
Abstract
Although there is evidence of both clinical and personal recovery from distressing voices, the process of recovery over time is unclear. Narrative inquiry was used to investigate 11 voice-hearers’ lived experience of recovery. After a period of despair/exhaustion, two recovery typologies emerged: (a) turning toward/empowerment, which involved developing a normalized account of voices, building voice-specific skills, integration of voices into daily life, and a transformation of identity, and (b) turning away/protective hibernation, which involved harnessing all available resources to survive the experience, with the importance of medication in recovery being emphasized. Results indicated the importance of services being sensitive and responsive to a person’s recovery style at any given time and their readiness for change. Coming to hold a normalized account of voice-hearing and the self and witnessing of preferred narratives by others were essential in the more robust turning toward recovery typology.
Keywords
Voice-hearing, referred to in the clinical literature as having auditory hallucinations, is commonly experienced in the context of schizophrenia and other psychological disorders, as well as in the general population (Beavan, Read, & Cartwright, 2011; Choong, Hunter, & Woodruff, 2007; Waters, 2010). The experience is highly stigmatized and associated with poor mental health, distress, and isolation (American Psychiatric Association [APA], 2000; Thornicroft, 2006). The predominant approach to treating distressing voices in the context of a psychiatric diagnosis is defined by the medical model, which aims to eliminate symptoms, primarily by administration of antipsychotic medication (Drake, Bond, & Essock, 2009; Read, Bentall, & Fosse, 2009). The definition of recovery varies between dominant medical model discourse versus consumer/survivor discourse, with the former focusing on symptom resolution and a return to a former state of functioning (clinical recovery), whereas the latter emphasizes living a “fulfilling and satisfying life, in the presence or absence of symptoms” (personal recovery; Carlton & Bradstreet, 2006, p. 16; Bellack, 2006; Slade et al., 2012). The medical model approach has been criticized for a narrow definition of recovery and pessimism regarding prognosis (Breeding, 2008; Fleming & Martin, 2011; Read et al., 2009). General population surveys indicate that a proportion of people who hear voices are not negatively affected by them (Beavan & Read, 2007; Johns & Van Os, 2001; Tien, 1991). Thus, hearing voices in and of itself does not necessarily cause distress (Peters, Williams, Cooke, & Kuipers, 2012). In addition, a substantial proportion of people who experience distressing voices functionally recover to a degree which would be considered “normal” by most people, with approximately 50% meeting criteria for clinical recovery over a 20-year period (Harding, Brooks, Ashikaga, Strauss, & Breier, 1987; Harrison et al., 2001; Slade, Amering, & Oades, 2008).
In contrast to clinical recovery, which has quite clear criteria, personal recovery is a deeply personal process and its definition varies from person to person (Brown, 2008). It is possible, however, to identify common threads in recovery processes and identify factors that support well-being (Brown, 2008). Recovery in this broader sense involves developing or regaining a positive sense of self, agency, hope, meaningful occupation, making sense of or reframing experiences, accepting the limitations associated with the illness and creating a satisfying life within those limitations, and improved quality of life (Andresen, Oades, & Caputi, 2003; Leamy, Bird, Le Boutillier, Williams, & Slade, 2011; Perkins & Slade, 2012). Others emphasize having the same work and living opportunities as other community members (Kirkpatrick & Byrne, 2009). A pivotal tenet of recovery-orientated approaches is that recovery is possible (Anthony, 1993, 2000; White, 2005). Influenced by consumer/survivor groups, interest in recovery-orientated mental health services and treatment has grown over the past 20 years (Anthony, 2000).
One of the most prominent strands of the consumer/recovery movement has been the hearing voices movement. This was born out of collaboration between consumers, clinicians, and researchers (e.g., Romme & Escher, 1989; Romme, Escher, Dillon, Corstens, & Morris, 2009), leading to establishment of extensive national and state networks which facilitate the running of peer-support hearing voices groups (HVGs) and promote connection between voice-hearers, referred to collectively as the Hearing Voices Network (HVN; Corstens, Longden, McCarthy-Jones, Waddingham, & Thomas, 2014). Principles adopted within the HVN align with both consumer definitions of recovery and the need for a more holistic treatment model which normalizes voices and takes into account contextual factors (Fischer, 2003). Distressing voices are understood as a manifestation of solvable emotional problems which may present in a figurative or literal manner (McCarthy-Jones & Longden, 2013). Derived from personal accounts of voice-hearing discussed at the first major voice-hearer congress in 1987, M. Romme and Escher (1989, 1993) proposed three phases of recovery: startling, which involves initial feelings of shock and being overwhelmed by voice-hearing experiences and trying to push voices away, organization, whereby the person starts to use some strategies in relation to their voices and place boundaries around their interactions and stabilization, wherein the hearer comes to integrate voices into their life, recognize them as “part of me” and no longer wishes to be rid of them.
Although evidence to date indicates that recovery from distressing voices—both clinical and personal—is possible, there is a lack of research into the recovery process in relation to hearing voices. Although many first-person accounts of recovery exist and are valuable in and of themselves (e.g., Romme & Escher, 1993), they were not generated using a qualitative method that allows for analysis of narrative genres or typologies of recovery over time. It is therefore unclear whether recovery processes align with the HVN approach. In addition, diagnoses and stage of recovery were not confirmed. This article addresses this gap in the literature, using Narrative Inquiry to examine recovery and including quantitative and diagnostic measures.
Method
Narrative analysis is the analysis of text, in this case interview transcripts, in “storied” form (Riessman, 2005). A narrative text involves the telling of a sequence of events, which, in the act of narrating are organized by the narrator. The narrator interprets the text, selecting information to include, how to describe it, and how various elements are connected (Riessman, 2005). Therefore, narrative analysis focuses on the narrator’s construction of meaning: in other words, not only what happened but how they understand or make sense of these events. It privileges knowledge gained from personal experience as opposed to master narratives or dominant discourse surrounding a given topic. The notion that meaning is partly or entirely socially constructed is implicit in the philosophical underpinnings of narrative analysis. It acknowledges the role of the researcher in the process of meaning making. Researchers must organize information generated from narrative interviews and interpret it (Riessman, 2005). Research output represents how the researcher has made sense of how the participant has made sense of their experiences. Taking an objective stance is not considered possible; instead, the researcher is required to be aware of and reflect on their subjective response to the research context, process, and content (Braun & Clarke, 2008; Hall et al., 2009, 2011; Oke, 2008). The first author, who undertook interviews, collection of questionnaire data, and lead data analysis, was aware of their tendency to understand voice-hearing as meaningful in context of a person’s life history, and expectation that active engagement and making sense of voices would be involved in recovery. Bracketing these assumptions during the research process allowed information which was not in keeping with expectations to be reflected on and acknowledged, rather than obscured (Fischer, 2009; Tufford & Newman, 2012). The first author had no formal or informal role in the HVN.
In keeping with trends in psychosis research (Schrader, 2013) and because of the advantages it affords, a single complaint approach was used (Bentall, 2003), examining voice-hearing rather than broader diagnostic constructs. However, it is important to confirm whether or not participants met criteria for a diagnosis during their lifetime. This allows comparison with research utilizing diagnostic constructs and also confirms that recovery has occurred from a clinically significant degree of distress. In addition to semistructured interviews regarding recovery over time, participants completed the Diagnostic Interview for Psychoses (DIP; Castle et al., 2006) to ascertain whether diagnostic criteria were met during the person’s lifetime. To comprehensively characterize individuals’ stage of recovery, measures of stage of recovery, distress, and quality of life were also obtained. The authors did not have access to participants’ medical records or diagnostic information. Participants were actively involved in the generation of narrative summaries and narratives were member-checked. Finally, an expert panel was involved in refining typologies of recovery over time.
Participants
Of the total 11 participants (7 women), 6 were recruited from the Hearing Voices Network NSW (HVNNSW) and 5 from the Australian Schizophrenia Research Bank (ASRB). The mean age of the sample was 47 years (SD = 12.6; range = 23–63), with 10 White and 1 Asian participant. Five were engaged in paid employment, 1 in full-time tertiary study, 3 were retired, and 2 received a Disability Support Pension. Three participants were married or in de facto relationships, 1 was divorced, and the remainder were single. The aim was to gain depth rather than breadth of understanding. The small number of participants was therefore considered sufficient.
Materials
Self-report measures
The Stages of Recovery Instrument (STORI; Andresen, Caputi, & Oades, 2006) is a 50-item self-report measure designed to identify a person’s stage of recovery from serious mental illness based on consumer accounts: (a) Moratorium, (b) Awareness, (c) Preparation, (d) Rebuilding, and (e) Growth. It taps into a process of change across four domains known to change during the process of recovery (hope, identity, meaning, and responsibility). The Manchester Short Assessment of Quality of Life (MANSA; Priebe, Huxley, Knight, & Evans, 1999) is a self-report measure of subjective quality of life which assesses satisfaction with various domains, including friendships, finances, leisure activities, safety, and health (both physical and mental). The Kessler Psychological Distress Scale (K10; Kessler et al., 2002) is a 10-item self-report measure of global psychological distress based on items concerning depression and anxiety symptoms over 4 weeks prior to assessment.
Diagnostic interview
The DIP (Castle et al., 2006) is a semistructured interview used to generate Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) and International Classification of Diseases (10th ed.; ICD-10; WHO, 1992) diagnoses for research purposes. Items are linked to a computerized algorithm which produces a likely diagnosis based on factor analysis, with certain items loading onto a particular diagnosis.
Semistructured interview
A semistructured interview was conducted with a view to eliciting information about participants’ experiences of voice-hearing and recovery over time. A time line was used to indicate when voices first started, when they were at their worst and how participants progressed from that point toward recovery. Open-ended questions were asked with counseling skills used to elicit further information regarding participants’ experiences.
Procedure
Ethical approval for the research was obtained from the University of Sydney Human Ethics Committee. This research was advertised through the HVNNSW and ASRB. Reimbursement was offered for travel expenses and time spent taking part. Interested participants contacted the researcher and the Participant Information Sheet was provided. Informed consent was obtained from all participants in writing. Inclusion criteria were (a) current or historical experience of distressing voices, (b) self-identified as recovered or recovering, and (c) adequate English language skills. People experiencing acute levels of distress were excluded. Degree of distress was initially determined by the first author through discussing what the research involved with potential participants. Participants were advised that interviews would involve talking about when voices were at their worst and that this could cause distress. As a result of this process, one potential participant decided not to take part. Interviews were conducted at a mental health center in Sydney where triage and mental health crisis intervention was available if required. Participants’ level of distress was noted at the end of the interview and the number for a mental health referral service provided. Interviews took between 60 and 90 minutes, with breaks as required.
Lifetime diagnosis was derived either by administering the DIP or by obtaining DIP data held on the ASRB databank. All participants completed the self-report measures. These data provided triangulation regarding recovery.
Semistructured interviews concerning participants’ recovery over time were conducted and audio-recorded. Interviews were transcribed and narratives of recovery over time generated by the first author. In generating narratives, information from interviews was reordered temporally, with attention given to how participants made sense of their experiences over time (Howie, 2010). Participants were given pseudonyms and identifying details removed or in one case changed to protect participants’ confidentiality. Narratives were sent to participants for member-checking to ensure that they were an authentic and accurate representation of their experiences. Information gleaned from interviews was used to inform subsequent interview questions (Clandinin & Connelley, 2000).
In contrast to methods which involve identifying extracting themes from data across participants, narrative analysis ensures that each participant’s experiences are kept intact, considered within the context of their lives over time. In addition to this, it allows for identification of typologies or types of recovery story. A preliminary model of recovery over time and typologies (types of recovery over time) were generated. A panel of four consultants who were experts by profession (academic research into voice-hearing, clinical work) and/or experience (V.B., N.T., D.L., and S.M.-J.) were asked to read the narratives and critique this model, providing feedback and suggestions for improvement. The model was revised incorporating four main critiques: (a) the need to exercise caution in producing models of recovery which suggest linear progression not in keeping with reality and the danger of clinicians applying such models in a prescriptive manner; (b) inclusion of disconnection from others; (c) noting factors which inhibited as well as encouraged recovery; and (d) checking the data to confirm the identified period of exhaustion/despair as well as proximal and distal stressors.
Results
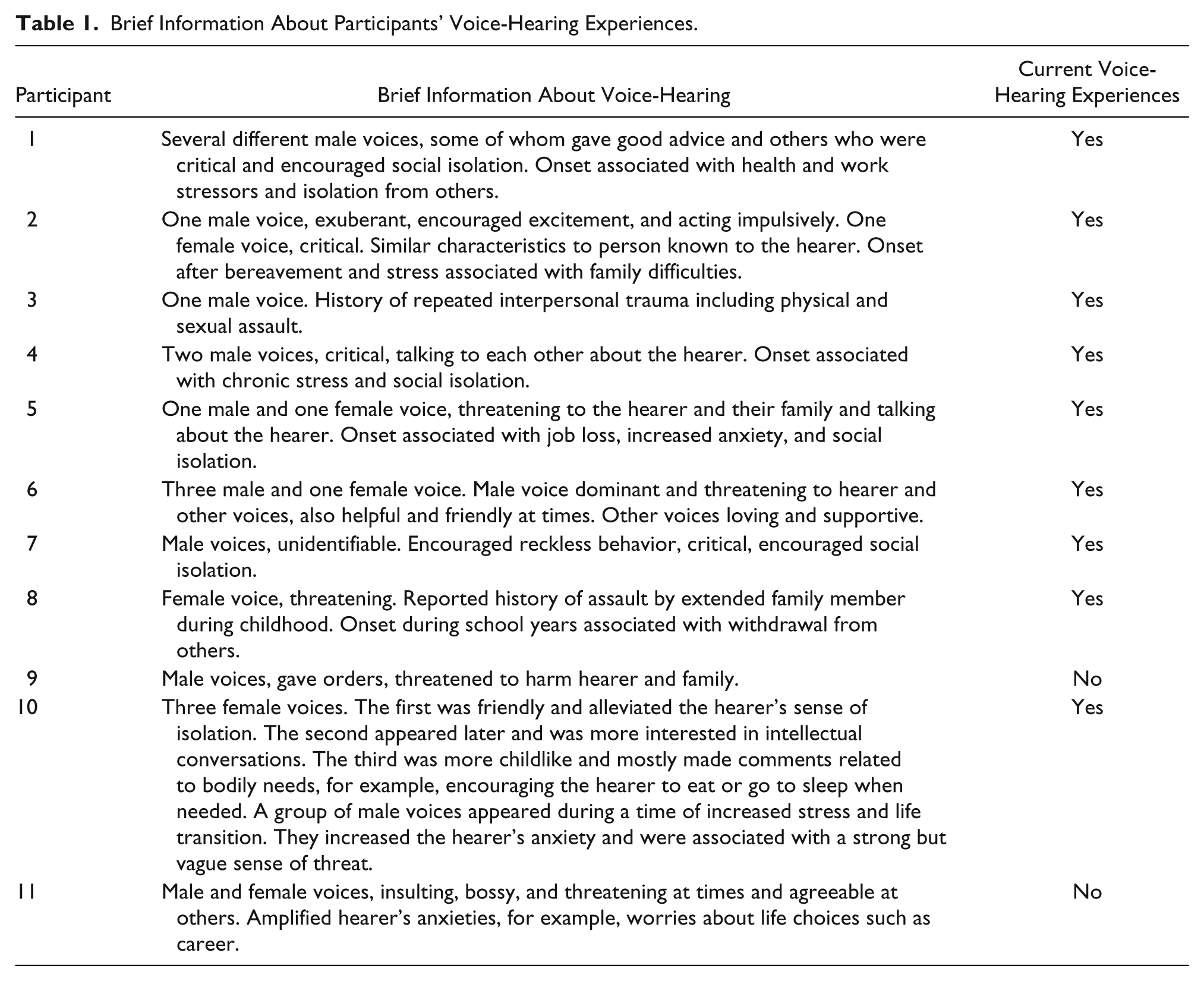
The results of the DIP indicated that during their lifetimes, participants had met DSM-IV diagnostic criteria for schizophrenia (4), schizoaffective disorder (4), or psychosis not otherwise specified (3). Self-report measures showed that nine participants were in Stage 5 (growth) of recovery and the remaining two were in Stage 4 (rebuilding). Participants reported mixed (5) or mostly satisfied (6) ratings of quality of life, and a broad range of global psychological distress (4 low, 2 moderate, and 5 high distress). One participant with a self-reported diagnosis of schizoaffective disorder did not consent to taking part in the diagnostic interview. Their diagnosis is thus based on self-report (see Table 1).
Brief Information About Participants’ Voice-Hearing Experiences.
Participants’ accounts indicated that recovery was not a neat, linear progression over time. They did not move through each stage progressively. Instead, stages were cyclical in nature, with participants repeating or reengaging in processes associated with recovery several times or in an ongoing manner. Processes occurred simultaneously rather than discretely and influenced each other. Participants also took time to rest and consolidate the progress they had made.
Given the shortfalls of any model of recovery over time in capturing the essence of individual narratives, as well as the capacity of models to oppress such narratives, one may well ask why production of such a model is advisable or indeed of value. However, to consider what type of story a person is involved in and which stories are being overlooked is to consider how their lives are defined (Frank, 2010). Identifying recovery typologies allows us to elucidate and reflect on the (usually obscured) power and function of such narratives and the concrete impact they have on people’s lives (Frank, 2010; Madigan, 1992). The description of recovery over time presented in Figure 1 is thus an approximation of what participants described and included to provide a rubric through which to consider recovery.
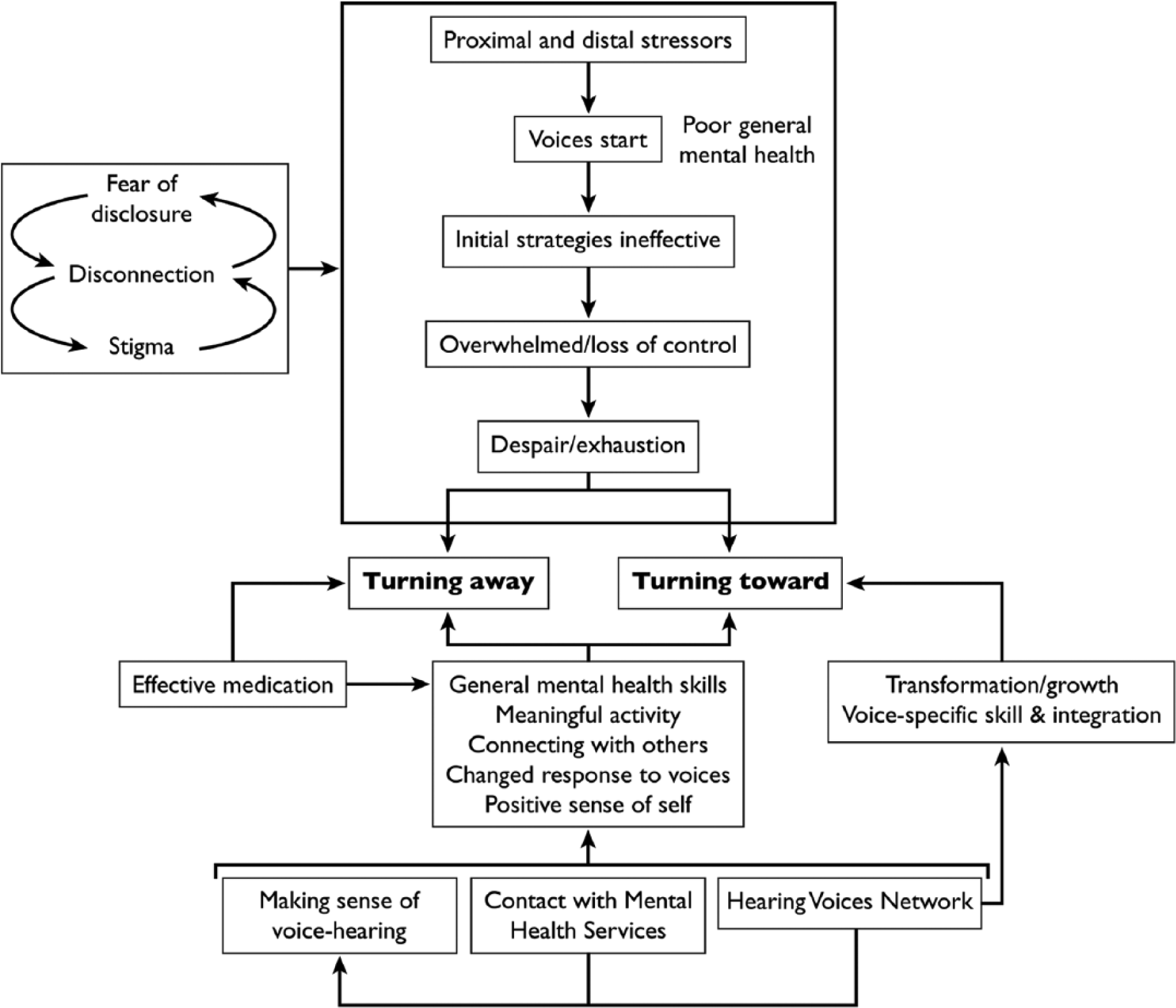
Diagrammatic representation of recovery processes.
Context of Voice Onset and Initial Responses
Most participants described poor general mental health, distal and proximal stressors, and disconnection from others prior to voice onset. Distal stressors included loss of parents at an early age and difficult family relationships, whereas proximal stressors included job loss and excessive stress due to workload. Participants feared the consequences of disclosing their experiences to others, expressing concern that they would be judged negatively because of stigma. They were acutely aware of the risk involved in disclosing that they were hearing voices to mental health professionals, fearing that disclosure may result in invasive treatments or involuntary admission to a psychiatric hospital: As soon as you mention voices—and you pick it up really early—is they want to fill you up with medication. So it became quite secretive for me . . . I never told people about them . . . it wasn’t until . . . I went to a workshop with . . . other voice-hearers that I actually—that I started to talk about them—because I was too embarrassed about telling people what was going on.
Reaching a Point of Despair/Exhaustion
Overall, strategies initially trialed for dealing with voices including resisting them, avoiding feared situations and people related to voices, were ineffective. Participants often described ongoing poor general mental health. In this context, participants became increasingly overwhelmed by their voices, which typically became louder and more intrusive after initial onset: They gave me some medicine and told me it would get rid of it, but they only just kept getting worse and worse and worse . . . until a week or two later, it was virtually nonstop, these two guys talking to each other about me.
Participants were generally less able to disengage from their voices or resist their instructions, as a result sometimes behaving in ways that were not in line with their values: When I was in trouble with hearing voices, I didn’t know myself . . . I lost my feeling, lost my self-knowledge . . . With the voice telling me to do things I just lost my self-control . . . I behaved toward people . . . just aggressively.
Participants described trying everything they could think of to improve their situation, to no avail. Although many had supportive friends or family members, participants felt disconnected from others, which was often encouraged by their voices. After enduring intolerable situations for months or years, participants became increasingly fatigued and/or reached a point of despair: I couldn’t see any hope . . . basically I suppose I felt if things didn’t get better then what’s the point of living? I was at my lowest level then. I prayed . . . deeply as to what was my purpose, what was the point of having a mental illness? How could I contribute (to society) if I had this prognosis? I think my self-esteem and everything was the lowest it could be.
Divergent Recovery Typologies: Turning Toward Versus Turning Away
Following this period of despair and exhaustion, two divergent recovery typologies were identified: turning away and turning toward. Five out of six participants with turning toward narratives were recruited from the HVNNSW, whereas four out of five with turning away narratives were recruited from the ASRB and had had no contact with the HVNNSW.
Turning Away
In turning away narratives, participants did not all reach an identifiable point of despair, however, clearly became fatigued as a result of ongoing difficulties. They responded by harnessing all available resources to batten down the hatches and weather the storm of voice-hearing experiences. This task demanded all of their attention and energy. Participants survived their experiences and generally noticed a turning point when they were prescribed effective medication. Medication contributed to recovery by enabling them to function better, communicate with others, engage in activities, and think more clearly: “I can function better and I can think better and I’ve been able to pass my courses.” These effects meant that participants felt more hopeful about their future: “I started to see the light at the end of the tunnel more and more it was not a train coming from the other way but a light outside.” Medication also eliminated voices in some cases or allowed participants to change their response to their voices, enabling them to hold a more comfortable distance from them. For example, instead of being overwhelmed, participants were able to listen to voices for a few minutes and then distract themselves from them.
Overall, for participants with a dominant turning away narrative, reflecting on their experiences and how they were able to survive and recover was a great deal more effortful than for turning toward participants. They gave sparser, less detailed information and appeared to be unused to telling their stories. These participants, for whom medication was effective, were perhaps unsurprisingly more accepting of a medical model explanation for their voices as symptoms of an illness. These narratives were told stoically, with little or no reflection on the meaning of voice-hearing or curiosity about voices or how to interact with them. Instead, there was a strong sense of wanting to put the experience behind them and get on with their lives.
Turning Toward
Turning toward narratives were characterized by a tendency to turn to face problems, active engagement with voices and curiosity about what the experience meant, testing beliefs about voices, and shifting one’s relationship with voice(s) over time. Participants described an essential transformation of self through voice-hearing and challenges associated with it. Participants learned how to interact with their voices in healthier ways over time, similar to changing a relationship with a social other.
It is of note that five out of six participants with this typology were recruited through the HVNNSW. The impact of involvement with the HVN on recovery trajectories was evident. Participants reported that the HVNNSW facilitated recovery by normalizing voice-hearing, exposing people to the notion that it is possible to live a fulfilling life with or without voices and encouraging consideration of alternative understandings voices. For example, some came to understand voices as communicating something valuable, albeit in a distressing manner. It also provided exposure to other voice-hearers’ ways of dealing with voices, social connection, and opportunities to contribute to others. Participants noted that each person’s process in coming to deal with their voices is different and that it is preferable to be supportive rather than prescriptive: Yeah (this is) my story, some things that work for some do not work for others, because we are excellent, you know, we all have own experience, no one can understand us same as us ourselves . . . I can’t say (the voices) are untrue, it’s not real, to other people with the voices, because . . . it just depends on how long they’ve been dealing with the voices and how much experience they have. Same as me.
Participants moved beyond developing a positive sense of self to describe an essential transformation in identity as a result of becoming unwell and hearing voices. They reported becoming less angry and more empathic toward others, becoming more communicative about their emotions rather than keeping their feelings to themselves, and having a stronger sense of self as a result of their voice-hearing experience: “In a way it’s been good that I got sick because I’m a lot less angry . . . It gives me heaps of empathy for other people too.”
Turning toward narratives were characterized by a shift in response to voices that went well beyond distraction or disengagement. Experiences of despair and exhaustion gave rise to participants challenging their voices or testing their beliefs about them. These acts often required a great deal of courage, particularly given that participants often strongly believed that their voices could harm them: Challenging the voices . . . they might say the whole world will end and your mother will die or people will come round and kill you. But I actually learnt if I said no, no one would come round and kill me.
The ability to challenge voices and test them developed slowly over time, with participants feeling incrementally stronger in relation to their voices. Those with turning toward narratives tended to integrate even very challenging voices into their lives. For example, one participant responded to his voices’ criticisms that he was stingy by donating an affordable amount to charity each month. Another had formal monthly meetings with her voices, however, she found this model too rigid and therefore supplemented it with less formal ad hoc discussions. Challenging commentary was interpreted as a metaphorical expression of her voices’ concerns, which were deserving of her attention. For example, she responded to threatening comments by framing her debate with her voices as a series of poetry: It was a way to be able just to listen to them in an artistic way. So rather than take it at face value . . . it sort of was speaking in a more metaphorical sense. They weren’t necessarily out to get me, it was more like they were concerned about something and I wanted to make sense of what was going on at the time.
Another described a shift in her relationship with her voices from them being in control to her helping them understand themselves: “My voices are now quite curious about who they are—they don’t know who they are, why they are.”
Participants tended to grant their voices the status of meaningful beings. Interacting with them in the context of a generally respectful relationship became a valued part of participants’ lives. This respect developed over time, facilitated by a stronger sense of self and ability to place boundaries around interactions with voices. Listening to what voices were saying and responding in a moderate and reasonable manner was characteristic of recovery. Voices were understood as being part of the person and therefore learning more about voices and engaging with them also meant learning more about oneself. Finally, participants described transferring skills with social others to their interactions with their voices: “I think having a social life really helps in developing my other skills and that in the way helps me; I can transfer those skills over to my conversation with the voices.”
Learning to nourish general mental health was much more strongly linked to learning about voices in turning toward compared with turning away narratives, with many commenting on the two being intertwined. For example, participants became acutely aware that their voices were likely to become problematic during times of heightened anxiety and vice versa, thus becoming a “litmus test” for psychological well-being: It’s got to do with when I’ve got myself under pressure . . . it only comes in now if I get overtired, so I’ve got a fairly rigid . . . routine around sleeping and doing a range of stuff. Because what happens is, I know as soon as she appears that I’m really overtired.
Finally, coming to hold a normalized account of what it means to hear voices was pivotal in turning toward recovery narratives, opening up the possibility of a normal, nonpathologized identity: It really opened up my mind to this as an experience that was normal in the world . . . Whereas before that I thought it was my shame. My shame, my fault, my illness. You know, it was all about me and me broken.
Overall, the importance of medication in recovery was not emphasized in turning toward narratives, and many participants commented that it was ineffective or associated with significant side effects which outweighed its benefits. They were characterized by a tone of empowerment and, at times, defiance. There was a commitment to advocacy for the rights of other voice-hearers. Participants described significant changes within themselves and their worldview as a result of their voice-hearing experiences and recovery.
Common Processes Across Typologies
Across typologies, participants emphasized the importance of learning about how to nourish general mental health. For example, many participants commented that voices amplified existing anxieties or vulnerabilities: “The voices always played on what was your vulnerable point.” Learning how to manage anxiety meant that when voices attempted to amplify concerns they had less traction or believability and participants were less distressed by their comments. This was a strong theme across narratives. Participants also learned how to manage their mood, balance activity levels to ensure that they were not over- or underactive, manage stress, ensure they got enough sleep and developed communication and assertiveness skills. Although at times mental health professionals played a role, it was also common for these skills to be developed without external assistance. Many participants used mindfulness and distraction techniques to create some space between themselves and their voices: “(Mindfulness) is really helpful . . . even if I think I do hear someone swearing at me, I don’t have to take it on board for myself.”
As shown in Figure 1, engaging in meaningful activities, connecting with others and (re)developing a positive sense of self were key recovery processes common to both typologies. These processes were centered around meeting needs to feel competent, valued, purposeful, and connected to others. They were strongly interrelated. For example, engaging in meaningful activities—whether paid work, unpaid caring duties, domestic activities, or voluntary work—provided routine, a sense of purpose and some distraction from voices. Participants felt more valued by themselves and others when they were able to contribute to others: “It makes me feel as though I’m contributing to something. And I want to feel valuable, I want to feel that I can contribute.” For many, it also provided regular, structured activity: I had a structure in the day and I used to do mum’s house work and cook dinner for the family. I enjoyed all my activities . . . that really got me activated and out of all that sedation. I felt I could do things and enjoy them . . . My life was good.
Similarly, developing supportive, nonjudgmental relationships with others was invariably associated with recovery: It’s good . . . sometimes I say “I don’t feel like talking for five minutes or at the moment, just feeling a bit stressed.” And she more than understands. We’ve got a lot in common and help each other . . . she’s a good friend to me . . . It’s very comforting that she can be a friend, whereas my family is quite cold.
Being related to and perceived by others first and foremost as a human being and for who participants are, and not based on stereotypes about people who hear voices, was particularly valued. Most participants likewise rejected stigma surrounding voice-hearing, commenting that they had to be strong people to achieve what they had in life and that they need not be ashamed of their experiences. However, most remained cautious about disclosing their experiences and only did so with trusted others. The importance of these processes emphasizes that recovering from distressing voices is not only about learning how to deal with voices; indeed, it was influenced by the hearer’s entire life context. It should be noted that the positive sense of self common to both typologies did not involve the transformation in self noted in turning toward narratives.
Participants’ experiences of mental health services and treatment varied. Mental health services were perceived as helpful when medication was effective and professionals worked with participants to develop strategies for dealing with mental health difficulties generally and voices specifically, and who spoke about voices without panicking. Access to housing, financial support, rehabilitation, and mental health services as well as antidiscrimination laws facilitated recovery.
Discussion
Turning Away and Turning Toward
This narrative research aimed to investigate recovery trajectories and critically appraise and further develop Romme, Escher, and colleagues’ seminal work on recovery from distressing voices, in particular the suggested startling, organization, and stabilization phases of recovery (Romme & Escher, 1989; Romme & Morris, 2013). In keeping with prior research, participants in the current research understood negative life events to be causally related to voice onset (e.g., Romme et al., 2009). They described an initial response of shock, confusion, and fear in response to voices, loss of sense of self, and becoming overwhelmed. This is in keeping with the startling phase. However, from this point, the research identified two typologies of recovery, rather than just one: turning toward and turning away. Turning toward narratives involved a transformation of self, active engagement with voices, adopting a normalized view of voices and integrating them into one’s life. This provides support for Romme et al.’s (2009) organization and stabilization phases. These narratives align with McGlashan, Levy, and Carpenter’s (1975) integrative recovery style, which involves curiosity about psychotic experiences, striving to make sense of them and integrating them into one’s life, as well as Frank’s (1995) quest auto-mythology narratives, which are characterized by a transformation in identity in response to physical illness. This also resonates with the Māori concept of voices as a “difficult gift” which are nonetheless an ordinary part of daily life (NiaNia & Bush, 2013).
Participants who were seen to “turn away,” however, had also recovered according to our objective criteria, in terms of symptoms, quality of life, and psychological distress. The focus was on the resolution or management of symptoms and leaving these experiences behind, rather than integration. This finding indicates a different type of recovery which does not involve active engagement, negotiation, acceptance, and meaning-making characteristic of the suggested organization and stabilization phases. Instead, this typology bears parallels to McGlashan et al.’s (1975) sealing over recovery style, characterized by cordoning off psychotic experiences from the rest of one’s life, and Frank’s (1995) quest memoir narratives, which involve acceptance of illness with trials told stoically and no special insight gained (France, Hunt, Dow, & Wyke, 2013). In considering this narrative, it is critical that these participants are not pathologized when compared with those who “turned toward.” Participants who turned toward had the benefit of HVN groups and professionals who supported them to normalize and respond to their voices. Turning away participants can perhaps be seen as more remarkable because they did not have access to such discursive resources.
While taking care not to pathologize either recovery typology, the stories that participants told about themselves were more restrictive in turning away narratives and more liberative for those who turned toward. Indeed, there is some evidence that in the long term, an integrative approach toward psychotic experiences confers better psychological health, predicting remission at 1-year follow-up (Staring, van der Gaag, & Mulder, 2011). This raises the question of how clinical services should respond to people with different recovery styles. There is evidence that people’s recovery style can change over time (Tait, Birchwood, & Trower, 2004). Consequently, periodic assessment of a person’s recovery mode would allow services to match their approach to the person’s natural inclination at that time. If someone persists in using a turning away style and this is perceived as limiting recovery, how should services respond: acknowledge that a limited recovery has sufficient meaning to the individual, or seek to facilitate the adoption of a turning toward style? Longitudinal studies examining recovery style would allow further clarification of this issue.
It is of note that despite significant differences between typologies, many recovery processes were common across typologies. These provided the foundations for further progress. They were centered around meeting participants’ needs for connectedness, positive identity, agency, opportunities to contribute to the community, and participate in meaningful activities (Andresen et al., 2003; Reis, Sheldon, Gable, Roscoe, & Ryan, 2000; Slade et al., 2012). This indicates a need to shift from the traditional mode of treatment focusing on the individual to inclusion of family, social networks, and broader community and social contexts (Sibitz et al., 2011; Tew et al., 2011; Williams & Collins, 2002).
Voices, Self and Others
Many people experience an initial sense of their identity being subsumed by that of being a patient or voice-hearer and losing their sense of self because of the overwhelming nature of voice-hearing experiences (McCarthy-Jones, 2012; Romme & Escher, 2011; Tew et al., 2011). Reclaiming a positive sense of self appears critical to recovery (Goodliffe, Hayward, Brown, Turton, & Dannahy, 2010; May, Strauss, Coyle, & Hayward, 2014). Indeed, in the current research, participants described being less distressed by critical or threatening voices when they had developed a stronger sense of self. Recognition of the importance of people’s self-esteem in mediating their affective response to negative voices has lead to this becoming a specific target of psychological interventions, with promising initial results (van der Gaag, van Oosterhout, Daalman, Sommer, & Korrelboom, 2012).
Reclaiming one’s sense of self, however, is a social as well as individual process: the antithesis to personal diminishment which can result from stigma (Livingston & Boyd, 2010). As participants reconnected with others and developed supportive relationships, they were more able to deal with their voices in an adaptive manner. This is in keeping with research demonstrating significant parallels between how people relate to others and how they relate and respond to their voices (Chin, Hayward, & Drinnan, 2009; Hayward, Berry, & Ashton, 2011; Paulik, 2011). It is plausible that as people accumulated more positive experiences with others, their beliefs about others and perception of relative social rank changed, positively affecting their style of relating to their voices. The tendency of people with turning toward narratives to engage with their voices rather than attempt to distance themselves is consistent with research indicating that relating to voices from a position of distance is associated with significantly higher distress (Hayward et al., 2011; Vaughn & Fowler, 2004). Engaging with voices and setting appropriate boundaries have been implicated in developing a positive relationship with voices (Jackson, Hayward, & Cooke, 2011). In keeping with May et al.’s (2014) and Newman-Taylor, Harper, and Chadwick’s (2009) findings, mindfully noticing voices contributed to a less distressing relationship with them.
Discursive Resources and Making Sense of Voices
The narratives people tell define how they understand themselves and their problems (Lock, Epston, Maisel, & de Faria, 2006; Weingarten, 1998). In the context of hearing voices, the dominant narrative, based in Foucauldian terms on “global” (privileged) rather than “local” knowledge, is that it is a symptom of a disease best treated by antipsychotic medication (Madigan, 1992; Schrader, 2013). Implicitly, this narrative promotes the notion of the person as the problem (Ben-Zeev, Young, & Corrigan, 2010; Lock et al., 2006; Madigan, 1992; Van Os, 2010). Those who “turned toward” in this research also “turned away” from the dominant medical model discourse. This act of resistance was conducted in solidarity with others in HVN groups, allowing for the “thickening” of alternative stories (Adame & Knudson, 2007; White & Epston, 1990). For example, participants described voices as a manifestation of distress understandable within their life context (e.g., Beavan & Read, 2007; Schrader, 2013). Although some participants still used aspects of a medical model explanation and vocabulary, they emphasized that voice-hearing is a normal variation in human experience, opening up the possibility of a nonpathologized self. This suggests that exposure to alternative understandings of voice-hearing, which might compliment rather than necessarily replace the dominant medical model narrative, might be helpful.
Parallels in Professional-Driven Treatments
Despite the impact of consumer-driven HVN groups in this research, it is important to recognize that promising professional-driven treatments are also coming to similar conclusions regarding the value of direct engagement with voices and a focus on the person, not just the problem, particularly in the field of clinical psychology. Turning toward voices by exploration of continuities with broader life experiences has long been a key element of therapies such as cognitive behavioral therapy for psychosis (CBTp; see Farhall & Thomas, 2013; Thomas et al., 2014). Contemporary therapy developments have gone further to more explicitly engage with voices, including role-playing interactions with voices (Hayward, Overton, Dorey, & Denney, 2009), the use of computer-generated avatars to represent voices (Leff, Williams, Huckvale, Arbuthnot, & Leff, 2013), and direct verbal engagement of voices by the therapist (Corstens, Longden, & May, 2012).
As a cautionary note, findings of the current research suggest that timing is critical. Turning toward participants reached a tipping point where doing something differently, although still frightening, was evaluated as a better option than continuing to tolerate their unbearable situation. This is similar to the crisis-induced change noted by Milligan, McCarthy-Jones, Winthrop, and Dudley (2013). In addition, those engaged in a turning away style of response might find such treatments unhelpful and require some time to be ready to undertake such work. These caveats aside, the critical role of interpersonal dialogue and solidarity is also becoming recognized in the network therapy of Seikkula and colleagues (e.g., Seikkula, 2002, 2008, 2011; Seikkula, Alakare, & Aaltonen, 2011). This approach involves intensive engagement with the client, the entire family, and any other loved ones and professional stakeholders involved. Treatment is based on the notion that psychotic reactions are prenarrative or metaphorical—attempts to make sense of experiences that are so difficult that they have not yet been situated in spoken discourse (Seikkula, 2002).
Despite the evidence for the efficacy of these treatments, however, several barriers to accessing them remain, resulting in significant unmet need (e.g., Farhall & Thomas, 2013; Mojtabai et al., 2009; National Collaborating Centre for Mental Health, 2009). It is important to emphasize that not one single participant reported receiving psychological intervention that was specifically aimed at dealing with voices. Those who engaged in behavioral experiments and other cognitive behavioral therapy (CBT) strategies did so without the help of a psychologist.
Role of HVGs in Recovery
Results indicate that the HVGs played a significant role in normalizing voice-hearing, exposing participants to different interpretations of what it means to hear voices, disseminating strategies for dealing with voices, and providing a sense of community. This is in keeping with other research reporting on the experiences of group members both in the HVNNSW and overseas (Dos Santos, 2014; Ngo Nkouth, St-Onge, & Lepage, 2010; Ruddle, Mason, & Wykes, 2010; Sørensen, 2013). However, current findings and the research mentioned are based on the experiences of participants who had chosen to attend HVGs and found them helpful. Choosing not to attend an HVG might be part of a turning away response and it is unclear from the current research whether people with this style of response would find attending a group helpful.
In addition, although the flat hierarchy and member-driven agenda of groups are valued by group members (Dos Santos, 2014), this results in significant variation between groups in how they are run (Corstens et al., 2014). It is therefore unclear whether the positive experiences reported by this sample would generalize to all groups and attendees. Finally, the aspects of the HVGs which participants found helpful might also be accessible through peer workers, spiritual groups, structured group therapy, or individual therapy. Indeed, some people report that they benefit from the structured nature of group therapy (May et al., 2014). Of course, people might choose to attend both types of groups. The issue is that, currently, only limited research (e.g., Dos Santos, 2014; Sørensen, 2013) is available on the impact of HVGs, suggesting that further investigation is required to clarify how they influence recovery in people who hear voices, how helpful they are, and for whom they are most useful. Some might reject the notion that such forms of evaluation would be helpful. However, the relative paucity of research means that such approaches are not as well-recognized and accepted by clinicians as might otherwise be the case. More quantitative and qualitative research is required to build a bridge between consumer- and professional-driven approaches, facilitating greater acceptance of HVGs in mainstream services.
Role of Medication in Recovery
The question of how medication may have affected recovery trajectories deserves some clarification. In turning away narratives, participants emphasized being prescribed effective medication as a significant contributor to their recovery. Most participants with a turning away typology described using effective medication as a turning point in their lives. They explained that medication facilitated other recovery processes such as connecting with others and participating in meaningful activities. In turning toward narratives, five out of six participants had used antipsychotic medication (or in one case, mood stabilizing medication) for many years. One participant had not been diagnosed with a mental disorder or prescribed medication. Of the participants who had used medication, two reported that it was ineffective for them and led to significant negative side effects. Three reported that medication was helpful in calming them down or dampening emotional responsiveness. It is of note that it did not eliminate their voices. Those who had used medication emphasized negative side effects, describing lethargy, weight gain, fatigue, and lack of emotional responsiveness and spontaneity. All turning toward participants had negotiated a reduced dosage in medication over time. Turning toward participants did not understand medication as being pivotal to or sufficient for their recovery. Instead, they emphasized the importance of coming to understand themselves and their voices, integrating them into their lives and developing voice-specific skills.
Limitations and Directions for Future Research
This research is limited by its retrospective design, because retrospective recall is less accurate than recording events as they occur (e.g., Schröder & Börsch-Supan, 2008). However, given that narrative research aims to elicit how participants understand their experience, and this involves their subjective recollection of experiences, this is in a sense not problematic. Nonetheless, prospective, longitudinal investigation of recovery style would allow examination of whether there are any people who initially turn away and then turn toward, and if so, what might contribute to this change. It would also be useful to examine whether regular assessment of recovery style and adjustment of treatment style to match patients’ needs lead to better treatment outcomes. A second limitation is the nature of the sample, which was small, involved self-selection and was more likely to attract people who had positive experiences of HVGs. It is also possible that other recovery typologies may be identified if participants were recruited through advertisements in general public settings. However, it is of note that the notion of turning toward and turning away is in keeping with other research into recovery (e.g., Hayward, Awenat, McCarthy-Jones, Paulik, & Berry, 2014; Hayward, Berry, McCarthy-Jones, Strauss, & Thomas, 2014).
Strengths of the study include the rigor used in generating narratives, which were member-checked by participants, and the focus group’s critique of the model of recovery generated. The use of reflection on the subjective values and expectations of the primary researcher was another strength. Through bracketing assumptions and remaining open to the data, it was possible to allow the turning away typology to be identified. Given the bias of the researchers toward understanding recovery as involving active engagement with voices and making sense of them, this finding was unexpected.
Footnotes
Authors’ Note
Portions of this article were presented at the World Hearing Voices Conference, November 20, 2012, Melbourne, Australia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Adèle de Jager received postgraduate research support funding from the University of Sydney which was used for participant reimbursement, obtaining Diagnostic Interview for Psychoses data from the Australian Schizophrenia Research Bank, and travel to Melbourne to present preliminary research findings. Simon McCarthy-Jones’ work on this article was supported by a Macquarie University Research Fellowship and a Wellcome Trust Strategic Award (WT098455).