
Abstract
Previous research inadequately explores processes and factors influencing the delivery of health services to sexual and gender minorities in ways that equitably attend to the infinite diversity held by these groups. This study employed Intersectionality and Critical Theories to inform Constructivist Grounded Theory methods and methodology; social categories of identity were strategically adopted to explore domains of power operating across multiple forms of oppression, think through subjective realities, and generate a nuanced rendering of power relations influencing health service delivery to diverse 2SLGBTQ populations in a Canadian province. Semi-structured interviews were conducted and the co-constructed theory of Working Through Stigma, with three interrelated concepts, depending on context, resolving histories, and surviving the situation, was generated. The theory depicts the concerns of participants and what they do about power relations influencing health service delivery and broader social contexts. While the negative impacts of stigma were widely and diversely experienced by patients and providers, ways of working within power relations emerged that would be impossible if stigma was not present, highlighting opportunities to positively impact those from stigmatized groups. As such, Working Through Stigma is a theory that flouts the tradition of stigma research; it offers theoretical knowledge that can be used to work within power relations upholding stigma in ways that increase access to quality health services for those whose historical underservicing can be attributed to stigma. In doing so, the stigma script is flipped and strategies for working against practices and behaviours that uphold cultural supremacies may be realized.
Keywords
This article outlines a study that furthers understandings of the processes and factors influencing the delivery of health services to diverse sexual and gender minorities (SGM) in Nova Scotia (NS) (Lane, 2022). Previous research fails to explore health service delivery to SGM in a way that is inclusive of the potential for infinite diversity therein. Using Intersectionality and Critical Theories to extend Constructivist Grounded Theory (CGT) methodology and methods, stigma, a negatively affirming social construct, was used as an investigative starting point and was grappled with in two ways: 1) the stigmatization of diverse SGM within the context of a cisheteropatriarchal public domain and 2) the institutionalization of stigma in health care, which shapes curricula in health professional programs, the health system, and interactions therein, including how health services are delivered to SGM. The generated theory highlights the utility of Intersectionality Theory in recognizing the infinite complexity within groups and informing broadly inclusive practices for equitable care delivery.
Background
Cultural norms are designed to create expectations that members of dominant groups can meet with ease. Practices and behaviours promoting cultural supremacies make possible the over-servicing of dominant groups, justify unequal access to resources, and create hierarchies of oppression by way of stigmatizing differences (Adorno, 1973; Adorno & Horkeimer, 1997; Bourdieu, 1977, 1989; Collins & Bilge, 2020; Haraway, 1988). Healthcare settings represent situated contexts that are reflective of broader cultural milieux, across which SGM are subjected to various human rights violations, including mutilation, torture, corrective rape, murder, unequal legal protections, and conversion therapy despite a lack of evidence to support its practice (United Nations, 2011). Existing within all cultures and experiencing health disparities that are well documented in the literature, SGM have been historically pathologized within health care, as evidenced by a legacy of stigmatization that can be traced in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (Canada, 2019; Cohen et al., 2007; Donald et al., 2017; Drescher, 2015b, 2015a; Flores et al., 2018; Hatzenbuehler, 2009, 2014, 2016; Hatzenbuehler et al., 2017; House of Commons of Canada, 2019; Lick et al., 2013; Meyer, 2003; Spurlin, 2019).
Cultural domination is often rooted in stigma and embedded in social practices and behaviours (Castro & Farmer, 2005; Link & Phelan, 2001, 2014; Metzl & Hansen, 2014). Bourdieu’s (1977) framework elucidates the structural nature of stigma in so far as practices inform policies and impact decisions; however, social structures are not static, rather they are fluid and under construction (Metzl & Hansen, 2014). Link and Phelan (2014) argue that dominant groups use stigma as a resource to reproduce social structures in ways that serve their own interests because they are positioned to do so; they construct themselves as superior and that which is different from them as inferior. Stigma thus catalyzes oppression from individual to structural levels, meaning that a person may gain benefits from stigma whether or not they actively stigmatize others (Hatzenbuehler & Link, 2014; Link & Phelan, 2014). Goffman (1963) contemplates the ways that stigma can be managed but highlights a burden that is often placed on the stigmatized to conceal negatively constructed differences. A functional implication of dominant cultures, non-stigmatized individuals may be unable to see how their inaction contributes to oppression because it is beyond the limitations of their knowledge. Structural stigma then makes it so those who are best positioned to influence social structures (because they benefit from behaviours and practices that disadvantage minoritized groups) fail to recognize the shared responsibility to work within power relations that reproduce cultural supremacies so that they can be transformed.
A form of cultural supremacy that operates across multiple forms of oppression by way of cisheterosexist practices and behaviours, cisheteronormativity is an ideological perspective that normalizes sexual bonds between men and women, evidences itself in narratives of biological reproduction (Rosaldo, 1980), upholds stigmatizing social structures, and is central to the oppression of SGM. Cisheteronormative ideology intersects with other social ideologies, reproducing hegemonic norms by way of naturalizing advantages, justifying cultural supremacies, and/or promoting entitlements for some that disadvantage others (Adorno, 1973; Bourdieu, 1977; Castro & Farmer, 2005; Collins & Bilge, 2020; Razack, 1998). Cisheteropatriarchal contexts promote and rely upon partially characterized social realities and reductive understandings of the implications of cisheteronormativity. Within cisheteropatriarchal contexts, power relations enable social structures that stigmatize sexual and gender diversity and negatively construct SGM using standards that are used by those with relatively more contextual power to judge those with relatively less contextual power. An anti-cisheteropatriarchal view might question the sustainability of heterosexual reproduction. There is an argument to make for non-heterosexual reproduction and adaptation, which is supported by Haraway’s (2016) position on making kin and inhabiting an Earth rendered vulnerable by humanity’s incomplete understanding of our responsibility to all who are living. As such, humans could respond to their impact on Earth by legitimating kin-making beyond the constraints of cisheteropatriarchal conformity.
Stigma impacts how all individuals, groups, and communities experience cultural norms, but its characterization and means by which it can be analyzed and intervened upon are poorly conceived (Hutchinson & Bhugra, 2000; Turan et al., 2019). Practice, including that which is involved in delivering health services, is structured action that represents subjectively understood externalized social worlds and reflects an individual’s perceived ability to react under given sets of circumstances (Bourdieu, 1977). Verifiable across cultures, the stigmatization of SGM and the negative impacts of the stress it causes are widely recognized (Abbruzzese & Simon, 2018; Austin, 2016; Basque, n.d.; Becasen et al., 2018; Canadian AIDS Society, n.d.; Cohen et al., 2007; Colpitts & Gahagan, 2016; Eliason & Chinn, 2018; Fish & Krueger, 2020; Flentje, 2020; Flores et al., 2018; Hatzenbuehler, 2014; Hatzenbuehler et al., 2017; Hatzenbuehler & Link, 2014; House of Commons of Canada, 2019; Huebner & Davis, 2005; Lefevor, Blaber, et al., 2019; Lefevor, Boyd-Rogers, et al., 2019; Shangani et al., 2020; United Nations, 2011; Whitehead et al., 2016). We remain stationed in a stage of acknowledgement of the deleterious impacts of stigma because dominant groups have an unquestioned monopoly on this valuable resource. Stigma is seemingly cast in an unwavering belief that it cannot be collectively repurposed. Despite efforts to eradicate stigma (Dubreucq et al., 2021; Tyler & Slater, 2018), it remains associated with negativity and operates across domains of power, intersecting by way of social categories of identity and sustaining unequal access to resources, including health services (Murney et al., 2020). Rather than seeing stigma as a resource that can be used by members of dominant groups to serve oppressive purposes, broadly inclusive practices and behaviours might be adopted so that the context of care invites disclosure of stigmatized differences as opposed to managing their concealment.
The objectively verifiable evidence of the institutionalization of cultural dominance via cisheterosexism in health care provided by the psychiatric discipline in the DSM highlights an opportunity to explore imbalanced power relations rooted in stigmatizing social structures (Drescher, 2015b, 2015a; Groff, 2014; Horkeimer, 2002; Lane, 2022; Metzl & Hansen, 2014; Spurlin, 2019). Cultural domination thus exposes human relationships as fundamentally flawed – the proclivity to eschew the consequences of shared responsibilities that accumulate through mutual pasts, presents, and futures is made possible by ongoing failures to recognize the broader implications of power imbalances (Adorno & Horkeimer, 1997; Haraway, 2016; Lane, 2022). When social realities are ‘characterized by partial connections' (Haraway, 2016: p. 104), the interconnectedness, shared responsibilities, and implications of cultural dominance arising from mutually constituted relations of power can be concealed (Collins & Bilge, 2020; Lane, 2022). This hinders increasing awareness surrounding collective responsibilities; the implementation of broadly inclusive practices that account for collective interconnectedness is jettisoned and the fundamental flaws in human relationships remain unquestioned.
Stigma connects us all, across contexts; citizens of all societies internalize stigma, but its impacts and externalization depend on the sociocultural context, personal circumstances, and the interplay there between. Stigmatizing social structures cause minorities to experience stress, which is recognized as a cause of health disparities, particularly among SGM (Donald et al., 2017; Flentje, 2020; Hatzenbuehler, 2009, 2014; Metzl & Hansen, 2014; Meyer, 2003; Spurlin, 2019). The impacts of stigma-related stress can be influenced, but opportunities to mediate these risks are often concealed from those who are best positioned to transform causal imbalanced power relations. This is because structural stigma can be internalized and externalized by members of dominant groups through practices and behaviours without having any awareness of doing so or its impacts, which means differences can be unknowingly negatively constructed and structural inequalities inadvertently sustained.
Methods
Setting
This study was conducted in NS, a Canadian province with a publicly funded health system that is managed across four geographical zones, and a primary care portfolio that aims to promote transformational change within the region (Fierlbeck, 2018; Nova Scotia Health, n.d.). Within the Canadian context, '2SLGBTQ' is one acronym used to describe SGM and signifies diversity beyond sexual orientation and gender. Using an acronym that begins with '2S' calls attention to the Two Spirit identity, which is particularly significant to the North American context, specifically within Canada, because it is associated with Indigenous cultures, where the ongoing impacts of colonialism continue to be grappled with (Carrier et al., 2020). Further, this acronym explicitly recognizes racial differences and creates a natural entry point for acknowledging other socially constructed differences among SGM (Lane, 2020). This is important because differences beyond sexuality and gender have been historically minimized within queer political activism (Smith, 2019). This hinders a shift towards exploring the impacts of power imbalances on diverse SGM, undermines an intersectional exploration of social justice issues, and impedes the interrogation of cultural dominance across multiple forms of oppression. It is thus possible for queer activism to attend to cisheterosexism and simultaneously promote White supremacy, ableism, and xenophobia if differences beyond sexual orientation and gender are not meaningfully addressed.
There are more Nova Scotians without a primary care provider as compared to residents of other Canadian provinces and territories, and a lack of confidence among 2SLGBTQ health service users (HSUs) in the competencies of those delivering care to meet their needs places them at a greater risk for health disparities (Colpitts & Gahagan, 2016; Gahagan & Subirana-Malaret, 2018; Government of Canada, 2017). While sexual minorities in Canada are rendered invisible by a lack of disaggregated Census data, larger percentages of gender minorities have been found in NS relative to other provinces and territories (Government of Canada, 2022; Waite & Denier, 2019). Nova Scotia was thus deemed a useful context to conduct research exploring the processes and factors influencing the delivery of health services to diverse 2SLGBTQ populations.
Constructivist Grounded Theory
Intersectionality Theory and the Frankfurt School’s Critical Theory were used together to extend Charmaz’s (2014) CGT methodology and methods, explore cultural domination reinforcing structural inequalities in primary care settings in NS, and promote the emergence of common themes. The methodological and theoretical complementarity between Intersectionality, Critical, and Constructivist Grounded Theories (Gibson, 2007; Kassam et al., 2020; Lane, 2021) was significant to this study’s aim to conceive health service delivery in such a way that power relations could be explored by way of stigmatizing constructions of 2SLGBTQ populations. Conceiving practice as an externalization of internalized social structures (Bourdieu, 1977) intended to uncover unrealized opportunities for social change (Adorno, 1973) by thinking through subjective realities (Charmaz, 2019; Gibson, 2007; Kassam et al., 2020) that are historically underrepresented and thus interrogate that which is normatively constructed within the studied context (Lane, 2021).
Methodological reflexivity was used to recognize knowledge as situated, partial, limited in terms of appreciating larger truths, and shaped by broader social contexts that impact perceptions of self and others (Marcus, 1994; Nader, 1972; Narayan, 1993; Salzman, 2002). Methodological reflexivity was also used to acknowledge subject positions and social interactions as influencers of meaning and its co-construction (Lane, 2022). As such, the production of knowledge through partial perspectives that are prioritized in accordance with prevailing power relations assisted the researcher in attending to participants’ subjectivities in relation to her own, promoting a practice of exploring subjective realities without having the requisite lived knowledge to fully understand them (Haraway, 1988; Marcus, 1994; Nader, 1972). Methodological reflexivity mitigated the risk of oversimplifying issues of identity and instead enabled an investigation that challenged preconceptions and identified biases through critical exploration. Stigma served as an entry point for broadly exploring diverse subjectivities through socially constructed differences and power-related themes within the studied context.
The method of negative case analysis was reconceived during the conduct of this study to purposively sample perspectives historically underrepresented in research (Lane, 2021). Called ‘Adornian negative case analysis', this method promoted theoretical sampling by way of creating points of comparison that would be available when data were being analyzed, thus supporting the emergence of common power-related themes (Lane, 2021, 2022). Points of comparison were created in relation to a dominant point of comparison that was defined according to the broader social context within which the study was conducted; minoritized points of comparison can be considered negative cases if differences are teased out of a sample population for the purpose of challenging dominant norms that promote assumed ways of being (Lane, 2021). This was done by conceiving differences across five social categories of identity, enabling an exploration of domains of power operating across multiple forms of oppression (Collins & Bilge, 2020). Differences were then reconceived as similar by way of adopting a social binary of 2SLGBTQ and non-2SLGBTQ. This was necessary to establish a collective standpoint on cultural domination within the sample population through which negative case analyses were employed to interrogate cultural dominance and confront imbalanced power relations through broad and intentional inclusion of diverse perspectives and groups (Chan & Howard, 2020; Cho et al., 2013; Collins, 1990; Lane, 2021; Waldron, 2002). Points of comparison could then be described across categories of identity to highlight the diversity within the sample population. If two or more participants self-identified with the same difference within a social category of identity, then a subcategory was created. There were two or more differences (boi, fluid, graysexual) within the sexual orientation and gender category that justified the creation of a ‘not otherwise categorized' subcategory. It is important to note that the quantification of points of comparison is inapt because they are created for the purpose of theoretical sampling. Expanding Charmaz’s (2014) understanding of theoretical sampling, Adornian negative cases are ‘not about representing a population' (p. 198). Rather, these points of comparison are created so they can become ‘the grist for emergent hypotheses that quantitative researchers might pursue' (p. 198).
Once REB approval was obtained, a diverse sample population (N = 30) was recruited. A recruitment questionnaire was developed and housed on the study website. Recruitment materials included a link to the study website and were distributed through listservs by collaborating partners and existing networks. Those who were interested in participating in the study were asked to complete the recruitment questionnaire, which confirmed eligibility, asked questions about identity and scope of practice, for consent to contact, and contact information. The recruitment tool was rudimentary and intended to serve the limited purpose of informing purposive sampling and promoting maximum variation within the sample population. Eligibility criteria included being 18 years old, having two or more years of experience accessing health services within NS, and self-identifying as 2SLGBTQ and/or being an individual involved in the delivery of primary care services. Eighty individuals responded to the questionnaire and confirmed eligibility. Those who did not consent to be contacted and/or left no contact information when completing the recruitment questionnaire (n = 4) were excluded from the study. Research participants were accepted into the study using a process that was informed by maximum variation sampling. If inclusion promoted diversity within and across social categories of identity, including scope of practice and geographic location, then they were accepted into the study. As recruitment progressed, this process became more selective because certain differences were saturated, meaning later in recruitment, acceptance into the study necessitated bringing new representation to one or more social categories of identity. A total of 30 research participants were accepted into the study.
Informed and written consent was obtained prior to participant enrolment in the study. Recruiting a diverse sample population resulted in an overrepresentation of historically underrepresented groups because extra attention was given to representing a broad range of experience and thus, meaning, among those involved in the research (DePoy & Gitlin, 2016; Flick, 2018). As such, the principles of equity, diversity, and inclusion were substantiated in the research design (Lane, 2021).
Data Collection and Analysis
The significance of stigma, and its broadly inclusive yet negatively affirming nature, supported its use as a sensitizing concept in this study, to initiate the conduct of research aiming to further understand the processes and factors shaping practices and behaviours that perpetuate negative outcomes among diverse SGM. An interview guide was developed and adapted as data collection progressed. The initial interview guide included questions pertaining to identity, role in the health system, and health service delivery experiences as and/or to 2SLGBTQ populations in NS. Stigma was not explicitly mentioned in the initial interview guide, and yet its significance was confirmed from the onset of data collection. As data collection and analysis progressed and the significance of stigma was confirmed by each participant in early interviews without provocation, the prompt question, ‘What, if any, role do you think stigma plays in that?' was added to the interview guide. The interview guide was further adapted for the purpose of theoretical sampling and saturation; examples that illustrated emerging concepts and sub-concepts were offered to test their meaning with participants. As such and in accordance with Charmaz’s (2014) approach, constant comparison methods were used to generate a grounded theory analysis. A total of 40 interviews were conducted (1 initial interview with each participant and 10 follow-up interviews), each lasting up to 90 min. Participants were given the option to choose their own pseudonym. Early data collection and analysis involved initial line-by-line coding of transcripts and memo-writing after each interview. As data collection progressed, the level of abstraction was raised through focused coding, more memo-writing, and diagramming. Theoretical sampling was informed by negative case analysis, which, in addition to member checking, was also used to enhance qualitative trustworthiness.
Findings
Points of Comparison for Theoretical Sampling According to Social Category of Identity.
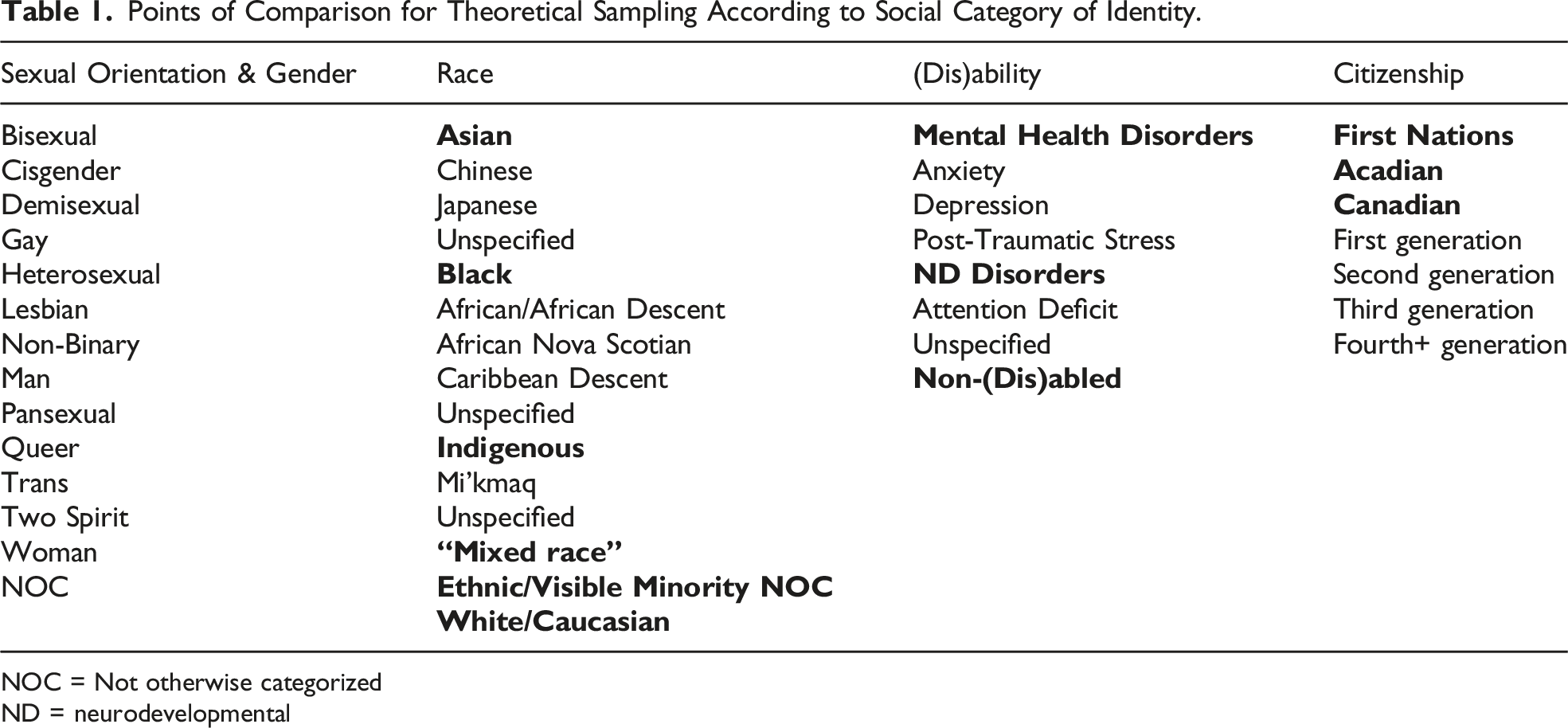
NOC = Not otherwise categorized
ND = neurodevelopmental
Working Through Stigma
The generated theory is one that furthers understanding of the processes and factors influencing conditions under which primary care services are being delivered to diverse 2SLGBTQ populations in NS. Participants described ways of working through stigma that were often but not necessarily negative on impact; they were able to positively impact care delivery that would have been impossible if stigma were not present. The significance of stigma was confirmed by participants from the first interview when Leo (2SLGBTQ HSU) described himself being higher up on the stigma scale because he is a gay man with HIV, but also stated, ‘my experience with the healthcare system has been a dream'. Despite the existence of HIV-related stigma that has been disproportionately experienced by gay men, this participant describes his overall experience in health care as positive. This contradiction invited questions around the inherently negative construction of stigma from the onset of data collection and called attention to what is possible when efforts to bring about change are collectively undertaken, such as the advances in AIDS and HIV treatments that have contributed to Leo’s overall positive experience in health care.
Figure 1 is a depiction of the process of Working Through Stigma, which is cyclical, operates simultaneously at multiple levels, has no beginning or end, and is comprised of three interrelated conceptual processes: depending on context, resolving histories, and surviving the situation. Working Through Stigma is mutually constituted by non-linear concepts – the structure of their presentation here only intends to assist the reader’s understanding of study findings. The work that needs to be done through stigma is contextual and situated. Sorrel illustrates how stigma needs to be worked through at multiple levels (intrapersonal, interpersonal, and structural) to get past the limitations that are placed on what we know about the world, ourselves, and each other: You don't know that there's stigma until you see it. When I was first growing into myself, I was like, ‘Oh, I guess there's that coming at me and other people. And where's it coming from? Is it coming from myself [intrapersonal]? Is it coming from other people [interpersonal]? Is it coming from the media [structural]?’ And eventually you learn that [it’s all of the above], but it takes time. […] When I was first introduced to the world of sexuality, I would play along. […] I was like, ‘Okay, I guess this is what people are supposed to be doing.’ It was hard to realize that because in my head, I wasn't thinking that I'm ‘other’. It was just what I had to do. When I was in high school, I was like, ‘Oh, so I'm actually different and not feeling the same things as these other kids are. And they don't really know what to do with that.’ There wasn’t a lot of information. It was a process. […] The more you're aware that these identities exist, the more you're willing to consider whether you are them or not. I had no idea that you could be trans or non-binary. I didn't know that that could exist. Diagram of a theory of Working Through Stigma.
Sorrel describes a process by which an awareness of stigma and the limitations it places on knowledge is gained, and how it takes time to relate that information to current understandings of the world and meaning made therein. This ‘is' Working Through Stigma.
Depending on Context
Participants across all subgroups recognized that upbringing was a key context upon which ways of thinking about differences depended. This set the stage for how differences were constructed by individuals within and across contexts. Participants with negatively constructed differences were stigmatized by normative assumptions, which could create more work for them as compared to those whose differences were constructed as superior but depending on the context, this shifted. For 2SLGBTQ participants, there was a perceived threat of losing member status, which set the stage for keeping stigmatized aspects of identity hidden from those who made assumptions about them.
If contexts change, then circumstances shaping outcomes therein might come about differently. When circumstances shaping outcomes come about, the stage is being set. If circumstances change, then the stage has been reset. What it takes to reset the stage depends on the context. The conditional nature of working through stigma and the potential for change is highlighted by the fact that a stage can be reset if stigma is used as a resource for normalizing differences that are stigmatized in broader social contexts. As such, how socially constructed differences are realized can change if the stage is reset in a way that supports such a shift.
When socially constructed differences are being realized, it matters who is involved in creating distinctions, and how they are impacted by prevailing contextual power relations. Each stage is set differently, meaning differences are realized in diverse ways, even when individuals use the same labels to describe their identity because no two lived realities are identical. Stigma therefore shapes what options are available and opportunities attainable through the contextual realization of socially constructed differences. As one 2SLGBTQ HSP participant explains, ‘It’s not making good choices, it’s that you had good choices to make'.
Ideally, one has access to all relevant information before making a choice, but stigma also shapes access to knowledge in ways that are unbeknownst to decision-makers, which impacts their situated understanding. Anna (non-2SLGBTQ HSP) is a manager in a primary care clinic in rural NS who shared an experience where she incorrectly addressed a patient using the name in the electronic medical record (EMR). This brought about the realization of a socially constructed difference in a way that was influenced by prevailing contextual power relations but expanded Anna’s situated knowledge in such a way that she could implement change and reset the stage to realize the same difference in non-stigmatizing ways. [A]nd this patient was very quick to go, actually, I go by such and such. […] I was embarrassed, but he was very, very good about it. And we sort of laughed it off. And he's like, ‘No, no, I haven't met you before. So, it's totally fine,’ sort of thing. And then it wasn't long after, a few months later, that we switched to a new EMR. And once we figured out that you could customize literally anything in that EMR, even the layout of the EMR itself, it was just a matter of, as those patients came in for the regular appointments, we would just make the changes.
Anna works in the community, which shapes her access to knowledge and brings forth different opportunities to reset the stage and build trust than what might be available to her in another context. The ability to make changes to an EMR is one thing, but the knowledge that is necessary to implement a change that promotes better outcomes in the clinic would not have been made available to this participant without sharing in the stigmatization that people who are gender diverse routinely experience when they are addressed by the wrong name. As such, knowing what to customize came about by way of an embarrassing experience that was born out of stigma. Knowing how to customize the EMR was thus expanded, as was Anna’s understanding of what she could do as manager of a primary care clinic to positively influence outcomes. Having such an impact would have been more challenging for Anna if gender diversity was not stigmatized.
When Working Through Stigma, outcomes depend on context and choices can be reshaped, but changes must happen so that stages can be reset, and opportunities for realizing socially constructed differences in non-stigmatizing ways can be identified. Making changes can thus support the realization of differences in non-stigmatizing ways and decrease the risk of using the wrong name to address someone. In the example given, this entailed customizing the EMR, creating a new practice that promotes equity for those who experience stigmatization when their birth name is used. As such, when individuals work through stigma in ways that expand upon their experience and existing knowledge of the world, then they can appreciate how they are positioned to bring about positive change.
Resolving Histories
Reconciling the implications of stigma at intrapersonal, interpersonal, and collective levels is resolving histories. Building on the concept of depending on context, resolving histories captures the temporality of shared consequences and actions taken to manage perceived threats across contexts. In addition to intrapersonal, interpersonal, and structural levels, impacts are collectively experienced, directly and indirectly. Resolving histories highlights the disproportionate burden to overcome negative consequences placed on those whose differences are negatively constructed by way of interconnecting through stigma in ways that benefit members of dominant groups.
Nailah (2SLGBTQ HSU) illustrates resolving histories by reconciling the implications of stigma on her access to health services. She stopped using primary care after she ‘could tell that his [family physician] assumptions on the cultural level impact[ed] the way he views me as a person […] [and the] care he gives me'. She now relies on the mental health system for her care. I feel like I'm just more seen and my identity is much more important [in] […] mental health care. It seems like that's more important than if I went to just the doctors [in primary care]. They don't care about anything. They’re just like, ‘Okay, what do you want? Okay, here, get it, leave me alone.’ […] Some [mental health clinicians] have asked me questions about the intersectionality of my identity. It’s starting to be acknowledged that these things impact your mental health. Being Black impacts your mental health, being queer impacts mental health, disabled, all these things that stray you from the neurotypical ideal, because the world is made for one, almost one cookie cutter type of person. Anybody outside that realm is suffering because of that, or at least has not been given adequate care. So, mental health seems to be where people, at least in some way, are getting acknowledged.
Nailah’s experience elucidates resolving histories in so far as she reconciles the impacts of stigma on her family physician’s views of her (intrapersonal level), their impact on the care he delivers to her (interpersonal level), and the impacts of racism, cisheterosexism, and ableism on health (structural levels). It is harder to change outcomes if power relations upholding structural inequalities are promoting the accumulation of benefits for members of dominant groups at the expense of those whose differences are negatively constructed, but solutions like Nailah’s illustrate the ways that one can mitigate stigma’s negative impacts. Resolving histories would see Nailah’s decisions as informed and influenced by past choices – personal and collective – and future outcomes under construction.
Other participants took a stand against institutional policy with the intent of mitigating the negative impact of stigma. Alison (non-2SLGBTQ HSP) shared the challenges she faces when developing exams because all questions must reference the textbook. Alison explains that questions about medication dosing are easy, but when the topic is influenced by stigma, she must work harder to get others to understand how existing knowledge can be expanded upon in ways that promote positive outcomes for those who are underserviced because of stigma. I said, ‘We need to put some questions on the exam about trans patients.’ Then someone says, ‘Well, you can't reference that in the textbook.’ I said, ‘You absolutely can. Go to the section in the text that's on tact and patient advocacy. It doesn't matter who you are. If Miss Stella White says, ‘Please call me Dot’, then that's what you call her. It doesn't matter who it is. So yes, you can reference that in the textbook.
Alison works within power relations and illustrates how the accumulation of negative impacts at various levels can be mitigated. She demonstrates work that she has done intrapersonally – as someone who is non-2SLGBTQ – in her ability to argue for the inclusion of exam questions that render gender diversity visible. Interpersonally, she does so with those who do not have this expanded understanding to promote an awareness surrounding what can be done to mitigate stigma-related barriers to care. Other participants shared examples of how they reconcile the implications of stigma at various levels, including self-disclosing stigmatized aspects of their identity, using neutral language, and advocating for equitable policy change.
Resolving histories also captures the ways that views can shift over time. Participants reflected on how their perceptions have been influenced by stigma in the past and the work they did to come to a new understanding. Lucy, a 2SLGBTQ HSP, explains, ‘[T]here are times in the past when I perpetuated a stigma. It’s not like I’m on the other side of that. So, I’m constantly learning and hoping I practice staying open to the learning and the challenging'. Personal and collective histories interconnect through stigma, across time, and power relations can be reproduced or transformed. There is an openness to learning that is required to appreciate the implications of decisions and how to make them in a way that historical injustices can be reconciled. Then an awareness surrounding what steps can be taken collectively to level the playing field, improve sense of belonging and pride, deal with minority stress and stigma, violence, and discrimination, and manifest healing through mutual pasts, presents, and futures can be created.
Surviving the Situation
The concept of surviving the situation means coping with and adapting to sets of circumstances. This way of framing coping behaviour supports a strengths-based approach that can be used to appreciate the responses of groups and individuals whose existence is shaped by stigma at intrapersonal, interpersonal, and collective levels. When Phoenix (2SLGBTQ HSP) says, ‘I always come at it with a defensive feeling. Like, what assumptions are people going to make today? […] What am I going to have to do? Fight back or just point it out in a nice way?', she is describing an adaptive response to the risk of being stigmatized when others make incorrect assumptions about her. When an individual is threatened, they cope with and adapt to the threat in ways that make sense within the context of the behaviour. What might be negatively framed as a flawed or dysfunctional way of coping can be reframed as adaptive within the context of power relations working through stigma. In so far as there is a weighing of risk (e.g. the risk associated with accessing care from places where there were past negative experiences vs. that of hoping a health issue resolves on its own), surviving the situation is a strategy for reducing one’s own risk of harm and/or working to avoid contributing to another’s need to cope with and adapt to situations and situatedness.
Participants saw flaws in the processes by which health services, education, and training are delivered, and rather than attributing problems to individuals, they connected them to systemic inequalities that contribute to the underservicing of 2SLGBTQ populations in NS and restrict those involved in delivering their care. Coming out in opposition to (cishetero)normative cultures caused participants to be negatively impacted by power relations working through stigma within healthcare settings. Participants shared experiences where providers called attention to discrepancies between gender presentation and legally documented sex in ways that were uncomfortable. When perceived discrepancies were not seen as flaws, opportunities to normalize differences (that may be a source of stigmatization and thus constructed as flawed) could be identified. Rather than calling individuals’ identities into question, oppressive norms, such as cisheteropatriarchal ideologies, could be called into question and acted upon in ways that were read as safe by others. As one 2SLGBTQ HSP participant explained, ‘I think the art of medicine is knowing when it’s a time to make someone comfortable and […] show them that you’re in their camp, and that your objective is their health'.
Emmanuelle (2SLGBTQ HSU) describes the survival strategy of reading, a skill whereby flaws are found and then exaggerated (Corey in Livingston, 1991). Reading situations helps to identify and navigate threats to survival – a good read on a bad situation means you identify the threat before it triggers your survival instinct. Emmanuelle reads others’ responses to disclosing things about herself that are stigmatized to identify threats. I can usually tell when […] I’m having a conversation. I don't miss it. […] I'll drop the fact that I have female partners […]. That's a way I'll do that… to see if they flinch or if I get a raised eyebrow. […] [I]f I'm getting a weird vibration from somebody. And, also sometimes in the language that they use and, and how they refer to people and the tone that they use. […] So, I sort of feel out how people express things and how they talk about things and then I can get a feeling of like, okay, this person would be safe.
When someone is dropping facts about themselves that are stigmatized in broader social contexts, they are trying to identify threats. This behaviour can cue others into the opportunity to normalize a difference that is negatively constructed in broader social contexts, be read as safe, and reduce the risk of being perceived as a threat. Avoidance, shutting down, protecting self and others, and defensiveness are cues that there is something about the situation that is being perceived as threatening. Depending on the context of a person’s existence, implications of stigma at intrapersonal, interpersonal, and structural levels that need to be resolved, and what risks are routinely encountered, everyday survival may be more difficult for some as compared to those who experience relatively less risk.
All participants recognized the importance of the skill of knowing how to make someone feel safe when health services are being delivered, to avoid being perceived as a threat, and make situations easier to survive. Steve (2SLGBTQ HSP) describes having to protect himself to mitigate the negative impacts of power relations working through stigma in ways that differed from participants in other subgroups. ‘[Y]ou have to compartmentalize. If not, you take it home with you. […] If you want to last a long time in this profession, you’ve got to protect yourself'. Protecting himself by way of compartmentalizing aspects of his professional experience is an adaptive strategy in mediating the risks of being an HSP who is out to their patients and colleagues.
Steve faces additional threats as a gay man, but because he is a 2SLGBTQ HSP, he can advocate for himself in ways that would be impossible if he was non-2SLGBTQ or a HSU without the training and education of a HSP. During his interview, Steve offered provider discomfort in prescribing HIV pre-exposure prophylaxis (PrEP) as an example of a barrier he has faced and overcame, explained that HSPs can push back as HSUs in ways that non-HSP HSUs cannot, and pointed out that this could mean the difference between getting the care you need from your primary care provider and being refused for the same because the provider is uncomfortable prescribing PrEP. In so far as Steve knows how to prescribe PrEP, he can explain what work through stigma his primary care provider must do to address his needs. ‘And so, it’s been kind of simple for me, in that sense, but I thought, “My god, if I was a teacher, or… what would I do? I would just leave the office without being on PrEP.” […] I think it’s your professional obligation then to become comfortable with it.' When providers prioritize their comfort over the needs of their patients in such ways, they avoid doing the work required to disrupt power relations working through stigma and they push the burden onto those who have relatively less contextual power, making it harder for them to adapt to situations and situatedness. While it may not be intentional, this serves the interests of dominant groups because individuals with relatively more contextual power can shirk their professional obligation at the expense of their patients. As such, opportunities to deliver equitable care are missed and limit access to a medication that literally increases the chances of surviving situations and subject positions where there is an increased risk of HIV.
Discussion
Working Through Stigma is a theory that accounts for the negative impacts of stigma and, however, provides an alternate perspective that can be used as a resource for anticipating the negative impacts of stigma and promoting better outcomes. In doing so, Working Through Stigma calls the meaning of stigma into question, flouts the tradition of stigma research, and challenges negative constructions that benefit dominant groups, and thus behaviours and practices that uphold cultural supremacies. Working Through Stigma is a theory that is broadly inclusive; the diverse perspectives held by the sample population promoted the generation of an absorbing theory with a polemic purpose. As such, strategies for working within power relations upholding cultural supremacies are provided so that access to quality health services is increased for those whose historical underservicing can be attributed to stigma.
The meaning of stigma has shifted since Goffman (1963) first described it (Kleinman & Hall-Clifford, 2009), but it remains stationed in negativity. The limitations placed on how stigma is defined are created and maintained by dominant groups, exposing it as partially characterized, reductive in terms of meaning, and oversimplified with respect to its utility. What happens if those limitations are challenged and worked through? What exists on the other side? Could it serve a different purpose if dominant groups were not using stigma to pass judgement on others and justify their advantages? Working Through Stigma is a way of thinking about differences that would have us ask these critical questions to further understand power relations and the strategies individuals use to gain access to what they need. As such, opportunities within and across contexts for changing practices and behaviours can be revealed. Transforming social structures thus becomes possible when partially characterized social realities constructing differences are exposed and reductive conceptualizations of stigma – and understandings of its implications – are called into question.
HSPs can be taught to realize socially constructed differences in non-stigmatizing ways with HSUs from populations historically underserved in health care by Working Through Stigma in ways that anticipate its negative impacts (Lane, 2022). Such a shift could bring about reform in healthcare settings where the stigmatization of sexual and gender diversity in public domains of cisheteropatriarchal societies has been institutionalized, shaping health service delivery to SGM, restricting access to health-related resources, and having far-reaching impacts within and across contexts. If stigma is a resource that is used by members of dominant groups at the expense of others (Link & Phelan, 2014), then its repurposing could bring about social transformation by collectively and equitably sharing in the burden of consequences accumulating through mutual pasts, presents, and futures. If a powerful minority did not have an interest in oppressing a subjugated majority divided by stigmatized differences that uphold the superiority of the former at the expense of the latter, then exploitation, control, and exclusion could be widely recognized for what it is: a brutishly potent mechanism that confers benefits upon members of dominant groups. Interconnectedness could broadly promote benefits for all, but the monopoly on this valuable resource must be relinquished.
Participants shared accounts of what work can be done through layers of intersecting stigmas when delivering health services to diverse 2SLGBTQ populations, the harm it can cause, and the complexities involved, but Adornian negative case analysis disproved the rule of stigma as being an inherently negative ‘thing'. Opportunities for social change can be uncovered by working through stigma in ways that question normative practices and behaviours and call attention to what must be done to address its negative impacts. If stigma is operating within broader social contexts, then it can be worked through so opportunities for structural change can be realized. Only then can stigma be used as a resource that is collectively used to benefit the stigmatized and those who work with them. As such, stigma-related stress could be intervened upon, and the negative implications of stigma reconciled at multiple levels if stigma was used as a resource for normalizing differences that are stigmatized in broader social contexts. Healthcare professionals could then be taught how to work through stigma equitably, and access to health services would be increased for populations whose underservicing can be attributed to stigma. Until then, those involved in delivering health services to diverse 2SLGBTQ populations may continue to work through stigma in ways that collectively contribute to the supremacy of dominant groups within and across contexts.
Strengths and Limitations
Strengths of the study include the methodological rigour that CGT offers (Glaser & Strauss, 2017; Rieger, 2019). Intersectionality and Critical Theories extended CGT methodology and methods and strengthened the generation of theoretical knowledge in so far as power relations operating across multiple forms of oppression were broadly explored, not by way of generalizations but through the differences that were teased out of the sample population when Adornian negative cases were created using maximum variation sampling (Lane, 2021, 2022). Embedding the principles of equity, diversity, and inclusion in research methods (by employing Adornian negative case analysis) enhanced qualitative trustworthiness and mitigated the risk of further subjugating those who are not explicitly prioritized in an intersectional analysis (Kassam et al., 2020).
Limitations include unequal diversity across subgroups. Beyond reasons outlined in the Methods section, detailed sociodemographics are not reported because the specificity of identities may risk the anonymity of participants. This is in keeping with CGT methodology and methods; highlighting the range of subject positions through which qualitative data were analyzed is more important than quantifying differences. Further, differences within the sample population were recorded using data collected from the rudimentary recruitment questionnaire and those that were voluntarily disclosed during interviews, which means that it is likely that more differences existed within the sample. This highlights the impossible task of fully capturing diversity within a sample population, which is another limitation of this study and research more generally. Finally, as one participant explained, those involved in co-constructing this theoretical knowledge ‘have some skin in the game'. As such, participants in the study were personally invested in promoting better outcomes among SGM. Even non-2SLGBTQ participants frequently cited family members, close friends, and professional obligation as reasons why they felt this research was necessary. This suggests that participants were all aware of the implications of stigma, which could be a limitation; some participants expressed views that this could also be a strength of the study.
Conclusions
Working Through Stigma provides a theoretical guideline on the conditional and circumstantial nature of delivering health services within power relations upholding cultural supremacies. Depending on the context, experiences can be positive for members of groups who have been historically disadvantaged if the meaning of stigma is expanded beyond its current conceptualization. This is a critical first step towards repurposing stigma and transforming social structures. Working Through Stigma is a way of intervening upon social structures at various levels because stigma is structurally embedded. Stigma could be more than a social construct that is shaped by the practices and behaviours of dominant groups who use it to control access to resources within and across contexts. If its negative construction was challenged, then stigma might be freed from its inherently negative traits without diminishing its scope and re-casted as a means by which unrealized possibilities for bringing about equitable change can be explored in primary care settings in NS and beyond. There is an immense amount of work to be done before the scale of transformation that is necessary for the eradication of stigma will be achieved. Until then, opportunities to transform social structures will be available to those working within power relations upholding cultural supremacies.
Footnotes
Acknowledgements
This research would not have been possible without the generosity and wisdom of the participants who shared their experiences to bring about a more equitable world for all. Drs. Ingrid Waldron, Marilyn Macdonald, Megan Aston, and Liesl Gambold contributed to this study in ways that transcend their roles as members of the author's doctoral committee. The support and encouragement they offered made it possible for the author to explore innovative approaches to conducting stigma research. Finally, the author would like to express gratitude to the peer reviewers and journal editorial staff who offered critically constructive feedback that further strengthened the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received funding to support this research from the Killam Trusts, Nursing Research & Development Fund (School of Nursing, Faculty of Health, Dalhousie University), Faculty of Graduate Studies, Dalhousie University and the Canadian Nurses Foundation.
Ethical Approval
This study was approved by The Nova Scotia Health Research Ethics Board (REB File #: 1026178). All participants provided written consent prior to enrolment in the study.