
Abstract
Domestic violence (DV) is a significant public health concern. Globally, the World Health Organization (WHO, 2021) estimates that one in four (26%), ever-married/partnered women aged 15 years and older have experienced physical and/or sexual intimate partner violence in their lifetime. DV is identified as a crisis in many countries, including the present study jurisdiction, Australia, where DV affects one in four women (Australian Institute of Health and Welfare [AIHW], 2019).
Australia has experienced increased attention and investment into DV responses at both national and state levels in recent years (see, for example, the Victorian Royal Commission into Family Violence [RCFV, 2016] and the development of the National Plan to End Violence against Women and Children 2022–2032). This has included increased funding for perpetrator interventions such as Men's Behavior Change Programs (MBCPs). There is also a focus on increasing the diversity of programs to ensure tailored programs to address the needs of individual perpetrators are available, including combined programs that target problematic alcohol and other drug (AOD) use alongside DV perpetration (Australia's National Research Organisation for Women's Safety [ANROWS], 2021; Karakurt et al., 2019; Langenderfer, 2013; RCFV, 2016; Special Taskforce on Domestic and Family Violence Queensland, 2015).
This paper expands on a previously published outcome study (Meyer, Helps, et al., 2024). In this article, we present findings from a pilot, group-based intervention for men who are recent respondents on a DV protection order and present with comorbid problematic AOD use. The pilot program included family safety contact (FSC), a service provided in conjunction with an MBCP, also called partner contact. FSC involves an FSC worker attempting to contact an (ex)partner and/or other family member affected by the program participant's use of violence, and offering support and guidance, safety planning, onward referrals, and information about the program the man is participating in as appropriate.
FSC is a requirement under the minimum standards for MBCPs in the study jurisdiction (Family Safety Victoria, 2017) and provides an opportunity to assess program outcomes from the perspective of victim–survivors. Despite being viewed as best practice, studies examining victim–survivor contact within perpetrator programs are few (Chung, Anderson, et al., 2020; Hague & Mullender, 2006). Our findings draw primarily on interviews with victim–survivors (n = 10) supplemented with paired male program participant data where available (n = 9). The study sample is limited to heterosexual couples and one mother and son. Our findings highlight the importance of victim–survivor voices and engagement in MBCPs and related research. The findings contribute to a growing evidence base that demonstrates the necessity of contact between social workers with victim–survivors of family violence to cross-validate perpetrator reports of behavior change and enhance support options.
Background
Prioritizing Women's Voices in Evaluating MBCPs
It is increasingly recognized that responses to DV need to reorient toward those who use violence, to shift responsibility away from victim–survivors and increase perpetrator visibility and accountability (Chung, Upton-Davis, et al., 2020; Mackay et al., 2015a, 2015b). The focus on perpetrators is essential to prioritizing the safety of women and children (Chung, Upton-Davis, et al., 2020; Pence & Paymar, 1993; Westmarland & Kelly, 2013). This is often operationalized through MBCPs, including increasingly, tailored interventions addressing, for example, comorbid problematic AOD use and use of DV.
Globally, ∼7% of the population aged 14 and above live with alcohol use disorders and 3.7% of the adult population live with alcohol dependence (WHO, 2024). Alcohol consumption contributed to 2.6 million deaths in 2019 (4.7% of all deaths) and many more poor health outcomes (WHO, 2024). The disease burden from alcohol is highest among men (WHO, 2024). Research by the AIHW (2020) shows a high prevalence of drinking in Australia, with 76.6% of people aged 14 and over classified as recent drinkers (defined as consuming alcohol in the previous 12 months). Of those, approximately one in seven men (13.5%) and one in 16 women (6.3%) were considered likely to meet the criteria for alcohol dependence. With regard to illicit substances, the AIHW (2020) found that ∼43.0% of people aged 14 and over had used illicit substances in their lifetime, with 16.4% having used them in the previous 12 months.
While alcohol is not causal of DV, there is an association, with DV incidents often more severe and more likely to result in injury where problematic AOD use is also a factor (Graham et al., 2011; Thomas et al., 2013). Integrated AOD and DV treatment models are rare (Langenderfer, 2013; Meyer et al., 2020; Thomas & Bennett, 2009); however, existing studies demonstrate some positive results (Thomas & Bennett, 2009), including for example, increased motivation to change, compliance with treatment, and reduced anger and consumption of alcohol (Easton & Sinha, 2002). While promising, greater evidence into combined treatment models is needed (Langenderfer, 2013; RCFV, 2016; Special Taskforce on Domestic and Family Violence Queensland, 2015).
Evidence surrounding the effectiveness of MBCPs is somewhat mixed (Bell & Coates, 2022; Karakurt et al., 2019; Langenderfer, 2013). There are many barriers to meaningfully assessing outcomes from perpetrator interventions, including high attrition rates, small sample sizes, the inability to randomly assign participants, and the lack of equivalent control groups. While gold-standard program evaluations would utilize experimental or quasi-experimental design with a randomized control group (cf. Cheng et al., 2021), this is difficult to achieve in the context of DV perpetrator interventions as an untreated control group could pose a greater ongoing risk to victim–survivors (Vlais & Green, 2018).
The mixed evidence base is also associated with variations in the data sources utilized (Akoensi et al., 2013; Cheng et al., 2021). For example, differences in reporting of DV behaviors between victim–survivors and perpetrator self-reports are common (Freeman et al., 2015; Vall et al., 2021), and where victim–survivor accounts are utilized, outcomes are less encouraging compared to studies based solely on perpetrator self-reports (Langenderfer, 2013; McLaren et al., 2020). Differences in reports of substance use between program participants and victim–survivors have also been reported in previous studies (Ting et al., 2009). There are also reported differences in how the use of violence is understood, particularly where alcohol is involved. For example, Gilchrist et al. (2019) found that while both victim–survivors and perpetrators linked intoxication to violent behavior, there were differences in how this was reported. Victim–survivors explained their (ex)partner's/other family members’ violent behavior while intoxicated as linked to a pattern of power and control, while perpetrators were more likely to blame their behavior on intoxication. Divergent reports from victim–survivors and perpetrators are significant and highlight the need to draw on data beyond perpetrator self-reports when evaluating interventions.
Victim–survivor accounts are pivotal to understanding perpetrators’ use of DV and validating reports of change (Day et al., 2019; Westwood et al., 2020; McGinn et al., 2016; Vall et al., 2023). Engaging victim–survivors also provides an opportunity to assess and manage individual and family safety concerns, ensure victim–survivors are informed about program content and men's engagement, and facilitate support and referral pathways for victim–survivors where appropriate (Day et al., 2019). FSC can also validate victim–survivor experiences of DV (Kelly & Westmarland, 2015; Smith et al., 2013). Research has found validation from contact workers, and their presence as a “safety net” to be associated with increased confidence in holding perpetrators accountable and calling out their use of violence (Howard & Wright, 2008, p. 23; Smith et al., 2013; Westmarland & Kelly, 2013, p. 1101). While this is a positive and empowering outcome for women, taking an assertive stance may also increase risk of reprisal (Smith et al., 2013). Victim–survivor perspectives are a critical component of meaningful evaluations and should be a central part of DV program development rather than an add-on (McGinn et al., 2019). The nature and extent of FSC in practice vary.
Approaches to FSC
While FSC presents a valuable accountability tool, with victim–survivor accounts utilized to (in)validate men's self-reports of behavior change (McGinn et al., 2019), previous research by McGinn et al. (2019) has found that victim–survivors may experience that their own support and information needs remain unmet where FSC is primarily focused on validating men's accounts of behavior change during program participation (cf. Smith et al., 2013). The nature and extent of FSC are inconsistent and, in some cases, have been found to only occur as routine practice where a “physical safety issue” is perceived (Day et al., 2019, p. 67; Smith et al., 2013). FSC can create an opportunity for victim–survivors to reflect on their relationship and what they want for the future (Kelly & Westmarland, 2015; McGinn et al., 2019). However, victim–survivors may experience FSC as negative or invasive where focused primarily on assessing safety without attempting to understand what victim–survivors wanted or needed from the contact (Day et al., 2019; Smith et al., 2013).
Method
This paper is a process evaluation of a previously published outcome study, and it draws on findings from a review of a pilot program (U-Turn) undertaken in 2019–2021 (Meyer, McGowan, et al., 2021; Meyer, Helps, et al., 2024). The review was a mixed method with concurrent triangulation design and it utilized both quantitative and qualitative data collected from program participants and victim–survivors at four time points: program intake, program exit, 6-month follow-up, and 14-month follow-up. For the present study, we focus on qualitative interview data collected from victim–survivors, supplemented with paired program participant data where available. This focus allows us to explore the nuances of victim–survivors’ reports of men's DV and AOD use and their experiences engaging with FSC throughout men's program participation.
The U-Turn Program
U-Turn is a 12-week group-based program (with an additional three orientation weeks) for men who are recent respondents on a protection order and present with comorbid DV and problematic AOD use. The program is a small, single-site intervention developed in partnership between the AOD service provider and a local Magistrates’ Court in Victoria, Australia. Participants are referred to the program via the Magistrates’ Court at the time of their protection order mention date. The program is intended as an “early intervention” aiming to prevent subsequent violence including breaches of protection orders. We note, however, that “early intervention” may not be an accurate description as victim–survivors have often experienced prolonged histories of DV by the time their victimization attracts police and/or court interventions. The program is informed by AOD harm minimization principles (Department of Health, 2017), feminist theory (Pence & Paymar, 1993), and a psychoeducational framework (Beck & Dozois, 2011; Dobson & Dozois, 2021) of behavior change. The pilot program was delivered to 35 participants across four groups.
During the U-Turn pilot, FSC was provided by a staff member separate to the U-Turn facilitation team in line with ethical guidelines (Family Safety Victoria, 2017). This contact is voluntary, ensuring victim–survivors have agency and autonomy over their engagement (Fitz-Gibbon et al., 2020; Tutty et al., 2011). To ensure continuity of care, only one FSC worker provided support where possible (and where victim–survivors requested ongoing contact). The nature and extent of FSC were client led and varied across victim–survivors from weekly to monthly contact and were conducted via text message and telephone.
Data Collection and Analysis
This paper draws on qualitative victim–survivor and program participant data collected at 6- and 14-month follow-ups after intervention. As a requirement of the program, participants provided contact details of their (ex)partners/other family members affected by their use of violence to the service provider. The number of victim–survivors identified through this process is unknown. The FSC workers contact each identified victim–survivor as part of their normal practice; it was at this point of contact that the workers informed victim–survivors of the study. No interviews were conducted with victim–survivors who chose not to engage in FSC. Eighteen victim–survivors consented to have their details shared with the research team, 14 victim–survivors (77.8%) consented to participate in the study, nine victim–survivors (64.3%) participated in the 6-month follow-up interview, and three victim–survivors (33.3%) participated in the 14-month follow-up interview. The rate for victim–survivors at 14-month follow-up is calculated out of the nine women who are associated with the men who participated in U-Turn Groups 1 and 2. Due to COVID-19-related lockdowns and program delays, Groups 3 and 4 had not reached their 14-month follow-up time point when data collection concluded. One of the victim–survivors who participated at the 14-month follow-up time point had not completed a 6-month follow-up interview, resulting in 10 victim–survivors (71.4%) participating in at least one stage of follow-up data collection.
Program participants were similarly recruited via the service provider. Participants were informed about the research during intake assessments, and where participants consented to be contacted for the research, contact details were shared with the research team. Thirty participants (85.7%) participated in the study, 16 participants (53.3%) completed a 6-month follow-up interview, and seven participants (36.8%) completed the 14-month follow-up interview. The rate for program participants at 14-month follow-up is calculated out of the 19 men who participated in U-Turn Groups 1 and 2. This paper is primarily concerned with victim–survivor accounts; we therefore only use paired men's data (n = 9) where available in relation to the 10 victim–survivors that are the focus of this paper.
Interviews with victim–survivors canvassed their feelings of safety and well-being (or lack thereof), whether/how things may have improved for themselves and their family since their (ex)partner/other family member's participation in the intervention, (ex)partner/other family member's AOD use, feedback on FSC, and hopes and expectations for the future. Interviews with men explored men's self-reports of change and their views on the intervention.
Qualitative data captured during the follow-up interviews were analyzed thematically using NVivo software. All authors contributed to the coding, with each transcript coded by two authors. Themes were identified using an inductive approach to analysis (Thomas, 2006). As such, while the coding framework was guided by the research aims and questions and relevant literature, the authors approached the analysis without preconceived hypotheses. For example, under the code “AOD behaviors,” second-level codes included “men's AOD behaviors as self-reported by U-Turn participants” and “men's AOD behaviors reported by victim–survivors.” Further codes at the third level included “current-ongoing use,” “recent past use,” and “historical from first use.” To acknowledge victim–survivors’ time and contribution to the research, participating women received an AUD$25 gift voucher at each stage of data collection. Pseudonyms are used throughout to maintain anonymity. This research received ethics approval from Monash University's Human Research Ethics Committee (Project ID 18864).
Participant Characteristics
In most cases (n = 9), victim–survivors were current or former intimate partners of the program participants. One victim–survivor was the mother of a program participant. Half the victim–survivors were born overseas (n = 5), and no one identified as Aboriginal and/or Torres Strait Islander. One victim–survivor identified as living with a disability. Five victim–survivors were married to the person named on the protection order, one was a current partner, one was a casual partner, two were separated, and one was a parent of the male program participant. Most victim–survivors were living separately from the male program participant (n = 7). Most victim–survivors had children (n = 9), and most identified that some or all their children were from the relationship with the male program participant (n = 7). Four victim–survivors were employed, one was unemployed, two were students, two had home duties, and one was a carer (for more details on the study methods, see Meyer, McGowan et al., 2021).
Results
Victim–Survivors Accounts of Men's Change
The analysis illustrates some alignment of victim–survivor and participant accounts, suggesting mutual agreement on some behavioral improvements, primarily related to communication. On others, findings show nuanced differences in victim–survivor and participant accounts, and in a small number of cases, paired data reveal disparate accounts, illustrating ongoing abuse, denial, and minimization. These categories are not exclusive. As shown in Table 1, of the nine victim–survivor program participant dyads, two reported improvements only with no ongoing concerns relating to the use of violence disclosed. While promising, this should be interpreted with caution as it is possible violence was ongoing and not disclosed to the researchers. Four dyads reported overall improvements with some differences in the perceptions of the significance of changes observed between victim–survivors and program participant accounts. Notably, in one of these cases, it was the interview with the paired program participant that revealed some ongoing minimization and denial of their use of violence. Two dyads reported overall improvements and ongoing abuse, denial, and minimization. In these two cases, victim–survivors attributed the “overall improvements” to having less contact. In both cases, victim–survivors noted ongoing abuse (for example, when communicating about childcare arrangements) while paired program participant data showed denial and minimization. This shows that improvements for victim–survivors may not reflect actual behavior change on the part of these program participants. The final dyad had no contact allowed and no contact reported and therefore data on ongoing violence were not available to cross-check with the program participant's accounts.
Victim–Survivors and Program Participants Accounts of Men's Change.
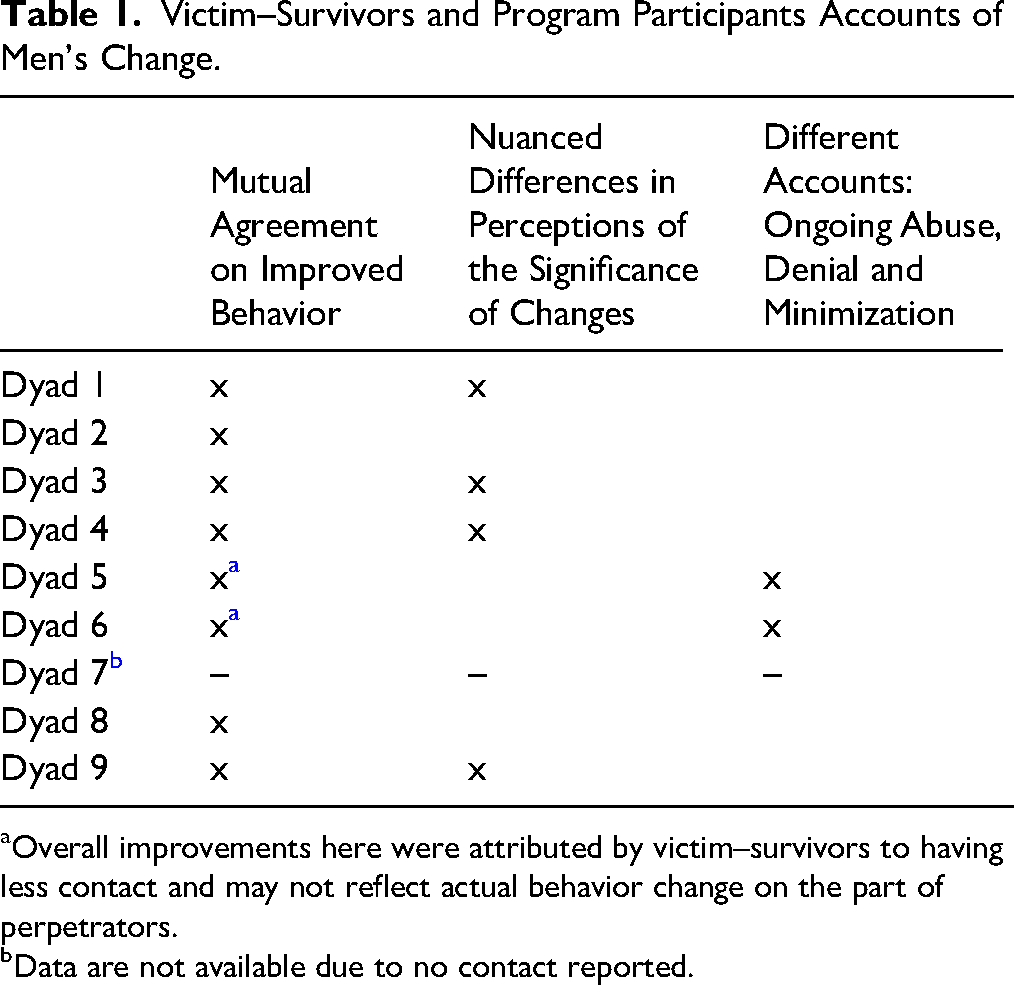
Overall improvements here were attributed by victim–survivors to having less contact and may not reflect actual behavior change on the part of perpetrators.
Data are not available due to no contact reported.
Mutual Agreement on Improved Behavior
Paired program participant and victim–survivor data suggest men's increased awareness of some abusive behaviors, predominantly related to the use of conflict interruption techniques and improved communication skills, as highlighted for example by Eva and Dima and Molly and Gavin: He is much calmer and doesn’t react strongly to things anymore. He has started to think before he says or does things and there is now more understanding that he needs to show respect. There have been no abusive behaviors. (Eva, exit interview) I’ve learnt at the program how to defuse it […] how to control my emotions. […] I definitely use the tools that I got from the actual program. […] All the time. Every day. (Dima, 14-month follow-up) He sort of like sits there and thinks before he says something (Molly, 6-month follow-up) I think before I do things or I say things. (Gavin, 6-month follow-up)
Like Eva and Molly, most victim–survivors who reported improvements in men's behavior pointed to changes related to an improved ability to manage emotions and communicate more respectfully. Research by Morrison et al. (2021) identified emotional problems, such as difficulty communicating feelings, as a key barrier to behavioral change for men who use violence. It is significant in our study that victim–survivors reported their (ex)partner's/other family member's improved capacity to express themselves, to identify how they are feeling and to manage that without using violence. These accounts highlight the importance of the intervention component focused on emotional and behavioral self-regulation and the usefulness of techniques learnt. This finding, of improved capacity to manage anger and defuse the situation—referred to as interruption methods—has been reported in other studies (see, for example, McGinn et al., 2016; Gondolf, 2000).
Nuanced Differences in Perceptions of the Significance of Changes
Comparison of victim–survivor and participant data also revealed nuanced differences in perceptions of behavior change. These nuances highlight the tendency for men to emphasize the significance of their progress and achievements in terms of behavior change, with victim–survivors presenting greater hesitation around the extent or significance of change. This is evidenced in the examples below where men's reflections on their acquired capacity to avoid being abusive are celebrated by participants.
Darren and Leah's reflections indicate this type of discrepancy. Darren attributes his behavior solely to his drinking, for him stopping drinking has meant the cessation of abuse he perpetrated while under the influence of alcohol: What destroyed my relationship […] was the alcohol […] I had a very short fuse, my fuse – the slightest thing I would just run off abuse people, family violence, break things in the house, damage the house […] If I was intoxicated I’ll just say the F – like, things would go off the handle [… Now] I don’t crack it as much […] I’ll just go out and I’ll walk away. (Darren, exit interview) We went away […] My wife couldn’t believe it because I wasn’t at the pub getting drunk all the time […] things have been up and down, […] I was pretty shocking in my past with my drinking. I was, I was never physically violent, but I was verbally and in other ways I was. (Darren, 6-month follow-up) Things are going to take a little bit a while to be like […] 100% again, because I’ve got a pretty dark past with my alcohol abuse and things like that […] Things have come a long, long way. (Darren 14-month follow-up)
Darren recognizes that he still gets angry sometimes, but that he does not “crack it as much” and will just “walk away”. While Darren recognizes that things are not “100% again,” he suggests that what is required now is time, rather than identifying more work for him to do to maintain and continue his behavior change. Leah similarly reported that Darren has stopped drinking and, at the exit interview, reported that “he's a lot more patient […] he hasn’t been going off.” However, Leah's observations at the 14-month follow-up reveal a slight deviation from the way Darren reports on his behavior change. Responding to a question about whether previous improvements have been maintained, Leah commented: I suppose it's still maintained, but […] he can still get angry easily, and he’ll just do the same thing and just sort of walk away, […] It just seems like maybe he's been getting angry more often, but it's probably just because the situation has been different [due to COVID-19 lockdowns … being] together 24/7 […] because since COVID started [Darren] hasn’t had a full week's pay […] and because [support meetings] were canceled during COVID, so I think it was just all those things together that the pressure was on. (Leah 14-month follow-up)
While both Leah and Darren report behavioral improvements and an increased capacity to manage the potential for abuse by leaving the home, their framing of the behavior and of the work still to do varies slightly. The study jurisdiction was subject to long periods of lockdown and significant restrictions due to the COVID-19 pandemic and Leah attributes Darren “getting angry more often” to stresses associated with the impacts of restrictions including spending months in lockdown, loss of work, and an inability to access some supports that were canceled during lockdowns, not solely to AOD use (which has ceased). Both Darren and Leah report that he's stopped drinking; however, while Darren reports a cessation of abusive behaviors, Leah's comments indicate that anger issues remain and are becoming more frequent, suggesting that there is still more work to do.
A similar dynamic can be seen in the reflections of Dima and Eva. As highlighted in the previous section, there were points on which Dima and Eva's views on behavioral improvements aligned, but there were also instances where their views diverged: I still drink. I don't drink as much […] I try to avoid when, as I said, situations where I'm over the top and can't control my emotions because I know I'm a different person […]. I just controlling how much I drink, because I don't know - I don't think I'm going to stop drinking, I enjoy it. It just relaxes me (Dima, exit interview). It's up and down […] But we don’t have major fights like we used to. I’m just trying to defuse it straight away […] I’ve learnt at the program how to defuse it and […] how to control my emotions. […] It helped me a lot, this program. (Dima, 14-month follow-up)
Like Darren, Dima connects his abusive behaviors to his drinking. Dima admits to continued drinking but does not see this as a problem; instead, he focuses on his reduction in drinking alongside his ability to “defuse” situations and “control [his] emotions.” Emotional regulation techniques are presented as key to change. In contrast, Eva offers more reserved reflections, suggesting that there is more work for Dima to do both in terms of behavior change and AOD use: [His alcohol use] unfortunately hasn’t changed. Now he drinks every day but not as much. Before, he drank more but less often. Every day he finds an excuse to drink […] It's naive of me to think that someone can change completely but I hope he continues to change and increase his understanding and respect. I’d like him to continue doing these groups but it's not up to me. (Eva, exit interview)
While success in the context of MBPCs is often associated with the complete cessation of violent behavior (and measured through limited mechanisms such as no police callouts or physical violence; Westmarland & Kelly, 2013), Vlais and Green (2018) argue that it may be more realistic to model outcome expectations on incremental improvements, as is common in AOD interventions. Accounts of program participants and victim–survivors indicate some, incremental level of change among men, predominantly associated with conflict interruption techniques, and indicate some level of increased safety. Research has found that victim–survivors often report changes in these behaviors; however, evidence suggests that changes in belief systems—which are associated with a greater reduction in violence—are less common (McGinn et al., 2016). While the data presented here do not speak specifically to shifts in attitudes, it does highlight that there are limits in the reported improvements in men's behavior.
Different Accounts: Ongoing Abuse, Denial, and Minimization
While most victim–survivors reported an overall improvement in their experiences of DV, some victim–survivors (n = 2) reported continued abusive behaviors. It is noteworthy that both victim–survivors reporting ongoing abusive behaviors had separated from the man participating in the U-Turn program. The continued abuse involved the instrumentalization of friends and family, neighbors, or children to facilitate ongoing surveillance of the victim–survivor along with other controlling behaviors. For example: There is a two-year good behavior bond on him […] he's not allowed here, and he has adhered to that, as in he hasn’t physically been here, but he has still continued his controlling behaviors from afar […] he has been working his magic legally, et cetera, and using his financially controlling things still, as he has always done […] that hasn’t changed. (Marie, 6-month follow-up) Handover is meant to be 8:00pm on a Sunday night. They get dropped home at 10:30am, 1:00pm, 5:00pm, but for the whole year not once did they get home at 8:00pm and the day before the Sunday they both start school for the whole new year, here they rock home at quarter to ten at night. And I'm texting at 8:30 going, like, call [child's name] at 8:30 to say, ‘Where are you? Are you running late?’ […] And I hear [(ex)partner] in the background go, ‘Tell your mother I'll drop you home at midnight. Ha ha ha ha ha’. (Georgia, 6-month follow-up)
Both victim–survivors reporting ongoing abusive behaviors stated that the abusive behaviors had decreased overall because there was less contact. However, ongoing contact with abusive ex-partners due, for example, to prolonged family law matters including property settlements and shared parenting arrangements, offered an alternative platform for coercive control and other forms of abuse. This pattern has been noted in previous research on victim–survivors’ postseparation experiences (Meyer & Stambe, 2022; Douglas, 2018; Easteal et al., 2018). Continued use of violence by participants of perpetrator interventions in similar contexts has also previously been reported in other studies (see, for example, Cheng et al., 2021; Karakurt et al., 2019). Indeed, some studies have found that participation in perpetrator interventions exacerbates violence as perpetrators use the knowledge gained in the program in their abuse (McGinn et al., 2016). McGinn et al. (2016) have highlighted the limited capacity for interventions to confront perpetrators about the ongoing use of violence reported by victim–survivors as this may put victim–survivors at risk of reprisal and further abuse.
Notably, accounts between victim–survivors who reported ongoing abusive behaviors and accounts from ex-partners differed. For example, while Georgia articulated ongoing abuse, her ex-partner articulated some insight into his abusive behaviors and thus a cessation of such behaviors: I've adjusted the way that I communicate because I was being antagonistic in the way that I was communicating. I was trying to get a result from that. I was trying to create - I was trying to cause pain […] I was being an arsehole basically […] I've learnt from I suppose time and also from the U-Turn program is that it's just to be communicating in that way is counterproductive, it might make me feel better for that 20 minutes after I've sent the email but then I've got a lot of remorse after that. So for me it was just better to look at, okay, what's the objective that I'm - what's my objective from sending this email because we can only communicate via email […] I'd look at the email and say, okay, will this achieve my objective or is it just - am I just doing it to try and hurt her? So that's certainly from learnings from U-Turn and also a bit of time. You know, I've calmed down. (James, exit interview)
While the above quote suggests that Georgia's ex-partner has ceased certain abusive tactics, her accounts of his ongoing behavior suggest that he has shifted from being abusive in communication to being controlling through the manipulation of shared parenting arrangements. Like James, Marie's ex-partner Jonathan also articulates a greater awareness of his own behaviors: When I do have a moment, I do tend to explode, I would probably have to make a much greater effort to be more restrained. [The program has] made me much more aware of these things. (Jonathan, exit interview)
Despite this suggested increased awareness, Jonathan's reflections on behavior change suggest a denial of ongoing abusive behaviors. For example, when asked about breaches or allegations of breaches to the protection order, contact, and whether there have been any aggressive behaviors, Jonathan responds: I have had no contact with my wife for approximately 12 months […] I have taken instructions from my lawyer, and he has been most specific in this regard, that I am not to breach the AVO […] She has [attempted contact …] I’m not allowed to engage. So I am adhering to the terms of the AVO […] I have not seen my wife. I’ve had no contact with her. (Jonathan, 6-month follow-up)
Jonathan's responses suggest a preoccupation with the protection order requirements of no contact and a deflection in responding to questions about abusive behaviors by reiterating the no contact requirements. Similar inconsistencies of accounts between (ex)partners regarding the occurrence of violence have been reported in other studies (Freeman et al., 2015; Vall et al., 2021). This reiterates the importance of including victim–survivor voices in examinations of perpetrator interventions to overcome data limitations associated with men's self-reports (Langenderfer, 2013; Westwood et al., 2020).
This section highlights that while at times men's self-reported behavior change is corroborated, victim–survivors’ data are critical to validating such change and to identifying behaviors and attitudes that may require further work or that pose an ongoing risk to women and children's safety and well-being. In addition to drawing on victim–survivor information in practice and evaluative research to identify ongoing safety concerns for women and children and progress toward men's behavior change then, there is increasing recognition that engaging victim–survivors needs to offer support beyond a focus on safety concerns. The qualitative data collected through interviews with victim–survivors is critical for understanding victim–survivor experience with, and satisfaction with, FSC. It is these data to which we now turn.
FSC as a Means of Identifying Support Needs and Creating Relevant Referral Pathways
As discussed in the methodology, FSC was offered to all victim–survivors. In line with other literature (see, for example, McGinn et al., 2019), all victim–survivors who participated in the research spoke positively about their experiences. Collectively, victim–survivors spoke about a range of benefits of the FSC that highlight the importance of support beyond the narrow focus on safety. This included offering emotional support, providing an opportunity for victim–survivors to discuss their experiences, and being provided with support referrals as well as practical support, such as tools for managing communication with an abusive ex-partner: Fantastic. Unreal. Especially at the start. Can’t thank [FSC worker name] enough […] really handy tools that she gave me to use. And some references to look – like gaslighting […] and with her advice to make the emails just go to a box so you don’t actually see them. And when I’m in the right frame of mind – so that it wasn’t interrupting my work […] some really handy hints to move forward. (Georgia, exit interview)
While safety remains a core component of the FSC work, offering wider, more holistic support and advice that are tailored to the individual circumstances and needs of victim–survivors is critical (Madoc-Jones & Roscoe, 2010; Nnawulezi & Murphy, 2017). Specific recovery and self-care methods including strategies for automatically indexing emails from an ex-partner to a separate folder that allow victim–survivors to control when the emails are read were spoken about positively by victim–survivors. This support has positive impacts on women's continued feelings of safety and agency and reflects the critical role of others, such as FSC workers, who support and encourage women to “find security” (Westwood et al., 2020; Pain, 2012, p. 24).
Being Informed About Program Content
Another key benefit of the FSC work described by victim–survivors was being informed about the U-Turn program, including the content and objectives. U-Turn facilitators and FSC workers engaged in regular discussions of safety concerns and risk monitoring and management practices based on information emerging during group facilitation and/or FSC. The close interaction and information exchange as it relates to potential risk to clients and their families forms a critical aspect of perpetrator monitoring and risk management and follows good practice in MBCP delivery (Chung, Anderson, et al., 2020; Smith et al., 2013; Westwood et al., 2020). However, the connection between facilitators and FSC workers also allowed FSC workers to keep victim–survivors informed about the program. This is useful as different topics may trigger different emotions or resistance among program participants. Creating awareness for victim–survivors of weekly content allowed women, particularly those coresiding with program participants, to consider whether specific content may increase the risk of abusive behaviors or to be able to understand where conversations program participants may introduce into the home are coming from: She just explained everything, just made me feel better […] you don’t know what's going on on the other side […] For her to explain it and what the objective was and just to have someone to talk to […] it was just what it was about, what the program was about, because I didn’t really know much about it. So there was a bit of hope there. (Leah, exit interview) [FSC worker name] rang me regularly. She was brilliant, absolutely brilliant. There were times throughout the thing where I’d be having a rough day and it just would coincide with [name] giving me a call. If there were any hiccups along the way where I thought, ‘He's struggling with this particular part of it,’ I’d make a note of it and [name] would give me a call and she’d be like, “We might mention that to the coordinators there and see if they can pop something in the course about it.” […] It was good knowing that there was someone there that was going to give you a call and make sure everything was going smoothly and if I needed help, I could get it […] She was very careful not to breach any confidence but she also kept me updated in a way that made me feel like I was confident that the right things were being done, that he was turning up, that he was actually participating and that sort of stuff. (Ruth, exit interview)
The importance of providing victim–survivors with information about program content and objectives as well as providing reassurances has similarly been identified in previous research by McGinn et al. (2019). In their study, some victim–survivors expressed a desire for greater availability of FSC workers and greater access to support and debriefing and to be more involved in the process.
All participating victim–survivors provided positive feedback about their experience with FSC workers; however, some victim–survivors also expressed frustrations or dissatisfaction. This included reflections that FSC was not particularly useful in contexts where the relationship between the victim–survivor and their (ex)partner/other family member was dominated by financial abuse, property, and legal disputes, which impacted on feelings of safety and security and the lack of guidance available to navigate interrelated systems such as the family law system and experiences. One separated mother described how she had to rely on friends for information that she would have expected service providers to provide: It was girlfriends that said sign up to Child Support […] If someone hadn’t told me that I wouldn’t have gotten into that system and yeah, probably more about the steps to take Family Law wise and financially. (Georgia, exit interview)
It is noteworthy here that the same mother experienced other aspects of the FSC as very helpful in addressing safety concerns and managing the levels of distress caused by her partner's ongoing behavior (e.g., through carefully managing email communication with him). However, such feedback highlights the importance of FSC workers identifying support needs beyond immediate safety concerns to provide referrals to other support mechanisms, including legal advice.
Particularly, victim–survivors who were subject to ongoing coercive control, including financial and systems abuse, noted the limitations of FSC, as illustrated by Marie: Look, I've gone through that loop with [name of FSC worker …] and yeah, it doesn't achieve anything. I mean, yes, it's lovely to talk to somebody, but it doesn't actually – I have to just focus now on […] getting through this next stage. (Marie, 14-month follow-up)
For Marie, safety concerns were related to concerns around financial security and housing stability over the course of prolonged family law proceedings. Marie's experience is consistent with previous research on victim–survivors’ perceptions of justice, which found that women frequently correlate justice with safety and security (McGowan & Elliott, 2019; McCulloch et al., 2020). Research shows that victim–survivors’ short- and long-term support needs may vary over time (Meyer, 2014). As a result, FSC, like many other support mechanisms, has its limitations in situations where ongoing abuse and related safety concerns remain present beyond the conclusion of the related MBCP. Findings on FSC suggest that overall FSC is experienced as useful in women's empowerment and the development of immediate protective strategies. However, they also highlight the need for additional and at times long-term support for women who have ongoing contact with an abusive ex-partner, for example, due to shared care arrangements for mutual children and/or prolonged family law matters. These scenarios offer an ongoing platform for coercive control and other forms of abuse (Kaye et al., 2021; Meyer & Stambe, 2022; Douglas, 2018; Easteal et al., 2018). This can have lasting adverse effects on victim–survivors’ feelings of safety and security (for themselves and where applicable their children) and on their ability to commence the recovery process (Douglas, 2018; Kaye et al., 2021; Meyer & Stambe, 2022).
Limitations
Findings reported here are based on a pilot program, are limited to a small sample, and are not generalizable to the broader experiences of perpetrators and victim–survivors. Furthermore, our sample is predominantly heterosexual couples, with one mother and son. The exclusion of same-sex couples is a limitation. We note the need for greater provision of DV behavior change services for LGBTQ+ people who use violence in their relationships (Gray et al., 2020; McGowan et al., 2023; Worrell et al., 2024). The small victim–survivor sample is consistent with other research into FSC (Chung, Anderson, et al., 2020). Practitioners have reported a variety of barriers to FSC including difficulty in contacting victim–survivors and a reluctance to receive FSC even when initial contact was successfully made (Chung, Anderson, et al., 2020). Reasons victim–survivors choose not to engage with FSC can include, for example, a fear of being involved with services, feelings of stigma or shame and/or fears of child removal, and limited capacity given the emotional and administrative burden of managing their family life in the context of violence (Chung, Anderson, et al., 2020). Furthermore, the nature and quality of FSC did not form part of the study. As a result, we do not intend to draw links between the nature and extent of FSC, and victim–survivors’ experience reported here. Despite these limitations, findings provide insights into the critical role of FSC as part of MBCPs. Furthermore, the exploratory nature of this study allows us to explore variations in perpetrator and victim–survivor accounts of behavior change. In doing so, this study demonstrates the critical need for evaluation research to incorporate victim–survivor accounts in assessing program outcomes. Critically, evaluation research must also account for the substantial attrition of victim–survivors. To establish a more meaningful sample size, it is necessary to fund multiple intervention groups at the pilot stage.
Discussion and Applications to Practice
The current study presents findings relating to the benefits of FSC for victim–survivors whose (ex)partner or other family member is participating in a perpetrator intervention, including combined AOD and DV interventions. While study findings are limited to a small sample and need to be interpreted with caution, they are overall positive and point to the importance of social work practice that provides holistic approaches to addressing intersecting needs related to the use of DV and AOD (see also Meyer et al., 2024). Addressing both problems through combined interventions is critical given the increased risk of harm where problematic AOD use is a factor (Capezza et al., 2015; Meyer et al., 2020).
Most victim–survivors in our study validated men's self-reported behavior change at least to an extent. However, variations were observed in some program participant and victim–survivor accounts. Specifically, the nature and extent of change being experienced were described as more nuanced by victim–survivors than reported by program participants. Additionally, some victim–survivor and program participant self-reports diverged strongly, with men denying ongoing abusive behaviors, while victim–survivors reported ongoing experiences of abuse. Divergent accounts between victim–survivors and program participants highlight the critical nature of including victim–survivor feedback in MBCPs and related research to better understand the nature, extent, and context of behavior change or lack thereof. This has implications for both social work research and practice.
For social work practice, men's ongoing denial or minimization of use of violence highlights limitations to program participants’ acceptance of responsibility and accountability for their use of violence. This may suggest a need for greater tailoring of interventions to individual needs, addressing readiness or motivation to engage in behavioral change, or the need for longer behavioral change work than the program affords. As such, social work practice may benefit from trialing targeted engagement strategies that address clients’ needs (see, for example, Fitz-Gibbon et al., 2024). Relatedly, combined interventions may benefit from research methods that allow social work practitioners greater flexibility and adaptability to embed learning as they arise and to respond dynamically to additional identified client needs (such as developmental evaluations). Additionally, for social work research, given the critical perspective of victim–survivors, and that recruiting and maintaining large sample sizes are a common limitation of MBCP evaluations, there is a need for the provision of funding to social work research to support large evaluation studies of multiple intervention groups. Without this, meaningful victim–survivor sample sizes will continue to be a challenge.
Furthermore, findings highlight the critical nature of FSC beyond cross-referencing and (in)validating men's self-reported behavior change. FSC can empower and inform victim–survivors, support their safety planning, monitor ongoing risk, and create referral pathways to additional support mechanisms that may be required to address the short- and long-term effects of DV experienced by many women. Social work practice must recognize the critical role of FSC work and ensure it is adequately funded and built into MBCP service delivery.
Finally, our findings contribute to a growing body of scholarship that prioritizes the perspectives of victim–survivors in evaluating perpetrator interventions. Findings highlight the importance of FSC established as a core focus of the intervention rather than an add-on. This is critical to better meet the diverse and intersecting support needs of victim–survivors, including immediate safety planning, practical advice, and access to ongoing and holistic support for victim–survivors beyond their (ex)partners/other family members engagement with an MBCP provider.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Program evaluation funding was provided by Taskforce Community Agency.