
Abstract
Spinal fusion surgery is one of the most common major surgical procedures in youth. Adolescent idiopathic scoliosis (AIS) is the most frequent reason for corrective spinal fusion. AIS (∼25%–47% of cases) and spinal fusion surgeries are associated with pain, including the development of new onset chronic pain for up to 15% of youth. This research used photovoice approaches to explore the journeys of youth from before, during, and after spinal fusion surgery, to demonstrate their experiences both of and beyond pain. Twenty participants were recruited from a previous study conducted by the senior author’s lab. Participants captured photos/videos in their daily life (Phase 1); collected previously taken photos/videos from before/during/after their surgery (Phase 2); and participated in individual interviews to reflexively discuss the meaning behind photos/videos (Phase 3). Before interviews, a questionnaire was administered to assess pain characteristics. Nineteen girls/women with scoliosis and one boy/man with kyphosis (12–19 years old, M age = 16 years) participated; they identified as white (80%), other (15%), and Southeast Asian (5%). The researchers used a reflexive thematic analysis approach, which generated five themes: (1) body aesthetic versus machine; (2) expectations and anticipation of surgery/outcomes; (3) desire of normalcy and freedom; (4) navigating a hoped-for positive surgery experience; and (5) the journey sculpts identity formation and sense of self. Findings support youth advocacy, underscoring the need to validate youth concerns and inform healthcare professionals of the importance of individualized care. Youth perspectives highlighted opportunities for optimizing surgery/healthcare experiences and the psychosocial impacts of scoliosis on body image and appearance.
Introduction
Spinal fusion surgery is one of the most commonly performed major surgical procedures in youth (Perry et al., 2018), with adolescent idiopathic scoliosis (AIS) being the most frequently referred condition (Dubousset, 2020). AIS is an abnormal curvature of the spine that appears in late childhood or adolescence. Although etiology is unknown, it affects between 1% and 5% of youth (Konieczny et al., 2013), with pain co-occurring in 25%–47% of cases (before surgery) (Théroux et al., 2015). Spinal fusion surgery is associated with severe acute and chronic pain post-surgery with significant impairments in daily functioning (Rosenbloom & Katz, 2022; Seki et al., 2018; Sieberg et al., 2013; Wong et al., 2007). However, minimal research exists on the journeys of youth from before, during, and after their surgery to explore their experiences and memories of and beyond pain.
Research literature examines how youth memories develop, why and how their memories develop differently from one another, and the influence of their memories in the development of chronic post-surgical pain (Kehlet et al., 2006; Noel, Pavlova, et al., 2019; Noel et al., 2019; Rabbitts et al., 2017; Rosenbloom & Katz, 2022). Chronic post-surgical pain is defined as pain lasting more than 3 months post-surgery that is not otherwise associated with pre-existing problems or post-operative complications (Kehlet et al., 2006). Research suggests that youth who develop negatively biased pain memories (i.e., recall higher pain compared to their initial report) following surgery are at risk for developing chronic pain (Noel, Pavlova, et al., 2019; Noel et al., 2019). Youth who develop negatively biased recall of pain after major surgery have reported higher pain intensity at 6 and 12 months post-surgery (Noel et al., 2017; Noel et al., 2019). Negatively biased memories tend to develop among youth with higher levels of anxiety and a tendency to catastrophize about pain (Noel, Pavlova, et al., 2019; Noel, et al., 2019).
A systematic review revealed that pre-surgical pain, child anxiety, child pain coping efficacy, and parental pain catastrophizing were pre-surgical factors predictive of chronic post-surgical pain (Rabbitts et al., 2017). Among youth with scoliosis undergoing spinal fusion surgery, moderate–severe pain has been reported in 35% of participants pre-surgery, in 11% one year post-surgery, and in 15% two years post-surgery (Sieberg et al., 2013). Among different pain trajectory groups (i.e., “short-term pain group” and “high-pain group”), youth have reported differences in mental health and self-image (Sieberg et al., 2013), underscoring the need to consider pain, mental health, and self-image in this population. Research has predominantly relied on self-report measures or descriptive qualitative interviews captured at a single time point (Rabbitts, Aaron, et al., 2017; Rabbitts, Fisher, et al., 2017). Moreover, youth with scoliosis who have undergone spinal fusion surgery have rarely been involved as research partners, identifying a missed opportunity.
Photovoice is an innovative data collection method that enables participants to capture and represent their personal experiences through photos and narratives (Wang, 1999; Wang & Burris, 1997). The approach involves people with lived experience collecting photos in their daily lives and expanding upon them in follow-up interviews (Wang, 1999). This approach is typically used in underserved populations where such stories would otherwise remain unheard (Wang & Burris, 1997). Photovoice can encourage important dialogue to promote and amplify diverse patient voices and foster change in healthcare systems (Wang & Burris, 1997). Previous photovoice research has explored transgender individuals’ experience in emergency healthcare (Hussey, 2006) and hospital discharge planning for medically complex families (Barone et al., 2020). Photovoice has been a beneficial research approach for youth, as it can unlock conscious and unconscious feelings about challenging life events (Woodgate et al., 2014) and can have therapeutic benefits (Zurba et al., 2017). The aim of the current study was to apply a modified photovoice approach to (i) explore the lived experiences of youth from before, during, and after their spinal fusion surgery; (ii) identify salient aspects of their surgery journeys (including pain), and (iii) describe future directions for optimizing youth surgery and healthcare experiences.
Materials and Methods
Study Design
This qualitative study is embedded within a larger longitudinal, observational research project on the role of memory in the transition from acute to chronic post-surgical pain in youth. Youth in the overarching project completed questionnaires, daily diaries, memory interviews, MRI scans, and optional saliva sampling. This study included a new data collection timepoint to expand on the overarching project by using photovoice. Five participants of the current study participated in a memory-reframing study conducted within the senior author’s lab (Pavlova et al., 2022). The study delivered a memory-reframing intervention six weeks post-surgery and assessed pain outcomes comparing intervention and control groups (Pavlova et al., 2022). Three participants of this study participated in the intervention and two participated as controls (see Supplemental Table 1). The current study explores what is salient/important to youth in their journeys of and beyond their pain experience; their participation in the previous study is specified to consider how this may have diversified youth experiences.
The authors adopted a social constructivist approach (Schwandt, 1994), providing an ontological understanding of how we can unearth individual experiences, by seeking to understand youth experiences through their photos/videos. Traditional photovoice approaches require participants to take photos in their daily life and participate in follow-up focus groups (Wang & Burris, 1997). The current study required participants to actively take photos/videos in their daily life (Phase 1), collect previously taken photos/videos from before, during, or after their surgery (Phase 2), and participate in an individual follow-up interview to discuss their photos and videos (Phase 3). The modifications were used to reflect what is salient in youth memories and their current experiences. Further, individual qualitative interviews provided a more idiographic approach.
Eligibility and Recruitment
Participants
Participants who completed all time points of the overarching project and consented to be contacted for future/other research were contacted via email. The authors selected a subgroup (spinal fusion patients) from the larger study, due to the greater prevalence of these participants in the overarching study. Narrowing the sample enabled optimized recruitment and prioritized focus on the unique association this surgery can have on social/emotional outcomes (e.g., body image). Fifty-five youth were contacted to participate. The initial recruitment email stated that the research team had previously conducted a quantitative study they were involved in about their pain after surgery, while the current study focused on understanding the whole story of youth experience, beyond numerical pain scales. Twenty youth who underwent spinal fusion surgery participated in this study. The youth who did not participate included 20 youth who underwent other orthopedic surgeries and 15 youth who were uninterested or unable to participate in the time commitment.
Procedure
Study procedures were approved by the first author’s institutional research ethics board. Upon initial contact with potential participants, the first author met with each youth over Zoom to discuss the project. Potential participants <18 years old were asked to have a primary guardian attend the initial meeting. During the initial meeting, if a potential participant was eligible and interested in participating, the first author provided a photovoice training session. This consisted of describing each phase of the study and the premise of what to capture in photos/videos. The first author described how photos could include activities in daily life (i.e., eating, going to school, and seeing friends/family) and/or could include imagery/things that they like or are symbolic to them (i.e., nature and artwork). The first author explained how youth had the opportunity for creative freedom and may capture things beyond the suggestions. Following, an explanation of the data collection app Ethica was provided. The mobile app provided a secure platform for participants to upload photos and videos with a corresponding description of each photo/video. Participants were informed that if they chose not to use the app, they could provide photos/videos and short written descriptions to the first author’s institutional email. A minimum of three photos/videos for each phase (1 and 2) was required (minimum 6 photos in total). The minimum number of photos/videos was selected to support the qualitative interview, as photos were used to facilitate more in-depth conversation. The maximum number of photos/videos was not defined; however, participants were asked to speak to their most meaningful photos/videos in their interview, which aimed to last 1–2 hours. If potential participants declared willingness to participate, they were emailed consent forms to be completed and returned. Participants <18 years old were provided an assent form and consent form for their primary guardian to complete. A start date for data collection was determined before the end of the meeting.
Ethical Considerations of Photo/Video Use
The representation of photos in this manuscript was critical as it enabled youth to share their data collection contribution and bring their stories to life. A photo/video release form was encompassed within the consent/assent forms, which provided three options in terms of how the visual data could be used (see Supplemental Table 2). All youth whose photos have been displayed in this manuscript consented to option 1 (i.e., use of photos in manuscript publication in the way they were shared), with the assurance/agreement that specific photos that were of interest to use were confirmed with families prior to use. Following completion of all data collection and analyses, the first author emailed each participant (and primary guardian if youth <18 years old) the photos that were of interest for use and provided detailed information as to where the photos would be shared (i.e., specific research platforms and scholarly journals). The first author obtained email or verbal confirmation from all participants and/or their primary guardian (youth <18 years old) stating they agreed their photos could be presented in this article. To protect anonymity, all photos depicted in this article exclude any signs/landmarks that would suggest specific locations. Some of the photos displayed in this manuscript include participants’ faces. For those photos (i.e., Figures 1, 5, 10, and 11), youth were contacted via email and provided with exerts from the manuscript to demonstrate how the authors illustrated the photo alongside their quotations and interpretations. All youth endorsed the use of how the information and findings were presented. Feeling pretty and not mishappen.
Measures
A pain questionnaire was administered at the beginning of each individual interview. This questionnaire was the same as the one previously administered in the overarching study at baseline (day of surgery, or up to 14 days before surgery) and at 4 months post-surgery (Palermo et al., 2004). Youth reported presence of a chronic pain problem present for at least the last 3 months (Yes/No), the location of their body wherein they experience pain, pain frequency in the past 7 days (rated on a 5-point Likert scale ranging from “not at all” to “daily”), and average pain intensity in the past 7 days using a validated 11-point numeric rating scale (0 = “no pain” to 10 = “worst pain possible”) (Castarlenas et al., 2017; von Baeyer et al., 2009). Participants were asked to verbally respond to the questionnaire (see Appendix B) displayed via Zoom screen share. The questionnaire took ∼5–10 minutes to complete. The purpose of the questionnaire was to holistically tie together this study and the overarching study. This further illustrates how the quantitative information is further understood within the context of qualitative findings.
Interview Guide
Qualitative interviews were conducted via Zoom and lasted approximately 1.5 hours. The focus of the qualitative interview was to gain an in-depth understanding of the meaning of participants’ photos/videos. Photos/videos were used as a facilitation tool; however, through reflexive conversation with the participant, the interviewer pointed out aspects of the photos to question. For example, the interviewer may have asked, “I see there is a painting behind you in this photo, does it have any meaning to the situation.” Photos/videos were not analyzed by the research team outside of the interview. The interview guide was based on the “PHOTO” prompt (Hussey, 2006; Mamary et al., 2007): (i) “Describe your
Data Collection
Phase 1
Participants actively captured photos/videos in daily life that explained their current state in their major surgery journey. A short description of each photo/video was requested.
Phase 2
Participants collected previously taken photos from before, during, and/or after their surgery that were important to them within their surgery journey. Participants were not given a range in terms of how many years before surgery they could provide photos from. For example, an important part of their journey could stem from pre-diagnosis. Participants were asked to upload a short description of each photo/video.
Phase 3
Participants met with the first author over Zoom to discuss photos/videos. The first author suggested 5–7 days each for Phase 1 and Phase 2 (∼2 weeks in total). The follow-up interview was to be conducted between 2 and 4 weeks from the end of Phase 2. Additional time for data collection was acceptable as needed. The first author checked in with participants during their data collection process, using their preferred contact method (i.e., email or phone) and provided two data collection guides (see Appendix A). The Phase 1 guide was provided upon starting the study, and the Phase 2 guide was provided once the participant acknowledged completion of Phase 1.
Analysis
Data analyses involved an inductive reflexive thematic analysis approach grounded in the guidelines developed by Braun & Clarke (2019). The six suggested phases of analyses were followed: (1) familiarizing oneself with the data; (2) generating initial codes; (3) searching for themes; (4) developing and reviewing of themes; (5) defining and naming themes; and (6) producing the report. The first author conducted all interviews, listened/reviewed interview audio-recordings several times, and immersed herself in reading the transcribed interviews (Braun & Clarke, 2019). NVivo 12 software (NVivo, 2018) was used to generate initial codes and create themes. A reflexive thematic analysis aligns with photovoice approaches as it enables the research team to generate themes actively and organically in a collaborative manner (Braun & Clarke, 2014, 2019, 2021). The interview was reflexive as the participant and the interviewer together learned the deeper meaning of the participant’s experience (Wang, 1999). There is both analytic work and subjectivity that is inherent to the development of the themes (Braun & Clarke, 2019), resulting in a richer understanding of the data and youth stories. When initial analyses were conducted, the first author met with participants to ensure their voices were accurately presented. The first author and senior author met several times to build upon further reflexive meaning of themes. Through a reflexive thematic approach, participant stories were emphasized and deeply known, without requiring a concrete sole truth to be known. Photovoice can promote personal and community change, documenting the stories of a group, communicating life experience, expertise, and knowledge. This can ultimately impact system-level change for youth undergoing major surgery.
Reflexivity in Qualitative Research
The first author reviewed a subset of the initial codes with the second author to ensure credibility (Elliott et al., 1999). The second author is a person with lived experience who has undergone spinal fusion surgery and lives with chronic pain. The collaboration with the second author throughout data analyses enabled opportunities for the first author to make sense of their interpretations and become grounded in the data with reflection upon lived experience expertise. The co-author with lived experience helped to develop appropriate language for themes. She was compensated to reflect her contributions, time, and expertise according to current standards (Richards et al., 2018). She made integral contributions during all phases of the research. The GRIPP-2 reporting checklist was used to ensure appropriate patient and public engagement in research (Birnie et al., 2018; Manafò et al., 2018; Staniszewska et al., 2017).
The first author practiced reflexivity throughout all research phases by consistently making notes and reflecting on how her experiences changed her insights (Braun & Clarke, 2019). Rigor was incorporated throughout the study. The first author presented themes and interpretations to other team members, describing the process/approach to interpretation. The researchers kept an audit trail of their decisions, striving for a clear process, described herein, which could be repeated by future researchers (Shenton, 2004).
The first author’s experiences shaped how interpretations were developed and the research approach. The first author completed a Doctorate in Rehabilitation Science, which focused on the biopsychosocial approach to understanding disability, health, and overall functioning. She approached the concept/experiences of pain and healthcare holistically with components rooted in biology, psychology, and sociology. Members of the research team included a person with lived experience, pediatric/pain psychologists, social workers, and international academic psychology researchers. Team members brought their own insights and individual perspectives to this paper through diversity in experiences, culture, geographical location, sexual orientation, marital and parental status, gender, and education.
Findings
Nineteen girls/women with scoliosis and one boy/man with kyphosis participated in this study (12–19 years old, M age = 16 years old). Both diagnostic conditions involve a curvature of the spine, with kyphosis involving a forward rounding of the upper back. Participants’ races were reported as white (n = 16; 80%), other (n = 3, 15%), and Southeast Asian (n = 1, 5%). Other races included Afghan, Hindu, and Biracial Chinese. During the time of the study, 14/20 participants (70%) reported having a chronic pain problem that was present for at least 3 months and had been greater than a 0 on a 0–10 scale at some point in the last month. Of the fourteen participants who reported chronic pain, 11 reported chronic pain at baseline (in the overarching study on surgery day or up to 2 weeks before surgery), five reported chronic pain at 4 months post-surgery, and five reported chronic pain at baseline and 4 months post-surgery. Two participants did not report chronic pain at baseline or at 4 months post-surgery (in the overarching study) yet reported current chronic pain in this study. Only one participant did not report chronic pain at any of the time points. Demographic information, pain location, and chronic pain presence were collected (see Supplemental Table 1). Participants provided 192 photos and 24 videos.
Five themes were generated: (i) body aesthetic versus machine; (ii) expectations and anticipation of surgery and outcomes; (iii) desire of normalcy and freedom; (iv) navigating a hoped-for positive surgery experience; and (v) the journey sculpts identity formation and sense of self. Together, the themes described narratives about the lived experiences of youth, and each theme is described below with accompanying youth quotations. Some quotations were directly supported with a corresponding photo, and other quotations were brought forth detached from photos/videos when searching for deeper meaning of one’s experience. Pain was consistently mentioned and represented in all themes. Accordingly, at least one quotation within each theme reflected insights related to pain experiences. A prominent concept woven throughout narratives was “normalcy” and how youth constantly compared themselves to peers/society. However, the authors found it important for Theme 3 to stand alone, emphasizing normalcy, with further relation to freedom and loss of youthfulness.
Theme 1: Body as an Aesthetic Versus a Machine
This theme described how youth viewed and experienced their bodies. The theme title was chosen to emphasize how some youth focused on how they viewed their body appearance in daily life (aesthetic), while others focused on body function (viewing the body as a machine). The authors reflexively developed this theme together with their insights in clinical work and lived experience which impacted their interpretation of participant quotations. Some youth described how they saw their bodies as abnormal, mishappen, and ugly, and yearned to feel pretty and normal. Adina described the first time she felt pretty in a long time, while reflecting on the engrained idea of something being “wrong” with her body. Her perception of her body was influenced by what others in her social environment were telling her, yet the surgery did not “fix” her perceptions engrained from before surgery. Her quotation and associated photo are presented (see Figure 1). This was the day I got my grad dress back from alterations. I remember genuinely feeling pretty and confident with myself for the first time in a long time. It made me realize that my body wasn’t as misshapen or ugly as I thought it was … Before my surgery, just kind of always being told like, oh, this is out of place … and this doesn’t look right, it kind of lowered my self-confidence and even after my surgery, even though everything was technically fixed, there’s still that thought in the back of my head that something was wrong with me. But kind of feeling pretty again just made me realize that … even though doctors and everyone kind of said that there was so much wrong with me, deep down there kind of wasn’t. (Adina)
Conversely, youth described their body similarly to a machine that functions differently than others. They described the surgery as a powerful procedure that could fix them and restore function. Being fixed encompassed the ability to complete daily tasks/needs (e.g., walking and breathing). Lauren’s photo and description are provided below, illustrating the impact her curve had on daily/bodily functioning (Figure 2). Impact on organs.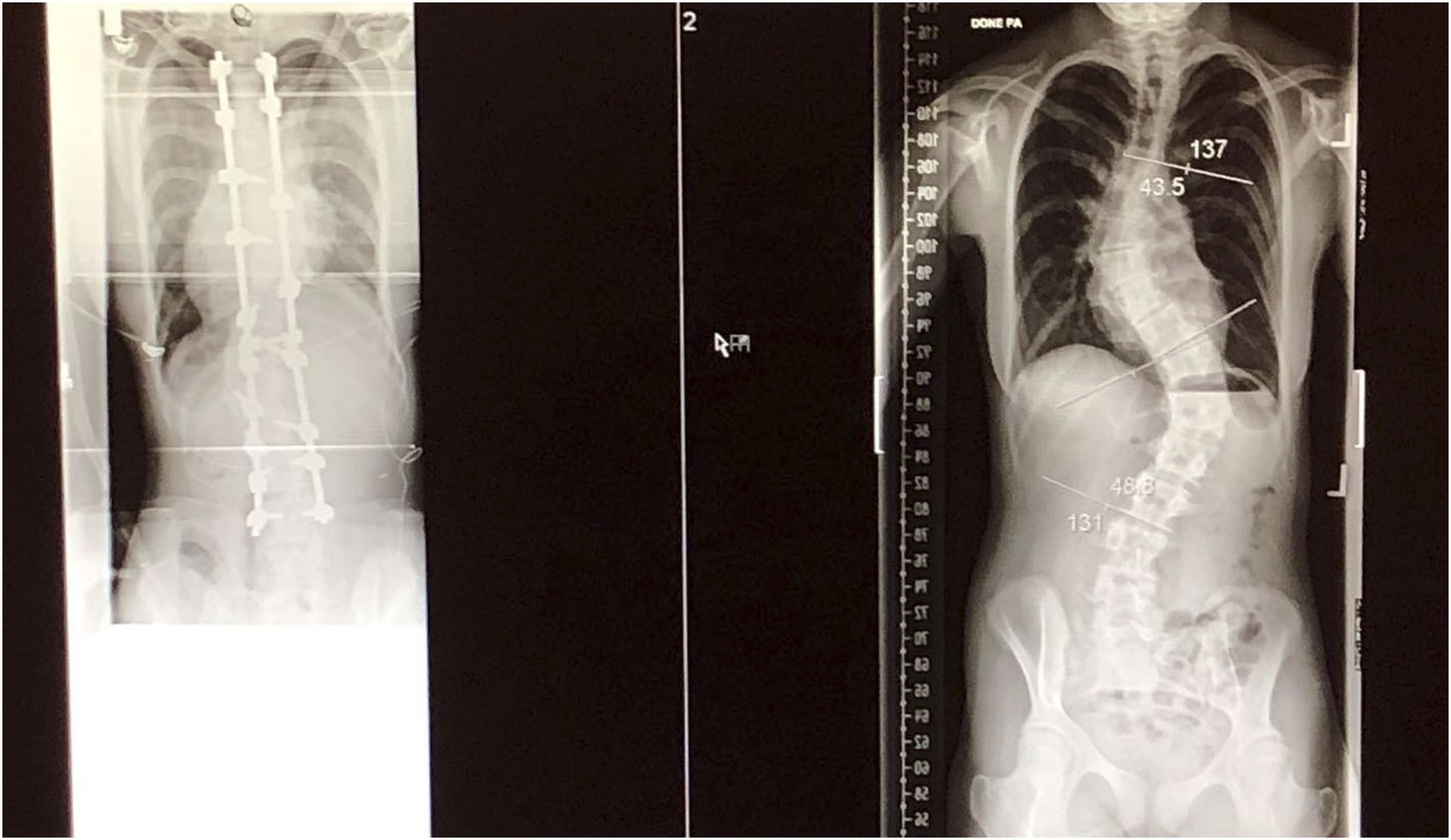
The importance that some youth placed on achieving a desired and normative physical appearance often outweighed their concern about possible negative outcomes after surgery (i.e., diminished functioning and pain). Youth would go to great lengths to attain normalcy. Jack described how despite good function, no pain, and “no real reason for surgery,” he “lied about” his pain to doctors to receive surgery. There was no pain associated with it [spinal curvature]. And like, my ability to be a human, to function, and to meet my basic needs was 100% ... I could walk, I could talk, I could read, I could write, right? And like, I could run … so, there was no need for the surgery from a surgical perspective, even though I lied about it, and I told the doctor that I was in pain because I wanted the surgery. (Jack)
Overall, this theme highlights the complexities of accepting one’s body and functioning, which evolves from before, during, and after the surgery. The surgery changes a one’s body and appearance, requiring youth to negotiate their body image relative to their peers, and their perceived and desired selves.
Theme 2: Expectations and Anticipation of Surgery and Outcomes
Each youth had a unique surgery journey that is marked by expectations and anticipations about their surgery, recovery, and long-term outcomes. Youth wanted their individuality and uniqueness to be recognized. It could be challenging for youth to notice their own progress and not compare themselves to others’ experiences and expectations. Social comparisons were generated from interactions with peers and the broader images/narratives about scoliosis in society.
Variable timelines from diagnosis to surgery impacted the anticipation of post-surgery outcomes. The gravity of processing a diagnosis and the surgery journey was immense for youth. Mental processing of one’s surgery journey was not always in sync with the pace of their physical progress. Adina, who had minimal problems pre-surgery and experienced pain and mental health concerns post-surgery, described how the rapid changes that permeated all realms of her life impacted her. When her healthcare team changed the timing of her surgery, this caused stress and left her grieving the time she could have had to “savor regular life.” Her use of the word “regular” pointed to the tendency of youth to anchor their pre-and post-surgery experiences in what they deemed to be normative in society. Upon reflection, not only did her spine and appearance change, “everything” changed. I guess just like how quickly everything changed, 'cause my first Doctors appointment was in November and then having the surgery scheduled for March and like originally it was supposed to be April and it got brought back to March. So that was kind of stressful, just how much the date had shifted and I thought I had more time to just savor regular life before everything changed. (Adina)
During the hospital recovery phase, standard protocols and timelines set by healthcare teams did not always align with individual needs; for some, it caused distress. Some youth described experiencing severe nausea and illness from the standard medication protocols, and others nearly fainted from being required by their healthcare team to walk immediately after their surgery when youth knew they weren’t ready. The quotation provided below describes Noelani’s belief in the critical need for healthcare providers to individually tailor care to the patients’ needs. Some people just need to be more understanding that this is a major surgery and that not everybody will be the same in their recovery process. And that just because you feel like they should be fine doesn’t mean they’re fine. (Noelani)
Uncertainty was inherent in all journeys and could cause distress, particularly early in the recovery journey. Youth were uncertain about their futures and their pain. In the present, Elena recognized that she would recover and be “fine,” but in retrospect, she recalled being in severe pain and not believing that it could get better. While she conveyed in the present that recovery and resolution of pain is “obvious” she underscored how this is not the case for many youth in the early stages of recovery. Like obviously I was gonna be fine … but like … the doctor would come and be like, oh, what’s your pain out of 10, I’d literally say 10. I was like, how is this gonna like, get better? (Elena)
It was important for youth to be able to reframe their expectations and grow over the course of their individual recovery journeys. Vera described her passion and investment in professional ski-racing (see Figure 3) before surgery but was able to let go of her expectations and create new goals that aligned with her own reality after surgery. Vera described how she adjusted her goal from becoming a professional athlete to being a coach and accepted her limits. She found her true yet unexpected passion that she never believed could be possible before her surgery and recovery. My end goal here was for sure to try to make team Canada for skiing, and I feel like, now, [that] completely changed like I would have loved to do that, but I, I feel like it’s important to also adapt to the change and like find other things that you love. I never thought I’d love coaching … I love it, like I never want to do something more. So I feel like that’s also important, that you can find new things in your journey that you never thought you’d like. And kind of like, give you different things to look forward to. (Vera) Pre-surgery skiing.
Theme 2 provides an understanding of how personal recovery journeys are unique yet are positioned against expectations that they and society have for them. This mismatch can lead to a relentless chase for “normalcy.” Uncertainty about their future and pain, particularly early in the post-surgical recovery journey, is common and resistant to change. Youth recalled pivotal moments at which they reached acceptance of their bodies and limits and realized new goals for their futures.
Theme 3: Desire of Normalcy and Freedom
Spinal fusion surgery is typically undergone during adolescence, a developmental period marked by substantial and rapid physical, emotional, and social changes (Christie & Viner, 2005). This theme underscores how undergoing a major surgery can accelerate development and maturity. Jennifer described an early childhood memory, when she was unaware that she had scoliosis. Jennifer described this stage as being “blissful” precisely because she was unaware of what would transpire. She is pictured wearing a swimsuit, smiling, and walking along a beach (see Figure 4), a contrast to the concealment that youth seek to hide their physical appearance and curve. This contrast is reinforced by Jennifer noting that this “ignorance is bliss stage” was precisely “before the back brace came into it.” This implied a loss of innocence that directly came from her experience of scoliosis/surgery and a yearning for that time. As a kid you don’t really know … like sure you’re like, “Oh I have scoliosis,” but it doesn’t really change, um, really who you are and what you do until you kind of like really understand it … And so I guess it was kind of that like ignorance is bliss stage before I really was like, oh, this is what it actually means. And then things, you know, like the back brace came into it. (Jennifer) Ignorance is bliss.
Jennifer learned of her diagnosis at ∼6 years old and quickly had to face the worry and restriction of her journey. Like Jennifer, some youth used back braces prior to surgery. Braces can be prescribed to be worn for up to 23 hours a day. Lauren described how her brace was part of her life from as early as she can remember (worn from 5–16 years old). The photo provides imagery where one can visualize the young woman growing alongside her braces, following her journey. She now sits beside her braces moving past this 11-year relationship with her ever-changing braces (see Figure 5). Back brace journey.
Narratives revealed insights about the desire for freedom and youthfulness. Youth shared wanting to be normal teenagers and to embrace their autonomy, the latter of which is a key developmental task for adolescence (Spear & Kulbok, 2004). During recovery, many youth expressed experiencing frustration with their lack of independence. Youth described requiring parental support to complete daily tasks such as eating independently. The deep need to be a “normal” teenager was consistent across all narratives. This stemmed from youth perceiving they were robbed of normal and desired aspects of childhood and their inability to function like their peers. Many youth struggled with returning to school post-surgery and fitting in with peers. Figure 6 demonstrates the numerous books necessary to carry throughout a day in high school, which exceeds the 2-kilogram maximum recommended post-surgery. Two quotations provided below demonstrate two different choices regarding implementing a doctor’s post-surgery recommendation. First, Lauren quotation described adhering to her doctor’s recommendation and experiencing embarrassment at school. In contrast, the second quotation described Harlow’s approach of choosing non-adherence and experiencing “constant” pain, to blend in. I still couldn’t carry more than two kilograms, so I ended up taking my gaming bag with my lunch kit and everything, and since I couldn’t carry it, I held the handle and I rolled it back and forth to classes, and that itself, I did not like that, because I kind of felt a bit embarrassed, because other people weren’t doing this, and I felt like “I’m the only one doing this.” (Lauren) I was carrying a really heavy backpack and that definitely affected it [my back] too. I was always in pain because of that. (Harlow) “Weight” of school.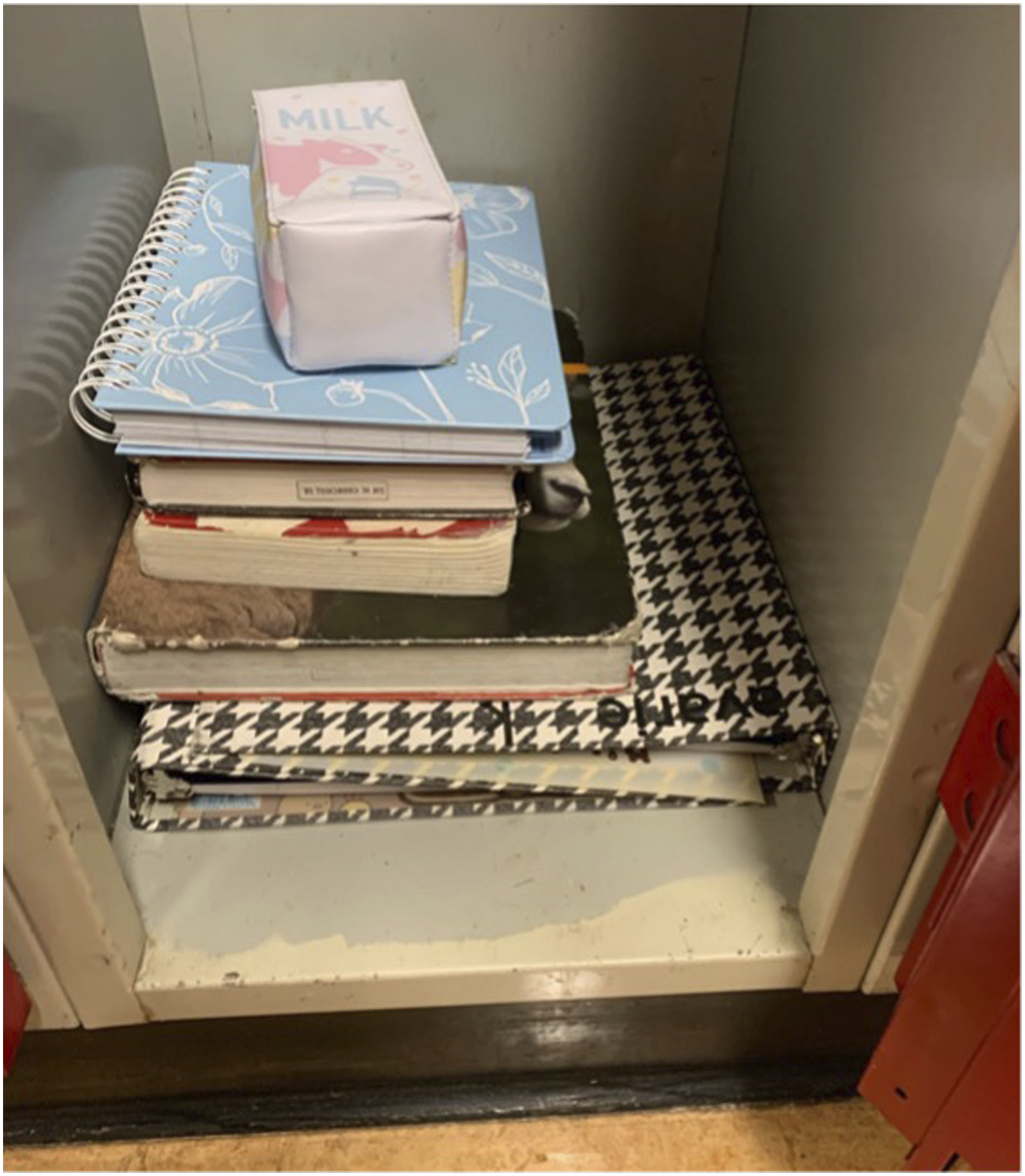
The quotations above demonstrate the choices youth must make, which their peers do not. It also reflects differences in the ways youth exert agency. Youth recognized how these choices had a direct impact on their pain/recovery, and their choices impacted and were impacted by their social and school functioning.
Theme 3 demonstrates a dialectic between accelerated and stunted growth for youth following surgery and a yearning for, and loss of, normalcy, independence, and youthfulness. Youth diverged in their adherence to healthcare recommendations due to a deep desire for normalcy; all choices had either social, physical, or emotional consequences.
Theme 4: Navigating a Hoped-For Positive Surgery Experience
This theme addresses aspects of the surgery and recovery journey that youth believed promote a positive experience. Primary facilitators that helped youth navigate through a more positive journey included animals/pets, hobbies/sports, social support, and meaningful mementos or rituals.
For many youth, a connection to pets was critical before surgery and during recovery. Youth described how physical touch between them and their pets was comforting. This provided social contact and functioned as a coping strategy to manage stress and pain. Danielle’s photo (see Figure 7) and quotation are provided below. Animal support.
“Obviously I was in pain, so when I got home he [cat] was laying with me a lot in my bed, so it kind of helped soothe me” (Danielle). Pets motivated youth to engage in physical activity, which was critical for optimizing their recovery. Nature also helped youth distract themselves from worrying and facilitated mindfulness.
During recovery, youth shared that they continued to engage in certain hobbies or acquired new hobbies that were accessible and could help pass the time. Youth who participated in active interests/sports before surgery struggled with the slow pace of progressing back into activity. However, many youth pivoted and acquired art-based hobbies, which could foster freedom when they were confined to their bed. Figure 8 depicts artwork created by Adina. Art as freedom and expression.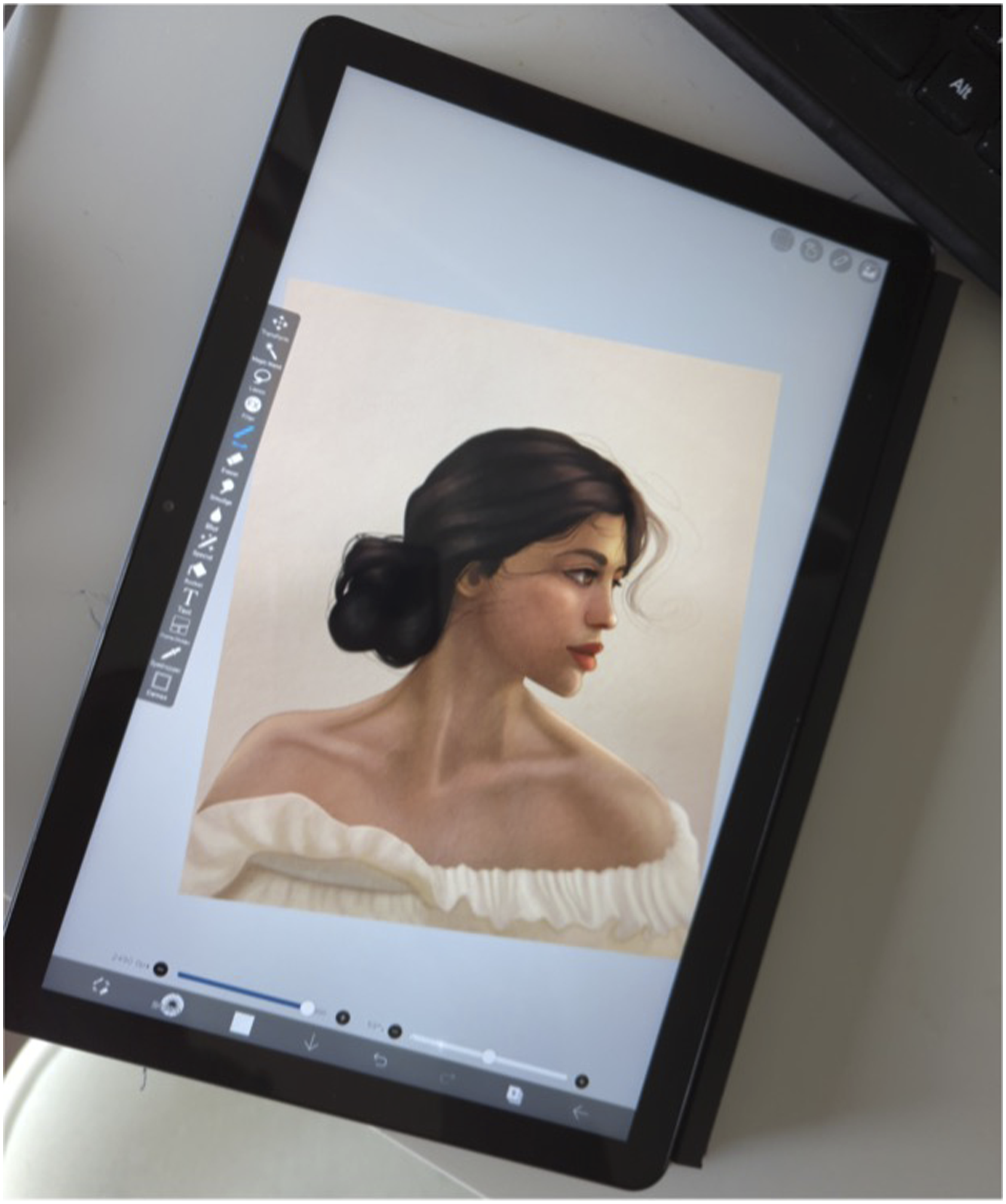
Social support was monumental in optimizing recovery. Many youth described their mother as being their primary support person. During recovery in the hospital, video calls helped youth to maintain connection with family and friends. Youth derived great benefit from having at least one reliable friend supporting them during their journey. Reliable friends were understanding/validating and provided company during challenges.
Aisling expressed the importance of knowing other youth who had also undergone spinal fusion surgery, for sources of community, empathy, and tangible advice. The #scoliosiswarrior social media community was described, wherein youth share their scoliosis journeys, providing solidarity and support. When I got my surgery date, I actually started the account [personal scoliosis account] and I was posting photos and stuff all the time to, I don’t know, share my story. Everyone that I became pretty good friends with like, we all were called the scoliosis warriors and like it’s a huge hashtag on Instagram, … it was a really awesome community because there was always someone that could understand what you were going through or they might have an answer to what you were going through. (Aisling)
Friends and family members provided small gestures or mementos that were meaningful to youth during their journeys. This was especially evident early in the recovery process when youth were in the hospital. These meaningful mementos or rituals were important for youth to focus on as sources of comfort and tangible reminders of their support networks. Some youth described new pyjamas and special stuffed animals they received; others described dying their hair blue for the surgery to mark the occasion as special. These mementos/rituals defined sources of strength and were cherished by youth throughout their recovery and to present day. Mae shared a photo (Figure 9) of a stuffed animal she was gifted at the outset of her surgery journey, and it has matching stitches along its spine. She described using the toy as a source of comfort/coping, especially on difficult days. Stitch the stuffed animal.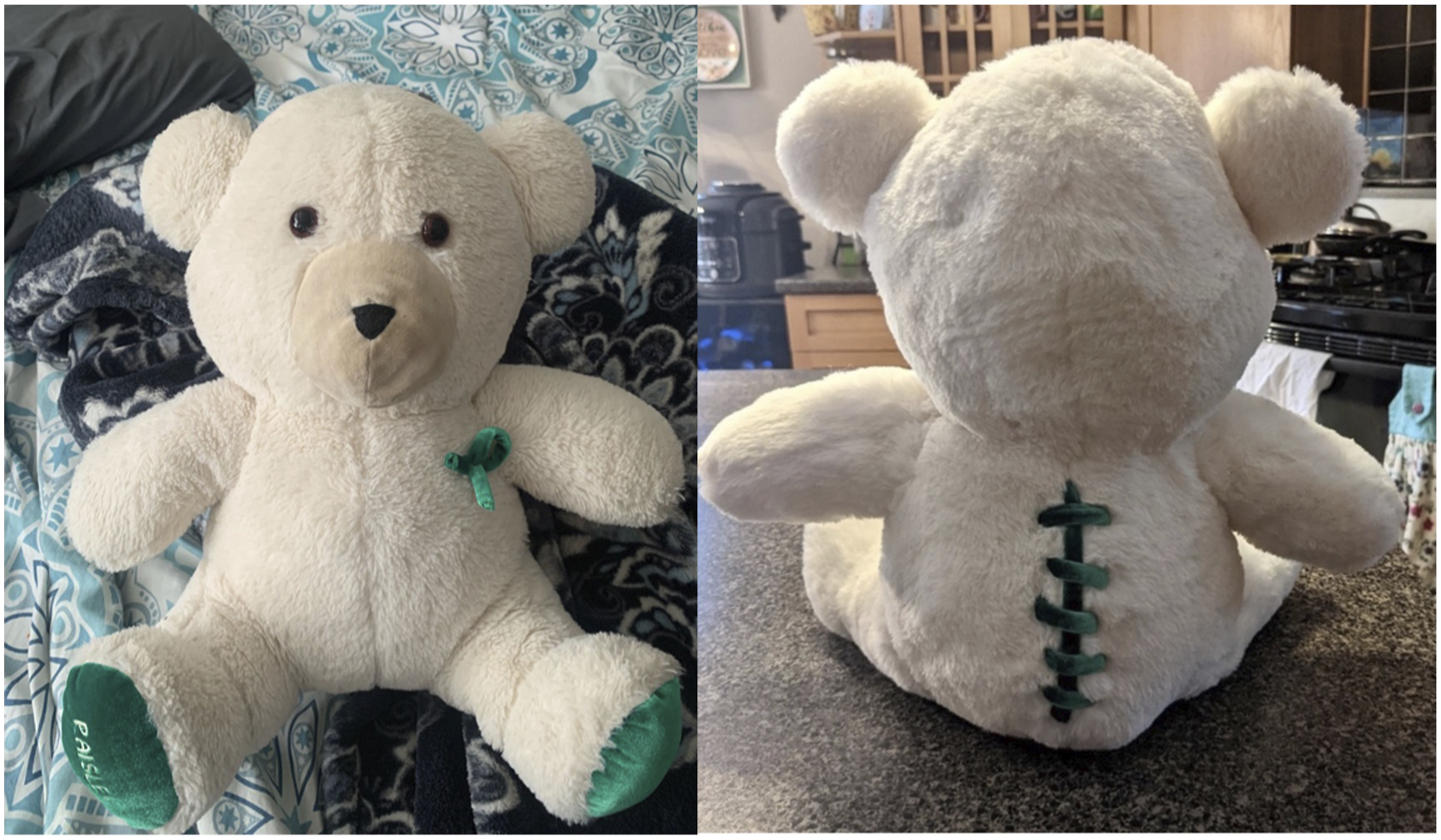
While navigating the surgery journey, youth faced several barriers. These barriers included bullying by peers, misunderstanding/invalidation by others (including healthcare providers), and aspects of the hospital environment (i.e., mundane physical environments). Jack described his experience of being bullied. People started making comments of like “hey, stand up straight” … So then the summer of Grade 7 I was like, “hey dad, like I’m tired of being bullied about this, can we look into options about this?” Like I want to fix it, I don’t want to be the weirdo that has hunchback, essentially. (Jack)
Indirect barriers included friends and family who were otherwise supportive (i.e., visits) yet overlooked situations that would cause exclusion/discomfort. These could include social gatherings that involved sitting on the floor, which could be painful or altogether inaccessible to youth post-surgery.
The hospital environment had positive and negative impacts on youth recovery. Some youth described the special moments in the hospital such as when Disney Princesses came to visit them. Youth provided several examples of how the hospital environment could be improved. Contextual changes included increasing comfort through plants and soothing music. Youth also expressed wishing they had received resources for psychological services before and after surgery. Adina described a lack of acknowledgement of her psychological distress from healthcare providers. She believed that resources and tangible support would have helped her to better navigate her journey. I remember all my doctor’s appointments after this, I was always in tears and the nurse didn’t suggest therapy until a couple months after. There was no mention of “oh maybe talk to someone.” (Adina)
Overall, this theme identifies factors that influence the emotional valence of each phase of the surgery and recovery journey that can be harnessed to optimize outcomes and experiences. Pets, hobbies, and nature were aspects that youth could control in their environments to foster mindfulness, physical activity, social support, and psychological/physical outcomes. Several youth shared distressing experiences of victimization from peers for their physical appearance. Further, youth expressed the need for mental health resources.
Theme 5: The Journey Sculpts Identity Formation and Sense of Self
Theme 5 underscores the personal transformation that occurred across, and in part because of, the surgery and recovery journey. Despite emotional, physical, and functional challenges, recovery enabled youth to start slowing down in their everyday life, be present in the moment, and appreciate the small but important joys. Many youth expressed that their surgery was a critical experience that catalyzed and accelerated their resilience and personal growth. However, it did not solely define who they had become.
Jennifer described that although there were heightened emotions and struggles in her journey, she was able to reflect upon and appreciate her life during recovery. Considering the contrasting events in her journey helped her orient her own life, identity, and sense of self. I don’t know if you’ve ever heard “The dance” by Garth Brooks? ... the lyrics not literally explained, but I think just the message where like the, the main chorus is, uh … “I could have missed the pain but, I’d have had to miss the dance” … And so like, you kinda have to have both in order to really appreciate what the good is, right? .... if you haven’t really experienced that rock bottom, you don’t know how high you really are. (Jennifer)
Several youth described recovery being marked by an ability to find deep meaning in everyday moments, such as viewing beautiful scenery and reflecting on their growth. Youth commented on their lives in a deeply interpretive way, which expressed emotional maturity that might be unexpected for their developmental stage/age. The memories and journeys of some youth permeated into areas of their present life; this could manifest as post-traumatic stress symptoms (e.g., intrusive memories), emotional distress, and pain. Not all youth returned “back to normal” physically and/or emotionally following surgery. The development of chronic post-surgical pain was common (70% of sample). Jack developed chronic pain and described continuing to vividly remember the pain (see Figure 10). His description implies that this memory of pain was both intrusive and he believed would never fade. Remembering the pain.
“There’s like no way to forget that pain I don’t think, ‘cause that pain will like forever stick in my mind” (Jack). Many youth described the strength and confidence they gained during and because of their surgery journeys. Their experiences provided transformative opportunities to transcend their former selves. One youth described how surgery equipped her with perseverance and confidence that emboldens her to tackle challenges and embrace adventure in her life today. The associated photo (see Figure 11) is at the top of a mountain she climbed to see a sunrise, which she was unable to do pre-surgery. This realization fuelled determination, confidence, and optimism for her future. I felt like I succeeded. I felt so proud of myself, and this journey had given me, so much … after surgery, I’ve had so much more determination and confidence and I’m always looking forward to more adventures and opportunity to make the most of things. (Lauren) Perseverance and confidence.
Overall, this theme describes how the surgery journey is pivotal in shaping the physical and mental health of youth and their identities. Youth physical pain experiences can be starkly contrasted such as Jack’s memories and current pain experiences in comparison to Lauren’s exceptionally positive pain outcomes. However, Jennifer, Jack, and Lauren all described their personal growth during their surgery journeys. Youth journeys extended well beyond their recovery, and youth were able to look back and reference their growth, strength, resilience, and ambition. By reflecting on these developments, youth learned about themselves and who they were (and could be) as people.
Discussion
This study is the first to apply a novel modified photovoice approach to represent the voices of youth who have undergone spinal fusion surgery. Varied and rich stories are described that can be relatable and meaningful to youth. The five themes demonstrate the uniqueness and complexity of each journey.
Theme 1 illustrated the importance that youth place on their physical appearance. Theme 4 highlighted the impact that healthcare providers can have on one’s surgery experiences. Further, findings within Theme 5 illustrated how youth surgery journeys have lasting impacts on lives by molding their identities. Taken together, these findings establish the importance of understanding the potential lasting impact healthcare providers’ language/behavior can have on youth with scoliosis. This can negatively influence their body image and experiences of being invalidated/validated within healthcare interactions. Some youth described feeling that their bodies were “different” and “ugly,” which may be reinforced by clinicians focused on fixing “abnormalities.” Previous work examining patient perceptions of weight-related language within care for childhood obesity lends insight into how language can impact the perceived self-image of youth (Puhl et al., 2011). Parents of youth perceived some words (e.g., “unhealthy weight”) to be motivating/advantageous to their child’s healthcare and recovery, whereas other words, like “fat” and “extremely obese,” were perceived to be stigmatizing and blaming (Puhl et al., 2011). Accordingly, when describing a spinal curvature, it may be advantageous to avoid terms such as “abnormal” or continuously pointing out what is “wrong” with their bodies. Several youth described experiences of invalidation from healthcare providers. Not only should there be consideration of body-positive or even body-neutral language, but healthcare providers should strive to validate youth so they believe that their concerns are understood and there is an alliance within the clinician–patient relationship (Wasson-Simpson et al., 2022).
Theme 2 provided an understanding of the worry and unpredictability inherent to surgery journeys, which can be impacted by pre-surgery physical abilities, the time from diagnosis to surgery, and expectations of post-surgery outcomes (physical and aesthetic). Some youth described concerns about whether pain would persist beyond recovery. For some, this could reflect catastrophic thinking about pain, which is a robust predictor of post-surgical pain (Noel et al., 2017). This reinforces the need to intervene and target pain-related cognitions, including catastrophic thinking about pain, before surgery and in the immediate post-surgical and recovery periods. Indeed, anxiety and catastrophic thinking about pain before surgery and in the acute recovery period are powerful predictors of pain months later (Noel et al., 2015; Noel et al., 2019; Rabbitts, Fisher, et al., 2017). Moreover, preoperative mental health, pain, and expectancies are predictive of patient satisfaction post-surgery (Sieberg et al., 2017). Many youth underscored that their mental health concerns were dismissed and/or not addressed before and following surgery and stated a strong desire for access to resources. A previous review found that simple psychological interventions, especially those used post-operatively (e.g., distraction) are effective in reducing short-term post-surgical pain (Davidson et al., 2016). Future research should assess whether these interventions impact other post-surgical outcomes including quality of life and school participation, and the efficacy of other approaches such as peer support. Accordingly, it is important to consider the benefit of community for youth who have undergone similar experiences such as major surgery, and this was evident through the mentioned #scoliosiswarrior support group. Those who care for patients who have similar experiences may be able to suggest joining similar support groups.
Theme 3 demonstrated how some youth experienced accelerated growth and transformation, whereas others experienced sustained distress and mental health challenges. Theme 5 underscored how youth were able to revisit and reflect on their journeys through their photos/videos, which many perceived to be deeply meaningful for them. Although some reflections were more positive than others, youth were able to take time to slow down and better understand their journeys. This speaks to the novelty of this methodology. Other research has applied photovoice methods where adults captured pre- and post-surgery photos to represent weight loss journeys and redefining body image post-breast cancer procedures (Johnson et al., 2018; Sloan et al., 2018). In the current study, photovoice was used to capture any aspect of one’s surgery and recovery journey that were most salient to them. By not solely focusing on pain or body image, a multifaceted understanding of lived experiences was revealed. Lived experiences encompassed pain, social development, identity formation, mental and physical health, and importantly their perceptions about how the systems (e.g., healthcare) that youth are forced to navigate can be improved. This method can bring to life and shape not only youth voices, experiences, and memories but can be used as an advocacy tool for system change.
Across all themes, pain and pain management emerged as a central aspect of youth journeys, both before and after surgery. This further underscores the necessity of providing pain and mental health resources from the beginning of surgery and well into recovery. In the current sample, 11 youth reported living with chronic pain before surgery and 14 reported chronic pain after the surgery. Previous research revealed that youth undergoing/had spinal fusion surgery felt unprepared to deal with the pain during recovery at home and feared becoming addicted to analgesics (MacCulloch et al., 2009). This underscores the need for multidimensional pain management and practical recommendations for youth healthcare. Youth in the current study expressed negative experiences with pain medication in the hospital; some experienced nausea and/or other negative side effects. They also expressed a need for, and lack of, resources for their emotional distress and mental health issues, emphasizing the need for a multi-pronged approach to pain and mental healthcare. The interaction between mental health and pain has been identified as a top 10 research priority by youth living with chronic pain (Birnie et al., 2019). Yang et al. facilitated preoperative patient education on pain management to reduce opioid use and measured prescription refill for youth undergoing scoliosis surgery. However, patients were not provided other additional psychological and/or physical strategies to manage pain (Yang et al., 2022). In the absence of providing youth with comprehensive multi-modal supports for pain and mental health before and following surgery, youth are at risk for experiencing long-lasting and deleterious health outcomes (Rabbitts, Fisher, et al., 2017).
Limitations
A limitation to photovoice approaches more generally is that those who may be uncomfortable sharing personal photos/videos may result in a barrier to their participation. Within this study, participant diversity was lacking; most participants were female, white, cis-gender youth; and sexual orientation was not assessed. Many voices (particularly marginalized and minoritized individuals) were not heard in this study and should be included in future research. Indeed, there is a need to apply antiracist frameworks and make efforts to embrace intersectional approaches in pain research (Morais et al., 2022; Sanders et al., 2022). A diverse sample can support a better understanding of the experiences of youth of equity-seeking groups who have been found to face stigmatization and inadequate care, which may further impact surgery experiences (Ezenwa et al., 2006; Szczepura, 2005). Second, all youth had their spinal fusion surgery at the same hospital, which may have resulted in similar processes across all participants. Moreover, all participants previously participated in a study conducted by our research team, and as such, they encompass a motivated group. Lastly, it was of interest to develop further knowledge translation outputs to have participants take part in digital galleries or exhibitions. The primary author is currently working with a community organization to facilitate an event with participants of the study. However, due to the busy lives of youth (many transitioning to high school or university) and their extracurricular activities, progress has lagged and will not align with the publication of this manuscript.
Conclusion
The current project used a novel photovoice approach to understand the rich and varied lived experiences of youth who underwent spinal fusion surgery. These journeys and narratives included, and extended beyond, pain. Five themes brought forth an understanding of how clinician language and behavior can have a lasting effect on youth and their recovery, with specific focus on body image. The worry and concern that youth recalled may reflect catastrophic thinking about pain, which is a powerful predictor of post-surgical pain outcomes. Youth described a dialectic of experiencing accelerated growth and challenges to their mental and physical health. While the surgery and recovery journeys of youth varied, the experience was integral in shaping their identities and futures. This work brings to life the voices of youth who have undergone spinal fusion surgery, enabling their experiences to be heard by other youth undergoing surgery, family members, friends, healthcare professionals, and researchers. This provides narrative possibilities and can be used to advocate for system changes to improve experiences for this population.
Supplemental Material
Supplemental Material - Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery
Supplemental Material for Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery by Samantha Noyek, Gillian Newman, Abbie Jordan, Kathryn A. Birnie, and Melanie Noel in Qualitative Health Research
Supplemental Material
Supplemental Material - Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery
Supplemental Material for Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery by Samantha Noyek, Gillian Newman, Abbie Jordan, Kathryn A. Birnie, and Melanie Noel in Qualitative Health Research
Supplemental Material
Supplemental Material - Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery
Supplemental Material for Photos Sculpt the Stories of Youth: Using Photovoice to Holistically Capture the Lived Experiences and Pain of Youth Who Underwent Spinal Fusion Surgery by Samantha Noyek, Gillian Newman, Abbie Jordan, Kathryn A. Birnie, and Melanie Noel in Qualitative Health Research
Footnotes
Acknowledgments
The authors thank all youth and their family members who participated in the study or supported youth in their participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by a grant received by Dr. Melanie Noel from the Canadian Institute of Health Research (Grant #: 427396).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.