
Abstract
In this article, I introduce the concept of the space-in-between. This space-in-between is born of the realization that, between the expression of any two polarities (across dimensions such as emotion, thought, geography, and ideology), there exists a philosophical construct useful for framing thinking about practice, research, and managerial relationships in the health professions. Out of this construct emerge practical considerations useful for structuring the conduct of meaningful interpersonal and intercultural interactions. I describe how the idea of a space-in-between developed out of my medical practice, grew as a result of my experiences in international environments. and has found fulfillment in my ongoing work. I explore the application of a space-in-between in public health, medical anthropology, medical ethics, and global health. I review how, as a result of incorporating this space in their daily work, clinicians, educators, researchers, and managers can grow as leaders by sharing the presence that arises from the space-in-between them and the people in the communities they serve.
Keywords
I lift both my hands up, from my lap to chest height, turn them palms up, and say, “This is why we have two hands. In one we hold hope.” I look at one palm, and then turn my gaze to the other. “In the other, reality.” My hands, momentary measures of meaningfulness, move ever so slightly, one up, one down, each in opposition to and in rhythm with the other. I continue. “We all have the power to find that place, that strength to live and be alive through it all, in-between the two.”
Thus, as is my wont in my work as a family physician, I talk with my adult patients when discussing a new condition. Sometimes I have done the diagnosing. Sometimes others have done it, and I am but an interpreter of a consultant’s words. In each situation, my intent is the same: to help people see beyond the despair of knowing they now live with an acute or chronic illness, yet not so far as to get stuck in the delusion of denial or magical cure. My intent is to open to my patients the power of the space-in-between. For in-between two polarities, there exists the possibility of finding deep meaning to it all: to the efforts made toward full resolution of disease, to the act of acceptance when resolution is not possible, and to the getting on with life in all its dimensions, including and in spite of the illness experience.
The idea of balancing reality and hope is useful for presenting and conceptualizing the management of medical problems, as is the concept of a space-in-between two polarities a practical way to see many co-occurring, often paradoxical truths: that although one has a disease, one is not defined by the illness; that although one is not alone in planning or implementing treatment, neither can one abdicate responsibility for working to realize a constructive outcome; and that although one may feel immense frustration and sadness upon realizing that life as it was previously experienced has changed, one may also find contentment in knowing that it continues anew, with both challenges and successes inevitably ahead—even, inexorably, as the approach of death nears.
As I have grown in my work over the years, my understanding of this space-in-between has grown as well. While I continue to use the concept in my medical practice, I also now see it as one framework for structuring and applying my thinking in public health, medical anthropology, medical ethics, and global health. I hope readers of this article might see how the power of the space-in-between can resonate in situations applicable to their work as health care professionals. My words here are meant to foster that recognition and promote the use of the space-in-between in clinical and public health practice, research, education, and administration.
Conceptualizing the Space-in-Between
The one-on-one interactions I have had with patients gave birth to this concept of the space-in-between (Ventres, 2012a). Visualizing it as something more expansive, a guide to understanding and managing the complexities inherent in the milieu of health care, has meant reflecting on three key factors: polarities, socialization, and boundaries.
Looking Between Polarities
In between reality and hope, in between North and South, rich and poor, new and old, or any other pair of polarities that exist, there is a space. This space is principally one of emotion and thought, yet may as well contain elements of geography, ideology, interpersonal relationships, and other dimensions (Figure 1). In between these polarities is a fluid core comprised of common characteristics all humans share, including hopes, fears, sadness, joy, vulnerabilities, and resiliencies. It is a place people can figuratively enter into to examine and appreciate differences, at once exploring commonalities, honoring boundaries, and expanding understandings. Into this place, people bring cultural and individual perspectives, personal and social histories, and the rich mixture of qualities—a blended combination of both facts and fictions that are, arguably, hard to differentiate at times—that inform human awareness and behavior. Out of this place can emerge thoughtful reflection, a resonant harmony resultant from shared presence (Ventres & Frankel, 2015), and both emotional and intellectual growth. This place is the space-in-between.
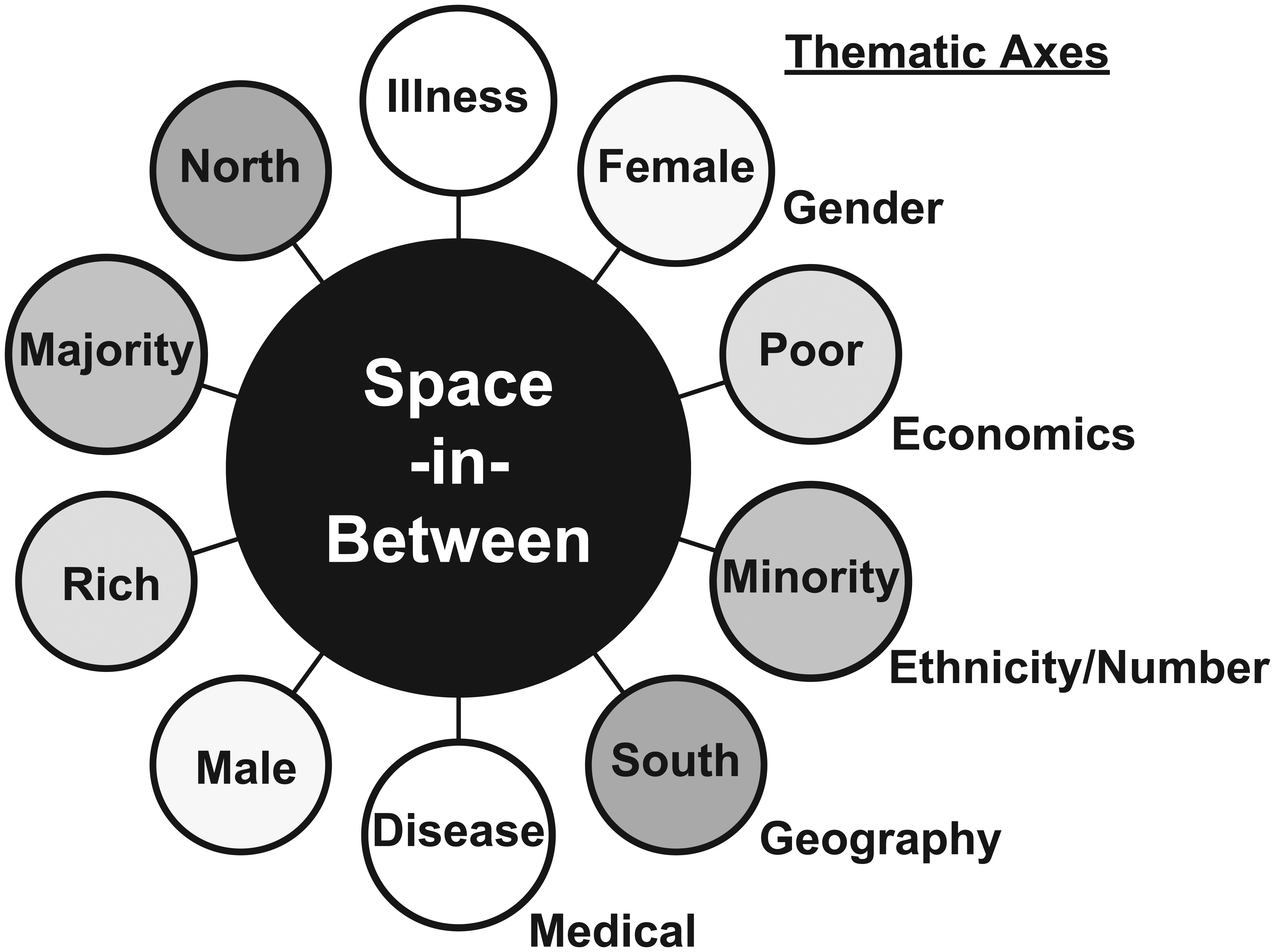
Example polarities and the space-in-between.
Growing My Understanding
Whether by intent or simply as an unintended consequence, my medical education succeeded in emotionally distancing me from those I was being taught to serve. Because of the lack of attention I learned to give to the social and psychological contexts of patients’ lives, I initially felt alienated from my patients as people. In response, I began to seek ways to repair the damage caused by this estrangement and find professional paths to connect in ways simultaneously enriching (for me) and therapeutic (for those in my care). My training in family medicine, cultural medical anthropology, and family therapy were direct results of that quest.
It still took me several years of community practice before I was able to find the right mix of relational connection and scientific competence, basic but not terminal goals of lifelong medical education (Ventres, 2014). My early alienation thus ameliorated, over the next two decades of daily practice, I used evidence-based techniques (drawn, for example, from motivational interviewing, narrative medicine, and patient and relationship-centered care) as well as a person-centered approach to help create and nurture that space-in-between my patients and me—a place where positive healing outcomes could take form (Ventres & Frankel, 2015).
Stepping Outside Traditional Boundaries
More recently, since 2010, I have lived and worked in El Salvador (Ventres, 2013), teaching and reflecting on issues of global public health, anthropology, and medical ethics. This Central American experience has opened my eyes to points of view (and new spaces-in-between) of which I was previously unaware, including,
how aggression and submissiveness create cultures in which fear and anxiety are pathologically normalized as day-to-day violence across various dimensions of power and wealth (Ventres & Fort, 2014);
how issues of core and periphery play out in everyday encounters between people of diverse social strata—in commerce, governance, scholarly life, and clinical encounters—made individually manifest as willful ignorance and abject despair, and amplified by ample doses of low self-esteem (Ventres & Gusoff, 2014);
how such simple words such as “here” and “there” make it challenging to develop an honest and accurate appreciation of people’s daily lives, especially when assessing their conceptions of what well-being means. (Here one notices that roughly a third of all Salvadoran citizens live, with or without official documentation, there—north of the Rio Grande river (Rubio, 2013). Here, one sees rural villages empty of men, all of whom have gone there—to the United States—for work. Here, one comes to understand just how U.S. policies, abetted by military and economic intervention, have established and maintained conditions that foster such a diaspora [Moodie, 2010]. Few see life here absent consideration of life there.)
It is difficult to make sense of it all. Within the realms of academic, political, and religious life, as expressed via the various media outlets (each partial to those from whom they receive support), people in El Salvador regularly stake out and defend positions in opposition to others. This opposition is commonly based more on the emotional weight of cultural history and personalized by perceived past injustices, than on any current rational vested interest. One cannot ascertain any semblance of truth without attempting to examine prevailing polarities and explore the space-in-between (Enosh & Ben-Ari, 2015).
Cultivating the Space-in-Between
This concept of a space-in-between is neither an artificial creation born of some magical illusion nor simply a phenomenological artifact that exists for the sake of philosophical discussion or research validation (Clifton-Soderstrom, 2003; Lopez & Willis, 2004; Norlyk & Harder, 2010). It is, rather, a practical construct, the use of which requires a thoughtful approach, a practiced plan of implementation, and a communicative repertoire encouraging of responsive engagement.
Approaching the Space-in-Between
Approaching the space-in-between, to use it as a guideline for embarking on any clinical, research, educational, or administrative endeavor, means integrating into consciousness five developmental steps, each with elements of observation, thought, and action (Ventres & Haq, 2014). These five steps include the following:
Recognize—Acknowledge the presence of other people as persons (and not just patients or informants, and learn especially from those who appear to look, think, and act in uncommon ways.
Engage—Create opportunities for dialogue with those with whom one comes in contact, employing an attitude of appreciation and positive regard, rather than focusing on deficits.
Reflect—Explore one’s cognitive and emotional responses to such dialogues. Consider the roles personal and professional development play in the expression of those responses. Accept that others will uniquely perceive their own cognitive and emotional responses. Make room for hearing their reflections.
Act—Conduct oneself in ways that increase the likelihood of growing a space-in-between with all those in one’s presence. Words, gestures, silence, and humor, among many other behaviors, can help set the stage for active communication. Remember that it is not always what one does, but what one does next that can further interpersonal growth: Accept making mistakes and taking corrective actions as part of the process.
Review—Examine, independently and in community with others, experiences that sustain, challenge, and help promote the growth of a mature space-in-between over time.
Although I present it as a list of steps, in reality, this approach is dynamic, asynchronous, and integrated in real time as a relational give-and-take, at once responsive to internal thoughts and feelings; sensitive to the nuances of others’ words, gestures, and intonations; and aware of the surrounding physical and cultural environment. Each step forms one part of a larger whole by which all can come to know the space-in-between through interpersonal and intercultural interactions.
Developing Habits of Practice
Several habits of practice can help health care professionals, whether working for therapeutic, investigational, or managerial purposes, gracefully integrate the above steps into their occupational interactions. These routinized patterns allow interpersonal conversations to emerge as natural rather than artificial extensions of the intent to explore the space-in-between. Such habits of deliberation and action include the following:
Developing a non-anxious presence. Carl Rogers’s (1961) suggestion for psychologists is equally applicable for health care professionals of whatever discipline.
Growing an openly inquisitive stance (Ventres, 2015b). Actively work to detect and uncover polarities, especially differences that may be deeply hidden under guises of etiquette, custom, or any other manifestation of power and inequity.
Recognizing our common humanity. Be aware that none of us are so far apart at heart, even those whose opinions radically diverge from one another (Hoffer, 2002). The ongoing rapid changes in information transfer, human migration, and the cross-national globalization of economies mean that we live in an increasingly inter-created and inter-dependent world.
Considering how people construct their beliefs. Expressions such as, “Tell me more” and “I don’t understand” invite others to examine underlying attitudes. Know that people’s self-identities have various facets and may take varied forms as they are expressed in conversation (Ventres, 2015a).
Engaging relational connections. Seek humanizing ties by sharing one’s own life stories, be they successes or failures, as appropriate.
Entering the Space-in-Between
The concept of space-in-between is about authentic engagement. It occurs when people come together and share. That these people come from different backgrounds, have different perspectives, and pursue different goals in life should be expected (Barry, 2002); it is a given. The space-in-between is a creative construction in which those differences are not ignored, but honored at the same time they are explored for meaning. This exploration is characterized more by open inquisitiveness than firm responses, more by honest unknowingness than arrogant know-it-all-ness, and more by a genuine willingness to understand than a need to be “right,” especially in relation to how others see things.
There may be times the creation of a space-in-between seems implausible if not impossible, whatever potential for building it made toxic by people’s dogmatic inflexibility, polluted by intended and unintended defensive postures, or drained by profound lack of interest. Yet part of envisioning a space-in-between is accepting that whatever histories people bring, and however they present them, there is hope. This hope stems from the belief that by bringing the value of integrity, the force of dignity, and the gift of generosity to interactions with others—through a process built on pillars of respectful listening, considerate sharing, and open invitation—meaning, understanding, and a sense of opportunity can arise out of and flourish as a result of the space-in-between. The accompanying personal narrative testifies to this possibility (see Box 1).
Personal Narrative.
Obviously, some people cannot or refuse to enter this space-in-between. They may need encouragement, including display of the benefits their engagement may bring. They may need a push, including demonstration of overt evidence that current realities demand their participation. Ultimately, they may need confrontation of some sort: Active resistance may be an option when all else fails.
Further Reflections
Some may find this idea threatening. Many within the health professions see their practice as one solely of diagnosis and treatment; anything that might suggest compromising the “pureness” of these goals has no place within its domain. Obviously, as a family physician whose work knowingly bridges boundaries between biology, psychology, and anthropology, I cannot disagree more (Ventres, 2012b). I invite those who fervently disagree with me to reflect on their histories, predispositions, and biases as a starting point before proceeding to the other steps of finding a space-in-between between their thinking and mine.
Others will submit that ruminating about such space is a fool’s errand. Power, profit, and prestige—and those who hold them—are the real determinants driving how the world and its inhabitants function. There may be some truth to this; few historical examples suggest those looking down from pinnacles of conventional societal or economic success are inclined to show genuine interest in those who live on society’s margins. As well, staunch ideological defenders of extreme political and cultural beliefs often seem unwilling to consider the existence of alternative views.
“Studying up” may offer answers as to how to broach these concerns (Nader, 1974). Community-Based Participatory Research may present alternative solutions (Belone et al., 2015; Israel et al., 2008; Montoya & Kent, 2011). Others may arise out of efforts to analyze how education, socialization, and outright manipulation are persuasive forces in personal and professional identity formation (Leo & Eagen, 2008). As well, cataclysmic changes have previously prompted consideration of how to find common ground; it may well be time to revisit their effects anew (Klein, 2014).
Conclusion
By recognizing this space-in-between, health care professionals—whether working as clinicians, investigators, educators, or managers—can build a framework for imagining and realizing personal and communal power. This power comes from recognizing and genuinely honoring differences. It comes from authentically appreciating commonalities. It comes from sharing vulnerabilities and resiliencies. This power comes from the space-in-between. May it offer new perspectives with which to find answers to the many challenges of the complex world in which we live, and may it guide our paths toward therapeutic healing, honest contentment in work well done, and a deep sense of life’s meaning in relationship with others.
Footnotes
Acknowledgements
The author thanks Meredith Fort, PhD, and Cindy Haq, MD, for their constructive comments on previous drafts of this manuscript.
Authors’ Note
The author presented this work at the 4th GQHR Conference, Meriden, Mexico, March 18-20th, 2015, and at the University of El Salvador’s Research Seminar in Sociocultural Anthropology, on May 26, 2015, in San Salvador, El Salvador.
Declaration of Conflicting Interests
The author (s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author (s) received no financial support for the research, authorship, and/or publication of this article.