
Abstract
Navigating the healthcare system with chronic pain, alongside navigating the experience of the chronic pain itself, is recognised to be highly challenging. Frequently available interventions do not fully meet the needs of people with chronic pain. This study aimed to explore the perspectives of people who have been through these experiences and now support and campaign for improved approaches to chronic pain management. Semi-structured interviews of 10 participants who independently support others through some form of chronic pain advocacy or support were conducted online. Data were digitally recorded, transcribed, and analysed using reflexive thematic analysis, through a critical realist and constructivist lens. Data were interpreted to represent a journey into chronic pain advocacy, represented by three overarching themes. Advocacy as healing incorporates sub-themes of pain trauma, gaining knowledge, and using my experience for good. Unequal partnership includes respect and unmet needs from institutions. The final theme, evolution, relates to two sub-themes of pushing boundaries and personal growth. Participants talked about the dual benefit of their contribution to pain advocacy, both in terms of helping others and also their own personal benefit. Overall findings indicated that pain advocacy can take multiple and various forms. Commonly, our participants who took on the role of pain advocacy were motivated by their own early difficult experiences, both navigating their pain and healthcare systems, and by a wish for others to not have similar difficult experiences. Having taken on the role, despite its challenges, rewards can include recognition and personal growth.
Introduction
Pain affects everyone in some way, in different ways, and at different points in life. For some, pain is severe and long-lasting. People with chronic pain face a multitude of challenges, both from within themselves and from the attitudes and actions of others. Negative popular discourses around disability, especially when that disability is not immediately visible, do not help this. Both universal and private healthcare systems produce mixed results for people suffering with chronic pain. In the United Kingdom, the National Health Service (NHS) provision has been unable to meet the needs of many patients, with one local study identifying experiences of a lack of integration between services, lack of specialist knowledge in primary care, long waiting times for specialist care, and a perceived lack of interest and empathy from professionals (Hadi et al., 2017).
Patients are in a unique position to understand the mismatch between service provision and patient need. Some act to help bridge this gap through sharing their own lived experience with other patients and clinicians. They do this in a variety of ways. They regularly speak at conferences, design patient resources, and provide their expertise to researchers and clinicians, with the age of social media allowing them to build up their own independent voices. Terms to describe this role include ‘patient representative’, ‘lived experience representative’, and ‘patient advocate’, amongst others. We have chosen ‘chronic pain advocates’ as the best term to provide both the breadth and specificity of experience needed for this study, while acknowledging that there is no perfect term.
There are no studies yet, to our knowledge, that explore the experiences and perspectives of chronic pain advocates themselves. There are, however, some studies analysing the perceptions of advocates/peer providers for other conditions, mainly in the field of mental health. Mowbray et al. (1998) discuss the growth of peer providers in mental health services, describing how through helping people like themselves peer providers gain more insight into their own challenges and pick up new skills through their work. This, alongside the empathic satisfaction in helping others, helped both providers’ self-esteem and perception of self-efficacy. Also discussed in this study is the shift in identity from that of a recipient of care to a provider of it. Moran et al. (2012) build on this, discussing the transformation of identity from that of a victim to that of a person with agency and opportunity. Despite these apparent benefits, the role of an advocate can also have some cost. The lack of remuneration can lead to a perception of lack of parity with professionals, with payment being seen as a symbolic recognition of the value of their role (Gillard et al., 2022; Mowbray et al., 1998). Further factors such as emotional stress (Ibáñez-Carrasco et al., 2019), ambiguity in their role as both a patient and a provider (Jack et al., 2018), maintaining boundaries with those that providers help (Hanly et al, 2020), and difficulty adapting to the physical demands of the role (Gillard et al., 2022) have been discussed elsewhere. We cannot assume that these experiences will generalise across to chronic pain advocates, but they can form a theoretical basis with which to direct our enquiry in this study.
Research Aims
The aim of this study is to use thematic analysis to explore the experience of those with chronic pain, specifically in their role as advocates. The research aims to unravel the personal experiences of these advocates, their experiences as an advocate, their motivations, and how these intersect with their experience of chronic pain.
Method
Methodology
Thematic analysis is a flexible method that can be used within a range of broad philosophical frameworks (Braun & Clarke, 2006). The current research is positioned within a Critical Realist framework (Bhaskar, 2020), adopting a constructivist epistemology with the expectation that different people will experience events differently within a realist ontology. Realist ontologies posit that, although they might be described or understood differently, experiences are based on real events with real observed or unobserved causes (Fletcher et al., 2017).
Researchers
The first author carried out all of the primary data collection and coding under close supervision from the senior author. The senior author, who has a long-standing interest in persistent pain through clinical and research roles, proposed the overall topic and recruited participants. After initial coding, both authors met together on a regular basis to discuss and refine the analysis. The importance of recognising the subjectivity of the researcher’s interpretation of their data, not as a threat to the validity of the conclusions but as a resource in itself, is well established in qualitative research (Braun & Clarke, 2019; Braun et al., 2014). The personal experiences of the researcher must be available to evaluate the bearing these have on analytical thinking.
We have provided a synopsis of the principal researcher to allow for external appraisal: I am a young MSc Clinical Psychology student, with a current background as a medical (MBBS) student. I have had no contact with chronic pain advocates prior to this research to my knowledge. However, I have met and helped treat patients with chronic pain in clinical primary and secondary care settings, giving me a basic awareness of the experiences of those with chronic pain. My motivation to study this topic comes from my interest in subjects where psychology and biomedicine meet, and how professionals can be advocates in these settings.
Data Collection
Ethics
This study was granted ethical approval by Newcastle University (Ref. 2298/19969). Participants read an information sheet and gave signed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Pilot Interview
We initially conducted a pilot interview with a chronic pain advocate to inform and refine our topic guide for the subsequent interviews. This participant’s data has not been used for analysis, nor has it been included in the final report.
Participants
Ten participants were recruited through social media via a mixture of purposive and snowball sampling, non-inclusive of the pilot interview. The description ‘pain advocate’ was chosen by the authors to represent anybody with lived experience of pain who was engaged in activities to help others with pain. This definition and the choice to study it arose out of personal contact between the senior author and several pain advocates occupying this space in diverse ways, and an emerging awareness of the breadth and challenges of such work. Inclusion criteria were as follows: over 18 years old, either currently or formerly involved in chronic pain advocacy in a substantial way, have experienced persistent pain, and able and willing to take part in an interview in the English language.
The sample size was determined to achieve adequate information power (Malterud et al., 2016) for the aim of the study. The specificity of the study and high quality of the data gathered supported a relatively small sample size which was pragmatically important due to the time available. We recruited initial participants through a public advertisement on the senior researcher’s Twitter page, tagging individuals and groups who we knew to provide pain advocacy or support. We used direct messaging or email to send a link to an information sheet and expression of interest form to those who replied and contacted everybody who filled out this information. Some participants suggested further suitable participants, who we recruited in the same way until the sample was complete.
Interview Process
We conducted all interviews via video call on Zoom. The interviews followed a semi-structured format to allow for a spontaneous and authentic conversation, while ensuring the interview remained focussed on the core topics. Each interview was digitally recorded and transcribed via the Otter AI (https://otter.ai/) online service. To maintain anonymity, we redacted identifiable locations and assigned participants a random letter to refer to them in text. We chose not to provide demographic data due to the highly public roles of some of our participants and the risk of breaching anonymity.
Analytic Procedure
The first author initially examined transcripts individually in detail in an idiographic approach, reading each transcript several times and producing semantic level codes to describe and interpret the participants’ experiences. We then assembled codes into prospective themes and analysed sub-themes with the aim of creating higher order themes to encompass them. As recommended by Braun and Clarke (2006), we reviewed the coded extracts for these themes to ensure they maintained internal consistency and then checked the candidate themes against the entire dataset to ensure an accurate representation. Themes were modified, combined, or subsumed throughout this process. Once we constructed the three higher themes, it became clear that they could be described as progressing from one to the other, akin to a journey.
Results
As expected, our participants’ experiences were diverse, from their experiences with pain to their chosen form of advocacy. Two participants defined themselves as ‘recovered’ from pain, with the rest experiencing varying degrees of pain. The majority of participants described experiences with pain medication, such as opioids, anticonvulsants, and antidepressants, although two had no significant medication use due to side effects. The forms of advocacy practiced by participants also varied greatly, examples being Twitch streaming, YouTube content creation, moderating online support groups, sharing resources via social media, being consulted in research, writing books or personal memoirs, producing media for charities and pain organisations, and sitting on health policy committees as a patient representative. We constructed three core themes from the data, expressed by all advocates: ‘advocacy as healing’, ‘unequal partnership’, and ‘realising potential’ (see Figure 1 for a thematic map). These themes describe the different stages in one’s journey into advocacy, capturing advocates’ motivations, challenges, perception of their role, and what advocacy has given back to them. Although the themes represent stages of a journey, they are not necessarily discrete blocks of time. Our analysis is sensitive to the fact that aspects of some themes that advocates described recurred throughout their advocacy journey. Thematic map representing ‘journey’ of pain advocates.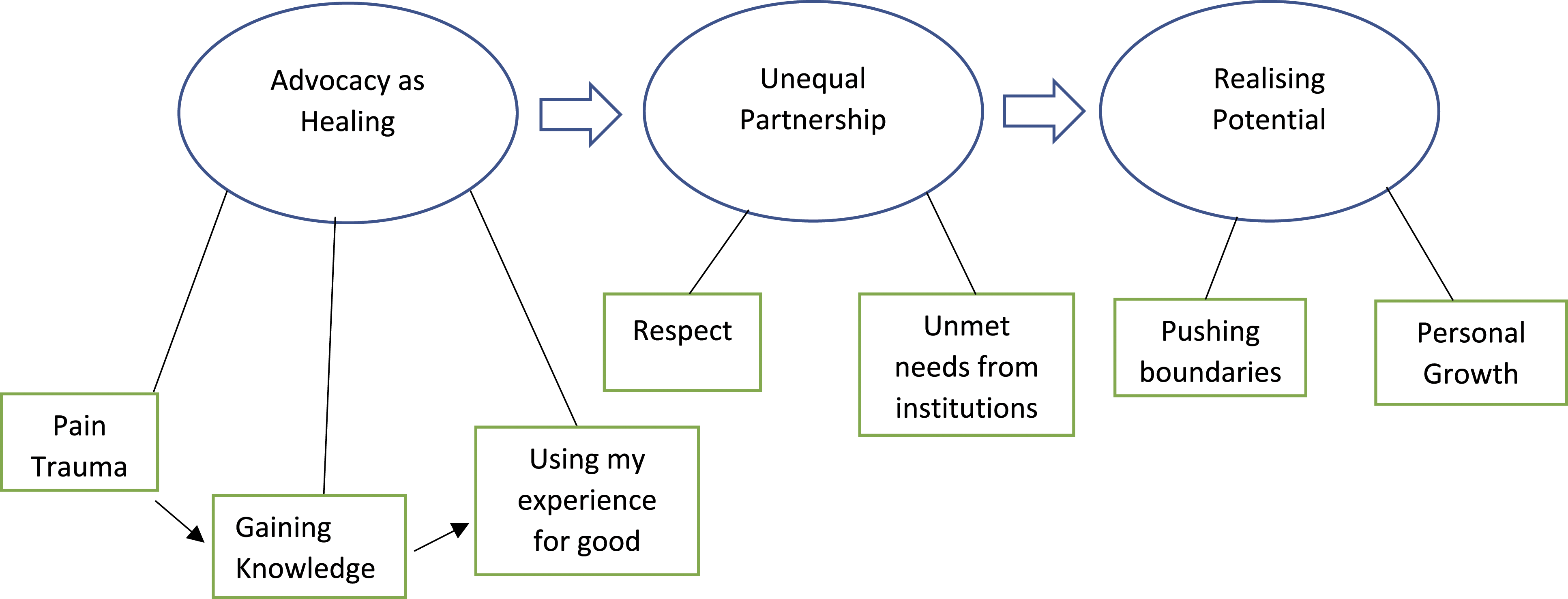
Advocacy as Healing
This theme encompasses the portion of the journey which led advocates into the world of chronic pain advocacy. It describes how advocates used their experience of pain to benefit others and how advocacy can be a vessel for healing the personal trauma from this experience. Three subordinate themes speak to this core theme: ‘pain trauma’, ‘gaining knowledge’, and ‘using my experience for good’.
Pain Trauma
It is beyond doubt that the experience of chronic pain is challenging, and all participants described difficult experiences, from both the pain itself and sub-par experiences in healthcare. Our participants’ experiences of pain are naturally diverse, with two experiencing pain from childhood. Both spoke of the sense of loss of their youth and early adulthood, and the formative experiences that usually come with this: I really suffered when I was in pain, I really lost out, you know, I lost a lot of my secondary education, I lost the ability to work through my 20s and my 30s. I missed out on my social life, I missed out, I missed like family weddings, family, christenings, parties, travelling, I missed [ ] so much, my life was very restricted. And I really am haunted by, if somebody had given me this information [ ], particularly when I was younger [ ], like 12/13 years old, found a way to communicate it to me and got me out of pain. My life would have been so different. (Participant W, lines 152–158)
W’s loss and the accompanying contemplation of ‘what could have been’ left a deep mark. Her consideration of how her life could have been markedly different had she had the information she does now represents an insight into why she advocates, preventing her experience happening to others. The loss of expected life experiences does not occur in a vacuum. It has a snowballing effect which leads to further loss. Fulfilling and enjoyable activities are a key protective factor in safeguarding one’s mental health, with social isolation reducing one’s ability to cope with the physical effects of pain. Here, M also discusses the impact of being forced to decline invitations to music gigs due to his pain: It was just, I didn’t get invited anywhere anymore. You know, [they would] ring me up and see how I was and that but yeah, it was a very solitude horrible life really. (Participant M, lines 36–37)
Six of our participants discussed their unmet needs in the healthcare they received for their pain. Some took medication for their pain, with some finding these experiences incredibly distressing. J discusses her experience with an ever-increasing morphine dose: I ended up in a pretty bad state, getting less and less mobile, needing almost, you know, around the clock, sort of help from my wife, who became my full-time carer. I was 25 Stone in weight, living in the armchair, basically, in agony, even though I was on all those drugs. (Participant J, lines 19–22)
This extract tells a story of decline from independence to dependence despite treatment that should have made her better. Helplessness features prominently here, from the lack of relief J’s medication brought and the degree that this left her dependant on her wife.
Gaining Knowledge
While the experience of chronic pain itself is not the primary aim of this project, conveying the perspective of advocates on this subject is imperative to understand their advocacy, as this is a universal ‘starting point’ for participants on their journey. The lack of benefit derived from medication and the lack of information on self-management and non-pharmacological therapies forced advocates onto the internet in search of alternative options. The gaining knowledge sub-theme represents learning about which skills can be developed to help with pain and why this helps according to our knowledge of pain science. This can be done through online courses, apps, and webinars and often represented a turning point for our advocates. F discusses the impact of the ‘Curable’ app here, which teaches mindfulness-influenced self-management and up-to-date information on pain science: And so it’s like these new ideas about you know, that hurt doesn’t necessarily mean harm, and just that you actually could have more sort of control. [ ]. Within a few months, I was put to 80%, pain, pain reduction. It was it was huge. [ ] really just took away a lot of the fear. And as soon as you do that, it just changes your life. (Participant F, lines 22–29)
Here, the helplessness in the experience of chronic pain is ameliorated by the sense of control described by F, her gain of agency contrasting with her experience of being a passive recipient of perceived ineffective healthcare. The experience being ‘life-changing’ speaks to a real breakthrough for F, a step change in her perception of her pain.
Using My Experience for Good
Advocates have described learning new ways of responding to their pain and gaining a new understanding of their pain, with their experience of it then changing for the better. This leads into the final sub-theme, ‘using my experience for good’. The concept of wanting others experiencing chronic pain to not have their experience was discussed by eight advocates, suggesting a degree of consistency in our sample with a very specific experience: I will fight for people to not have the experience I’ve had with, either with the pain but, but you know, sort of, because it’s a bit rawer and more traumatic at the moment, the opioid thing, I will fight for people to not have that experience. (Participant F, lines 450–452)
We see F’s recognition of her experience as something deeply wrong and, importantly, avoidable. This sense of empathy with other chronic pain patients acts as a focus to anchor her advocacy around, with the sense of trauma acting as a motivating driving force to affect change. The importance of this concept to advocates is evidenced by the feelings experienced when they do manage to make a difference to someone’s life: I’ve had really quite a few people contact me privately and say, ‘oh, you know, by listening to that, I then got better. And it was, I’ve got my life back’. And that’s, that’s the most incredible feeling. (Participant W, lines 160–162)
W’s experience with pain trauma and her sense of growth and improvement when she learnt new ways of approaching her pain herself leads to a sense of achievement and validation of her efforts when she helps to facilitate this breakthrough in another.
In sum, this theme describes the beginning of the journey for our group. We have seen the route from feelings of helplessness and loss through pain and the trauma it leaves; to the discovery of self-management and the step change this leads to in chronic pain patients; to the desire to use one’s experiences for the betterment of others and the therapeutic effect this creates for the advocates themselves. It is important to note, however, that while the motivations for advocacy fit into the ‘beginning’ of a journey, they are ever present and evolving throughout the journey.
Unequal Partnership
Once firm in their commitment and desire to use their lived experience for change, the paths our participants took in practicing their advocacy diverge into many different routes. These routes do, however, often involve interactions with professionals in the ‘professional’ pain world. This theme is only briefly outlined here, due to word restrictions. It explores how advocates and their lived experience are recognised in this world, particularly by the professionals and organisations that comprise it. We have illustrated this through two sub-themes which tell opposing stories: ‘respect’, detailing the feeling of respect and value conferred onto our participants by healthcare professionals in the pain field; and ‘unmet needs from institutions’, speaking of our participants’ simultaneous feeling of lack of respect for their role in this space.
Respect
In light of advocates’ experiences with healthcare professionals and the system as patients, it was somewhat surprising as a researcher to hear of their almost entirely positive interactions with healthcare professionals in an advocacy context.
R acknowledges this complicated relationship: I think the big the big difference in the short time I’ve been doing it is how we’ve gone from [ ] the patient and the doctor being at loggerheads, the enemy, if you like, to, suddenly we all realised that collaboratively, we can fix a lot of the issues. (Participant R, lines 46–48)
R’s comment is sensitive to the need for professionals to acknowledge and value lived experience. It represents the transition point where R realised the need to put past experiences aside to form a new relationship based on collaboration. For this to happen, however, there needs to be true inclusion of advocates. Here, L discusses how professionals have received him in his advocacy work: Very warmly. [I] felt that every meeting I’ve had with professionals has gone well, and I’ve come away [ ] with the impression that there’s a genuine desire to learn on their part. They think that patients have something genuinely useful to say, and that it’s genuinely important for them to hear it. It’s been quite inspirational, really. (Participant L, lines 196–202)
The genuine collaboration L has experienced has been achieved in part through active inclusion from the professionals involved. ‘Inspirational’ is a powerful and emotive use of language. L feels recognised, both in that his lived experience is valuable and that he is in turn valued by his colleagues.
Unmet Needs From Organisations
While participants did describe the affirming effects of true collaboration, their experiences were not universally positive. As advocates develop in their role over time, they may begin to assist organisations in writing guidelines, or creating media content. This work can be taxing in both time and effort, while expectations around payment for this work can clash with what organisations offer. This can lead to questions from advocates about how their role is truly perceived.
J and S both articulate the tension that can exist between actively contributing and being valued: And I think it, so I believe we should be recognised, especially with work that we do with the NHS. [ ] on the one hand, they’re telling us that our expertise is invaluable. But on the other hand, they don’t want to pay me, [ ], if you put me side by side with a pain consultant, now he knows what he’s talking about, because he’s done the [ ] the work if you like, the study, and he’s got letters after his name to say that. I know what I’m talking about, because I’ve lived it. (Participant J, lines 298–309) We’ve got an expertise, and we’ve given away the information of our expertise for free. Would healthcare professionals do that? No, they wouldn’t. (Participant S, lines 479–480)
J draws attention to the prevailing narrative from organisations in outwardly valuing lived experience, while tacitly categorising it as ‘less than’ clinical experience. ‘Side by side’ here is important as it relates to how advocates can be in the same setting and working towards the same goal as a professional, yet one is remunerated, and one either is not or is but at a fraction of the rate. S’ comment further draws attention to this inequality, classifying lived experience as a form of expertise and comparing the perception of it to clinical expertise. The desire for parity of esteem between the two types of expertise features strongly in our data. This lack of equality may act as a barrier to meaningful co-production, as it may not just be advocates who recognise how their experience is valued less, but professionals themselves may be susceptible to bias due to this lack of recognition.
In sum, this theme covers the stage of the journey where advocates enter the academic-professional pain world and negotiate their place in it. Pain professionals are hugely affirming and supportive of advocates and their lived experience; however, there remain misgivings from advocates around how much their role is truly recognised. To answer the question of why this is, organisations retain some policies around exclusivity and remuneration that go against the warm words of their members, raising the danger of the perception of paying lip service to patient inclusion.
Realising Potential
This theme covers the stage of the journey where advocates must confront some of the internal and external challenges of their role, and the learning and growth that occurs from mitigating these and from the practice of advocacy more generally. While this occurs throughout our participants’ journey, we are presenting it as an ‘end point’ in the journey as it captures the learning and growth which has occurred for advocates up to this point and what it means to them today. This theme contains two closely linked subordinate themes: ‘pushing boundaries’ and ‘personal growth’.
Pushing Boundaries
The role of an advocate varies widely, which can present challenges to how advocates define themselves. Here, we explore how advocates address the challenges in their role and the limits to what they can offer. A key aspect of the intersection between the experience of advocacy and the experience of chronic pain comes from the potential for overload. Coping with chronic pain is an intensive experience, and advocates can have difficulty meeting the demands placed on them, sometimes by their own desires and expectations: I’m not really good at saying no? I do [ ] have to be careful. I have several times sort of gone, probably gone a bit too far and brought on a bit of a flare that I needn’t have had. (Participant N, lines 70–71) I don’t think it’s that I’m frightened of letting people down. I think it’s just that everything that that people asked me to do sounds so interesting, [ ], it’s more of an odd, ‘you don’t want to miss out on that’. (Participant N, lines 84–86)
These two extracts from N show how she often needs to negotiate with the position of advocacy being a passion, while still entailing an often-intensive workload. The conflict between pain and the desire to contribute and ‘be involved’ can have consequences down the line. While this self-imposed overload featured more prominently, J also mentioned her difficulties in co-production: We’ve noticed that where we need two or three weeks’ notice of a job needing to be complete. Clinicians tend to work in a space where, they’ll do it tonight, and it’s got to go out tomorrow, you know, it’s all last minute stuff. And we can’t work like that. So when you bring the two together to work, You’ve almost got to say, ‘well, you know, [ ] this is what we need. And this is the only way we can do it. So you need to give us a little bit more time’. That can be a challenge trying to explain. (Participant J, lines 248–253)
This extract shows a mismatch of working style and how in J’s experience their working style can seem alien to clinicians. There appears to be a scenario where the clinician working style is seen as the ‘default’, with J specifically intervening to create a working environment that facilitates each member of the team. Her final sentence indicates that this is not an uncommon occurrence, further playing into the question of accessibility and recognition for advocates as part of a multi-disciplinary team.
Personal Growth
As advocates find their boundaries pushed, they must adapt their approach to deal with this. There is often a learning curve; overcoming these challenges helps advocates to pursue their goals, with the journey of advocacy providing a wealth of new skills and personal insight for advocates. Learning to prioritise oneself is an important early lesson for advocates, as discussed by F here: And saying, ‘Do you know what? No, I don’t want to do that’. Or ‘I don’t have the capacity to do that at this point’. And then not feeling guilty about it, [ ] and I still get a bit of FOMO you know? (Participant F, lines 434–436)
F makes reference to her passion for advocacy through her ‘FOMO’ (Fear Of Missing Out) and her fear of letting others down with her reference of guilt. The strain is not being imposed on her externally but through her internal desire to contribute and be involved, with a direct conflict between what she can do and what she wants to do. She makes a conscious decision to rationalise the feeling of guilt and accept the limitations that her pain places on her. Pacing is a method that is used by some advocates to manage their workload. The flexibility in the role of an advocate allows advocates to set their own schedule to a degree, with L describing here how he strategically organises his workload in a way that mitigates the impact of his pain: But usually, I would try to make sure that I’ve got, you know, a good couple of hours between different appointments or different demands. I try to spread deadlines as much as I can. (Participant L, lines 240–242)
Beyond overcoming challenges inherent in the role, our participants described a variety of poignant ways in which advocacy has helped them grow as people. Here, V articulates how chronic pain has affected her confidence and the way that advocacy has helped this: Pain can wear away your confidence, especially when you’re constantly not believed. [ ] And you know, ‘people wouldn’t want me in that space anyway’, because, you know, ‘I need some help for this, I need help for that. So it would just be awkward if I was in that space, it would be difficult for people so I won't enter that space’. Whereas the stuff that I’ve done [ ] has made me realise that actually, I can curate a space. [ ] And consequently, it’s also okay for me to be in that space. And so most of it, I think it’s about confidence, and feeling like I’m allowed to take up some space. (Participant V, lines 417–425)
V describes her past experiences of being doubted and disbelieved with her pain and how she internalised this message, affecting the spaces she felt comfortable being in. Her directed efforts towards curating a space where people like herself feel accepted have allowed her to show similar grace to herself, thus internalising this acceptance. R also mentions gaining confidence through advocacy: My confidence, my ability to live my disease, my acceptance as well, because let’s be honest, chronic illness is one big grief cycle. So my acceptance of it, and it being part of me and trying to do something that allows me to scratch that sort of creative itch I have from when I was younger and used to play in bands and, and things that I don’t do now. (Participant R, lines 538–542)
R spoke earlier in his interview about how he viewed his condition, saying: ‘I was one of these people that just hid my condition’ (lines 30–31). His advocacy has allowed him to transform his relationship with his pain, from that of a hidden shame to an integral part of his sense of self. His experience of pain advocacy allowed him to display his creative passions, opening a side of himself which had been hidden since childhood. This also relates to how advocates gain new skills through their work, discussed by R and others.
A final extract that speaks to this theme comes from L, describing how advocacy has changed him as a person: It’s made me… God without, without going all sort of reality TV… I, I’m, I’m a better husband, better father. A more sympathetic listener. [ ] Because in in gaining a level of acceptance and understanding of myself [ ], I’ve been able to benefit from the support of other people. (Participant L, lines 364–367)
In sum, this theme has shown how advocates must negotiate their role with their physical and emotional limitations and how these experiences, and those of advocacy as a whole, have contributed to their present-day self.
Discussion
This research sought to unravel the experience of chronic pain advocacy through exploring why participants advocate, their interactions with other patients and professionals, and the process of negotiating the challenges brought by the role. Through analysis of participants’ experiences in these areas, we have constructed a narrative that shows how these factors interact to form their overall journey: from their experiences with pain, their desire to use these to help others, the negotiation of their role in the academic-professional world, to how they have confronted challenges to bring them to where they find themselves today.
Although we are not aware of any other studies specifically considering the role of pain advocates, our findings resonate with other studies. Participants described the transition from a position of the patient with a sense of helplessness and loss to that of sharing their success with others and supporting them to change, and thus finding a sense of catharsis and healing. This finding appears to mirror that of the journey of adaptation and empowerment for people with chronic pain, starting from a position of feeling torn apart from self and others and ending with a sense of re-integration and meaning (Toye et al., 2021). The journey is reliant on receiving sensitive education and support and supports the dynamic of starting with difficult experiences of pain and care provided before moving through stages of new understanding and integration. It is known to be important that pain management is delivered sympathetically and tailored to individual needs (Spink et al., 2021) and that often these elements are perceived to be missing for people living with pain (Upshur et al., 2010). Several of our advocates described a strong motivation for providing what was missing in their own healthcare journey for others.
Throughout the narratives, participants discussed moving from an unwanted identity as a pain patient to taking on qualities of an advocate, offering insights and solutions. Social identity is thought to develop through the identification of an individual with groups of people who share certain characteristics (Haslam et al., 2009). The reframing of experience described by advocates, transforming from something that weighed heavily on them to an asset benefitting the lives of others, is similar to findings in mental health peer providers (Moran et al., 2012). Moran et al. (2012) posit that this shift allows the formation of new meaning and identity from illness, from one of victimhood to one of agency and opportunity. Like peer support workers for unhoused people (Kennedy et al., 2019) and mental health peer advocates (Moran et al., 2012), participants of this study highly valued the new skills that they had acquired. Moran et al. (2012) further link advocacy with improved wellness through self-actualisation and reaching one’s potential. This is consistent with the improved confidence featuring prominently in accounts of participants in the current study.
As the patients in this study progressed into the roles that they adopted, they experienced a tension between an identity as a pain patient and a relatively unformed identity as a patient advocate. The latter appears to exist in something of a liminal space, with advocates neither fully inhabiting a patient nor professional identity. The meeting of their diverse experiences with standardised organisational expectations created dissonance for them. Trainee doctors from diverse backgrounds can experience a similar tension between personal and professional identities (Frost & Regehr, 2013).
The benefits experienced by advocates thus do not come without challenge. Advocates experience tension between having insights that are welcomed, valued, and important professionally, yet being unable to fully step into the health professional world due to organisational constraints. It is challenging to occupy space where there is an expectation of the ‘norm’ that does not include you or take your experiences into account (Fanshawe, 2021, p 89). Too often our advocates found themselves navigating this space for little financial reward, but with a strong motivation to help to change things for people with persistent pain. The value given to their input, by individual professionals at least, indicates a recognition that as in other contexts (Phillips et al., 2006) the diversity that advocates bring (in this case their experience with pain) is important for broader and more creative thinking to solve problems. The burden of contributing to this diversity as unequal partners who did not fit the ‘norm’ as defined by the service structure often took a high toll on advocates who had to negotiate the roles that they had taken on alone.
Despite the challenges involved, the overall experience of participants was positive. Overall, the way in which advocates perceived their work as ‘giving back’ to them explains and cements the importance of advocacy in their lives.
Limitations
This study does have some limiting factors. The relatively small size of the eligible population necessitated a mixed approach of purposive and snowball sampling. As such, our sample is potentially vulnerable to sampling bias if our advocates come from linked social networks with similar views. We took a broad approach to defining an ‘advocate’ to allow us to examine the breadth of the role. However, someone who produces content on YouTube is doing something quite different to someone who works as a patient representative for clinical commissioning groups. While this is important for identifying broad overarching themes in the role, it may dilute some of the more subtle messages from a given aspect of advocacy.
Conclusion
Chronic pain advocacy incorporates a diverse set of activities that may be linked by the overarching themes of advocacy as healing, unequal partnership, and realising potential. Many of the experiences described resonated with previously reported findings of advocates for other health conditions. People living with pain have much to offer both to their peers and professional networks; however, in doing so they find themselves working within structures that are not set up to accommodate them. Questions remain about how this emerging contribution can be appropriately recognised and rewarded.
Footnotes
Author Contributions
CH contributed to conceptualisation of the research, conducted the interviews, carried out the analysis, and wrote the first draft. CP contributed to conceptualisation of the research, oversaw the analysis, and reviewed the finished article. Both authors agreed to the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was granted ethical approval by Newcastle University (Ref. 2298/19969).