
Abstract
Understanding and respecting different linguistic and socio-cultural needs of health service users is critical to design, adapt and provide appropriate health services. We explored access to male family planning methods in The Democratic Republic of Timor-Leste, a linguistically and culturally diverse nation, by conducting 14 participatory group discussions (PGDs) with 175 participants across seven municipalities. Participants (84 men and 91 women, aged 18 to 72) spoke 13 different languages. PGDs were audio-recorded and translated to English using a multilingual panel translation approach that enabled rigorous and reflexive discussion and learning between researchers about context and meaning. Planning for language diversity helped us to centre participant voices and to hear perspectives that may have otherwise been excluded or misrepresented. Our study affirms the need for research teams to include diverse members who help ensure meaning and voice is not lost across cultural and linguistic differences. Linguistic respect, inclusion and transparency are required to realise improved health and development outcomes.
Introduction
Understanding and respecting different linguistic and socio-cultural needs of health service users is critical to design, adapt and provide appropriate health services. Qualitative research can provide insights to help guide health policy and programmatic decision-making, particularly when research is conducted in an inclusive and participant-centred way. Key to this is effectively factoring into research design the diversity of languages spoken and the communication styles used across and within communities.
Qualitative research conducted by researchers who speak the same language as their research participants is appropriate and avoids many of the limitations associated with the use of translators or interpreters (van Nes et al., 2010). However, this approach becomes more complex when working in multilingual contexts. Logistical, practical and social factors may all contribute to challenges in identifying appropriate researchers who speak the same language as participants, resulting in the need to limit participant inclusion by language use or incorporate translation processes into research design (Squires, 2009; Temple, 2002). Indeed, if not effectively factored into research design, the use of language and translation itself has the power to reinforce longstanding cross-cultural relationships and power imbalances, or to exclude people from full and meaningful participation (Hole, 2007; Oxley et al., 2017; Temple & Young, 2004). Temple and Young (2004) argue that ‘The relationships between languages and researchers, translators and the people they seek to represent are as crucial as issues of which word is best in a sentence in a language’ (Temple & Young, 2004, p. 164).
Study context
The Democratic Republic of Timor-Leste (Timor-Leste) is a small and mountainous half-island nation in South-East Asia (World Health Organisation, 2022). With an estimated population of 1.318 million and a median age of 20.8 years, it is the 29th youngest population in the world (United Nations Department of Economic and Social Affairs Population Division, 2019). Most people live in rural locations (70.6%) and identify as Catholic (97.6%) (General Directorate of Statistics Timor-Leste, 2015). Archaeological, ethnographic, linguistic and genetic research indicates a long and rich history of multilingualism, with migrations of many different ethnic groups dating back for at least 42,000 years (Gomes et al., 2015; Hawkins et al., 2017).
Timor-Leste has a complex history of colonisation by Portugal (formally colonised from 1702 to 1975, although Portuguese travellers impacted Timor from as early as 1515), and violent occupation by Japan (1942–1945) and Indonesia (1975–1999) (Government of the Democratic Republic of Timor Leste, 2021). A referendum in 1999 resulted in the majority of voters (80%) opting for independence from Indonesia (Kingsbury, 2012). Timor-Leste was administered by a United Nations mission until full independence was restored in 2002 (Government of the Democratic Republic of Timor Leste, 2021).
One of the many impacts of colonisation and occupation is the significant influence on shaping language and communication across Timor-Leste. During Portuguese colonisation, Portuguese language was used within governance systems and the Catholic Church (Taylor-Leech, 2008). During Indonesian occupation, Bahasa Indonesia (Indonesian language) was enforced in institutional structures, including the education and health systems (Taylor-Leech, 2009). The repression of Portuguese language during Indonesian occupation helped build the status of the Timorese language, Tetun Prasa (Tetun), as a unifying symbol of national identity, and the language used by the Timorese Catholic clergy (Taylor-Leech, 2008; Williams-Van Klinken & Hajek, 2018). Until 1999, Tetun was a predominantly oral language used mostly in informal settings, with the exception of the Catholic Church (Williams-Van Klinken & Hajek, 2018). During the United Nations administration of Timor-Leste (1999–2002), English was rapidly introduced as a key language for governance and planning purposes, including within the health sector (Taylor-Leech, 2009).
Tetun and Portuguese were adopted after independence as co-official languages, with Indonesian and English designated as ‘working languages’ (Cabral et al., 2021). More than 30 other languages spoken across Timor-Leste are considered ‘national languages’ (Cabral et al., 2021; General Directorate of Statistics Timor-Leste, 2015), which is the terminology we use in this paper. We also use the government classification and spelling of national languages, defined in the 2015 Census, although we acknowledge that differences and debates exist about the classification and total number of these national languages, along with how data are collected around language use (Cabral et al., 2021; Williams-Van Klinken & Hajek, 2018; Williams-van Klinken & Williams, 2015; Williams-van Klinken et al., 2016).
Population of Timor-Leste by mother tongue language, second language and third language spoken as directly provided in 2015 Census data (General Directorate of Statistics Timor-Leste, 2015).
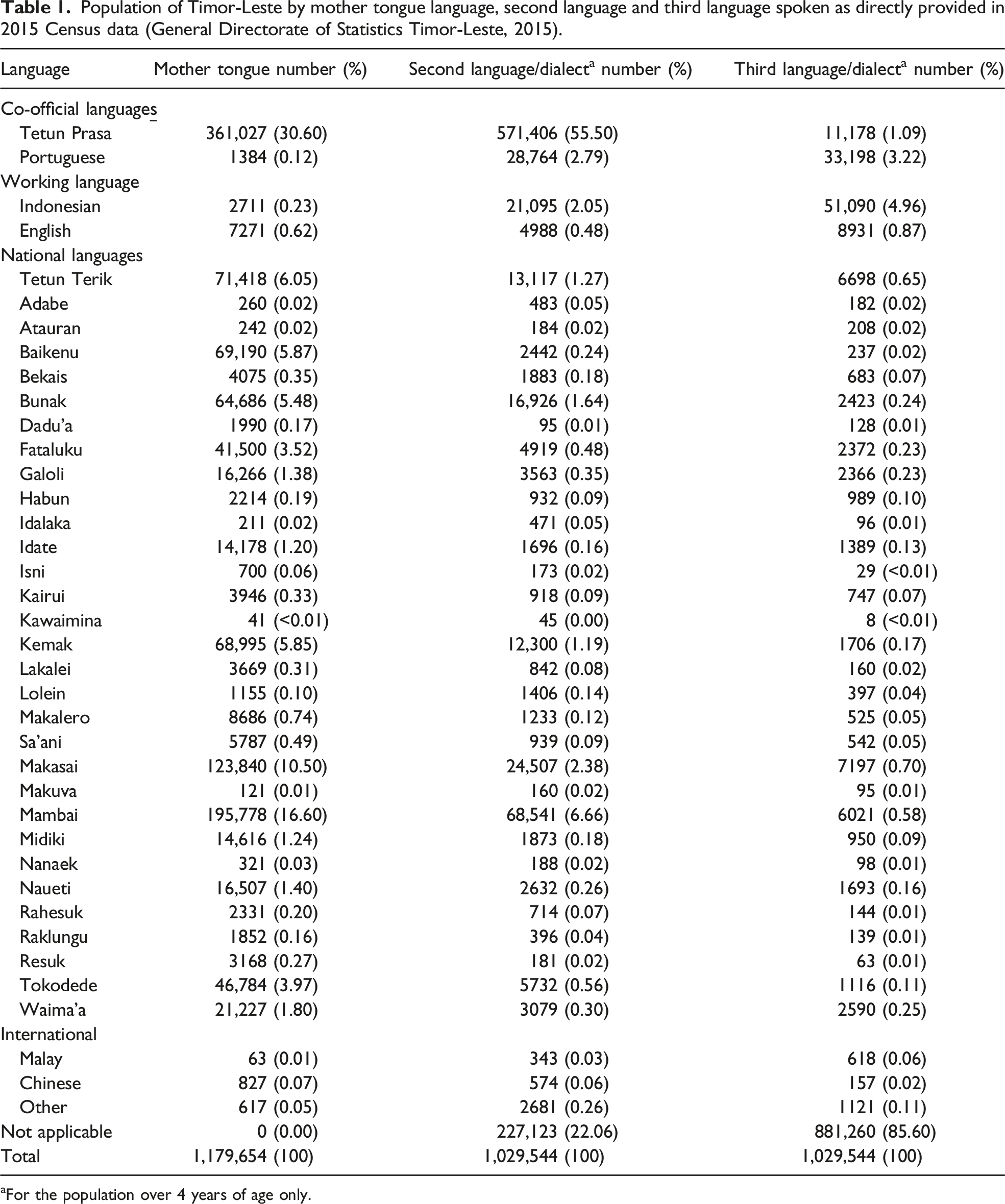
aFor the population over 4 years of age only.
Language remains a complex and important factor in national governance and society. For example, language policy and practice within the education system continues to be researched and debated (Newman, 2021; Taylor-Leech, 2013). Less documentation exists about language policy and practice in the Timor-Leste health sector, including within important and specific health areas, such as sexual and reproductive health (SRH).
Sexual and reproductive health and rights in Timor-Leste
Timor-Leste has made remarkable progress in improving SRH outcomes over the last 20 years, with significant reductions in maternal mortality and total fertility rates (Alkema et al., 2016; General Directorate of Statistics, Ministry of Health, & ICF, 2018). Challenges remain around several key SRH indicators, however, including access and uptake of comprehensive family planning services. The modern contraceptive prevalence is low, with just 24% of married women of reproductive age using a modern method of family planning in 2016 (General Directorate of Statistics, Ministry of Health, & ICF, 2018). While studies have explored understanding of and influences to women’s uptake of family planning methods in Timor-Leste (Wallace et al., 2018), limited evidence exists about male methods of family planning. Male methods of family planning include methods that require men’s direct use or cooperation, including condoms, vasectomy and certain natural family planning methods (Ross & Hardee, 2016; World Health Organisation, 2018). The use of male methods of family planning accounted for 27.4% of family planning practice worldwide in 2019 (United Nations Department of Economic and Social Affairs, 2019). Available data shows that access and use of male family planning methods in Timor-Leste is lower than global comparisons, with less than one in 10 men reporting ever use of male methods in 2009 (more recent data not available) (United Nations Department of Economic and Social Affairs, 2019)
We explored the beliefs, understanding and access to male family planning using operational and participatory research methods that respect and celebrate Indigenous knowledge and language diversity in Timor-Leste. We acknowledge Timor-Leste’s complex history and current context, and the importance, both methodological and political, of the languages used in our research. In this paper, we aim to demonstrate the effectiveness of using a multilingual panel translation approach to gain comprehensive and contextually accurate insights about sexual and reproductive health and rights (SRHR) through a robust and inclusive process that ensures voices of participants remain central.
Methods
Research team
Our multilingual field research team included two female (AS, SM) and two male (MS, HSX) Timorese from four municipalities in Timor-Leste (Ainaro, Baucau, Bobonaro and Manufahi). They each speak four to six languages, collectively speaking 16 languages (Bunak, English, Fataluku, Galoli/Galolen, Indonesian, Kairui, Kemak, Lakalei, Lolein, Makalero, Makasai, Mambai, Portuguese, Tetun Prasa, Tetun Terik and Waima’a). They are all proficient in spoken and written English, meeting all of the language knowledge competency skills identified by Squires (Squires, 2008). The fifth field research team member (HH) is a white Australian woman who has lived and worked in Timor-Leste since 2012. Her first language is English, she is proficient in spoken and written Tetun and has beginner Indonesian language skills.
At the time of data collection (August to December 2019, just prior to the start of the COVID-19 pandemic), we all worked for Marie Stopes Timor-Leste (MSTL), an SRH specialist organisation, working in partnership with the Timor-Leste Ministry of Health. We had established productive and trusting professional relationships and extensive experience as a team working in Timor-Leste conducting community outreach, health promotion, health services and research. As individuals, we were all new to at least one element of the research (for example, cultural understanding or scientific process). As a group, we had practical experience of how language use can exclude or limit community participation in health and research in Timor-Leste and wanted to actively address this in our research design and approach to language use.
We used the ethics of reflexivity and solidarity at all stages of our research process, both as individuals and as a team. Our reflexive approach involved regular team discussion about what worked well and what could be improved (Barry et al., 1999). At an individual level we used reflexive practice (for example, writing in a reflexive research journal) to track and explore our own beliefs, positionality, knowledge and assumptions.
We worked closely with key stakeholders, including two professional translators, in the design of the research questions and methodology, including our approach to language use and translation. Technical support and expert guidance was provided by three experienced and multi-disciplinary health and research supervisors, one based in Dili, Timor-Leste (RA) and two based in Melbourne, Australia (CV, MAB).
Study design
We conducted participatory group discussions (PGDs) with community members across seven municipalities in Timor-Leste (Ainaro, Baucau, Bobonaro, Dili, Lautem, Manufahi and Oecusse). We recruited participants purposively based on their age, gender and location. A minimum age of 18 years was required for participation. We conducted two PGDs in each study municipality, visiting both a rural and urban location. Within each PGD, participants were invited into age and gender-specific groups to participate in three activities: 1) body mapping; 2) talking about a fictional Timorese couple (vignettes) and 3) engaging in a facilitated discussion about family planning methods, using national health promotion tools and example contraceptive methods as prompts.
We co-led the gender specific group activities in pairs, which supported us to effectively manage the flow of research activities, build rapport, be adaptable with language use and deeply listen to participants. After the research activities were complete, participants were invited to join an SRHR education session. The PGD process is described in Figure 1. Overview of PGD process.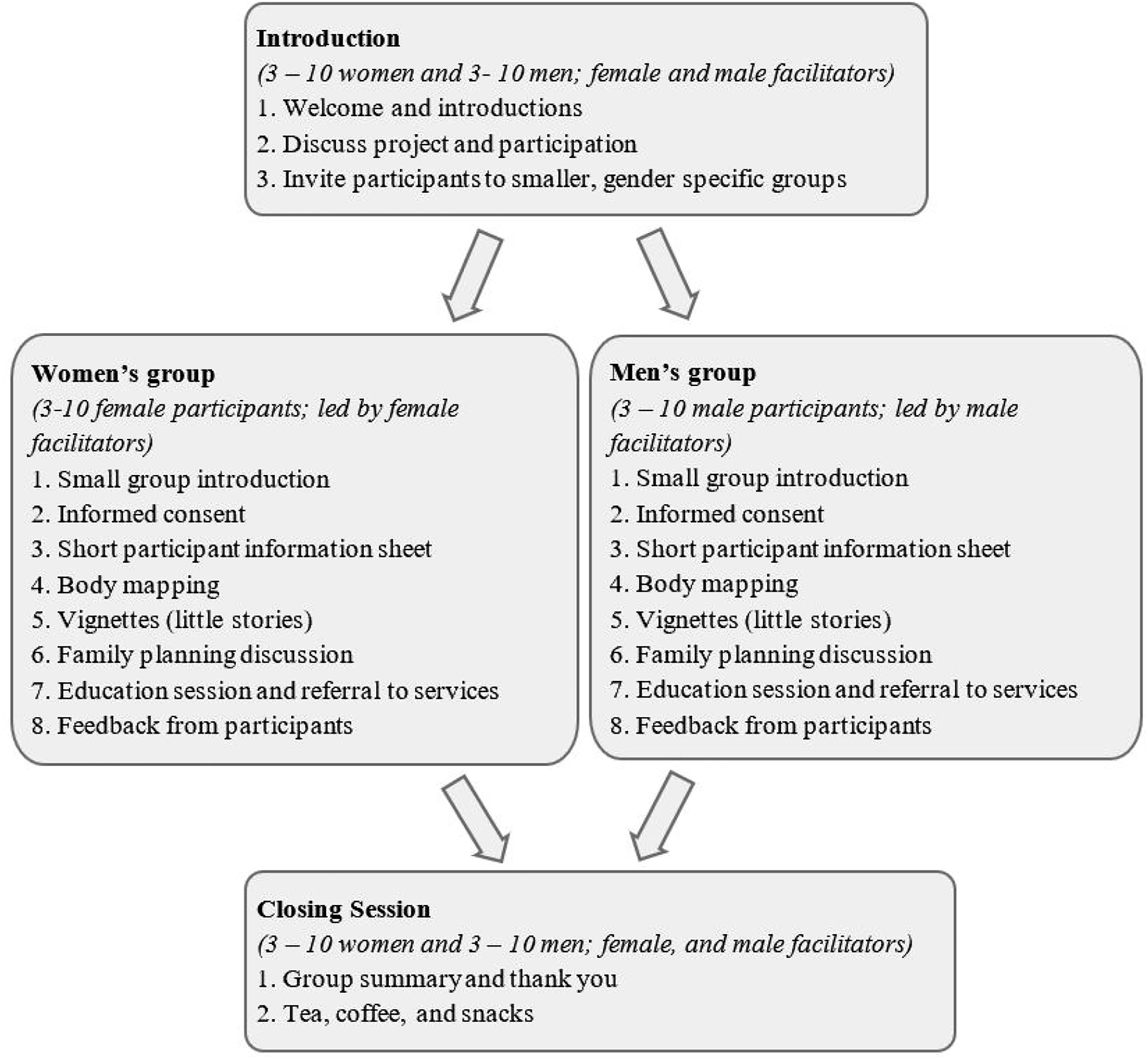
The PGD exercises were designed and piloted in Tetun. They were initially explained to participants in Tetun and then conducted in Tetun or another language, depending on the language preference of the participants and language ability of the researcher. We encouraged participants to use the language they felt most comfortable using when expressing themselves verbally or if writing words in the body map exercises.
Data collection
Data collection occurred from August to December 2019, after receiving ethics approval from the National Health Institute of Timor-Leste, the University of Melbourne in Australia, and MSI Reproductive Choices in London, UK. Written consent (in Tetun) and verbal informed consent (in the language preference of the participant) were provided by all participants. A plain language information statement was provided to all participants in Tetun and included phone numbers for participants to use if wanting to verbally discuss the research at a later date with us or any of the involved ethics committees.
Across all research activities, a total of 13 different languages were used by participants: Tetun, Portuguese, Indonesian, English, Tetun Terik, Baikenu, Bunak, Fataluku, Kairui, Kemak, Lakalei, Makasai and Mambai. Most participants spoke in Tetun or a mix of Tetun with one of the national languages in Timor-Leste and/or Indonesian. For example, a male PGD group in Manufahi was conducted in a mix of Tetun and Mambai, with some participants speaking only in Mambai; a male PGD in Bobonaro was held in Tetun and Bunak, with some participants only speaking in Bunak and a female PGD in Baucau was held in Tetun and Makasai, with some participants only speaking in Makasai. In these examples, at least one of the field research team members was fluent in the language spoken by the participants and was able to freely communicate.
Several PGD participants spoke in a mix of Tetun with Portuguese or Tetun with English. Several participants preferred to fully use either their national language or Indonesian. For example, a female PGD in Lautem was held in Tetun and Indonesian, with some participants only communicating in Indonesian not as their first language, but as the most comfortable common language between participant and the researchers.
Three participants communicated in Tetun and a national language not understood by the field research team. While understanding and speaking some Tetun, these three participants felt more comfortable or confident speaking the language of their choice, rather than adapting to speak a language common with the field research team. When this occurred, we ensured the participant knew we could not understand the language but still wanted to listen, and that we would get translation support after the research activities. We also reminded these participants that they did not have to say anything they did not feel comfortable sharing and that their participation was de-identified and confidential. Translation support was provided later by a professional translator, employed by MSTL.
While some body mapping images contained written descriptions in different languages, most were pictorial and had no writing at all. After completing the body mapping activities as a group, participants would briefly speak one-on-one with a research team member, providing a verbal description about their completed body map design.
Multilingual panel translation
As a research team, we gathered as soon as possible after conducting the PGDs to discuss data collection and start the multilingual panel translation process. This practice was informed by ethnographic reproductive decision-making research carried out in Micronesia, Pakistan and Timor-Leste (Brewis, 1994; Mumtaz & Salway, 2009; Wallace, 2019). We played the audio recordings from the PGDs and the five multilingual members of the research team translated the recordings verbally to English, with a focus on contextual interpretation rather than literal translation. English was chosen to be the primary language for translation and transcription, as a common language of the research team and due to its wide technical vocabulary to translate both words and meaning. This vocabulary range was important as non-Tetun language was often used by participants when describing words or themes that were not easily available in Tetun language. Lack of technical terminology in Tetun most likely contributed to the increased multilingualism within the SRHR discussions, as has been described in other health and education literature (de Araujo, 2001; Newman, 2021). However, as described below, translating the data to English as the one common language also has notable study limitations and implications.
Translation from the audio recordings was informed by an ‘early phase’ translation process, as described and recommended by Santos et al. (2015). The process of early phase translation provides an early, interactive process for researchers to engage with the data collected, which is especially useful for those who do not speak the language used in data collection (Santos et al., 2015). This was especially important for HH as a foreigner living in Timor-Leste with only Tetun and limited Indonesian language skills. She was dependent on her co-researchers for translation of other languages spoken and contextual translation. This process was also important for the Timorese researchers who each had different national language skills and contextual frameworks within Timor-Leste.
The panel translation process started immediately after the field research began in August 2019 and continued until February 2020, at which point approximately 85% of the translation had been completed. The process was paused from March to September 2020 due to logistical impacts from the COVID-19 pandemic. The remaining 15% of the translation occurred between October and December 2020.
The panel translation process involved the field research team listening to a short segment of audio once or several times as a team and then verbally translating the recording into English. This verbal translation process was audio-recorded. HH transcribed the English translation and took notes during these sessions. We also took turns transcribing selected quotes and phrases in the primary language of the participants. We referred to English, Tetun, Portuguese and Indonesian dictionaries for spelling support. This panel translation process was mostly straight-forward, with the panel usually unified in agreement about the linguistic and contextual translation. When there were questions or ambiguity in what was being said, we established a process for review which involved playing the audio back several times, writing the words verbatim in the primary language used and then translating this written text into English. This process was necessary when some participants used colloquial or locally specific language or concepts that could be interpreted in different ways.
An audit trail of discrepancies, ambiguities and translation decision-making processes was kept (Santos et al., 2015). When necessary, a professional translator (fluent in Tetun, English, Indonesian, Kairui, Portuguese, Spanish and Waima’a) was asked to confirm or verify the translation of certain words and concepts that we were unable to resolve or agree on alone. This professional translator was employed by MSTL, had extensive experience translating SRHR terminology and concepts, and was familiar with the research design. Although not part of the regular translation panel due to logistical constraints, they were a valuable resource to call upon throughout all stages of the research project.
HH cleaned and finalised the verbatim transcripts in English using the audio recordings of the panel translation sessions. The selected quotes and phrases transcribed in the language of data collection were included in these transcripts. The completed transcripts were read and verified by the Timorese members of the field research team. Again, if there was a discrepancy or query, the team went back to the original audio recording from the PGD, listened to, translated and verified as appropriate.
Body maps and transcription data were uploaded into the computer program NVivo (NVivo qualitative data analysis software, 2018) for storage and data management. Data were then analysed using thematic and content analysis (Braun & Clarke, 2006). The first round of systematic data coding was conducted as a team and occurred in a mix of English and Tetun. A plain language report was produced in English and Tetun and shared with key stakeholders. Findings were also shared verbally in the national languages of participants, through municipality-based educators and team members, employed by MSTL. Refer to Figure 2 for an overall summary of language use during the research process. Language use in the research process.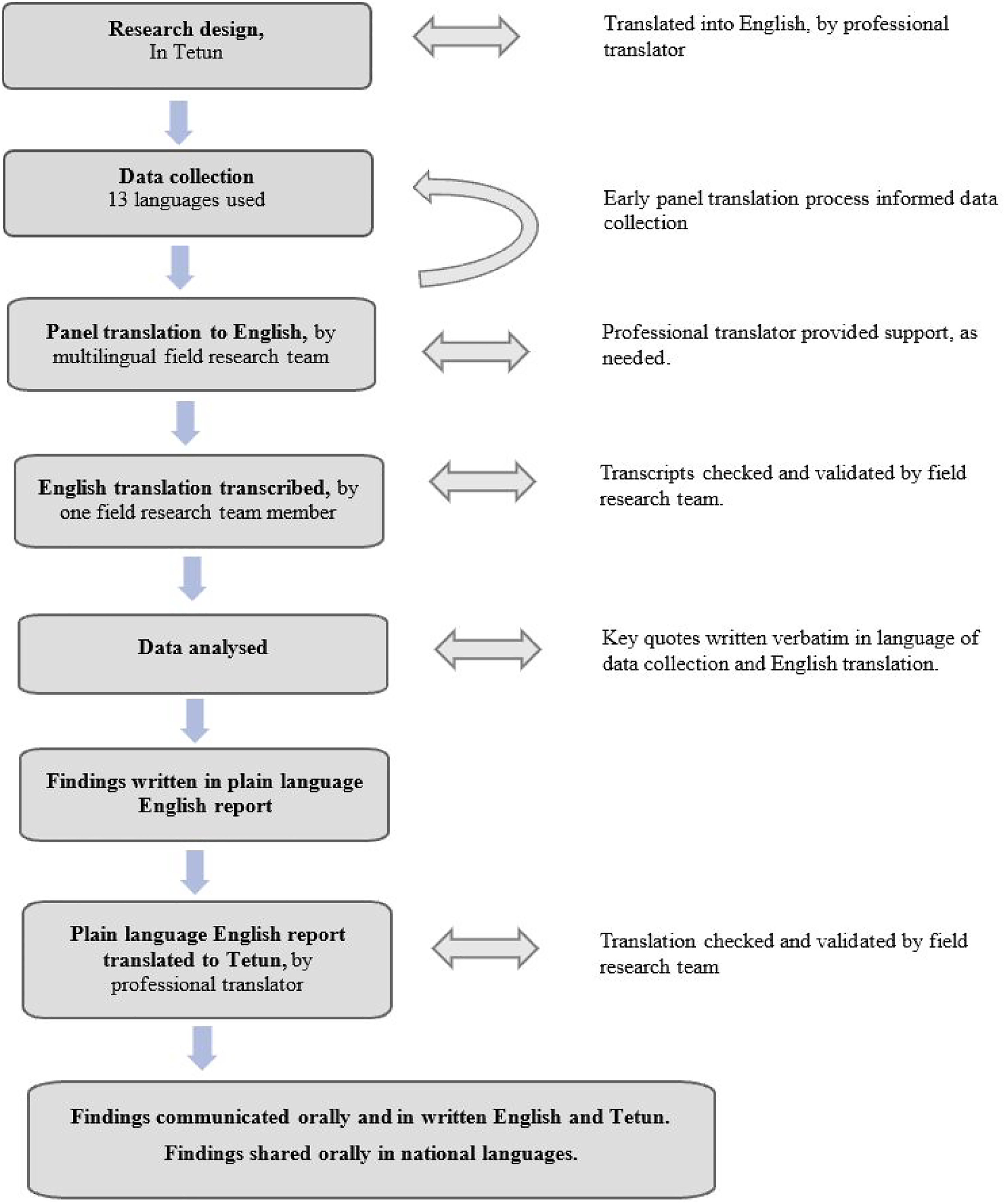
Results
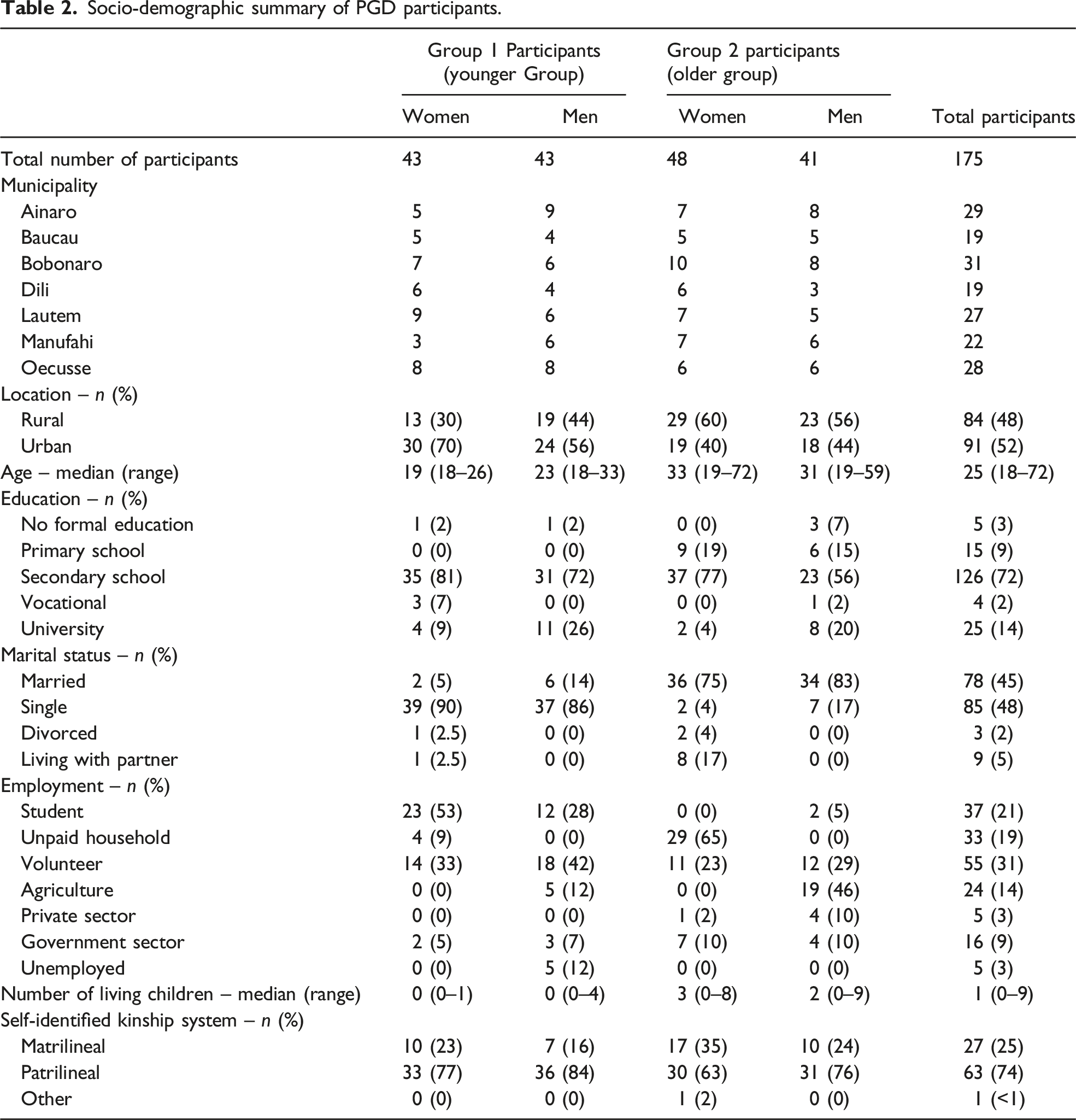
Socio-demographic summary of PGD participants.
The 14 PGDs lasted between one to three hours each. The gender-specific PGD activities ran for a total of 67 hours and 40 mins. Group translation of the 14 PGDs took 258 hours to complete. A further 172 hours were required to finalise the English transcriptions, using the audio recordings from the panel translation sessions. All transcription was completed manually (without automated transcription software) due to the multilingual nature of our study. In total, for each one hour of research activity, approximately six hours were needed for translation and transcription.
We translated the first two PGDs within two days of being conducted, as a multilingual panel of five. This enabled us to reflect on and improve facilitation skills for future PGDs and better understand what was happening in the other gender-specific group. For logistical reasons, the remaining 12 PGDs were translated with a panel of between three to five researchers present. The researcher who led the one-on-one body mapping discussion was always present for that translation, to provide insights on the participants’ expressions and to guide and connect the body map images to the participants’ verbal description.
In the following sections, we identify and reflect on five key findings related to why multilingual panel translation was important for this research: 1) improved inclusion; 2) improved translation quality; 3) improved data collection; 4) strengthened data analysis and 5) practicality and impact.
Improved inclusion
The use of a multilingual panel translation process enabled a diverse range of people to participate in our study, and to express themselves in their own language and communication style. The research methodology and methods used provided multiple ways for participants to contribute and be heard, as indicated by the 13 different languages used by participants. Further, while many participants contributed openly and confidently verbally, others were more comfortable to draw and/or write about SRH on their body map images. For example, one male PGD participant reflected: “I drew this here, it’s the woman’s part. In our culture it’s difficult to say the proper name. It’s the place for the baby, menstruation, and urine.” (Group 2, male participant, rural location)
Some participants who were less active in the group discussions were more vocal when expressing their thoughts and opinions through the individual body mapping exercises. In contrast, some participants were more active in the small group activities.
Ensuring flexibility in how language and communication was used was an important characteristic of this inclusion. For example, one participant with a physical disability was unable to hold a pen, so verbally described to one of the researchers what they wanted the body map to include and look like. The researcher was able to use the verbal guidance to draw the participant’s directions. Refer to Figure 3 for two examples of completed body map images. Example of two different body mapping images, demonstrating how the method can be used with participants of different literacy levels, and across different languages.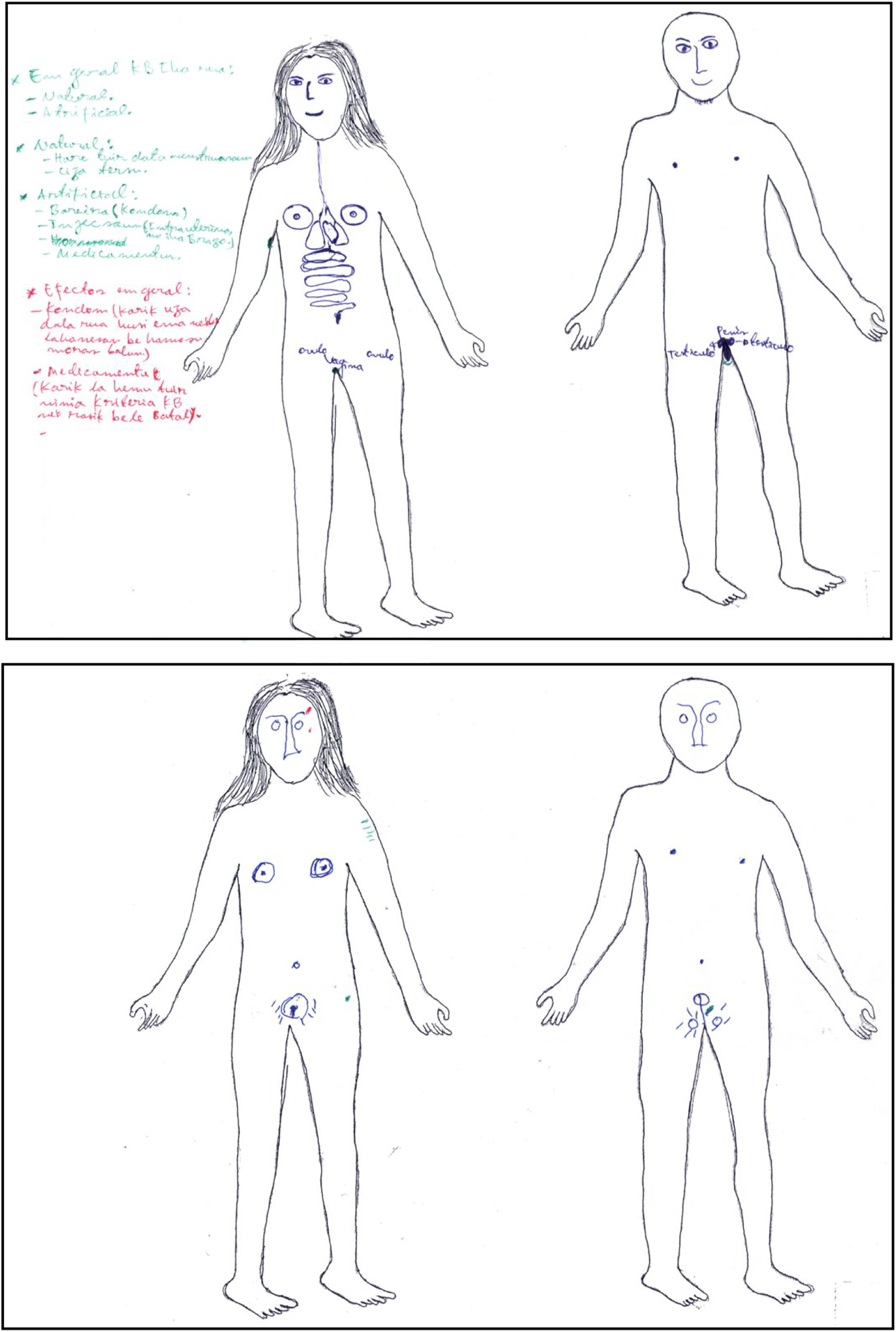
Improved translation quality
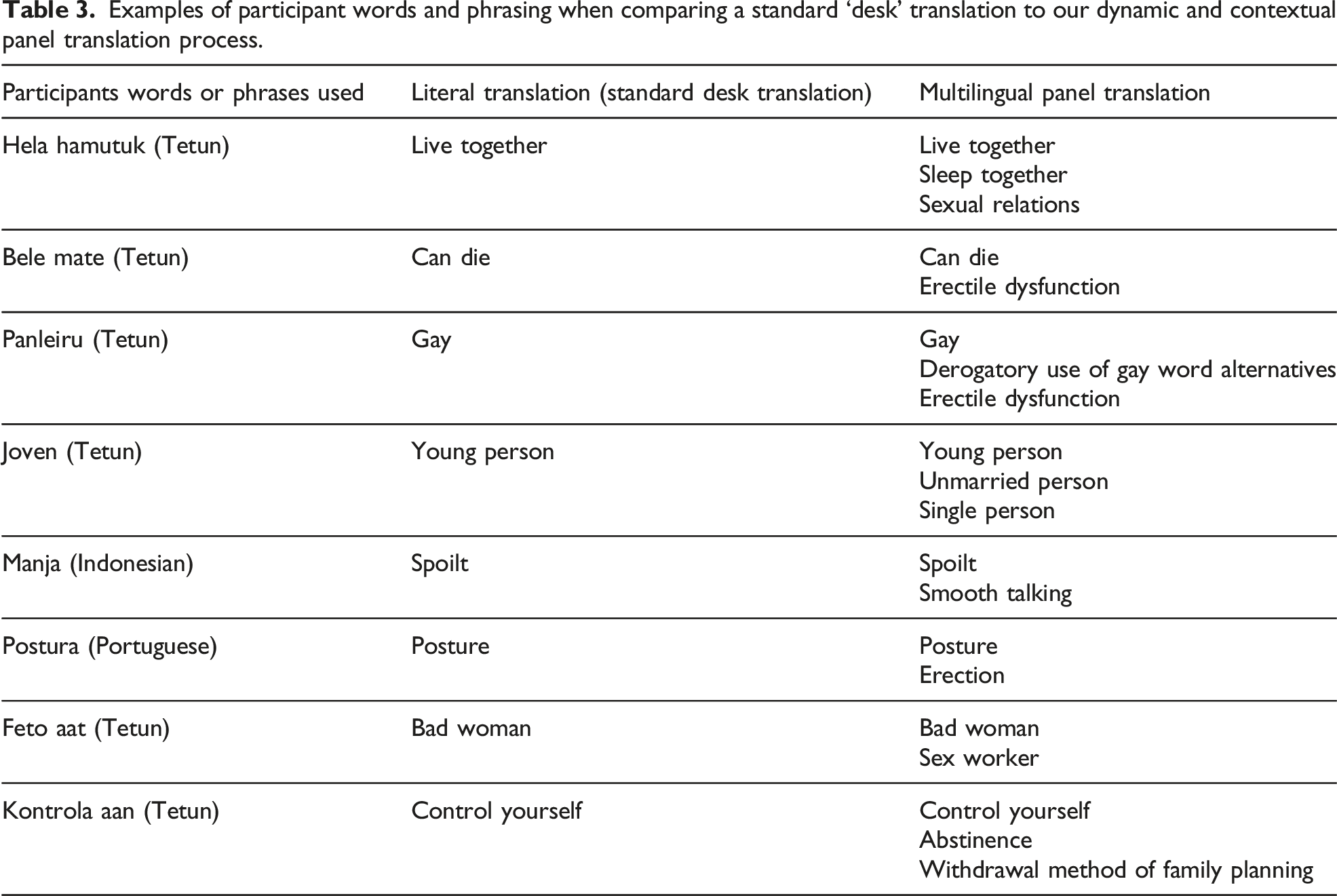
Using a multilingual translation panel comprised of the research team allowed for a robust and thorough translation process with ‘checks and balances’ (Lopez et al., 2008). The team approach to translation provided rigour, critical thinking and unique insight into the process, especially given the team’s specialist experience and knowledge of SRHR in Timor-Leste. Not uncommon for conversations about SRH in any language, participants would often speak in colloquialisms, euphemisms or metaphors to describe genitalia, sexual activity or relationships. For example, ‘the water cannot enter the flower’ was used by one participant to describe the withdrawal method of family planning. As a multilingual translation panel, the language used would be discussed as a group to ensure contextual meaning was captured. Some phrases may have been lost or misunderstood if translated using standard desk translation processes that focused on literal translation. For example, ‘panleiru’ is included in standard Tetun-English dictionaries as ‘gay’ and is often translated this way. However, in common practice it can be used as a derogatory describer and is not considered rights-based language, with the use of English words gay or homosexual preferred. While not all participants used ‘panleiru’ in an intentionally offensive way, many did, as indicated through their tone, sentence structure and content. Two participants also used the term ‘panleiru’ to describe erectile dysfunction and the inability of a penis to get an erection. In these instances, a standard translation to ‘gay’ would have been inaccurate, losing contextual meaning of the negative implication attached to its use.
Examples of participant words and phrasing when comparing a standard ‘desk’ translation to our dynamic and contextual panel translation process.
Improved data collection
The early and team approach of using multilingual panel translation enabled us to identify and discuss ways to improve research practice as individuals and a group, including facilitation style and words used. For example, rather than exclusively using the Tetun words ‘vantajen’ and ‘dezvantajen’ when asking about side-effects of using contraception, the Indonesian words ‘efek-samping’ resulted in some participants more easily understanding these questions. Identifying terminology that was more easily understood for different study locations saved time within the PGD process and helped ensure research activities within the male and female groups remained similar and focused on the research topic.
Examples of common Tetun words and phrasing meaning different things to participants.
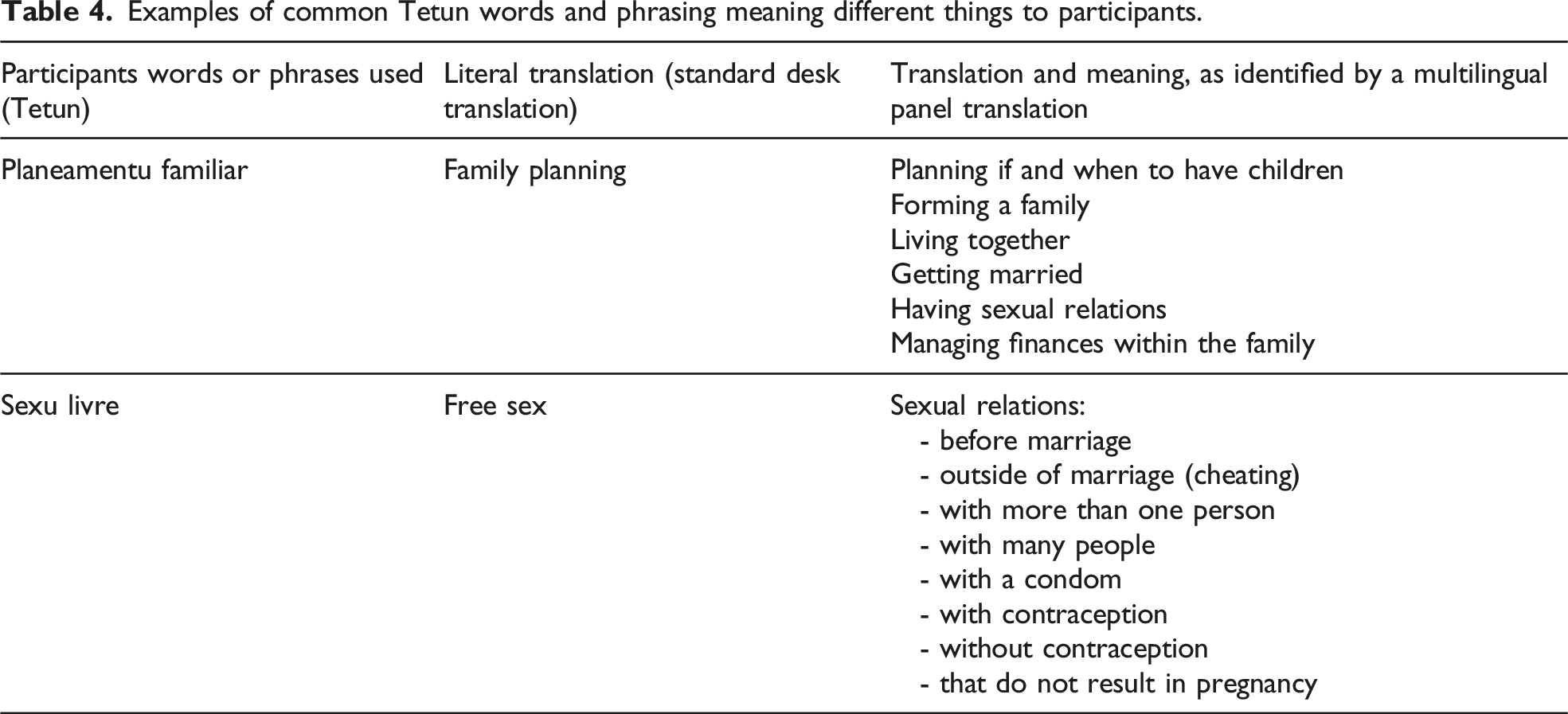
Another example of a commonly used Tetun phrase meaning different things among participants was ‘sexu livre’ (free sex). It was understood and described differently by participants in relation to sexual relations and use of contraception (see Table 4).
The use of a multilingual panel translation process helped identify this nuance and contextual richness.
Strengthened data analysis
The panel translation process was an essential step after data collection, to prepare data for the more formal and systematic analysis phase. However, the panel translation process was more than just an intermediary step between data collection and analysis: it provided us with the opportunity to interactively engage with and immerse ourselves with the data, as a team, in an early or pre-analysis manner. This meant that when we started the more systematic data analysis phase, we were already deeply familiar with the data from both male and female PGD groups and were well-prepared to collaboratively code data, identify, define and agree on research themes. Further, the audio recordings from the panel translation sessions provided invaluable documentation for future reference about translation decisions, research process and to support the communication of research findings (for example, retrospectively transcribing participant quotes in Tetun, for reporting in Tetun).
Practicality and impact
It would have been extremely challenging, if not impossible, for one researcher or an external translator to both understand all the languages used by participants and have experience and understanding about the content discussed. A multilingual team-based approach was therefore necessary to collect, translate, transcribe and understand the data collected. The unique skills, experience, dynamics and size of the field research team made the methods used in this research possible and feasible while working in a resource-limited setting. Having ongoing access to an experienced and professional translator, who was familiar with the research, served as additional and important support when needed. The operational research approach we used enabled many of the lessons we learnt while conducting data collection and multilingual panel translation to be immediately integrated into SRHR programming. This included informing project design, team training and health promotion activities.
Discussion
The benefits of working in a team to conduct qualitative research have been well documented, including improved research quality and rigour (Barry et al., 1999). This was true in our study, with our collaborative team approach improving the quality, rigour and integrity of our work. Our use of multilingual panel translation resulted in rigorous discussion about both context and meaning, ensuring different perspectives and understandings were discussed and agreed upon as a research team. Having the dual role of researcher and translator was appropriate and possible as we were deeply involved throughout the entire research process and had in-depth understanding and knowledge of what we were asking and why (Temple & Young, 2004).
The respectful relationship within the research team enabled honest and critical checks and balances of each other throughout the data collection and panel translation process. The trust, respect and collegiality were important in enabling each team member to participate fully in the decision-making process. We were able to work effectively by embracing and drawing from our different backgrounds, perspectives and skill sets. Prior experience of working together and having common ground around SRHR knowledge and values helped facilitate this open and effective team dynamic (Barry et al., 1999).
Our reflexive practice as individuals and as a team was also important. This included reflexivity about the multilingual panel translation process and how our research findings were understood (Sherrie, 2017). This was especially important given we were all MSTL staff at the time of data collection and needed to actively push and challenge our biomedical way of thinking and positionality as a health NGO working in partnership with the Timor-Leste Ministry of Health.
We acknowledge that multilingual panel translation involving the research team may not always be possible or appropriate however, and external translators may need to be used. When this is required, we suggest that translators are deeply involved in the research process and have sufficient time, support and connection with the research context and research team to ensure quality of translation and meaning. As demonstrated in our research, this is especially true in the SRHR sector where the language used between formal and informal settings may be different, and the ability to understand local colloquialisms, euphemisms and metaphors is important. Engaging with key stakeholders may also help guide the appropriateness of language use and linguistic approach within a research or translation process.
We note that our research is not an academic study about language, but an operational and participatory research study focussing on how to understand and improve SRHR in Timor-Leste. We demonstrate through our work, however, that by incorporating language diversity into our approach in a practical and operational way, we were able to strengthen research process and the quality and usefulness of our findings (Temple & Young, 2004; van Nes et al., 2010). As a result, insights gained through our multilingual panel translation process have real world applications in how SRHR concepts, information and services are planned, promoted and made available within communities.
Our findings support the recommendation that it is inappropriate to simply translate cross-language health promotion activities, and that the need to carefully adapt for meaning and understanding is vital (European Centre for Disease Prevention and Control, 2016). Sufficient time and appropriate resources should be allocated to ensure meaning, integrity and cultural appropriateness are maintained in health promotion initiatives, and that the end users of SRHR programming benefit.
Our work also highlights the need for improved communication and coordination between health systems, academics (schools, universities and ethics committees), practitioners, linguists, researchers, communities and the media about the development and use of SRHR language and terminology. This collaboration, of a critical and ethnographic nature, would be beneficial to improving health policy and practice in multilingual contexts like Timor-Leste.
Challenges and Limitations
Multilingual panel translation is time-consuming and human resource intensive. We believe we had the right dynamics and skills for this research, but also note that multilingual panel translation may not work as intended if there are power imbalances between individuals in the panel or if there are significant knowledge gaps in language or context. In our study, the panel translations of the final two PGDs were delayed by over six months due to impacts from the COVID-19 pandemic, including the inability to meet and the need to focus on essential SRH service provision.
The many languages used needed to be translated and transcribed into one language for ease of analysis. English was chosen for the practical reasons of being a common language among the research team and having a wide technical vocabulary to translate both words and meaning. However, some participant meaning is still likely to have been lost during this translation process (van Nes et al., 2010). It is also important to acknowledge that English is a language that has become the privileged means of expression within science and health (for example, writing this manuscript in English) and is often used in international development and global health work (Goitom, 2020; van Nes et al., 2010). Although a working language in Timor-Leste, English is not widely spoken in the general community, and we therefore have a responsibility to ensure these findings are also communicated in the languages and ways our participants and stakeholders can understand. Further, although our field research team had solid and diverse language skills (16 languages collectively), we did not speak all the languages used by the participants. We also acknowledge possible power imbalances between researchers and participants, through our associations with a health NGO and an Australian university.
Conclusions
A multilingual team was necessary in our study to accurately manage data collection, translation and transcription for the many languages and modes of communication used by participants. The use of multilingual panel translation, conducted by people with deep knowledge of the research methodology, enabled a critical and in-depth translation process to occur and improved overall quality of our work. Centred around participant voices and expression, the process embraced the uniqueness and diversity of individuals and the many ways in which we communicate. The process valued and promoted shared learning between participants and researchers, and demonstrated the importance of both linguistic and contextual translation in the research process and SRHR initiatives. Our research experience has affirmed the imperative for health, research and development initiatives to be linguistically and culturally aware and inclusive, if they are to realise sustainable development outcomes.
Footnotes
Author Contributions
HH, AS, MS, HSX and SM were co-researchers in the design, data collection and early analysis of research findings. RA, CV and MAB provided support and supervision throughout the research, including the conceptualisation of the research idea, methodology and methods used. HH coordinated research activities and led the writing of the initial draft manuscript. All authors reviewed, edited and approved the final manuscript submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MSTL received financial support from the Australian Department of Foreign Affairs and Trade to conduct this research. HH is supported by the Human Rights Scholarship, awarded through The University of Melbourne. MAB’s time is supported by an Australian Researcher Council Discovery Early Career Researcher Award (DE200100264) and a Dame Kate Campbell Fellowship.
Ethical Approval
Permission to conduct this research was received from three separate ethics committees: 1) Instituto Nacional de Saude – National Health Institute of Timor-Leste – Research Ethics and Technical Committee (INS-RETC). No. Reference: 1168MS-INS/DE/DEP/V112019; 2) The University of Melbourne – Medicine and Dentistry Human Ethics Sub-Committee. Ethics identification number: 1954731.1; and 3) MSI Reproductive Choices - Ethics Review Committee. MSI Protocol number: 020-19. Members of the INS-RETC conducted quality monitoring of the field research in two separate trips, observing three PGDs in two municipalities.
Disclosure
The five field research team members (HH, AS, MS, HSX and SM) worked for MSTL at the time of data collection.