
Abstract
Obesity as a disease remains poorly understood by key stakeholders. Here, in people living with severe obesity, perceptions and beliefs relating to obesity as a disease and obesity causality were examined. Semi-structured interviews were conducted in a tertiary care obesity clinic. 23 people with obesity (10 males, 13 females) volunteered. An overall agreement that obesity is a disease was present. Perceptions related to why obesity is and is not a disease were diverse: Lack of control and addiction, biological determinism, and personal responsibility. For weight loss maintenance, the perceptions and beliefs were heterogeneous with biological factors not considered a determinant of success. Instead, exercise, support, and willpower were described as associated with success. Barriers related to remaining in a weight-reduced state included the following: Emotional eating, sustainability of diet, occupational impact, and defeatism due to misaligned expectation and outcome. In conclusion, people living with obesity tend to agree obesity is a disease yet an incomplete understanding of the disease is present.
What Is Already Known on This Topic:
Key stakeholders related to obesity tend to agree obesity is a disease, yet it is not treated as such.
Obesity, as a disease, is not homogenously described or defined by leading organizations.
There is a need to explore knowledge gaps in key stakeholders related to beliefs regarding obesity as a disease and the biomedical definition of obesity.
What This Study Adds:
Obesity as a disease is poorly understood from a biomedical standpoint.
We found diverse perceptions and beliefs related to obesity as a disease and obesity causality.
A sense of personality responsibility appears to be a barrier to fully accepting obesity as a disease which may negatively impact on seeking treatments and thus health outcomes.
Key Terms:
Introduction
Obesity is formally defined as a body mass index ≥30 kg/m2 and is characterized by excess adiposity with multiple comorbidities. The World Health Organization (WHO, 2018) details that worldwide 1.9 billion adults are living with overweight and 650 million with obesity. First-line treatment for obesity is lifestyle intervention which includes dietary management, increased physical activity, and psychological support. While the efficacy of this approach is limited for many (Look AHEAD Research Group, 2014), pharmacotherapy and bariatric surgery more frequently lead to ≥15% weight loss, with surgery associated with increased life expectancy (Carlsson et al., 2020; Wilding et al., 2021).
Spanning history there have been divergent perspectives of body weight within culture: Venus of Willendorf (2,500BC) suggested to signal admiration for a larger female body size (Johnson et al., 2021) while in contrast gluttony was canonized as one of the seven deadly sins. Within contemporary society body weight remains heterogeneously framed and constructed. In some African and Arab countries, a larger body size has been associated with wealth and good health (Musaiger et al., 2004; Renzaho, 2004). In Western culture, a slim body size has been perceived as favorable (Swami et al., 2007). In the West, left-leaning and central voters perceive society as responsible for addressing obesity, while right-leaning voters perceive obesity as the individual’s fault (Curtin et al., 2021). The framing of obesity as a news topic is reflective of its location in sociocultural space. Recent analysis of the framing of obesity in U.K. press between 2008 and 2017 shows a paradoxical increase in both biomedical and stigmatizing portrayals (Baker et al., 2020). This was described by the authors as reflective of neoliberal rationality. Nonetheless this highlights a misunderstanding of obesity as a disease. Ultimately, independent of sociocultural constructs, obesity is now a severe public health crisis (WHO, 2018).
It is unsurprising then that the concept of obesity as a disease has gained ground (American Medical Association, 2013). Despite key stakeholders agreeing obesity is a disease, people living with obesity (PWO) continually experience social devaluation, denigration and discrimination (Rubino et al., 2020; Sabin et al., 2012). This stigma impacts upon obesity treatment as evidence-based approaches such as pharmacotherapy and bariatric surgery adjunct to lifestyle changes remain inadequately utilized. A pertinent question to ask is why does this persist despite obesity declared a disease?
The Just World Hypothesis within a culture of individualism has been suggested to play a key role in the belief that obesity is ones fault leading to weight bias and stigma (Brownell et al., 2010; Ebneter et al., 2011). In this context, body weight is perceived as under one’s conscious control. This conflicts with contemporary understanding of the biological and environmental determinants of body weight (Grannell, Fallon, Al-Najim et al., 2021). These biological determinants lead to the generation of appetite signals within sub-cortical regions of the brain which project to the cortex where conscious percepts are generated. In people with monogenetic or some syndromic types of obesity, these biological determinants are inherently associated with genetic factors while in common obesity genetics factors may interact with the obesogenic environmental factors causing a disease state to emerge. These obesogenic environmental factors are deeply embedded into neoliberal attitudes and modern culture: Urbanization leading to automation and resultant sedentariness (Levine et al., 2005), psychological stress and poor sleep (Prinz, 2004; Tomiyama et al., 2018), energy density of foods (Hall et al., 2019), and seasonal cultural events (Díaz-Zavala et al., 2017). This interaction of biology with environment calls upon us to question the role of agency in preventing and treating excess adiposity (Grannell, Fallon, Al-Najim et al., 2021). Importantly, the rationale for stigmatization is rendered questionable in light of empirical evidence and philosophical insights. Thus, the answer to the question, “Do PWO deserve to be blamed?” is emphatically, no as appetite control does not appear malleable to volition particularly in those with the disease of appetite dysregulation.
Still, PWO are held responsible for their weight challenges as eating behaviors are perceived as under significant control (Brownell, 1991). It is thus unsurprising that PWO agree obesity is a disease but feel personally responsible for their weight as captured in survey studies (Grannell et al., 2020; Kaplan et al., 2018). Similar findings have been captured through interview with PWO stating “I don’t blame anyone else, it’s my hand that’s putting the food in my mouth” (Greener et al., 2010) and weight gain “is self-inflicted” (Owen-Smith et al., 2014). Kirk et al. (2014) found PWO live with a deep sense of shame and embarrassment. This ideology of personal responsibility impacts on disease prevention and treatment. This is apparent when considering the United Kingdom’s recent attempt to address the obesity epidemic during the COVID pandemic has focused on education regarding lifestyle changes as opposed to addressing the obesogenic environment (UK Department of Health & Social Care, 2020).
As presented above, the root of this issue is how obesity as a disease is perceived. A starting point is to further examine all key stakeholders’ perceptions regarding obesity as a disease in-depth. Highlighting knowledge gap’s it will be possible to ascertain key areas where people can develop their understanding about the disease of obesity. For example, obesity causes along with determinants of weight loss and weight loss maintenance. However, and perhaps most importantly, gaps can only be highlighted if there is a shared agreement as to what actually makes obesity a disease. This topic has not been explored extensively in the literature. Furthermore, the concept of obesity as a disease from the perspective of the philosophy of medicine is a contentious subject (Hofmann, 2016).
While obesity is considered and recognized as a disease by most organizations, many do not attempt to describe why obesity is a disease (Supplement). According to the philosophy of medicine, a disease from the naturalistic stance is characterized by a deviance from normal biological functioning (Hofmann, 2001). With the exception of Obesity Canada, organizations refer only to signs of obesity and associated comorbidities such as diabetes and heart disease. In contrast Obesity Canada refers to obesity as a disease of the brain, which impacts appetite regulation. Similarly, within the literature, few attempts have been made with just Kilov and Kilov (2018) describing obesity as a disease from a naturalistic stance as disturbances to the central appetite regulating system where individuals are vulnerable to weight gain and weight regain after intentional weight loss due to biological factors.
Within the philosophical literature, Hofmann (2016) states obesity is not a disease from the naturalistic stance as there is no clear biological dysfunction present. Instead, he argues obesity is a socially defined disease. Hofmann argues health care and health policy literature despite unanimously declaring obesity a disease, do so without a principled definition according to the philosophy of medicine. While the Hofmann does push for obesity to be recognized as a disease due to pragmatic issues and believes in improving the lived experience of PWO, there is a strong empirically based argument for obesity to be considered a disease based on the traditional naturalistic concept of disease: Deviance from normal functioning as proposed by Kilov and Kilov (2018).
While it is beyond the scope of this article to present a philosophical argument for obesity as a disease, it has been necessary to broach the topic as it holds immense relevance with regards to the aim of this study. Readers can refer to a recent discussion regarding obesity as a disease which raises important philosophical questions (Grannell, Fallon, Al-Najim et al., 2021). The research questions in this study were as follows (a) What are the perceptions and beliefs of PWO regarding what makes obesity a disease and (b) What are the perceptions and beliefs of PWO regarding obesity causality along with determinants of and barriers to weight loss maintenance. It is anticipated that combining novel research findings with a renewed attempt to define obesity as a disease will potentially improve the lived experience of PWO and help promote improved prevention and treatment strategies.
Method
Ethics
The study was approved by the UCD Human Research Ethics Board Committee and conducted in accordance with the principles of the Helsinki Declaration (HS-20-12-McGillicuddy). Patients were informed taking part would have no impact on continued treatment and reminded they could withdraw at any stage without penalty. Written informed consent was obtained from all subjects.
Study Design, Participants, and Setting
To address the research questions, an exploratory qualitative research design was utilized which incorporated in-depth semi-structured interviews. Eligibility criteria required participants to be living with obesity and to actively be involved in weight management (diet, exercise, medication, and/or surgery) under the supervision of medical professionals. Purposive sampling strategy was used to capture rich and varied data relevant to the research questions and to allow for patients treated with lifestyle intervention, pharmacotherapy, and/or bariatric surgery to be included. Patients typically referred to clinical weight management have a body mass index (BMI) ≥ 35 kg/m2, thus all approached had a classification of Class II obesity or greater. Within this weight management clinic lifestyle treatment is prescribed to all patients and includes exercise training. Medications and surgery are also available to patients and delivered along with lifestyle interventions.
Recruitment took place during the first wave of the COVID-19 pandemic in Ireland where lockdown restrictions were in place. Out of the 24 patients approached, 23 patients consented to participate in the study. The sample was not homogeneous with regard to severity of disease, complications, time course of treatment, or type of treatment received. Descriptive characteristics are presented in Table 1 with BMI (kg/m2) at baseline reported. All patients were Irish Caucasian and presented with severe and complex obesity (BMI ≥ 35 kg/m2 with at least one weight-related co-morbidity).
Participant Characteristics.
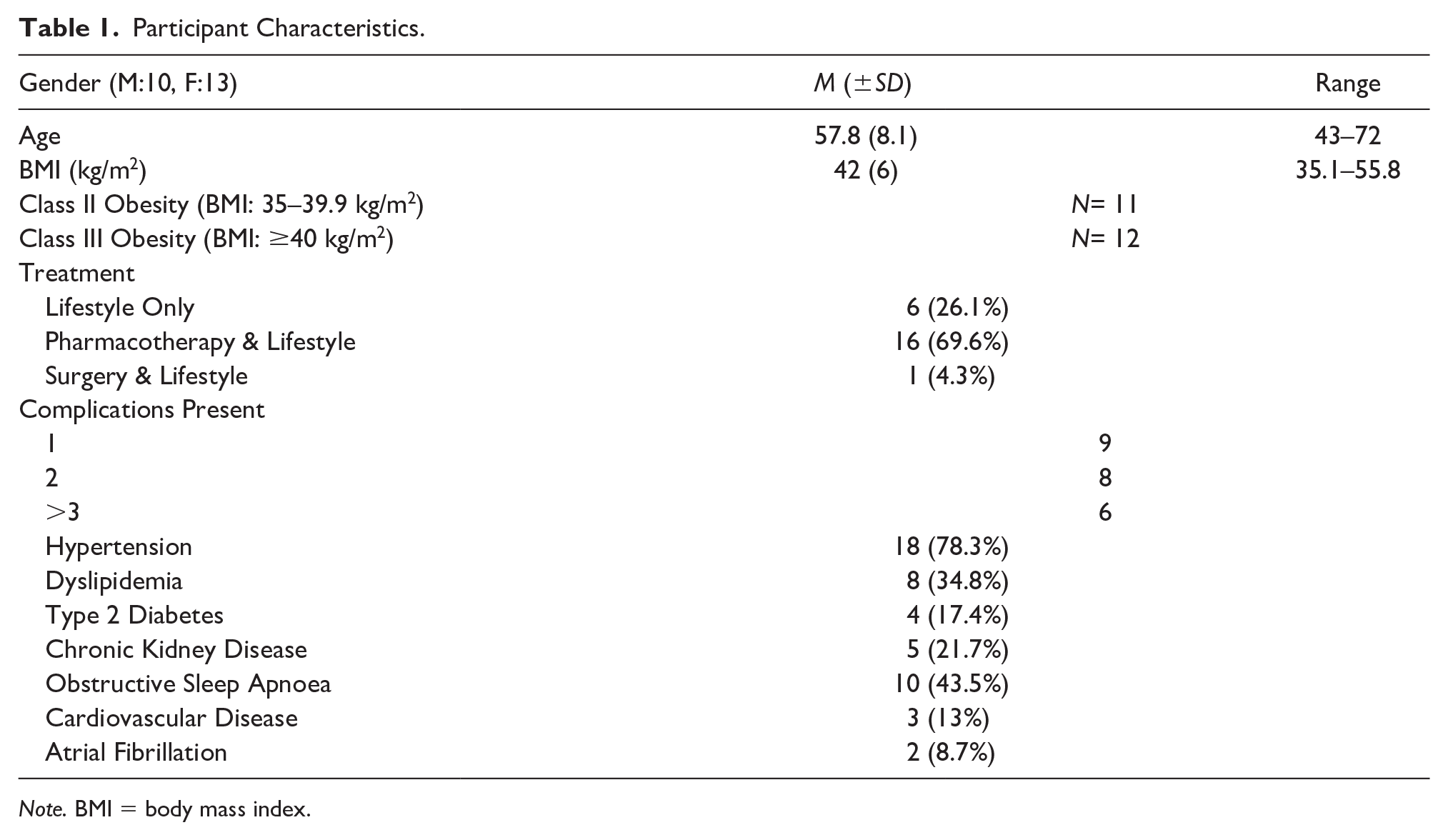
Note. BMI = body mass index.
Data Collection
Data were collected via semi-structured interviews. Interviews were conducted in English with audio recorded digitally. A distress protocol was put in place, taking into consideration the potentially sensitive nature of topics (Draucker et al., 2009). While phone interviews have been suggested to result in lower quality of data compared to face to face due to challenges establishing rapport and inability to respond to visual cues; they are advantageous from a logistical and practicality standpoint. They may indeed improve data quality as the subject may have a heightened perception of anonymity and privacy (Novick, 2008). A total of 23 patients were interviewed between April 25 and May 6, 2020. The interviewer utilized an interview guide with open questions and prompts where necessary (Supplemental Appendix). The research questions were designed to explore multiple themes and aligned with the boarder themes underpinning the Stratification of Obesity Phenotypes to Optimize Future Obesity Therapy (SOPHIA) Project (Table 2). Examples of key questions were (a) What are your thoughts on the statement “obesity is a disease”? and (b) What in your opinion makes obesity a disease? The impact of COVID-19 on the lived experience was also part of the interview schedule.
An Overview of the Themes Explored in the Semi-Structured Interviews as it Relates to the Broader SOPHIA Project and This Study.
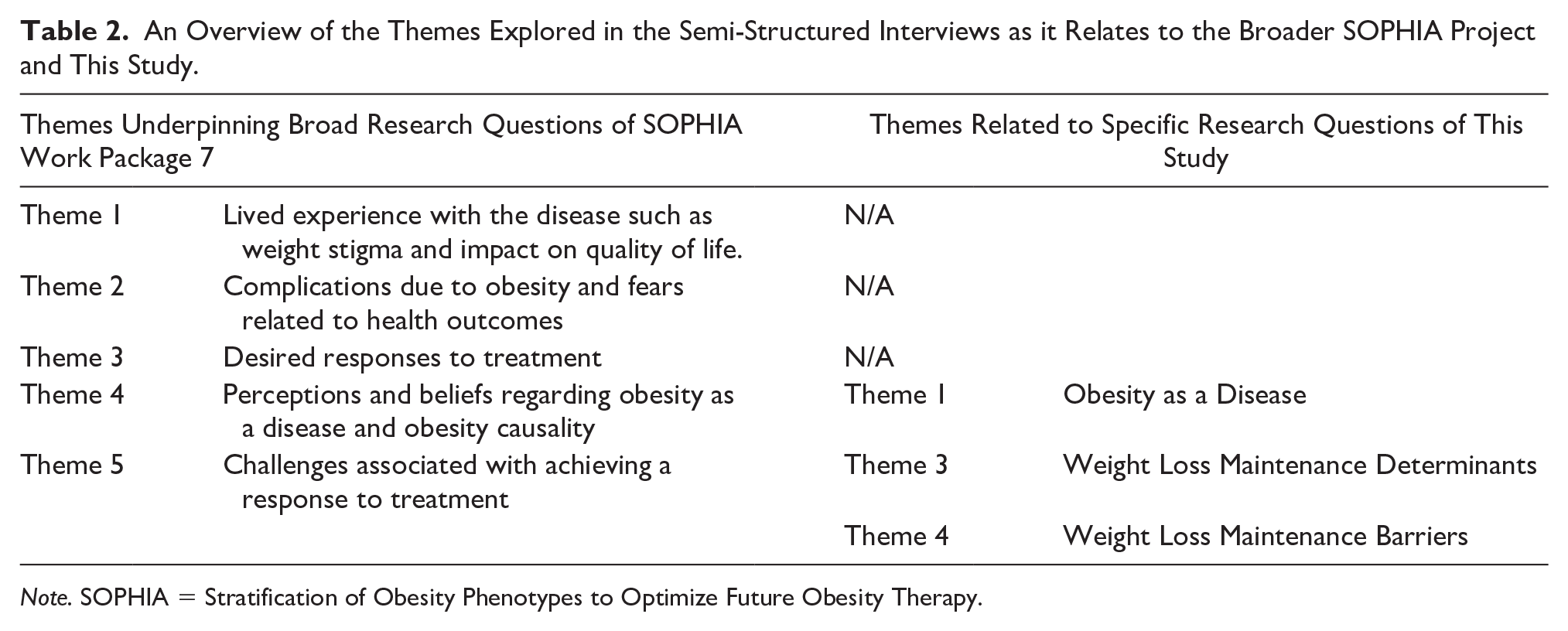
Note. SOPHIA = Stratification of Obesity Phenotypes to Optimize Future Obesity Therapy.
The purpose of these questions was to explore how their perceptions regarding obesity as a disease and factors related to weight loss and weight loss maintenance (WLM) align with the concept of obesity as a disease as it relates to naturalism. Before commencing digital recording of the interview, 5–10 minutes was spent in general conversation making sure the participant had an opportunity to feel at ease. The objective of the interview was reiterated to the participant and once they felt comfortable to commence, the interview was started. The interviews lasted between 16 and 56 minutes. All interviews followed the schedule with regards to the order of questions and necessary prompts. Where necessary, follow up questions such as “what do you mean by that. . ..?” And “could you say some more about that. . .?” were used to extract as much rich and relevant information as possible with both specifying and interpreting questions also utilized for the same reason and to provide clarity.
Data Analysis
Interviews were transcribed verbatim. Thematic analysis was performed using Microsoft Word. To derive themes, inductive thematic analysis used the six phases proposed by Braun and Clarke (2006):
Familiarization with the transcribed verbal data
Generation of initial codes
Search for themes
Review of themes
Defining and naming themes
Production of the final report
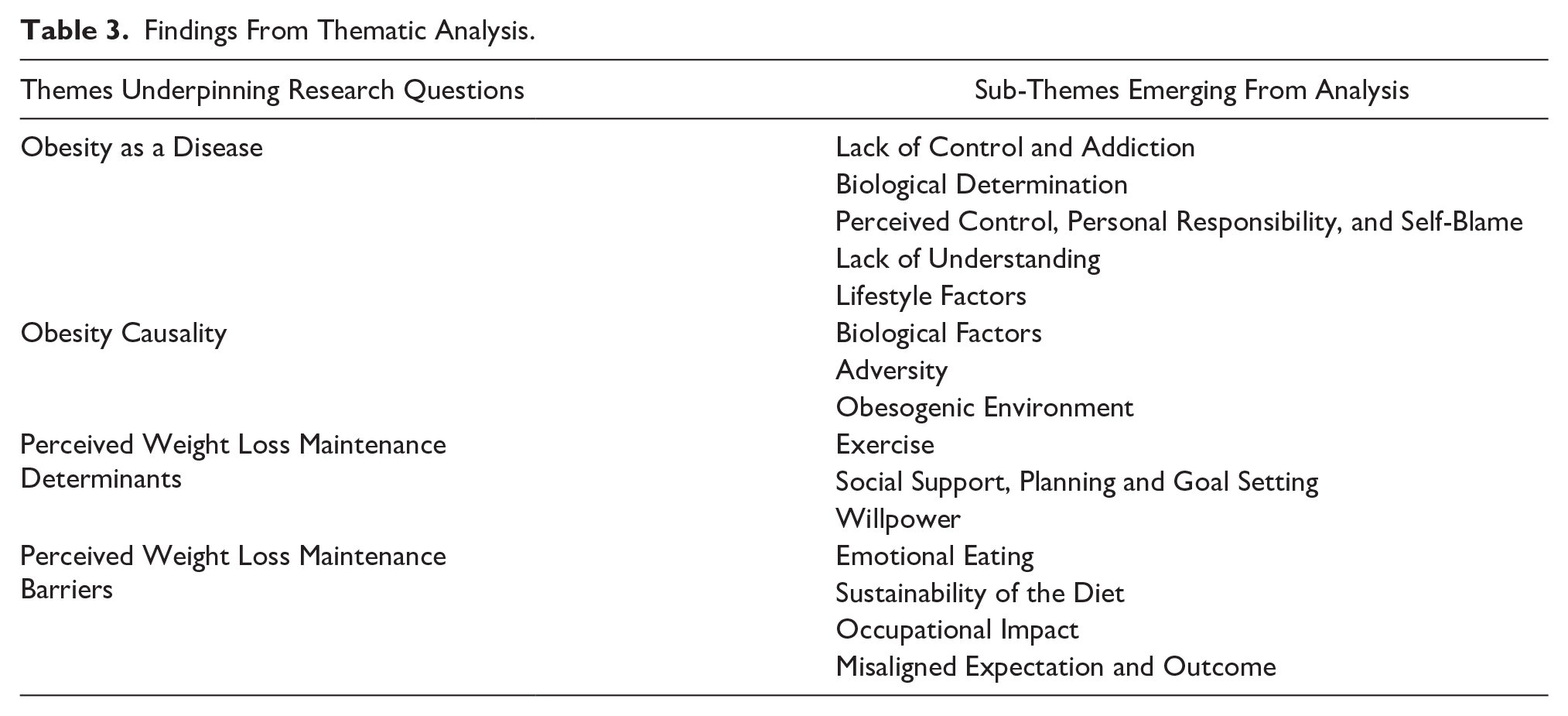
The approach to coding was open, a process of fracturing the data by highlighting concepts, philosophical perspectives, and general similarities to develop categories. Codes were reviewed by the team of three researchers. This process facilitated the consolidation of codes, the identification of any outliers/conflicts, and ensured validity of the data. This resulted in the re-coding of data and the re-identification of two sub-themes relating to obesity as a disease and obesity causality. This approach facilitated cross-checking and the validation of the codes presented in this article. This process was followed for all transcripts being thorough, inclusive, and comprehensive via basic labeling (highlighting). The process was iterative and comparative, whereby codes were collated into categories reflectively with a thorough investigation into trends and contrasts between participants undertaken before finally collapsing them into overarching themes and sub-themes. Thus, the process can be thought of as inductive thematic analysis with elements of a grounded approach (Chun et al., 2019). In producing the report, quotations (phrases and paragraphs) corresponding to each theme were extracted and organized into a coherent storyline. Within each theme underpinning the research questions, a number of sub-themes were arrived upon through the analytical process which is summarized in Table 3.
Findings From Thematic Analysis.
Results
Obesity as a Disease
Participants in this study were divided whether obesity could be defined as a disease. Four core themes were emergent from the data including (a) addiction and lack of control, (b) biological determined, (c) personal responsibility, and (d) a lack of understanding.
Addiction and lack of control
Participants in this study equated lack of control to addiction, which they defined as a key characteristic of obesity as a disease. This perceived lack of control was saliently captured by one participant stating obesity is “something you get that you don’t want.” Perceived lack of control was mirrored in other participants highlighting their internal struggle: “it makes it a disease if you catch it or if you are born with it and it’s out of your control.” The chronicity of the perceived lack of control was reflected when one participant stated, “you cannot switch it off, it is a lifelong thing, constant thing.”
One participant expressed, “you are always at war with yourself” suggesting an internal conflict as “it’s terrible because my brain is telling me something, my heart is telling me something, my heart is saying please cop onto yourself and my brain is saying no, just deal with it you are fat.” This perceived lack of control reflects a sense of diminished agency where a desire for a smaller body size is challenged by the disease of obesity itself.
It was the perceived lack of control that led several participants to opine that obesity is a disease because it is like an addiction. For one participant, obesity “is a disease, it’s a bit like alcoholism, drug addiction, it is an addiction” which for him manifests itself whereby “you have no control over your urge to eat.” This connection between obesity and addiction was complex as it was additionally perceived as “obviously the cause of obesity.” One participant elaborated further suggesting that “If you drink too much you become an alcoholic and if you eat too much you become sick as well” with alcohol and food “the same thing.” One participant drew a similar comparison but paradoxically does not perceive herself addicted to food, “All of these things are in the one sort of family: alcohol, drugs and food, but then I am not addicted to food.”
Evident from participants’ narratives equating obesity with alcohol and/or drug addiction is a profoundly affective response evoking feelings of lack of control. Such affective responses impact not only on how patients understand their disease but also on how they attribute their perceived responsibility as “out of control” or “addicts.” The implications of such findings are profound for how patients understand obesity as a disease and the mis/understanding of their ability to “control” or be responsible for their “addiction.”
Biologically determined
Some participants drew upon genetics as a reason for obesity to be considered a disease. Drawing on observations of family they stated, “it is an hereditary disease,” “it has to be in the DNA,” “there is a certain amount of it genetic, all of us would be on the heavy side” and “genetics are a huge element, I would have had a very physically large father and a physically large mother.” The link between genetics and obesity as disease made by participants in this study highlights the role of visual representations of obesity manifested through a larger body.
While genetics can be thought of as a cause of obesity, from the perspective of the philosophy of medicine, it can also be argued that genetic factors determine the label of disease due to emergent biological dysfunction or deviation such as that seen with monogenic obesity such as MC4R mutation. Within common obesity, it is not one gene per se that causes obesity. As detailed through genome-wide association studies, it is the interaction of most likely several genes with the obesogenic environment that makes many vulnerable to weight gain. This highlights an opportunity to fill a knowledge gap regarding the role genetics play in determining body weight.
Perceived control, personal responsibility, and self-blame (partial agreement)
Several participants agreed obesity is a disease yet perceived body weight as controllable. This led to a sense of personal responsibility and created a barrier to fully accepting the outright label of disease. This nuanced perspective was captured by a participant who stated, “We are all partially responsible for weight gain, coming from ourselves. It’s not an easy question to answer. Is it a disease? Partially”
Sharing a similar perspective one individual stated, “Rationally I completely agree with it. It’s the people who are perfect weight that are good role models for the overweight people.” For him this is due to one’s ability to control their weight and in fact leads to a form of weight discrimination which he describes as irrational as when he sees some people with obesity it goes through his head “wouldn’t you think the person would cop themselves on and just do something about it.” This complex perspective further compounds narratives of self-stigmatization and shame.
Referencing media portrayal of PWO one individual stated, “you see some people obese on TV but they are just eating all the time.” This was coupled with a sense of frustration and blame that one should take personal responsibility for their actions as “they’re not helping themselves either. They should be out doing a bit of walking.” With a perception that obesity resulted from lack of self-control came a sense of self-blame. This was evident from one participant who suggested that living with obesity is “still something I am trying to accept” and “I still struggle with it.” For another participant, this struggle and difficulty in self-acceptance stemmed from her life history living with the disease as “the way you grow up you always think you are doing something wrong.” This sense of self-blame and doing wrong is tightly interwoven with a narrative of failure as “you are at fault and it’s not a disease, it’s your personality, you eat wrong, you move wrong and it’s still at the back of my mind always.” This narrative of failure and doing wrong has a deeply embodied impact, which one participant carries with her “always.” The implications are profound, resulting in what one participant demonstrates to be a constant questioning of self, which manifests in a narrative of self-blame: is it? (a disease) . . . I am the one who puts the chocolate in my mouth, I still have a choice, I know what’s bad for me, I still make bad choices, bad food . . . high sugar sweets.
Based on these responses, it is clear a complex and nuanced perspective regarding what makes obesity a disease is present in several PWO. The perceived ability to control one’s weight is a clear barrier to full acceptance of obesity as a disease and highlights itself as an obvious target for future education strategies.
Lack of understanding: The complexity of obesity
Obesity as a disease is complex and the challenge in attempting to understand it based on lived experience was saliently captured here: I don’t know whether it is or not. I feel if somebody put a gun up to my head and said I’m going to murder both your children, unless you lose weight that I would be able to do it. Now is that a disease or what is that? I don’t have an answer to that. I don’t understand this really, so my answer to that is I suppose I’m just confused about it.
Some participants in this study perceived causal factors such as lack of knowledge and greed define obesity as a disease rather than clearly communicating any information regarding the biological dysfunction which, from a medical standpoint, defines the disease. This was illustrated by one participant who argued, “it’s how you are reared, how you are trained to eat and how you are brought up eating . . . it’s knowledge and it’s psychological.” These narratives relating to familial practices, habits, knowledge, and psychological deficit are woven through typical approaches to obesity treatment which place the onus on the individual to improve their behavior (Lewis et al., 2010).
Although there was an awareness that obesity is not “all self-inflicted . . . (or) people being greedy,” it became apparent that for some participants they were unsure as to what makes it a disease. While metabolism was identified as being linked to obesity, there was a lack of clarity of its contribution to obesity as a disease. Two narratives emerged relating to body composition and to metabolic function. While one participant suggested that obesity occurred as a result of “the body makeup or in the cells,” another participant believed it was linked to metabolic dysfunction whereby “if your metabolism is not working properly . . . you food doesn’t get broken down enough.”
The confusion around the link between obesity and disease was especially evident from one participant who stated, “The disease in me is that I don’t exercise enough. My disease is that I don’t see sport as being something that is beneficial to health.” It is clear from this statement that knowledge is absent regarding the biology of obesity as a disease and instead a sense of inadequacy and self-infliction. This limited understanding similar emerged when examining themes related to obesity causality.
Obesity Causality
Participants described in most multiple factors which they position as the causes of obesity. Collectively these factors shed light on the complex and diverse lived experiences of patients and their experiences shaped beliefs. There is a clear need to improve education strategies regarding the diverse factors driving the obesity epidemic. The PWO did not refer to several important biological factors while social determinants such as the environment were only briefly touched upon by a select few.
Lifestyle: Diet and exercise
For many participants, excess food intake and lack of exercise were causes of obesity: “the cause of obesity has got to be overeating” and “your intake of food is greater than your output of exercise.” Traditionally, obesity as a disease has been framed simplistically through energy in, energy out descriptions. The physiology governing appetite and body weight regulation is immensely complex yet PWO are perhaps unable to answer as to why energy intake is beyond energy needs from a biological perspective. This highlights a need to improve education regarding the factors driving dysregulated appetite and the role of exercise in body weight regulation.
For some, a reflection upon their own lived experience provided an important look into how they perceive lifestyle as the cause of their obesity. Here, the participants described life events which impacted upon lifestyle and then caused weight gain: “I was very slim up until I had my first surgery. When I lose my mobility the weight piled on,” “When I stopped playing sports I forgot to change my eating habits, I started to put on weight,” and “If you give up sports you kind of put on weight very quickly.” Exercise is important in weight stability (Paixão et al., 2020) and while moving more does not lead to significant weight loss, a lack of exercise appears to be an important risk factor for weight gain.
Biological factors
Within the literature, biological factors are well described as determinants of obesity. However, few participants suggested a relationship may exist. Describing how biology might drive obesity one participant stated, “Certain things in your brain maybe gives you the wrong directions in terms of cravings or doesn’t tell you when you’re really full.” This highlights from an education standpoint the need to bring to the forefront the deterministic nature of biology concerning both hunger, fullness, and appetite dysregulation that emerges with the disease of obesity.
As discussed, participants described genetics as the justification to consider obesity as a disease. Concurrently, genetics were deemed causal of obesity with one individual stating, “I think genetics are a huge element and I am very conscious of that.” One participant speculated more in-depth on the causal role of genetics in obesity, drawing upon observations in family members. In the case of her daughters, she describes a divergence in weight which has led to weight stigma from her husband: I think that it’s a gene and I think it comes from your parents, it comes from their parents, comes from their parents. My husband is skinny, which makes him judgmental. Now I see my daughter living through it because unfortunately I believe she’s got the fat gene from me. My youngest daughter she eats what she wants, she’s never had to worry about weight.
Owen-Smith et al. (2014) found similarly that PWO perceive family traits and genetic predisposition as important in the development of their condition. There is a clear need to unpack monogenic, syndromic, and common obesity from an educational standpoint to highlight the deterministic nature of body weight and the strong role the environment plays in driving weight gain in vulnerable individuals.
Adversity
Diverse psychosocial factors were described by some participants as causing weight gain. With “a huge emotional part in it, where you would say emotional eating . . . you can turn to food for comfort,” for many their obesity was perceived as caused in part by emotional factors leading to comfort eating as a coping mechanism. One participant suggested, it can be emotional, can be comfort, can be lack of confidence, more mental than physical, the mental side of it is always overlooked, you are feeling down because of your weight, you feel sorry for yourself, you eat more, it’s a vicious circle as well like.
The emotional element to eating was embodied similarly by another participant who stated, “I just start eating so I keep everything afloat, I would be upset with myself, I’d eat myself you know to make me feel better.”
Animal and human studies reveal emotional eating is caused by stress, with the hormone cortisol thought to play a key role (van Strien et al., 2013). It is unsurprising then that stress and depression were acknowledged directly: “there is stress, depression or other things that happen within your life. My partner dying had an awful effect on me,” “I suffered a lot from depression. And when I do have it I would eat for comfort” and “probably a bit of depression, could be a lot to do with it.” These are important descriptions and highlight the significant impact of emotional factors in driving the obesity epidemic and the current vulnerability of these PWO during the COVID-19 pandemic (Grannell et al., 2020).
Adverse childhood events and early exposure to unhealthy foods were described as causal toward obesity in some individuals. This has similarly been found by Owen-Smith et al. (2014) who detailed that PWO perceive early childhood socialization patterns as causal toward their condition. On what causes obesity: “when I was young, you would always empty your plate” and “your upbringing, your food intake, what you have been eating as a kid” were causal factors for one participant. An unhealthy and underprivileged childhood was described by some participants as causal with one participant stating “I am still addicted to bread. Things that go on early in life set a template or pattern.” A challenging environment was described more in-depth by one participant: “it’s how you are reared, how you’re trained to eat and how you are brought up eating.” She describes food being in short supply as a child whereby they were in “starvation mode.” Finally, one participant painting a similar picture as his family came from “a reasonably poor background” where “everything was stretched” which then impacted food availability where dinner was “a slice of bread and margarine and maybe a bit of sugar on it or something and the same going to school.” The prevalence of obesity is higher in underprivileged populations who are more likely to suffer with stress and be exposed to an obesogenic environment (Pavela et al., 2016; Scott et al., 2012). The voices captured here highlight the need to increase awareness within society at large regarding the risk of obesity for these individuals which will serve to improve the focus of prevention strategies and help remove a sense of self-infliction.
Obesogenic environment
Few participants described changes in the environment as important. “Societal changes, ready meals, what they are putting into foods to make then tasty and our eating patterns have changed” were drawn upon as a cause of obesity by one individual. Education in the obesogenic environment was described by just a very small number of individuals as causal. One participant placed an emphasis on “education about food” being important, with another stating simply “it’s knowledge.” Only one participant digressed further with “people aren’t educated around how much to eat, when to eat, exercise as well.” Given that the majority of anti-obesity prevention and treatment strategies have been educational in nature, this highlights that PWO do not perceive their obesity as being due to limited knowledge which may indeed increase the sense of personal responsibility for their condition. However, given that the obesogenic environment was mentioned by just a select few as important, this highlights a bring to the forefront of education the role it has in determining body weight. Without changing the obesogenic environment directly, these strategies which have relied upon individuals changing their behaviors will continually fail.
Weight Loss Maintenance: The Perceived Determinants and Barriers
A range of factors were perceived as determinants of and barriers to successful weight loss maintenance (WLM).
Exercise
“What you put in you have got to exercise out” stated one participant which again captures the simplistic energy in versus energy out paradigm so common in mainstream thought. For this individual “continuing to exercise” was essential to remain in a weight-reduced state. This simplistic view of energy balance perturbation was mirrored in two other participants: “increasing your calorie burn over your intake” and “when I lose weight, I am still fired up that I have lost it, that I am doing a lot more physical activity stuff so I tend to keep it down . . . you’d be burning off.” While exercise has been empirically shown to predict WLM, the physiology behind this phenomenon appears to be more complex than a simple increase in how much you “burn” (Paixão et al., 2020). Moving forward it is essential that exercise is framed from an evidence standpoint regarding its effectiveness for bodyweight stability as opposed to its perceived role in burning off excess calories.
Social support, planning, and goal setting
Having a “support system is really very very important.” For this individual, “sociability, if I can do things in a social setting, I am away in a hack.” Social support and a group setting were a determinant for WLM in some while its absence was a barrier for two participants. For one participant what made WLM difficult was a “lack of support” feeling “there is nowhere to turn” much like another participant who stated “being independent (living) on my own” was a challenge as opposed to “when I was living with someone you know, you have to impress somewhat.” The challenge for many PWO starts once the weight has been lost. Given that many weight loss programs are temporary lasting only weeks or months raises the need for long-term strategies. However, it should be questioned if indeed group support is causal as within the Look Ahead study, despite significant contact time and support for several years, weight loss was underwhelming and the phenomenon of weight regain was not offset (Wadden et al., 2014). The idea of having targets, something to aim for was described by three of the participants as a determinant to maintain weight loss. For one participant, it was imperative to “have a plan . . . have a structure,” for two other participants respectively “having a purpose and a goal” and “a goal and time frame.” These are common elements of commercial weight-loss programs and highlight the need for long-term strategies based on individual preferences.
Medication
Despite a significant proportion of participants having been prescribed anorexigenic medication to drive weight loss, it was described by just two individuals as being important for WLM. For one participant, the medication was important to help it not “bounce back up” and for one participant for her to facilitate WLM, medication is important as it “helps that I’m not completely overeating, the medication helps me eat less.” Medication such as Liraglutide 3.0 mg has been shown to favorably impact long-term WLM (le Roux et al., 2017). This reflects the need for patients to be educated regarding the favorable impact it may have on WLM relative to lifestyle intervention alone.
Willpower: Agreement and disagreement as a determinant of weight loss maintenance
The majority of individuals felt WLM is dependent on willpower: “you have to have a lot of willpower” and “willpower is extremely important; you have got to tell yourself you can do it. You have got to see yourself being able to do it. All of that is down to your willpower.” With all participants having previously lost and regained weight in the past, it was unsurprising that in many who felt willpower is important concurrently felt they lack it: “I haven’t got an awful lot of it” and “it’s very important and I know I don’t have it. I wouldn’t say that I am motivated at all but I am desperate.” This aligns with perceptions of feeling personally responsible for one’s obesity. Indeed, having the will to simply eat less and move more should be possible if one perceives weight gain in the first place to be due to controllable factors.
In contrast to those describing themselves as having an absence of willpower, this was not the case for the entire cohort. For many, it was impossible to question their own willpower given they have it in such abundance in other elements of their life: “I have the willpower but I’m not getting the results. I mean, if willpower would do it I wouldn’t be overweight,” “I am fairly strong on willpower, the exercise slips a bit, with the exercise and diet regime but I would call it slippage, I wouldn’t call it my willpower had let me down totally,” and I used to think it was all willpower and you know, I had no willpower, but then when I kind of looked at that I would have I would have really good willpower in loads of areas, I used to always say I can manage anything but I can’t manage food.
Given that a sense of personal responsibility is embodied in their psyche this must lead to a sense of immense confusion and internal conflict, “always at war with yourself.”
Emotional eating
Emotional eating was perceived as a barrier to WLM and as detailed above emotional eating and stress have been linked to the obesity epidemic. For one participant he described, “using food as a comforter” as a result of challenges that were described as “emotional . . . a crisis.” This was echoed for another participant who described “emotional eating” as a barrier. Indeed, one participant felt that “sometimes I think if you can get your head right you would stick to reducing diet.” For another individual “it’s very easy to fall away from a routine if certain things are going on that are making you, I suppose a bit unhappy” such as “a bit of stress.” This reflects the need for treatment strategies to highlight individuals at risk of being impacted by stress and thus emotional eating.
Sustainability of diet
The sustainability of the diet was a barrier for many participants. “It’s not a sustainable way of life” described one participant. This was similarly a barrier for another participant as “the diet becomes boring; it becomes like you are not living so that’s not sustainable.” This inability to persist with the diet led to one participant breaking the diet “I have to accept some personal responsibility because as I said sometimes you get fed up taking the diet food and you start treating yourself to the odd chocolate bar” and end up “not staying away from the fridge more often and just slipping into maybe your old ways.” Not being able to sustain it was for one participant a barrier, she feels “I need to have the willpower to do it and I need to be happy with the eating plan that I can sustain it” but at the same time “I’m bored stupid.” Again, many commercial programs are temporally constrained and focus on caloric restriction. The sustainability of these diets is highly questionable. However, even within randomized controlled trials where diets are professionally prescribed and support is provided over several years, WLM is an elusive outcome for most (Wadden et al., 2014).
For one participant, the diet was not boring but simply led to severe fatigue and hunger “what I would do is just have breakfast and then dinner and nothing and it meant that it was a very tough to sustain that during the day.” Being on this diet he felt “very weak, like most days I would be weak and my legs would actually get weak, trying to walk would actually become an issue because I would have to sit down because I would be physically out of energy” and he would be “consciously hungry.” This is a phenomenon expected in response to starvation yet occurs in response to weight loss for many PWO and is likely a strong determinant of weight regain (Sumithran et al., 2011). Despite this, physiology was not suggested by any participant as a determinant of WLM.
Occupational impact
The demands of work from a temporal standpoint were a barrier for several participants. Due to time constraints, the ability to adhere to a dietary and exercise regime was negatively impacted: “If you miss a meal and you are at a meeting you just think ah sure a bag of chips on the way home.” The occupational impact made WLM challenging for one participant who stated: “At one stage I had got into fitness, I was eating well. I found I was working through lunch at the desk, I was kind of a bit stressed and then got into dashboard dining.” For another individual, working night shifts had a detrimental impact on his ability to adhere to lifestyle changes: At 3 o’clock in the morning you would be tired so you drink a cup of tea, you might have a bar of chocolate. If you wanted an apple or an orange they are not very available. You can’t have a structure. You are tired and you won’t go out for a walk or run or anything like that.
These are important considerations for PWO regarding their treatment as the environment presented by work can serve as a serious barrier to both weight loss and WLM. These reflect the need for bespoke interventions at a micro level and perhaps policies which call for workplaces to provide a healthy environment in relation to food at a macro level.
Misaligned expectation and outcome
An important barrier described by the participants was the lack of progress with regards to weight loss. Specifically, the outcome did not match the expectation, which reinforces the need for realistic goals. Ultimately a sense of defeatism was caused by this misalignment and led to weight regain. This was captured by participants who stated: “If it’s taken so long to achieve and it’s so hard, I feel like, I can’t be dealing with this, I’m fat and I just have to live with it” and “If you are not losing enough then you lose heart and you end up back to square one again.”
Evidence suggests PWO should expect on average less than 10% weight loss from diet and exercise alone, which highlights a need for expectations to be managed early on (Wadden et al., 2014). Indeed, even with pharmacotherapy alone just 50% will lose >5% of their weight while 25% and 11% will lose 10% and 15% of their weight, respectively (le Roux et al., 2017). While this weight loss might disappoint many PWO, they are still capable of eliciting health gain by favorably impacting cardiometabolic risk factors. It is reasonable to predict that shaping expectations based on empirical evidence may lead to better long-term outcomes for some.
Discussion
In this study, the perceptions and beliefs of PWO regarding obesity as a disease and obesity causality along with perceived WLM determinants and barriers were explored. The novel findings of this study show that PWO have an incomplete understanding of obesity as a disease relative to the biomedical concept of the disease (Kilov & Kilov, 2018). This is expected as obesity as a disease has been poorly described (Hofmann, 2001). In line with the philosophy of medicine, obesity as a disease involves dysfunction of the appetite regulation system which can emerge due to genetic and environmental interactions as seen in common obesity (Heymsfield & Wadden, 2017), due to rare mutations as seen in monogenic obesity (Farooqi & O’Rahilly, 2005) or be associated with a variety of syndromes as seen in syndromic obesity (Chung, 2012). The inherent biological dysfunction(s) present within these diseases is far from completely understood by scientists. However, what is clear in these cases is that obesity is not due to sloth or gluttony but instead biologically determined to varying degrees. In contrast, many of the PWO interviewed in this study felt a strong sense of personal responsibility for their obesity suggesting a perception that they have agency when it comes to body weight regulation.
This is similar to previous work by Lewis et al. (2010) as the participants struggled to accept an outright label of “disease.” Instead, partial agreement regarding the label of obesity as a disease was present due to the perceived ability to control feeding behaviors and thus body weight. This perceived ability to control body weight resulted in the sense of self-infliction; that they had given themselves the disease. These findings are similar to previous studies involving surveys in that PWO tend to agree obesity is a disease but feel a sense of personal responsibility for managing the disease themselves (Grannell et al., 2020; Kaplan et al., 2018).
Many of the PWO in this study suggested obesity is a disease because it is comparable to addictions like alcoholism and concurrently described a lack of perceived control and thus agency. While for some obesity as a disease might relate to pathological changes in mesolimbic, dopaminergic signaling pathways, and associated neural networks, it is perhaps unlikely this is the case for most (Berthoud, 2012; Naef et al., 2015). It could be interpreted that this belief regarding addiction emerges as PWO attempt to understand their own lived experience and attach this to traditional cultural narratives. Lewis et al. (2010) also found that in people with severe obesity a strong motivation to lose weight along with a sense of powerlessness or lack of control was present. In the study of Lewis et al. (2010) PWO felt “at war” with their body and “out of control” with their weight which was also described by participants in this present study: “you have no control over your urge to eat.” This sense of “war” with one’s body was also captured by Kirk et al. (2014) with a participant describing “it is a daily battle. It’s constant, actually. It’s not just daily: it’s every minute of every day. Overall, both the present study and that of Lewis et al. (2010) and Kirk et al. (2014) show that many PWO feel responsible for their obesity. Our study highlights novel findings in that PWO struggle to recognize obesity as a disease due to the perception that they should be able to control themselves as they have agency with regards to body weight regulation. With this narrative and lack of options to treat their disease it is unsurprising many end up feeling trapped with no hope of ever finding resolution and “always at war with yourself.” Owen-Smith et al. (2014) examined the perspectives of PWO in relation to the development of their weight challenges. The authors found mixed views were present regarding the role of personal responsibility with one individual stating “I’ve got the sort of body which is difficult to lose weight” suggesting biological determinism while another participant stated their weight gain “is self-inflicted.”
This internal struggle stemming from a mismatch between a motivation to reduce body weight and inability to change eating behaviors is likely driven by biology due to the interaction between genetics and environment and the subsequent dysfunction that emerges which undermines volitional attempts to control one’s weight (Heymsfield & Wadden, 2017) and is not reflective of akrasia. The PWO who suggested genetics play a large role in determining obesity appeared to have an incomplete understanding as one individual suggested it was possible to break the “genetic connection” by making their children hyperaware of their parents’ weight. None described biological dysfunction impacting appetite regulation as per the biomedical concept. Unsurprisingly, a lack of understanding regarding obesity as a disease was present. Some participants gave vague descriptions of problems with metabolism, others suggesting obesity has a lot to do with knowledge and psychology, while others explicitly stated they did not know what makes obesity a disease. These are novel findings as this is the first study to capture the voice of PWO about their beliefs regarding what makes obesity a disease.
Gender disparities relating to weight exist in developing countries where women are more likely to suffer with overweight and obesity while the inverse is true in developed countries such as Ireland (Dee et al., 2015; Kanter & Caballero, 2012). Logically it might be hypothesized that gender as a sub-theme would emerge in the data analysis yet this was not the case. Females did not describe gender related issues as causal to their obesity and this did not shape their perception of obesity as a disease. This is despite menopause being associated with unintentional weight gain and female health issues such as polycystic ovarian syndrome linked to overweight and obesity. Similarly for male’s gender was not a theme emerging in the data analysis.
An additional aspect of obesity as a disease is the phenomenon of weight regain after successful weight loss. A recent survey found that PWO tend to believe WLM depends on willpower (Grannell et al., 2020). We examined for the first-time perceived determinants and barriers to WLM. There is an abundance of evidence WLM is dependent on biological changes associated with weight loss (Grannell et al., 2019). However, many of the participants described in detail the key role they perceive willpower to play, suggesting it a key determinant of WLM. In contrast, some felt that for them willpower was not a determinant as they have this trait in abundance. Exercise was described as important due to the effect it has on “burning calories.” However, evidence suggests adherence to exercise facilitates WLM due to the effect on appetite regulation as opposed to generated a caloric deficit (Beaulieu et al., 2016). The participants also described social support, planning and goal setting as important factors which have been suggested in the literature as key determinants (Hall & Kahan, 2018).
Regarding barriers to WLM, several factors were described that should be considered by treatment providers including emotional eating, the impact of their occupation and a misalignment of expectations and outcome. The latter suggests the need for realistic outcomes which have been previously suggested (Hall & Kahan, 2018). Emotional eating has been described by PWO as a determinant of weight regain (Sainsbury et al., 2019; Thom et al., 2020). Within these same PWO lower glucagon-like peptide-1 at baseline and after weight loss was associated with weight regain with the PWO not perceiving appetite changes unlike previous studies (Coutinho et al., 2018; Nymo et al., 2018; Sumithran et al., 2011). A lack of understanding regarding the physiology of weight regain may lead to the PWO rationalizing their adaptive eating behaviors as emotionally and not physiologically driven. Given that appetite changes may occur outside conscious awareness it is unsurprising PWO may rationalize in this sense. However, emotional eating should be considered as a modifiable factor by clinicians yet more research is needed to ascertain the link between physiological responses to weight loss and changes in eating behaviors. Given that within our study sustainability of diet was a barrier for many, this collectively suggests the need to bring forth the physiology of weight loss into patient education and also a need for appropriate dietary management such as diets that emphasize satiety as opposed to those generating metabolic hunger. Overall, these findings further highlight the incomplete understanding of PWO regarding what makes obesity a disease and call for education strategies that highlight the limited role agency within a lifestyle intervention setting may play for some due to biological determinants.
While little research has been undertaken regarding the voice of PWO about what makes obesity a disease, more has been undertaken regarding the causes of obesity. Lewis et al. (2010) found that PWO believed they could lose weight via lifestyle changes and thus positioned lifestyle factors as causal, highlighting the coherence effect. Similarly, this perception that PWO are responsible for their condition was mirrored in this present study as some blamed themselves for causing their obesity. In contrast, others felt their own obesity was due to factors outside their control such as adverse events and a minority felt their obesity was caused by environmental and biological factors. Greener et al. (2010) through in-depth interviews also examined PWO beliefs relating to causality. They found beliefs that obesity was due to personal shortcomings, excess eating and lack of exercise. All had lost and regained weight previously, feeling personally responsible for this perceived failure and despite this remained adamant that diet and exercise were the solutions to their weight problem. Similarly, to the present study, they positioned genetics, learned behaviors, family habits, and adverse life events as leading to their obesity which the authors curiously described as “blame absolving.” Stating “I don’t blame anyone else it’s my hand that’s putting the food in my mouth” echo’s statements from participants in the present study. Within the present study, there was an in-depth discussion regarding these factors, which showed that many do not fully understand how obesity is caused by biology or the environment which are strong determinants of obesity. Rather PWO tended to feel lifestyle factors were most important, which matches similar survey studies (Grannell et al., 2020; Kaplan et al., 2018).
Luig et al. (2020) examined how PWO in primary care settings respond to alternative narratives regarding obesity. They found that PWO initially portrayed self-depreciating narratives about their disease. Importantly, when presented with a compassionate co-constructed alternative narrative that considered biological and social determinants, the participants well-being improved along with their perceived ability to gain health. Their study describes the ability of health care providers to transform the lived experience of PWO and help them understand obesity as a disease. From a clinical perspective, findings from our study highlight the need for HCPs to upskill in their understanding of obesity as a disease. Only when equipped with knowledge as it pertains to obesity as a disease will the HCP be able to effectively treat the PWO. Treatment for PWO must focus on education regarding the biological and social determinants of their weight gain with a thorough examination of their medical history and lived experience. A compassionate and educated HCP with regards obesity will be able to deliver the right evidence-based treatment to the patient at the right time.
Strengths and Limitations
This is the first time the voices of PWO have been captured on the question of whether obesity is a disease in this manner and the insight provided can help change clinical practice. However, this study included a small sample size located in one hospital of PWO living in Ireland. As with all qualitative research, the findings presented cannot be extrapolated beyond the individuals who supplied the data. It is important to consider the views of other PWO from different cultural backgrounds both within and beyond Ireland. There is a need to capture the voice of all key stakeholders in relation to this topic along with PWO across the BMI and socioeconomic spectrum as this will enhance shared value. Finally, the individuals in this study were undergoing elective weight management. There is a need to examine the beliefs of individuals with different weight statuses not undergoing weight management such as individuals experiencing unintentional weight gain and those who are weight stable.
Concluding Remarks
PWO appear to have an incomplete understanding regarding obesity as a disease which is characterized by appetite dysregulation promoting both unintentional weight gain and regain after weight loss. Given the complexity of obesity, it is unsurprising the participants gave diverse perspectives with Luig et al. (2020) similarly detailing that PWO feel their disease is a puzzling experience. There is a need to educate all key stakeholders regarding the biology of the disease and push toward a better understanding of obesity as a disease. We suggest a biomedical definition similar to Obesity Canada and Kilov and Kilov (2018). Here, the pathway to obesity involves strong biological determinism in those with syndromic and monogenic obesity. In those with common obesity an immense vulnerability due to environment and genetic interactions is present with an emergent disease state presenting itself in this cohort. This biological dysfunction is extended to the weight reduced state where physiological changes oppose the weight loss. Collectively, this disease undermines volitional attempts to control one’s body weight and thus agency appears to be significantly undermined. Combining this with an understanding of the causes of obesity will help shift the narrative away from personal responsibility and ideally better the lived experience of PWO by improving access to adequate treatments and furthermore help tackle the obesity epidemic through prevention policy changes together with better biological treatments. The beliefs of HCPs, policymakers, and the general public regarding the themes explored in this study are also vital. Previously Kirk et al. (2014) detailed policy makers express concerning perspectives regarding obesity as a disease: “In and of itself, obesity is not a disease. I don’t know what it is.” This highlights the need for immediate action: Thereafter it may be possible for thought leaders in the field to agree upon a universal definition of obesity a disease(s) which will require a philosophical discussion regarding the role of personal responsibility and agency in preventing and treating the disease.
Applying Findings
These findings will be used to improve the understanding of the lived experience of people with obesity. The objective is to develop the understanding of all key stakeholders (health care providers, policy makers, industry, patients and public) regarding obesity as a disease. Improving education strategies will enable common language, shared agreement, and shared value. Findings from this article will be disseminated at international conferences.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211040767 – Supplemental material for “You Are Always at War With Yourself” The Perceptions and Beliefs of People With Obesity Regarding Obesity as a Disease
Supplemental material, sj-pdf-1-qhr-10.1177_10497323211040767 for “You Are Always at War With Yourself” The Perceptions and Beliefs of People With Obesity Regarding Obesity as a Disease by Andrew Grannell, Carel W. le Roux and Deirdre McGillicuddy in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323211040767 – Supplemental material for “You Are Always at War With Yourself” The Perceptions and Beliefs of People With Obesity Regarding Obesity as a Disease
Supplemental material, sj-pdf-2-qhr-10.1177_10497323211040767 for “You Are Always at War With Yourself” The Perceptions and Beliefs of People With Obesity Regarding Obesity as a Disease by Andrew Grannell, Carel W. le Roux and Deirdre McGillicuddy in Qualitative Health Research
Footnotes
Author Contributions
AG, DMG, and CLR conceived and designed the study. AG recruited participants and conduced the semi-structured interviews and is guarantor. AG and DMG performed the analysis. AG, DMG, and CLR drafted the analysis. AG, DMG, and CLR critically revised the document and approved the final version of the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the Unified Competing Interest form. Authors declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work. CLR reports grants from Science Foundation Ireland, grants from Health Research Board, during the conduct of the study; other from NovoNordisk, other from GI Dynamics, personal fees from Eli Lilly, grants and personal fees from Johnson and Johnson, personal fees from Sanofi Aventis, personal fees from Astra Zeneca, personal fees from Janssen, personal fees from Bristol-Myers Squibb, personal fees from Boehringer-Ingelheim, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Stratification of Obesity Phenotypes to Optimize Future Obesity Therapy (SOPHIA) project. SOPHIA has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 875534. This Joint Undertaking support from the European Union’s Horizon 2020 research and innovation program and EFPIA and T1D Exchange, JDRF, and Obesity Action Coalition.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.