
Abstract
Explanatory models are culturally informed representations of illness that convey understandings of the etiology and expected course of disease. Substantial research has explored lay explanatory models, but examining physicians’ clinical explanatory models can also provide insight into patients’ understandings of illness because physicians are a foundational source of authoritative knowledge that shapes lay concepts of illness and disease. This study characterized the explanatory models used by pediatric gastroenterologists when explaining inflammatory bowel disease (IBD) to children. We conducted semi-structured qualitative interviews with 20 pediatric gastroenterologists across the United States about their clinical communication and explanatory models. We identified two primary explanatory models used to describe immune dysregulation in pediatric IBD: the defense and protection model, which characterizes the immune system as an army that erroneously sees the body as “non-self” and attacks it; and the switch model, which conceptualizes treatment as activating a switch that turns off a faulty immune response. We also identified two models used by some physicians to describe inflammation: the scratch and scrape model, which compares IBD inflammation to scratches or scrapes on the skin; and the bonfire model, which compares inflammation to a fire in need of extinguishing. While the use of militaristic metaphors is pervasive in medicine, describing autoimmunity as a battle against the self may lead children to perceive their body as the enemy. This may be compounded by describing the immune system as “confused” while noting its ongoing protective function. Use of these explanatory models may nevertheless improve patient disease-related knowledge.
Keywords
Introduction
The physician-anthropologist Arthur Kleinman (1981) initially proposed the concept of explanatory models to describe how individuals conceptualize their diseases. Explanatory models are culturally informed representations that convey practical rather than theoretical notions of illness (Kleinman, 1986). Kleinman differentiated “disease” from “illness,” describing the former as a pathophysiological disorder, while the latter encompasses the psychosocial components of being in a sick body (Kleinman, 1986). By characterizing how a person understands their disease, its etiology, and expected course, explanatory models provide a conduit between “disease” and “illness.” Physicians’ awareness of patients’ explanatory models can help bridge the physician–patient gap in clinical counseling, enabling clinicians to link treatments to individual understandings of disease (Hoy, 2014).
In the years following Kleinman’s foundational work, explanatory models research fell into three domains. The first explores how patients’ explanatory models of illness inform their self-understanding (Ailinger & Dear, 1997; Kinavey, 2006; Kirmayer et al., 2004; White, 2005). Lay explanatory models are culturally, clinically, and personally constructed (Kirmayer et al., 2004). For example, White (2005) found that patients with Hansen’s disease, or leprosy, in Brazil, combine culturally held beliefs of Hansen’s disease as an “unclean” disease with observations of their surroundings. Doing so creates an explanatory model that attributes their disease pathology to impurity and poor hygiene rather than to viral transmission via respiratory droplets. Examining patient explanatory models like these can enhance understanding of how patients experience illness.
The second domain of explanatory models research explores variation between laypeople’s and physicians’ explanatory models (Baer et al., 2004, 2008; Cohen et al., 1994; Maupin, 2015; Weiss, 1997). Cohen et al. (1994) demonstrated that patients prioritize symptomatology in their illness conceptualizations, while physicians emphasize pathophysiology. However, even though physician explanatory models are informed by the “medical gaze” (Maupin, 2015), physicians and laypeople share explanatory models for the common cold (Baer et al., 2008), diabetes (Maupin, 2015), and AIDS, heart disease, and cancer (Weiss, 1997).
The third domain explores clinical explanatory models, which clinicians use when describing diseases to patients. White (2005) notes that patients’ understandings of illness are shaped by the explanatory models given to them by physicians at diagnosis and that patients accept these models if they match their personal experience of the disease. For conditions in which the etiology is presumed to be primarily psychological, such as some forms of chronic pain, clinical explanatory models can influence patients’ sense of personal responsibility for illness, which may lead to stigma and shame (Buchbinder, 2015; Kirmayer et al., 2004). Examining physicians’ clinical explanatory models can provide insight into patients’ understandings of illness because physicians are a foundational source of authoritative knowledge that shapes lay concepts of illness and disease.
Research into explanatory models of the immune system has spanned these three domains. In Flexible Bodies, Emily Martin (1994) describes explanatory models of the immune system held by laypeople, immunologists, alternative medical practitioners, and the popular media. Martin shows how explanatory models characterizing the immune system as an army that combats external pathogens dominated popular and clinical understandings at the time. The immune system was described as aware of “self” and “non-self,” targeting and attacking pathogens it deems as “other.” Martin’s respondents often expressed concerns with the violent imagery of battle metaphors and sometimes provided alternatives—such as conceptualizing the immune system as a communication system that “can learn from and adapt to experience” (p. 109) or as a collection of cells that “eat” pathogens rather than destroy them (p. 70).
Brada (2013) also analyzes explanatory models of the immune system, in her case, those used to disclose positive HIV status to children in Botswana. She shows how children are taught to think of their antiviral treatment as assisting the “soldiers of the body” in fighting the “bad guy”: HIV. These terms help to cultivate children’s positive orientation toward their treatment, which is seen as vital to adherence. As in Martin’s description, this explanatory model also maintains the “self” and “non-self” dichotomy of battle metaphors for the immune system.
Using such figurative language when communicating with children may increase disease understanding when developmentally tailored (Whaley, 1994). This communicative strategy is particularly valuable because children with chronic illness may have poor disease-related knowledge (Deyk et al., 2010; Eiser et al., 1988). Developmentally appropriate explanations for diseases may also reduce children’s distress and improve chronic disease self-management (Eiser et al., 1984). Given these potential benefits, a better understanding of the clinical explanatory models used in pediatric populations is warranted. The purpose of this qualitative study was to understand the clinical explanatory models pediatric gastroenterologists use to explain inflammatory bowel disease to children.
Inflammatory bowel disease (IBD) is an umbrella term for Crohn’s disease and ulcerative colitis, which are characterized by inflammation and ulceration of the intestinal lining (Malaty et al., 2010). Historically, Crohn’s disease and ulcerative colitis have been considered autoimmune diseases (Plevinsky et al., 2015). The clinical course of IBD generally involves periods of remission and disease recurrence. During recurrence, patients may experience weight loss, diarrhea, and abdominal pain. Pediatric patients with IBD face challenges that are common to other pediatric chronic illnesses such as medication non-adherence (LeLeiko et al., 2013) and high rates of anxiety and depression (Blanchard et al., 2000; Burke et al., 1989; Taft & Keefer, 2016). Because the average age of IBD diagnosis has decreased while the global incidence has risen, more individuals with IBD are being diagnosed as children (Sýkora et al., 2018). Examining clinical explanatory models used with pediatric IBD patients may help to improve treatment adherence and emotional distress.
Research Design and Methods
We conducted a qualitative descriptive study using interviews with pediatric gastroenterologists from across the United States about their communication with patients. The goal of qualitative descriptive research is to “offer a comprehensive summary of an event in the everyday terms of those events” (Sandelowski, 2000, p. 336). It differs from other kinds of qualitative description, such as phenomenology, grounded theory, or ethnography in that it offers low-inference interpretations, staying closer to the “surface of words and events” (Sandelowski, 2000, p. 336). In this sense, its primary purpose is to produce descriptions rather than theory. We chose an interview design rather than audio-recording patient consultations due to the sensitive nature of initial diagnostic appointments, in which a researcher’s presence could be disruptive. Furthermore, conducting remote interviews permitted us to sample a wider range of explanatory models from physicians across the United States than would have been possible in a clinic-based study.
Physicians were eligible for the study if they routinely explain new diagnoses to pediatric patients with IBD as part of their clinical practice. Recruitment was facilitated via an announcement sent to a listserv for ImproveCareNow (ICN), the largest pediatric IBD learning health network. This announcement was reviewed and approved by ICN’s research committee. We identified additional pediatric IBD physicians via health center website listings and contacted them directly with information about the study. We also employed a snowball sampling strategy, in which participants were asked to identify eligible colleagues and share information about the study. The study protocol was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill. All participants provided verbal informed consent prior to enrollment in the study.
CBT conducted semi-structured interviews over a secure video conference platform between June and August 2021. The interview guide was developed inductively by the first author, informed by the explanatory models and IBD literatures. MB, a medical anthropologist with expertise in qualitative methods, reviewed the draft interview guide and made substantive changes. Both authors were diagnosed with Crohn’s disease as children, which enhanced their identification of relevant domains. The guide began with questions about the participant’s professional background and interest in pediatric IBD. It then included questions about how they communicate a diagnosis of pediatric IBD, how they explain disease etiology and treatments, how they assess patient disease understanding as the patient ages, communication with caregivers, and communication challenges. We pilot tested and refined the interview guide before beginning data collection.
Interviews lasted 60–75 minutes, and audio-recordings were supplemented with ethnographic field notes. We determined sample size by saturation of themes. We used a qualitative descriptive approach to analyze interview transcripts (Sandelowski, 2000). After all interviews were transcribed by a professional transcriptionist, the first author created a structured coding dictionary based on emergent themes. We used Dedoose (Dedoose Version 9.0.17, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data, 2021), a qualitative data management and analysis platform, to assign codes to units of interview text that matched the code definition. During an initial training period, we both coded three transcripts while blinded to the other’s work. We discussed and resolved discrepancies and updated the coding dictionary as needed to reflect necessary definitional changes. By the third transcript, we attained complete agreement so that the remaining transcripts were coded by the first author. We analyzed coding reports to identify patterns for various coding themes.
Findings
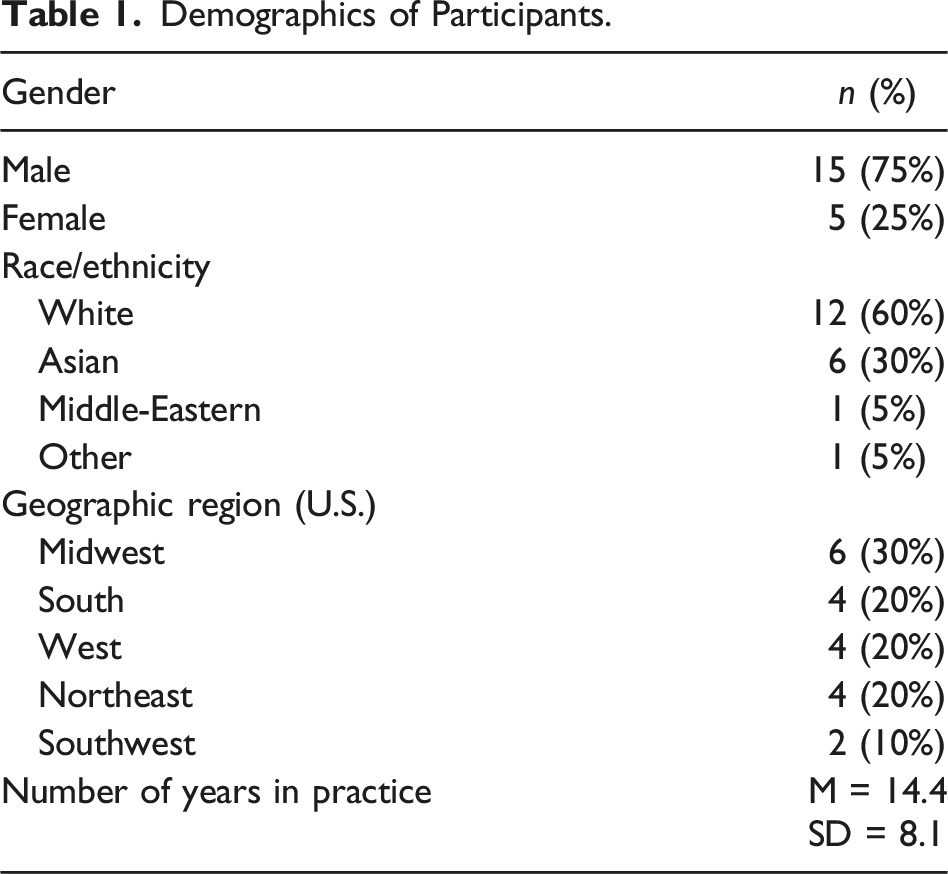
Demographics of Participants.
Participants noted that before receiving a formal diagnosis, most patients and their families are informed that their symptoms may be explained by IBD. Most participants indicated that after the child’s diagnostic colonoscopy, the IBD diagnosis is explained to the caregiver(s) while the child remains anesthetized. Aside from providing families with resources about IBD to review together, no participants reported that they prepare caregivers with information about how to explain IBD to children once they regain consciousness. Most physicians explain the disease to the child during the first diagnostic visit, 1 to 2 weeks following the colonoscopy.
Participants described two primary types of explanatory models in pediatric IBD. The defense and protection model and the switch model were used to describe immunity and autoimmunity, while the scratch and scrape model and the bonfire model were used to describe inflammation. We describe these models further below.
Defense and Protection Model
The defense and protection model characterizes the immune system as either an army or, more generally, as a defense or security system. As one participant explained: Let’s say you were fighting in a war and you had an army. And your army was very loyal to you as the general of your army .... And you said, “Okay, we’re gonna go over that hill and we’re gonna attack the opposing army.” Well, what if on the way to attack your army, people all of a sudden decided they didn’t like you so much, and they decided to instead turn around and help the other people attack you? (Participant 09)
In this model, the immune system is characterized as a network that helps keep the patient safe by fighting off infections or “invaders.” Six participants explicitly described the immune system as an army that patrols the body, while other descriptions were broader, referring to it as a defense system or an alarm system for the body. In some instances, participants did not explicitly compare the immune system to an army but did use militaristic language, such as “attack” and “patrolling.” The following example demonstrates this approach: But I literally just say that there are spectrums or different types of autoimmune conditions, where your immune system is literally attacking its gut. And I’ll say that sometimes, it’s frequently maybe brought on by an infection and your body was trying to actually recognize and attack this germ on you. And instead of just turning itself off and going back to patrolling, it, for whatever reason, it started seeing your gut as something to attack and started causing that inflammation. (Participant 05)
This model depicts the immune system as erroneously perceiving the body as “non-self” rather than “self,” which prompts it to help the opposing army to attack. Participants using this model sometimes referred to the child’s immune system as “it,” whereas the child’s body or intestine were referred to as “your,” implying a separation between the self and the dysfunctional body. This differentiation contradicts the autoimmune dimension described by this model, encouraging patients to consider their rogue immune systems as independent entities.
Some participants suggested that the immune system was doing its job “too well” or that it was “too strong” rather than characterizing it as abnormal or dysfunctional—perhaps to promote a more positive self-image. And this idea that this protective force on behalf of ... we’ll just say Billy. … It’s there to protect Billy, but for some reason, for reasons we don’t know, that force decides that your intestines are the enemy. And instead of just fighting bugs and viruses and things like that, it decided to also fight your intestines and, unfortunately, do a really good job ... As good of a job as it does fighting infections, it’s doing a good job of fighting your intestines. (Participant 12)
Several participants expressed concerns about the use of violent metaphors with children (see also Martin, 1994), but the majority did not. Their lack of concern may reflect the dominance of violent metaphors for the immune system in American culture more generally.
Switch Model
In the switch model, the dysregulated immune system is conceptualized as a switch that does not turn off when it should. One participant attributed “turning on” the switch to infections, while the other suggested that the etiology was broader. Because the immune system does not “turn off” as it normally would, medications are required to turn it off; continuing medications over time keeps the switch “off.” Notably, the switch model provides a clearer explanation of treatment than the defense and protection model does. Think about your immune system as a light switch, right? So you get an illness, cough, cold, something and your light switch turns on to fight off this, but it should turn off, but it doesn’t. So now it’s just broken, and it’s turned on. So it’s just over-activated. It’s constantly just fighting, and there is nothing to fight anymore, but it’s just in that on phase. So you have to turn it off and turning it off is—you’re using medications, diets, things like that, to keep it off. (Participant 04)
This participant’s clinical explanatory model refers to the immune system’s function in fighting infection as contributing to turning the switch “on.” However, they also state that medications keep the switch “off.” This may suggest to patients that the immune system is “turned off” and therefore not able to fight off infections when the patient is medicated.
Unlike in the first quote, this next participant does not explain the role of the immune system in protecting the patient, instead focusing on its dysfunction. So, the body’s immune system, your genes get flipped on, and go into overdrive and then attack itself. And, the attacking, at least, focuses on the bowel but because your whole body’s immune system is involved, other organ systems can also be involved. ... But in essence, it’s where the body’s immune system, something flipped the switch. And it’s probably multiple things that led to the switch being flipped on. And then, your immune system now in overdrive is attacking itself. (Participant 06)
By overlooking its protective role, this model emphasizes how the immune system attacks the patient and leads to symptoms. Both participants use militaristic words like “fight” and “attack,” which, as in the defense and protection model, suggest a combat-based framework for understanding the immune system’s function.
Confusing and Deceiving the Immune System
Across both the defense and protection and the switch models, participants personify the immune system, referring to it as “confused” or “deceived.” Three participants explained that the immune system attacks the body and causes disease because of this confusion. One participant described the immune system as “tricked” into being “over-excited” and causing injury. I tell them that the immune system is overactive. It thinks that there’s an infection and behaves like there’s an infection, which is a good thing if you have an infection. And usually when we get infections and our immune system wakes up to fight the infection, it goes to that area where the bug is, it releases a lot of chemicals, these chemicals try to break down the entire tissue around the bug and the bug itself. ... And in IBD, with a lot of research that has looked into this, we do not know why the body thinks that there’s an infection, because there’s no infection, usually, that we can put our fingers on. And the body then doesn’t know how to stop this immune overdrive, so it can go back to balance. (Participant 16)
This model uses a similar framework to the switch model, describing the immune system as “waking up” rather than being “turned on.” This participant describes the immune system as an entity within the patient that has woken and cannot put itself back to sleep. Rather than comparing the immune system to an army or a light switch, this model relies on the patient’s understanding of the state of confusion.
Another participant integrated concepts of confusion and deception with the defense and protection model: So I say that’s ... try and liken it to our defense system. So, therefore, the immune system is constantly on guard and defending us against germs. But also, you know, it surveys the body for abnormal cells or precancerous cells. So I just sort of say it’s our defense system and it helps protect us, but sometimes it can be tricked into attacking or defending against something that isn’t really an outside invader. But it can’t tell the difference and so it attacks, and does its job almost too well. (Participant 15)
As in other defense and protection models, the immune system is described as doing its job “too well.” However, whereas in previous examples the immune system “decides” to attack the body, here it does so without agency. Describing the immune system as confused or deceived removes some of the blame assigned to it, and therefore to the child’s body, in the attack. Instead, the blame is displaced onto an unidentified third party.
Using the defense and protection model and switch model, most participants described how the immune system malfunctions in IBD. One participant additionally described the immune system’s ongoing protective function for the patient, stating: So things that would make you sick, things that could give you the common cold, viruses that could do that, or tummy bugs or rashes, or all sorts of things. And so it’s supposed to be a friend, right? And it does really good things for you and it has done really good things for you for your whole life. And it still is doing really good things for you. It just happens to also right now be doing something to you that’s not that good. So it serves multiple functions, right? But it’s still doing those things. It’s still fighting off infections. It’s still keeping you healthy, but it’s also making you sick in this way. (Participant 10)
Here, the participant emphasizes that despite the immune system’s contribution to disease, it continues to keep the patient “healthy” in other ways. This account permits the patient to see their immune system as both “friend” and foe. As with models that incorporate confusion, the immune system, and therefore the patient’s body, is not as villainized.
Autoimmunity Versus Immune Dysregulation
Among those participants who offered explanatory models of the immune system, two indicated that they did not conceptualize IBD as an autoimmune disease. Some participants noted that the target of the immune system was not the intestinal lining but rather the bacteria in the microbiome. So I describe it, the physiology, as their immune system, which is supposed to be helpful in fighting off bad guys, invaders, pathogens, and helping to determine what is self and what you should allow into your body, and what is foreign and what you shouldn’t allow into your body. That while your immune system is healthy, it’s doing all those things and that inflammatory bowel disease, in either condition, that the immune system is inappropriately activated. So it is recognizing something most likely in the gut or at the interface between the bowel and the immune systems, the inside world/outside world, that interface, the immune system is recognizing likely microbes as foreign. And so, as what happened if you got a viral or bacterial infection in the intestine, your immune system, because they recognize these microbes as foreign, will send the immune cells, lots of white blood cells, to help fight off those microbes. And that process causes the intestinal inflammation. (Participant 10)
This explanation is consistent with new understandings of IBD as an inflammatory disease in which the immune system attacks bacteria in the digestive system rather than an autoimmune disease where the immune system attacks the intestine itself (Wu et al., 2020). This participant also employs the switch model in suggesting that the immune system is “inappropriately activated” or turned on.
Scratch and Scrape Model
In addition to explaining the immune system, some participants offered explanatory models for inflammation. Of those who did so, many employed the scratch and scrape model, which compared IBD inflammation to scrapes or scratches that are on the inside of the gastrointestinal tract instead of on the skin. One participant explained: So ongoing inflammation can make it so that your intestines don’t feel well, you can feel some pain, you may have loose stools, it may make it more difficult for you to eat. So I kind of try to keep it very generic and basic when I'm talking to a young child … we talk about sort of like when something gets irritated. And I think a simple example is if you scrape your hand on something, oftentimes, it’ll become red and swollen. That’s because there are cells from your body helping for things to heal up or to fight off things that are foreign. (Participant 17)
This participant refers to something the child is familiar with—a small injury on the skin—to help the child visualize what is going on inside their body and causing their pain and diarrhea. Even a child who cannot conceptualize their intestines can likely relate how previous injuries may relate to their IBD pain.
Another participant used the scratch model to explain how this inflammation progresses or worsens: I’ll say, “Well, the way I like to think about inflammation is what would happen, for example, if I were to take my fingernail, and I were to start scratching the surface of my wrist in the same spot and continue to do that for two hours, what would happen? What would you start seeing on my skin first?” And they might say, “Well, it would get red.” And I go, “Okay, good. So redness would be a first sign of inflammation. And then what would happen?” Well, it would get kind of puffy okay, would get swollen. So then swelling and redness are signs of inflammation. And then what would happen, eventually, if I kept scratching? Well, the skin will start to peel off. Yeah, right, so you start kind of slough some tissue, right? And then what would happen? Well, you might bleed from that area, you would make a sore, right, so you would bleed. So, these are all different stages of inflammation that you kind of created. Well, your body is creating that inflammation on the inside of your intestinal lining, not because you’re scratching it but because your immune system is programmed to behave that way. So, the very immune system that helps us normally fight off infection, in your case, is giving the wrong signals to the lining of your digestive tract and causing this inflammation process to occur. And that’s what’s causing your pain, and cramps, and diarrhea, or bleeding, you know, whatever the case may be. (Participant 09)
Here, we see how this model not only explains inflammation in IBD but also the symptoms a patient may have. It briefly describes the immune system’s function in fighting infection but focuses primarily on the impacts it has on the child’s body. In focusing on the child’s symptoms and grounding the model in experiences the child is familiar with, this participant provides a more tangible explanation for the child’s disease.
Bonfire Model
Two participants described inflammation in IBD as a bonfire that needs to be put out. This model relies on a patient’s ability to picture the bonfire as a metaphor for inflammation. Bonfires provide a parallel to inflammation that is not as directly linked to the patient’s personal bodily experiences as the scratch and scrape model. However, it does suggest heat and injury, which are consistent with the secondary effects of inflammation in the body. I think it makes a lot of sense to picture a bonfire. Everyone’s seen it, across all cultures and nationalities and religions. Everyone can picture that. And I find that it helps really get across the idea of induction therapy versus maintenance therapy. … And so with this idea of bonfire, I talk about how that fire originates. The autoimmune component in genetically susceptible people. … And what our goal is going to be is, using some kind of combination of nutrition and medicines and lifestyle, is we want to put that fire out first, right? But just by the nature of the disease, if we take the lid off the fire, that immune system, just all those contributing factors are still there. And so that fire is going to, unfortunately, start up again. And so, it’s important that we put the fire out, step one. But then step two is trying to come up with an approach to keep the fire out. (Participant 12)
As in the switch model, this model provides a clear link between the patient’s disease and treatment and uses language that suggests “turning off” or “putting out” inflammation or the immune system. Here, the function of treatment is to turn off inflammation—as this participant suggests: “If we take the lid off the fire, that immune system, just all those contributing factors are still there” (Participant 12). Induction therapies, usually steroids, are primarily anti-inflammatory, whereas maintenance therapies for IBD suppress the immune system. Linking treatments to inflammation provides a clear link between the patient’s symptoms and their medications.
Discussion
Participants described a variety of explanatory models used with pediatric IBD patients at the first clinic visit post-colonoscopy. We identified two primary explanatory models used to describe immune dysregulation in pediatric IBD: the defense and protection model, which characterizes the immune system as an army that erroneously sees the body as “non-self” and attacks it; and the switch model, which conceptualizes treatment as activating a switch that turns off a faulty immune response. In both models, participants characterized the immune system as “confused” or “deceived.” Only one participant emphasized the ongoing protective functioning of the immune system in IBD. Others described the immune system as “too strong.” We also identified two models used by some physicians to describe inflammation: the scratch and scrape model, which compares IBD inflammation to inflamed skin, such as abrasions or sores; and the bonfire model, which compares inflammation to a fire in need of extinguishing. By incorporating concepts familiar to children, these models tailor explanatory models to a pediatric audience, which may be helpful for disease understanding (Kirmayer et al., 2004).
Most participants employed the defense and protection model to describe the immune system and its dysfunction in IBD. While a few participants expressed concerns with the use of a violent metaphor with children, it nevertheless dominated. Participants who employed the switch model also used words like “fight” that imply a combat-based model for immune system function. Unlike the defense and protection model, this model specifies a direct function for medications: to turn the “switch” off.
This study contributes to the explanatory models literature by highlighting clinical explanatory models as a promising site of inquiry. Most explanatory models research was conducted in the 1980s and 1990s, and focused primarily on lay understandings of illness. A smaller body of research has highlighted the explanatory models used by clinicians in interactions with patients as critical to understanding the formation of lay concepts of disease and illness (Buchbinder, 2015; Kirmayer et al., 2004). Here, we build on this work to illustrate the explanatory models developed by pediatric providers, who have received much less attention in the literature. Methodologically, we show that interviews with clinicians can yield important information about clinical communication that complements naturalistic observations and audio-recordings.
This study also builds on existing research on clinical metaphor. Our findings reflect a broader use of battle metaphors in medicine. In cancer treatment, these metaphors may increase fatalistic beliefs about disease prevention and may make treatment seem more difficult (Hauser & Schwarz, 2020). However, for some patients, especially those for whom treatment may be curative, battle metaphors can provide a sense of hope and agency against their disease (Wackers & Plug, 2022). Militaristic metaphors were especially prevalent at the beginning of the COVID-19 pandemic, signaling public alarm (Schnepf & Christmann, 2022). However, these metaphors showed limited effectiveness in increasing support for strict COVID-19 policies (Schnepf & Christmann, 2022).
In IBD, unlike in cancer or COVID-19, battle metaphors describe a civil war rather than one against a virus or disease. Although battle metaphors may provide a convenient way to describe the immune system, they may have detrimental impacts on patient self-understanding when the battle is internal. Patients to whom these models are presented may be left wondering whether to cheer on or villainize their bodies. While the consequences of battle metaphors in autoimmune disease have not been established, this study also identified alternative metaphors that may avoid these potential harmful effects.
Clinical Implications
Pediatric IBD patients have significant gaps in disease-related knowledge when they transition to adult care (Abraham & Kahn, 2014; Gray et al., 2015; Sebastian et al., 2012). Evaluating disease-related knowledge has emerged as a topic of interest in pediatric IBD with the development of the IBD-KID2 tool (Vernon-Roberts et al., 2021). Increased disease-related knowledge has been associated with better medication adherence, self-management, and symptomatology for several pediatric chronic conditions (Brada, 2013; Couper et al., 1999; Hughes et al., 1991; Street, 2013).
Explanatory models can enhance disease-related knowledge, which may improve medication adherence (Fishman et al., 2010; Hommel et al., 2013). As Kirmayer et al. (2004) note, effective explanatory models of illness take into account the patient’s background knowledge and are consistent with the treatment plan offered. When accurate and developmentally appropriate, explanatory models can assist pediatric patients in conceptualizing their diseases and the role of their medications. The models described here may be used clinically even with limited knowledge of the immune system and physiological processes.
Assessing whether they enhance patients’ disease-related knowledge may provide a valuable and clinically relevant direction for future research.
While many participants provided explanatory models to understand the main treatments of pediatric IBD—immune-suppressing agents (Guariso & Gasparetto, 2017)—alterations in the microbiome are also thought to be critical to the underlying pathophysiology of IBD. Some families attempt to address this using probiotics and dietary changes (Eindor-Abarbanel et al., 2021). The defense and protection and switch models do not provide a framework with which to understand the use of these treatments. As medical understandings of IBD develop, these explanatory models may evolve as well, perhaps utilizing the microbiome as a common foe that the child and their immune system can combat together.
Limitations
This study has several limitations. All physicians interviewed were from sites that participate in the largest learning health network for pediatric IBD and therefore may be more adept at discussing the issues we asked about. Most participants were from large academic health centers and may not represent the views of specialists practicing in rural or private practices. Additionally, elicited accounts of clinical explanatory models may diverge slightly from the actual language that physicians use in clinical conversations with patients. The data associated with this study can be accessed by reaching out to the corresponding author with reasonable request.
Conclusion
Clinical explanatory models provide patients with a framework with which to understand their disease, including how it affects their bodily functioning and therapeutic options. Understanding clinical explanatory models provides a window onto how patients may view their diseases and identities. Effective clinical explanatory models may enhance disease- and treatment-related knowledge, which may, in turn, improve medication adherence and decrease patient distress. The use of battle metaphors by participants in this study raises questions about the effects of militaristic language when describing autoimmunity, particularly regarding their impact on children’s self-image and self-understanding. Because children’s comprehension of metaphor develops as they age (Deckert et al., 2019), further investigation of how patients understand and internalize clinical explanatory models is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant number T35-DK007386 from the National Institutes of Health.