
Abstract
In this article we explore the process leading to help seeking following childhood trauma among women who were currently in treatment. We interviewed 13 participants from six treatment groups for clients exposed to human-inflicted traumas. Transcripts were analyzed using a hermeneutical-phenomenological approach. Help seeking was initiated after a prolonged period of time (13 to 58 years after first trauma exposure), during which participants relied heavily on a strategy of managing on their own. Self-management contributed to delays in help seeking, but was also an important resource. High levels of distress were reported prior to help seeking, often without help seeking being considered as an option. The participants sought help when encountering situational demands exceeding available resources, resulting in experiences of exhaustion and loss of control. We present a model of the help-seeking process, underlining the importance of respecting and exploring the individual process of seeking help when offering trauma-specific treatment.
Keywords
Researchers focusing on the life trajectories of women who thrive following childhood trauma have reported that religion, therapy, personal efforts, and relationships with significant others were important elements in their “redemption narratives,” wherein a negative situation translates into a positive outcome (Thomas & Hall, 2008). Even though being in therapy potentially contributes to thriving following childhood trauma, little is known about the process leading individuals to seek therapy following such exposure. Understanding this process can help to promote health and thriving following childhood trauma.
Although exposure to childhood trauma is consistently related to an elevated risk of developing long-lasting health problems such as depression, anxiety, and trauma-specific symptoms (Briere & Elliott, 2003; Foote, Smolin, Kaplan, Legatt, & Lipschitz, 2006), the question of recommending therapy following childhood trauma is complex. Whereas some survivors of childhood trauma benefit from therapy, others do not (Thomas & Hall, 2008). The efforts to reach those in need of treatment as early as possible, as part of health-promotion activities (Jané-Llopis & Anderson, 2006), have to be balanced with the recognition that many individuals thrive following trauma without therapy. This raises the question of what promotes help seeking among survivors of trauma who are in need of treatment.
Generating knowledge about this issue is particularly important because people with posttraumatic stress disorder (PTSD) seem to be overrepresented in non-help-seeking or delayed help-seeking populations (Fikretoglu, Liu, Pedlar, & Brunet, 2010; Wang et al., 2005). Exploring the observed delay in treatment seeking following trauma, researchers have often focused on a core symptom in PTSD: avoiding trauma-related stimuli (Sayer et al., 2009). In addition, many researchers have focused on the belief that one can handle things on one’s own as a specific barrier to help seeking, both in quantitative (Kessler et al., 2001; Wang, 2006) and qualitative studies (Sayer et al., 2009). Previous studies on help-seeking behavior, both in general and regarding trauma survivors, were, to a large degree, quantitative (Kessler et al., 1999; Koenen, Goodwin, Struening, Hellman, & Guardino, 2003; Mojtabai, Olfson, & Mechanic, 2002), and the subjects were often war veterans (Campbell & Raja, 2005; Fikretoglu, Brunet, Schmitz, Guay, & Pedlar, 2006; Hoge et al., 2004; Sayer, Clothier, Spoont, & Nelson, 2007).
The existing research provides some knowledge regarding trauma victims’ use of available services and service contact patterns (Henning & Klesges, 2002; Lipsky, Caetano, Field, & Larkin, 2006; Macy, Nurius, Kernic, & Holt, 2005); the average delay in seeking help (Fikretoglu et al., 2010; Wang et al., 2005); and barriers to seeking help (Kessler et al., 2001; Sayer et al., 2009; Wang, 2006). Researchers have devoted less attention to help-seeking behavior among survivors of interpersonal trauma—such as domestic violence, rape, and assault—and in particular, help seeking following childhood trauma (Johnson & Zlotnick, 2007; Macy et al., 2005). There is still a need to gain a more in-depth understanding of why people seek help at particular times and the key experiences that prompt them to seek help following trauma. This is unfortunate, because a better understanding of these processes might inform and direct efforts toward health promotion (Burgess-Proctor, 2011). Clients’ perspectives have also proven valuable in psychotherapy research (Elliott & James, 1989; Hodgetts & Wright, 2007). Therefore, it is important to understand the first-person perspective of the processes leading to help seeking following childhood trauma. In this study we explored this issue by interviewing women survivors of childhood trauma who were currently undergoing trauma-specific treatment about the experiences that led to their initial help-seeking behavior.
Methods
Study Setting
The study took place in an outpatient setting of specialized mental health services in a remote area of northern Norway. The Norwegian mental health care system relies on decentralized, specialized health centers to provide both outpatient and inpatient treatment. The aim is to provide treatment in the local community rather than relying on centralized, specialized hospital settings. Given the low population density and long geographic distances, clients in remote areas of Norway nevertheless might have to travel up to 2 hours each way to receive outpatient treatment.
All research participants in the study had attended stabilization groups tailored to include clients who had been exposed to a wide range of human-inflicted traumas and exhibited a wide range of trauma-related symptoms. By “human-inflicted traumas” we mean traumatic exposure wherein another person inflicts harm; for example, childhood abuse or neglect, partner violence, rape, assault, robbery, and so forth. The stabilization group approach was developed by the first author, and has been described in detail elsewhere (Stige, 2011). Briefly, the approach consists of 17 weekly group sessions focusing on understanding and managing trauma-specific symptoms. Building on Herman’s (1992) work, it emphasizes safety, the restoration of control, empowerment, skill building, and the establishment of new relationships. The approach is currently offered in gender-specific groups. At the time of the study, six treatment groups for women and one for men had been completed.
Clients who were considered eligible for the treatment groups had experienced human-inflicted traumas in childhood, adulthood, or both. All clients had been referred to the specialized health services by their general practitioner (GP). At the start of treatment in the stabilization group, they reported active trauma-related symptoms defined as symptoms of PTSD (World Health Organization [WHO], 1993), complex PTSD (Herman, 1992), and/or symptoms or disorders of dissociation (WHO). Trauma-related symptoms were assessed by clinical interviews and self-report measures. All clients received concurrent individual treatment. Under the Norwegian health care system, all costs for medical care (somatic and psychiatric) exceeding 1,840 NOK a year (approximately US$320) are covered by the government. Hence, the economic and work-related barriers to seeking help are minimized.
Design and Methodological Approach
A hermeneutical-phenomenological approach was chosen for this study because we were interested in exploring the lived experience of individuals’ process leading to help seeking, while acknowledging the inevitable influence of interpretation in all human activity (Alvesson & Sköldberg, 2000; Angen, 2000; Laverty, 2003). In line with this approach, we believe that we, as researchers, interpret and understand the emerging data and phenomenon of interest from a particular context-dependent perspective. The meanings we derive from hermeneutical-phenomenological studies represent a “fusion” of our own and the participants’ experiential “horizons.” A dialogical view of reflexivity was, therefore, central to the research process. The encounters with the participants’ experiential horizons during interviews and analysis were used actively to discover and reflect on our own preunderstandings and how these influenced the emerging research process (Alvesson & Sköldberg; Lopez & Willis, 2004; Smith, 2007; Stige, Malterud, & Midtgarden, 2009).
Because we were seeking rich narratives from each participant, we chose semistructured in-depth interviews. The main topics in the interview guide were the process leading to help seeking, the experience of change, and the experience of treatment participation. The significance of exploring the process leading to help seeking in more detail became clear to us during the first interview. Consequently, a procedure was developed that required participants to draw a timeline to illustrate their experienced fluctuations in distress over time, the time of their traumatic exposure, and when they initially sought help, and this procedure was included in the interview guide. The participants’ drawings allowed us to explore the first-person perspective of the process leading to help seeking more freely, and to stay closer to the participants’ experiences and words choices without introducing clinical terms such as trauma, flashbacks, and so forth, thus introducing the interviewer’s preunderstanding at an early point in the interview.
During the interviews, participants were asked open-ended questions about help seeking in general, including the following questions: When did you first seek help? What made you seek help at that particular time? What changed during that period that led you to seek help? How did you cope with your problems prior to seeking help? Follow-up questions were used throughout the interviews to allow participants to clarify and elaborate on what they had shared. This also gave the interviewers an opportunity to ensure they fully understood the participants’ responses and validate their interpretations (Kvale, 1996).
The study received ethical approval from the Regional Committee for Medical and Health Research Ethics, North Region (REK North) and from the Norwegian Social Sciences Agency. Because the research participants were clients in the specialized mental health care system at the time of the interviews, REK North required no explicit focus on the type of traumatic exposure or the participants’ experiences of this exposure during interviews. Information about trauma exposure was thus obtained from scores on the Traumatic Experience Checklist (TEC; Nijenhuis, van der Hart, & Kruger, 2002), which participants had completed as part of their treatment. Therefore, it was not possible within the context of this study to explore how different types of trauma exposure influenced individuals’ decisions to seek help.
Recruitment and Participants
At the conclusion of the stabilization group treatment, all 31 clients from the six treatment groups for women received a written invitation to participate in the research project. To ensure that no one felt pressured to participate, no information about the research project was provided until group treatment had been completed. Information was provided in a letter sent by mail, and those who wanted to participate returned their contact information by mail as well. We then contacted interested women to arrange a time and a place (i.e., the participant’s home or the clinic) for the interview. All clients who volunteered to participate were enrolled in the study. Written consent was obtained at the time of the interviews.
On the conclusion of the fifth treatment group we had recruited 10 participants, and we were observing converging patterns of meaning in our preliminary data analysis. We then chose to recruit participants from the sixth treatment group to ensure that we did not exclude important and new perspectives from our analysis. The final sample comprised 13 clients from six treatment groups. The interviews were conducted from August 2008 to March 2011. The resulting data was considered rich and suitable for a meaningful hermeneutical-phenomenological analysis.
The research participants were between 18 and 60 years of age (mean: 39 years), and all reported being younger than 5 years of age at the time of their first traumatic experience. All participants had experienced multiple traumas, including incest, sexual abuse, physical abuse, rape, partner abuse, and/or psychological abuse. At the time of the interviews, 4 participants were studying or working and 9 were either on sick leave, on disability benefits, or receiving rehabilitation money. Ten participants had children. We have de-identified the participants’ personal information in the presentation of the findings.
Data Collection Procedures
The first author is a clinical psychologist with a special interest in the field of psychological trauma, and was one of two group therapists in five of the six stabilization groups. To prevent participants from being interviewed by their former therapist, a team of three conducted the interviews. This was important in ensuring free consent and avoiding power differences between therapists and clients that might have influenced the interview situation and emerging data. Two trained mental health care workers who were associated with neither the treatment nor the study conducted interviews with participants from the five groups in which the first author had been a therapist, and the first author conducted interviews with participants from the sixth group.
Participants were interviewed within 3 months of completing the stabilization groups, and all interviews took place in the clinic, at the participants’ request. The interviews were exploratory in nature, and lasted 1 to 2 hours each. They were audio-recorded and transcribed verbatim by the first author. A total of 17 interviews were conducted with the 13 participants. One follow-up interview was conducted to clarify certain information from the original interview, and three other participants were interviewed twice at their own request because they did not have time to complete the interview the first time.
The first author listened to each interview shortly after it had been conducted and provided feedback to the two mental health workers (external interviewers) to ensure that the interviewers were up to date on any adjustments to and developments in the research focus. Feedback was related to the interview style (e.g., the first author asking an interviewer to probe in more detail for descriptions of concrete situations or experiences) and adjustments to the research focus (e.g., extended focus on the process leading to help seeking following the first interview, and beginning to have participants draw a timeline to better understand this process). This arrangement also permitted follow-up interviews with participants to clarify information gathered in interviews not conducted by the first author.
Data Management and Analysis
NVivo 8 software (QSR International, 2008) was used as technical support for the analysis of the interview transcripts. Stories, examples, and information regarding experiences related to help seeking appeared throughout the interviews because they were semistructured and followed the participants’ subjective presentation of their own experiences. Part of the analytic process, therefore, was to structure the dataset from a chronological perspective, so we could obtain an impression of the experiences that led the participants to seek help.
Despite the constant alternation between parts of the data (extracts from individual interviews) and the whole (patterns of meaning across interviews), the general sequence of the analysis can be described as follows. We initiated the analysis by reading through the transcripts several times to obtain a clear overview of the material. We studied each interview in detail and identified all text relevant for help seeking. We labeled segments of text expressing different elements of the help-seeking process as meaning units, staying as close to the informants’ use of language as possible. We condensed meaning units across interviews and then abstracted them to form themes and subthemes. We viewed themes and subthemes in the different interviews all together, looking for patterns of meaning that incorporated both converging and diverging meaning units. The emerging analysis was presented to the external interviewers in a series of meetings. Their responses on how the preliminary analysis resonated with their first impressions of the data from the interview settings served as the starting point for discussions and reflections on ways to organize the data. The first author used this information to deepen and focus the analysis.
One of the main challenges in this study was protecting the identity of the participants, given the rural setting, the specific treatment approach, and the multiple roles of the first author. Therefore, quotes are presented with less contextualization and participant-specific information than is ideal, to balance the desire to properly situate the study and the researchers against the need to stay true to the participant’s descriptions in the presentation of the findings without compromising their anonymity.
Findings
All participants identified the first time they sought help as when they took the initiative to obtain health care assistance. The period of time that elapsed from when the women sought health care assistance to when they received trauma-specific treatment varied greatly (because of space restrictions we cannot explore the participants’ journeys within the health care system in this article). Our analysis also revealed that there was a clear distinction between self-initiated and other-initiated first contact with the health care system. Therefore, these two paths are presented separately.
Among those participants who initiated help seeking themselves, a long-running process (13 to 58 years) led to their decision to seek help. As time passed, each experienced new traumas, and all but one participant had experienced rather high levels of distress at an earlier time without seeking help. Despite high levels of distress and new traumatic experiences, the women reported ways of coping with their life situations that allowed them to feel as though they were on top of things. Only when new situational demands exceeded their available resources, leading them to experience a loss of control, was help seeking initiated—often because of a perceived negative influence on significant others. In Figure 1 we present an overview of the process leading to help seeking, as conceptualized by our analysis. The boxes below the timeline represent the main themes and subthemes of our analysis. The graph above the time-line illustrates the women’s reported fluctuations in distress over time and is based on their own drawings.
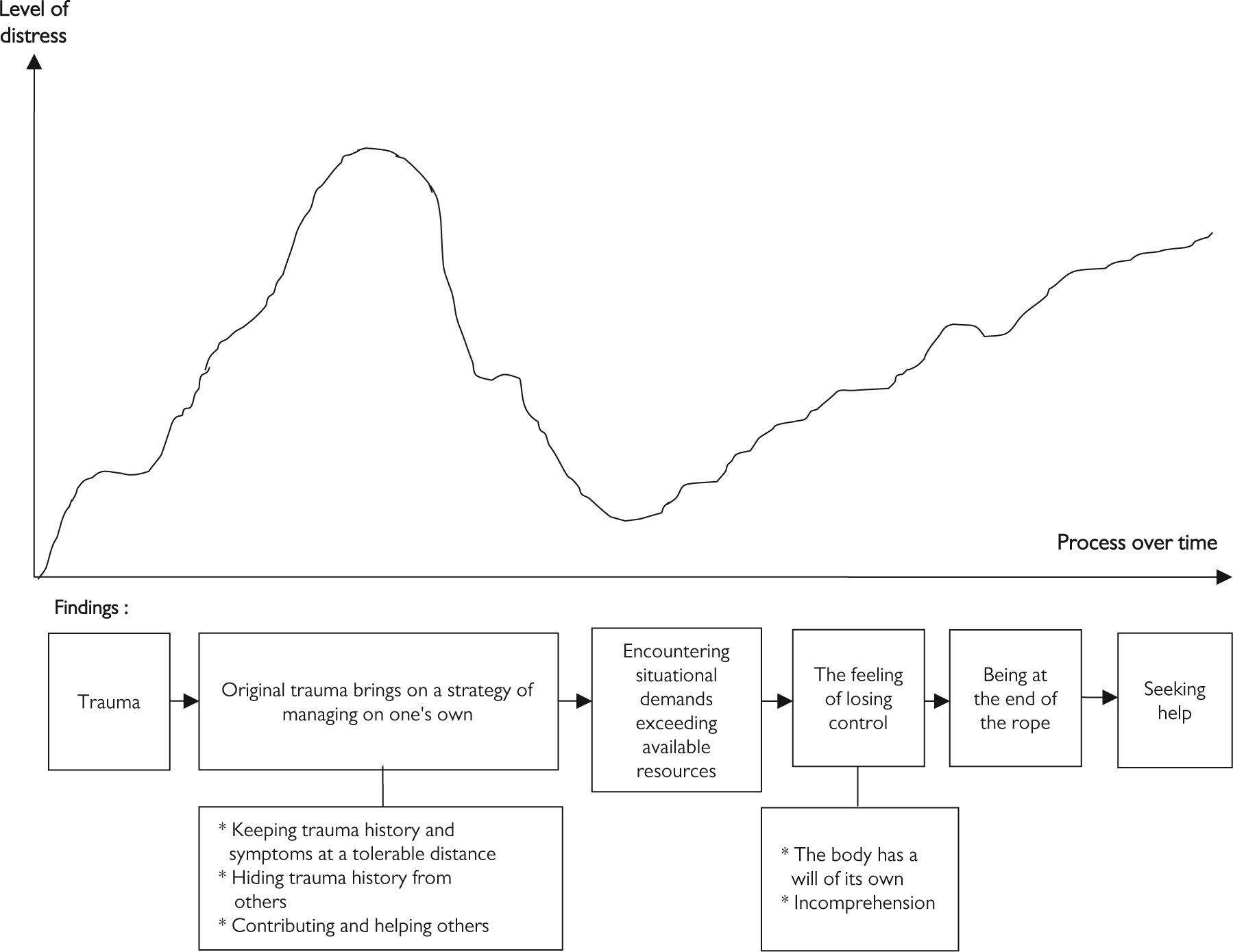
A model representing the help-seeking process.
Original Trauma Brings On a Strategy of Managing on One’s Own
In telling their stories of how they experienced and managed their lives following traumatic experiences, and prior to seeking help, the participants consistently shared experiences, coping methods, and values that were consistent with a strategy of managing on their own. The different components of this self-management strategy include the following subthemes: keeping trauma history and symptoms at a tolerable distance, hiding the trauma history from others, and contributing and helping others. These components all had the function of promoting self-management by minimizing the women’s risk of being overwhelmed by their trauma histories and symptoms and avoiding the interest and involvement of others.
The degree to which self-management and its components were adopted as conscious strategies from the beginning varied across participants. Some women had only recently realized what strategies they had used; for instance, saying, “I have just done it, automatically. It has always been like that. I have focused on others, in a way that it almost became about me.” Others took pride in being strong and being able to influence their own situation; for instance, by actively intervening in family interactions to prevent new episodes of domestic violence:
At home, I read the expressions of the other [family members]. I was on guard all the time. And if there were arguments, and they got angry or something, then I thought, “What happened now?” Then I had to try to make them stop arguing.
Regardless of how conscious their strategies had been, the core issue was to find management methods that did not involve anyone else: “Well, I have worked! Worked, worked, and worked to manage by myself in every possible way.” None of the participants had reached out and disclosed their childhood traumas. They found self-reliant ways of dealing with their life situations, posttraumatic symptoms, and new traumas. For some participants, this was very demanding: “I have struggled to be a good girl. I have pulled it together. I have worked and given it my all.”
This self-reliant way of being in the world and the hardships these women endured somehow became normal to them. Several of the participants admitted that they did not realize that their situation was different from other children’s everyday lives until they began school. Often participants had not considered their trauma-related symptoms to be abnormal: “Well, I have been influenced all my life by the experiences I had as a child. I have been overwhelmed by feelings all my life, really, but that is normal for me.” Meeting the world in this self-reliant manner, the participants managed to lead relatively “normal” lives for several years. They studied and worked. They were productive citizens. They managed to keep up their “façade,” as one participant phrased it.
Keeping trauma history and symptoms at a tolerable distance
All participants described how they were not fully in touch with or even fully aware of their trauma histories. They accomplished this in different ways. Some participants talked about building a “mental wall” between their traumatic experiences and conscious attention. They remembered the traumatic experiences, but managed to keep a mental distance from them. Others had “cut away” their trauma history, as they described it, to such an extent that it was no longer consciously accessible to them. Many participants also reported having chosen not to pay attention to their symptoms, and finding ways to ignore them whenever they came up. For several participants, a crucial strategy to maintain this distance was to stay active all of the time and consciously change their focus—mentally or physically—whenever they encountered something trauma-related. Although mentioned as separate elements here, several components of this strategy were often used simultaneously to keep things in check:
I managed to divert. I mean, not thinking about it, doing other things. Well, steer the focus, do something all the time. That became the drive for everything. . . . That [the trauma history] was a part of my life that I had cut away.
Together, these different ways of keeping trauma content at a tolerable distance helped the participants manage on their own by reducing their likelihood of being flooded by their trauma histories and symptoms, thus helping them to function in their daily lives.
Hiding trauma history from others
A necessary element of self-management was to actively hide their histories so that no one would understand that they were, or had been, exposed to trauma: “I have tried to hide as much as possible. So when people came over I used all my energy on being as normal as possible.” This component of self-management also related to experiences indicating that others could not be trusted, and that one was on one’s own in life. A few women said that people close to them had asked them directly if they had been exposed to childhood trauma. They denied it, even when asked directly. This response was experienced as necessary at the time to make sure no one else became privy to their problems and experiences. It did, however, also make the decision to seek help even harder, because they were afraid no one would believe them:
He [husband] tried to ask me in the beginning [when I got sick] if something had happened in my childhood. And I denied it! Denied! My doctor asked me, and I denied and denied! All the way up until last spring. . . . So when I opened up, it wore on me. “I have denied! I have denied to everyone who asked! Now they will think I am lying.”
Contributing and helping others
Shifting the focus away from themselves and toward others became a form of self-management for several participants. They talked about how they became the problem solvers for everybody around them. Some were aware that this behavior helped them keep their own problems at a distance. It kept them occupied and left them no time to think about their own situation, and also kept others from asking how they were doing. By being the helper or the fixer, they maintained an image of being the strong one, the one who needed nothing. However, some participants only recently discovered that this had been a strategy for them, and realized that, over time, helping had become an imperative rather than a choice. This realization troubled a few of these participants, and they reported working actively to change this pattern and to begin using “no” as a viable response when someone asked for favors. Helping others also provided some participants with new perspectives on their own experiences:
You are not alone having experienced such things. I have had that in mind all the time as I got older. I have been a person who has been there for others when they have problems, but I have never told them anything about myself. . . . Sometimes I have been fed up listening to people and thought, “My God! If I had gotten paid for this, I would have been loaded!” And comparing what others have experienced with what I have experienced, it has been hard at times to find sympathy for those I listen to, because I have experienced so much in comparison. But still, people experience things differently. So what might be a normal day in somebody’s childhood might be a terrible day for someone else.
Even though some participants had negative experiences associated with adopting the strategy of contributing and helping others, the strategy also provided them with experiences of coping and positive feedback:
Because that is what I always have done—keeping it [the trauma history] to myself, and trying to find solutions that suited everyone. . . . Because I was so good at things! That is what I heard over and over. So then, I became even better at things! I was so good at things! I worked hard, fixed things for others. . . . I had to show myself that I could fix something.
The women’s experiences illustrate how they found various ways to manage on their own. Over time, the ability to manage on their own became an important value in and of itself. These factors, together with a strong motivation to keep trauma-related content at a distance, pulled them away from seeking help, and therefore contributed to long delays in doing so.
Encountering Situational Demands Exceeding Available Resources
At some point the participants encountered life events that challenged how they related to their trauma histories, to themselves, and to others. Their acquired equilibrium was broken, resulting in trauma-related content getting uncomfortably close. An accumulation of stressors and/or physical illnesses that made their previous strategies unavailable, major life changes (e.g., getting married or divorced, giving birth), or encounters with people who had different perspectives from themselves, represent examples of situations that participants found knocked them off-balance.
These situations were not necessarily negative, however. One participant found that getting married led to a collapse of her existing strategy. The change from always having been on her own to realizing that there was someone there whom she could trust was positive, yet so fundamental that she lost her balance. The mental wall she had maintained between her traumatic experiences and her conscious attention collapsed and traumatic memories intruded, such that she experienced a drop in her level of functioning:
The only explanation I have been able to find is that at that point [when I got sick] I understood, or my body understood, that “you are not alone anymore. You do not have to manage everything on your own anymore.” Because then I had married the man I am married to today, and then I fell down like a wet cloth. There was nothing left. And then the wall that I had managed to keep up all these years against those things that happened in my childhood also fell.
For another participant, the accumulation of stressors led to her history coming too close for comfort:
I moved away from my partner. I had a divorce. I moved away from the village I lived in, my job, and everything. And when I had used, well, strength to establish a new life here and things got quieter, it was as if I got hit by my own life! Everything caught up with me!
Some participants fell ill, and therefore could not continue using their preferred strategy of remaining active to keep things in check. The result was an increase in symptoms:
When I had my second child I got sick, and I was put on a lot of penicillin. And I did not get to go outside. I am obsessed with working out. I have worked out all my life. When I was pregnant, I was working out until the day I gave birth because that’s the kind of person I am: active. So, when I did not get to go outside and had to be inside and was on penicillin, it made me a lot worse.
One participant encountered a psychologist who asked her directly about potential traumatic exposure as part of her somatic treatment. Her method of coping with her traumatic experiences had previously been characterized by not looking back but always looking forward. She had remained active, never stopping to think about how she had been affected by all the horrible things she had experienced. She found that the psychologist’s questions made her stop to reflect on her own experiences. This changed how she looked at herself, her need for help, and her history:
Then, all of a sudden, there was a person asking me about something other than my somatic illness! “How are you doing?” she asked! “Well,” I replied, “I am doing fine,” and I just spoke about medication, and then she asked, “Have you ever been sexually abused?” “Yes!” I replied. “How do you mean?” I knew the answer, but no one had ever asked me before. It had not even occurred to me [that I might need help for that]. . . . Then I suddenly started to think about the things I had gone through. . . . and everything that had been going on in my family, and it was strange because I had never thought about that before. I had not had the time to think about it!
The participants’ stories illustrate that an array of different situations can disrupt one’s equilibrium, resulting in available strategies and resources being experienced as insufficient to deal with the current situation.
The Feeling of Losing Control
Faced with situations that exceeded their available resources, the participants felt they were starting to lose control. The experience of losing control had the following subthemes: the body has a will of its own—exhaustion and intrusive physical symptoms, and incomprehension, whereby participants reported not understanding what had happened to them. This change was experienced as threatening: “I have always worked! . . . And, when I could not do that anymore, because of physical reasons, I lost my parachute, so to speak. I was free falling.”
The body has a will of its own—exhaustion and intrusive physical symptoms
As symptoms increased, the women found that their feelings of exhaustion and forceful physical symptoms eventually demanded their attention. Their bodies made sure the message came through:
I was so exhausted all the time. I was constantly tired. I did not manage to do anything at home except things I was forced to do. I managed to work, but that was it. And over time, I felt I did not manage that either. . . . I was so dizzy and nauseous. I had a body scan because they thought it might be a tumor. That was how sick I was. The body was giving a message! And it had started to send messages long before, with other symptoms.
These experiences were reported by the majority of participants, many of whom reported feeling as though the body had a will of its own, and that they could no longer manage to fight it. The participants had endured years of not being fully in touch with all of their experiences and bodily sensations. In fact, this was part of their self-management strategy. It was not the numbing of feelings or the lack of contact with their own histories that brought about a sense of losing control. It was the bodily sensations that intruded on them, the way they lost control over their body and their feelings, and the impact their trauma histories had on them.
Incomprehension
The women also noted that their ability to understand what was happening to them and to construct meaning slipped away as their trauma histories came too close for comfort. Several participants thought they had put such things behind them, and could not understand why these things had come back to haunt them:
My life now is stable; I’m safe. It has been like that the past eight or nine years, and that is why I do not understand! Why is it coming back now? And to haunt me? All those things. All those feelings. I do not understand! I cannot manage to get a grip on them. Why on earth does it happen?
Faced with these threatening experiences of losing control and not understanding what was happening to them, the participants reported feeling like they were running out of options.
Being at the End of the Rope
As the informants experienced a rise in intrusive symptoms as well as decreasing control and energy, they described experiences and feelings of balancing on the edge. They reported feeling as though they were at “the end of their rope.” The women found that their preferred strategy of managing on their own was no longer sufficient. They did not know how to regain control of their symptoms, and this was very distressing:
The dark train [traumatic memories] just came, and crashed into [me]. It ruined everything. You did not get on the right track again. You tried desperately, but it was like rowing against the current, with the current just growing stronger and stronger.
Some participants experienced it as everything coming to a stop after they had managed to push forward through numerous obstacles for years:
I got to a point where I got up in the morning and thought, “I cannot take any more! I cannot do it! I cannot take going to work. I cannot relate to anything.” It was as if everything came to a stop.
For a few participants, the experience of not managing anymore became so strong that they saw death as a viable alternative:
It had come to the point where I did not want to live anymore because I did not believe that it was possible to feel okay again. I had the feeling that I was destroyed, and that my life was so destroyed—that it was not possible to feel better. There was no hope. I realized that I was getting sick when I was thinking that if I hurt myself I would have to hurt my children too, not to leave them alone.
Often it was the combination of forceful physical and intrusive symptoms and how their symptoms had a negative influence on significant others that ultimately led them to seek help:
I was at home with my child. I was lying on the floor, my head completely destroyed. It was insane to see that I could not do anything to snap out of it. I could not do it on my own. And at the same time it affected my children. It was so tough! I did not know what to do.
Feeling that they were balancing on the edge, these participants came to realize that they could not do it all by themselves anymore:
I cannot do this on my own! I need help! Up until that point I had believed that I could manage on my own. I will fix this on my own. Because that is what I have been used to doing.
After a long and strenuous journey, the participants eventually reached a point where they abandoned their preferred strategy, but they did not give up. Instead they reached out to get help.
Seeking Help
Getting to the point of seeking help had taken years, and even decades, for many of the participants. Seeking help was experienced as neither easy nor positive; however, “It was a defeat [having to seek help]! Because I was going to manage it [on my own]! But at that point I just had to do it [seek help].” Most of the participants reached out to their GP for help, presenting with somatic complaints. Only a couple of the participants actually disclosed their trauma histories when seeking help. Often the GPs discovered more general mental health problems and referred the women to the specialized mental health service without being aware of their trauma histories.
The time that elapsed from when the participants sought help to when they actually received help varied. Although most participants received treatment, and often trauma-specific treatment, relatively quickly after seeking help, a few participants reported that despite their efforts to seek help, their need for help was unacknowledged. One participant had waited decades before she sought help. In the GP’s opinion, she was not “ill enough” to be referred to mental health care, despite the fact that she was one of the few participants who forced herself to talk about her traumatic background. She had to wait another year and change her GP before she was eventually referred and received trauma-specific treatment. This example illustrates how the needs of trauma survivors, who have been used to managing on their own, are not necessarily acknowledged when they eventually reach out for help.
From Others’ Initiative to Perceived Need for Help
Although the majority of the participants initiated their first contact with the health care system, 2 participants got in touch with the system before the age of 18 because their drug use and behavioral problems caught the attention of those around them. At that time, however, no one was aware of their trauma histories. Even though the actions of others resulted in earlier contact with the health care system for these 2 women, they did not receive trauma-specific treatment for years. They did not believe they needed help, and were not ready to discuss their traumatic backgrounds. They quit treatment several times and were in and out of treatment for many years before they eventually initiated treatment independently and were ready to address their trauma histories.
The good intentions of others also became an obstacle to help for these 2 participants: “Everyone was so eager to help me that I backed out.” Even after they decided to seek help they used time to become ready to work with themselves: “Eventually I realized that maybe I needed some help. Today I must admit it was 50/50 between wanting help and wanting more pills.” Only several years and new traumas later was this woman ready to initiate help seeking and relate to her problems, the time she referred to as “the time it was for real.” Her descriptions of her state once she was truly ready to receive help are similar to the descriptions related to “being at the end of the rope”:
I was completely destroyed! At that point, there was nothing left of me, I think. There was nothing more to give. . . . It became so tough that I realized that I had to do something about it. Now it is either/or!
These participants experienced that the way they benefited from therapy changed over time as well. As they grew older and their life situations became more stable, they slowly became ready to approach their trauma histories and trauma-related symptoms:
I have not related to it [the trauma history]. I have been in therapy for God only knows how many years, and still I have not approached it. Maybe I have looked at a few minor things, seen some of my patterns, but still. All that I have experienced has been left alone. . . . I was not ready to be in therapy and look at those things at all. It was too tough for me, really. So I think I shut out a lot of things at that time, and now I manage to open up, and to, in a way, be more in touch with it. . . . In a way, I understood that it was bad back then, but I had not come far enough to look at myself in that way. Not at all.
These stories illustrate how important it is to explore and respect individuals’ perceived need for help and their attitude toward receiving help when planning and offering trauma-specific treatment. This is particularly true in cases in which others initiate contact with the health care system. Timing needs to be attuned to a woman’s readiness to accept help if she is to benefit fully from treatment. Earlier might not always be better when it comes to providing trauma-specific treatment following childhood trauma.
Overall Discussion of the Help-Seeking Process
The strategy of managing on one’s own was a self-reinforcing path for these women, and one that ruptured when they encountered situational demands that exceeded their resources, resulting in an intolerable increase in intrusive symptoms and experiences of losing control. When taken together with a perceived negative influence on their significant others, the women felt they could no longer manage on their own and made the decision to seek help. The important role of bodily experiences in the process of help seeking following childhood trauma is also underlined by these women’s descriptions of their experiences immediately before they sought help. Having endured years of not being fully in touch with their feelings and experiences, it was the intrusive and bodily character of the symptoms experienced prior to help seeking that ultimately led to their decision to seek help. This reminds us of the importance of integrating a focus on the body when working with survivors of trauma (Ogden, Minton, & Pain, 2006), as well as the importance of exploring the types of distress and experiences that put the person in touch with the health care system.
The reported delays in help seeking in the present study support existing research (Fikretoglu et al., 2010; Wang et al., 2005), and underlines how help seeking constitutes a process over time (Burgess-Proctor, 2011). The delays were not related to low levels of distress experienced by participants in the present study prior to seeking help, however. On the contrary, the participants’ stories and timelines show that they experienced high levels of distress and new traumas, and still did not consider help seeking as an option. Originally dependent on others for help as young children, the participants found that their legally acquired autonomy and independence at the age of 18 did not become decisive for seeking help. They still did not trust others, did not want to experience painful memories and bodily sensations, and had decided that the trauma history was something they had put behind them. They had found their own ways of dealing with their experiences. Even though this meant that they avoided and ignored their trauma histories and symptoms, it also indicated a strong will to manage and an ability to cope with their aversive experiences in ways that did not interfere with their everyday functioning.
The participants’ stories therefore nuance the conceptualization of self-management as a mere barrier to help seeking (Kessler et al., 2001; Koenen et al., 2003; Sayer et al., 2009; Wang, 2006). The findings also shed light on how substantial delays in help seeking can come about. The strategy of self-management, despite its downsides, has several positive outcomes as well. It represents an active effort to regain control, and therefore a counterbalance to traumatic experiences, in which lack of control is central (Saporta & van der Kolk, 1992). Additionally, participants received positive feedback from others because they were so strong and self-sufficient, and they contributed and helped others. Almost paradoxically, non-help-seeking became vital for their ability to navigate in life, and was an important resource for these women.
Being sensitive to the multiple functions of self-management is arguably very important to clinicians. Working as clinicians, we run the risk of being so focused on providing accessible, efficient treatment as quickly as possible that we lose sight of the benefits of self-management. The capacity to struggle and overcome life’s adversities is an important path to development. Self-management therefore bears the potential for developing a stronger sense of agency, self-efficacy, and sense of coping—all of which are important to thrive and experience good quality of life. Our findings also illustrate, however, that an overemphasis on self-management, at the expense of seeking support from others, might be problematic. Help seeking might not feel like an option to survivors of childhood trauma until they have pushed themselves to the edge. Clinicians need to be sensitive to how a certain degree of self-management might be beneficial, promoting well-being while also noticing when a one-sided reliance on self-management stems from seeking help not being perceived as an option.
Is there then a way to promote help seeking as a viable option following childhood trauma? Given our results, GPs and other health care workers might play a crucial role in promoting help seeking as an option following childhood trauma. Our results indicate that probing for trauma experiences might be particularly important in this respect. GPs might encourage their patients to seek help sooner by querying them about traumatic experiences when they present with multiple physical and/or mental complaints, or a drop in experienced self-control. Mental health care workers might be able to begin trauma-specific treatment sooner, as well, by probing for traumatic experiences when clients present with general mental health problems. In addition, it seems reasonable to assume that making more information available to the public about the problems that typically arise following childhood trauma and available help might make therapy a more viable option for those in need of help.
Although probing for adverse life events might be important in terms of facilitating individuals’ readiness to receive help, probing once might not be sufficient for them to disclose their traumatic experiences. As a prerequisite, therefore, questions should respectfully communicate the possibility that the person might not be ready to admit to such experiences. Parallel to such probing, health care workers should collect information about individuals’ current readiness to accept help. Our findings seem to indicate that excessive enthusiasm on the part of the health care provider during the initial phases might scare people off, whereas unresponsiveness to the expressed need for help, even if the symptoms presented are not typical of trauma-related disorders, might exclude those in need of help. Hence, our findings imply that previous unsuccessful treatment should not automatically disqualify people from receiving new treatment, or be interpreted as an indication for a poor prognosis.
Finally, our findings illustrate how self-initiated help-seeking behavior might represent a substantial change for survivors of childhood trauma, and a sign of indomitable hope. Once they reached the end of their rope, the participants finally realized that they could not manage on their own. They did not give up, however. Instead, they showed courage by reaching out, hoping that change was possible with the help of others. Therefore, help-seeking actions should be seen as indicating a strong possibility for change, and exploring these actions and the experiences leading to them as part of the initial phase of treatment might prove important in terms of gaining access to clients’ resources and potential for change.
The present study took place in a context in which all participants were receiving health care and had recently received trauma-specific treatment. All interviews were also conducted in the clinic, at the participants’ wishes. This interview context might have rendered experiences related to health care more easily accessible to the participants. Therefore, the interview context might help to explain why all participants shared their experiences of seeking health care assistance, despite being asked more general questions about help seeking not specific to health care assistance.
Conclusion
The presented findings provide new knowledge on the experiences leading women to seek help following childhood trauma and the potential reasons such help-seeking behavior might be delayed. The findings also highlight how proper timing between an individual’s help-seeking process and the type of help offered might ensure that he or she receives the full benefit from treatment. Prior to seeking help, self-management was a key strategy for the participants in this study. Despite the fact that it delayed help seeking, the strategy of managing on one’s own represented an important resource for participants, giving them a feeling of control, providing them with positive feedback from others, and enabling them to function satisfactorily in their everyday lives. Help seeking was the last resort for participants and thus, in itself, represented a substantial change. Clinicians need to recognize this. Ultimately, it was the experience of losing control over their symptoms and the resulting negative influence they felt they were having on their significant others that led them to seek help.
Footnotes
Acknowledgements
We thank the participants for generously sharing their stories and experiences with us. The cooperation of the two external interviewers, Kristin J. Dahn and Ragnhild Dalvik, made this research possible. Thank you! We also extend our gratitude to Tush Grafisk for helping with the model’s design.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was received from the Northern Norway Regional Health Authority and Finnmark Hospital Trust.
Author Biographies