
Abstract
Background
Nurse care coordinators strive to build connections between different organizations to assist patients with complex needs in navigating the healthcare system. However, they often lack adequate support in their roles and encounter challenges related to the tasks themselves and to organizational and systemic factors.
Purpose
This study aims to evaluate a care coordination program in Quebec from the perspectives of both providers and beneficiaries.
Methods
We used a qualitative research design following an experience-based co-design approach.19 semi-structured interviews were held, ten with nurse care coordinators and nine with older adults and informal caregivers. An interview guide based on Valentijn et al. framework was used. Data were analysed using both deductive and inductive approaches.
Results
Factors influencing care coordination practice and the experience of older adults were identified. These include growing complexity of needs, patient-centered care, trusting relationships, interprofessional collaboration, communication tools, role clarity, shared values and objectives, the merger of health and social care institutions, and governmental guidelines and standards.
Conclusion
Many integrated care objectives are effectively implemented. Despite nurses’ efforts, older adults have expressed a need for more presence from care coordinators and better communication. This stems from the increasing complexity of patients’ needs and situations, as well as the nursing shortage. The study provides a systemic perspective on the challenges of a care coordination program at various levels. As such, it offers valuable insights for care providers, staff managers, and policymakers in integrated healthcare systems, enabling targeted improvements and offering guidance for broader application.
Keywords
Background and Purpose
With the rising prevalence of chronic conditions, an aging population, complexity of needs, and the consequent rise in healthcare expenses, it becomes imperative to enhance the delivery of health and social care. Care coordination has been recognized as an essential part of the strategy in achieving cost containment (Prokop, 2016), and an effective method for providing comprehensive, continuous, and person-centered care and services (McDonald et al., 2014). Research indicates that fragmented care and inconsistencies within the healthcare system undermine the quality of patient care, reduce patient satisfaction, and contribute to poorer health outcomes. (Chang et al., 2018; Ehrlich et al., 2009). Consequently, several developed countries, including Canada, have relied on nursing care coordination between health and social care services to effectively meet the needs of the population and improve their experience within the systems (Satylganova, 2016).
Care coordination involves the provision of multidisciplinary services, fostering enduring and collaborative relationships, and offering a range of healthcare interventions particularly for individuals with chronic conditions (Carney Moore et al., 2015) and multiple and complex health needs (Doessing & Burau, 2015). Coordinating care and services for these patient populations becomes significantly more difficult when they must transition between two different contexts, involving multiple professionals across various settings and sectors to ensure seamless patient transitions between services and locations (Hussain & Dornhorst, 2015; Olsen et al., 2020). However, despite the advantages of care coordination for both systems and patients, nurse care coordinators often lack adequate support in their roles and encounter challenges not only related to the tasks themselves but also due to organizational and systemic factors. Gaining a deeper understanding of the contextual difficulties faced by these nurse care coordinators would enable the development of tailored strategies rather than a “one size fits all” approach.
Moreover, over the past two decades a greater emphasis was put on the importance of considering patients’ perspectives in evaluating service quality (Peer & Mpinganjira, 2011). This initiative aims at fostering a trusting relationship, while enabling professionals to collaboratively uncover patient life circumstances, priorities and values, and develop a care plan with the patient (Staines et al., 2020). Patients’ feedback and opinions have been recognized as crucial in driving quality improvement efforts and providing valuable opportunities for organizational learning, in addition to providing an excellent patient-centered care (Carlucci et al., 2013; Kingsley & Patel, 2017).
At the same time, it's also crucial to highlight informal caregivers’ experiences within the systems. Caregivers tending to patients with complex needs typically assist with a range of tasks including household chores, mobility support, medication management, and arranging medical appointments (Schulz et al., 2020). In addition, they frequently serve as advocates and care coordinators, identifying and ensuring access to essential healthcare resources for the care recipient (Eden & Schulz, 2016). Hence the need to assess the experiences of informal caregivers, and incorporate their feedback to guarantee optimal healthcare quality and seamless coordination of care (Locatelli et al., 2015).
In the Quebec healthcare system, the organization, management, and delivery of health and social services to the local population are overseen by a single governing body called the Integrated Health and Social Services Center (IHSSC) 1 . This body is formed by merging neighboring health and social services centers with other public healthcare organizations, such as youth centers and rehabilitation centers (Wankah et al., 2018). Quebec, like many other countries, has made significant investments in care coordination. The IIHSSC of Laval has been actively implementing various services and care coordination functions for several years, particularly targeting patients with complex needs. These functions are dedicated to primary care level as well as hospital settings and include the roles of pivot nurses in home support and palliative care; liaison nurses in oncology, mental health, and physical health; case managers for complex patients in primary care and frequent users of healthcare services; “network” nurses who play a vital role in facilitating the transition of older patients from emergency departments; and more recently “nurse manager of an episode of care” who plays a proactive role in preparing the patient for discharge from the moment of admission. Whether in hospital or community settings, these nurses strive to build connections and bridges between different organizations to assist patients with complex needs in navigating the healthcare system (MHSS, 2021). While their titles may vary, several aspects of their roles remain consistent, including assessing patient needs, planning and coordinating care and services, facilitating access to services, supporting self-management, and ensuring effective communication and information transfer (Danish et al., 2020; Hudon et al., 2018; Loiselle et al., 2020).
However, despite these efforts, their experience with care coordination and the facilitating factors and obstacles to their role have never been identified. Gaining a deeper understanding of these aspects from the viewpoints of care coordinators and the patients who have benefited from this service, as well as their informal caregivers would streamline the identification of pathways for improvement and enhance decision-making processes. This study is carried out in partnership with the Nursing Care Directorate (NCD) of the IHSSC which has sought to establish a diagnosis of its current practices in a continuous quality improvement approach to care and services provided to individuals with complex needs.
The objective of this study is to evaluate the care coordination program by comparing the perspectives of providers and beneficiaries. The specific objectives are as follows: 1) analyze the barriers and facilitators to care coordination from the perspective of healthcare professionals; and 2) explore the experiences of patient with complex needs (and/or their informal caregivers) in terms of coordinating their services and care.
Methods and Procedures
Design
We conducted a qualitative study using an experience-based co-design approach. This approach aims to provide designers and researchers with access to user experiences, empowering them to design experiences rather than just services. It focuses on understanding how users perceive and experience the service, how effectively it meets their needs, and how well it fits within their context (Bate & Robert, 2006). Therefore, this approach relies on user narratives and storytelling, which are crucial for comprehensively grasping the strengths and weaknesses of existing services and determining considerations for future improvements (Shaw, 2005).
Theoretical Framework
As a conceptual framework, we used the Rainbow Model of Integrated Care (RMIC), which aims, through a systemic approach, to understand the multifactorial and complex nature of integrated care, with care coordination as its main component (Valentijn et al., 2013). This model proposes that integration should be sought across various levels within a system to enable the seamless, comprehensive, and coordinated provision of services to both individuals and populations. In addition, it illustrates the type of integration that must exist at the macro (system integration), meso (professional- and organizational integration to serve specific populations), and micro (clinical integration to ensure ongoing care) levels to improve the health and well-being of individuals and the population. Lastly, functional and normative integration ensure connectivity across all micro, meso, and macro levels of the system.
Setting and Participants
The study took place within various facilities of the IHSSS of Laval, where a nursing care coordination function (such as pivot, liaison, or case manager) was present, spanning different levels of care. Consequently, we included the primary care level, specifically home care services, one hospital, and one residence for older adults.
Participant recruitment was conducted through purposive sampling in order to identify nurse care coordinators with at least six months of experience in their roles, who could provide in-depth insights into their coordination practices. The nursing services department identified and contacted eligible nurse care coordinators and provided the research team with a list of those who expressed interest in participating. We then contacted these coordinators by email to explain the study and invite them to participate. They were provided with the consent form several days before the scheduled interview date, allowing them the opportunity to ask questions beforehand.
For patients, the IHSSS administrative system generated a list of patients who had had three or more visits to the emergency department and/or hospitalizations in the past 12 months, were aged 65 years and older, and experienced physical vulnerability, whether due to a chronic condition, functional impairment, or both. These selection criteria aligned with the definition of complex health and social care needs (Karam et al., 2021). This list was submitted to the care coordinators who participated in the individual interviews so they could identify the patients who had benefited from their services. An IHSSS secretary contacted patients and/or informal caregivers to obtain their permission to share their contact details with us. The research team contacted the patients and/or informal caregivers who agreed by phone and invited them to individual interviews following the same recruitment process used for the care coordinators.
Data Collection
Data collection from coordinators occurred between August and December 2022 through one-hour semi-structured interviews conducted online via Teams. An interview guide based on Valentijn et al.'s (2013) framework explored facilitating factors and barriers to care coordination. Between February and June 2024, one-hour individual interviews with patients and informal caregivers were conducted at their homes. These interviews, guided by the same conceptual framework, focused on participants’ narratives, experiences, and needs.
Data Analysis
The analysis was conducted iteratively alongside data collection, following a mixed thematic approach (Fereday & Muir-Cochrane, 2006). This approach combined deductive coding, guided by the dimensions of Valentijn et al.'s (2013) framework, with inductive coding to allow themes to emerge directly from the data. Coding was initially performed independently by two researchers (MK and MK) to ensure reliability, and subsequently completed by one researcher. All data were managed and analyzed using QDA Miner, a qualitative analysis software.
After analyzing and structuring the data and considering the time gap between the two phases of data collection, a crucial group meeting was held to validate the results. This meeting included the nurse care coordinators who participated in the interviews, a patient representative, and a caregiver representative. Participants were invited to validate the analysis of their contributions. They were then asked whether they wished to clarify, correct, or add any elements that may have changed since the interviews. The meeting was recorded and transcribed, and its content was used to refine the final results. The one-hour meeting, conducted online, was essential for ensuring the accuracy of the findings.
Results
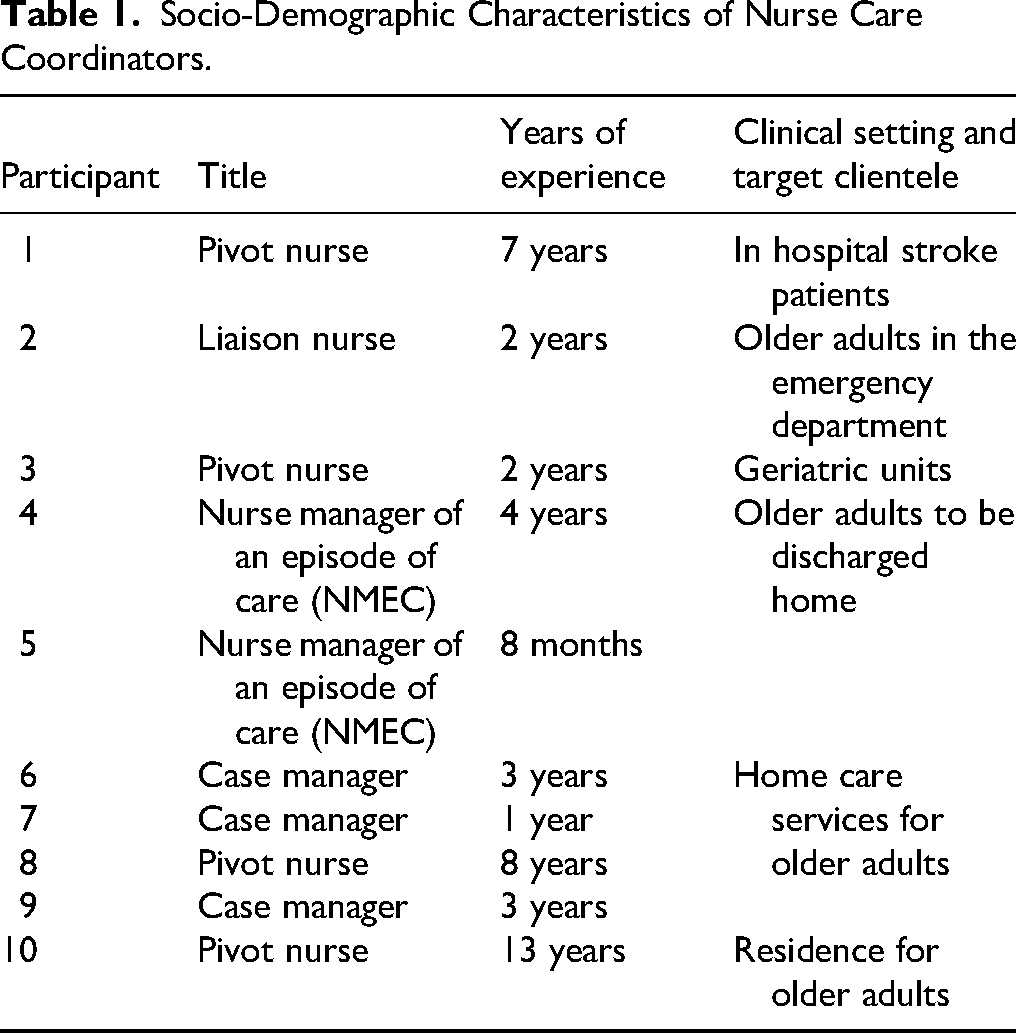
Nineteen individuals participated, including 10 nurse care coordinators and 9 patients or informal caregivers. The nurses had between 8 months and 13 years of experience and occupied various functions related to care coordination (see Table 1). The patients were aged between 65 and 86 years, all experienced physical vulnerabilities, and had visited the emergency department at least three times in the past year (see Table 2).
Socio-Demographic Characteristics of Nurse Care Coordinators.
Demographic and Health Data of Patients.
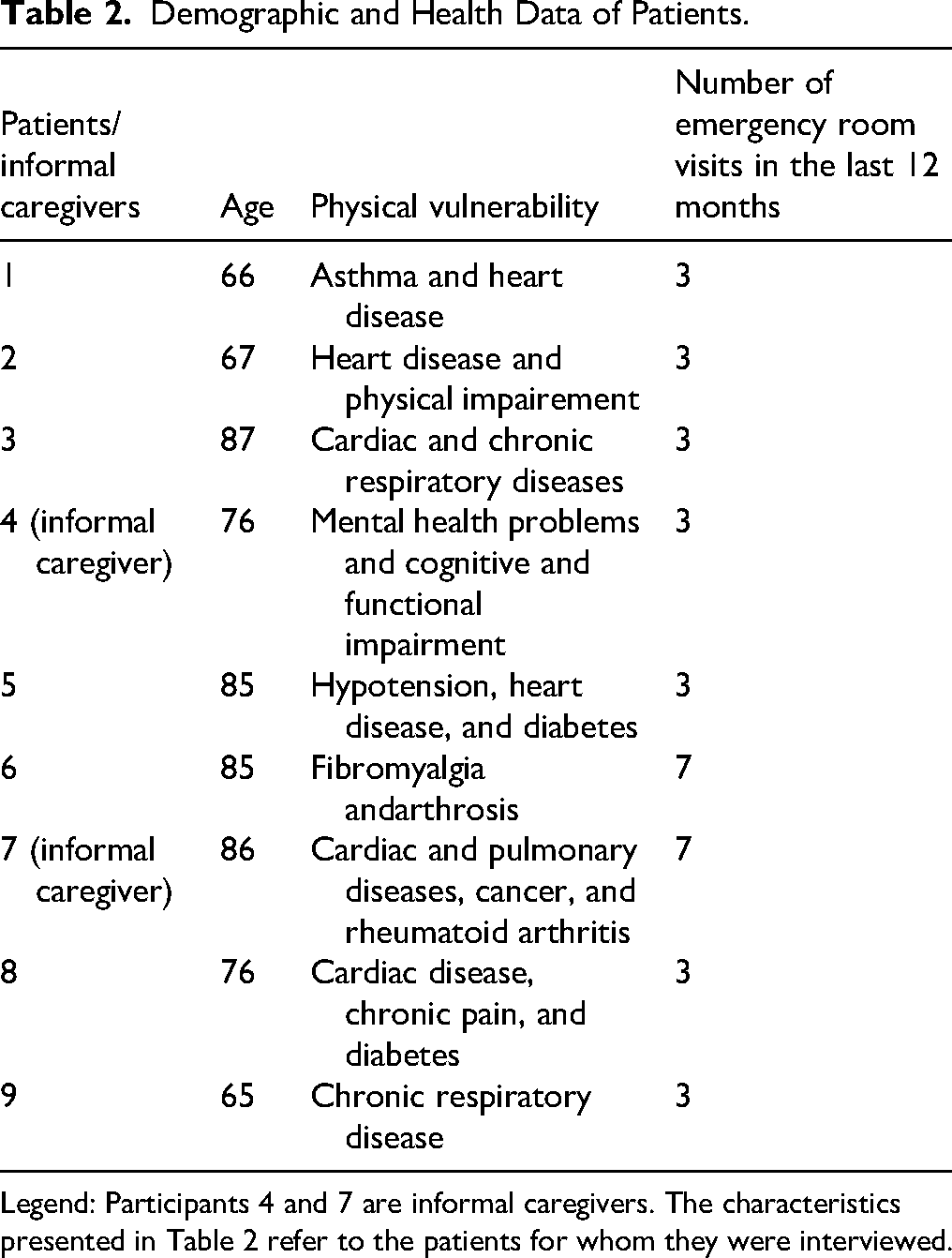
Legend: Participants 4 and 7 are informal caregivers. The characteristics presented in Table 2 refer to the patients for whom they were interviewed.
The findings of our study will be presented according to the levels of integration outlined in Valentijn's model (Valentijn et al., 2013). For each level, we will explore the intersecting perspectives of nurse care coordinators and patients.
Clinical Integration
The conceptualization of clinical integration is defined as the harmonization of patient-centered care within a unified process across time, space, and professional domains (Valentijn et al., 2013). Three main influencing factors were identified regarding clinical integration: complexity of needs and situations, patient-centered approach and trusting relationships, and patient empowerment.
Complexity of Needs and Situations
Nurse care coordinators shed light on the complexity of needs among the aging population, stemming from a combination of behavioral, cognitive, and physical vulnerabilities that required multifaceted interventions. Older patients often exhibited challenging behaviors and cognitive issues, such as wandering and aggression, which posed significant risks to their safety. “Now it's so complicated. They exhibit behavioral problems; I have cases of violence that I never had before. Problems that didn't exist, but we're moving towards another era, also with elderly people. The cases are so burdened, and they're also so complex.” (ECNM)
Also, patients often had multiple diagnoses that interacted in complex ways, requiring careful coordination of medications and treatments to avoid adverse effects and effectively manage their overall health. This complexity is compounded by inadequate support networks, hindering effective patient care management. Without family members or caregivers present, healthcare providers often assume multiple roles, from medical care to emotional support.
Patient- Centered Approach and Trusting Relationship
Nurse care coordinators discussed their patient-centered approach and how, along with maintaining a trusting relationship with patients and caregivers, it served as an essential facilitator in care coordination. They explained that they actively engage patients and families in their care, acknowledging their preferences and concerns, and actively seek solutions to address them. Participants also believed that this approach strengthens trust between healthcare providers, patients, and their families, making them feel empowered and valued, ultimately enhancing the care experience. “It's about trying to understand the concerns of both the families and the patients themselves, point by point, and finding an adapted solution to address their needs.” (Pivot nurse)
The patients’ perspective echoed that of the nurses. They emphasized the importance of continuity of their care providers and maintaining a consistent healthcare team they could trust. Specifically, they expressed frustration when dealing with frequent changes in care coordinators. “But it's true that what I don't like is that they often change the person who takes care of you. I have an excellent nurse now, but I know that in a year, I'll lose her.” (Patient 1)
Nurses also discussed the challenge of balancing a patient's desire for independence with concerns for their safety. Some patients refused assistance or support services, preferring to manage their affairs independently, despite having cognitive impairments or physical limitations. These situations could lead to internal conflicts because, despite being aware of potential risks, nurses must respect patients’ decisions regarding their care, even if it means accepting a higher risk of falls or other adverse outcomes: “Personally, sometimes that's what's really challenging for me. I really like to help. And when they refuse, it's necessary to respect their choice too…” (Pivot nurse)
Patient Empowerment
To address the challenges described earlier, nurse care coordinators emphasized the importance of empowering patients in healthcare. They highlighted several strategies aimed at enabling individuals to take control of their health and make informed decisions about their care. These strategies include obtaining consent and collaboratively establishing shared objectives with patients. Furthermore, nurses stressed the significance of providing clear explanations about the benefits and available options to assist patients in making informed decisions: “So, we try our best to explain to them and make them understand the benefits or advantages so that they can make the most just or informed decision.” (Case Manager)
Additionally, participants emphasized actively engaging patients in learning about their conditions and treatment, beginning from hospitalization through follow-up care and home care services. They underscored the importance of collaboration among healthcare professionals to ensure patients receive comprehensive information and support throughout their healthcare journey. “If there is a capacity for learning, it starts at the hospital and is continued by the nurse during the course of care.” (Case manager)
Despite these efforts, some patients felt that the care coordinators should spend more time with them to better understand their needs, and an informal caregiver highlighted a need for more information on how to navigate the healthcare system: “It's a world we’re not used to dealing with, so we don’t know much about it. We don’t know who to turn to, so we just go with what we think. I would have liked more support and more information; that was really, I think, the biggest gap.” (Informal caregiver 4).
Professional Integration
Professional integration refers to the collaborative effort among professionals from different disciplines to work together effectively. It involves combining their skills, roles, responsibilities, and accountability to deliver cohesive and seamless care or services to individuals or populations (Valentijn et al., 2013). The main factors influencing professional integration were interprofessional collaboration and communication, and role clarity.
Interprofessional Collaboration and Communication
Nurse care coordinators emphasized the importance of shared decision-making within and across care levels, particularly in early discharge planning to optimize patient care transitions. They actively participated in regular team meetings to foster interprofessional collaboration, ensuring comprehensive and coordinated care delivery. These practices demonstrated their commitment to effective interprofessional teamwork aimed at enhancing patient outcomes and healthcare quality. “We now hold team meetings three times a week. During these meetings we check if a certain patient already has services like home care, discuss their needs and resources to establish their care plans, and ensure coordinated care planning and resource allocation.” (ECNM).
Patients were aware of this communication and shared decision-making, even if they were not fully aware of the specific processes involved. They expressed reassurance knowing that the professionals involved in their care communicate with each other: “She [the pivot nurse] told me she was going to discuss my case with her colleagues to determine the best course of action.” (Patient 8)
In addition, it was discussed that home care nurses played a crucial role in early discharge planning by proactively communicating with the hospital team to inform them about the specific needs a patient would have upon discharge. This proactive approach helped streamline the discharge process, ensuring necessary arrangements were in place and reducing potential delays or complications post-discharge, thereby contributing to better continuity of care and patient outcomes. “I would inform the healthcare team that a specific patient would need these interventions upon discharge; it facilitates a smoother transition.” (Pivot nurse)
Overall, participants also emphasized that team members felt heard and valued when expressing their opinions during decision-making processes. This collaborative approach ensured that any uncertainties or concerns were promptly addressed with concrete actions, promoting a shared understanding and commitment to patient care outcomes. “Team members feel they have a voice and the opportunity to express their opinions. Concrete actions are taken if there are any doubts.”(Pivot nurse)
However, participants described varying levels of openness among healthcare professionals towards collaboration, with some preferring to work in silos, which directly impacts their engagement and proactivity in patient care processes. This underscores the need for proactive engagement to expedite patient care processes. “Some healthcare professionals are open to collaboration, embracing its potential benefits. However, others remain skeptical and reluctant to engage until they fully understand its advantages and potential impact.” (Nurse case manager)
Role Clarity
Several nurse care coordinators reported a challenge related to the clarity of their role scope for themselves, their colleagues, and sometimes their hierarchical superiors, as well as its distinction from other roles such as those of social workers. “We sometimes face challenges with role clarity and overlap. It's important for each of us to understand exactly what our roles as nurse coordinators entail to avoid duplicating efforts or missing critical aspects of patient care.” (Nurse case manager)
Informal caregivers were not always clear about the roles and responsibilities of coordinators, even though they know they are their point of contact. “I know that the liaison nurse is something different [from a regular nurse], but whether they are mandated to communicate with families, I don't know.” (Informal caregiver 7)
Participants suggested several strategies to improve clarity around roles and responsibilities. These include defining expectations and task distributions more clearly at the level of direct supervisors, especially when multiple professionals are involved in a case (e.g., social workers, ECNM); creating educational materials, such as explanatory videos, to help new staff and current team members better understand these roles; revising and regularly sharing updated job descriptions to ensure transparency and alignment; and organizing interprofessional meetings to discuss roles, responsibilities and collaborative practices.
Organizational and System Integration
Organizational integration involves inter-organizational relationships (e.g., contracting, strategic alliances, knowledge networks, mergers), including common governance mechanisms, to deliver comprehensive services to a defined population. System integration refers to the political, economic, and regulatory frameworks that provide a real continuum of care for individuals and populations (Valentijn et al., 2013). However, since health and social services organizations in Quebec are mainly public and have been merged following a government healthcare system reform, these two levels of integration are particularly interdependent in our context, as shown by the results below. Therefore, we will present them together. The main influencing factors were the organization within and across the IHSSS borders, the high pressure for early discharge, and the universal access to care.
The Organization Within and Across the IHSSS Borders (Territorialization of Care):
Participants believed that the merger of health and social care institutions by geographic area to serve the population of this specific territory has created some fluidity in the organization of services within the IHSSS but has isolated them from the outside world. They report not knowing whom to contact or how to coordinate care and services beyond their territory, in addition to the absence of a centralized provincial directory containing contact information for network partners and external services.
Additionally, the care coordinators denounced an inequity in access to services based on the patient's place of residence, as the availability and waiting times vary from one geographic area to another.
As for informal caregivers, they mentioned being unaware of the available care services in their geographic area and even less so in other areas, complicating the transition of the patient from their home to that of a caregiver or a residence when these options are outside the territory covered by the IHSSS.
Ministerial Standards for Early Discharge to Home and Directive to Avoid Relocating Patients from Hospitals
Nurse care coordinators are caught between two conflicting realities. On one hand, they face long waiting times to establish safe and adequate home support services, with few intermediate solutions available between home care and long-term care facilities. On the other hand, they are under significant pressure stemming from government guidelines that promote early discharge and discourage transfers from hospitals to long-term care.
This pressure is passed down from the health ministry to organizations, and ultimately to the coordinators themselves, who must navigate these constraints daily. As one liaison nurse expressed: “They want us to discharge the patient at all costs, but there's no in-between.” (Liaison nurse).
Universal Access to Healthcare
Participants emphasized the importance of universal access to healthcare services, ensuring that all individuals receive necessary services regardless of financial status. They noted instances where patients or families initially refused care but were persuaded upon learning that it was provided at no cost. This highlighted the critical role of care coordinators in educating and advocating for patients, ensuring equitable access to essential healthcare services. “Sometimes the family or the patient refuses care, but when we explain that it's free, they change their minds.” (Pivot nurse)
Functional Integration
Functional integration involves the organization of critical support functions and activities, including management and information systems, focused on the primary process of delivering services, ultimately contributing to the overall value of the healthcare system (Valentijn et al., 2013).
Accessible Nursing Notes and Shared Electronic Records Within the IHSSS
Participants reported that within IHSSS, nursing notes are shared through electronic health records (EHR) allowing all healthcare team members to access comprehensive patient information. This accessibility streamlined communication and facilitated transitions of care: “The fact that we had access to the same notes meant we could provide more consistent care. It allowed us to stay updated on each patient's status and ensured we were all on the same page when making decisions about their treatment.” (Nurse case manager)
When asked about their access to their EHR, patients and informal caregivers did not express this need. They wish to be informed about the progress of their health status or their case but do not feel the need to consult the records themselves.
Use of Fax and Paper Forms
Nurse care coordinators stated that despite advancements in EHR, IHSSS continued to rely on fax machines and paper forms for certain administrative tasks and communication with external stakeholders. This introduced delays and inefficiencies in transmitting critical information. Healthcare providers often found themselves navigating between electronic and paper systems, which complicated the process of updating patient records and exchanging information with external healthcare facilities. “Unfortunately, we often have to use both fax and paper forms, which can be cumbersome. This dual-system approach slows down communication and complicates the process.” (Liaison nurse)
Normative Integration
Normative integration establishes a unified perspective that links all tiers of an integrated system. It involves the creation and maintenance of a shared mission, vision, values, and culture among organizations, professional groups, and individuals (Valentijn et al., 2013). Shared values and objectives were a main factor in fostering care coordination.
Shared Values and Objectives
Shared values and objectives centered around ensuring seamless continuity of care and services during transitions. This commitment was underscored by the collective effort to avoid gaps or disruptions in patient care. Participants highlighted this collaborative approach, reflecting dedication to coordinating services effectively for timely and appropriate care delivery. They mentioned: “We strive to provide the right service at the right time, which demands a lot, but sharing the same values makes it easier.”(Nurse case manager)
Another shared objective among participants was to facilitate optimal patient outcomes by aligning services with patient needs and ensuring smooth transitions between care settings. “We have excellent collaboration, but we are each our own person. Nevertheless, the goal is always the same: the well-being of the patient.” (ECNM)
Discussion
Our results show that many objectives of integrated systems, such as patient-centered care, interprofessional collaboration, and continuity of care, are being successfully implemented. However, they also highlight a significant challenge: the isolation of providers from the broader healthcare environment outside their IHSSS. The territorialization of care, which has expanded in several countries worldwide, aims to facilitate access to services, sustain healthcare provision in local areas, and promote a more integrated health system that ensures greater health equity for local populations (Bourgueil et al., 2021). However, our findings suggest that this territorialization hampers effective care coordination across regions and contributes to a fragmented experience for both patients and informal caregivers. While this does not question the relevance of providing care and services close to the individual's living environment, for policy, it emphasizes the need to strengthen communication channels with the external healthcare environment and build stronger inter-organizational partnerships and mutual exchange of information (Wankah et al., 2022). Bridging these gaps seems crucial to ensuring cohesive care and enhancing the overall experience for patients and caregivers.
Reducing hospitalizations and length of stays, as well as shifting from hospital-based to community-based care, are also key objectives of integrated healthcare systems (Usher et al., 2021). Participants discussed the pressure these goals create as they strive to minimize the impact of this policy on patients while managing increasingly complex home care situations following early discharges. Home hospitalization programs are in their early stages in Quebec, and even with broader implementation, these initiatives are selective (Lorthios-Guilledroit A, 2021) and will not address the needs of patients with complex cognitive and psychosocial conditions. Furthermore, these programs will not entirely alleviate the pressure or reduce the workload of nurse care coordinators, as they require ongoing and enhanced coordination between primary and secondary care levels. To address these challenges, it is essential to strengthen proactive strategies for managing early discharges. This includes establishing standardized, interdisciplinary care pathways to promptly identify patients who would benefit from them and facilitating collaborative discharge planning. Equally important is providing support for care coordinators by increasing human resources and offering continuous training on managing complex home care situations.
Our results reveal several convergences in the perspectives of both nurse care coordinators and older adults, particularly regarding continuity of care. This aspect emerges as critical for patient satisfaction and outcomes, underscoring the preference for consistent care coordinator to foster trust and familiarity. This finding is supported by existing literature on nursing care coordination (Karam et al., 2021) and highlights the global impact of caregiver shortages and high turnover rates. At both the policy and clinical practice levels, it emphasizes the need for strategies that ensure stable caregiver-patient relationships and effective communication about care transitions (Ljungholm et al., 2022). With the increasing complexity of patient needs and care situations, as highlighted in our results, the impact of nursing turnover and shortages is likely to intensify. Indeed, older adults and informal caregivers have expressed a need for more presence from nurse care coordinators, despite coordinators confirming that they provide significant support and dedicate the necessary time to it. To address this, empowering older adults and informal caregivers to navigate the complex healthcare system should therefore be an interdisciplinary effort (Paterick et al., 2017). It is crucial to explore coordinated strategies where all caregivers are informed about available services and resources and can actively participate in education and support programs that enable patients and informal caregivers to effectively advocate for their health needs.
Finally, improving communication has emerged as a common need, though preferences vary among participants. Nurse care coordinators particularly stress the importance of strengthening interprofessional communication through better information sharing and digital tools, to facilitate seamless care transitions and more effective decision-making (Vos et al., 2020). In contrast, patients prioritize improved communication with nurse care coordinators and do not express a desire to access their own records. While granting access to health records is believed to promote transparency and patient autonomy (Stanhope & Matthews, 2019), this does not align with the needs of our participants, likely due to the characteristics of our target population.
Strengths and Limitations
The primary strength of this study is its dual perspective from both patients and care coordinators. This approach helps identify discrepancies between service provision and patient perception, thereby facilitating targeted improvements that might be overlooked when considering only a single perspective. Another significant contribution is its exploration of care coordination in the context of merged and integrated healthcare facilities. Findings from our study provide a multi-faceted understanding of the challenges and benefits associated with these healthcare models, providing valuable lessons for broader applications.
The study's sample size, particularly regarding informal caregivers, may be a limitation, but the results could serve as a basis for future research focused on their specific needs. Another limitation of this study is the time gap between the interviews conducted with professionals and patients. This gap was primarily due to logistical challenges and the intention to gain a more comprehensive understanding of the care coordination program over an extended period. Despite this gap, rigorous methodological approaches were employed to guarantee the validity and reliability of the findings, thus providing a solid and accurate evaluation of the program.
Conclusion
This study provides a multidimensional analysis of care coordination within a Quebec IHSSC, based on the perspectives of nurse care coordinators and patients with complex needs. While several integrated care principles—such as patient-centeredness, interprofessional collaboration, and continuity—are being implemented, the findings reveal persistent challenges related to territorial organization, role clarity, and access to intermediate care services. Importantly, the study draws attention to areas that remain underexplored, such as the limited visibility of coordination roles among patients and caregivers, and the tension between institutional expectations and the practical constraints faced by coordinators. These insights suggest the need to refine coordination strategies by fostering cross-sectoral collaboration, improving communication beyond organizational boundaries, and supporting care teams in adapting to increasingly complex care environments. Further research is needed to examine how these findings apply across different settings and to identify scalable solutions that enhance both provider capacity and patient experience within integrated care systems.
Footnotes
Acknowledgments
We thank the Nursing Care Directorate of the IHSSC of Laval for assistance with patient and care coordinator recruitment and for discussing the implications of these results with the research team.
Ethical Approval
Ethics committee approval was obtained from the Scientific and Research Ethics Committee of the IHSSS of Laval, approval number 2023-932.
Consent to Participate
Each participant received an invitation to participate, and verbal and written consent was obtained before beginning the interviews. Participants were made aware that they could withdraw their consent to participate at any time throughout the study.
Author Contributions
All authors made substantial contributions to this work. They contributed to the conception and design of the study, as well as to data collection and analysis. They were also involved in drafting the article and/or revising it critically. Finally, all authors approved this final version of the manuscript.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by Social Sciences and Humanities Research Council of Canada (grant number 892-2021-3020).
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The entire dataset is not available for secondary access due to the specifics of ethics approval related to participant anonymity and confidentiality. Some data supporting the findings of this study are available within the article.