
Abstract
LGBTQ+ people are no stranger to loss and grief, particularly during times of pandemic such as the 1980s–90s HIV/AIDS pandemic and now, the COVID-19 pandemic. Current COVID-19 loss and grief research remains relatively silent on LGBTQ+ peoples’ loss and grief experiences. The aim of this research was to conduct a qualitative evidence synthesis of LGBTQ+ people’s COVID-19 loss and grief experiences reported in the literature. A systematic search and inclusion strategy identified 22 relevant articles for review. Inductive thematic synthesis resulted in five loss-focused themes across the articles: (1) loss of work and livelihood, (2) loss of social and kinship connection, (3) loss of LGBTQ+ community connection, (4) loss of physical and mental health supports and (5) loss of LGBTQ+ identity authenticity, affirmation and visibility. Discussion of these themes highlights the many layered and often disenfranchised nature of LGBTQ+ people’s loss during the COVID-19 pandemic.
The COVID-19 pandemic has created significant upheaval, with nearly 6 million reported deaths and over 400 million cases recorded to date (February 2022) on the John Hopkins COVID-19 Global Dashboard (Dong et al., 2020). The impacts of the pandemic on people’s lives are not homogenous and in cis-heteronormative societies, a disproportional impact is felt within marginalised communities such as women (UN Women, 2021) and the world’s LGBTQ+ peoples – lesbian, gay, bisexual, transgender, queer or any other minority sexuality or gender identity (e.g., two-spirit or third gender) (Bishop, 2020). The COVID-19 pandemic for LGBTQ+ people has either brought new challenges or has amplified pre-COVID marginalisation which has negatively affected their sense of belonging, social connectedness and identity affirmation (Bishop, 2020). Associated with such COVID-19-related challenges are experiences of loss and grief.
Loss and grief are as ubiquitous with life as they are with death, involving changes in concrete and more abstract parts of people’s lives, selves and identities (Weenolsen, 1988, 1991; Wheat & Thacker, 2019). Weenolsen (1988) defined loss as ‘anything that destroys some aspect … of life and self. Loss is not change, but change incorporates both loss and its overcoming’. (p. 19). This overcoming, or response to loss, is often viewed as grief that ‘permeates all facets of our lives’ (Goldsworthy, 2005, p. 167). Most of what we understand about loss is based on death losses (e.g., bereavement) rather than non-death losses (e.g., loss of employment) (Fernandez et al., 2014; Goldsworthy, 2005; Harris, 2019). Dominant approaches to understanding people’s loss and grief tend towards more individualistic, psychological and clinical/medical lenses (Goldsworthy, 2005). As such, loss and grief are considered internal, largely private, individual reactions relating to significant changes in people’s environment requiring equally individualistic therapeutic pathways, such as counselling or psychotherapy. These dominant therapeutic approaches include psychodynamic theory (Freud, 1917; Lindemann, 1944), attachment theory (Bowlby, 1980), phase/stage/task models (Kessler & Kubler-Ross, 2005; Parkes, 1987; Raphael, 1984; Worden, 2018) and cognitive-behavioural models (Malkinson, 2001; Stroebe & Schut, 2010). While contributing to greater understanding of loss and grief, these approaches do not always consider the impact of imposed cis-heteronormativity within the context of intersecting social identities (e.g., age, sexuality and gender identity, religion, class, culture) in shaping LGBTQ+ people’s experiences (Schwartzberg, 1992; Wheat & Thacker, 2019).
Wheat and Thacker (2019) argued that LGBTQ+ people often experience loss and grief that have common features to that of their cis-heterosexual counterparts, as well as experiences uniquely related to socially imposed cis-heteronormativity that marginalises LGBTQ+ identities. For example, common losses, according to Wheat and Thacker, include death of a relative from an LGBTQ+ person’s Family of Origin such as their parent, partner/spouse, sibling, or child or the death of LGBTQ+ community members. In such death-related losses, an LGBTQ+ person can face unique experiences such as whether the deceased’s and/or a surviving partner’s sexuality and/or gender identities are affirmed by family and friends (McNutt & Yakushko, 2013). They can also uniquely face challenges surrounding legal recognition of spousal relationships, parental status and child custody arrangements (Chauveron et al., 2017). A loss related to an LGBTQ+ person’s Family of Choice, that is, their LGBTQ+ kinship networks (Prasad, 2020), may be deeply grieved. This is due to the strong sense of solidarity and safety often found within the Family of Choice compared with the Family of Origin who might be hostile towards anyone who is not cis-heterosexual (Wheat & Thacker, 2019).
Loss and grief experiences unique to LGBTQ+ people include loss of visibility, affirmation and authentic self-expression of their sexuality and gender identities. For example, LGBTQ+ elders may experience and subsequently grieve the loss of visibility and authentic self-expression from having to move into residential aged care facilities run under the auspices of religious organisations that are not affirming of LGBTQ+ peoples (Arthur, 2015). In the case of LGBTQ+ experiences of reproductive loss, Craven and Peel (2017) described how cis-heteronormative cultures can strip LGBTQ+ parents of their parental status. Likewise, the process of ‘coming out’ to others as LGBTQ+ can involve loss of belonging and social connectedness particularly when coming out within religious or spiritual communities and/or within particular non-LGBTQ+-affirming racial, ethnic or cultural communities (Wheat & Thacker, 2019; Wood & Conley, 2014). As such, loss and grief related to visibility, affirmation and authentic self-expression as LGBTQ+ can become disenfranchised (Doka, 2008; Thompson & Doka, 2017).
A key thread across many LGBTQ+ peoples’ experiences of loss and grief prior to the COVID-19 pandemic is the degree to which their experiences are disenfranchised, or conversely enfranchised, within cis-heteronormative cultures. Disenfranchised grief is ‘grief that persons experience when they incur a loss that is not or cannot be openly acknowledged, socially sanctioned or publicly mourned’ (Doka, 1989, p. 4). The nature of disenfranchised grief is that of a social phenomenon encompassing death-related and non-death losses (Thompson & Doka, 2017) which arises from cultural norms surrounding who ‘has a right to grieve or a claim for social sympathy or support’ (Doka, 2008, p. 224). Cis-heteronormative cultural norms largely dictate whether such grieving rights are extended to LGBTQ+ peoples. This includes if LGBTQ+ people are afforded the right to publicly mourn deaths in their family of choice and broader kinship networks, as highlighted by Schwartzberg (1992) during the HIV/AIDS pandemic in the 1980s and 90s. Further examples include if an LGBTQ+ parent is permitted to be present when news of their child’s death is announced in the hospital (Craven & Peel, 2017), or whether the LGBTQ+ elder is permitted the safe space to express their lost sense of visibility in a religiously auspiced residential aged care facility (Arthur, 2015). In such examples, cis-heteronormative cultural norms gate-keep the right to grieving these losses.
How cis-heteronormative cultural norms during the COVID-19 pandemic have had an impact on LGBTQ+ people’s lives are still evolving; although grey literature points to an amplification of pre-COVID-19 experiences (Bishop, 2020). The general loss and grief literature (e.g., Bertuccio & Runion, 2020; Kumar, 2021; Reneau & Eanes, 2020; Walsh, 2020; Zhai & Du, 2020) is not clear on LGBTQ+ people’s experiences. Therefore, a useful starting point in understanding the COVID-19-related loss and grief experiences from the perspective of LGBTQ+ people themselves, is in reviewing and synthesising the published qualitative research in the area; and as such this is the aim of the review reported in this article. An additional aim is to bring to the fore the rich and subjective experiences of LGBTQ+ people. This article is the first, to the knowledge of the author group, that focuses on the review and synthesis of the qualitative research as an attempt to make visible and affirm LGBTQ+ people’s COVID-19-related loss and grief experiences to inform health practice and policy.
Aim and Review Question
The aim of this research was to conduct a qualitative evidence synthesis of LGBTQ+ people’s COVID-19-related loss and grief experiences reported in the literature. The review question posed was, ‘What are LGBTQ+ people’s COVID-19 loss and grief experiences?’
Author Group Positioning
The author group consists of a cross-disciplinary team (social work, occupational therapy and disability and social inclusion) of LGBTQ+ identifying people and their genuine allies; all of whom are committed to promoting the health and wellbeing of LGBTQ+ people and challenging oppressive cis-heteronormative cultural norms. The author group worked reflexively together in reviewing and synthesising the qualitative research to reduce unconsciously imposing our personal beliefs and assumptions; and to hold each member of the author group accountable in ‘doing justice’ to the LGBTQ+ voices in the qualitative research. In this way, the author group was committed in remaining mindful of the benefits and challenges of conducting research from an LGBTQ+/ally insider–outsider perspective (Nelson, 2020).
Methods
The synthesis included four steps as follows: (1) systematic search and sampling of the literature, (2) methodological quality and risk of bias assessment, (3) data extraction and (4) data synthesis (Zimmer, 2006). This review did not require formal ethical review from the Human Research Ethics Committee.
Search and Inclusion Strategy
Inclusion and Exclusion Criteria Using the SPIDER Tool.
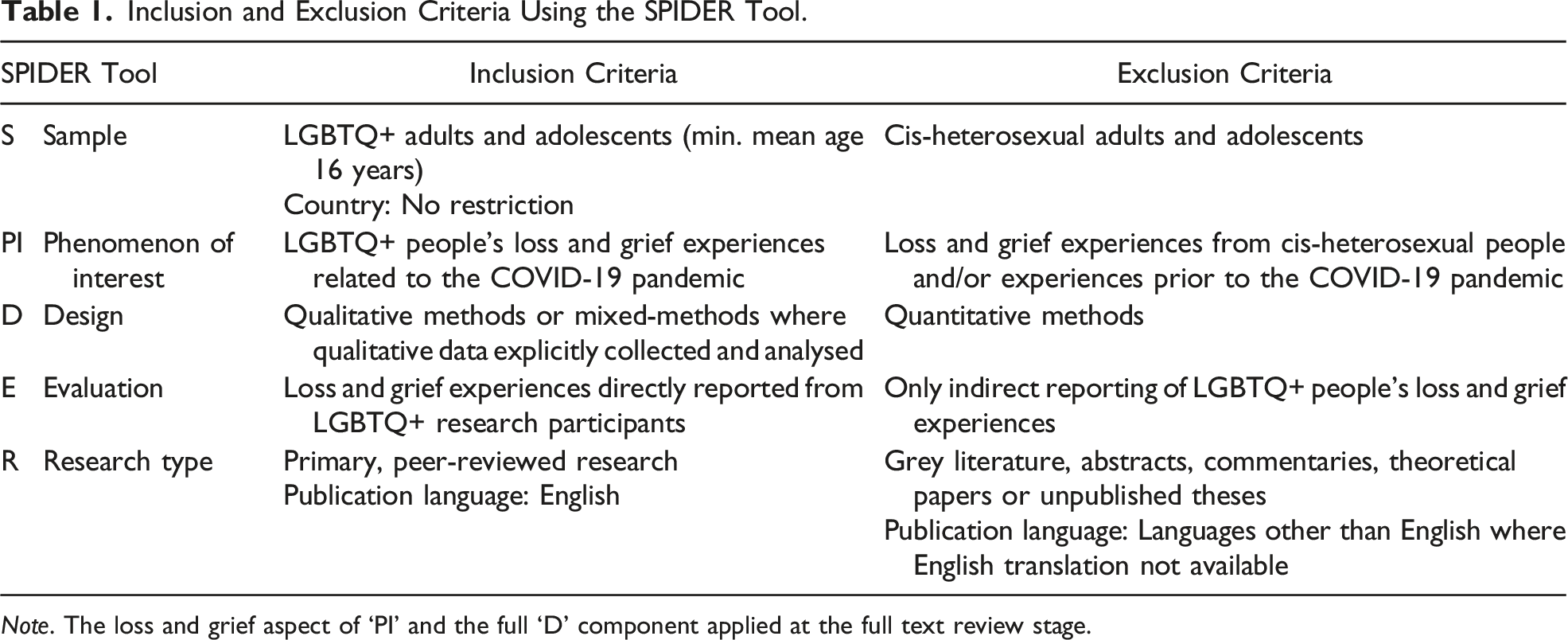
Note. The loss and grief aspect of ‘PI’ and the full ‘D’ component applied at the full text review stage.
Specific inclusion and exclusion criteria, using the SPIDER tool (Cooke et al., 2012), are outlined in Table 1. The SPIDER tool is specifically utilised for qualitative research questions. Given the identified issues with how qualitative studies are indexed in electronic databases (Cooke et al., 2012), the ‘D’ component of the SPIDER tool was not included until the full-text review stage. The ‘loss and grief experiences’ component of the ‘PI’ was also not applied until the full-text review stage as preliminary searches did not yield any relevant results (Table 1)
Two authors (JJL, SLB) independently screened the titles and abstracts of all records from the initial search yield against the inclusion and exclusion criteria. Full text articles were then retrieved for all relevant records and further reviewed for their relevance. The same two authors then cross-checked all included full-text articles and all excluded full-text articles. Any disagreements amongst the authors were discussed and resolved through consensus. If consensus was not reached, a third author (SLB-O) independently assessed the article and made the final decision. The online systematic review platform, Covidence, was utilised to facilitate the article selection and inclusion process. The results of this process are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (Page et al., 2021).
Methodological Quality and Risk of Bias Assessment
The methodological quality of the included articles was assessed using the Critical Appraisal Skills Programme’s (2018) Qualitative Checklist (CASP-Q). For each of the ten CASP-Q appraisal questions, a score of 1 (Yes), 0.5 (Unsure), or 0 (No) was selected. All articles were then provided an overall quality rating as per Butler et al.’s (2016) recommendations: ‘high-quality’ (score: 9–10), ‘moderate-quality’ (score: 7.5–8.5) and ‘low-quality’ (score: <7.5). Two authors (RA, KR) independently completed the CASP checklist for each included article. Any disagreements amongst the authors were discussed and resolved through consensus. If consensus was not reached, a third author (JJL) independently assessed the article and made the final decision. No article was excluded based on their overall quality rating, but rather informed the author group of the methodological strengths and limitations of the included article pool (Dixon-Woods et al., 2006). Sensitivity analysis (i.e., assessment of whether exclusion of inadequately reported/low methodological quality studies affected the synthesis findings) was then conducted to assess for risk of bias attributed to methodological quality (Carroll et al., 2012).
Data Extraction
Summary data from each article were initially extracted: authorship, publication year, study country, sample, phenomenon of interest, design, evaluation and research type (i.e., ‘SPIDER’). Key findings, including direct participant quotes, were also extracted from the articles. Data extraction was undertaken predominantly by one author (JJL) and checked for accuracy and completeness by a second author (SLB) using the qualitative data analysis tool, NVivo (Version 20). Any conflicts between authors not resolved through consensus were done so with the support of a third author (SLB-O).
Data Synthesis
The extracted data were then submitted to inductive thematic synthesis (Thomas & Harden, 2008; Zimmer, 2006). The first author initiated the coding by identifying phrases when reading line by line first-ordered data (direct participants quotes)- and second-order data (papers’ data analysis) from each article. Next, identified phrases were grouped into smaller meaning units that described LGBTQ+ people’s loss and grief experiences related to the COVID-19 pandemic. Similar meaning units were then grouped into larger analytical themes. Larger, overarching themes were then discussed by the research team and formed the basis of the results and the discussion in the synthesis.
Results
Quantity, Characteristics and Quality of Included Articles
Results of Screening and Selection Process
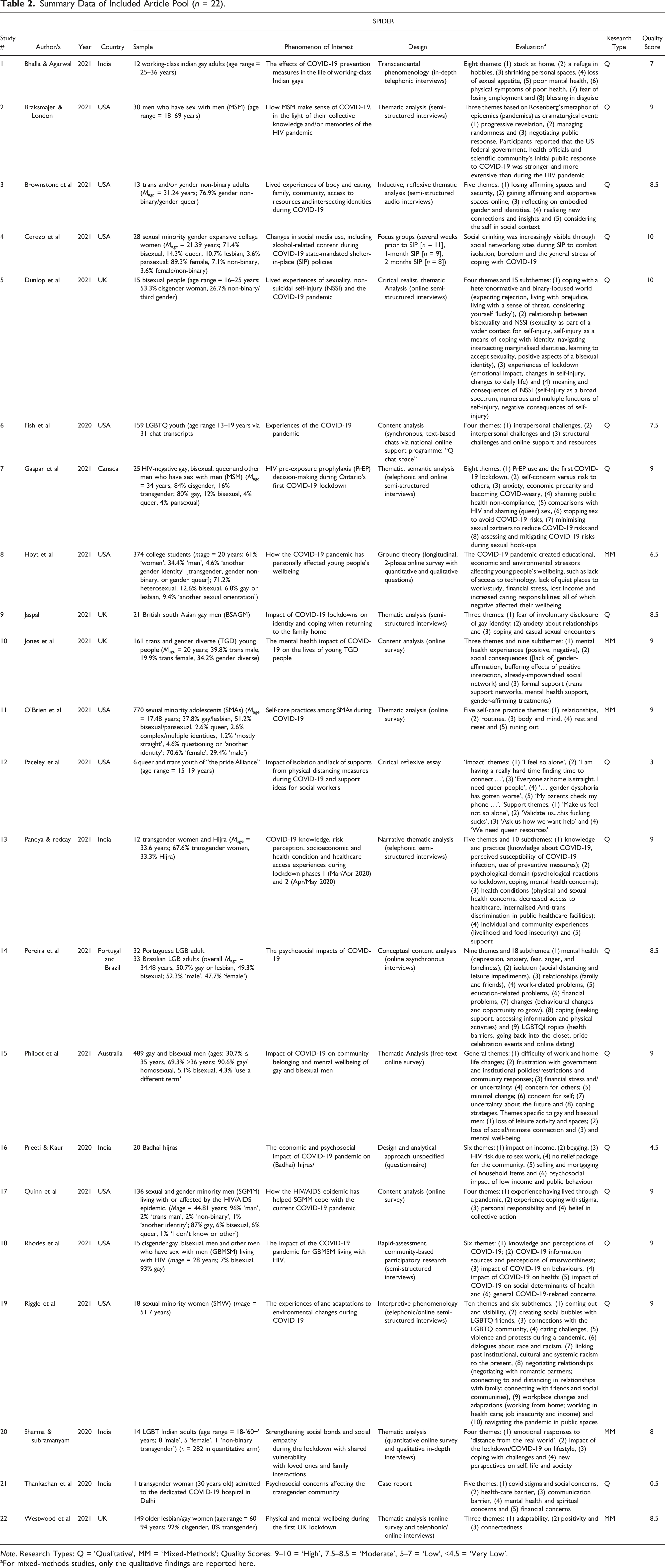
There were 1327 records retrieved using the search and inclusion strategy. An additional four records were retrieved through reference chaining. After duplicates were removed (n = 435), title and abstract screening commenced and resulted in a further 621 records being excluded. At this stage of screening, there was an 85% agreement rate between the two authors when independently reviewing the titles and abstract. All disagreements were resolved through consensus discussions, with no instances requiring a third author to make a final determination. In reviewing the full-text of the remaining records, there were 22 articles deemed eligible for inclusion in the synthesis (Figure 1; Table 2). There was an 87% agreement rate between the two authors when independently reviewing the full-text articles. There were 14 articles (5%) that required a third author to make a final determination on inclusion. All articles were published in 2020 or 2021. There were 17 (77%) qualitative articles, with the remaining five articles (23%) reporting a mixed-methods design. None of the included articles reported on LGBTQ+ people’s loss and grief via their title or abstract; rather, such information was found through the full-text review. PRISMA-2020 flow diagram of the article screening and selection process. Summary Data of Included Article Pool (n = 22). Note. Research Types: Q = ‘Qualitative’, MM = ‘Mixed-Methods’; Quality Scores: 9–10 = ‘High’, 7.5–8.5 = ‘Moderate’, 5–7 = ‘Low’, ≤4.5 = ‘Very Low’. aFor mixed-methods studies, only the qualitative findings are reported here.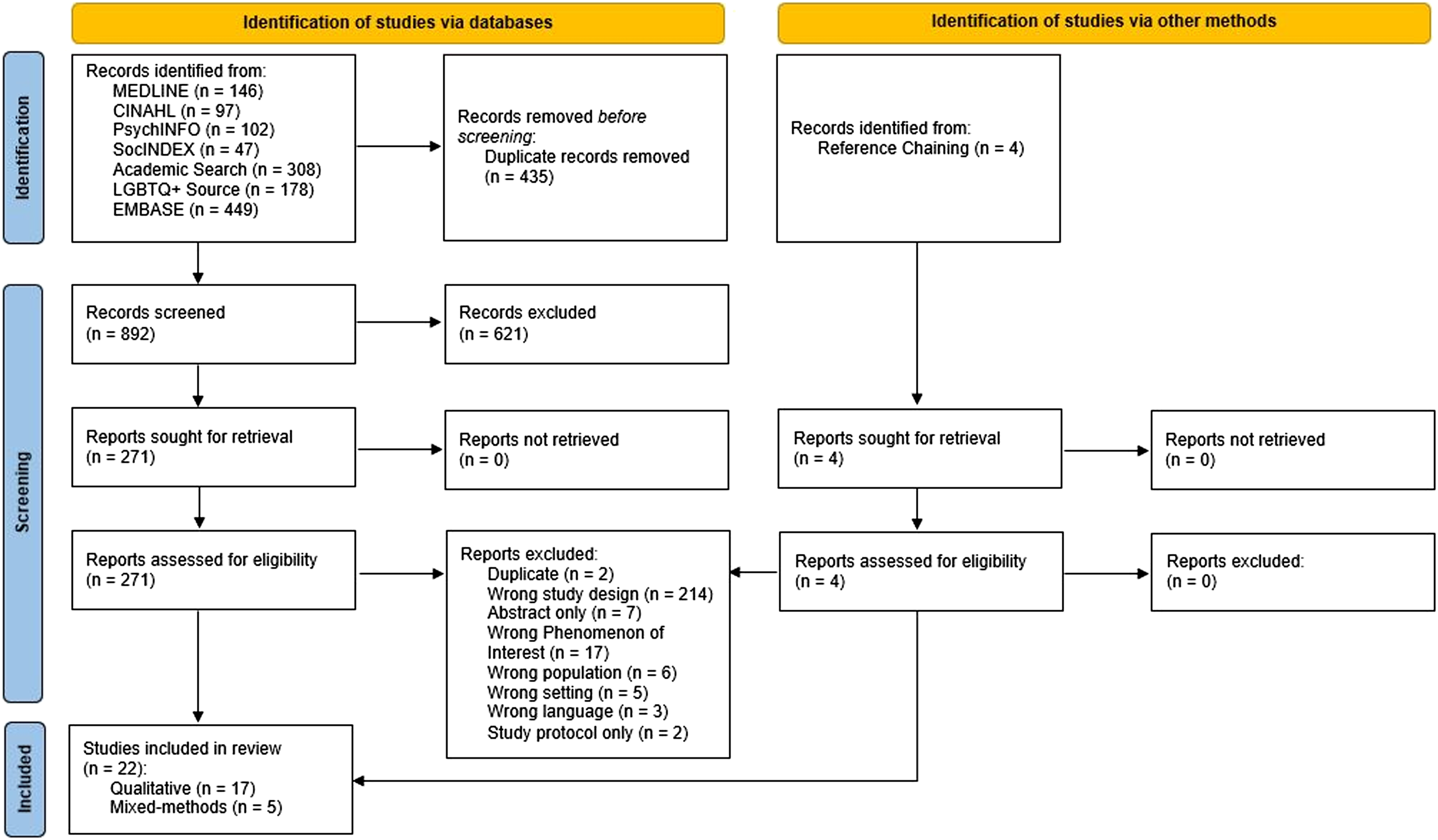
Countries
Ten articles (45.5%) reported studies undertaken in the USA. The remaining articles reported studies from India (22.7%; n = 5), UK (18.2%; n = 4), Canada (4.5%; n = 1), Australia (4.5%; n = 1) and one article (4.5%) reported a Portugal-Brazil cross-national study. The included article pool is northern-hemisphere dominant (91%; n = 20) and all include predominantly Western European countries.
Participants’ Ages, Sexualities and Gender Identities
There were approximately 2533 LGBTQ+ voices represented across the included articles. Participants’ mean ages ranged from 17.48 years to 66.4 years, with ages ranging from 15 years to 94 years. Participants’ reported sexualities and gender identities were diverse and not always possible to disaggregate across articles due to varying reporting methods of authors. Common sexualities and gender identities across the articles were lesbian, gay, bisexual, queer, pansexual, men who have sex with men, asexual, questioning, two-spirit, demisexual, cisgender woman, cisgender man, trans-woman/trans-feminine, trans-man/trans-masculine, non-binary, gender queer, agender, third gender, (Badhai) Hijra, gender fluid, gender questioning, trans and gender nonconforming.
Quality and Risk of Bias Assessment
In using the CASP-Q checklist, which contained 10 appraisal questions, the two authors (Author Initials Here) assessed 220 criteria over the 22 included articles and independently agreed on 152 items (69.1%). The majority of articles (n = 11; 50%) were rated ‘high’ quality, with six articles (27%) of ‘moderate’ quality and five articles (23%) of ‘low’ quality. Of the low quality papers, there were three that were rated of ‘very low’ quality (CASP-Q score ≤4.5) with scores of 4.5 (Preeti & Kaur, 2020), 3 (Paceley et al., 2021) and 0.5 (Thankachan et al., 2020), respectively (Table 2). The primary limitation across all articles, regardless of their overall quality rating, was in their adequately addressing the relationship between researcher/s and participants. For those articles rated ‘moderate’ or below, limitations also related to whether the analyses were of sufficient rigour. Sensitivity analysis indicated that the five articles rated ‘low’ or ‘very low’ quality did not provide unique contribution to the synthesis findings. This result, taken together with the reliance on high and moderately quality articles supported a lower risk of bias from methodological quality on the synthesis findings.
Inductive Thematic Synthesis
Through the process of inductive thematic synthesis, five themes were developed as follows: (1) loss of work and livelihood, (2) loss of social and kinship connection, (3) loss of LGBTQ+ community connection, (4) loss of physical and mental health supports and (5) loss of LGBTQ+ identity authenticity, affirmation and visibility. It is important to note that while the original aim was to review the loss and grief experiences, the literature notably focused more explicitly on the losses experienced (hence the focus on loss in this section). Not all themes involved contribution from every article, but each article contributed to at least one theme. It is important to note that these themes are not considered mutually exclusive, but rather interdependent – each having influence on the other as outlined below.
Theme 1: Loss of Work and Livelihood
The loss of work or livelihood was reported in eight articles (Bhalla & Agarwal, 2021; Brownstone et al., 2021; Pandya & Redcay, 2021; Pereira et al., 2021; Preeti & Kaur, 2020; Rhodes et al., 2020; Riggle et al., 2021; Thankachan et al., 2020). Participants across these articles described how they had lost their work and their sole source of income, they also lost their livelihoods as a result of governments’ public health lockdown measures and physical distancing (also referred to as social distancing) requirements. At times, the threat of lost work and livelihood and the anxiety around its implications for participants’ future livelihood was felt just as keenly as if it was occurring, as though in a form of preparation for the possibility. Implications for livelihoods included having no money to buy food and supplies, an inability to pay rent and (if available) living off savings.
Compounding the loss of work and livelihood was for those participants, now unable to afford living independently, being forced to move back into the family home (to avoid homelessness) where queerphobia was often present. Access to social security benefits was identified by Pandya and Redcay (2021), as a barrier to mitigating the effects of lost work and livelihoods owing to participants’ (the Indian transgender Hijra community) inability to access the required government identity documents (e.g., birth certificate). Indeed, the challenges arising from lost work and livelihood were experienced most saliently by the participants who were predominantly from India, identified as a transgender woman or Hijra, of working-class or living with HIV.
Theme 2: Loss of Social and Kinship Connection
The loss of social and kinship connection was reported across eight articles (Braksmajer & London, 2021; Gaspar et al., 2021; O'Brien et al., 2021; Pereira et al., 2021; Philpot et al., 2021; Quinn et al., 2021; Riggle et al., 2021; Westwood et al., 2021). This type of loss largely related to losses in the quality and quantity of friendships, LGBTQ+ people’s Family of Choice, their Family of Origin and romantic or sexual partners (Wheat & Thacker, 2019). Loss of these forms of connection resulted in feelings of isolation and reduced wellbeing (O'Brien et al., 2021) given their central role in social support provision for LGBTQ+ people. For example, Philpot et al. (2021) reported how Australian gay and bisexual men’s families of choice were strongly missed during the pandemic as: “they provided … supports typically believed to be entrenched in families, such as love, safety, and comfort. [They] were now no longer able to find a sense of belonging [they] would usually derive from this close personal community. (p. 6).
Pereira et al. (2021) also reported how lesbian, gay and bisexual people in Portugal and Brazil felt vulnerable and experienced low self-esteem when they were not able to maintain their friendships during the pandemic and lockdown, owing to feelings of guilt as they thought they were responsible for the lost connection. The loneliness and social isolation that arose from lost social kinship connections were so intense in some instances that suicide was seen as the only way forward (O'Brien et al., 2021). The close link between LGBTQ+ people’s loss of social and kinship connections and, the negative impact on mental health and wellbeing is well documented (Bishop, 2020).
In addition, the loss of social and kinship connections experienced during the COVID-19 pandemic resonated with the losses that LGBTQ+ people experienced during the HIV/AIDS epidemic of the 80s and 90s, particularly in terms of the new threat and subsequent actuality of loss of life from COVID-19 (Braksmajer & London, 2021; Quinn et al., 2021). The participants in Braksmajer and London (2021) and in Quinn et al.’s (2021) studies were also acutely aware of the uncertain and adverse life-changing nature of such global public health crises, but that having lived through the HIV/AIDS epidemic provided LGBTQ+ people with a sense of resilience to face such uncertainty and adversity that such crises bring (Quinn et al., 2021).
Theme 3: Loss of LGBTQ+ Community Connection
The loss of LGBTQ+ community connection was reported across three articles (Paceley et al., 2021; Philpot et al., 2021; Riggle et al., 2021). This theme relates to the loss of a sense of connection to the ‘LGBTQ+ community’ from reduced ability to attend safe LGBTQ+-specific or LGBTQ+-friendly spaces and leisure activity participation (Paceley et al., 2021; Philpot et al., 2021). In the COVID-19 pandemic, many safe LGBTQ+ spaces were closed, and associated leisure activities cancelled. The sense of personal meaning and sense of belonging derived from being immersed in these LGBTQ+ spaces and taking part in the leisure activities was subsequently lost (Philpot et al., 2021), resulting in a feeling of yearning or longing for a return to normalcy (Riggle et al., 2021).
In addition, lost access to LGBTQ+ spaces were further compounded from living with non-affirming, often unsupportive family in an effort to avoid homelessness during lockdown periods (Paceley et al., 2021). In instances where no loss of connection was experienced, some LGBTQ+ people attributed this absence to their privileged positioning as ‘largely white, middle-class men, who most likely had access to available resources to remain ‘safe’ during COVID-19 restrictions’ (Philpot et al., 2021, p. 6), thus shedding light on the intersectionality between sexuality, gender identity, class and culture in shaping LGBTQ+ community connection during the pandemic. The worry over the threat of losing such connection, nonetheless, was felt even in such privilege.
Theme 4: Loss of Physical and Mental Health Supports
The loss of physical and mental health supports was reported across four articles (Fish et al., 2020; Hoyt et al., 2021; Jones et al., 2021; Paceley et al., 2021). This theme relates to the loss of formal supports normally accessed in-person via school welfare services, medical clinics, and mental health services. While some of the services became accessible via telehealth arrangements, this online access was for some an additional barrier to fostering positive health and wellbeing during the COVID-19 pandemic as privacy at home was not guaranteed. For example, in Fish et al.’s (2020) article, LGBTQ+ youth in the USA described hesitancy in utilising telehealth services out of fear that their unsupportive parents would overhear their conversations with the therapists.
For the LGBTQ+ young adults in Hoyt et al.’s (2021) article, the loss of access to mental health services delivered via USA college-based programmes was exacerbated by, as one lesbian participant stated, having to ‘leave all my support at school and come back to a homophobic household where I have to remain in the closet’ (p. 6). As such, there was a subsequent loss of connection with ‘supportive, affirming, and trusted mentors and friends’ (Paceley et al., 2021, p. 10). In instances where access to formal telehealth community support was possible in lieu of in-person support, barriers to engagement included ‘timely referral to the services was low due to an overwhelmed system’ (Jones et al., 2021, p. 9). For the young trans and gender diverse people in Jones et al.’s (2021) article, this barrier meant lost access to gender-affirming medical services and interventions (e.g., gender-affirmation hormone treatment and surgery). This loss was additional to lost access to non-medical gender-affirming interventions (e.g., haircuts) crucial for authentic gender expression and maintaining overall mental health and wellbeing.
Theme 5: Loss of LGBTQ+ Identity Authenticity, Affirmation and Visibility
The loss of LGBTQ+ identity authenticity, affirmation and visibility were reported across six articles (Brownstone et al., 2021; Cerezo et al., 2021; Dunlop et al., 2021; Jaspal, 2021; Jones et al., 2021; Sharma & Subramanyam, 2020). This theme was perhaps the most significant in that it appeared that the culmination of the losses in the other themes, created a sense of loss of LGBTQ+ identity authenticity, affirmation and visibility. For example, participants who were forced to disconnect from their LGBTQ+ family kinships (i.e., Theme 3) and live in the family home with unsupportive, queerphobic parents resulted the loss of identity authenticity from having to conceal their LGBTQ+ selves from their loved ones to remain safe (Brownstone et al., 2021; Jaspal, 2021; Sharma & Subramanyam, 2020). At times, living in this way combined with living in a largely unaccepting society felt like a suffocating cage, as one LGBTQ+ adult in India expressed: … spending time with family when you are not open, was already like a cage, with family having lot of expectations and along with societal pressures and humiliations. Closing in (being confined to) a non-accepting society and with high-in-expectation family members is destroying my mental health in COVID-19 times. I want to go away from this Society and breathe in fresh air once again where I will not be judged for how I was born. (Sharma & Subramanyam, 2020, p. 13)
While physical freedom from a restrictive and non-affirming living situation forced an inauthentic existence of hiding one’s LGBTQ+ identity during government-mandated lockdowns, for some there was escape via social media and other online avenues (Cerezo et al., 2021; Jones et al., 2021).
In addition, the loss of authenticity, affirmation and visibility was experienced in the context of seeking support to manage the stress and anxiety from living in non-affirming and inauthentic environments. For example, Jones et al. (2021) reported how the loss of affirming formal support via community organisations (i.e., Theme 4) for young trans and gender diverse people in the UK left them feeling ‘invisible and invalidated’ (p. 9) and thus reinforcing a sense of isolation that existed prior to the COVID-19 pandemic.
Discussion
The purpose of this review was to synthesise the COVID-19-related loss and grief experiences of LGBTQ+ people reported in the qualitative research. Overall, the diversity of experiences was focused on feelings of loss that were sustained rather than grief per se. In particular, lost work and livelihoods, lost connection from social and kinship relationships and from the LGBTQ+ community. Lost access to physical and mental health supports as well as experiencing lost LGBTQ+ identity authenticity, affirmation and visibility was prominent. These losses and associated grief experiences operated in various ways in the lives of the LGBTQ+ people.
The loss of work and livelihood that was experienced during the lockdown periods, coupled with the loss of physical connection with LGBTQ+ friends, chosen LGBTQ+ family and with sexual partners are what Weenolsen (1988, 1991) called ‘secondary losses’ in that the concrete losses directly related to another concrete ‘primary loss’ event. The losses included the loss of physical movement due to government-imposed lockdowns or the loss of safe LGBTQ+ spaces and leisure activities. These concrete forms of loss are more readily visible and their effects (e.g., loss of income, food security and overall wellbeing) are more open to formal government and non-government support, for example, government income support payments, moratoriums on rental eviction during lockdown and a reduction in interest rates.
Threatened primary and secondary losses, such as the threat of losing work and their sole income source (e.g., Bhalla & Agarwal, 2021), was for some LGBTQ+ people just as anxiety-provoking as an actual loss in a form of anticipatory or ‘pre-loss’ grief experience that prepares the person for potential future loss (Reynolds & Botha, 2006; Weenolsen, 1988, 1991). As such, in supporting LGBTQ+ people during the pandemic, it will be important for health workers to address both actual and threatened loss to avoid making invisible or disenfranchising LGBTQ+ people from their pre-loss grief experiences (Doka, 2008; Thompson & Doka, 2017).
While supports to mitigate the effects of these primary and secondary losses are made available, unfortunately accessing those supports are not always straightforward or even possible as seen for members of the Indian Hijra community who lacked the government identity evidence required to access social security benefits during the pandemic (Pandya & Redcay, 2021). A consequence of such situations is the further marginalisation and oppression of certain groups in society through sending the message: ‘you don’t belong’, forcing either assimilation or isolation. These messages are often experienced not only by LGBTQ+ communities but across many other marginalised groups in society, such as refugees and asylum seekers (Robinson, 2014) and the world’s First Nations peoples (Nolan-Isles et al., 2021). Health policy and interventions focused on addressing the negative impact of primary and secondary loss need therefore to be designed in a way that does not further contribute to the marginalisation of LGBTQ+ people.
In terms of lost sense of connection with LGBTQ+ social and kinship relationships as well as with the ‘queer community’, these forms of loss relate to changes in social status and identities, future plans and opportunities and beliefs about how the world, society and life operates (Weenolsen, 1988, 1991). The feelings of loss are also related to the experiences of losing personal meaning in life, such as what was experienced from the lost sense of ‘love, safety, and comfort’ (Philpot et al., 2021, p. 6) from connection with the LGBTQ+ community and associated LGBTQ+ kinship relationships. These more subtle, yet just as acutely felt losses are not so open to verbal articulation, visibility or necessarily of focus in formal community supports (Weenolsen, 1988, 1991) and are therefore more susceptible to disenfranchisement (Doka, 2008; Thompson & Doka, 2017).
The current synthesis findings resulted in the identification of various instances where LGBTQ+ people felt the non-affirming, ‘suffocating cage’ of hiding their LGBTQ+ identity. Their true selves were rendered invisible as they were not able to connect with their LGBTQ+ family and community and thus felt a sense of loss. This form of disenfranchised, personally chosen yet socially imposed, self-conceptual loss has been documented in previous non-COVID-related research (McNutt & Yakushko, 2013; Prasad, 2020; Wheat & Thacker, 2019). In giving voice to such losses, it will be important for health workers to bear witness in genuinely listening to this hidden Queerstory and promoting LGBTQ+ resilience, strength and hope through their practice.
The synthesis findings highlighted how certain combinations of intersecting social identities (e.g., age, gender, sexuality, class and culture) are afforded certain privileges, while other combinations are systematically marginalised or oppressed (Crenshaw, 1989; Gkiouleka et al., 2018). For example, the eight articles that contributed to the first theme of lost work and livelihood included participants from predominantly Brown, Black or Latinx countries of low socioeconomic status (India or Brazil) who identified as a transgender woman or Hijra, of working-class or living with HIV. This compares with the eight articles that contributed to the second theme of lost social and kinship connection in which the participants were predominantly from largely White-European countries of higher socioeconomic status (USA, UK, Canada, Australia, Portugal), who identified as cis-male, and gay or lesbian.
This contrasting focus between concrete losses related to physical survival versus abstract losses related to connection and relationship suggests intersecting oppressions imposed and privileges afforded to certain sexualities, genders, social classes and cultures by a cis-heteronormative society within a pandemic. This phenomenon has been seen in other pandemics such as the HIV/AIDS epidemic (Abreu et al., 2021; Braksmajer & London, 2021; Quinn et al., 2021). In the cis-heteronormative societies that dominate the world’s countries, the closer a person’s identities align with or assimilate into the ‘ideal’ (i.e., cis-gendered, heterosexual, white-European, religious, middle/upper class adult) the higher the societal privilege – the converse often leading to social exclusion, isolation and oppression (Chan & Henesy, 2018). Intersectionality is an important factor in LGBTQ+ life and identity and important for health practitioners to take into consideration to avoid ironically contributing to marginalisation in the name of belonging and social connection (McNair, 2017).
Limitations and Future Research Directions
While this synthesis provided insight into the loss experiences of LGBTQ+ people during the COVID-19 pandemic, it cannot be extrapolated to the potential grief involved, nor to the full breadth of LGBTQ+ lived experience reported in the qualitative literature. Repeating the synthesis with perhaps a revised set of inclusion criteria is suggested to explore such pandemic-related LGBTQ+ lived experience in greater depth. How LGBTQ+ people who lived through the HIV/AIDS pandemic experienced the current COVID-19 pandemic, in terms of their resilience, growth and meaning reconstruction may further contribute to a narrative of strength, hope and meaning within the qualitative literature (Walsh, 2020).
In the synthesis, it was not possible to disaggregate participants’ sexualities and gender identities, which limits exploration of how intersecting identities influence loss (and grief) within a cis-heteronormative world. Future research that aids such disaggregation while also resisting the cis-heteronormative drive to categorise or create binaries from fluid concepts is warranted. Translation of the synthesis findings into health practice can focus on how non-medicalised approaches to cultivating people’s belonging and social connectedness (e.g., social prescribing) (Zurynski et al., 2020), also known as the ‘connection prescription’ (Martino et al., 2017), can be ‘queer-loss-informed’ to make visible the concrete and abstract loss experienced and ensure LGBTQ+ identities and lived experiences during this global health crisis are enfranchised.
Conclusion
Loss and grief for LGBTQ+ people share commonalities with their cis-heterosexual counterparts, as well as a uniqueness owing to living ‘queer’, that is as a LGBTQ+ person, within a cis-heteronormative society. The COVID-19 pandemic has brought new and has amplified existing, challenges regarding loss – particularly in being afforded (or not) the right to experience loss as a LGBTQ+ person. This article is the first to present the qualitative experiences of LGBTQ+ people’s COVID-19-related losses published in the literature and provides insight into the many layered and often disenfranchised nature of LGBTQ+ people’s loss and grief during times of pandemic brought about by dominant cis-heteronormative cultural norms that pervade many of the world’s societies. In challenging cis-heteronormativity during the COVID-19 pandemic, it is important that health workers and services elevate, making visible, these voices and lived experiences of LGBTQ+ people. One step in this direction is through consideration of the sense of relationship, community and identity authenticity that underscores many of the COVID-19-related loss experiences reported internationally in this synthesis.
Supplemental Material
Supplemental Material - LGBTQ+ Loss and Grief in a Cis-Heteronormative Pandemic: A Qualitative Evidence Synthesis of the COVID-19 Literature
Supplemental Material for LGBTQ+ Loss and Grief in a Cis-Heteronormative Pandemic: A Qualitative Evidence Synthesis of the COVID-19 Literature by James J. Lucas, Stéphane L. Bouchoucha, Rojan Afrouz, Kirk Reed, and Sharon L. Brennan-Olsen in Qualitative Health Research
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.