
Abstract
Cannabis has long been stigmatized as an illicit drug. Since legalization in Canada for both medical and recreational purposes, older adults’ cannabis consumption has increased more than any other age group. Yet, it is unclear how the normalization of cannabis has impacted perceptions of stigma for older adults consuming cannabis medicinally. Qualitative description was used to elucidate the experiences of older Canadians aged 60+ related to stigma and their consumption of cannabis for medicinal purposes. Data collection involved semi-structured interviews. Data analysis examined how participants managed stigma related to cannabis use. Perceived stigma was evident in many participants’ descriptions of their perceptions of cannabis in the past and present, and influenced how they accessed and consumed cannabis and their comfort in discussing its use with their healthcare providers. Participants employed several distinct strategies for managing stigma—concealing, re-framing, re-focusing, and proselytizing. Findings suggest that while medical cannabis consumption is becoming increasingly normalized among older adults, stigma related to cannabis persists and continues to shape older adults’ experiences. A culture shift needs to occur among healthcare providers so that they are educated about cannabis and willing to discuss the possibilities of medicinal cannabis consumption with older adults. Otherwise, older adults may seek advice from recreational or other non-medical sources. Healthcare providers require education about the use of medical cannabis, so they can better advise older adults regarding its consumption for medicinal purposes.
Keywords
Introduction
Cannabis is one of the most widely used illicit drugs globally but has been legal in Canada for health reasons since 2001 and for recreational use since 2018 (Cox, 2018; Statistics Canada, 2019). Since recreational legalization, cannabis use among Canadians aged 60+ has increased by 4%—a greater increase than any other age group (Cox, 2018; Statistics Canada, 2019). Older Canadians are more likely to consume cannabis for medicinal reasons than are younger people (Abuhasira et al., 2018; Bobitt et al., 2019; Choi et al., 2017; Kamnrul et al., 2019; Kaskie et al., 2017; Vacaflor et al., 2020). Similar spikes in usage have been reported in the United States since 2018, when ten states and Washington DC passed laws allowing medical and recreational cannabis use (Willams, 2021).
It has been argued that growing medical cannabis use among older adults can be explained by the ongoing normalization of cannabis due to increased access and public acceptance (Baumbusch & Yip, 2022). This suggests that the stigma surrounding cannabis may be decreasing for this population. Other evidence, however, indicates that stigmatization related to cannabis use persists for both medical and recreational uses (Bottorff et al., 2013; Clary et al., 2022; Duff et al., 2012; Gibson et al., 2021; Hathaway et al., 2011; Krediet et al., 2020; Reid, 2021). Given that cannabis has been illegal and highly stigmatized for most of older adults’ lives, stigma may still influence their decisions to use medical cannabis, how they learn about it, and how they access and consume it. Moreover, older adults may have internalized stigmatized perceptions about cannabis consumption based on their past experiences with it being an illicit drug. These conflicting results leave us with an unclear understanding of the role of stigma in older cannabis consumers’ experiences with medicinal cannabis.
Cannabis and Older Adults
Cannabis has been used to treat a variety of health conditions such as rheumatism, pain, depression, sleep, inflammation, nausea, anxiety, and various neurological and inflammatory conditions (Abuhasira et al., 2018; Bauchhuber et al., 2019; Briscoe et al., 2018; Kamnrul et al., 2019; Stockings et al., 2018; Tumati et al., 2022; Zuardi, 2006). However, evidence of cannabis efficacy and safety in older adults is scant because previous studies have overwhelmingly focused on younger people (Minerbi et al., 2019). Cannabis consumption among older adults is complicated by the proportion of tetrahydrocannabinol (THC) in the products consumed, which may potentially lead to cognitive changes, falls, heart attacks, or psychotic episodes (Minerbi et al., 2019). Due to physical, age-related changes and use of other medications for chronic conditions, cannabis can cause unpredictable and negative side-effects, leading healthcare providers to suggest caution with cannabis consumption in older adults (Minerbi et al., 2019; Wu et al., 2011). The risk of possible drug interactions with cannabis and/or the inappropriate use of cannabis to treat medical conditions makes it essential to understand how stigma may influence older cannabis consumers’ behavior, to ensure that they are able to access and consume cannabis for medicinal purposes safely and effectively.
Stigma
In his seminal work, Goffman (1963) defined stigma as “a discrediting mark” that is attached to individuals, groups, organizations, or products. Stigma can lead to stigmatization, which “is the social process by which the [discrediting] mark affects the lives of all those touched by it” (Pescosolido & Martin, 2015, p. 91). Goffman conceptualized stigma as dynamic and socially constructed and maintained that during periods of change, social actors can become more or less stigmatized (Lamont, 2018; Lashley & Pollock, 2020; Zang et al., 2021). Stigma can be rooted in different sources, whether they are physical, such as a disability, or moral, such as engagement in activities deemed morally wrong (Zang et al., 2021). While sometimes stigma is associated with elements that are non-modifiable (e.g., race and age), other stigmas are seen as controllable such as with cannabis use (Crocker et al., 1998; Hudson, 2008; Jones et al., 1984; Ragins, 2008). Generally, the more controllable a perceived stigma, the greater the risk of stigmatization, including social ostracization, shaming, decreased employment opportunities, low morale, and poor personal wellbeing (Ali et al., 2017; Creed et al., 2014; Crocker et al., 1998; Harding et al., 2018).
Some individuals who exhibit stigmatized characteristics or behaviors come to internalize dominant societal attitudes and thus engage in “self-stigmatization” (Jones & King, 2014). In cases of self-stigma, individuals involved in an “undesirable” activity are not only aware of public stigma toward their actions but agree with those societal stereotypes and apply them to themselves (Corrigan & Rao, 2012). Those experiencing stigma (be it from self or others) may have poor self-esteem, be reluctant to access health services, and suffer from poor health outcomes (Corrigan & Rao, 2012). To avoid or minimize stigmatization, individuals experiencing self-stigma may use stigma management strategies such as education, withdrawal, and secrecy (Ray et al., 2014) or engage in active concealment of their stigmatized identity (Quinn et al., 2017).
Cannabis, Stigma, and Normalization
There is an extensive body of literature in the social sciences on cannabis in relation to stigma going back to Howard Becker’s “Becoming a Marijuana User” (1953). Over the last two decades, scholars in the field have focused on the changing nature of cannabis-related stigma, both in jurisdictions where cannabis use remains criminalized and, more recently, in what Reid (2021) terms “post-prohibition” states where medicinal and/or recreational cannabis are now legal. A key debate in this thread of the literature has centered on the applicability of “normalization” theory to public attitudes toward cannabis (Newhart & Dolphin, 2018).
On the one hand, proponents of normalization theory assert that attitudes toward cannabis have softened and that the increasing consumption, availability, and tolerance of cannabis in many contexts (Han & Palamar, 2020; Statistics Canada, 2019) signals that moral boundaries have changed and that cannabis use has been redefined as a “normal” activity (Lashley & Pollock, 2019).
On the other hand, detractors of the normalization thesis argue that evidence of attitudinal change is not indicative of the widespread evaporation of the stigma associated with cannabis (Hathaway, 2004a; Hathaway et al., 2011). Thinkers in this camp, such as Hathaway (2004a), Reid (2020b, 2021), and Sandberg (2013), suggest that the normalization thesis mistakes increased frequency of cannabis use for normative acceptance. Indeed, as Sandberg (2013) maintains, there are numerous indicators that cannabis use remains a conspicuous marker of difference. Reid (2020a, 2020b) similarly contends that claims of normalization have been exaggerated and are premature because, if cannabis use had truly become fully normalized, both medical and recreational consumers would not perceive any enduring stigma surrounding it.
Reid’s qualitative review of the literature on cannabis (2020b) suggests that claims of normalization overlook the intersecting structural (macro), social (meso), and individual (micro) sources of stigmas and that the diverse nature of stigma for distinct groups requires more nuanced analysis to avoid the pitfall of generalizing group-specific findings. Crucially, Reid notes that perceptions of cannabis differ enormously generationally. Accordingly, unpacking the experiences of different age groups of cannabis consumers—such as older adults, the fastest growing segment of users—is needed to elucidate how stigma is manifested and responded to differently depending on social location.
Cannabis, Stigma, and Older Adults
Although the previous literature on cannabis and stigma has generally overlooked older adults—they typically represent a small minority of study participants (e.g., Sandberg, 2013) or are not included at all (e.g., Hathaway, 2004a)—some previous studies, conducted predominantly in the United States and Europe, have examined cannabis and stigma among older adults. A study in Colorado found that people over 60 lacked information about cannabis yet were reluctant to seek information from healthcare providers due to potential stigmatization (Bobitt et al., 2019). In a study examining the experiences of middle-aged and older veterans in the Netherlands with medical cannabis, participants expressed stigmatized views of their use, which they attributed to their history with cannabis (Krediet et al., 2020). In Krediet et al.’s (2020) study, even though participants reported that medicinal cannabis was beneficial, their belief that cannabis was a recreational drug influenced their internalized feelings of stigma. Similarly, Clary et al.’s (2022) study of older veterans from Illinois found they adhered to common stereotypes about cannabis users, partially perpetuated by the media, which led them to be cautious about exposing their medical cannabis consumption to others.
Canadian studies related to cannabis and stigma have been extremely limited. Participants in one Canadian study restricted their cannabis consumption to places and times where they were less likely to encounter other people—a form of hiding (Duff et al., 2012). Bottorff et al. (2013) found that the stigma associated with cannabis use affected Canadian consumers’ social, professional, family, and healthcare provider relationships. However, these studies were conducted prior to the legalization of recreational cannabis and did not focus explicitly on older adults. Baumbusch and Yip’s (2022) more recent study of twelve older Canadians reported that their perspectives on stigma surrounding cannabis differentiated between recreational and medicinal use. Baumbusch and Yip suggested that in the Canadian context, public perceptions of cannabis may be changing due to the normalization of recreational cannabis following legalization. Nonetheless, older Canadians have a long history of conceiving of cannabis as an illegal and stigmatized drug and as a result may project those views onto themselves as consumers.
To explore stigma among older medical cannabis consumers, we draw on prior work examining the stigma management strategies (Hathaway, 2004; Zang et al., 2021) and resistance to the imposition of stigmatizing labels (Thoits, 2011). As Hathaway (2004a) maintains, we need to explore how different cannabis consumers make sense of their own consumption. Accordingly, in this study, we apply the previous literature on responses to stigma and coping strategies to older Canadians’ experiences with medicinal cannabis.
Aim
Older cannabis users are a diverse group with multifarious experiences, who may also hold divergent views of the stigma associated with cannabis use. Our aim was thus to understand how such fears and experiences of stigma affect older persons’ experiences with cannabis for medicinal reasons.
Research Design and Methods
A naturalistic inquiry using qualitative description (QD) (Sandelowski, 2000, 2010) was used to elucidate the perspectives of older persons consuming cannabis medicinally. QD aims to capture the key elements of phenomena in the terms of the social actors (participants) involved rather than the researchers’ interpretation, as is often expected by other qualitative approaches (Sandelowski, 2000). The analytical process of QD brings the researcher close to the data of a poorly understood phenomenon (such as older persons’ experiences with stigma and cannabis) and describes participants’ experiences in their own words (Sandelowski, 2000).
Consent
Ethics approval was obtained from the Research Ethics Office at the University of Alberta, Certificate#: Pro00112287. Verbal informed consent was obtained from all participants to mitigate logistical barriers to obtaining consent (i.e., sending and returning consent forms via mail for participants who were not comfortable doing so via computer) and was approved by the REB of record. Verbal consent was documented on the consent form by the interviewer. All methods were carried out in accordance with the relevant guidelines and regulations of the World Health Organization’s Declaration of Helsinki.
Sample
Using purposive sampling, we sampled English-speaking older Canadians aged 60+ who resided in Canada and had previously used or were currently using cannabis to manage a health problem.
Recruitment
The flyer advertisement for the study was circulated widely via email in all provinces (to ensure participant representation from across Canada) to a wide range of settings where potential participants were likely to see it (e.g., newsletters for organizations for older persons such as the Canadian Association for Retired Persons, cannabis clinics, retailers, and medical distributors). Potential participants self-selected to enroll in the study by contacting the researchers via email or telephone and were then screened for eligibility by a research assistant S.S or the project manager JB, who followed up with eligible participants and provided them with the study information letter, answered any questions participants had about their involvement, and scheduled an interview. Participants were asked if they understood their rights and if they wished to participate, which was recorded at the start of each interview. Participants received a $30 Amazon gift card in appreciation of their time, a strategy that has been found to facilitate recruitment (Dillman et al., 2014).
Data Collection
Data collection occurred between October 2021 and October 2022. Interviews were conducted by the study research assistants (RAs) (J. L. was a recent MN graduate, S. S. and R. D. were current PhD nursing students, and all had received training in one-on-one interviewing from the study PI (S. D., who holds a PhD in nursing and was an associate professor of nursing with extensive qualitative research experience) and project manager (J. B., who holds a PhD in sociology and has over 15 years of experience in qualitative research). All the RAs and the PI self-identified as women, and the project manager self-identified as a man.
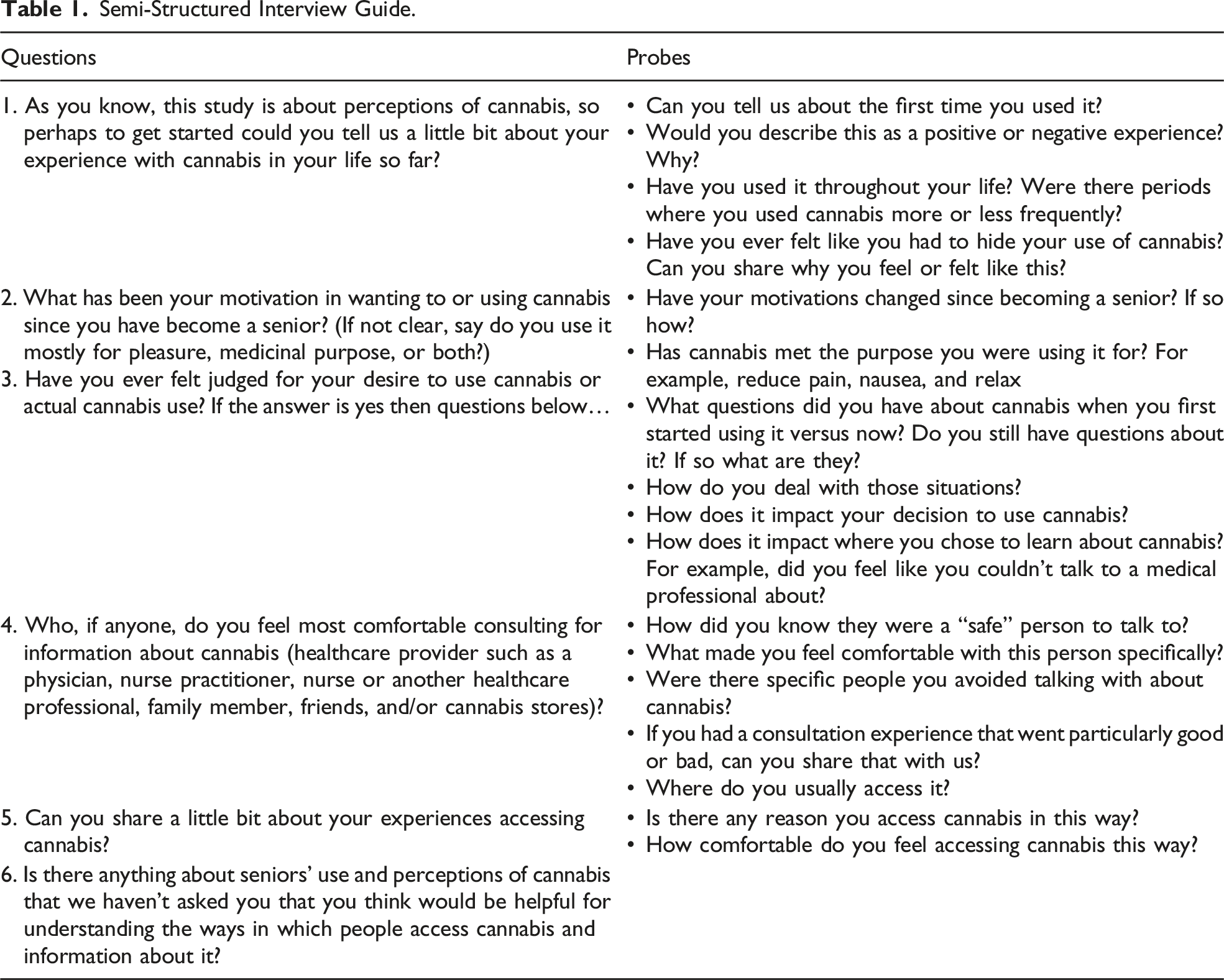
Semi-Structured Interview Guide.
Data Analysis
Data analysis was performed concurrently with data collection and involved a thematic analytic approach that was deductive, inductive, and reflexive. First, an initial, deductive codebook was developed based on our research objectives and interview guide, which were based on the theory of stigma (Goffman, 1963). Next, we used an inductive approach to develop codes that represented older adults’ experiences with stigma (Braun & Clarke, 2017, 2019). The RAs and project manager coded the first three transcripts. This enabled us to develop new, unanticipated codes about older adults’ experiences of stigma for the codebook. The full research team, including the PI, co-investigators, RAs, and the project manager, reached agreement about the codebook. The remaining transcripts were coded, also including unanticipated codes that researchers developed as significant to older adults’ experience with stigma. We used NVivo to support systematic coding across team members. The team met to discuss and group salient concepts within codes together to form categories and sub-categories. After further reflection, discussion, and analysis among the research team, categories and sub-categories were collated to develop coherent themes that described older adults’ experiences of stigma (Braun & Clarke, 2006, 2017, 2019; Vaismoradi et al., 2013). To help contextualize the thematic analysis, conceptually clustered matrices were used to map out participants’ demographic characteristics (e.g., age when first consumed cannabis) and the key features of participants’ narratives (e.g., reason for consuming, duration of cannabis use, and whether they had hidden cannabis consumption previously) and described their activities and interactions related to cannabis. Participants were given pseudonyms and are referred to by the sex they reported.
Analytic Rigor
Strategies to ensure trustworthiness were implemented throughout the research process (Lincoln & Guba, 1985; Shenton, 2004). Confirmability was ensured by maintaining an audit trail of coding decisions and researcher reflexivity. Credibility was achieved through methodological triangulation, remaining open to all potential themes, careful analysis of negative cases, and independent analysis of data by members of the research team. Reduction of the data and conclusion-drawing were supported by detailed verification. When disagreements arose about coding decisions or key categories to be integrated into themes, the research team debated our interpretations until intersubjective consensus (Miles et al., 2019) was achieved. Dependability was assured through in-depth methodological description, and transferability through the inclusion of participants’ demographic characteristics put the study in context (Lincoln & Guba, 1985).
Findings
Sample Characteristics (n = 36).
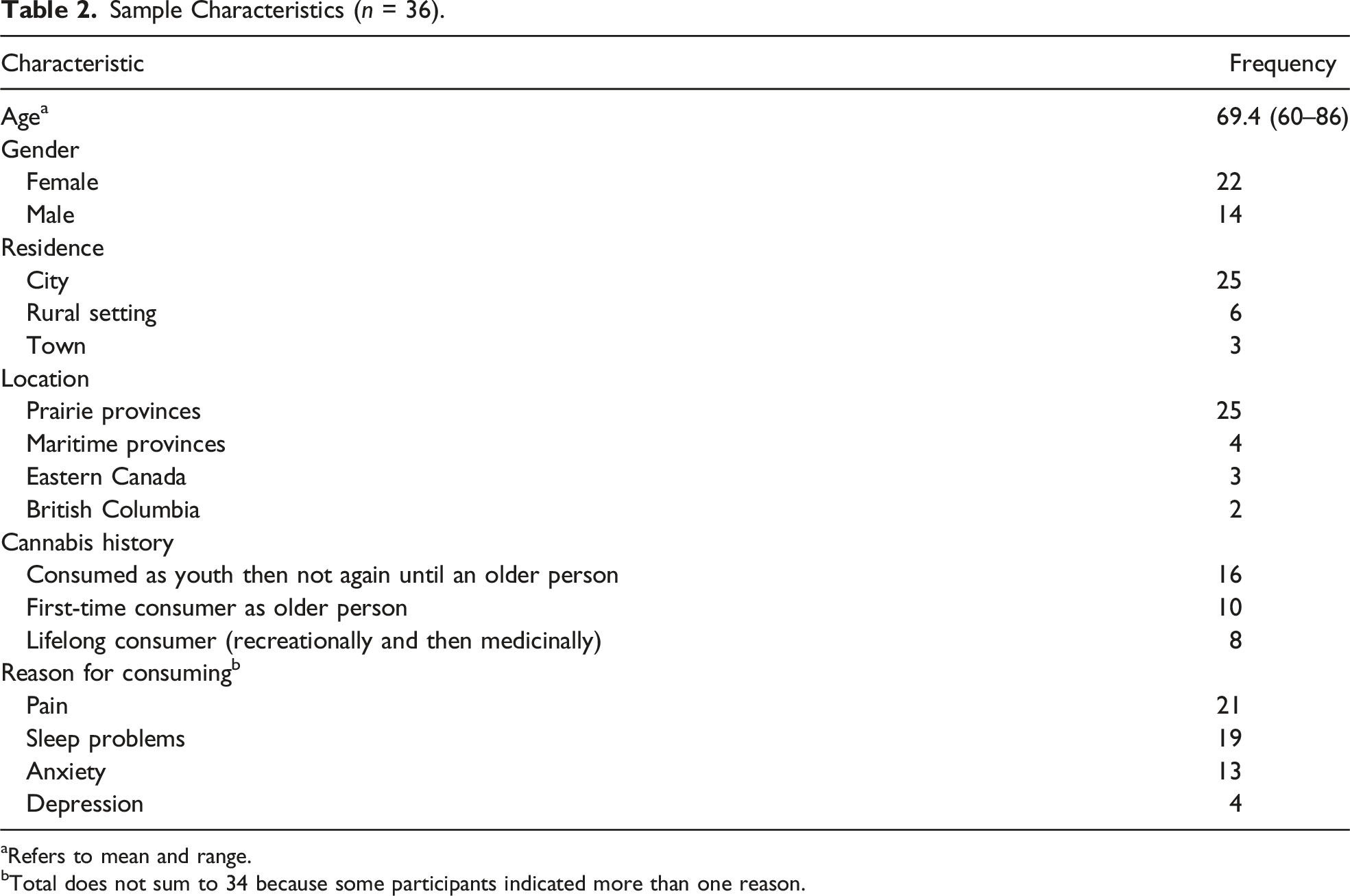
aRefers to mean and range.
bTotal does not sum to 34 because some participants indicated more than one reason.
Overall, participants’ descriptions demonstrated that they were keenly aware of the longstanding negative societal attitudes associated with cannabis and often internalized them. Participants who had consumed cannabis as youths, for instance, such as Dae and Kerry, explained that “when we were growing up it was considered a gateway drug. If you used cannabis you were going to turn into a drug addict.” Jay (who began consuming cannabis as a youth) recounted, “there was a stigma attached to it … you’d have to hide it from family members and schoolteachers … you’d have to hide it from the whole world.” Shiloh, who started consuming cannabis as an older person, conveyed the stigmatization he felt when he lamented that his physicians “put me on dope.” Jamie, who was a lifelong consumer, was an extreme case of stigma, recounting the profound impact on both her and her daughter’s social life due to her cannabis consumption leading her to not invite people to their home. She reflected: about how marijuana affected us and our family … it really affected my life.. socially, it really has affected me. It inhibited me. It crippled me socially … So I really feel it impacted me. And now, I feel I’m socially crippled. I struggle—like I’m seeing a counsellor over this.
Coping Strategies
We identified that older cannabis consumers employed four distinct coping strategies to manage stigmatization: concealing, re-framing, re-focusing, and proselytizing.
Concealing
Concealing involved carefully hiding cannabis consumption. Some participants felt they had to conceal their consumption more than others. Some responded to perceived stigma by remaining in the closet through “social avoidance” and removing themselves from settings where their stigmatized behavior may be judged. Other individuals chose to keep the sources of their stigma closely guarded through “secrecy,” refusing to disclose to anyone. Still other individuals engaged in “selective disclosure,” a variation of the secrecy strategy, which entails sharing sources of stigma openly with select people while maintaining secrecy with others.
Social Avoidance
Reagan (lifelong consumer) demonstrated social avoidance when he explained that previous experiences of being judged for cannabis use had taught him to simply avoid situations where he may have to disclose his consumption and described himself as “very much [in the] closet with it … Just for the stigma of it.” Similarly, Jamie (lifelong consumer), who is quoted above, practiced social avoidance to such an extreme that she identified the withdrawal as socially crippling.
Secrecy
Taylor (long-time cannabis consumer) related that he believed his cannabis consumption was something to be kept secret even if authorized to consume medicinally: “I still hide it. I mean even though I don’t have to anymore, I still do.” Paxton (who began consuming cannabis as a youth) explained that the enduring belief that cannabis is bad for one’s health spurred her to “keep it mostly to myself …. Just feeling that I might be judged or blamed … If I got sick in another way because [I] used cannabis.” Similarly, Shawn, Aron, and Paxton (all of whom who began consuming cannabis as youths) explained they concealed smoking cannabis “because some of the strains of the cannabis smells like skunk. Other people are impacted by the smell.” Participants who smoked cannabis often took extra precautions such as odor neutralizers or turned to other modes of consumption to mitigate the negative reactions of others.
The importance of concealing cannabis use through secrecy from children or grandchildren, especially when they were young, was underscored repeatedly in interviews. Often, participants’ rationale was that they did not want to be a poor role model or encourage younger people to start consuming cannabis recreationally. Casey (who started consuming cannabis as an older adult) felt that consuming cannabis was something to be ashamed of and, even though it had helped with his pain, ultimately stopped to avoid being a “negative role model” for his grandson. Casey explained that since: I had my grandson with me … It’s not really reasonable or appropriate to see that … it’ll probably encourage him to start using as well …. And so, the last people I want to talk to about it is my children. So yeah. I’ve been quite secretive about it … [I have not told] my wife ... It’s just me and myself.
Selective Disclosure
Other participants managed stigma by concealing it selectively, sharing their use only with those judged as safe to disclose to. Kennedy (who began consuming cannabis as a youth) expressed concerns about bringing up her cannabis consumption with a new social circle: “I haven’t said yet I’m on cannabis, because I don’t want somebody to maybe use that in a negative way … I don’t really want to start off on the wrong foot, because some people do have a wrong perception.” Skyler (long-time consumer) explained that she selectively disclosed her consumption secret by discerning, “If I’m in a place where no one is doing marijuana I wouldn’t bring out a joint … I just assessed the comfort level, of doing it where I don’t know if other people are comfortable with it.” It was unclear how participants assessed if others were comfortable and who might be accepting of their cannabis consumption.
Lifelong consumer Nico drew boundaries between: your personal life and your professional life. Sometimes there needs to be a line drawn between them, and I guess that [cannabis consumption] was something that was part of my personal life and people in my professional life didn’t necessarily need to know about it.
Parker (who began consuming as a youth) conceded that “I haven’t widely announced … and there’s certain people I wouldn’t tell.” Regular cannabis consumption thus required a balancing act for participants, who had to discern who they could openly share their cannabis use with and who they could not. Participants worried that they would be judged, like Jo who began consuming cannabis as a youth and described herself as being “judicious about who I would share it with, because there’d be raised eyebrows … I would definitely feel judged.” Thus, she was careful to only share her cannabis consumption with those she believed were “not judgemental. I would definitely feel judged if I exposed myself to some people.”
Some participants concealed their cannabis consumption to their healthcare providers because they feared judgement. Paxton (who began consuming cannabis as a youth) was forthright that “I still think there is stigma attached to it … I haven’t said anything to my doctor.” Jo (who began consuming cannabis as a youth) also indicated that she does not divulge her cannabis consumption to her healthcare providers because she was worried that they would not be supportive: “All of my doctors … they don’t know that I was using cannabis. And I guess I just—I didn’t want to hear a lecture … because of some perceived stigma.” Similarly, Nico (a lifelong consumer) did not disclose his cannabis use to his healthcare provider because he feared they would be judgemental and did not think his physician would have the necessary knowledge leading him to consuming cannabis without professional guidance: “I’ve had to self-medicate … I don’t think she would be comfortable prescribing it … I don’t think she would have the knowledge …. and I just don’t think she would support the use of cannabis.” Some of the participants who were brave enough to disclose their cannabis use to their healthcare provider had been rebuffed.
When Shawn (who began consuming cannabis as a youth) asked about the possibility of cannabis or homeopathic treatments as alternatives to pharmaceuticals, her provider responded dismissively, “no, no, there’s no room for that hocus pocus here.” Similarly, Brady (who began consuming cannabis as an older adult) recalled how: I asked my doctor if she would get me a prescription for it and my doctor said, “I don’t want to know about that.” … [even though] The pharmacist suggested to me that [I] should ask [my] doctor for a prescription for [my health condition].
When participants were discouraged from consuming cannabis to manage their health problems, they typically found a cannabis-friendly healthcare provider or clinic to assist them or turned to a recreational retailer. Aiden (who began consuming cannabis as a youth) explained that because “my previous family doctor, he wanted nothing to do with it … I had to go find a doctor that would prescribe [authorize] me.”
Other participants mentioned concerns about revealing their cannabis use to their religious communities. Jamie (lifelong consumer) described “religious” colleagues who hid their medicinal cannabis: “Some of the people I worked with were quite religious and yet they were doing CBD oil … the legality had changed and it was a medical prescription, [but] they were still hiding it from people in their congregation.”
Re-Framing
Re-framing is a stigma management strategy that involves “transforming the meaning” (Ashforth & Kreiner, 1999, p. 421) of something stigmatizing, often by infusing it with value and justifications of appropriateness. We discovered that older consumers sought to normalize medicinal cannabis by using language to re-frame its meaning and underscore its appropriateness. Artimis, who had been consuming medical cannabis for years, became bolder about their consumption “once it became legal, I’m willing to talk about it publicly.” Sage (who began consuming as a youth) captured what many participants conveyed—that even though she had used cannabis legally for health reasons, having the drug completely legal for all types of use allowed her to re-frame her medicinal cannabis consumption as normal and not something to be afraid of: It’s been a lot easier in the last couple of years to have a conversation than it was before it was legal. Because I got my first medical prescription before that it was legal … I remember looking over my shoulder. Is there anybody that I know … because in the back of my mind, I know that I’m going to a cannabis store.
Others also believed that the stigma attached to cannabis consumption was diminishing over time. Jay (a lifelong consumer) explained that negative judgement of cannabis has diminished as it has become more normalized in society. He expressed that: I think that as the populations changed and the baby boomers sort of grew up I think it was more acceptable. I don’t think I felt judged, I’ve told all my coworkers and such, they don’t judge you as much anymore this day and age.
Charlie (a lifelong consumer) concurred that older peoples’ “perception has softened and they’re definitely more open to it and they’re curious about it … society has shifted, and particularly because we’ve legalized cannabis.” Nico (a lifelong consumer) suggested that “the stigma was greater before it was legalized. I think there’s still a stigma now, because it’s just newly legalized, and I think as time goes on, as time passes, the stigma will be less intense,” and Harper (a lifelong consumer) described “coming out of the closet” when cannabis was legalized. Parker (who began consuming cannabis as a youth) expressed, “I’d be anxious if I was using cannabis and it was not legal, even if people had said to me, oh it’d be really good for your pain … I’m pretty sure I wouldn’t have used it.” Addison (lifelong consumer) suggested that “it’s finally legitimate, it’s regulated.” Similarly, Taylor (a long-time cannabis consumer) explained that “the culture’s better than it was 20 years ago, 30 years ago … I was, not advertising it exactly, but I was more open … so I had very, very, very positive results and I had very, very negative results.”
Participants noted that medicinal cannabis had recently become perceived as more legitimate among older people. Finley (who began consuming as an older adult) felt that: People our age are now being much more open talking about it, and saying here’s what I use and here’s what effect it’s had, and … my joints are hurting less, and … And I think perhaps up until not too long ago they would be hiding it.
Re-Focusing
Re-focusing as a strategy involves shifting the attention from stigmatized aspects or features to those that are not (Ashforth & Kreiner, 1999; Toubiana & Ruebottom, 2022). We saw this play out in our study as older consumers focused on cannabis as a legitimate treatment for health problems, in contrast to recreational users who got “high” or “stoned” as Bailey (who began consuming as an older adult) expressed emphatically, “I have never been stoned!”. Parker (who began consuming cannabis as a youth) was frustrated that many people: Still don’t understand that this is medical and I’m not using it get high ... It was really important to me to go to a clinic and the doctor … he’s been working with people using cannabis for a long, long time.
Part of the legitimacy was getting approval from a healthcare professional. Participants were deeply concerned that those who knew of their cannabis consumption understood that it was for “legitimate,” “medical” reasons. For Shawn (who began consuming cannabis as a youth), cannabis was merely one aspect of managing her medical condition: I have multiple myeloma and I’ve been living with it for 20 years. So, no. I mean, the two things kind of go together …. I don’t want to get high … I don’t bring it up … but if it does come up I’ll say I use the oil.
The positioning of cannabis consumption as therapeutic appeared to differentiate themselves from the stigma they associated with recreational use by re-focusing attention to therapeutic use as not stigmatized. Quinn (who began consuming cannabis as a youth) expressed that “I don’t think it’s the same realm [as recreational products] … it’s a registered medical use.” Artemis (who began consuming cannabis as an older adult) indicated that having a prescription made him more willing to openly discuss his consumption: “I have no problem telling people that I’m taking it as a prescribed [authorized] drug.”
Participants also emphasized that their choice of cannabis products (such as CBD oil) was not associated with recreational use and it could be easily hidden, and if they did smoke it, they would limit the times and places where they did so. Kerry (who had consumed as a youth) described CBD oil “as a therapeutic drug … I don’t think CBD oil is a recreational drug, I really don’t.” Aron (who began consuming as a youth) recounted “when it’s an oil like that, you don’t have to really hide it, because it’s, nobody really sees it.” Other participants who did consume THC therapeutically modified their consumption by only consuming it at night, as a sleep aid. Kerry explained, “The CBD is for pain management [during the day], the THC is for sleep.” Similarly, Brady (who started consuming as an older adult) described having “both the daytime and the nighttime” products.
Smoking cannabis was conflated with recreational use. To quote Robin (who began consuming as an older adult), “I would not use for recreation … I would certainly not want to smoke it.” Aiden (who began consuming cannabis as a youth) similarly explained: I don’t combust any cannabis … that’s used for people that smoke cannabis, they’re stoners. But I don’t consider myself a stoner. I consider myself someone that’s using this plant for medicinal purposes.
Participants described numerous alternative modes of delivery that they saw as more benign, such as topical gels or creams, capsules, or mouth spray. Paxton (who began consuming as a youth) noted that “some of the creams are really good for aches and pains,” and Artemis (who began using as an older adult) described her process for using a topical cream: With the CBD oil that has the THC in it, I mix two millilitres of oil with two tablespoons of cream that I use and I apply that to the arthritic in my hands and any other spots … before I go to bed.
For Jamie (lifelong consumer), who had recently retired, “if there was me getting caught smoking a joint at work ... I would have been fired ... I think for me, the real change has been since I’ve retired.” If cannabis could help with their chronic health conditions and possibly help them get off other medications, then it was entirely acceptable. Consequently, they re-focused attention from the stigma of recreational use to medicinal use. As Morgan (who began using as a youth) put it, “now that I’m retired … I realize … it’s something that we could use for medicine.” Hayden (who began using as a youth) similarly stressed that the combination of being retired and the legalization of cannabis made it seem less harmful “because I am retired ... it’s probably not so bad.”
Some participants such as Jude (who began consuming cannabis as an older adult) explained the difference between perceiving the product as medicinal or recreational cannabis could be related to where you obtained it: “I wouldn’t go into any of the popup stores or the franchise stores that are out there … I would rather deal with a company and people who deal with the high controlled part of distribution.” When participants found healthcare providers who were knowledgeable about the medicinal use of cannabis and a reputable source of obtaining it, they reported feeling comfortable sharing their cannabis consumption with them and it reinforced the differentiation between medicinal and recreational consumption. For example, Alex (who began using as a youth) was pleased with the ongoing support he received after accessing a cannabis clinic and noted that “the doctor ... phones me once a month just to see how it’s going and go over the amounts I’m taking.”
At times, participants had to rationalize and re-focus their consumption as medicinal with family members, as Alex (who began consuming cannabis as a youth) relates when caught using cannabis by an adult grandchild, he was quick to explain that it was a legitimate use with a prescription: “I went outside to do it, and here’s my granddaughter staring at me, and I went, ‘you know I have a licence for—or a prescription for this’, and they just kind of laughed.” Despite this legitimacy, Alex also noted how stereotypes about cannabis were still widespread even in his family relationships: “I have older sisters, they—you know, the old stereotype. I’m 62, and there is the stereotype out there … You’re a rebel.”
Proselytizing
We identify proselytizing as a stigma management strategy aimed at reducing and eliminating stigma. Specifically, the older consumers utilizing this approach sought to manage stigma associated with cannabis by seeking to persuade others about the benefits of medicinal consumption. Terry who began using as an older adult explained that “I belong to a cannabis club—about 90% of them are medical users here in the city, and I am as open as I can be about my cannabis usage.” Similarly, Tandy (who also began consuming as an older adult) educated others about the benefits of cannabis: “I tell everybody about it … when it stopped migraines … I was, you know, praising the value of it.” These participants were sharing their positive experiences with medicinal cannabis so that others could also experience the benefits.
A couple of participants shared their experiences of challenging the stigmatization of medicinal cannabis. Jo (who began consuming cannabis as a youth) suggested that she had become very vocal about her cannabis consumption: “I’m kind of outspoken about it with other people. And then they laugh, and think I’m kidding, but I’m not kidding.” Yet, she was careful to only be candid with those she believed were “not judgemental … I would definitely feel judged if I exposed myself to some people.” Harper (a lifelong consumer) felt a responsibility to be open to break the stigma, going so far as to put working at a cannabis grower on his resume because “(a) it’s legal, (b) I need to play a role in breaking the stigma because I think it’s not helpful.” However, it was notable that some participants who otherwise had no problems discussing their medicinal consumption of cannabis did not include their children. As Harper related, “I didn’t really talk about it with my kids until they started using … I didn’t put fear or encouragement into their minds, and I kept my cannabis use hidden from them.” It appears that even those who were trying to educate others still concealed their medicinal consumptions from some.
Coping Strategies and Cannabis Normalization
Notably, two of the strategies outlined above (re-framing and proselytizing) work to normalize cannabis consumption, while the other two (re-focusing and concealing) reinforce existing explicit and latent stigma. Re-focusing leads to the perpetuation of stigma by contrasting medicinal consumption with recreational consumption and concealing reinforces stigma by not confronting it. Our findings thus highlight the existence of a “stigma paradox”—older consumers’ attitudes and behavior simultaneously both disrupt and reinforce associated stigma. Thus, even those older adults who are medicinal cannabis consumers are tacitly reinforcing and reproducing stigma by rearticulating it. In effect, these forces neutralize or work against each other, potentially leaving processes of normalization at a standstill.
Discussion
One of our key findings was that older adults’ past experiences with cannabis as an illicit substance and the enduring stigma associated with it contribute to many believing they may be judged for consuming cannabis, even if it is for medicinal purposes. To manage stigma, participants concealed, re-framed, and re-focused their consumption, as well as proselytized to others about the benefits of medicinal cannabis. Most participants demonstrated or hinted at stigma regardless of whether they were a long-time cannabis consumer or had started consuming as an older person. Although there was variation in descriptions of stigma among participants, those who had consumed cannabis throughout their lives and those who had consumed as a youth were more likely to express the desire to conceal their consumption. Participants’ concealment to mitigate stigma parallels prior research related to mental health and chronic diseases (Corrigan & Rao, 2012; Link & Phelan, 2001, 2014; Quinn et al., 2017; Thoits, 2011). Armentor (2017), for example, reported that fibromyalgia patients concealed their symptoms and cannabis consumption from healthcare providers, family, friends, and employers for fear of stigmatization. Similar to our findings about the various forms of concealment (social avoidance, secrecy, and selective disclosure), Hathaway (2004a) and Reid (2020b) documented precautions users take to avoid broadcasting their cannabis consumption in public such as only consuming at home with familiar people; using eye drops to mask reddened eyes; and disguising odors by changing clothes after smoking, using scented products, substituting smoking with edibles, or eating mints or using mouthwash.
Another key finding was that many participants were reluctant to disclose their medicinal cannabis consumption to their healthcare professionals and those who did often encountered stigmatizing attitudes. This finding parallels previous research. Skliamis et al. (2022), for example, compared cannabis consumers’ perceptions of stigma in European countries and found that healthcare providers often held stigmatizing views about cannabis and cannabis consumers.
Our study adds to the debate regarding the intersection of medicalization and normalization, and how recreational legalization affects that debate, by exploring the post-recreational legalization landscape in Canada. Some of our participants discussed that medicinal cannabis was becoming more normalized since the legalization of recreational cannabis, and that retirement made their use more acceptable. Yet, there were still certain people who believed they had to conceal their consumption, even though it was medicinal, and others believed it had to be concealed from children and often from healthcare professionals. Normalization can be understood as a social process through which changes in thinking and behaviors are incorporated into mainstream society and also occurs in healthcare settings (May et al., 2009).
Much of the research on normalization and cannabis consumption has focused on youth and adults (Krediet et al., 2020; Mostaghim & Hathaway, 2013; Reid, 2020b; Sandberg, 2013). Reid (2020b) argues that cannabis stigma persists, and true normalization will not occur until those who do not consume cannabis no longer view those who do as deviating from normal society. However, scholars such as Sandberg have suggested that the normalization of cannabis has occurred in the “margins of mainstream society” (Sandberg, 2013, p. 65) with social stigma still occurring on both macro levels (i.e., cultural norms) and micro levels (i.e., individual experience; Reid, 2020b). This helps to explain why some of our participants were more comfortable proselytizing to others about the benefits of medicinal cannabis use and others concealed, re-framed, or re-focused their consumption.
Legalization seems to have helped legitimize cannabis consumption and reduce the perceived risks for older adults in the United States (Han et al., 2021). Baumbusch and Yip (2022) suggested that the normalization process in Canada has influenced older adults’ perceptions, making medicinal cannabis more acceptable than recreational consumption. Our participants were quick to differentiate themselves from recreational consumers, stressing that they were consuming medicinally and often under the supervision of health professionals, associating recreation use with more stigmatizations. Other scholars have also suggested that medicinal cannabis is less stigmatized than recreational cannabis (Reid, 2020b). Our study adds to this emerging body of literature by showing how older adults’ past experiences with cannabis as an illegal substance are enduring and contribute to their perceptions of stigma and varying levels of comfort with disclosure.
That many of our participants were only willing to disclose their cannabis consumption with those they felt were “safe” speaks to the continued stigmatization of cannabis, despite legalization. Moreover, the hesitancy of some participants to disclose their consumption of medicinal cannabis with their healthcare professional indicates that stigmatizing views of cannabis remain pervasive in mainstream medicine, due in part to the lack of clinical trials to determine its efficacy (Reid, 2020b). A cultural shift among healthcare professionals toward willingness to discuss possible cannabis consumption for health conditions and how it might interact with older adults’ medications is thus necessary. If older patients are unable to discuss these concerns with their healthcare providers, they may seek advice from less reputable sources that are unaware of their health conditions and prescription medications. Clearly, it is problematic that several of our participants described “self-medicating” because they were unable to discuss medicinal cannabis consumption with a healthcare provider.
Participants who engaged in re-framing or re-focusing their cannabis consumption for medical purposes did so by stressing its legality, differentiating their use from recreational cannabis as well as the type of products they consumed, as has been found in prior research (Newhart & Dolphin, 2018). This is an important distinction because most of the studies of stigma have tended to focus on the ways that consumers cognitively manage or manipulate stigma perceptions. In contrast, our finding of re-focusing stresses the importance of paying attention to the material dimensions and the way they can entrench stigma while also alleviating it for some groups. This can be understood as a social distancing mechanism achieved by altering the materiality of the products to avoid being considered recreational cannabis consumers, who were perceived as more deserving of stigma (Ashforth & Kreiner, 1999; Baumbusch & Yip, 2022; Canales, 2000; de Meis & House, 2002; Garcia et al., 2005; Meisenback, 2010).
By claiming that medical consumption of cannabis was entirely different from recreational use, participants endeavored to distinguish themselves from stereotypical recreational cannabis consumers (Bos et al., 2013; Meisenbakc, 2010) and enacted a “stigma hierarchy” (Toubiana & Ruebottom, 2022) that elevates medicinal users, while framing recreational consumers as meriting stigma. Most participants consumed CBD oil describing it as a medicinal treatment that was odorless and easy to conceal. Cannabis researchers confirm that CBD oils are the most common treatment for medical symptoms in the older adult population (Yang et al., 2021). This approach can be linked to some prior literature. Athey et al. (2017), for instance, have underscored the heterogeneity of how medical cannabis consumers define their use as medical. Accordingly, Athey, Boyd, and Cohen maintain that the boundary between recreational and medicinal use is blurred as many consumers pursue cannabis for both therapeutic and recreational effects. The authors stress that motivations for using cannabis are context-specific (pg. 226) and that usage and the meaning associated with it are variable. Thus, rather than viewing recreational and medical marijuana use as dichotomous, it should be conceptualized as “existing on a continuum” (Athey et al., 2017, p. 227).
Limitations
Despite the rich descriptions that participants provided to illuminate the role that stigma plays in their experiences with medicinal cannabis, this study is limited by a relatively small number of participants and was conducted exclusively in Canada. The findings may therefore not be transferable to all jurisdictions. Additionally, many of our participants received authorization for cannabis from a medical cannabis clinic. Given the reluctance of many older adults to discuss cannabis with their healthcare professionals, our findings may not be representative of all older medicinal cannabis consumers’ experiences. Finally, our remote interview approach facilitated recruitment during the COVID-19 pandemic, but also precluded observing participant body language and non-verbal cues that may have enhanced the interview dialogues.
Implications
Understanding older adults’ stigma management behavior related to medicinal cannabis will help to inform knowledge products and provide guidance to healthcare professionals in their conversations with this population. The frequent occurrence of older adults being discouraged from consuming cannabis by a healthcare provider or their provider being unknowledgeable is problematic. Our finding that long-time cannabis consumers were less likely to disclose their use to healthcare providers suggests the importance of healthcare professionals inquiring about possible use in a non-judgemental manner. While the literature indicates that older cannabis consumers are at risk of developing psychosis, as well as diminished attention, memory, and learning (and one can thus understand why physicians are reluctant to recommend or authorize it), there is also early evidence suggesting that cannabis is effective for treating numerous conditions (Bobitt et al., 2020; Choi et al., 2021).
Furthermore, given that older adults are actively seeking cannabis as a potential treatment, it is crucial that healthcare providers are open to discuss it and sufficiently informed to credibly answer older adults’ questions. If older adults do not receive guidance from their healthcare providers, they may seek information from unqualified retailers or consume recreational cannabis for medicinal purposes and actively hide use from their healthcare provider. Both of these scenarios increase the risk of interactions with other medications. Education for healthcare professionals about the potential for cannabis in treatment of medical conditions is therefore needed. Accurate information about cannabis for medical issues and possible negative consequences needs to be available to older people in many different forums. Further research is needed to understand how best to provide older people with accurate information about medicinal use of cannabis in ways that can minimize stigmatization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the Social Sciences Humanities Research Council #430-2021-00003.