
Abstract
Keywords
Adult survivors of sexual violence often enter community-based services with substantial psychological distress, requiring intake assessment of event-related symptoms alongside broader internalizing problems that can impair functioning and elevate risk. Meta-analytic evidence based on Diagnostic and Statistical Manual of Mental Disorders (DSM-5)-defined outcomes indicates that sexual assault victimization is associated with elevated risk for a wide range of mental disorders, with particularly high burden for depressive disorders and posttraumatic stress disorder (PTSD) (Dworkin, 2020). Complementing this, additional meta-analytic work suggests that PTSD symptoms during the first year postassault are common and frequently severe (Dworkin et al., 2023). Importantly, trauma-related distress rarely occurs in isolation; presentations commonly include symptoms of depression, anxiety, and general stress reactions (e.g., Angelakis et al., 2020; Davis et al., 2022; Dworkin, 2020; Dworkin et al., 2017; Flory & Yehuda, 2015; Karatzias et al., 2020; Sareen, 2014). This co-occurrence underscores the practical value of brief trauma-focused screening tools that efficiently measure event-related distress and have convergent validity with broader emotional distress.
In practice, agencies must identify symptom burden quickly at intake to support triage, guide referral and care planning, and establish a defensible baseline for monitoring. Because intake is time-limited and survivors may be fatigued or distressed, feasibility is central to routine screening. Services therefore require brief measures that can be administered consistently across high caseloads without overburdening clients or staff, while maintaining adequate psychometric support. Against these routine-care constraints, instrument choice in sexual violence services is shaped by a practical tension between DSM-5-aligned instruments and legacy tools that may remain embedded in intake workflows because they are familiar, relatively brief, and easy to administer repeatedly. Accordingly, the present study evaluates the psychometric performance of the Impact of Event Scale–6 (IES-6; Thoresen et al., 2010), an abbreviated version of the IES–Revised (IES-R; Weiss & Marmar, 1997), for routine intake screening in community-based sexual violence services, with particular attention to total-score interpretation, validity evidence, and gender comparability.
Literature Review
DSM-5 PTSD Measurement and Legacy Measures in Routine Care
Contemporary PTSD assessment is anchored in DSM-5 and DSM-5-TR (American Psychiatric Association, 2013, 2022), and DSM-5-aligned instruments such as the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013) and the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5; Weathers et al., 2018) have strong psychometric support across clinical and research contexts (e.g., Blevins et al., 2015; Bovin et al., 2016; Oliveira-Watanabe et al., 2021; Rivest-Beauregard et al., 2022; Roberts et al., 2021; Weathers et al., 2018; Wojujutari et al., 2024; Wortmann et al., 2016). At the same time, community practice does not always operate with the newest instrument as its default. Legacy measures often remain embedded in intake workflows because they are familiar, relatively brief, and easy to administer repeatedly. This is especially true for the IES family, including the original IES, the IES-R, and abbreviated derivatives such as the IES-6, which continue to be used internationally as brief indicators of trauma-related distress in trauma-exposed populations (Giorgi et al., 2015; Horowitz et al., 1979; Hosey et al., 2019; Jeong et al., 2022; Thoresen et al., 2010; Weiss & Marmar, 1997).
Consistent with this applied orientation, the present study treats IES-based scores as indicators of trauma-related distress severity for intake screening and potential practice-based monitoring rather than as diagnostic determinations (Weiss & Marmar, 1997). Because the present data are cross-sectional, however, conclusions about longitudinal responsiveness and sensitivity to change remain beyond the scope of this study. This distinction is important because changes in diagnostic frameworks do not remove the service need for brief, feasible measures of event-related distress; instead, they increase the importance of showing that a given measure functions adequately in the target setting and population. More broadly, the PTSD measurement literature does not always support identical factor structures across samples, and self-report symptom scales do not necessarily reproduce the same dimensions in all populations (Elhai & Palmieri, 2011). Accordingly, the present study evaluates the factor structure and score interpretation of the IES-6 within routine intake screening in community-based sexual violence services. In doing so, it responds to the need for psychometrically defensible, practice-based assessment tools that can support triage, care planning, and routine outcome monitoring in community social work settings.
The IES-R: Foundations and Structural Considerations
The IES-R (Weiss & Marmar, 1997) is a 22-item self-report measure designed to assess trauma-related distress across three domains—intrusion, avoidance, and hyperarousal. It has been widely used in trauma research and applied settings, in part because it is brief enough to be feasible yet comprehensive enough to capture core posttraumatic stress reactions tied to a specific event. Despite its extensive use, studies have reported variability in the IES-R's latent structure across contexts and populations. For instance, in some veteran and community samples, evidence has supported more parsimonious representations (e.g., one- or two-factor solutions) rather than the original three-domain structure (Creamer et al., 2003). In other trauma-exposed civilian samples, expanded multidimensional models have been favored, including solutions that differentiate sleep disturbance as a distinct factor (Gargurevich et al., 2009) and five-factor structures that separate domains such as numbing and sleep disturbance (Morina et al., 2010). Across studies, findings indicate that no single IES-R factor structure consistently dominates across samples, with support varying between the original three-domain model and alternative one-, four-, and five-factor solutions depending on the population and assessment context (Creamer et al., 2003; Gargurevich et al., 2009; Morina et al., 2010). This variability has been attributed, in part, to methodological and contextual differences, including symptom query instructions, trauma exposure characteristics/severity, cultural or ethnic context, and timing of assessment (Elhai & Palmieri, 2011).
For applied screening, this variability has practical implications. Specifically, if the IES-R is best represented by a single underlying factor in a particular service population (i.e., one core dimension of event-related distress rather than separable intrusion, avoidance, and hyperarousal domains), then using a total score may be defensible; if a multidimensional model fits better in that setting, reliance on a total score alone may warrant greater caution.
For brief screening tools derived from the IES-R, such as the IES-6, the structural question becomes even more consequential because short forms typically prioritize feasibility and low-burden repeated administration. A shortened assessment tool that shows an interpretable scoring structure can be especially valuable for routine intake screening and may also be practically useful for ongoing monitoring, provided that its score interpretation is supported empirically in the population and setting in which it is used.
Rationale and Utility of the IES-6
Although the IES-R remains widely used, its 22-item length can create an administrative burden in high-volume service systems. Even measures such as the 20-item PCL-5 may be perceived as overly lengthy during intake sessions where survivors may be in acute distress and services must prioritize rapid assessment. Brief tools may reduce respondent burden and improve the feasibility of repeated practice-based assessment—features that may support measurement-informed clinical decision-making across sessions when score interpretation and responsiveness are appropriate for the intended use.
To reduce burden while retaining coverage of core posttraumatic stress content, Thoresen and colleagues developed the IES-6 by selecting two items from each IES-R domain (intrusion, avoidance, hyperarousal) using a stepwise regression approach (Thoresen et al., 2010). In their development work across four trauma-exposed samples, the IES-6 showed very high correspondence with the full IES-R (pooled r = .95) and good agreement with an external PTSD checklist reference (PCL-S), supporting the use of a simple (unweighted) total score for rapid screening (Thoresen et al., 2010).
To our knowledge, subsequent studies have extended validity evidence in medical, occupational, and population contexts, but published psychometric evaluations have not specifically focused on routine intake workflows in rape crisis centers or sexual assault clinics. For example, in acute respiratory distress syndrome survivor cohorts, the IES-6 showed strong internal consistency across follow-up time points, convergent patterns with related constructs (e.g., anxiety/depression), weaker relations with less-related constructs, and criterion validity against CAPS-based PTSD diagnosis (Hosey et al., 2019). In an occupational trauma sample (bank robbery victims), confirmatory factor analysis (CFA) supported a three-factor solution and adequate internal consistency (Giorgi et al., 2015). In a COVID-19 population study, Jeong and colleagues reported evidence consistent with unidimensional measurement and evaluated convergent validity via correlation with the PHQ-4, a brief screening measure of anxiety and depression (Jeong et al., 2022).
At the same time, what remains comparatively untested is the IES-6's performance as part of routine workflow in community-based sexual violence services, particularly at intake and as a potential tool for subsequent practice-based monitoring. The present study focuses on whether its factor structure, total-score interpretability, reliability, and validity evidence support its use as a brief indicator of trauma-related distress in this specific service context; longitudinal responsiveness and sensitivity to change remain important questions for future research.
Existing work includes validation in general healthcare samples in which the indexed traumatic event may include sexual violence—for example, among Zimbabwean primary care attendees, the trauma exposure assessment explicitly included rape and assault (Abas et al., 2023). Because the trauma exposure assessment in Abas et al. (2023) explicitly included rape and assault, those findings may have indirect relevance to sexual violence service contexts; however, they do not constitute psychometric validation conducted within sexual assault service systems as part of routine intake screening.
Validity Evidence Relevant to Routine Intake Screening
Because the IES-6 is used in routine sexual violence service intakes primarily as a brief indicator of event-related distress severity—and is often interpreted using a total score—validity evidence should prioritize support for this intended interpretation and use. In the present study, the primary intended use is intake screening and baseline severity documentation, with potential relevance for practice-based monitoring if future longitudinal research supports responsiveness to change. Adopting a use-focused validation approach, the present study evaluated key sources of evidence relevant to intake screening: (a) the IES-6 internal structure to determine whether a unidimensional model is supported (and therefore whether total-score interpretation is defensible in intake settings), (b) internal consistency reliability, (c) convergent validity through associations with broader internalizing distress (i.e., depression, anxiety, and stress), and (d) known-groups validity using intake information routinely collected in service settings. Other forms of evidence (e.g., test–retest reliability, responsiveness, diagnostic accuracy) were beyond the scope of the available cross-sectional intake data.
To support equitable interpretation in mixed-gender service samples, we also assessed measurement invariance (MI) across men and women. Measurement invariance evaluates whether the IES-6 functions equivalently across groups by testing increasingly restrictive forms of invariance (configural, metric, scalar) and applying established decision criteria (Chen, 2007; Cheung & Rensvold, 2002). Establishing MI is essential when comparing mean scores across groups because observed differences may reflect measurement nonequivalence rather than true differences in latent distress severity. This consideration is particularly salient in sexual violence services that provide care to both men and women, given documented sex differences in trauma exposure patterns and PTSD burden that may shape symptom presentation and score interpretation (Tolin & Foa, 2006). If full scalar invariance is not supported, mean comparisons should be interpreted cautiously, and agencies may need to avoid drawing strong conclusions about gender differences in symptom severity based solely on observed total scores.
As an additional, practice-relevant validity check, we examined known-groups validity using partner status, a routinely collected intake variable. Known-groups evidence is informative when an intake indicator is plausibly related to symptom severity through clinical mechanisms such as social context and access to relational resources. More broadly, posttrauma social support is a robust predictor of PTSD symptom severity, with lower perceived support associated with higher PTSD symptoms (Ozer et al., 2003; Wang et al., 2021; Zalta et al., 2021). Evidence from sexual assault survivor samples suggests that the postassault social context is meaningfully related to PTSD symptom course over time: higher perceived support has been linked to subsequent reductions in PTSD symptoms in longitudinal work, and disclosure-related social reactions (including supportive vs. negative responses) have shown prospective associations with PTSD severity (Dworkin et al., 2018; Ullman & Peter-Hagene, 2016). Because partner status is only a coarse proxy and does not capture relationship quality, perceived support, or disclosure responses, we treated this comparison as a pragmatic, intake-based known-groups test rather than a direct test of social support mechanisms.
The Present Study
Building on this use-focused rationale, the present study evaluates selected psychometric properties of the IES-6 in a large intake sample of adult survivors of sexual violence, with the goal of informing defensible total-score interpretation for routine intake screening and potential practice-based monitoring in community-based sexual violence services. Measurement invariance was evaluated using established multigroup CFA decision criteria (Chen, 2007; Cheung & Rensvold, 2002). Convergent validity was evaluated using associations between IES-6 scores and internalizing distress indicators operationalized as Depression Anxiety Stress Scales–21 (DASS-21) scores (Lovibond & Lovibond, 1995a, 1995b), and known-groups validity was examined using a social-context indicator (partnered vs. not partnered) derived by collapsing the marital status variable into two categories. This study provides practice-relevant measurement guidance by addressing the following questions:
Factor Structure and Total-Score Use: Does the originally proposed one-factor IES-6 model demonstrate acceptable fit in this intake sample, supporting the defensible use of a total score as a brief indicator of trauma-related distress for intake screening and potential practice-based monitoring? Reliability: Does the IES-6 demonstrate acceptable internal consistency reliability in this clinical sample? Convergent Validity: To what extent are IES-6 scores associated with broader indicators of internalizing distress, specifically DASS-21 scores? Known-Groups Validity: Do IES-6 scores differ by partner status (partnered vs. not partnered), derived by collapsing the original marital status variable into two categories? Measurement Invariance Across Gender: Does the IES-6 demonstrate configural, metric, and scalar measurement invariance across men and women? If full scalar invariance is not supported, what are the implications for interpreting gender-based mean differences?
Method
Study Design and Data Source
This study used a secondary analysis of de-identified archival intake data collected as part of routine practice within community-based trauma services in Southwestern Ontario, Canada. The dataset was coordinated by a lead community-based trauma agency overseeing a network of publicly funded programs supporting survivors across multiple counties in the region. The original de-identified database contained 2,986 client intake records collected over a 12-year period between January 2010 and May 2022. Intake assessments were completed prior to, or at the initiation of, services and were used for screening and program monitoring.
A multistage screening process was used to refine the administrative intake database into the final analytic sample. First, analyses were restricted to adults (≥18 years). Second, because standardized symptom measures (the IES-R and the DASS-21) were collected as part of routine intake but were not required for access to services, item nonresponse was common in the raw database. Cases were retained only if they provided item-level data on both the DASS-21 and the IES-R item pool from which the IES-6 items were drawn. Third, to limit the impact of extensive item nonresponse and support stable item-level estimation, cases with more than 10% missing item responses on either the DASS-21 or the IES-R item pool were excluded. Following these sequential steps, the final analytic sample included 893 service-seeking adult survivors of sexual violence (451 men; 442 women). Ethics approval was obtained from the University of Windsor Research Ethics Board (#12-080), and all analyses were conducted using de-identified data.
In the retained analytic sample, remaining item-level missingness on the IES-R and DASS-21 symptom items was low (5.6%–6.3% across items). Missing values on these symptom indicators were imputed using the Expectation–Maximization (EM) algorithm in SPSS, a maximum-likelihood approach for handling item-level missingness assuming missing at random (Little & Rubin, 2002). Expectation–Maximization was applied only to symptom items (IES-R and DASS-21 items), not to demographic variables. Unless otherwise noted, subsequent CFA and correlational analyses were conducted using the EM-imputed dataset.
Participant characteristics are summarized in Table 1. The sample included 893 adult survivors of sexual violence (451 men; 442 women). The mean age was 38.57 years (SD = 13.52; range = 18–88), based on available data (n = 854). Table 1 presents distributions for education, employment status, annual income, and marital status for the full sample and separately for men and women. Annual income was not used in substantive analyses because of substantial missingness overall and because income data were unavailable for women in the administrative dataset. Indigenous status (but not broader race/ethnicity) was assessed; among participants with available Indigenous-status data, most identified as non-Indigenous (93.6%), with 2.2% identifying as Indigenous and 4.2% selecting “Unknown” (14.6% missing overall). For known-groups analyses, partner status was derived by collapsing marital status into partnered versus not partnered. Because the administrative dataset recorded participants only as men or women at intake, we use “gender” pragmatically to refer to these recorded groups, while acknowledging that sex and gender are not interchangeable constructs.
Demographic Characteristics by Gender.
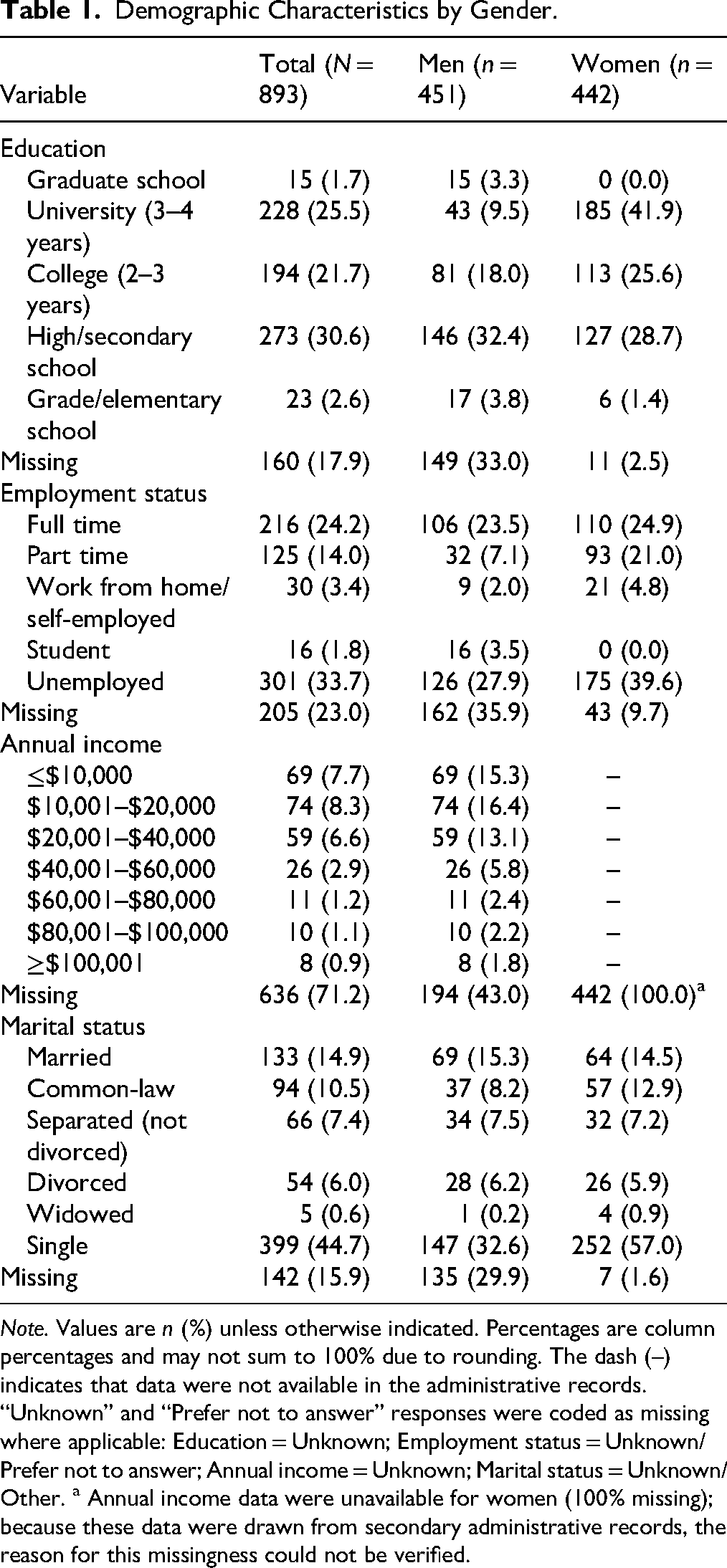
Note. Values are n (%) unless otherwise indicated. Percentages are column percentages and may not sum to 100% due to rounding. The dash (–) indicates that data were not available in the administrative records. “Unknown” and “Prefer not to answer” responses were coded as missing where applicable: Education = Unknown; Employment status = Unknown/Prefer not to answer; Annual income = Unknown; Marital status = Unknown/Other. a Annual income data were unavailable for women (100% missing); because these data were drawn from secondary administrative records, the reason for this missingness could not be verified.
Measures
Trauma-related distress was assessed using items from the IES-R (Weiss & Marmar, 1997). The primary instrument evaluated in this study was the IES-6 (Thoresen et al., 2010), a six-item abbreviated measure drawn from the 22-item IES-R pool, with two items representing each of the intrusion, avoidance, and hyperarousal content domains. Items are rated on a 0 (“not at all”) to 4 (“extremely”) response scale, referencing experiences in the past seven days. Consistent with the IES-6 development work indicating that scores may be expressed as either a mean or a sum (Thoresen et al., 2010), the primary IES-6 score in the present study was computed as the sum of the six items (range 0–24). For descriptive purposes, the equivalent mean item score (range 0–4) is also reported.
General psychological distress was measured using the DASS-21 (Lovibond & Lovibond, 1995a, 1995b). The DASS-21 is a 21-item self-report measure comprising three correlated subscales—Depression, Anxiety, and Stress—with seven items per subscale, rated on a 4-point scale from 0 (“did not apply to me at all”) to 3 (“applied to me very much, or most of the time”) with reference to experiences over the past week. In the present study, DASS-21 Depression, Anxiety, and Stress subscale scores were used as external indicators of internalizing distress to examine the convergent validity of IES-6 scores.
Preliminary Analyses
Data were screened for distributional characteristics and outliers prior to model estimation. Univariate normality was evaluated using skewness and kurtosis indices for the IES-R item set and the IES-6 indicators. All variables fell within conventional guidelines (e.g., |skew| < 2.0; |kurtosis| < 7.0; West et al., 1995). As expected in a large, trauma-exposed sample with ordinal symptom indicators, formal normality tests (e.g., Kolmogorov–Smirnov and Shapiro–Wilk) indicated statistically significant departures from normality (p < .001). Multivariate normality was examined using AMOS's multivariate kurtosis estimate; the multivariate critical ratio (c.r.) was large (c.r. = 7.14), indicating a departure from multivariate normality (Kline, 2016). Consistent with Kline's guideline, values exceeding |3.29| indicate statistically significant multivariate kurtosis (approximately p < .001 under a z-approximation) (Kline, 2016). Because the IES-6 items are ordinal Likert-type indicators, and the data showed significant multivariate kurtosis, standard maximum likelihood (ML) estimation may be sensitive to violations of multivariate normality. Accordingly, Bollen–Stine bootstrapping (5,000 resamples) was used as a robustness check to obtain a more reliable p-value for the χ2 statistic and to strengthen confidence in model fit evaluation under non-normality (Bollen & Stine, 1992).
Multivariate outliers were evaluated using the Mahalanobis distance computed from the six IES-6 indicators. Using the χ2(6) critical value of 22.46 (p < .001) as a conventional cutoff for multivariate outlier screening, no cases exceeded the threshold (maximum Mahalanobis distance = 21.55); results were unchanged under a more stringent criterion (e.g., p < .0001; χ2(6) ≈ 27.88). Accordingly, all cases were retained for analysis.
Analytic Strategy
Analyses were conducted in SPSS 31 and AMOS 31, with an ordinal CFA sensitivity analysis conducted in R using the lavaan package (R Core Team, 2025; Rosseel, 2012). Confirmatory factor analysis evaluated the IES-6 factor structure, with the primary model specifying a single latent factor representing global trauma-related distress, consistent with the intended use of the IES-6 as a brief screening and potential practice-based monitoring indicator (Thoresen et al., 2010). The primary CFA was estimated in AMOS using ML to maintain continuity with the original analytic approach. Model fit was evaluated using χ2, CFI, TLI, RMSEA (90% CI), and SRMR, interpreted using often-cited cutoff recommendations (e.g., CFI/TLI ≥ .95; RMSEA ≤ .06; SRMR ≤ .08) and the overall pattern of evidence rather than any single cutoff (Hu & Bentler, 1999). Given non-normality, the Bollen–Stine bootstrap was applied to obtain a robust test of overall fit. To address the ordinal item response format more directly, the one-factor models were also reestimated in R/lavaan using WLSMV estimation, with the six IES-6 items specified as ordered categorical indicators. This sensitivity analysis was used to evaluate whether the substantive interpretation of the IES-6 factor structure was robust to an estimator more appropriate for ordinal indicators.
Internal consistency of the IES-6 total score was evaluated using Cronbach's alpha. Construct validity was evaluated using complementary sources of evidence available in routine intake data, including convergent associations with internalizing symptoms and subgroup comparisons. Convergent validity was examined via Pearson correlations between IES-6 scores and DASS-21 Depression, Anxiety, and Stress subscale scores. Known-groups validity was examined using partner status (partnered vs. not partnered), specified in advance as a pragmatic subgroup indicator available in routine intake data and operationalized by collapsing the marital status variable into two categories. Because partner status does not directly measure perceived support or relationship quality, findings were interpreted as pragmatic subgroup evidence rather than a test of relational mechanisms.
Measurement invariance across men and women was evaluated using multigroup CFA in a sequential framework. A configural model (same pattern of fixed and free parameters across groups) was first estimated, followed by a metric invariance model constraining factor loadings to equality, and a scalar invariance model additionally constraining item intercepts. Invariance decisions emphasized changes in approximate fit indices rather than χ2 difference testing, given the sensitivity of χ2 to sample size and minor model misspecification. Following Cheung and Rensvold (2002), a decrease in CFI of no more than .01 was taken to indicate that added equality constraints did not meaningfully degrade model fit (ΔCFI ≤ .010). Consistent with Chen (2007), changes in RMSEA were also examined as a complementary criterion (ΔRMSEA ≤ .015).
When full scalar invariance was not supported, partial scalar invariance was examined by freeing a minimal set of item intercept constraints guided by modification indices while retaining the metric invariance constraints (Byrne et al., 1989). The implications of any remaining intercept noninvariance for interpreting observed or latent mean differences were reported transparently, with greater emphasis placed on comparisons of associations across gender where metric invariance was supported.
Results
IES-6 Item Descriptives and Internal Consistency
Descriptive statistics for the six IES-6 items are shown in Table 2. All items spanned the full response range (0–4). Item means ranged from 2.38 to 2.94 (SDs = 1.20–1.43). The IES-6 sum score (range 0–24) had a mean of 15.70 (SD = 5.47), corresponding to a mean item score of 2.62 on the 0–4 metric. Internal consistency was good in the full sample (Cronbach's α = .81; standardized α = .82). Interitem correlations were moderate to strong (r = .31–.65), with the strongest association between the two intrusion items (I3 and I6; r = .65). Corrected item–total correlations indicated adequate to strong discrimination (.46–.66), and deleting any single item did not improve reliability (α if item deleted = .77–.81), supporting the retention of all six items. For descriptive purposes, Cronbach's α was .83 for men and .76 for women. As expected when reliability is estimated in split samples, these subgroup coefficients differed modestly, reflecting gender-specific item covariance patterns, although both groups were above .70.
Impact of Event Scale-6 (IES-6) Item Descriptives and Internal Consistency.
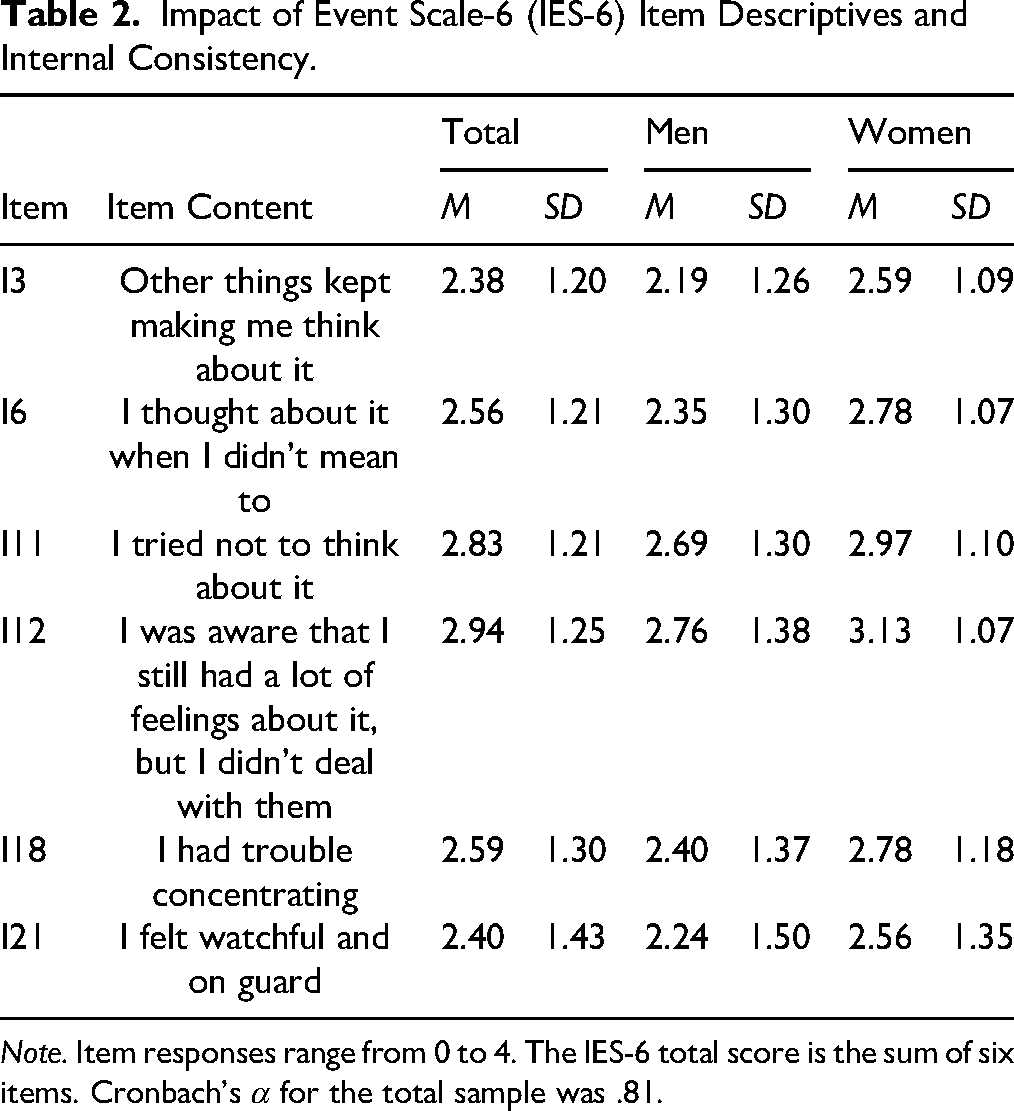
Note. Item responses range from 0 to 4. The IES-6 total score is the sum of six items. Cronbach's α for the total sample was .81.
In terms of observed group differences, women reported higher IES-6 total scores than men (women: M = 16.80, SD = 4.64, n = 442; men: M = 14.62, SD = 5.98, n = 451), and this difference was statistically significant, t(891) = −6.08, p < .001. The mean difference (men – women) was −2.18, 95% CI [−2.88, −1.48], corresponding to a small-to-moderate effect size (Cohen's d = −0.41, 95% CI [−0.54, −0.27]). However, because scalar invariance across gender was not supported (detailed below), this observed mean difference is reported for descriptive purposes only and should not be interpreted as clear evidence of a latent gender difference in trauma-related distress.
Confirmatory Factor Analysis of the IES-6
A one-factor CFA was estimated for the IES-6 (items I3, I6, I11, I12, I18, I21) in the full sample (N = 893), consistent with its intended use as a brief total-score indicator of trauma-related distress for routine screening. The initial one-factor model was then refined by allowing two residual covariances (I11 with I12; I18 with I21), reflecting clear item-content overlap and plausible local dependence within an ultra-brief item set. Specifically, I11 and I12 both involve avoidance or emotional nonengagement with the event, whereas I18 and I21 both involve hyperarousal-related concentration/vigilance content. This limited, theory-consistent refinement improved local fit and remained consistent with a practical one-factor total-score interpretation, although the residual covariances indicate localized item dependence and therefore caution against a claim of strict or “clean” unidimensionality. Alternative multidimensional CFA models were not estimated because each hypothesized domain would have been represented by only two indicators, which can limit the stability and interpretability of such solutions (Kline, 2016). As shown in Table 3, the refined model demonstrated improved fit and was retained as the final one-factor model for the present analyses. See Figure 1 for a visual depiction of the final CFA solution and standardized loadings.
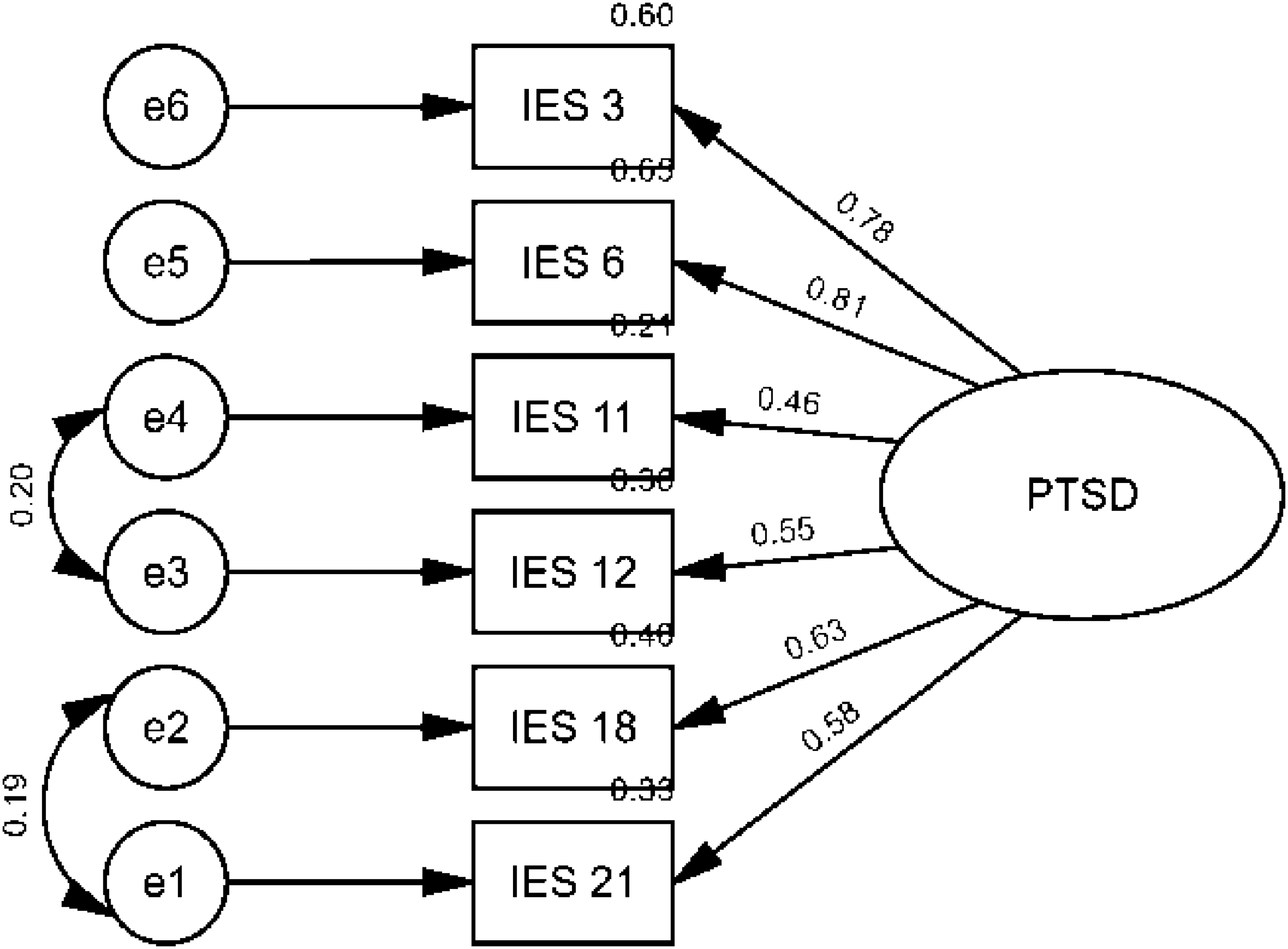
One-factor confirmatory factor analysis (CFA) model for the Impact of Event Scale-6 (IES-6) with two correlated residuals. Note. Standardized solution for the final one-factor IES-6 CFA model (N = 893), including correlated residuals between I11–I12 and I18–I21 to account for localized item-content overlap. Standardized factor loadings are shown on single-headed arrows.
Confirmatory Factor Analysis Results for the IES-6.

Note. Models were estimated in AMOS using maximum likelihood. The final one-factor model freely estimated correlated residuals for I11–I12 and I18–I21. These residual covariances reflect localized item-content overlap and should be considered when interpreting the model as evidence for total-score use. An ordinal CFA sensitivity analysis using WLSMV in R/lavaan is reported in the CFA Results subsection. CFA, confirmatory factor analysis; IES-6, Impact of Event Scale-6.
The fit of the retained model was acceptable by most approximate fit indices, χ2(7) = 34.41, p < .001, CFI = .983, TLI = .964, RMSEA = .066, 90% CI [.045, .089], and SRMR = .028; however, the Bollen–Stine bootstrap test of exact fit was significant (p = .001; 5,000 resamples). Standardized factor loadings were all positive and statistically significant, ranging from .46 to .81 (I3 = .78; I6 = .81; I11 = .46; I12 = .55; I18 = .63; I21 = .58), supporting the interpretation of the IES-6 as a coherent global index of trauma-related distress in this intake sample, while acknowledging localized residual dependence among two item pairs.
To address the ordered categorical response format of the IES-6 items, an ordinal CFA sensitivity analysis was conducted using WLSMV in R/lavaan (R Core Team, 2025; Rosseel, 2012), with the six IES-6 items treated as ordered categorical indicators. The model without correlated residuals showed mixed fit, scaled χ2(9) = 122.89, p < .001, CFI = .966, TLI = .943, RMSEA = .119, 90% CI [.101, .138], SRMR = .045. After allowing the same two theoretically interpretable residual covariances used in the AMOS model (I11–I12 and I18–I21), fit improved substantially, scaled χ2(7) = 49.84, p < .001, CFI = .987, TLI = .973, RMSEA = .083, 90% CI [.062, .105], SRMR = .029. Standardized factor loadings were positive and statistically significant, ranging from .50 to .83. These findings were broadly consistent with the AMOS ML results, although RMSEA remained somewhat elevated in the ordinal model. Thus, the sensitivity analysis supports cautious interpretation of the IES-6 as a brief global indicator of trauma-related distress while reinforcing the need to avoid claims of strict or perfectly fitting unidimensional measurement.
Measurement Invariance Across Gender
Multigroup CFA evaluated the measurement invariance of the IES-6 across men and women (Table 4). The configural model demonstrated acceptable fit, supporting a comparable pattern of fixed and free parameters across groups. Constraining factor loadings to equality (metric invariance) produced minimal change in fit relative to the configural model (ΔCFI = −.006; ΔRMSEA = −.001), supporting metric invariance and indicating that associations involving IES-6 scores can be compared across gender. Thus, the IES-6 appears to measure the same underlying construct in men and women at the level required for comparing associations (e.g., correlations, predictors, regression paths).
Measurement Invariance Across Gender for the IES-6.
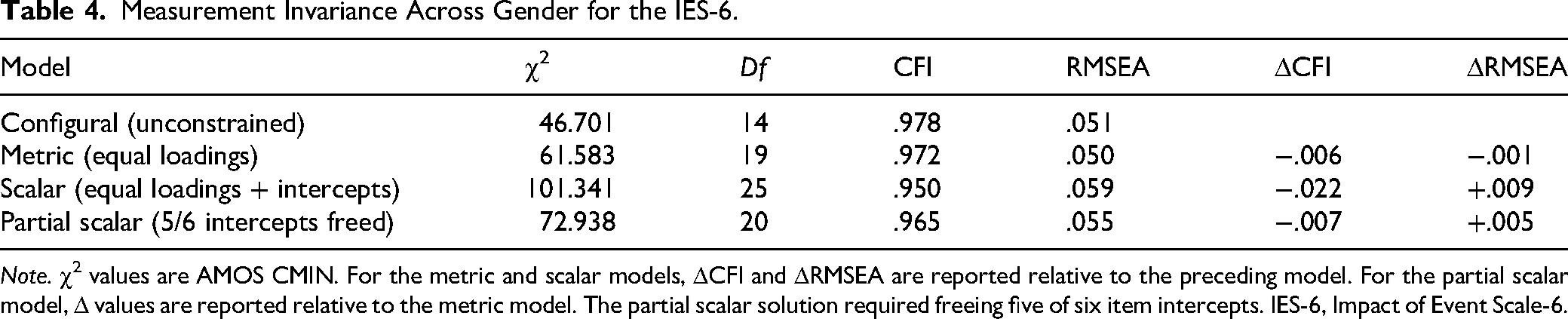
Note. χ2 values are AMOS CMIN. For the metric and scalar models, ΔCFI and ΔRMSEA are reported relative to the preceding model. For the partial scalar model, Δ values are reported relative to the metric model. The partial scalar solution required freeing five of six item intercepts. IES-6, Impact of Event Scale-6.
When item intercepts were additionally constrained (full scalar invariance), model fit worsened relative to the metric model (ΔCFI = −.022; ΔRMSEA = +.009), indicating that full scalar invariance was not supported. A partial scalar model improved fit relative to the full scalar model (CFI .950 → .965; RMSEA .059 → .055), but this improvement was achieved only by freeing five of six intercept constraints based on modification indices—leaving only one intercept invariant across gender and indicating substantial intercept noninvariance. Relative to the metric baseline, the partial scalar model showed only a small decrement in approximate fit (ΔCFI = −.007; ΔRMSEA = +.005), but the extent of freed intercepts suggests that scalar invariance was largely unsupported in practice. Accordingly, gender comparisons of associations are supported, whereas gender-based mean comparisons were treated as descriptive only because observed mean differences may reflect intercept nonequivalence rather than differences in the underlying construct. Consistent with the descriptive findings reported in Table 2, women had higher observed IES-6 total scores than men (t(891) = −6.08, p < .001; d = −0.41), but this difference should not be interpreted as a latent mean difference given the limited support for intercept invariance. In short, observed gender mean differences are reported for descriptive purposes, whereas gender comparisons of relationships involving IES-6 scores are psychometrically more defensible.
Validity Evidence
Parent-Measure Correspondence and Convergent Validity
As evidence of correspondence with the parent measure, the IES-6 total score was highly correlated with the full IES-R total score, r(891) = .932, 95% CI [.923, .940], p < .001 (N = 893). This is consistent with the IES-6 closely reproducing the overall scoring patterns of the full scale in this sample, noting that this strong association is expected because the IES-6 items are drawn directly from the IES-R. In addition, the IES-6 demonstrated moderate positive associations with general distress on the DASS-21, including depression, r(891) = .507, 95% CI [.457, .554], p < .001, anxiety, r(891) = .550, 95% CI [.503, .594], p < .001, and stress, r(891) = .541, 95% CI [.493, .586], p < .001, providing convergent validity evidence using external distress indicators.
Known-Groups Validity: Partner Status
Partner status (partnered vs. not partnered) was used as a known-groups indicator, operationalized by collapsing the original marital status variable into two categories. Participants who were not partnered reported significantly higher IES-6 scores (M = 16.24, SD = 5.19, n = 524) than those who were partnered (M = 14.85, SD = 5.64, n = 227), t(749) = −3.28, p = .001. Framed as not partnered minus partnered, the mean difference was 1.39, 95% CI [0.56, 2.22]. The effect size was small (Cohen's d = 0.26, 95% CI [0.11, 0.42]), indicating modest group separation; partner status provides only a broad grouping and does not directly index perceived support or relationship quality.
To examine whether this partner-status difference varied by gender, we conducted an exploratory 2 × 2 ANOVA (Gender × Partner Status) predicting IES-6 total scores in cases with available partner-status data (analytic N = 751). The interaction was not significant, F(1, 747) = 0.04, p = .843, partial η2 < .001, 95% CI [.000, .005], indicating that the association between partner status and IES-6 scores did not differ meaningfully between men and women.
Discussion and Applications to Practice
This study evaluated the psychometric performance of the IES-6 in a large intake sample of adult survivors of sexual violence receiving community-based services. Overall, findings provide preliminary support for the IES-6 as a brief global indicator of trauma-related distress for routine intake screening in this setting, with potential relevance for practice-based monitoring pending future evidence of longitudinal responsiveness. At the same time, the findings identify important interpretive limits related to localized residual dependence, ordinal item response categories, and incomplete scalar invariance across gender. The retained one-factor CFA model showed acceptable approximate fit and coherent standardized loadings, consistent with the intended interpretation of the IES-6 as a brief total-score measure of trauma-related distress (Thoresen et al., 2010). At the same time, two correlated residuals were included in the final model, likely reflecting localized overlap in item wording or content within this ultra-brief instrument. This does not undermine the practical value of the total score but it does qualify the strength of any claim that the IES-6 is strictly or cleanly unidimensional. Taken together, the overall pattern of evidence—meaningful loadings across all items, good internal consistency, and adequate item discrimination—supports cautious total-score use for intake screening and potential practice-based monitoring, provided that the score is interpreted as a brief global distress indicator rather than as evidence of a perfectly unidimensional construct.
The Bollen–Stine bootstrap test was significant despite acceptable approximate fit indices. In large samples, especially those involving ordered Likert-type symptom items and non-normal distributions, exact-fit tests are often sensitive to small deviations from the model (Hu & Bentler, 1999; Kline, 2016). For that reason, model evaluation is better guided by the overall pattern of approximate fit, parameter estimates, and substantive interpretability than by any single fit statistic. Importantly, the ordinal CFA sensitivity analysis produced broadly similar conclusions when the six IES-6 items were treated as ordered categorical indicators. The model with the two theoretically interpretable residual covariances showed strong CFI, TLI, and SRMR values, although RMSEA remained somewhat elevated. Taken together, these findings strengthen confidence that the IES-6 can be interpreted as a brief global indicator of trauma-related distress in this intake sample, while still requiring caution because of localized residual dependence and the limits of cross-sectional data.
The validity findings were broadly consistent with theory and clinical expectations. The IES-6 scores were moderately associated with DASS-21 Depression, Anxiety, and Stress scores, supporting convergent validity while also indicating that the IES-6 is not merely a duplicate of general distress measures. This pattern is consistent with prior IES-6 research showing expected convergence with related internalizing constructs, including anxiety and depression indicators in both clinical and population-based samples (Hosey et al., 2019; Jeong et al., 2022). The IES-6 also showed a very strong correlation with the full IES-R total score, indicating that the abbreviated form retains substantial information from the parent measure. This is practically important in routine-care settings, where longer measures may increase respondent burden and contribute to missingness.
Known-groups evidence based on partner status provided modest but clinically interpretable support. Participants who were not partnered reported somewhat higher IES-6 scores than those who were partnered, although the effect size was small. Because partner status is a coarse subgroup indicator derived from marital status and does not directly measure perceived support, relationship quality, or disclosure responses, this finding should not be interpreted as a direct test of social support mechanisms. Still, the direction of the effect is consistent with broader literature linking lower social support to greater posttraumatic stress symptom severity (Ozer et al., 2003; Tirone et al., 2021; Wang et al., 2021). Exploratory moderation analyses further suggested that this pattern did not differ meaningfully across men and women.
Measurement invariance testing adds an important interpretive boundary for mixed-gender service samples. Metric invariance was supported across men and women, suggesting that the IES-6 items relate to the latent construct in broadly similar ways across groups. This supports comparisons of associations involving IES-6 scores across gender, such as correlational patterns or regression coefficients. In contrast, scalar invariance was not supported, and partial scalar invariance required freeing five of the six intercepts. Substantively, this indicates considerable intercept noninvariance across gender and limits confidence in straightforward mean-level comparisons.
Women in this sample reported higher observed IES-6 scores than men, and that direction is broadly consistent with literature documenting higher average PTSD symptom burden among women in many trauma-exposed populations (Tolin & Foa, 2006). However, because scalar invariance was not supported, these observed score differences should not be interpreted as clear evidence of latent gender differences in trauma-related distress. More cautiously, the findings suggest that men and women may not endorse observed IES-6 scores in fully equivalent ways at the same underlying level of distress. For practice, this means that agencies should be careful about interpreting cross-gender mean differences or applying a single gender-blind threshold in high-stakes ways. The more defensible psychometric uses of the IES-6 in this study are total-score interpretation within groups, comparison of associations across gender, and repeated within-person use over time, pending direct longitudinal validation.
A contemporary concern is whether an IES-based measure remains meaningful in the DSM-5 era. Because the IES-R item pool was developed prior to DSM-5 and emphasizes intrusion, avoidance, and hyperarousal, the IES-6 should be framed as a brief indicator of trauma-related distress severity rather than as a DSM-5 diagnostic proxy. At the same time, community services often need short, feasible instruments that can be administered efficiently during intake and incorporated into routine workflows. From that perspective, the continued use of the IES-6 can still be justified when its score meaning is evaluated empirically in the population and context where it is being used. The present findings support that a narrower but important practice function.
For social work and community trauma services, the IES-6 appears to be a practical low-burden measure for documenting trauma-related distress at intake. Its brevity is especially relevant in sexual violence service settings, where clients may present in acute distress and lengthy assessment batteries may increase fatigue or nonresponse. Used appropriately, the IES-6 can support early care planning, baseline documentation, and identification of clients who may benefit from more comprehensive assessment.
The findings suggest a reasonable role for the IES-6 within practice-based assessment and stepped-care workflows as a low-burden intake screening and baseline documentation tool, with possible value for repeated practice-based monitoring if future longitudinal evidence supports its responsiveness to change. Agencies may use the IES-6 as a frontline screening tool or baseline severity indicator, while reserving more resource-intensive instruments, such as the PCL-5 or CAPS-5, for cases in which symptoms appear more severe, clinically complex, or diagnostically ambiguous. In that sense, the IES-6 may help improve efficiency while reducing burden in high-volume service settings. However, because longitudinal responsiveness was not directly tested, the present findings should be interpreted as supporting the IES-6's potential monitoring value rather than establishing it as a fully validated repeated-monitoring measure.
Interpretation should also reflect the invariance findings. Metric invariance supports comparing relationships involving IES-6 scores across men and women, but the lack of scalar invariance means that observed gender mean differences should be treated as descriptive rather than as evidence of latent differences in trauma-related distress. For program reporting, a defensible approach would be to emphasize within-group patterns and, when longitudinal data are available, within-person change over time rather than strong conclusions based on cross-gender mean comparisons alone. The modest partner-status difference also highlights that relational context may matter clinically, but partner status should be treated only as a broad intake flag rather than as a substitute for direct assessment of social support or relationship quality.
Finally, agencies should communicate clear interpretive boundaries. The IES-6 is best viewed as a brief severity indicator for screening and practice-based assessment, not as a stand-alone DSM-5 diagnostic tool. When diagnostic clarification is needed, it should function as a prompt for more comprehensive trauma assessment rather than as a replacement for it.
Several limitations should be noted. First, the study relied on routine-care archival data from a single regional service network, which may limit generalizability to other jurisdictions, service systems, or survivor populations. Second, some sociodemographic variables showed substantial missingness, particularly annual income, which was unavailable for women in the administrative dataset. This limited socioeconomic characterization and precluded meaningful gender-stratified analyses involving income. Third, the primary CFA models were estimated in AMOS using ML and therefore treated the 0–4 IES-6 symptom items as approximately continuous. To address this issue, an ordinal CFA sensitivity analysis was conducted using WLSMV in R/lavaan (R Core Team, 2025; Rosseel, 2012), which treated the IES-6 items as ordered categorical indicators. This sensitivity analysis produced broadly similar conclusions, particularly for the model including the two theoretically interpretable residual covariances, although RMSEA remained somewhat elevated. Future studies should continue to evaluate the IES-6 using ordinal estimators, larger and more diverse samples, and longitudinal designs that can test responsiveness to change. Fourth, invariance testing was limited to men and women as recorded in the administrative data. The findings therefore should not be generalized to transgender, nonbinary, or other gender-diverse individuals, and future research should incorporate more inclusive, self-identified gender measures. Additional work is also needed to examine the IES-6 across more diverse cultural, racial, ethnic, and religious groups and to test longitudinal responsiveness directly before strong claims are made about repeated monitoring over time.
Taken together, the findings provide preliminary support for the IES-6 as a feasible brief indicator of trauma-related distress for routine intake screening in community-based sexual violence services. The measure showed an acceptable one-factor structure after allowing limited, theoretically plausible residual covariances, good internal consistency, and meaningful associations with broader distress indicators, while also showing important limits in strict unidimensional interpretation and cross-gender mean comparability. In practice, the IES-6 appears well suited to low-burden intake assessment and baseline severity documentation and may have value in broader routine outcome workflows. However, further longitudinal research is needed before responsiveness to change and repeated-monitoring utility can be considered established. More broadly, this study helps address a practice-relevant gap by evaluating a brief trauma measure in a sexual violence service context where feasibility and psychometric defensibility must be considered together.
Footnotes
Acknowledgments
The data used in this study were originally collected by the Sexual Assault Crisis Centre of Essex County (Windsor, Ontario). The authors used ChatGPT (OpenAI) to assist with English-language editing, clarity, and organization. No AI tool was used to generate data, conduct statistical analyses, produce results, or draw conclusions. All final content, interpretations, and decisions were reviewed and approved by the authors.
Ethical Considerations
Approved by the University of Windsor Research Ethics Board (# 12-080).
Consent to Participate
The present study involved secondary analysis of de-identified archival data. Informed consent for participation in this secondary analysis was not required.
Consent for Publication
Not applicable. No individual-level data requiring publication consent were included.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Canadian Institutes of Health Research (CIHR; #392373) and the Social Sciences and Humanities Research Council (SSHRC; #892-2023-3003 and #890-2024-0022).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not publicly available due to REB-approved ethical restrictions.