
Abstract
In Ontario, Canada, rising rates of caregiver distress have been the ‘canary in the coal mine’ for a health system out of balance with the needs of an ageing population. Community-based health and social care professionals are well placed to play an important role in the caregiver support process; however, a gap has remained in the understanding of if and how caregiver support strategies are operationalized or experienced by community service providers (CSPs). The goal of this study was to describe how CSPs interpreted policy and how those interpretations may enable their work in supporting unpaid caregivers. Using a qualitative constructionist design, we interviewed 24 participants and reviewed 92 publicly available documents. Braun and Clarke’s method of thematic analysis was used for analysis strategy. Four overarching themes were identified: (1) community care as a priority, (2) sidewalk accountability, (3) creative care planning through partnerships, and (4) challenges to care delivery. We found that the importance of caregivers to the health system was reflected in organizational policy and strategy. There is an opportunity to improve health outcome for caregivers and the population alike through strong leadership and a clear shared vision. Our findings also suggested that social capital was a significant factor in enabling providers in their work, leveraging long-standing relationships, and accumulated local knowledge to implement highly creative care plans.
Keywords
Introduction
Current community-based health and social care systems are failing unpaid family and friend caregivers (hereafter referred to as caregivers) in Canada (National Institute on Ageing, 2018). Despite the increasing prevalence of chronic care needs among an ageing population (Steffler et al., 2021), public funding for community-based health care has not kept pace, resulting in resource rationing and growing waitlists for services (Donner et al., 2015; Home Care Ontario, 2018). In Ontario, the rising rate of caregiver distress (Health Quality Ontario, 2016) is the ‘canary in the coal mine’ for a system out of balance with today’s requirements (Peckham et al., 2018). With the demands for caregivers across Canada expected to double in the coming decade (Fast, 2015) and demands on caregivers in every province expected to increase by 40% by 2050 (MacDonald et al., 2019), it is imperative to better our understanding of how best to support caregivers, both indirectly and instrumentally, if we are to mitigate a crisis of care.
Indirectly, many health authorities and organizations have acknowledged the crucial role of caregivers through their strategic priorities, performance indicators, and targeted investments (Khayatzadeh-Mahani & Leslie, 2018). Supporting caregivers through meaningful engagement can increase participation in health systems (Bennett, 2020; Elliott et al., 2018; Health Quality Ontario, n.d.; Kuluski et al., 2019; White et al., 2018) and contribute to reduced distress (Reinhard et al., 2008). Policy tools have been shown to be part of an effective strategy to engage caregivers (Kuluski et al., 2019). Policymakers have begun to directly recognize the importance of unpaid caregivers through tax credits, workplace policies, and a seat at planning tables (Kuluski et al., 2019; Torjman, 2015).
Community health and social care professionals are well placed to also play an important role in supporting caregivers. In Ontario, this group of publicly funded professionals includes home care coordinators, community support service staff, illness-based community not-for-profit staff (e.g. Alzheimer’s Society and Parkinson Society), family health team nurses, and social workers. Together, these individuals will be referred to as community support providers (CSPs) throughout this paper. The value of a flexible, collaborative, and integrated team approach by CSPs is associated with meaningful engagement and effective care delivery (Goldhar et al., 2014; Kuluski et al., 2017; Larsen et al., 2017; Ploeg et al., 2019). The wider literature about community health and social care professionals (nurses, primary care providers, and home care workers) has primarily focused on capturing the perspectives of specific professional designations in their work with defined populations, including those managing complex social care needs (Kuluski et al., 2017), people with multiple chronic conditions (Elliott et al., 2018; Kuluski et al., 2012; Larsen et al., 2017; Ploeg et al., 2019), older adults living with frailty (Sadler et al., 2019), people with dementia (Lang et al., 2015; Sun et al., 2014), and support for people at the end of life (Reeves et al., 2020).
A gap has remained, however, regarding if and how caregiver support strategies are operationalized or experienced by CSPs. Increasing that understanding may lead to improved policy implementation and enhanced CSP practice approaches with caregivers. This paper is drawn from a broader qualitative case study that aimed to explore how the policies, practices, and geographic culture of a former health authority in Ontario, Canada, interconnected in a manner that mitigated caregivers’ distress. The goal of this study was to describe how CSPs interpreted policy and how those interpretations may enable their work in supporting unpaid caregivers.
Methods
This research is a work of qualitative inquiry. A constructionist case study was used to develop an optimized understanding of the participants’ experience of working with caregivers (Stake, 2003). Case study design is well suited to “how” and “why” questions and allows researchers to “explore or describe a phenomenon in context using a variety of data sources” (Baxter & Jack, 2008, p. 544). The focus is on detailed inquiry and experiential knowledge, informed by sociopolitical influence (Suryani, 2013). For that reason, it was important to look at the interconnection between multiple data sources and stakeholders to provide a comprehensive understanding of the caregivers in the SW LHIN (Crowe et al., 2011). The study was approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (file no. 6027381).
Context
Ontario, Canada, was divided into 14 regional health jurisdictions, known as Local Health Integration Networks (LHINs) from 2006 to 2021. The LHINs were responsible for the planning and delivery of health and social care services at the regional level, with accountability to the Ontario Ministry of Health and Long-Term Care (Bhasin & Williams, 2007). The former South West Local Health Integration Network (SW LHIN), a health authority in the southwest region of Ontario, reported the lowest rates of caregiver distress across the province for almost a decade (Health Quality Ontario, 2015, 2018). This observation was unexpected and worthy of exploration for two reasons. First, the regional jurisdiction included a predominance of rural communities and small population centres, and caregivers in such locations are known to face challenges related to the access, applicability, and availability of services (Crouch et al., 2017; Ehrlich et al., 2017; Keating et al., 2011). Second, the SW LHIN was an underperformer in many respects. The SW LHIN often ranked 13th or 14th out of 14 LHINs on metrics argued to be the most important to caregivers’ general well-being, specifically, same day/next day access to primary care, alternatives to emergency department care, timely access to community-based nursing, and personal support worker (PSW) wait times (South West LHIN, 2017). Clearly, something distinctive in this region appeared to have insulated caregivers from distress. It was important to consider how contextual conditions – that is, social, political, cultural, and economic factors of the region – may have influenced the low rates of caregiver distress in the former SW LHIN. These conditions informed the planning and delivery of health services and influenced the approaches of CSPs working with caregivers.
Recruitment
Participants were recruited for a one-time focus group via email distribution lists and posters through the network of LHIN-affiliated organizations responsible for delivering community-based care, specifically those responsible for the development and implementation of care plans, and the ongoing monitoring of clients and their caregivers in the community. We used posters, social media, and email distribution lists to connect with potential participants. Eligibility criteria were as follows: (1) employed by an LHIN-funded/affiliated organization, (2) worked with older adults and unpaid caregivers in one of the five sub-LHIN regions, (3) worked in a coordination or navigation position for at least 6 months, and (4) available to participate in a focus group or interview. For maximum variation of professional designations across multiple organizational types, a purposive sample was recruited from across the five sub-regions of the SW LHIN. All participants in the in-person focus group provided written consent. When interviews were moved to online during the pandemic, we took recorded verbal consent prior to enrolment in the study, in keeping with the advice of our research ethics board.
Data Collection
Multiple sources of data strengthened the trustworthiness of the findings (Stake, 2003). Three sources of data were used: document analysis, a focus group, and interviews. Focus groups and interviews allow researchers to explore in-depth insights into individuals’ experiences and perspectives. This gives a richness of data and a contextual understanding of the topic, particularly when used together with document analysis, as is common in case study design.
Document Analysis
A strategic document analysis was developed to identify specific priorities, initiatives, investments, and/or measures the SW LHIN had enacted that may have supported unpaid caregivers. There are several advantages of document analysis, including cost-effectiveness, efficiency, and the unobtrusive nature of the collection strategy (Bowen, 2009). As a method, it also offers a stable, non-reactive process (Hurworth, 2005) that can offer a unique perspective for a case study into the social, political, and economic dimensions of a situation (Olson, 2010). Documents are a tangible proxy of an entity’s values and therefore help the researcher uncover meaning.
Bowen (2009) and Merriam (2009) both recommend determining what types of documents are to be included in the study: public records, internal documents, personal documents, or physical artefacts. A decision was made based on availability, access, and timing to use only formal documents, that is, external facing and publicly available documentation and communication (McMillan & Schumacher, 2010). Documents were considered from the period of 2015–2020. This timeframe was consciously chosen to reflect the importance of the publication of Health Quality Ontario’s report on caregiver distress released in the spring of 2016 based on data from 2015.
To be considered eligible for the study, documents had to be available on the SW LHIN website. A sample of documents was drawn based on an “assessment of each document’s importance, relevance, and reliability for the project at hand …” (Miller & Alvarado, 2005, p. 352). These documents included a sample of annual reports, strategic and quality improvement plans, and board meeting minutes. Documents that made mention of older adults, caregivers, care partners, and community care delivery were deemed relevant. Excluded documents were webpages pertaining to French language services, Indigenous engagement, children- and youth-focused engagement and planning, expense reports, and capital planning. These were deemed out of scope for this specific research project.
Document Analysis Extraction Guide.
Focus Group and Interviews
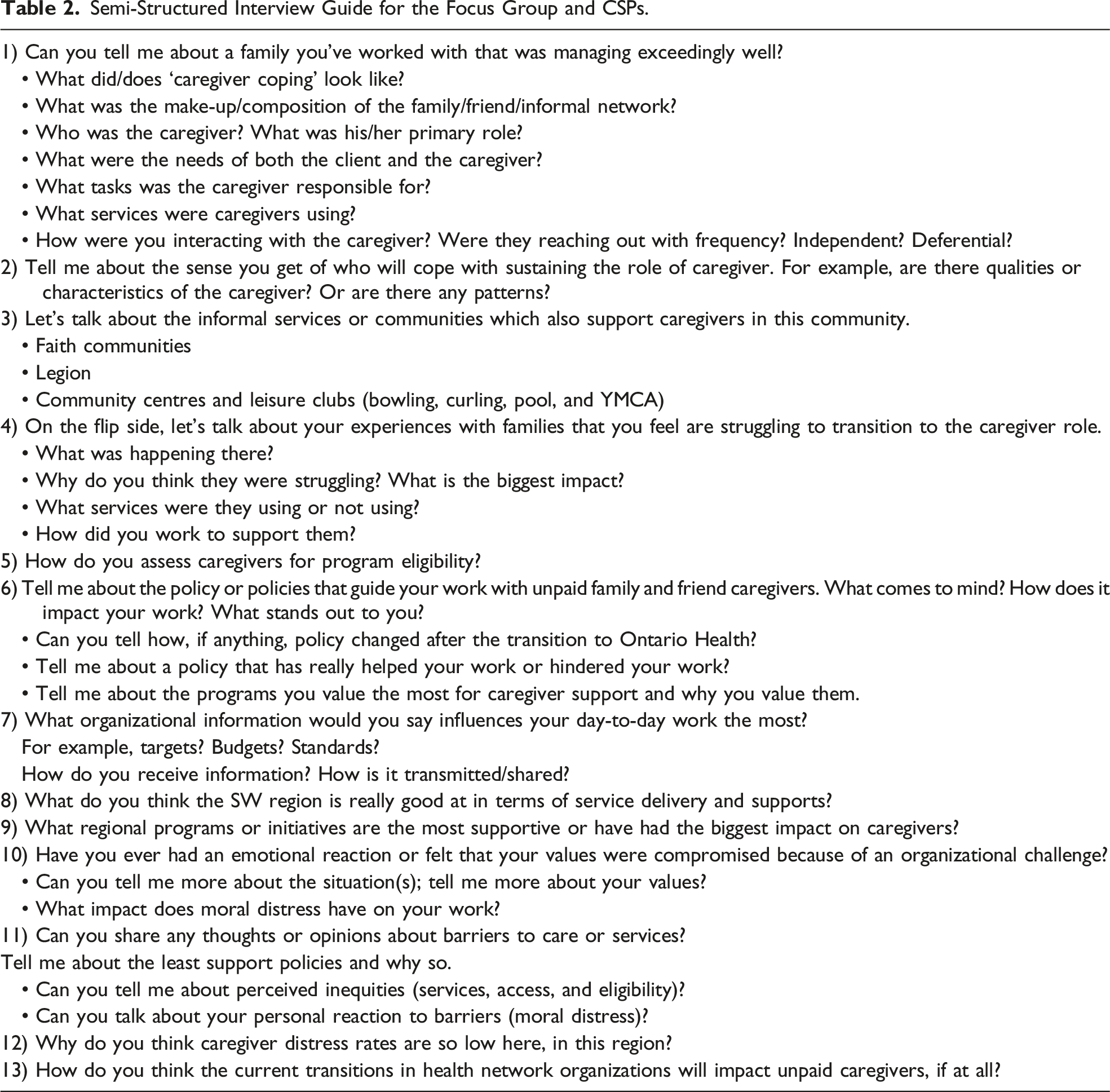
Semi-Structured Interview Guide for the Focus Group and CSPs.
Data Analysis
The Braun and Clarke (2006) approach to thematic analysis was used for data analysis in NVivo 12 Plus. This analytic strategy is consistent with both case study design and suggested for a document analysis that also uses interview data (Bowen, 2009). The single focus group and individual interviews were transcribed verbatim and anonymized with ID numbers maintained in a password-protected file generated by JW. Once transcribed, all audio-recordings were immediately deleted. A sample of transcripts and documents were read several times for familiarization by JW and MF independently. Following this, initial codes were generated, and early themes were constructed from pattern identification and mapping. The codes were refined and synthesized before assigning descriptions to the final themes. Direct quotes were included to support each theme. Documents were also imported into NVivo 12 Plus and analyzed in the same manner as the participants’ transcripts, though not anonymized.
Qualitative rigour was enhanced through several strategies. JW maintains a strong personal connection with many of the communities researched, both through family background and professional connections. As such, she was conscious of the need to resist assumptions and probe self-evident responses from interviews. The other members of the research team had no connection with the people or the places. Unconscious biases were challenged and discussed during the research team’s regular meetings.
Detailed field notes and the triangulation of multiple data sources and researchers also strengthened the credibility of the study. Data collection and analysis were iterative. A decision was made about data saturation based on information redundancy, sufficient, nuanced code descriptors with robust examples and pragmatism (Braun & Clarke, 2021). Member checks were used to enhance trustworthiness. All participants were sent a summary of the findings and invited to offer input. No changes were suggested by participants.
Findings
Participant Characteristics.
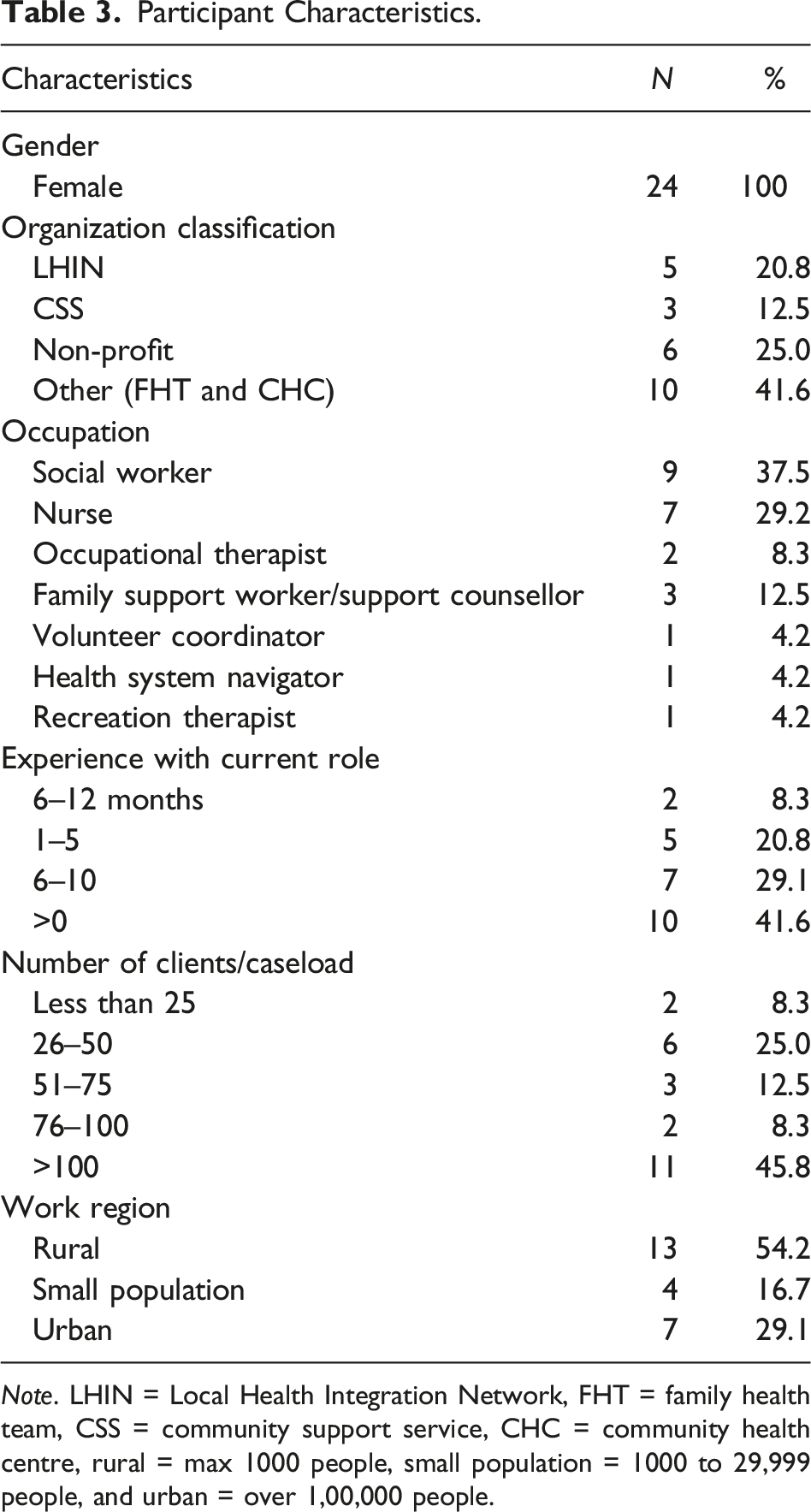
Note. LHIN = Local Health Integration Network, FHT = family health team, CSS = community support service, CHC = community health centre, rural = max 1000 people, small population = 1000 to 29,999 people, and urban = over 1,00,000 people.
Community Care as a Priority
The SW LHIN made it clear in their documents that community care was an integral part of their strategy. Of the seven priorities in the Integrated Health Service Plan 2016–2019, the document considered the blueprint for regional health care delivery, four were community based (SW LHIN, 2017). One goal included “Optimized health for people and caregivers living at home, in long-term care and in other community settings” (SW LHIN, 2016a, p. 4). Annual reports and board meeting minutes also reflected the SW LHIN’s commitment to all parties involved in the community sector. Financial investment was made to “enable the expansion of front-line nursing and personal support services provision for high-needs, complex clients and their caregivers …” (SW LHIN, 2017, p. 24); patient and caregiver stories were shared to connect policy with the people (SW LHIN Board, 2017). When discretionary investment was permitted, caregiver-related programs were strengthened or created, such as increases to adult day programs, respite services, and Behavioural Services Ontario expansion (SW LHIN, 2016b, 2017).
Participants rarely, if ever, named specific health policies that guided their practice with clients and caregivers. Instead, they discussed programs, tools, standardized assessments, and service guidelines. For CSPs, ample flexibility to shape and tailor care plans as needed was most important. Regarding policy, respondents acknowledged that the best policies were those adaptive and open to improvisation. A few participants appreciated what they interpreted as the supportive adoption of policy by the SW LHIN, which they thought enabled local solutions to local problems. SP09 was quick to praise the approach: “I don’t know if it’s across Ontario, but what I’m really impressed within our LHIN is the flexibility.” And SP10 echoed the sentiment: “We also really benefit from ... the flex fund. So that’s unique in our LHIN. It’s not all the LHINs.” The flexible attitude towards policy supported more individualized care plans and contributed to CSP satisfaction in their role.
Despite the well-intentioned priorities, numerous provincial health targets were missed, in many cases substantially (SW LHIN, 2020). Of particular relevance to caregivers were same day/next day access to primary care, alternatives to the emergency department, and timely access to in-home nursing and personal support workers.
Sidewalk Accountability: Social Capital in Community
Accountability was a pattern identified through the documents and the participant descriptions during the focus group and interviews. Social capital was represented exogenously through board meeting minutes; performance metrics and scorecards and annual reports reflected the social reality of the LHIN’s authority and responsibility. The very existence of the SW LHIN website and all of the documentation accessible on the site were the embodiment of accountability.
Sidewalk accountability reflected accumulated social capital among rural and urban participants alike. Social capital was established through actual and potential social networks, trust, and regional norms, helping to enable continuity of care for clients and caregivers. As CSP04 shared, “We have had some care coordinators that have been doing this for years, and they know their patients inside out and backwards ... because of that continuity, they have a good sense of the family and the caregivers.”
For CSP14, sidewalk accountability included a strong sense of responsibility to both colleagues and the community, and a willingness to act: “You want to play nice in the sandbox because you never know when you’re going to need someone or you’re going to need their resource or you going to need their network of people.” Participants typically reported lengthy employment tenure, combined with living in their community. The community-based health and social care organizations were staffed by a close-knit, experienced cohort of professionals. Employment mobility typically occurred within a limited set of employers, which enhanced relationships: “Staff that work here have previously worked for other organizations. So, information is easier to get” (CSP12).
Many of the participants, regardless of whether they were currently urban or rural, had grown up in or nearby the communities they served; this history was described as a blessing and curse by CSP20: “We’re all very connected and all know each other. It helps and hinders a little bit … but then sometimes they only want to talk to you because they know you. They have that relationship with you.”
A lack of professional anonymity, particularly outside of the urban centre, was described by participants who discussed frequently crossing paths with clients, caregivers, and colleagues on the sidewalk in their town. This quote comes from a participant from the focus group: I might run into CSP04 in the grocery store. There's more familiarity with the care partners that we’re working with and with our agencies. There is something to be said about that, and so it’s easier to pick up the phone and talk to CSP03, or talk to CSP04, or talk to whoever. (CSP07)
Creative Care Planning Through Partnerships
Creativity was central to the vision of the SW LHIN and was a stated value: “Innovation: We will be creative and embrace new ideas to respond to the changing needs of our communities” (SW LHIN, 2014). Patient stories presented to the board of directors often had a story of organizational collaboration, “working differently together” at the heart (SW LHIN Board, 2016, p. 33). For participants, supporting clients and caregivers meant drawing on a wide array of community resources, often leveraging knowledge and relationships beyond agency scope. As CSP03 shared, “I love to gather resources because I just never know when I’m going to come into something where I’ve got to pull on that reserve, resilience, creativity to MacGyver a care plan.”
The most effective care plan required CSPs to think outside the box and broaden the membership of the care team by including non-traditional resources from community groups, the library, and the Legion (the local branch of the Royal Canadian Legion, Canada’s largest veteran support and community service organization). Knowing who to ‘call’ for what and when was essential to effective support. This knowledge was gleaned from daily practice, relationships, and collective history. Religious organizations were also frequently acknowledged for their contribution to care plans in providing instrumental support such as meals, transportation, yard work, and emotional and spiritual support. As CSP04 said, “We’re getting really creative in the church groups and our friendly visitors; we were using them for respite hours, where we used to do PSW for respite. We don’t have them now.”
Partnerships across organizations, particularly in rural communities, were developed and maintained through shared workspace and shared clients and characterized by a high degree of trust among the larger, multi-organizational team. Consider the following example: We join in partnership with other agencies like Home Care, where we’re supposed to be very separate. Home Care does this, and we do this …. So, we might join and share a client with home care, which you’re really not supposed to do, because it makes sense. And it makes sense in these times because we have a PSW shortage in our area. (CSP10)
Another participant described efforts to better collaborate to maximize well-being for clients and caregivers alike: We’re really trying to work together and say, “Okay, you’re offering this on this day, we have it two weeks later.” They could be coming to both and utilizing. The adult day away [day away programs for older adults provide support care and socialization for older adults with chronic conditions and cognitive impairment] is adding staff on their days when we have programs, so that caregivers can come. So, we really are trying to be more aware of that. (CSP02)
A cooperative care approach was characterized by a commitment to person/family-centred care emphasizing care coordination and reducing duplication.
Challenges to Care Delivery
Participants described challenges that limited their ability to create fully integrated teams, develop meaningful care plans, and ultimately meet client and caregiver needs. Human resource availability was the most frequently cited challenge for rural and urban participants, with personal support workers and long-term care beds in very short supply, regardless of sub-LHIN. As a participant explained: I said [to a caregiver and his wife, the care recipient], “I could probably get you two hours a week for a PSW, but you’ll be on a wait list.” That’s all that our healthcare system can offer this person is two hours a week, and even that you’re on a wait list … She [the care recipient] is on the list for long-term care, but they tell them three to five years [to wait for a long-term care bed]. (CSP15)
The lack of shared client records inhibited effective communication and was regarded as a barrier to care. But in terms of what’s actually happening day-to-day, a care coordinator [from the LHIN Home and Community Care team] will not know that I’ve been involved six times that week, unless I call them. So, the sharing of documentation still remains very poor, in terms of the electronic health records and stuff like that. (CSP07)
Geography and the lack of transportation also impacted the ability to delivery services. Some more remote communities could not find PSWs willing to do the driving, especially in the winter. As CSP24 explained, “I find in some of the more rural areas where that’s a shortage … a lot of the PSWs would spend a lot of time traveling because people are living in more remote areas. And that impacts care.”
A final challenge discussed was specific to rural communities: inconstant access to high-speed Internet. CSP20 was one of several CSPs who expressed frustration: We have a lot of dead spots in Huron County in that and they’ve [the employers] definitely worked very hard through COVID [to get CSP staff connected remotely]. I know several of my … coworkers had to upgrade packages, attach dishes to trees and to do all sorts of things.
There was an acknowledgement by the SW LHIN Board Quality Committee of both the human resource shortage and quality of care issues (SW LHIN Board, 2018). However, the former health authority was chiefly focused on challenges pertaining to MOHLTC performance indicators such as hospital-acquired infections, readmissions, and surgery wait times (SW LHIN, 2016a).
Discussion
The intent of this paper was to describe key practice approaches and policy elements that enabled CSPs from the SW LHIN region to support caregivers. While existing literature has documented the perspectives of community-based health and social care providers working with clients/patients and caregivers with specific conditions and defined populations (Krutter et al., 2020; Kuluski et al., 2017; Larsen et al., 2017; Ploeg et al., 2019; Pope et al., 2019; Sims-Gould & Martin-Matthews, 2008), a gap has remained in the understanding of what enabled CSPs to effectively help caregivers and contribute to reducing caregiver distress.
Participants described flexible policy tools and practice approaches to support caregivers that were consistent with research from Kuluski et al. (2019) on principles of caregiver engagement. Recent publications have recognized the role of policy incentives and tools in any comprehensive caregiver support strategy (Khayatzadeh-Mahani & Leslie, 2018; Kuluski et al., 2019; National Institute on Ageing, 2018). The importance of older adults and community care to the regional health strategy of the SW LHIN was evident throughout the documents reviewed. The stated priorities were inclusive of caregivers and recognized their valuable contribution to the health system, though the CSP participants reported being largely detached from the regional vision and goals of regional planning. Well-aligned strategy with vision, mission, and organizational purpose has been found to be positively associated with organizational performance (Andrews & Beynon, 2011; Walter et al., 2013), and this work reinforces the literature base. Our findings suggest that the newly established Ontario Health Teams (OHTs) – smaller, more localized health authorities that have replaced the LHINs – have an opportunity to improve health outcomes for caregivers and the population alike through strong leadership and a clear shared vision (Kitch, 2017; Martin et al., 2014; Ontario Ministry of Health, 2019; Preston & Karahanna, 2009).
Social capital, especially as it extends to the concept of sidewalk accountability, was a significant factor in enabling CSPs in their work with colleagues and in the intuitive operationalization of caregiver support strategies. The impact of living in the community in which one served was a recurrent thread through the experiences of participants from rural communities and small population centres and was in keeping with previous work by Elliott et al. (2014). Their research found that community-based professionals’ relationships with patients and caregivers were strengthened through shared history and multigenerational connections. Social capital, the invisible currency amassed through social bridging, and the perceived trust networks of people who live and work together (Cloete, 2014; Keating et al., 2005) created a sense of belonging and willingness to act that was instrumental in CSPs’ ability to support caregivers. The role of social capital and the concept of sidewalk require further exploration, particularly the meaning of accountability to policymakers, in the provision and experience of delivering community-based health and social care.
The value and commitment to creativity and innovation was reflected throughout the SW LHIN’s public documents, from the vision, mission, and values statements to the Integrated Health Service Plan to the patient stories to the board of directors. For participants, the value of creativity was actualized in the development and implementation of resourceful care plans for clients and caregivers, built across multiple agencies, community groups, and churches. This finding extends work completed by Kuluski et al. (2017) that highlighted the need for community-based health and social care professionals to build ‘workarounds’ and ‘bend rules’ in care planning. These effective support plans depended on collaboration and cooperation of CSPs across agencies. In this case, creative care plans were in part successful because of the established trust and relationships, which are factors known to contribute to effective teams (Kirst et al., 2017; Larsen et al., 2017; Madden et al., 2020; Ohta et al., 2020; Ploeg et al., 2019; Rosen et al., 2018).
In reality, the reliance on workaround solutions, notwithstanding their positive impact, reveals a deeper issue within the community health and social care sector. The community-based sub-sector was largely removed from the Ontario Health Insurance Plan in the 1990s, leaving individual communities to develop and deliver programs and services for older adults and caregivers through a highly variable patchwork of organizations (Peckham et al., 2018). If these workarounds are dependent on accumulated knowledge and well-established relationships, the quality of care in the community in the future could be threatened by any significant staffing turnover, such as the predicted exodus of health care providers in the wake of the COVID-19 pandemic (Registered Nurses' Association of Ontario, 2021).
The challenges to care delivery we observed, namely the lack of shared client records, rural geography, poor access to high-speed Internet, and human resource shortages, reinforce previous research in other regions both in Ontario and beyond (Brown et al., 2018; Elliott et al., 2018; Forbes & Edge, 2009; Friedman et al., 2016; Sims-Gould & Martin-Matthews, 2008). However, our findings suggest that CSPs navigated and circumvented these barriers by leveraging community knowledge and their relationship network. Participants were not constrained by the boundaries of their own organizations, in part because of social leveraging.
Staff retention in rural communities has been a well-documented problem, particularly among the poorest paid, such as PSWs and in-home nurses (Hines et al., 2020; Jamieson et al., 2020). With an ageing population, it will be imperative to not only stabilize but to grow the paid community workforce if our care system is to bolster caregiver support. The newly established OHTs would be wise to consider innovative recruitment and retention policies. Preventing staff shortages may require fundamental structural changes to employment contracts, diverse service delivery models, including funding for family-managed care, and incentivizing the local population in education and training (Hines et al., 2020). Fostering population health through the redress of these challenges demands our society renew its commitment to ‘health in all policies’ (Kershaw, 2018; World Health Organization, 2014). This notion implies integrating the social and structural determinants of health into policymaking across sectors.
Limitations
This research was conducted within a defined geographic boundary, specifically exploring perspectives constructed working in that specific region. It would have been insightful to capture where participants lived, in addition to where they worked, so as to empirically demonstrate community connection. We were remiss not to include this on the background questionnaire. The sample size was relatively small, therefore limiting the transferability of the findings, though the interviews did provide rich data for this exploratory study. Furthermore, of the wide selection of documents reviewed in this study, some may have been incomplete or had insufficient detail to fully reflect the social reality.
Finally, the impact of COVID-19 must also be considered. The rapidly evolving circumstances and restrictions of the pandemic in Ontario in the spring/summer of 2020 meant that data collection could only be completed virtually. Community health and social care providers were working in erratic conditions and from known broadband-limited areas. The inadequacy of the Internet coverage and data limits of those working remotely may have limited our ability to recruit, suggesting some viewpoints were not captured. The findings about limited Internet availability may have been stronger if those viewpoints had been captured. Also, in keeping our interview guide the same from the pre-pandemic period, we may have failed to capture the impact of COVID-19 as we did not explicitly ask participants to describe similarities and differences in their experiences.
Conclusion
The community-based health and social care sector remains underfunded to meet the demands of an ageing population with increasingly complex chronic needs in Ontario. The impact of that underfunding has transferred greater responsibilities for care to unpaid caregivers and, as a result, contributed to the steady rise in caregiver distress rates. This study contributes to understanding the interconnection of factors that enabled CSPs to have effective practice approaches with caregivers. This research shows that the SW LHIN made community care a policy priority and leveraged the considerable legacy of social capital in a region largely composed of close-knit rural and small communities. Both factors contributed to reduced caregiver distress rates.
The continued out-migration from rural communities combined with pandemic-era human resource volatility threatens the provision of community care. The successes of the former SW LHIN may not be sustainable. If we are to enable caregivers in their role, Ontario can no longer rely on the precarious patchwork of community support services nor the current funding model.
Footnotes
Author Contributions
JW conceptualized the study and designed the methodology with substantial input from MF and KN. JW wrote the ethics application. Data were collected by JW, and initial coding was completed by JW and MF with contributions on theme generation and continuous input from KN. The manuscript was initially prepared by JW, with input from MF, KN, and TT. All authors provided feedback and editorial commentary on draft versions before approving the final submission for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Deidentified data that support the findings of this study are available on reasonable request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.