
Abstract
Pediatric hematopoietic stem cell transplant (HSCT) is an intensive treatment that can be life-threatening. All family members experience distress. We conducted a grounded theory study using a family systems-expressive arts framework to develop a theoretical understanding of the family experience of HSCT. Six families (15 family members) participated in two interviews, drew an image, and were guided through a “dialoguing with images” process. Participants did not always perceive HSCT as an experience they had lived as a family and were surprised to hear other family members’ experiences. While one mother drew, she suddenly understood it was not only her ill child, but the entire family who had “fallen down the rabbit hole.” The family experience of HSCT is described across (a) the pre-HSCT trajectory, (b) family fragmentation (hospitalization), and (c) family reintegration. We identified a critical need for targeted family intervention during the transition into HSCT, throughout and following hospitalization.
Keywords
Imagine your child becomes seriously ill, and you are asked to live in an isolation room, 7 days/week, 24 hours a day, for weeks, even months. In this room, you witness your child’s suffering while facing overwhelming caregiving responsibilities. What would this mean for you as a parent, your ill child, your family? This is what families face when their child needs a hematopoietic stem cell transplant (HSCT). HSCT is an intensive treatment that represents a unique period of illness crisis for child and family, and there is no guarantee the child will survive (Packman et al., 2010).
HSCT is increasingly used as a treatment modality for a wide spectrum of serious pediatric illnesses, including malignant disease, primary immune deficiencies, hemoglobinopathies, inherited bone marrow failure syn-drome, metabolic/genetic disorders, and leukodystrophies (Guilcher, 2016). Despite the expanded use of HSCT, there has been limited research on the emotional and relational impact on the family (Jobe-Shields et al., 2009; Packman et al., 2010; Pentz et al., 2014; Ullrich et al., 2016). We do know family functioning plays a pivotal role in determining the distress experienced by the ill child (Jobe-Shields et al., 2009; Packman et al., 2010). Uncertainty, distress, worry, and fear are prevalent for ill children and family members (Packman et al., 2010; Ullrich et al., 2016). Family members have also reported anxiety, depression, mood symptoms, behavioral/social problems, low self-esteem, and post-traumatic stress symptoms (Chang et al., 2012; Manne et al., 2004; Packman et al., 2010). During HSCT, siblings yearn to feel they are a part of the family, but this is challenging due to marked changes in family roles and relationships (Wilkins & Woodgate, 2007). When a sibling is the HSCT donor, families face heightened complexity in treatment decision-making, and siblings’ needs are not fully met during the donation process (Pentz et al., 2014; Wallace et al., 2014). Family life becomes consumed by the survival and care of the ill child (Kazak et al., 2020; White et al., 2017). High family expressiveness and cohesion play a protective role against ill child distress during HSCT (Ho et al., 2002; Jobe-Shields et al., 2009) and also contribute to improved adjustment in the long term (Phipps & Mulhern, 1995). However, conversations about HSCT are emotionally painful for families and often do not occur (White et al., 2017).
All family members experience distress, not just the sick child (Jobe-Shields et al., 2009; Kazak et al., 2020; MacLeod et al., 2003; Packman et al., 2010; Pentz et al., 2014; Ullrich et al., 2016; Wilkins & Woodgate, 2007). It is not sufficient to focus on the emotional care of the ill child and the parent at the bedside (Rolland, 1987, 1994; Rolland & Walsh, 2006; Wright & Leahey, 2013). The unique suffering experienced by the family needs to be addressed more comprehensively (Packman et al., 2010; Rolland & Walsh, 2006; West et al., 2015). The first step toward this goal is to better understand what it is like for families to live through HSCT.
The key limitation in previous research is that “family” has been primarily studied from the perspective of individual family members (i.e., recipients, siblings, mothers), rather than the family unit (Jobe-Shields et al., 2009; Loiselle et al., 2016; Packman et al., 2010; Ullrich et al., 2016; Wilkins & Woodgate, 2007). To address this limitation, we used a family systems-expressive arts theoretical framework (McNiff, 1991, 2004; Rolland, 1987; Wright & Leahey, 2013) to study the complex relational interactions that occur in the family, as well as between family members and clinicians during HSCT.
Theoretical Frameworks
Family Systems
When a child is ill, family members are also impacted; reciprocal influences are constantly occurring between illness, child, and the family (Arestedt et al., 2014; Jobe-Shields et al., 2009; Packman et al., 2010; Rolland & Walsh, 2006; West et al., 2015). A family systems approach to research in pediatric illness has been increasingly supported. Despite this, there is limited evidence about the impact of HSCT on the family system (Packman et al., 2010; Wilkins & Woodgate, 2007). We adopted a family systems theoretical orientation: The family was viewed as a relational system in constant interaction internally, and with external systems (i.e., health care system) (Rolland, 1987, 1994) (Rolland & Walsh, 2006; Wright & Leahey, 2013). This orientation challenged us to focus on multiple levels of relational interaction, rather than the distress of individual family members (Wright & Leahey, 2013).
Expressive Arts
We simultaneously adopted an expressive arts orientation based on the work of Shaun McNiff, (1992, 2004, 2008). McNiff (2004) suggested that art diagnosis systems (i.e., expert interpretation, scoring of art images) can work to reduce the complexity and richness of images. He argued for an open engagement with art in the research process, honoring different interpretations, particularly those of study participants. He implores arts-based researchers to affirm the otherness of phenomena, to treat art images as an imaginal other, and to facilitate the images’ presence and voice in the research process. Within the “dialoguing with images” data collection process adopted in this research, the image was understood to have its own voice, as being “other,” rather than being only a symbolic representation of the inner lives of the participants (McNiff, 1991). The image became personified through the dialogue process and had something to say about the research topic that was unique to what would have been possible through words alone. The “dialoguing with images” process holds a kinship with constructivist grounded theory (Charmaz, 2014), as it provided a more nuanced, arts-based approach to extending the co-constructed dialogue within the interviews. New understanding was facilitated as a dialogue was created between family participants, researchers, and the image.
The “dialoguing with images” data collection approach used in this work had been described previously (McNiff, 2004), but had limited use in prior research (Dusome, 2010). To our knowledge, it has never been adapted for use with families in the context of serious pediatric illness. Family members who participated in this study were invited to draw images of their experience of HSCT during the second interview. The images were then brought to life and given agency by being actively engaged in a dialogue with the researcher(s) and participant(s) (McNiff, 2004). This occurred through an eight-stage “family level dialoguing with images” process (see Table 1).
Stages of the Family-Level Dialoguing With Images Process: Arts-Based Data Collection.
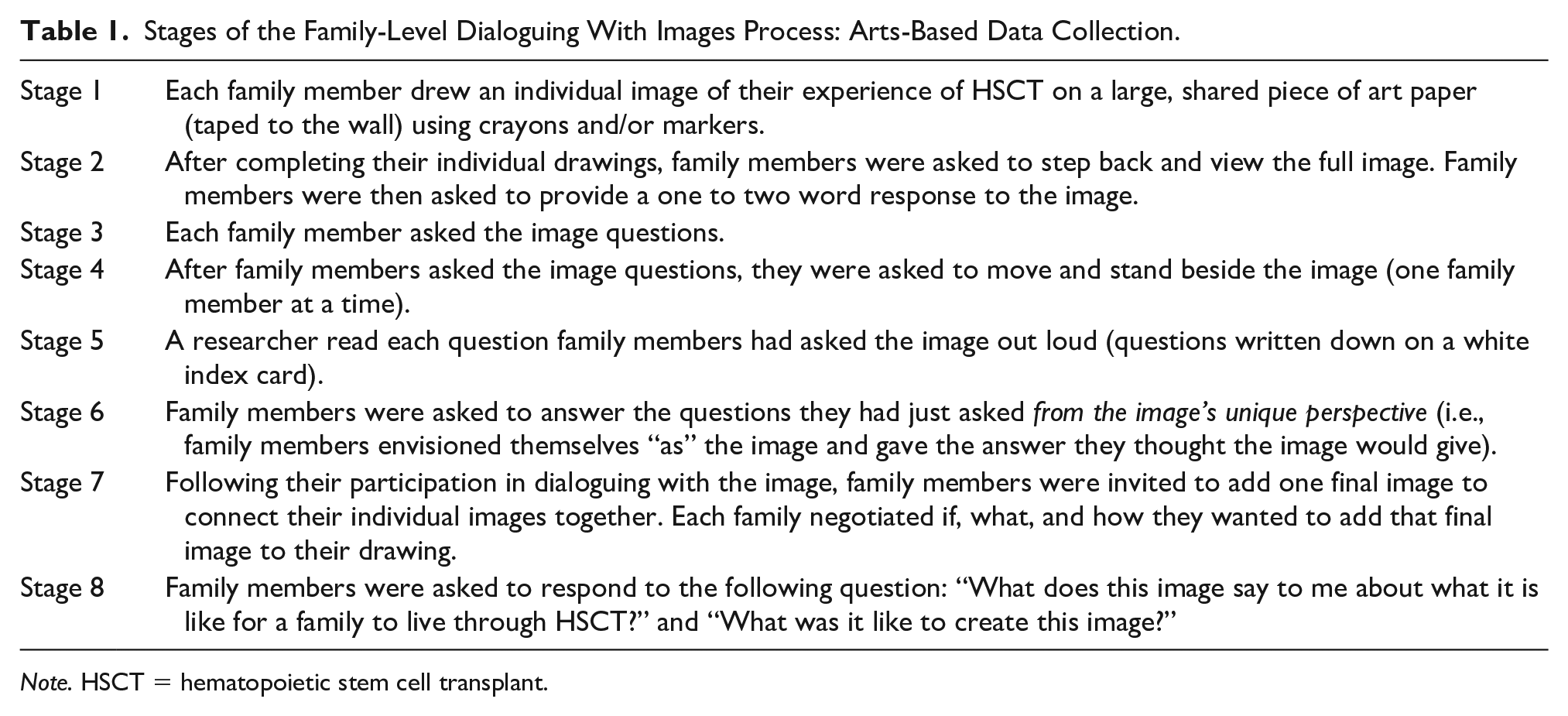
Note. HSCT = hematopoietic stem cell transplant.
Five of the six families in this study chose to participate in the “family level dialoguing with images” process. Throughout the family-image-research dialogues, the researchers facilitated conversation by directing questions to different family members. The “dialoguing with images” process has been used in clinical and education contexts previously (McNiff, 2004), but in this study, we specifically adapted this approach as a research method.
The research questions that guided this study were the following: (a) How do families transition through the process of HSCT in serious pediatric illness? and (b) What contextual factors influence the family transition through HSCT in serious pediatric illness? Our research findings will lay the foundation for addressing the complex needs of family members through the advancement and testing of family systems-expressive arts intervention approaches in future research and practice.
Method
We employed a qualitative research design to develop a theoretical understanding of child and family experiences of HSCT. Using constructivist grounded theory methodology, we explored the social processes that occur across HSCT by examining socially embedded meanings and actions within child and family experiences (Charmaz, 2014). This sensitized us to action and process with the aim of generating theory, rather than providing a thematic descriptive account. This qualitative research study was conducted between 2015 and 2018.
Study Participants
We recruited participants using purposive and theoretical sampling (Charmaz, 2014; Corbin & Strauss, 2008). Family members eligible for participation included parents/legal guardians, parent partners who were not biological or adoptive parents, child/adolescent HSCT recipients, and siblings. Participants were aged 7 years or older at the time of enrollment in this study. Additional inclusion criteria included the following: HSCT occurred no less than 6 months or more than 5 years before enrollment in this study, the ill child needed to be living, and participants needed to speak and read English. Although our intent was to enroll all eligible family members in each participating family, in some families, only certain family members chose to participate. In this situation, the focus remained on the family system through the type of questions asked and orientation of the data collection strategies. Participants were recruited through a major blood and marrow transplant program in Canada, following study approval from the university ethics review board and site access committee.
Data Collection
After a research coordinator identified potential participants, a letter of introduction from the clinical medical director and the lead study investigator was mailed to the parents/legal guardians. The research coordinator then contacted each family by phone to see if they would like to receive further information. The lead investigator contacted families who agreed to receive further information. Parents provided written informed consent, which included their permission for research team members to approach the eligible children in their family. Eligible child participants were then introduced to the study and completed verbal and written assent. Research participants could choose to withdraw from this study at any point.
Data collection and analysis occurred concurrently (Charmaz, 2014). Each participating family was asked to complete two qualitative interviews. An interview guide was used for only the first narrative interview (see Supplementary File, Interview Guide). During the second qualitative interview, the “dialoguing with images” process was followed (see Table 1). Two researchers facilitated each interview (digitally recorded [audio]). Five of the six families completed two interviews. One family only completed one narrative interview (chose not to complete the drawing/dialogue process). The time between interviews ranged from 2 to 6 weeks. The drawing/dialogue activity to be completed in the second interview was introduced at the end of the first interview. Each family member was asked to think of an image that would represent his or her experience of pediatric HSCT. They were told that when they returned for the second interview, they would be given an opportunity to draw that image and the researchers would help them share a conversation with their image, allowing them to express aspects of their experience which might not be accessible with words alone.
Data Analysis
Following each interview, the researchers met to debrief and discuss their initial analytical impressions. The transcribed research interviews were coded using line-by-line and focused coding (Charmaz, 2014). Focused codes were clustered leading to the development of theoretical categories (Charmaz, 2014). Theoretical integration occurred as we explored the relationship between the substantive categories (Charmaz, 2014; Glaser, 1978). Ongoing memo-writing occurred concurrently throughout data collection and analysis, documenting the theory construction process (Charmaz, 2014). This analytical process facilitated an interactive and prolonged engagement with the data, in which a critical conceptual dialogue occurred between the researchers, data, codes, and categories. ATLAS.ti (2013), computer-based qualitative data management software program, supported the analysis process. All participant names have been replaced with pseudonyms to maintain confidentiality.
It is important to note that we coded and analyzed the corresponding dialogue of each image, rather than the image itself. This relates to the expressive arts orientation adopted within the research process and the construction of meaning that is an integral aspect of constructivist grounded theory (Charmaz, 2014). McNiff (2004) clearly identified that in using an expressive arts orientation, it is the research participant’s interpretation of their art (created images) that must be privileged. The image interpretations included in the analysis process were carefully elicited through the “family level dialoguing with images” process used in this study.
Constant comparative analysis (Glaser & Strauss, 1967) facilitated a careful comparison of similar and different data from diverse sources (research interviews, field notes, analytical memos, transcribed dialogue for each image). In addition, we conducted a detailed analysis across family–family data, as well as within specific groupings of family member data (i.e., mothers, fathers, siblings, ill children, parent–ill child, parent–parent, ill child–sibling[s]). This systematic analysis across family member groupings was also guided by constant comparative analysis (Glaser & Strauss, 1967) leading to the development of the inductively derived theory reported (see Figure 1).
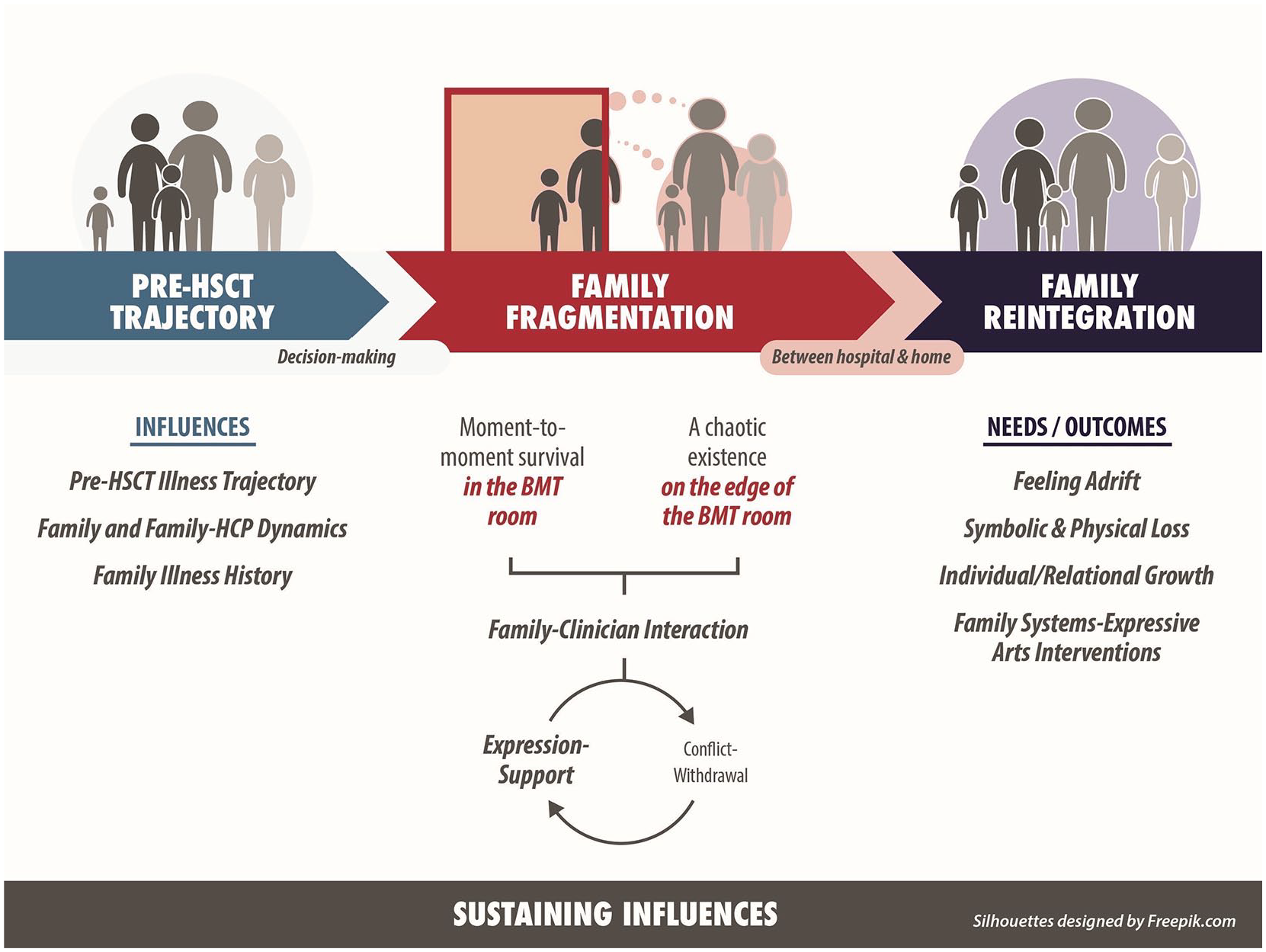
The family transition through pediatric HSCT.
Multiple research team members were involved in the concurrent data collection and analysis. Two team members coded each of the research interviews for the first three participating families. As the analysis proceeded, there was strong consistency in the focused codes and categories used for later coding processes. Due to this consistency, one researcher coded the interviews completed with the final three participating families. All team members similarly reviewed those coded transcripts, and any coding discrepancies were resolved through team discussion. Ten separate coding templates detailing the analytical evolution of the categories, subcategories, and focused codes were developed, which informed the inductive theory (see Figure 1). Individual research bias was addressed within the analysis discussions and the researcher debriefings that followed each research interview.
Results
Study Sample
We enrolled a total of 15 family members from six families: six mothers, two fathers, one male partner, three HSCT recipients (8–21 years), and three siblings (11–16 years; note: these were the ages at the time of study participation). The time since HSCT in the recruited sample ranged from 2.5 to 5 years. The HSCT recipients ranged from 3 to 17 years at HSCT. The diagnoses included cancer, hematological, and genetic disorders. All family members in this study continued until completion. One family chose not to draw an image as part of their participation in the study, participating in only one research interview.
Research Findings
The family transition through pediatric HSCT based on the unique experiences of children and families is detailed in Figure 1. Each of the three distinct phases of HSCT brought unique difficulties into family life (pre-HSCT trajectory, family fragmentation [during hospitalization], and family reintegration). The hospitalization period was a particularly distressing period. Within the drawing process, HSCT was described by families as “fearful chaos” (mother), “stormy” (father), “turmoil and despair” (mother), “wanting to go home” (recipient), and “ground hog day . . . reliving a bad day over and over . . . they were never ending” (mother).
One of the key findings is that family members did not always see HSCT as an experience they had lived as a family, but rather, one experienced by the ill child. As they participated in this study, they came to see the distress experienced by others. Participants had not been able to voice their experiences with one another during or after HSCT. When one mother was asked to think of an image that would represent HSCT, she immediately envisioned her ill child “falling down the rabbit hole,” as in Alice’s Adventures in Wonderland (Carroll, 1907). It was only during the drawing process, that Jane (mother) came to understand it was not just Amy (recipient), but the entire family who had fallen down the rabbit hole. This knowledge was not available to her until she drew her image (see Figure 2).
When I started thinking the image, it’s like . . . in Wonderland down the rabbit hole . . . and my vision was of Amy [recipient] . . . falling . . . having to make choices, but what came out for me . . . it was all of us that went there . . . As I started drawing it, I ended up drawing all of us . . . holding hands . . . it was our journey as much as it’s hers . . . It was ours together.
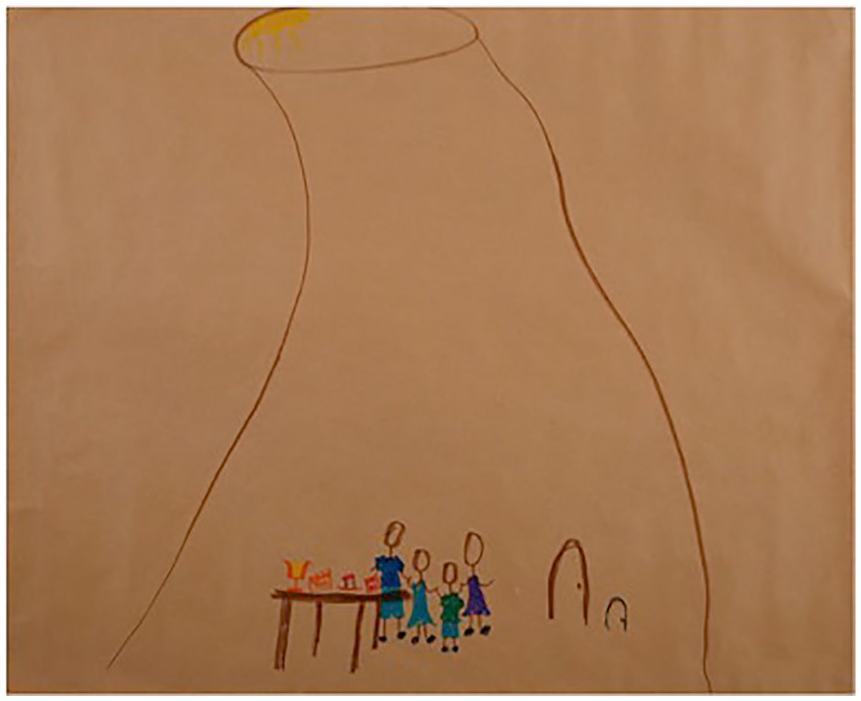
“Inspiring ~ It’s a Long Way Down”: drawn by mother (Jane), who later reflected on the impact of creating her image: “I didn’t think I was going to cry.”
Phase I: The Pre-HSCT Trajectory
The pre-HSCT illness trajectory
The period pre-HSCT was unique for each family. However, for all families, their individualized trajectory prior to HSCT hospitalization influenced their treatment experience. For example, when a child had lived through intensive treatment pre-HSCT (such as in cancer care), families were left exhausted emotionally and instrumentally. When the child had not undergone intense therapy or extended hospitalizations prior to HSCT (such as in hematologic and genetic disorders), there were increased family resources available as families entered the HSCT hospitalization period.
Family and family–clinician relationship dynamics
Relationship dynamics within the family and those shared with clinicians pre-HSCT also had a meaningful impact on the HSCT experience. Family fragmentation across hospitalization was accentuated when families had experienced challenging relationship dynamics internally, or with the health care team. For the one family who experienced significant conflict with clinicians pre-HSCT, that interactional pattern became a defining aspect of their HSCT experience.
Family illness history
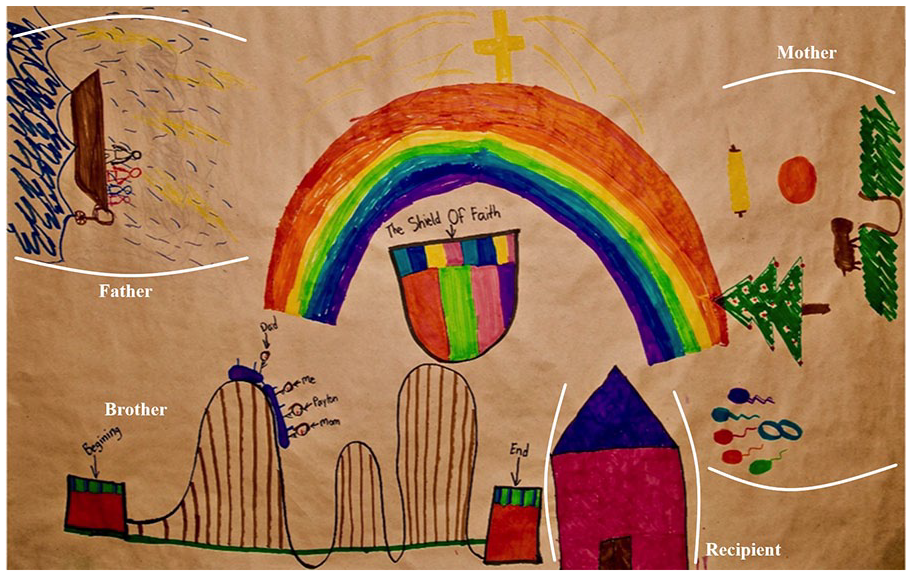
The family illness and loss history was also a potent mediator of family experiences. For example, one family had experienced the death of another child from the same disease, a number of years prior to the recipient’s transplant. The child who had died was an important source of strength for all family members; they felt that Zoe acted as their “guardian angel” during HSCT. She sustained the family and provided hope that Alex (recipient, adolescent at HSCT) would survive. In this family’s drawing, each family member represented Zoe in their individual drawing in some manner (note: Alma [mother] wrote her real name on the drawing above her broken heart, but it was removed for confidentiality reasons; see Figure 3).
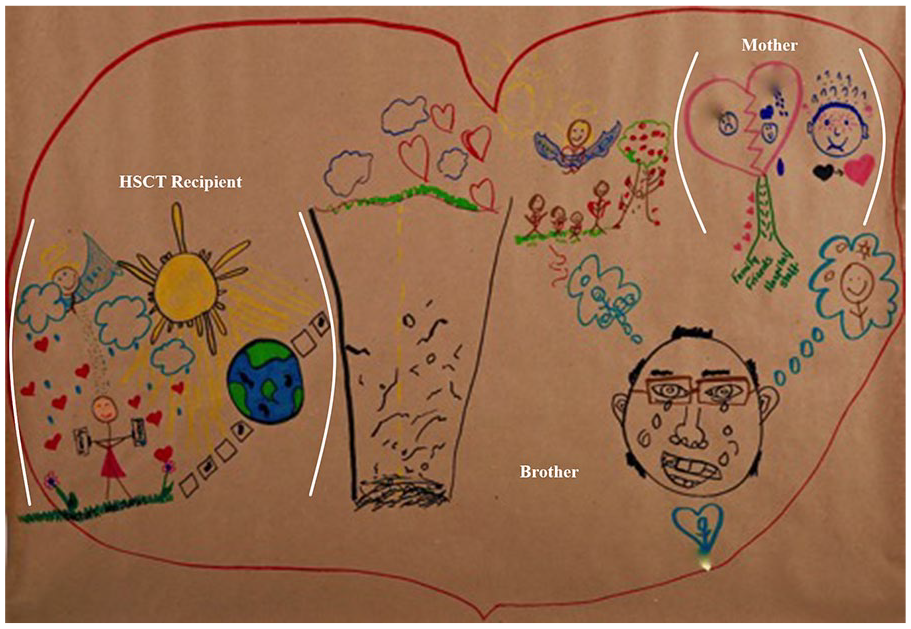
“Fearful Chaos”: brackets attached to specific images indicate family members’ individual drawings (Alex, recipient; Alma, mother); images in the drawing with no brackets are images Kevin drew (brother): the road with “potholes” (center of full image), and Zoe (“guardian angel”) with family, tree, and hearts. After this, Kevin drew his dad (beside bumpy road), with tears coming down his eyes. He started by drawing his dad’s nose and “boogers.” At first, Alex (recipient) was slightly annoyed, thinking he was not taking the drawing activity seriously. During the “dialoguing with images” process, Kevin shared that his father had cried at home. His mom and Alex learned about this for the first time in this interview.
Phase II: Family Fragmentation
Moment-to-moment survival in the transplant room
A tenuous process of family fragmentation occurred across hospitalization, which included family role strain and separation. Families felt torn apart, physically and emotionally; they focused on the ill child’s survival while existing in fragmented pieces across different life spaces. At least one parent from each family lived in the transplant room in protective isolation, 24 hours/day. These “parent caregivers” left the treatment room for only short periods of time: to eat, shower, and shed the tears they carefully contained while with their ill child. The unrelenting caregiving demands made it almost impossible for most parents to meet their own physical needs, let alone those of an emotional nature.
We had to bathe him four times during the day, I had no one to help me . . . That was killer on me . . . to wake him up and have a barf bucket . . . floating in there [bath tub] . . . because he was vomiting . . . oh, man! . . . Tommy’s mucositis was so intense . . . we actually had to . . . suck it out of him . . . when he was vomiting . . . pure blood and pooping blood . . . the lining of his intestines were all sloughing off and I really can’t believe he lived. (Alala, mother)
A different mother described this existence as living with a “torn heart” (see Figure 3). The parent in the room knew they needed to be at the hospital, but emotionally, they existed in a space between the transplant room and home, feeling intense guilt for the separation from other family members, particularly siblings. This was symbolically represented in Alma’s image of a broken heart. On either side, she wrote the name of each of her living children: the recipient and her brother. Above this, she placed the name of the sister who had died of the same disease (names removed from image to protect confidentiality).
Parents were traumatized as they witnessed their child’s suffering, but had no ability to emotionally process this distress due to the intense caregiving demands. Parents felt that clinicians primarily interacted with them as caregivers and sustainers of the ill child. This was particularly apparent during the hospitalization period when the treatment intensity and suffering of the ill child was heightened. During hospitalization, the unique suffering of these “parent caregivers” was not always explicitly addressed. Parents also recalled the heavy workloads carried by clinicians, which had been communicated in an implicit manner. Although not voiced, the scenes parents witnessed in the hospital communicated this information: That was the one little piece in the whole process for me that was missing . . . in that room I was fine . . . I knew what my job was in there. It was once I walked outside . . . I was . . . at a complete loss . . . just to have that [support] for me as a parent . . . I was in there all day, every day . . . I missed my son . . . my husband . . . I’m watching my kid . . . in a horrible experience and now there’s a nurse . . . who’s going to be here . . . Where do I go? You can’t ask the nurse . . . you walk out in the hallway and everybody else is so busy . . . It is very trying . . . I didn’t want to eat in front of Amy . . . I would snag whatever I could . . . I mean the nurses didn’t have time . . .there’s no way I wanted to take up . . . 10 minutes of . . . these people are doing amazing things with these children . . . I’m sure if I had . . . said, “can I cry on your shoulder for 10 minutes?” they would have . . . (Jane, mother)
Across hospitalization, parents’ attention and resources were intensely focused on supporting the ill child’s physical and emotional survival from one moment to the next. During this time, parents and children genuinely appreciated instances of human connection with clinicians, which sustained families during treatment.
Alex (recipient): I . . . cracked her shell [HSCT physician] . . . joke about silly things . . . Researcher: How did you know you cracked her? Alex: I think one time she cried in front of me when I wasn’t doing very well. And that was like the moment that I knew that she . . . really cared for me . . . she changed over the time . . . She became like family more than our doctors . . .
It was important to family members to feel that the child/family–clinician relationship existed on a human, as well as a professional level.
A fearful, chaotic existence on the edge of the transplant room
Family members who lived on the edge of the transplant room experienced a precarious existence: They reluctantly carried on with everyday life while bearing intense, unseen grief. They lived a fearful, chaotic existence that remained largely invisible to the parent and child in the transplant room, or to clinicians (see Figure 3). During this study, participants were surprised to hear how other members of their family had experienced HSCT. Prior to this research, they had not fully understood what others had endured emotionally and had not shared their experiences.
The emotional separation between those in the transplant room and those on the edge of it became further evident during the “dialoguing with images” process (McNiff, 1992, 2004). For example, in Jane’s (mother) image of her family at the bottom of the rabbit hole, she left all family member’s faces blank; there were no facial features or expressions added (see Figure 2). After drawing the outline of each family member, Jane physically backed away from the drawing, but then slowly moved back toward it to draw the faces. She stopped herself, stepping back again. She did not speak about this while drawing. During the dialoguing process, Jane was asked what she thought her daughter (recipient, not present) would ask the image. The question she gave for her daughter was: “Mom . . . Why no faces?” Later, Jane responded as the image in answer to this question: “Because I didn’t know how you were feeling.” Jane came to a new understanding about her family’s experience of HSCT as she entered a dialogue with her image. As she spoke, there was a hushed, almost sacred tone shared between Jane and the researchers. Jane further explored why she could not draw faces on family members after drawing her image: I couldn’t. I thought about it. I went to do it . . . I don’t even want to guess at where their thoughts . . . heads were . . . I would put a smile on my face . . . But that wasn’t what I was thinking then . . . That was the part that . . . surprised me the most, I . . . didn’t even know what to put there . . . I couldn’t pick . . . because I was feeling 857 things . . . you try and know what your kids are thinking but I wouldn’t want to guess what kind of monsters were in their heads at the time. My husband and I . . . as much as we talked . . . I had a job . . . I had to do this . . . I had a purpose . . . He just had to . . . stand by and hold the walls up . . . I don’t even know what he was . . .
A father from a different family drew his family in a boat on the sea in a storm, and said, “no matter how hard I tried I could not make the storm dark enough.” He, similarly, did not draw expressions on any of the faces. Instead, family members’ faces were again left blank, empty space (see Figure 4). Of additional note, a mother from another family drew a dark, black tornado to express her HSCT experience. She used very similar words to describe her frustration with not being able to make her drawing dark enough: “no matter how hard I push on this, I can’t make it dark enough” (see Figure 5).
“Ups and Downs”: brackets surrounding images drawn by Joe (father), Judy (mother), Payton (recipient), and William’s roller coaster (no brackets) are family members’ individual images. After the dialoguing process, Payton/William eagerly (laying their bodies on the table over the image) drew the family “shield of faith” and a rainbow (mother’s idea) to connect their images. Mom and dad helped to choose the colors for the rainbow.
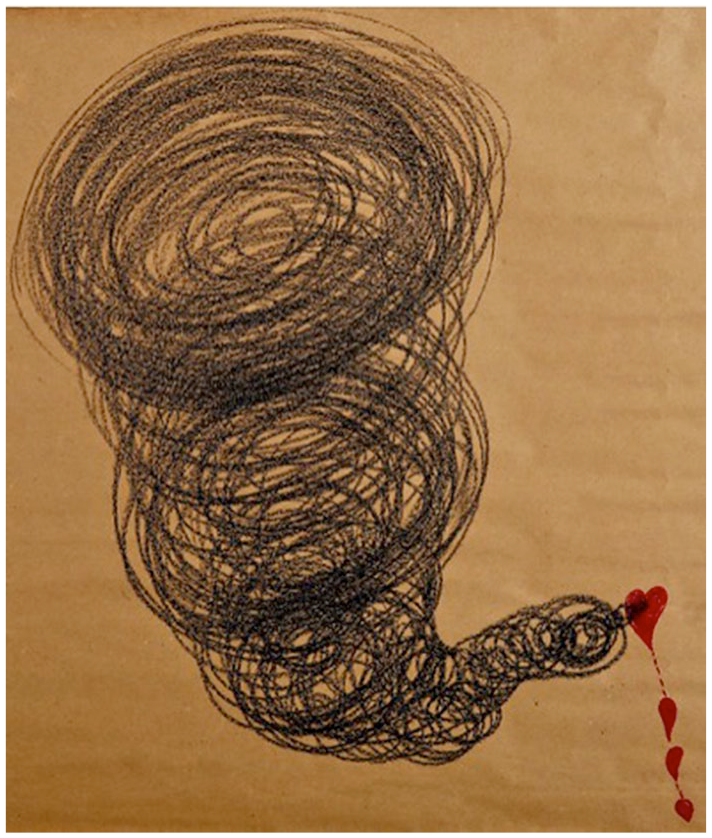
“Turmoil and Despair”: “No matter how hard I push on this, I can’t make it dark enough” (visceral, heavy thumping on the table as Alala drew this image). “Show them this, maybe then they will understand what it is like to go through HSCT.”
Two Patterns of Family–Clinician Interaction: Expression–Support or Conflict–Withdrawal
During hospitalization, one of two key patterns of family–clinician interaction was evident: expression–support or conflict–withdrawal (Tomm, 1980; Wright & Leahey, 2013). Families who experienced a supportive relationship with clinicians also experienced instances of conflict. However, it was short lived. Similarly, the one family who experienced an ongoing pattern of conflict also experienced supportive moments with clinicians. Families felt gratitude for clinicians’ efforts to save their child’s life. They understood that their child was not the only child receiving a transplant and were acutely aware of the emotional burden carried by clinicians.
Expression and support
Five families experienced an expression–support family–clinician pattern (Tomm, 1980; Wright & Leahey, 2013). Here, relationships were characterized by mutually determined care goals, respect, and the creation of a therapeutic space where family questions and thoughts were actively explored and heard. This pattern led to meaningful relationships with clinicians; the impact of this care endured for years after treatment.
Clinicians acted in specific ways to establish and maintain this interaction. One of the ways that clinicians sustained this pattern was by playing the role of an illness guide, anticipating events that may occur as treatment progressed and preparing family members ahead of time. Having an illness guide provided families with comfort, mitigating the uncertainty they lived with. Families also appreciated clinicians who remained available to them across different phases of the HSCT trajectory, through face-to-face and digital interaction. Finally, professionals’ efforts to engage family members on a human level (i.e., sharing social conversation for short periods of time, talking about their lives), as well as their efforts to really “hear” child and family perspectives, were highly valued.
Conflict and withdrawal
For one family, there was a dominant conflict–withdrawal pattern of interaction with clinicians (Tomm, 1980; Wright & Leahey, 2013). Alala’s (mother) account of HSCT was markedly different. She shared a highly chaotic and disjointed narrative during the first interview that moved back and forth between different treatment periods. It was visceral, painful to listen to, and difficult to follow. Even though it had been 3 years since her son’s HSCT, she had continued to reexperience being in the transplant room at night when she closed her eyes to sleep. As this family’s experience of difficult interactions with the health care team increased, Alala had noticed clinicians becoming less present in the transplant room.
This family’s pre-HSCT and prediagnosis illness trajectory strongly influenced this interactional pattern. For 3 years prior to diagnosis, Alala had tried to convince family members and multiple clinicians that her son was ill, but no one had listened. Tommy was diagnosed only when he was very ill. This family then experienced strained relationships with clinicians during the treatment period prior to HSCT. Further aggravating the situation was the emotional and instrumental exhaustion the family experienced from many months of hospitalization for chemotherapy treatment.
This mother had an assertive approach to advocating for her son and expressing her own suffering. The conflict seemed to have made it challenging for clinicians to hear the suffering lying underneath Alala’s anger. Certainly, the clinical team was sensitive to her distress. They made a psychiatry referral for her early in her son’s treatment. Unfortunately, she felt this pathologized her human response to illness, only further aggravating the relationship strain: I refused to take medications, the first thing the doctors wanted to do was medicate me . . . anti-depressants and anti-anxieties . . . psychiatrist . . . I just told them all to fuck off . . . I’m sorry! You need to calm a woman down, give her a pill . . . I hate to say that, it’s the truth though! . . . I talked to another mom . . . she said her husband had to be on drugs . . . she chose not to. She said, “I wanted to feel the pain that my son felt” . . . And I said, “that’s exactly” . . . I wanted to feel what he felt . . . I wanted to be there for him. I want to be present.
It is important to note that the findings related to the family members’ interactions with clinicians came from the perspectives of participating family members. Furthermore, although health care professionals were not central figures in the images created, they were part of some of the family dialogues associated with the created images.
Phase III: Family Reintegration
Between hospital and home
One day, without warning, families reported receiving an unexpected announcement that their child was going home. They felt they had been carefully managing one day after another, on ground that was familiar, and suddenly, they stepped forward into an uncertain place. What they had most wished for was suddenly possible—their child was coming home—but their child was still very ill. This tenuous point brought a heightened level of uncertainty and anxiety into family life; some parents felt they did not have the time that they needed to transition to carrying this increased responsibility. Concerns about preparing the home existed, despite families having previously received information about care/home cleaning requirements following discharge. What was most helpful to families at this time were assurances from clinicians that they would remain available for ongoing guidance, and the continued contact through follow-up.
Once families returned home, they were both hopeful and terrified. Initially, the home environment became an extension of the hospital; those from outside the family were asked not to visit, and the risk of a catastrophic outcome remained. However, the ground underneath the family slowly became more stable, and routines were reestablished. This process took time, occurring gradually over months. HSCT did not end after hospitalization but continued for months and years.
Feeling adrift
The reintegration of child and family into the life they had previously known was not possible. They entered a new life. Influencing the complexity of reintegration was family members’ differing needs and approaches to managing this process. Family members reentered life together but also felt alone and adrift as they carried individual, unvoiced experiences (see Figure 1). The lack of understanding about what other family members had endured and the inability to share those experiences left them emotionally isolated.
A need for family systems-expressive arts interventions
For parents who had cared for the child inside the transplant room, there was a need to give voice to their experience as a mother or father. Family members were clear that the emotional processing of their experiences had not been possible during hospitalization due to the intense caregiving demands they carried. They did, however, identify the value of talking about their treatment experiences and felt the drawing process used in this research was an effective way to express what they had experienced: Katrina (recipient): Every time we talk about it, it’s a little bit more therapeutic . . . just getting everything out, it feels like . . . something’s been lifted off our shoulders . . . there’s a lot of people out there . . . don’t want to hear about it . . . push it to the corner . . . Elma (mother): After [first interview] . . . we were talking about it . . . on the way home . . . It was . . . lots of tears . . . lots of memories come up . . . a lot of things you just . . . put away . . .
Symbolic and physical loss, individual/relational growth
Family members’ narratives included trauma and ongoing emotional strain, but they were also marked by growth: there was a new appreciation for life, relationships, and their family. Most families felt an intense gratitude for the new life made possible for their child and described a desire to “give back” or to take on an advocacy role. Yet, the uncertainty that remained following hospitalization simultaneously left families with difficult questions and worry: Drew (father): There’s no silver lining. (Samara, mother: yea, it’s not like) . . . It’s not like . . . we’ve been through this so now everything is that much greater and, you know, you count your blessings every day. It’s not like that. Samara: It’s not like that. Drew: You know . . . the scars and the worries outweigh everything it seems. Samara: Maybe someday it won’t feel that way but (Drew: someday, yea) . . . it’s not like, oh my God I’m so thankful . . . (Drew: yea) Yea. I mean we are obviously but . . .
Furthermore, ill children experienced life-altering physical changes, which included fertility loss, loss of hair, and increased dependence on the family due to the physical sequelae of treatment. One recipient almost died following discharge and faced multiple neurological complications. She had difficulty ambulating and was physically dependent on her family for many months.
Parents faced the symbolic death of the child they dreamed they would have. One mother drew a tombstone with the letters “RIP.” (see Figure 6). She then drew a flower beside the tombstone (“beauty and growth”). When asked about her image, Elma shared, “the tombstone is for . . . the grieving of your healthy child, the thought of what your child’s life should be . . . it’s going to be altered . . . a new version.” When asked what it was like to draw her image, Elma shared, “As soon as I started thinking about it [what to draw], it was ‘how do you put pain and hurt?’ It was really painful for me to watch her” (here, Elma is referring to the pain of hurt of watching her daughter go through HSCT).
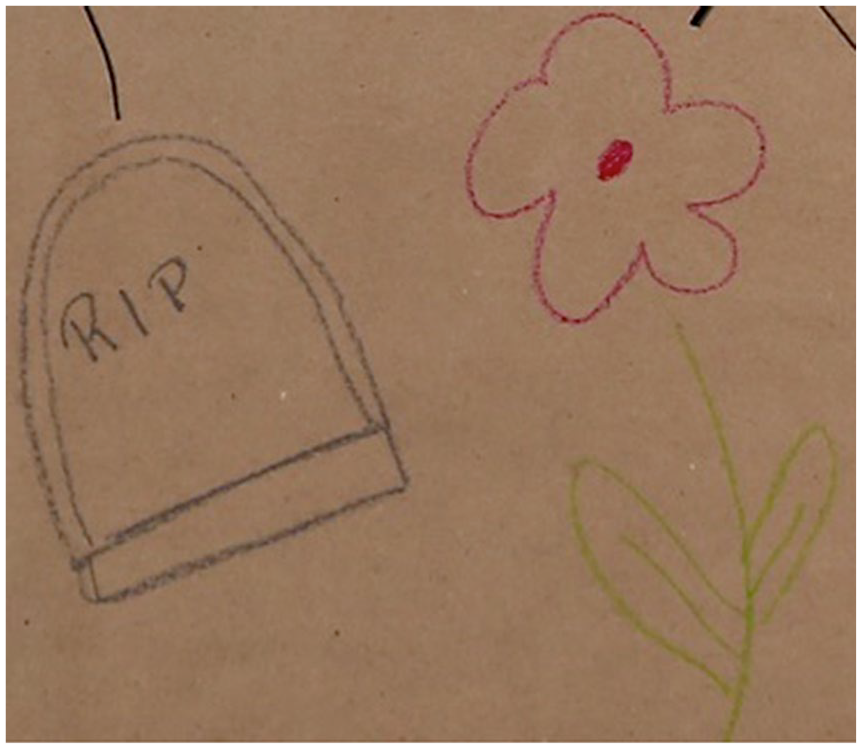
“Grief (Tombstone), Beauty and Growth (Flower)” (mother’s individual drawing from within a larger family image).
Sustaining Influences
For all participating families, there were critical sustaining influences that provided strength to family members across HSCT. These included family and extended community support, digital connection/social media, spirituality/faith, as well as key relationships with clinicians. Furthermore, family members found inspiration from the strength they witnessed in one another. For each family, different sustaining influences were influential. Therefore, it is critical for clinicians to be curious about each family’s resources, individualizing their care to a family’s unique strengths to mitigate the extraordinary challenges faced. Financial resources, as well as having only the ill child to focus on (no siblings) mitigated the degree of fragmentation experienced across hospitalization. The important role clinicians played as an illness guide through HSCT was also highly valued: As hard as Alice in Wonderland . . . is . . . our story . . . it’s got a good ending. It’s got a whole bunch of really, really, really weird stuff . . . between the beginning and the ending . . . coming out the other side however, whichever door you go through [see Figure. 2, black/brown doors behind family] . . . all you can do is . . . go through it . . . they really, really, really are in a world where they’re meant to be . . . Even in the story, as Alice went into Wonderland, she couldn’t have navigated it by herself . . . the people that are in that world know how to get through it . . . there’s a certain amount of trust that you’ve got to put in . . . the people that are working with you . . . they’ll navigate you through it (Jane, mother).
Discussion
HSCT is an intense treatment that occurs over a condensed time period, and there is no assurance that the ill child will survive (Packman et al., 2010). These research findings highlight the psychological distress experienced by different family members prior to, during, and following HSCT hospitalization. The pre-HSCT illness trajectories experienced by these families were powerful influences on their HSCT experience. It is important for clinicians to consider the specific pre-HSCT trajectory that each family has experienced as families prepare for HSCT hospitalization, individualizing their care to address any conflict, or previous losses that have occurred (Rolland, 1987, 1994).
Family members in this study concentrated all their emotional and practical resources on the survival of the ill child during hospitalization, which is consistent with previous family research (Kazak et al., 2020; Packman et al., 2010; White et al., 2017; Wilkins & Woodgate, 2007). The emotional distress expressed by family participants is congruent with previous reports that have included anxiety, depression, and post-traumatic stress symptoms for patients, parents, and siblings (Barrera et al., 2000, 2012; Chang et al., 2012; Packman et al., 2010; Wallace et al., 2014). Similarly, adult HSCT studies have reported decreased quality of life, emotional distress, and caregiver burden for patients and their partners/caregivers during inpatient (El-Jawahri et al., 2015; Poloméni et al., 2016) and outpatient HSCT treatment (Applebaum et al., 2016).
The emotional and physical fragmentation of family life that occurred for family members in this study brought impacts not only during hospitalization but also for months and years after HSCT. Previous pediatric HSCT research has reported a steady decline in psychological distress for parents following HSCT (Barrera et al., 2012; Phipps et al., 2004). However, our research findings were not consistent with those reports. These findings are more in line with adult HSCT populations, where patients and close relatives have reported ongoing psychological distress, challenges in returning to “normal life,” and hesitancy to discuss these ongoing difficulties with members of the HSCT team (Poloméni et al., 2016).
From the family’s perspective, clinicians did not always seem to fully explore the suffering of family members beyond the ill child; the distress experienced by family members not present in the transplant room was at least partially obscured from view (see Figure 1). The central position of the medical treatment within the transplant room also seemed to be at play in family members not fully seeing or understanding the experiences of other members of their family. Similar to a camera that focuses intensely on one image, blurring other images from view, efficiency and disease-focused discourses in health care (Basu et al., 2017; Maxwell, 2009) may be partially obscuring the experiences of family members who exist outside of the transplant room. Furthermore, clinicians focused primarily on the treatment and daily physical care of the ill child with the “parent caregivers” living in the transplant room. The suffering they experienced as parents was not always as much of an explicit focus as it could have been. However, the moments of care in which clinicians connected with family members on a human level were particularly meaningful for participants and evident across the research data.
Preliminary work on the integration of early palliative care consultation in the context of HSCT treatment in both pediatric and adult populations has highlighted the value of providing intensified supportive care during the transplant process (Lafond et al., 2015; Loggers et al., 2016). In a pilot study with families who had a child receiving an HSCT, one of the most requested interventions provided by the palliative care consultation service was supportive counseling during the hospitalization period (Lafond et al., 2015).
Our research findings highlight the need to focus psychosocial care on the entire family during HSCT and the need to address challenging family–clinician interactions when those emerge. The “family level dialoguing with images” process (McNiff, 1991, 2004) used as a method in this study holds promising potential for development into a family systems-expressive arts intervention that assists clinicians to facilitate important conversations between family members. The need for family-level intervention prior to, throughout, and following discharge, which was evident in our findings, resonates with Kazak et al.’s (2020) recent research on caregiver perspectives about psychosocial intervention in pediatric HSCT.
Furthermore, during hospitalization, there is a pressing need to more fully integrate the experiences of family members who live outside of the hospital into the day-to-day HSCT experiences of parents and children who live in the transplant room. Currently, there are some innovative approaches using online formats for psychosocial intervention with parents and adolescent/young adult childhood cancer survivors in Australia (Sansom-Daly et al., 2012, 2019; Wakefield et al., 2015, 2016). Internet-based psychosocial intervention may hold new possibilities for working with family members living in different locations during HSCT hospitalization in the future.
Limitations and Future Research
Key limitations of this work include a small sample that included various pediatric diagnoses. Although the data were limited to qualitative interviews, this is the first study to integrate a “family level dialoguing with images” process into interviews. Despite the importance of pursuing family interviews, it is possible that participating children and/or parents may not have shared all aspects of their experience, given they spoke to the researchers in the presence of each other.
In addition, given the small sample, we cannot claim to have reached theoretical saturation in the theory developed from these data. The work was limited by the availability of children/families who had received an HSCT in the previous 5 years in one treatment center, and we excluded families whose child had died during or following HSCT treatment. The death of a child is a critically important aspect of the child/family experiences that needs consideration in future work. The continued evaluation of the inductive theory and theoretical categories reported from this study is part of our current work, where the theory will be further modified. Weiner (2007) argued that saturation is about judgment, and practical considerations need to be involved in decisions about when to complete a study. What is seen as problematic are saturation claims in the absence of considered judgment (Thorne & Darbyshire, 2005). The marked depth and quality of the data provided by the child and family participants within this study were part of the carefully weighted judgment about the theoretical sufficiency (Dey, 1999) of the findings reported here.
Future research studies should aim for a larger sample of families with the inclusion of distinct diagnostic groups. This study led to subsequent funding for a multisite constructivist grounded theory study about child and family experiences of pediatric HSCT, which is currently underway at two research sites in Canada. Children and families are being followed prior to, throughout, and to 1-year post-HSCT. We have integrated into this subsequent research the “family level dialoguing with images” process, additional expressive arts activities, digital storytelling (Lambert, 2006), and participant observation (Carnevale et al., 2008).
Conclusion
The transition into HSCT hospitalization and the period following HSCT is an important time to explore the unique experiences of each family member within the context of family-level psychosocial intervention. During hospitalization, family members also have intense emotional support needs, which require tailored psychosocial intervention approaches. Not all family members will be open to targeted psychosocial support, and their choices need to be carefully respected in the context of psychosocial intervention. Despite this, the integration of family systems-expressive arts approaches to intervention holds significant therapeutic potential for lessening the distress of family members across the HSCT treatment trajectory.
Supplemental Material
Supplementary_File_1_Interview_Guide – Supplemental material for Falling Down the Rabbit Hole: Child and Family Experiences of Pediatric Hematopoietic Stem Cell Transplant
Supplemental material, Supplementary_File_1_Interview_Guide for Falling Down the Rabbit Hole: Child and Family Experiences of Pediatric Hematopoietic Stem Cell Transplant by Christina H. West, Debra L. Dusome, Joanne Winsor and Lillian B. Rallison in Qualitative Health Research
Footnotes
Acknowledgements
We would like to acknowledge and thank the children and families who generously shared their time and experiences with us. We would also like to thank the Children’s Hospital Research Institute of Manitoba for funding this research.
Authors’ Note
Portions of this article were previously presented at the Qualitative Health Research conference in Kelowna, Canada, in October 2016, the 13th International Family Nursing conference in Pamplona, Spain, in June 2017, the 49th Congress of the International Society of Pediatric Oncology conference in Washington, United States, in October 2017, and the Canadian Association of Psychosocial Oncology conference in Toronto, Ontario, in May 2018.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received support through a research operating grant from the Children’s Hospital Research Institute of Manitoba. Children’s Hospital Research Institute of Manitoba Operating Grant (June 2014–2017).
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.