
Abstract
Recovery narratives are personal stories of health problems and recovery. A systematic review proposed a conceptual framework characterising alcohol misuse recovery narratives, consisting of eight principal dimensions, each with types and subtypes. The current study aims to apply and extend this preliminary conceptual framework. Semi-structured interviews were conducted to collect alcohol misuse recovery narratives from adult participants. A two-stage inductive and deductive thematic analysis approach was used to assess the relevance of the dimensions and types included in the preliminary conceptual framework and identify new components. The sample consisted of 11 participants from diverse socioeconomic backgrounds who had previously displayed varying degrees of alcohol misuse. All conceptual framework dimensions (genre, identity, recovery setting, drinking trajectories, drinking behaviours and traits, stages, spirituality and religion, and recovery experience) were present in the collected narratives. Three dimensions were extended by adding types and subtypes. Whilst the existing conceptual framework fitted the collected narratives, a new dimension describing the alcohol environment was required to fully characterise narratives. Types included in the alcohol environment dimension were policy and practice and social dynamics. The extended framework could guide the production of resources enabling clinicians to engage with narratives shared by their clients.
Keywords
Introduction
In mental health research, recovery narratives have been defined as personal stories presenting internal or external events that occur over time, which describe adversity or struggle and self-defined strength, success, or survival (Llewellyn-Beardsley et al., 2019). They can be presented in a range of forms, including video, audio, prose, and poetry (McGranahan et al., 2019). They are frequently shared with others (Rennick-Egglestone et al., 2019b). The sharing of recovery stories is a phenomenon present across a range of treatment programs for alcohol misuse, such as Alcoholics Anonymous (AA) (Lederman & Menegatos, 2011). For alcohol misuse, recovery can be defined as a period of sustained abstinence from alcohol, improvement in social and employment functioning, and mental and physical health (Witkiewitz et al., 2019). Personal stories have been used by humans to share adversities such as alcohol misuse which can help to reappraise and achieve recovery (Weegmann & Piwowoz-Hjort, 2009). Sharing narratives can motivate personal recovery and open opportunities for working on positive behaviour change by encouraging and supporting oneself and others (Witkiewitz et al., 2019).
Narrative approaches are well-known in healthcare research (Barton, 2008; Haas, 2012; Jordens et al., 2001). A broad range of lived experience narratives have been studied, of which recovery narratives are just a subset. Researchers collect and analyse narratives describing experiences of health and illness, allowing for the intimate, in-depth study of an individual’s experiences over time and in context (Clandinin & Caine, 2013). Recovery narratives have been studied across a range of health concerns and can provide insights into the phenomenology of recovery (Zwerenz et al., 2017).
Repeated studies across a broad range of populations have demonstrated the formation of a recovery narrative can promote mental and physical health in the narrator (Pennebaker & Seagal, 1999). A growing evidence base suggests recovery narratives can be used by healthcare practitioners as an intervention to support patients’ recovery, for example, through the inclusion of recovery-oriented autobiographies in psychotherapeutic practice (Boylstein et al., 2007; Sommer, 2003). Recovery narratives have been used in stroke rehabilitation, where they can help patients to reconstruct their identity and to re-orientate themselves towards the possibility of recovery post-stroke (Boylstein et al., 2007). Representing a similar function, sharing a recovery narrative in an AA session can help an individual reorient their sense of identity towards maintaining sobriety (Lederman & Menegatos, 2011). Sharing narratives can help patients make informed choices on selecting a specific treatment and can improve compliance (Yaskowich & Stam, 2003). Moreover, sharing personal accounts of illness publicly can lead to increased social awareness and reduced stigma both for the narrator and the recipient, can contribute to changes in health policy, and can improve understanding of research (Sharf, 2001).
Recovery-orientated interventions are becoming more popular in drug and alcohol treatment settings (Neale et al., 2015). However, there remains an ongoing debate in contemporary literature concerning the optimal definition of recovery (Best et al., 2016). Some researchers focus on recovery as a relatively objective phenomenon that can be empirically measured across various domains of functioning. Others see recovery as a purely subjective phenomenon that is heterogeneous and reveals underlying idiosyncrasies of the recovery process (Best et al., 2016). Our work is aligned with this latter definition; we have turned to recovery narratives to understand and document these idiosyncrasies and hence to develop a conceptual understanding of their characteristics. In addition, being valuable to alcohol misuse recovery research, a clear understanding of the characteristics of alcohol misuse recovery narratives could optimise their use in clinical practice and maximise their positive impact (Llewellyn-Beardsley et al., 2020).
A conceptual framework describing the characteristics of alcohol misuse recovery narratives has previously been developed through a systematic review and narrative synthesis (Subhani et al., 2022). The review identified a rich source of existing literature describing the characteristics of alcohol recovery narratives. The review synthesised characteristics into eight overarching dimensions, each containing specific types and subtypes. Dimensions identified in the Alcohol Recovery Narratives Conceptual Framework (ARNCF) were genre, identity, recovery setting, drinking trajectories, drinking behaviours and traits, stages, spirituality and religion, and recovery experience. The ARNCF synthesises characteristics identified in analyses of narratives collected from 1055 participants across 32 empirical studies.
The ARNCF was produced with the intention of facilitating the research community to interpret and develop knowledge from alcohol recovery narratives, by introducing concepts, which can be adopted, modified, or challenged. This is in keeping with a tradition of treating conceptual frameworks as legitimate knowledge products in research, for example, as advocated by Blumer (1954) (in relation to conceptualisations of social settings) and Jabareen (2009). A better conceptual understanding of the characteristics of alcohol recovery narratives as a genre can enable the identification of knowledge gaps (e.g. around particular types of narrative) and inform the development of new behavioural interventions making use of narratives. It can also provide a framework to facilitate structured conversations between clinicians and patients to improve behavioural compliance and reduce stigma (Manning, 2006).
The current study aims to apply the ARNCF to a new corpus of alcohol misuse recovery narratives generated through semi-structured interviews. The objectives are (a) to evaluate the fit of the ARNCF to this corpus, (b) to identify candidate extensions, and (c) to explore individual experiences within the sample.
Methods
The study was conducted as part of ‘The Knowledge of Liver Fibrosis Affects Drinking (KLIFAD) feasibility randomised control trial’. Ethical approval was obtained from the West of Scotland Research Ethics Service on 20 January 2021, REC reference: 20/WS/0179. The RCT was prospectively registered (ISRCTN16922410), and the trial protocol was published (Subhani et al., 2021). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
The KLIFAD trial is investigating the feasibility of integrating transient elastography (TE) into community alcohol services to facilitate early diagnosis of liver disease and promote positive change in addictive behaviours (Subhani et al., 2023). Fibrosis is the medical term for the scarring of the liver. TE is a type of ultrasound technology that measures the degree of stiffness in the liver caused by this scarring. Alcohol misuse recovery was defined as ‘a deeply personal, unique process of change, a way of living a satisfying, hopeful and contributing life even with limitations caused by illness [and] a process involving the development of new meaning or purpose in one’s life’. This drew on prior conceptualisations of recovery and recovery narratives developed by mental health researchers (Anthony, 1993; Rennick-Egglestone et al., 2019a).
Participants
Inclusion criteria were as follows: (a) aged 18 years and over, (b) has been diagnosed with alcohol use disorder (AUD) or alcohol-related liver disease (ARLD), (c) self-identifies as ‘recovered’ or ‘being in recovery’ from their condition (as per recovery definition provided above and in supplemental material (S1 Text)), (c) has previously received one or more transient elastographies, (d) able to give informed consent, and (e) willing to be video recorded.
Exclusion criteria were as follows: (a) known to have any other liver disease apart from ARLD and (b) has a primary substance misuse other than alcohol.
Participants were purposively identified for variation in age, gender, ethnicity, and liver stiffness (Coyne, 1997), prioritising variation in liver stiffness as assessed at initial TE. They were recruited through existing patient forums at community alcohol services, by offering information to patients self-presenting to any of the trial treatment settings, and by snowball methods. A maximum variation sample on liver stiffness was sought, covering self-reported TE scores indicating normal, intermediate, and advanced liver stiffness (Benoot et al., 2016). Details of the recruitment process have been reported (Rennick-Egglestone S, 2023).
Procedure
The following variables were collected on case report forms at the start of face-to-face interviews: age, gender, ethnicity, peak alcohol intake, living arrangement, occupation, current drinking status, length of sobriety, and liver stiffness measure (LSM).
Qualitative Semi-Structured Interviews
Qualitative semi-structured interviews were conducted by the lead researcher (MS). Each participant took part in a 30- to 60-minute interview conducted in a clinical setting or at the participant’s usual place of living, as selected by the participant. A topic guide was drafted in consultation with a patient and public involvement (PPI) group consisting of members with personal experience of alcohol misuse and recovery. Following accepted practice in narrative research, the initial part of the topic guide comprised open-ended questions to elicit alcohol recovery narratives, with minimal or no interruption from the researcher so that the narratives produced were presented within the frame of reference of the participant (Llewellyn-Beardsley et al., 2020; Spector-Mersel & Knaifel, 2018). Through this initial question, participants were asked to narrate their alcohol recovery story over time with a beginning, middle, current situation, and future plans (Llewellyn-Beardsley et al., 2020; McAdams, 1993). A sample interview guide is in Table S1. All interviews were video recorded, transcribed, and pseudonymised.
Eleven participants were recruited. Two participants had a history of homelessness; five were unemployed, four were working, and two were retired. One participant had engaged with AA. There were no narratives from people identifying as LGBTQIA2S+.
Analysis
Transcribed interviews were uploaded to NVivo version 12. To maintain anonymity, the name of participants, third parties, institutions, and places were either redacted or replaced with a unique identifier. A two-stage qualitative thematic approach was used (Spector-Mersel & Knaifel, 2018). The initial coding frame was derived from the ARNCF (Subhani et al., 2022). Two researchers (MS and UT) independently coded and analysed the data at the sentence and paragraph levels.
The deductive and inductive analysis consisted of the following steps: (a) organisation of data, (b) obtaining the general sense of narratives, (c) coding of narratives, (d) identifications of themes and subthemes, and (e) data interpretation and compilation of results (Butina, 2015). Through stages d and e, the authors also attended to the contents of coded transcript fragments and used this material to develop narrative descriptions of phenomena relevant to alcohol misuse recovery processes.
Alcohol Recovery Narratives Conceptual Framework (ARNCF).
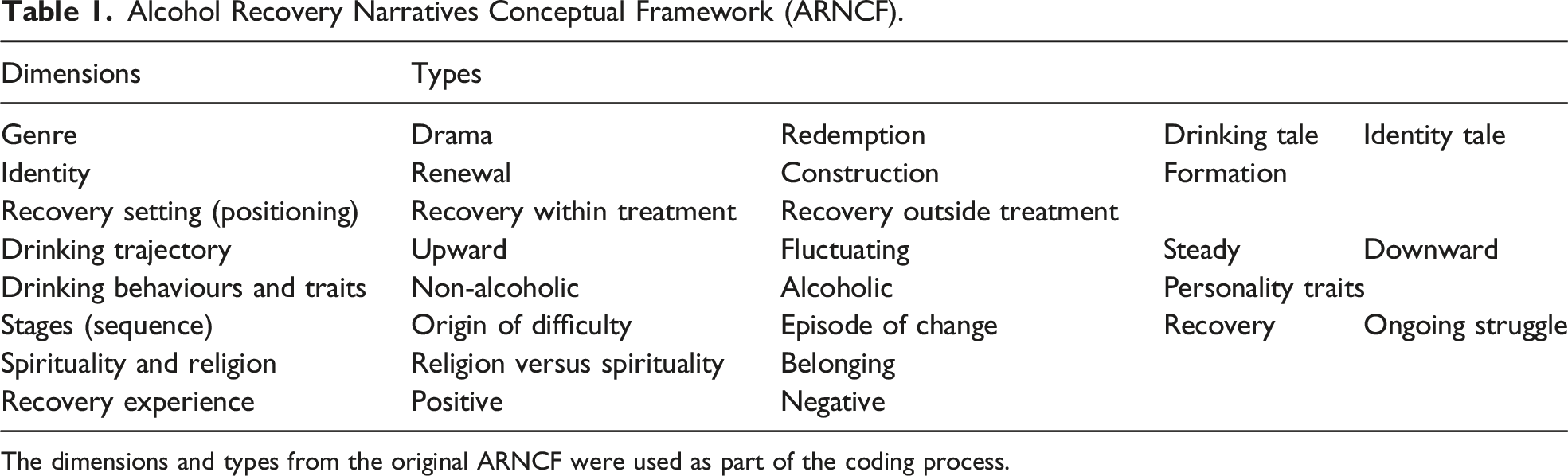
The dimensions and types from the original ARNCF were used as part of the coding process.
In the second stage, the interview material not covered by the existing conceptual framework was inductively categorised into new codes. These codes were later classified as either new dimensions or types, thereby extending the ARNCF. The approach from the original systematic review was adapted to develop a preliminary frame organising new themes. Two authors (MS and UT) identified new themes and produced a preliminary framing presenting these themes. The preliminary framework was reviewed, and relationships between entities in the framework were explored. The agreed new themes were added to the pre-existing ARNCF.
Coder 1 (MS) completed the initial coding, created a duplicate file, and removed code names. Coder 2 (UT) coded this file independently. Coders then discussed the codes to reach an agreement, and any conflicts were resolved through discussion with the senior author (SRE). The process was supervised by two researchers (SRE and HK), including monitoring the transparency of coding and addressing any potential conflict.
Where possible, the language used by participants was preserved while maintaining the clarity of analysis. The overarching CHIME (connectedness, hope, identity, meaning, and empowerment) framework (Best & Lubman, 2012; Slade et al., 2014) was also used.
Examination of Other Characteristics
Sub-group analyses were conducted to explore the impact of specific characteristics, the subgroups were predetermined a priori from the previously published systematic review (Subhani et al., 2022). These were (a) gender, (b) history of homelessness, and (c) presence of mental health problems. The two-stage analysis process was repeated to assess the validity of ARNCF for these different characteristics.
Results
Mean age was 56.0 years (SD 9.9 years), six (54.5%) participants identified as male and five (45.5%) as female. Ten identified as white and one with a minority ethnicity. Median peak alcohol intake was 190 units per week (range 105–300). The length of sobriety ranged from 3 years to over 10 years. The median LSM was 14.3 (range 3.6–27) kilopascal (kPa).
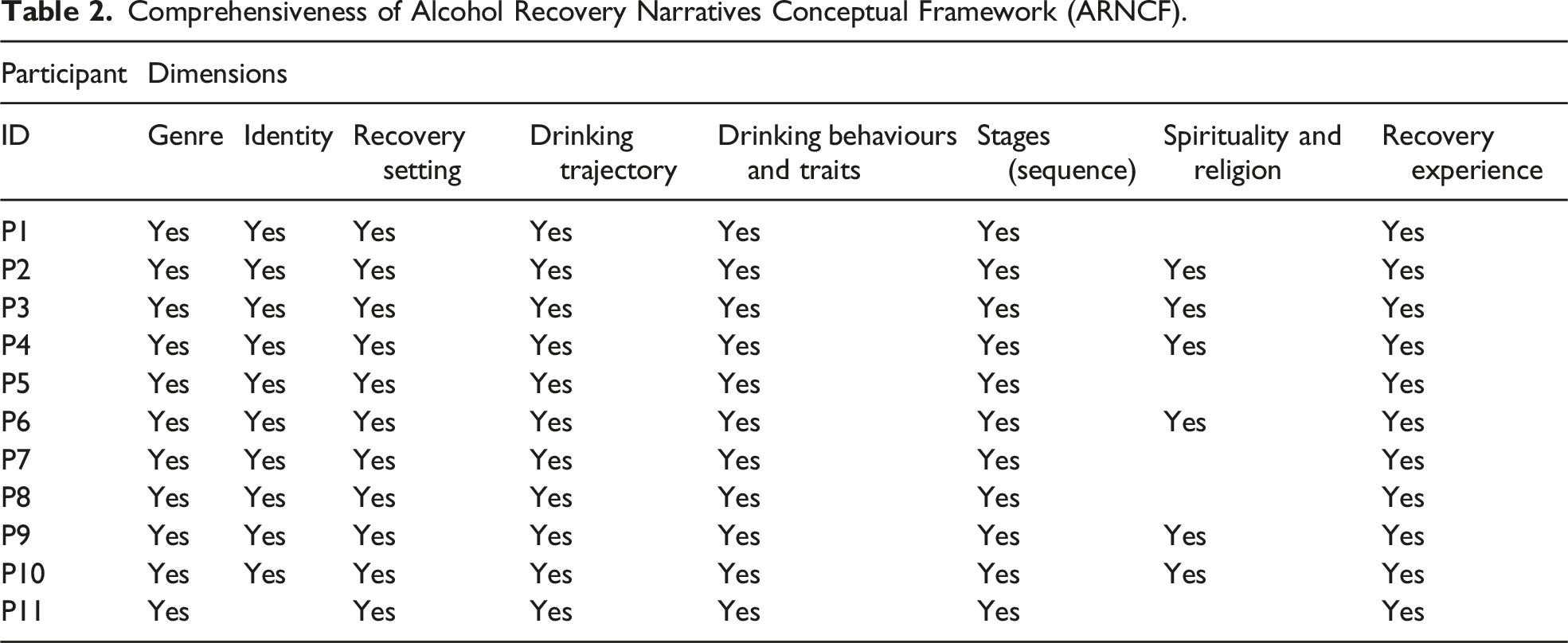
Comprehensiveness of Alcohol Recovery Narratives Conceptual Framework (ARNCF)
Comprehensiveness of Alcohol Recovery Narratives Conceptual Framework (ARNCF).
Dimension 1: Genre
Illustrative Examples for Genre.
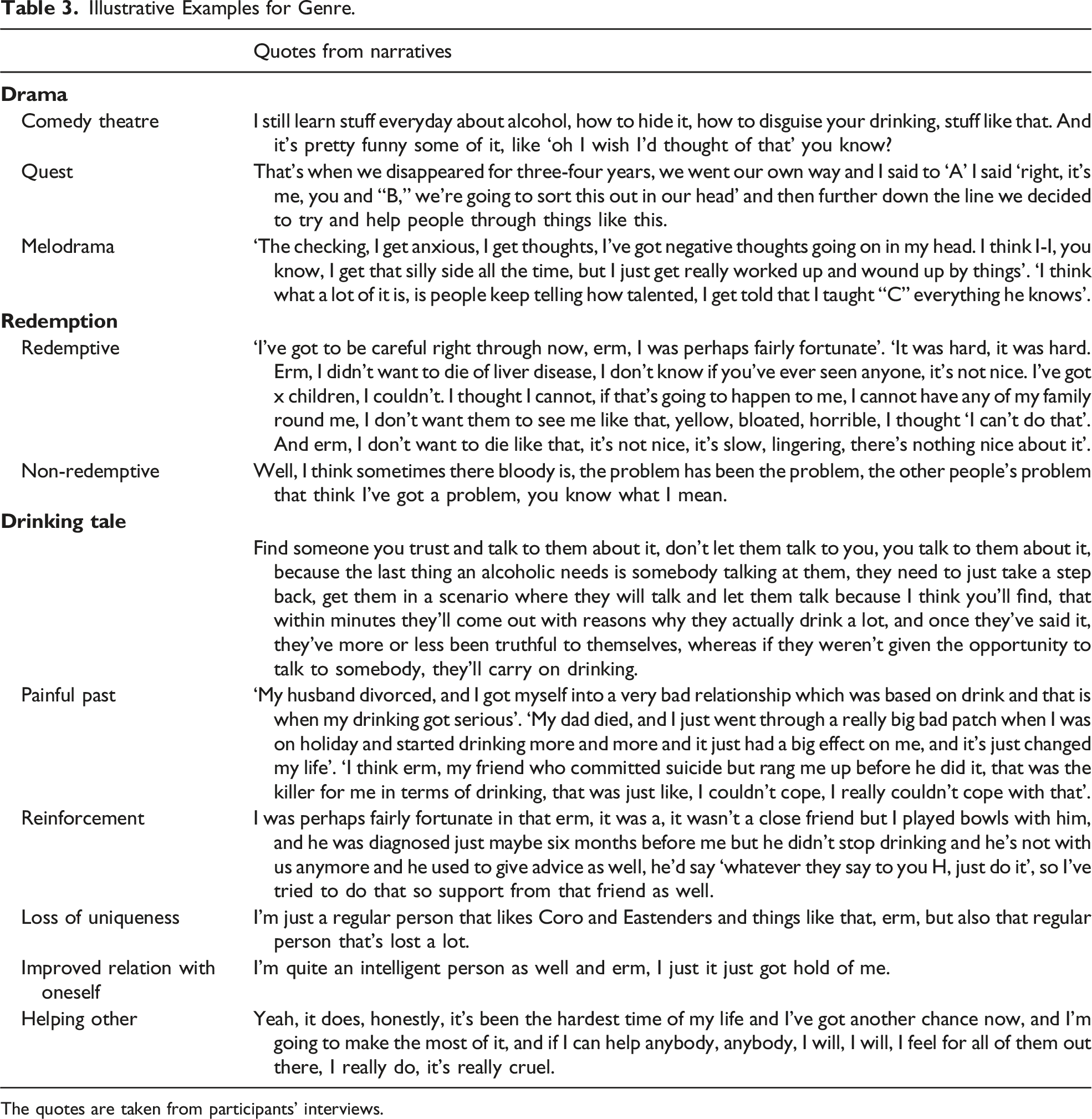
The quotes are taken from participants’ interviews.
Dimension 2: Identity
During their recovery journeys, participants went through different stages of identity transformation including ‘identity renewal’, ‘identity construction’, and ‘identity formation’. Participants shared emotions of guilt, shame, and hitting rock bottom. They went through cognitive restructuring to construct a new identity. I just got to that real rock bottom that somehow, I just managed to stop. (P2) Completely different, yeah, I have acceptance of myself today. I can’t believe, I can’t believe how the difference in myself, of my thinking, of who I am. In fact, even before I started drinking even you know err as a child up to my drinking, I am a different person, yeah. (P2) Those friends that I met, voluntarily we set up an extra group and just people, I still see those people once a week every week now, three years on. (P11)
Eventually, the participants adapted to their new roles and reconstructed their social relationships. The multiple stages of identity transformation involve a shift in perspective that may be sustained through positively reinforcing cues such as social processing of emotions, change in recovery capital, and self-nurturing. This shift in perspective eventually leads to a change from addictive to non-addictive behaviour.
Dimension 3: Recovery Setting
Most of the participants apart from one (P11) had ‘recovery within treatment settings’. The most common institutions participants formally interacted with were community alcohol services, community alcohol detoxification units, primary care substance misuse clinics, Alcoholics Anonymous, mental health services, and secondary care hospitals. The participants described their interaction within treatment settings as positive and supportive towards recovery. I went into that place in ….., and it was good, it was a structured. (P6) I decided to, through the help of my GP and my liver specialist, I sought out a local group and I volunteered myself. (P8)
The participant who achieved ‘recovery outside treatment setting’ (P11) did not like group therapy, due to other group members telling them to stop drinking and change their behaviour. They disagreed with diagnosis labelling and believed that though they were drinking more than recommended, they were still in control. I would read about it, I mean I always read what I could about being an alcoholic and how it creeps up on you and everything and about recovery and the twelve steps and sitting with a group of people saying, ‘I’m an alcoholic’ and I thought it’s not for me, I don’t want that. I actually ended up not saying anything cos I thought well I’m going to have to stop some of these people in order to say, ‘I have a fairly normal life, I just drink too much bloody alcohol and I want help stopping it’, but this isn’t helping me I’m afraid, so that was the end of that. I never had that breakthrough; I could certainly never sit in a group and say, ‘I’m an alcoholic’. (P10)
One person shared their experience of natural recovery, which represented an internal locus of control. The tendency to give control away to agents in the recovery setting may require the building of either trust over time with others or a self-driven attempt to come full circle with one’s addiction. This involves processing shame in some cases.
Dimension 4: Drinking Trajectory
In the drinking trajectory dimension, participants exhibited the ‘upward’, ‘downward’, and ‘fluctuating’ trajectories, whilst the ‘steady’ drinking trajectory type was absent. Nine participants demonstrated a ‘slow’ upward trajectory, whereas two had a ‘sharp’ upward trajectory. Participants alluded to factors, which supplemented different types of trajectories. Specifically, in the context of how ageing relates to drinking habits and the ensuing impact on addiction, participants displayed a tendency to account for their narrated experiences in terms of changes in their social and personal circumstances. This suggests that recovery narratives involve the socioeconomic and highly personalised experience of ageing as a catalyst in piecing together the old identity one revisits, now, in recovery retrospectively. Participants talked about the impact of retirement, change in social responsibilities, and surplus income supplementing increases in alcohol intake, whereas a decline in physical health, enhanced family support, and a change in social capital supported a reduction in alcohol consumption. I’d got my normal money going in, the mortgage being paid, normal things being looked after and then this bonus money, so of course, the amount that I was drinking went up quite steadily. (P7) I’d started to drink a little more heavily I was what now is called an assistant head in a secondary school. (P5)
Dimension 5: Drinking Behaviours and Traits
At the time of interview, seven participants were abstinent, three had significantly reduced alcohol intake, and one participant was drinking in a controlled manner (as defined by UK Department of Health recommendations). In relation to the ARNCF, the following ‘personality traits’ were present: passive, prosocial, anti-social, and dishonest. The grandiose trait was not observed.
In the context of reviewed narratives, ‘prosocial’ and ‘passive’ personality traits supported addictive behaviours. Some participants began drinking due to peer pressure or in the form of companionship drinking, largely to maintain social acceptance. On the other hand, passive traits made participants vulnerable to abuse, exploitation, and manipulative practices by others, particularly where spousal relationships were involved. At the same time, dependence on alcohol promoted dishonesty and anti-social tendencies such as stealing, conflict, lying, and self-harm. I used to be the, go to the pub on the way home from work, five o clock, couple of pints, you know with the mates and that kind of thing. (P1) I took me to a part in a very dangerous, dark time where I was considering taking my own life, laid on tram tracks, stole from shops, stole bottles of wine. (P9)
Dimension 6: Stages (Sequence)
Illustrative Examples for Stages.
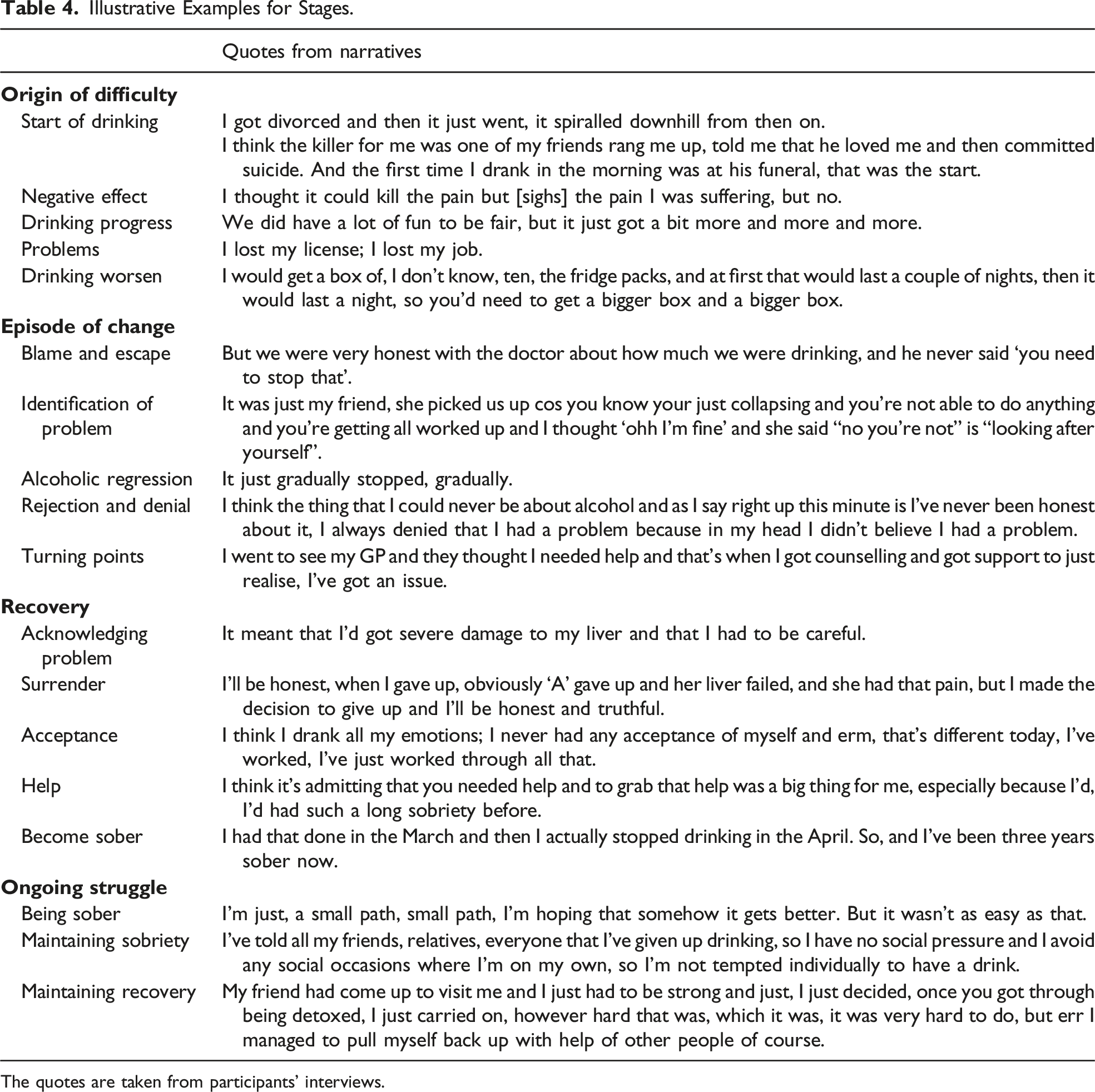
The quotes are taken from participants’ interviews.
Dimension 7: Recovery Experience
Participants had a combination of ‘positive’ and ‘negative’ recovery experiences. The ‘positive’ type was predominant across the narratives. The commonly recurring positive recovery experiences were empowerment, improved relationship and family trust, finding lost opportunities, enjoying new activities, and improved mental health. Participants revised their roles to better reintegrate into local communities and felt happy to be alive. Some described ongoing experiences of wandering thoughts about their painful past, lost friends, and financial burden. Associated physical and mental health comorbidities such as fibromyalgia, anxiety, and depression made life harder.
Dimension 8: Spirituality and Religion
‘Spirituality versus religion’ as a type was not identified in the narratives. Participants did talk about a sense of belonging. ‘Belonging’ as a type represented the adaptive feelings participants exhibited across key events to do with reintegration into society. In the ‘Belonging’ type, participants further shared experiencing ‘lack of belonging’, ‘a search for belonging’, and ‘attaining belonging’.
Variation in Individual Experiences Within the Sample
Gender
Of all included participants, six identified as male and five as female. Those who identified as female were younger with a mean age of 51.2 years (SD +/−3.9) compared to males who had a mean age of 59.9 years (SD +/−10.6). Female participants had consumed a higher quantity of alcohol (units per week) at peak compared to males (mean 236.0, SD +/−55.9 vs 164.1, SD +/− 36.6). Female participants had higher liver stiffness measures (mean 15.2 kPa, SD +/− 8.6 vs 10.7 kPa, SD +/− 5.3). Some female narrators acknowledged the impact of harmful relationships with men as a trigger for alcohol misuse. Some female narrators described drinking behind closed doors to avoid social stigma and shame. Like most of my problems in my life have been bad choices in men. I don’t really have much to do with men anymore. (Female) I was never, I was a drinker behind closed doors, I was never a pub drinker or going out. I always used to do it in secret. (Female) I thought all the things I knew that I shouldn’t be thinking I just thought I could just control it and, and I couldn’t. I think a lot of shame around that as well. (Female)
Homelessness and Alcohol Recovery
Two participants had personal experiences of homelessness. They had a shared history of a painful past. Both lacked a sense of belonging, making them vulnerable to addictive and anti-social behaviours. I’ve been taken to hospital that many times, I’ve been arrested that many times, erm, I’d been in fights, I’d had black eyes, I was, I’ve been sectioned. It took me to a part in a very dangerous, dark time where I was considering taking my own life, erm, tried numerous occasions, laid on tram tracks, stole from shops, stole bottles of wine, and obviously when I was homeless. (P3)
For both, recovery was only made possible within a treatment setting by a multiagency integrated healthcare approach involving mental health, community alcohol, and social care services. As part of their recovery, these participants went through a significant identity shift from a non-functional person to a more functional and integrated member of society. Therefore, they found the path to recovery was hard but achievable within a holistic multidisciplinary framework. I had that many fallbacks when I went through this process, it’s not easy, I’m not going to say it’s easy, nobody who has ever been in my position will ever say it’s easy, cos it’s not, it’s not. (P4)
Alcohol and Mental Health
Alcohol misuse and mental health problems were common themes across all the narratives. The analysis confirmed participants’ experienced low personal self-esteem, cognitive dissonance, and lack of love from others and a sense of belonging, denial, rejection, and shame. Poor mental health could be the cause or consequence of alcohol addiction. I was very anxious, very anxious. I think on the outside I always looked confident, so I always had that anxiety and fear and I always used to. I think what it did looking back, it gave me confidence that I never had to be, you know, to be in those, I think socially I was quite awkward as well, so it gave me that ability to be more confident, yeah. (P2)
Participants frequently perceived alcohol as a medication to numb physical or psychological pain, suppress anxiety, and look more confident by suppressing internal conflict and insecurity. I just feel what happened to me could really happen to anybody. It’s that alcohol is the best painkiller, is the best reliever of stress and anxiety that’s out there. (P3)
Common mental health problems reported by participants were anxiety, depression, post-traumatic stress disorder (often associated with childhood trauma or abusive relationships), obsessive–compulsive disorder (OCD), anti-social behaviours, lack of self-confidence, emotional instability, feeling on edge, and suicidal thoughts. Affective disorders were the most prevalent, and these disorders influenced participants’ construal of inter-personal reality driving and acted as a driver for alcohol addiction. Although participants narrated that input from mental health services was useful both in obtaining and maintaining recovery, they were put off by long waiting times and felt let down by the system. They promised from a personal point of view, they said, ‘you get clean and stay sober for say 6 months, we’ll give you’ and I have this in writing actually, he gave me therapy/counselling that I need, and he said, ‘and you will have earned it’. Erm so I’m sober nearly three years and I’m still waiting, yeah, still waiting, so yeah, the system, I feel let down a bit by the system. (P11)
Refinement of Alcohol Recovery Narratives Conceptual Framework (ARNCF)
Refinement of Alcohol Recovery Narratives Conceptual Framework.
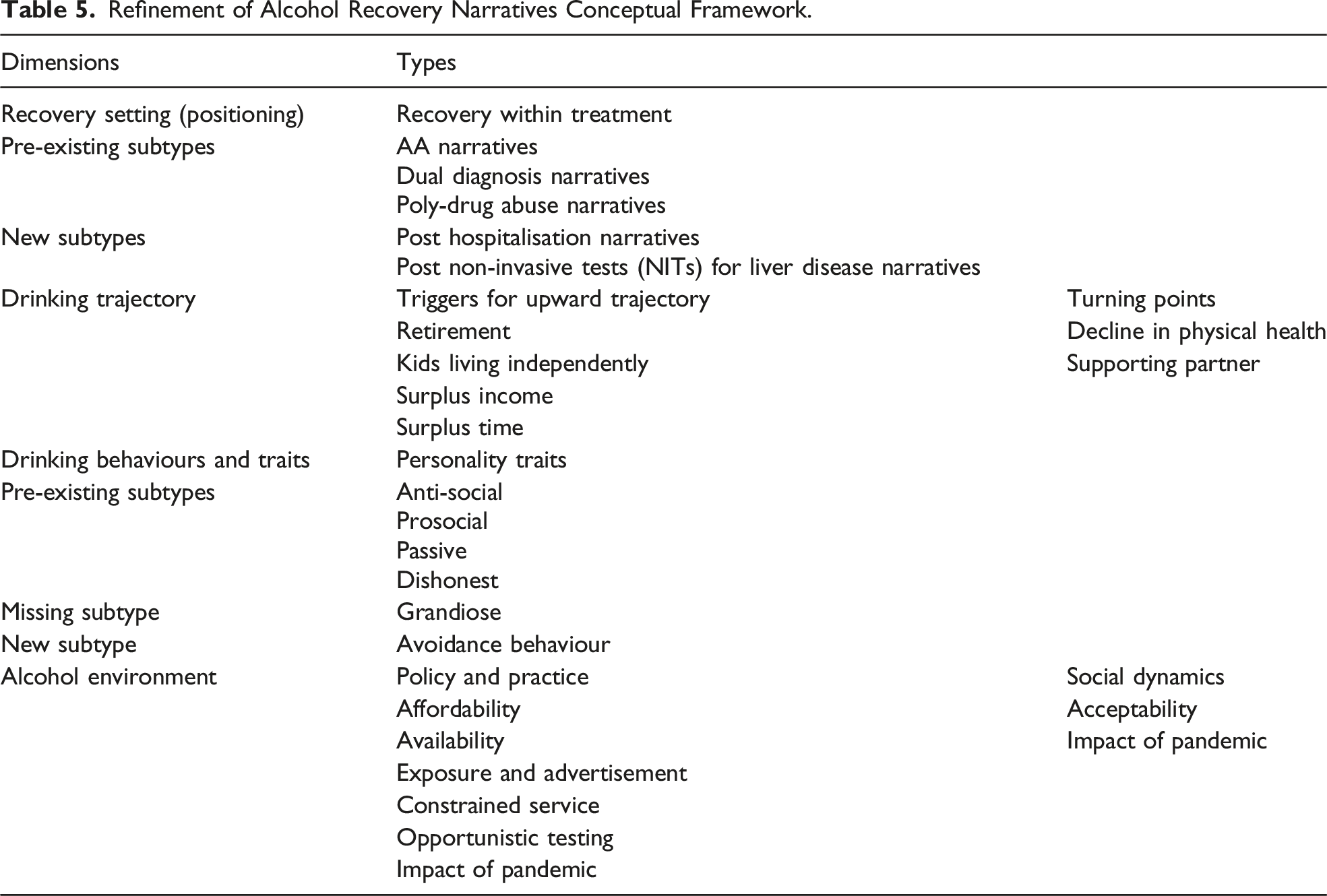
The ‘recovery settings’ dimension originally represented the mode of recovery either within or out of formal treatment settings (former termed ‘natural recovery’). In the type ‘recovery within treatment settings’, there were initially three subtypes. Two further subtypes were identified: ‘post hospitalisation narratives’ and ‘post-non-invasive tests (NITs) for liver disease narratives. Hospitalisation and interaction with medical healthcare providers facilitated recovery. You know I’m lying in that hospital bed in the liver unit absolutely scared stiff and I didn’t know why apart from reading the thing ‘liver unit’. So, during that night, it was praying and also realism and truth, I was there in bed that night and I was facing truth. My consultant, I said to him I said ‘what is it? What else can I do to get my liver better?’ he says, ‘you’re okay, well you’re not okay but’ he says, ‘because you’ve taken the problem away from your liver, you should be okay. (P3)
Moreover, additional non-invasive tests for liver disease conducted in primary or secondary care supported change in high-risk drinking behaviour. Participants indicated that knowledge of liver disease obtained through NITs supplemented a change in their drinking behaviour. In certain cases, participants preferred to have follow-up tests to see the progress they had made. Positive changes (e.g. lower scores at subsequent tests) induced feelings of reward, and lower stiffness scores were reassuring. So started at 27, 29, 27, the next time I went back it was 24, that was six months later. Six months later 19, so there’s my motivation again ‘ohh it’s working, not drinking, my liver’s getting better, it’s getting softer. (P8) I think it would have knocked me more the other way if it had been bad, definitely, because I knew what I was doing, even though I couldn’t stop. I think it, yes it would of, it would have had a different impact on me. (P1)
The ‘drinking trajectory’ dimension describes the impact of ageing on drinking but lacks the detail of the associated changes in socioeconomic circumstances. We observed that during the process of ageing, the following factors acted as a trigger to increase alcohol consumption: retirement, children transitioning to live independently, and having surplus income and time. However, a decline in physical health and a supportive partner acted as a turning point. But eventually erm after I retired, I got depressed, I had nothing to do, it was horrible, and of course, you’re thinking about drinking. (P5) I’d got my normal money going in, mortgage being paid, normal things being looked after and then this bonus money, so of course, the amount that I was drinking went up quite steadily. (P7)
The ‘drinking behaviour and traits’ as a dimension represented antecedents or consequences of alcohol misuse. We identified a new subtype which we have labelled ‘avoidance behaviour’ related to alcohol misuse. Participants possessing this trait found it difficult to manage others and found alcohol as a way to escape their responsibilities. I knew it right from being a child that I couldn’t control other people, and I didn’t want to control other people, so internally I had a big conflict that each time I moved on I felt like I was moving away from the bit that I liked. (P7)
The current study provides information on ‘homelessness and alcohol misuse’, which hitherto remains absent in the previously proposed framework. For these participants, their recovery was only possible by an integrated multiagency approach due to the complexity of associated social and mental health issues.
New Dimension
‘Alcohol environment’ as a dimension comprises the following types: ‘policy and practice’ and ‘social dynamics’. The policy and practice iteratively inform each other wherein the former relates to the generation of ideas followed by the latter, which typically covers implementation concerns. Here, it describes the impact of alcohol-related policies on addictive behaviours and subsequent recovery. Social dynamics as a type indicates the impact of change in social practice over time. Following subtypes were found: affordability, acceptability, availability, exposure and advertisement, constrained services, pandemic, and role of opportunistic testing for early detection of liver disease in populations at risk.
‘Affordability’ describes the buying capacity of a person to buy alcohol. One can consume more alcohol if purchasing power is increased or otherwise can turn to cheap alternatives if purchasing power decreases. ‘Acceptability’ describes the social acceptance of different drinking behaviours; specifically, our participants found that certain factors within a culture supported detrimental levels of alcohol consumption to the extent that was experienced as a normal behaviour validated by others. ‘Availability’ describes the ease of access to alcohol. Our participants narrated that over the years, alcohol has become easier to access due to policies such as changes in supermarket alcohol licensing and seasonal deals, allowing alcohol sales outside pubs with extended hours of business, and the adjacent propensity of drinking at home. ‘Exposure and advertisement’ describe how alcohol has been promoted through multimedia, at times ambiguously labelled or often lacking details concerning the harmful impact of alcohol on health. ‘Constrained services’ describes the pressure on health services to deal with alcohol misuse and associated mental health problems in a timely manner, which can result in reduced trust among service users. The ‘pandemic’ describes the impact of the coronavirus outbreak and imposed social restrictions on drinking behaviours. Participants described their alcohol consumption as increasing during the pandemic. ‘Early detection of liver disease’ describes the impact of having non-invasive tests (NITs) of liver disease and knowing the results. Participants narrated that knowing the results of transient elastography supported them to change addictive behaviour. The illustrative examples for ‘alcohol environment’ as a dimension are given in Table S2.
Discussion
All conceptual dimensions were present in collected narratives, with three of these dimensions extended by adding types and subtypes. A new dimension ‘alcohol environment’ was added to the framework, and this functions to discern and identify broader policy level as well as nested individual level factors driving various patterns of alcohol misuse. During their recovery, participants went through cognitive restructuring to build a new identity. Most participants described recovery as a non-linear process comprising multiple interactions with health services, relapses, and struggles before eventually identifying as recovered or in recovery.
The triggers for alcohol misuse were diverse and included companionship drinking, occupational stressors, psychological trauma such as childhood abuse or toxic relationships, loss, grief due to the death of a family member or friend, mental health issues, and having surplus income or time. In addition, we identified avoidance behaviour as a strong trigger for alcohol misuse, whereas common turning points were seeking help, having a near-death experience, being informed of having liver disease, changing from negative to positive social connections, self-realisation, and observing others having physical diseases due to alcohol. The co-existing mental health issues were a recurring theme. Anxiety, depression, post-traumatic stress disorder (PTSD), emotional instability, OCD, and anti-social behaviour were commonly reported mental health problems.
Implications for the ARNCF
The refined framework enhances the understanding of recovery from AUD and poses implications for policy, healthcare practice, and research. Multiple dimensions and types were present across the narratives. The findings demonstrated that recovery from alcohol misuse followed a non-linear path and often required a multiagency approach. This supports the evidence from the original systematic review stating that there are multiple constituent dimensions with associated types and subtypes of alcohol recovery narratives (Subhani et al., 2022). It highlights the need for an integrated healthcare model to effectively mitigate rising alcohol-related harm (Christian & Gilvarry, 1999; Seeling, 2001). It provides more evidence on the importance of regulatory and statutory enforcement policies such as alcohol minimum unit pricing (MUP) at population level to effectively mitigate alcohol-related harm.
The extended ARNCF describes the characteristics of recovery narratives. Future work should explore the application of the framework in larger and more diverse samples to examine any gaps. Recovery narratives have been used to promote and encourage engagement with health services (McGranahan et al., 2019) where they might be used to extend clinical practice. In particular, narratives are a resource for people who are finding recovery challenging (Roe et al., 2020). It can be used to develop material, which supports clinicians in comprehending the subtleties of the recovery journey described by patients during consultations, enhancing the clinician–patient relationship and opening communication channels. In turn, this might enable clinicians to make the most effective choices about treatment, by considering the complex influences sustaining alcohol misuse. The framework can provide structure for future research, policymaking, and the development of personalised interventions for alcohol misuse.
People with drug and alcohol use disorders often suffer from social stigma and stereotyping, and this could be due to inadequate knowledge and awareness and negative attitudes towards patients with AUD (Probst et al., 2015). There is an urgent need for a reference shift away from negative attitudes towards addiction both within the community and among healthcare professionals. In this context, the alcohol recovery narratives can be used to educate the public and healthcare providers to facilitate this reference shift.
Context and Potential Applications
The notion of narrative psychology can contribute to better understanding of recovery. Sabrin (1986) drew attention to narrative psychology as ‘storied nature of human conduct’, discussing how humans use stories to create meaning and share life experiences. The act of sharing alcohol narratives has been an important component of the AA 12-step programme (Lederman & Menegatos, 2011). In part, the sharing of narratives is important because this method provides the context of personal recovery from addiction, opening opportunity for recognising and working on behaviours in a group setting.
In 2021, there were over 274,000 homeless people in England (Public-Health-England, 2021). This could be a cause or consequence of addictive behaviours (Martijn & Sharpe, 2006). Dame Carol Black’s (2020) independent review concerning illicit drug prevention, treatment, and recovery reported almost a quarter of people engaging with drug and alcohol services have severe housing problems, often associated with higher morbidity (Black, 2020). The current study provides insight into the recovery dynamics of people with a history of homelessness; specifically, the cases suggest increased vulnerability to addictive behaviours and chances of recovery are higher in structured recovery programmes.
The dual diagnosis of AUD and a mental health disorder is a recurring theme and is often related to poor outcomes (Buckley, 2006). The chronic underfunding of drug and alcohol services in the United Kingdom and the lack of provision of integrated healthcare services including mental health services have contributed to a soaring number of alcohol-related harm. A recent audit of drug and alcohol services in Scotland in 2020 showed funding cuts were related to increased drug-related deaths specifically among people from lower socioeconomic backgrounds (McPhee & Sheridan, 2020). Pathological avoidance behaviour can also induce a variety of mental health problems such as anxiety, depression, and PTSD, and the management involves the removal of trigger sources and cognitive restructuring (Treanor & Barry, 2017). Actively addressing mental issues at both policy and practice levels promote longevity of sobriety (Burman, 1997).
Strengths and Limitations
A pre-existing robust two-stage methodology was adapted (Llewellyn-Beardsley et al., 2020). Participants had diverse socioeconomic characteristics, with a diverse history of homelessness, unemployment, severity of alcohol use disorder, and liver disease stage. The current study suggests developing a conceptual framework can facilitate understanding of narratives and their characteristics in relation to alcohol recovery. Another strength of this study was the collection of data on alcohol consumption and liver stiffness to contextualise narrative information. Future larger studies may wish to examine group differences quantitatively based on these scores.
A limitation of this study is the lack of ethnic diversity which may limit generalisation of results. Our sample was recruited through alcohol treatment services in England, and the majority of people who come into contact with English alcohol and healthcare services identify with a white ethnicity (Subhani et al., 2021). Minority ethnic groups have been identified as disadvantaged in accessing drug and alcohol services (Bayley & Hurcombe, 2010). Future studies should use different methods such as community partners and advocates to include a more diverse sample of people. Further, the current study only recruited participants from the United Kingdom, interviews were conducted in the English language, and none of the included narrators identified as LGBTQIA2S+. The mean age was 56 years which could have an impact on descriptions of drinking trajectory. In this respect, a pool of younger participants may provide novel drinking trajectories and corresponding behaviours.
‘Religion versus spirituality’ as a type was not identified from these interviews. This may have been due to the under-representation of narratives from participants who experienced recovery within an AA setting. In this sense, spirituality and religion may have been a catalyst to recovery in the AA model (Subhani et al., 2022). Participants did share experiences of belonging. Due to distinct and divergent behaviours across the cases with regard to sense of belonging, there is potential for further exploration to determine any dimensionality in this regard.
Conclusion
The study applied the preliminary ARNCF to a new sample of recovery narratives and confirmed these narratives are composed of multiple dimensions each with distinct types and subtypes. The findings demonstrate that recovery from alcohol follows a non-linear path and is often achieved through interactions with multiple services. Consequently, the study highlights the need for an integrated healthcare model involving a multiagency approach to effectively mitigate rising alcohol-related harm, holistically. The validated ARNCF can provide an enhanced approach to inform narrative-based research, policy, practice, and intervention development in the field of drug and alcohol addiction.
Supplemental Material
Supplemental Material - Application and Extension of the Alcohol Recovery Narratives Conceptual Framework
Supplemental Material for Application and Extension of the Alcohol Recovery Narratives Conceptual Framework by Mohsan Subhani, Usman Talat, Holly Knight, Joanne R. Morling, Katy A. Jones, Guruprasad P. Aithal, Stephen D. Ryder and Stefan Rennick-Egglestone in Qualitative Health Research
Footnotes
Acknowledgments
We would like to thank KLIFAD patient and participants involvement (PPI) group for their support and the participants who came forward to share their lived experience.
Authors Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by MS, UT, and SRE. The first draft of the manuscript was written by MS, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health and Care Research (NIHR) under its Research for Patient Benefit (RfPB) Programme [grant number: NIHR201146].
Ethical Approval
Work presented in this paper was supported through a favourable ethical review from West of Scotland Research Ethics Service on 20 January 2021 [REC reference: 20/WS/0179].
Clinical Trail Registration
The RCT was prospectively registered (ISRCTN16922410).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.