy, he was smiling. We felt like we had finally started to get in a routine with all of his medicines, and just, kind of—it was a, “We got this” trip. I would say that it probably helped normalize our new normal. (Mother, Methylmalonic Acidemia, child age 2)
Although many of the experiences of these trips were described in terms similar to above—marked by a sense of stability or mastery over their child’s needs—several parents characterize their early decisions to engage in trips and other “normative” family experiences as more of a choice than as a reflection of their mastery. Such a scenario was elaborated on by one parent: … we … had this awful series of appointments and a hospital admission for CB tubes, and then, like a day after we got out of the hospital, we hopped on a plane and went to another family reunion … and I think having those bookended experiences was—I think my husband and I were kind of determined, like, “We’re going to do this, dammit.” (Mother, Primary Mitochondrial Disease, child age 3)
Evident in the above mother’s account is a sense of persistence: in this excerpt, the reunion and choosing to attend amidst medical appointments is an active decision made by her and her husband to continue to live life with their child that is inclusive of non-medicalized experiences. The discernment and decisions that parents in our sample are making in their everyday actions, particularly in the early months of their child’s life, in effect set the expectations for what their family’s capacity and livelihoods will look like over time.
Discussion
The purpose of this paper was to examine the experiences and perspectives of rare disease parental caregivers during their child’s early life. We identified a number of changes experienced during the postpartum period along with ways caregivers made sense of their new realities during this time, which often coincides with their child’s initial diagnosis. Although illness and caregiving trajectories in these groups undoubtedly differ over time within these condition groups, we believe that the critical early life intersections found in this analysis are valuable to highlight. Observation of convergence, divergence, and overall granularity across these experiences may highlight areas to target and tailor caregiver intervention. This is especially the case for caregivers to infants and young children with undiagnosed disease, who may report higher levels of isolation in this critical period (Martinussen et al., 2022). Overall, the themes in this analysis represent disruptions within the self and family under the context of living with rare disease that must be addressed, acknowledged, and processed.
In their accounts of their child’s early life, parents described distinct, yet intertwined, identity shifts reflective of both normative changes involved with becoming a parent and those of becoming a caregiver to a child with a rare disease. This transition to the parental identity, its accompanying roles and responsibilities, and extreme feelings of change are common (Nomaguchi & Milkie, 2020; Saxbe et al., 2018). Although our study does not examine the normative parenting experience, it is important to remember that the transition to becoming a parent is marked by change and stressors regardless of context. This is especially important for families in our sample, whose reconciliation of more normative parental roles and responsibilities may be overlooked in the face of their child’s medical complexity and management (McConkie-Rosell et al., 2018; Woodgate et al., 2015).
Our findings reinforce several themes related to emergence of the caregiver identity, including difficult parent–provider encounters, the need for self-education, and the need to become a parent-advocate (Cardinali et al., 2019; Gómez-Zúñiga et al., 2021). The cognitive demand placed on parents to integrate large quantities of medical information in a short period of time is a known stressor for parents of a child with a rare disease (de Ru et al., 2012; Jacobs et al., 2019; Siddiq et al., 2016). Previous literature of parental caregivers of children with other disabilities also reported a lack of access to tailored information and services early on in their diagnostic journey (de Ru et al., 2012; Rajasekar et al., 2020; Siddiq et al., 2016), as well as feelings of frustration with medical professionals’ lack of knowledge (Kelso et al., 2005). This work extends these findings to illustrate the nuances and conflicting needs parents may have as they enter into this unique caregiving space.
Our analysis highlights distinct experiences that inform parents’ negotiation of both their parental and caregiving identities. What is indicated is that integration of these roles does occur over time but is undoubtedly a complex and conflicting process. In their exploration of the parent-caregiver role formation, Gómez-Zúñiga et al. (2021) propose a conceptual model that accounts for a fluid representation of the relationship between parental and caregiving roles. Future research might explore the critical points of integration of the parental and caregiving roles in parents to children with rare disease, as well as resources and events which support this integration.
In addition to the intra-individual struggle of shifting identities, parental caregivers also described interpersonal changes associated with the postpartum period. Past research has documented how the diagnosis of a chronic condition can impact the entire family system (Gramer et al., 2014; Helgeson et al., 2018; Pelentsov et al., 2016), and indeed, caregivers described how family members “stepped up” and engaged in various care roles. This is consistent with other studies of parental caregivers of children with rare diseases, who often report taking a team approach to managing the illness (Rajasekar et al., 2020; Zajdel et al., 2022) and with other methodological designs (e.g., social network analysis) that identify multiple caregivers in familial networks (Marcum et al., 2018). Collectively, this team approach to illness management was framed as a positive and adaptive approach to managing care. There were also a variety of positive outcomes described, such as partners becoming closer to one another and gratitude for other family members adopting caregiving responsibilities. However, there were some limitations or negative outcomes described by some caregivers in this study when familial support became intrusive or misguided. These maladaptive effects of familial support have also been described in other studies as well (e.g., Rajasekar et al., 2020). Our analysis highlights some of the boundaries of communal coping in this population that may emerge in some familial structures.
Evolving family dynamics were also described more generally, not solely within a chronic illness context. However, the impacts of these evolving dynamics may be exacerbated when caring for a child with a rare disease. One particularly salient change caregivers described was the explicit impact to siblings. The impact on unaffected siblings is a recurring theme amongst qualitative methods (see Granovetter et al., 2023; Rajasekar et al., 2020), indicating the need for future studies to pay close attention to these individuals. Additional family dynamics were also described by our sample and often appraised in terms of the valence—ranging from positive and negative, to ambivalent. As caregivers adjust to their new realities, they must additionally accept and reconcile changing interpersonal relationships.
The first year of a child’s life poses continual opportunities for parental adjustment, reflection, and growth. Such opportunities are consistent with the model of cognitive adaptation to stressful events proposed by Taylor (1983), which proposes that adaptation is informed both by a sense of intrinsic meaning-making and a perceived sense of mastery. As parents reassessed how and if their child would meet conventional milestones, they inadvertently asked themselves: “What does my life”—or their child’s life—“mean now?” (Taylor, 1983). For these parents, mastery was reflected in the peace made with their child’s different abilities. Additionally, triumphant feelings when a child reached a milestone instilled a sense of mastery in parents.
As parents came to terms with the idea of losing their child, they recognized the moments in which they could create meaning. A sense of mastery emerged as participants took steps to anticipate the impact of a future loss by utilizing and embracing resources like palliative care. Parents also discussed at length the ways in which they constructed a new reality for themselves during this period to seek a new normal. A review of qualitative studies in the rare disease context indicated that participants acknowledged new limitations and functional changes to daily life in more than half of studies reviewed (von der Lippe et al., 2017). This study extends and replicates this result as participants echoed the idea of creating a new normal in daily life given their child’s condition; it also illustrates how so-called “normalcy” can be conceived via varied mechanisms for parent-caregivers.
We acknowledge several limitations to this analysis. Caregiving roles are often shaped by societal norms and expectations, and mothers are often identified as primary caregivers for pediatric chronic diseases (Cardinali et al., 2019; Pelchat et al., 2003). The experiences of mothers versus fathers may differ based on societal and biological factors in the postpartum period (e.g., the demand of breastfeeding). The specific experiences of fathers in parent-caregiving is an area that demands targeted research. Finally, the interview was designed to retrospectively capture parent-caregivers’ appraisal of significant events in the child’s life. Life histories represent reflection on the past; therefore, they are imbued with an individual’s own meaning and framing (Järvinen, 2000) and may not accurately depict each facet of the recounted experiences. Even with this limitation, it is important to note that the structure of this particular life history interview—which asked parents to share five events in their caregiving journey that were most significant to them—inherently yields insight about what continues to resonate in these parent-caregivers’ lived experiences of their role. Given that this was a limitation imposed by analysis of secondary data, future research may employ methods that examine daily illness management during this critical period, including the use of participant observation, to enhance our understanding of caregivers’ day-to-day experience.
Conclusion
This study examines the experiences of parental caregivers during the postpartum period across a variety of rare genetic illnesses including inborn errors of metabolism, mitochondrial disorders, and undiagnosed disease. This work follows in a small, but necessarily growing, literature base on these unique caregiving contexts. The grounding in IPA is particularly well-suited to explore how these parental caregivers make sense of the postpartum period when facing medical complexity in that it allowed us to explore the meanings that these rare disease caregivers apply to this critical transition.
Supplemental Material
Supplemental Material - Becoming a Rare Disease Parent: An Interpretative Phenomenological Analysis of Parent-Caregivers’ Postpartum Experiences
Supplemental Material for Becoming a Rare Disease Parent: An Interpretative Phenomenological Analysis of Parent-Caregivers’ Postpartum Experiences by Hannah Rochelle, Davidson, Shani, Gelles, Krystyna R., Keller, Melissa, Zajdel, and Laura M., Koehly in Qualitative Health Research
Footnotes
Acknowledgements
The authors thank Drs. An Dang Do, Peter McGuire, Cynthia Tifft, and Charles Venditti for referring the participants in this study. Finally, the authors thank the participants and their families for their involvement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Intramural Research Program of the National Human Genome Research Institute (Grant ZIAHG200395).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.