
Abstract
Keywords
The co-occurrence of alcohol and drug use (AOD) misuse and domestic violence (DV) is well established in existing literature (Foran & O’Leary, 2008; Freeman et al., 2015; Gilchrist et al., 2019; Kraanen et al., 2010; Langenderfer, 2013; Thomas & Bennett, 2009; Thomas et al., 2013). Evidence of this link is demonstrated by higher rates of DV perpetration found among people engaged in AOD treatment programs (Freeman et al., 2015; Gilchrist et al., 2017; Stuart et al., 2009), as well as higher rates of AOD misuse among perpetrators engaged in DV interventions, such as Men's Behavior Change Programs (Kraanen et al., 2010; Stuart, 2005). While prevalence rates on the overlap of DV perpetration and problematic AOD use at a nationally representative level in Australia are unavailable, DV prevalence rates have been described as a national crisis (Our Watch, 2023), with one in six women experiencing DV (inclusive of coercive control, physical and/or sexual violence) by a current or former partner since the age of 15 (Australian Institute of Health and Welfare [AIHW], 2018). The equivalent prevalence rates for Australian men experiencing DV are one in 16 (AIHW, 2018). Global prevalence estimates of intimate partner violence (inclusive of physical and/or sexual violence) by a current or former partner are higher than those in Australia. The World Health Organization (WHO, 2021) estimates that the lifetime and past 12-month prevalence of physical and/or sexual violence (perpetrated at least once) for ever-married/partnered women between the ages of 20 and 44 by a current or former partner is 26% to 28% and 10% to 16%, respectively. While equivalent disaggregated global prevalence data on men is not available, previous research by WHO (2012) has noted the “overwhelming burden” of DV “is borne by women” and that men are more likely to have violence perpetrated against them by “strangers or acquaintances than by someone close to them” (p. 1).
The latest national survey on Australians’ AOD consumption revealed that among the 76.6% of people aged 14 and over considered recent drinkers (defined as those who had an alcoholic drink in the previous 12 months), 13.5% of men and 6.3% of women were likely to meet the criteria for alcohol dependence (AIHW, 2020, p. 22). In Australia in 2019, 43.0% (9 million) of people aged 14 and over had used illicit substances in their lifetime, and 16.4% (3.4 million) had used in the past 12 months (AIHW, 2020, p. 28). The WHO reports that the “harmful use of alcohol” is responsible for 7.1% of global burden of disease for males and 2.2% for females (WHO, 2023a). On the harmful use of psychoactive drugs, the WHO estimates that it accounts for the loss of 42 million years of healthy life or 1.3% of global disease burden (WHO, 2023b).
While there is clear evidence of an association between AOD misuse and DV, there is little evidence of a direct link (Graham et al., 2011). Instead, the relationship is dynamic and is subject to individual differences (Klostermann & Fals-Stewart, 2006; Radcliffe et al., 2021; Stuart et al., 2009). Regardless of the nature of the association between AOD misuse and DV, evidence consistently shows that where AOD is involved, incidents of DV are more severe and are more likely to result in injury (Graham et al., 2011; Lund, 2014; Our Watch, 2021; Thomas et al., 2013; Thompson & Kingree, 2006).
Recognizing the differences between AOD and non-AOD DV perpetrators is essential for aligning services and interventions with their specific needs (Thomas et al., 2013). Despite recognition of this, interventions often remain siloed (Wilson et al., 2014; Capezza et al., 2015). There are a number of reasons for siloed, “treatment as usual” approaches within AOD misuse interventions, including for example, that there is no standard process to assess or screen for DV, there is often a lack of staff training and knowledge, a shortage of time, and screening processes can be overwhelming for clients (Klostermann et al., 2010; Timko et al., 2012). Further, integration is hindered by views that combining AOD misuse and DV treatment programs would undermine the integrity of either treatment model (Chartas & Culbreth, 2001).
Coordinated interventions targeting comorbid DV and problematic AOD use remain rare (Langenderfer, 2013; Meyer et al., 2020; Thomas & Bennett, 2009), as are studies and evaluations of such programs. While not without limitations (see, e.g., Kraanen et al., 2013; Easton et al., 2007), existing studies examining combined interventions demonstrate some positive results (Thomas & Bennett, 2009). For example, combined interventions have been shown to have better attendance outcomes and lower rates of same-victim re-offending (Goldkamp et al., 1996), increased motivation to change, treatment compliance and reduction in anger and alcohol consumption (Easton & Sinha, 2002), as well as greater number of days abstinent from alcohol and greater reductions in their use of physical violence (Easton et al., 2007). While these findings are encouraging, the overall dearth of scholarship on combined AOD and DV interventions poses challenges for effective treatment as it results in limited understanding of the impact and role of these interventions in long-term behavior change.
Prior studies have stressed the need for greater research into combined programs that target problematic AOD use alongside DV perpetration (Langenderfer, 2013; Macy & Goodbourn, 2012). In Australia, this is also highlighted by government inquiries and research agendas acknowledging the need for service responses that better address the intersection of problematic AOD use and DV (Australia's National Research Organisation for Women's Safety [ANROWS], 2021; Special Taskforce on Domestic and Family Violence Queensland, 2015; State of Victoria, 2016). The purpose of the present study is to expand the currently limited evidence base on combined AOD and DV interventions via analysis of an Australian pilot program. In this paper we focus on a 12-week group-based intervention—the U-Turn program—for men who are recent respondents on a DV Intervention Order (DVIO) and present with problematic AOD use. The study incorporates data from 30 program participants and 14 victim-survivors, and our findings indicate the potential benefits of combined interventions at the intersection of DV and problematic AOD use. Results also highlight the ability of combined interventions to increase family safety and assist men in maintaining behavior change around the use of DV and problematic AOD use.
Method
Background
This research was conducted between February 2019 and April 2021 by researchers at the Monash Gender and Family Violence Prevention Centre. The research used a mixed-methods concurrent triangulation design in order to undertake a review of the U-Turn pilot program. The research was designed in close consultation with the program provider TaskForce Community Agency (hereafter referred to as TaskForce) to ensure it captured critical and meaningful outcome measures to inform future service delivery at the intersection of men's use of DV and problematic AOD use. The program provider received funding for program delivery and review. The study received ethics review board approval from Monash University's Human Research Ethics Committee (Project ID 18864).
Sample
There were two participant samples utilized in this study: male perpetrators participating in the U-Turn program and their victim-survivors. Over the course of the study, a total of 35 men were referred and assessed as eligible and group-ready to commence U-Turn. Of these, 30 men (85.7%) participated in the study. During intake assessments, TaskForce staff informed participants about the research and, where participants consented to be contacted for the research, TaskForce provided researchers with participant contact details. Female victim-survivors were recruited via the family safety contact worker. All program participants were required to provide contact details of their victim-survivors to TaskForce as a requirement of the program. It is not known how many victim-survivors were identified through these processes. The family safety contact worker(s) at TaskForce made contact with victim-survivors as part of their standard processes, and at this point the worker informed victim-survivors about the research. Where victim-survivors expressed an interest in participating, their contact details were shared with the researchers via the family safety contact worker. As victim-survivors were recruited into the study via the family safety contact worker, only those who responded to the family safety contact were eligible to participate. Eighteen victim-survivors consented to have their details shared with the research team and 14 female victim-survivors (77.8%) consented to participate in the study.
Participating men (n = 30) answered a series of demographic questions as part of the intake assessment. Half of the sample identified as Australian born (n = 15, 50.0%), with two of these men (6.7%) identifying as Aboriginal and/or Torres Strait Islander. The average age of the sample was 43.1 years old (standard deviation [SD] = 10.9). The majority of the sample was employed (n = 16, 53.3%) and living with other family members (n = 12, 40.0%). Over three-quarters of the sample (n = 23, 76.6%) had at least one child. Less than one-third of the sample reported being the primary caregiver of and/or living with their child(ren) (n = 7, 23.3%). Fourteen victim-survivors consented to participate in the study and were asked a series of demographic questions. This sample comprised of nine victim-survivors (64.3%) who reported being current partners of a U-Turn participant (including eight married or de facto partners and one casual dating partner), four victim-survivors (28.6%) who identified as separated ex-partners of a U-Turn participant, with one of these having resumed the relationship at the time of the 6-month postprogram follow-up wave of data collection, and one (7.1%) parent of a U-Turn participant (for an overview of data collection waves see Table 1). More than half of the sample (n = 8, 57.1%) reported being born overseas. None of the women identified as Aboriginal and/or Torres Strait Islander. Over one-third of women were employed (n = 5, 35.7%) and almost half had a trade certificate (n = 6, 42.9%). The majority of the sample reported having children (n = 13, 92.9%), with most women (n = 12, 85.7%) identifying that their children were from the relationship with the male program participant named as the alleged perpetrator of DV on their DVIO.
Response Rates for Each Wave of Data Collection
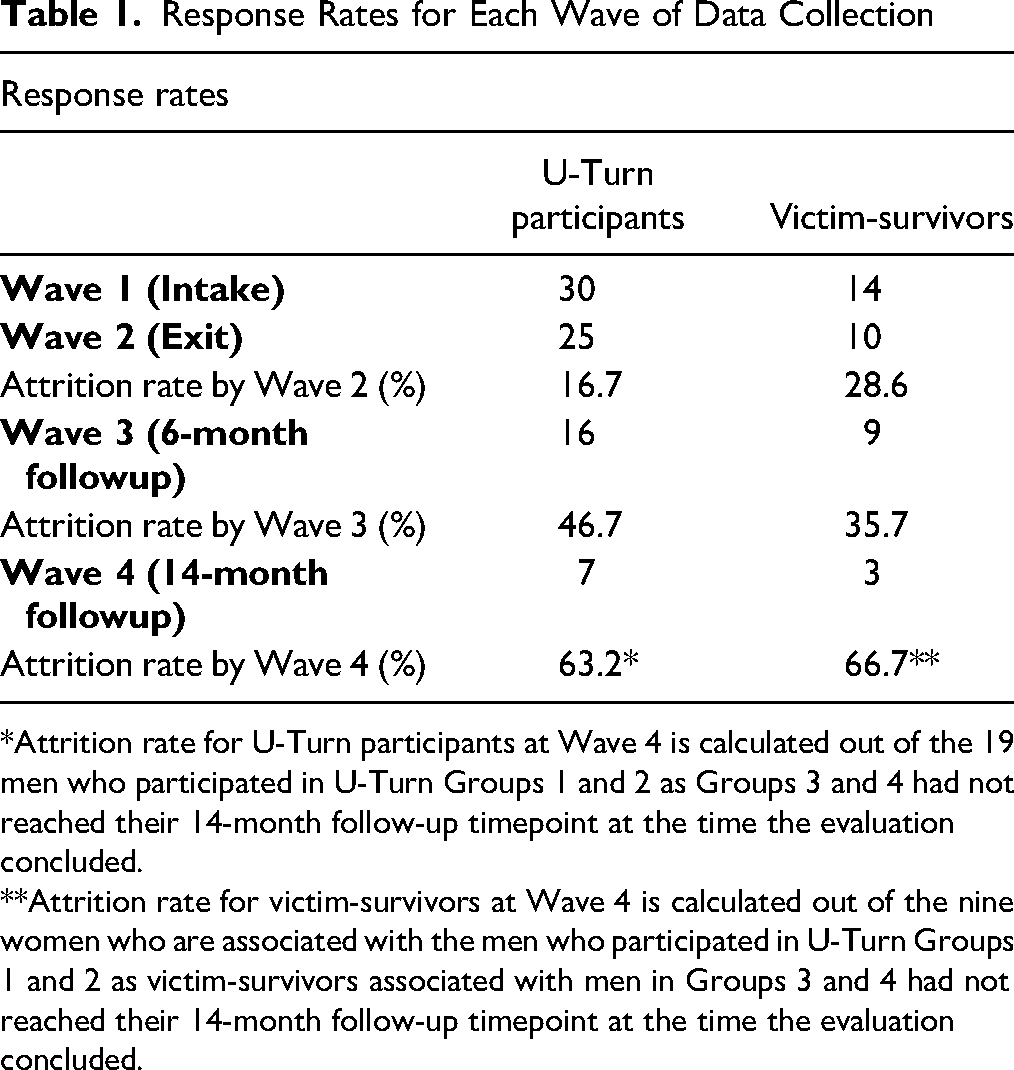
*Attrition rate for U-Turn participants at Wave 4 is calculated out of the 19 men who participated in U-Turn Groups 1 and 2 as Groups 3 and 4 had not reached their 14-month follow-up timepoint at the time the evaluation concluded.
**Attrition rate for victim-survivors at Wave 4 is calculated out of the nine women who are associated with the men who participated in U-Turn Groups 1 and 2 as victim-survivors associated with men in Groups 3 and 4 had not reached their 14-month follow-up timepoint at the time the evaluation concluded.
Intervention
Findings presented here are based on the U-Turn program; a local, single site Australian pilot program aimed at addressing the intersection between DV and problematic AOD use. The program was developed through a partnership between a local Magistrates’ Court and an AOD service provider for men who are alleged perpetrators and respondents on a DVIO. Program participants entered the program via referrals from the local Magistrates’ Court at the time of their DVIO mention date. TaskForce was funded to develop the 12-week group-based intervention and deliver it to four groups of up to 14 participants between February 2019 and October 2020.
The U-Turn program is framed as an “early intervention” due to the timing of the referral pathway during men's contact with the local court as part of the civil DVIO proceedings (and, where applicable, related criminal charges). The term “early intervention” however, may not be an accurate description of the victim-survivors’ perspective as victim-survivors have often experienced prolonged histories of DV by the time their victimization attracts police and/or court interventions. A key objective of the program is to keep men who have had minimal or no prior contact with the criminal justice system (CJS) out of the system. All referrals were assessed for risk and eligibility. It is not known how many men were referred by the Magistrates’ Court to the U-Turn program. Those who were not eligible to participate in the intervention group due to presenting risks and support needs deemed to be too complex for an early intervention were referred to more suitable programs or one-on-one counseling options. Those who were assessed as “group-ready” (n = 35) joined an orientation group prior to commence the 12-week group-based intervention. The purpose of the orientation group was to offer up to three sessions of general introduction to DV, their referral pathway, implications of nonattendance and opportunities for change. The orientation group acted as a “holding space” for men who were referred up to 4 weeks prior to group commencement to maintain current motivation to engage in the U-Turn program. Depending on the timing of the court referral, men may have attended between zero and three orientation sessions. All men attended the one-on-one intake assessment session to establish group eligibility and support needs. TaskForce report (see Meyer et al., 2021) that the U-Turn program is informed by AOD harm minimization principles (Department of Health, 2017), feminist theory (Pence & Paymar, 1993) and a psychoeducational framework (Beck & Dozois, 2011; Dobson & Dozois, 2021) of behavior change. While the development of program content draws on three key bodies of evidence-based practice (related to both DV and therapeutic AOD work), the content was newly developed for the pilot and was not validated or evidence-based. Topics covered in the 12-week intervention included harm reduction; the relationship between AOD and DV; the gendered nature of DV; the impacts of violence on women, children, and the community; respectful communication (including postseparation); emotional regulation; and basic legal education (with regard to understanding and complying with DVIOs, including any possible variations to the DVIO). The program was co-facilitated by a female AOD clinician and a male AOD clinician with additional MBCP facilitator qualification. The group met weekly for 90 min sessions. Both the orientation and 12-week program were conducted in-person and no sessions were audio or visually recorded. The minimum attendance requirement was 9 weeks (75.0%). Men who missed more than 3 weeks were exited from the program. Of the 35 men assessed as eligible to begin the program, 30 commenced the program (a preprogram attrition rate of 14.3% [n = 5]). Among men who started the program, 26 men (86.7%) completed the program. The majority of men (n = 17, 56.7%) attended all 12 sessions. The mean attendance rate was 11.38.
Measures
The study utilized a mixed-methods approach, following a concurrent triangulation design (Creswell et al., 2003) to examine program suitability and effectiveness. The study design reflects the absence of literature on combined interventions and their effectiveness. The concurrent collection of both quantitative and qualitative data, and the subsequent merging of results, can be effective in enabling researchers to understand an emerging research problem (Creswell & Plano Clark, 2007). This type of study design also compensates for the respective weaknesses of quantitative and qualitative methods (Creswell & Plano Clark, 2007). This study has a small sample size, and the findings are not generalizable.
Program participant and victim-survivor data were collected at four different timepoints:
Wave 1—men's intake Wave 2—program exit Wave 3—6-month postprogram followup Wave 4—14-month postprogram followup (not presented here)
Data sources included surveys and interviews with program participants and their victim-survivors. Victim-survivors completed scales from Project Mirabal (Kelly & Westmarland, 2015), at men's program intake (Wave 1) and exit (Wave 2), and interviews at men's exit (Wave 2), 6-month followup (Wave 3) and 14-month followup (Wave 4). Program participants completed interviews at program exit (Wave 2), 6-month followup (Wave 3) and 14-month followup (Wave 4). In addition to the primary data collection described above, the study included access to men's court records for the 12 months following their U-Turn referral for all four groups. Response rates to each wave of data collection are outlined in Table 1.
The broader program review captured a range of data sources from program participants and victim-survivors. This paper focuses primarily on victim-survivor reports of men's DV and AOD behaviors, collected through Project Mirabal scales and qualitative interviews, supplemented with program participants’ data. Additionally, as shown in Table 1, there was a high attrition rate by Wave 4 for both victim-survivors (n = 6, 66.7%) and program participants (n = 12, 63.2%) in pilot Groups 1 and 2 (noting that due to COVID-19-related delays, pilot Groups 3 and 4 had not reached the 14-month followup at the time this study concluded). Wave 4 data has therefore been excluded from the analysis presented in this paper.
Quantitative
Survey Data
Quantitative survey measures were used to gain insights into women's experiences of abuse at men's program intake (Wave 1) and exit (Wave 2). The study utilized measures from Project Mirabal (Kelly & Westmarland, 2015) that captured victim-survivors’ experiences of violence and abuse. Three measures were utilized: “Respectful Communication,” “Expanded Space for Action,” and “Safety and Freedom from Violence and Abuse” (Kelly & Westmarland, 2015). All measures utilized five-point Likert scales (1 = never to 5 = always). The “Respectful Communication” scale contained five-items related to victim-survivors’ experiences of respectful communication in their relationship with program participants (such as, whether their (ex)partner/other family member [perpetrator] listens to what they [victim-survivor] have to say). The “Expanded Space for Action” scale contained 12-items related to victim-survivors’ experiences of controlling and coercive behavior by program participants and captured behaviors such as social isolation, financial control, and sexual jealousy. Finally, the “Safety and Freedom from Violence and Abuse” scale contained 14-items, comprising seven questions related to victim-survivors’ experiences of nonphysical harassment and other abusive acts (such as verbal and emotional abuse and property damage) and seven questions related to experiences of physical and sexual violence (such as threats with a weapon). The Project Mirabal scales utilized in this study have been used in previous DV research (Kelly & Westmarland, 2015), but have not been tested for reliability and validity. Further evidence on the utility of these measures is required and as such, these findings should be interpreted cautiously. The research team conducted the surveys with consenting victim-survivors via the telephone at both timepoints (men's intake and exit). Victim-survivors’ demographic data was collected by the research team at the first timepoint (men's intake). Men's demographic data was collected at intake by the TaskForce staff as part of the program assessment forms. This was done in-person and where participants consented this was then shared with the research team.
Administrative Court Data
All 30 U-Turn participants who participated in the wider study gave consent for the research team to access their 12-month follow-up court data from the day of their initial DVIO mention date, which is where the U-Turn referral was made. The research team was able to obtain court data for 29 of the 30 male participants. The court was unable to retrieve court records for one participant as his name and contact details held by the program provider and research team did not yield any results in the court database. The purpose of the court data was to identify whether participants had subsequent court contact after being referred to the U-Turn program to determine if U-Turn achieved its aim of diverting alleged perpetrators of DV from the CJS. The court data was provided as an excel spreadsheet which outlined for each individual participant each of the following DV-related and other offending matters:
whether any criminal charges were associated with the initial DVIO matter; whether U-Turn participants returned to court for new DV matters (including breaches of the original DVIO as well as new civil or criminal DV matters against another partner or family member); and whether U-Turn participants appeared in court for other criminal matters (including AOD-related offending behavior as well as any other offending behavior) during the 12-month follow-up period.
Court data was descriptive only and did not require coding. The data was provided as a binary (presence or absence) of each matter listed above. No further information was provided, and the research team did not have access to raw court data files.
Qualitative
Interviews were conducted by the first and third authors, using a semistructured interview guide. Interviews were audio recorded and professionally transcribed. Interviews were conducted at program exit (Wave 2), with shorter interviews being conducted at 6-month and 14-month followups (Waves 3 and 4, respectively). The exit interviews were approximately 30 to 45 min long, with follow-up interviews running for 15 to 30 min. Qualitative interviews were an opportunity to understand changes to men's AOD use (as reported by victim-survivors and where victim-survivor data was unavailable self-reported by men), and victim-survivors’ accounts of change and maintenance of change related to DV behaviors.
The shorter follow-up interviews at 6-month followup (Wave 3) were primarily conducted to ascertain if any potential change identified at the conclusion of the program (during the exit interview and survey) was maintained. For this purpose, we present quantifiable data from follow-up interviews in descriptive format. Data presented here and used for the study primarily draw on victim-survivor reports. Reasons for drawing primarily on victim-survivor reports include that variation in reports of DV behaviors between victim-survivors and perpetrator self-reports are common, with perpetrator self-reports typically presenting a more encouraging account of behavior change compared to victim-survivors (Vall et al., 2021). Where Wave 3 victim-survivor data was unavailable, U-Turn participants’ data were used to identify self-reported AOD use. The research team did not use men's self-reports of the use of DV when victim-survivor data was unavailable because prior program evaluations have observed that men who use DV tend to underreport their DV perpetration (Herman et al., 2014; Meyer et al., 2019; Westwood et al., 2020). DV-related findings reported for Wave 3 are therefore limited to data from program participants who had a participating victim-survivor across all three waves of data collection.
Data Analysis
Quantitative data was analyzed using descriptive statistics and paired samples t-tests. Paired samples t-tests were employed to analyze change in survey responses between Waves 1 and 2. This analytic technique allows researchers to test whether there is a difference in mean scores for individuals between both timepoints. Due to the small sample of victim-survivor participants in Wave 2, t-tests were unable to be performed on all scales. Where t-tests were not able to be computed, descriptive statistics are presented instead. We use the 95% confidence threshold whereby a p-value ≤0.05 denotes statistical significance. Given the small sample sizes in both the male (n = 30) and female (n = 14) groups, caution should be taken when making causal claims based on the paired samples t-tests, as these limit the validity of results. However, despite the limitation in the statistical power of the analyses, due to the small sample sizes, nonstatistically significant findings still contribute meaningful descriptive insights into the experiences of women affected by men's comorbid use of AOD and DV and the benefits associated with a combined intervention addressing men's support needs.
Qualitative data captured during follow-up interviews in Waves 2 and 3 was analyzed using thematic analysis in NVivo 14 software. Themes for analysis were developed collaboratively by the research team, with relevance to the research aims and questions and prevalence of issues within existing literature. By way of example, within the parent node “AOD behaviors,” second level nodes included “men's AOD behaviors as self-reported by U-Turn participants” and “men's AOD behaviors reported by victim-survivors.” At the third level, child nodes included “current-ongoing use,” “recent past use,” and “historical from first use.” Given the dearth of literature on the effectiveness of combined interventions, researchers took an inductive approach to analysis (Thomas, 2006). That is, while guided by the project aims and existing evidence in the field, researchers did not approach analysis with any “prior assumptions” to be proved or disproved (Thomas, 2006, p. 38). Qualitative analysis was conducted by the first, second, and third author, with each transcript analyzed by two authors, conflicts in coding were discussed and resolved collaboratively. Each U-Turn program participant and victim-survivor was allocated a matching participant/victim-survivor number. These numbers are used in the results section when presenting direct interview quotes.
Results
Quantitative
Respectful Communication
The respectful communication scale includes five-items that capture victim-survivors experiences of respectful communication. The sample size to conduct paired t-tests for victim-survivors’ perceptions that the named person in their DVIO was respectful towards them in their communication was small. Additionally, the reported respectful behaviors scale at Wave 1 (n = 14) and Wave 2 (n = 10) was not normally distributed. For these reasons, a Wilcoxon signed rank test was conducted. However, it did not yield sufficient statistical power and was statistically nonsignificant. When examining the mean scores, results show that there was an increase in women's perceptions that the named person in their DVIO was respectful toward them at Wave 2 (M = 3.82; SD = 0.60) compared to Wave 1 (M = 3.39; SD = 1.12). In other words, limitations of nonsignificance and small sample size notwithstanding, participating women reported that their abusive (ex)partner/other family member was more respectful in their communication at program exit compared to intake.
Expanded “Space for Action”
The expanded “space for action” scale measures whether victim-survivors have space “which empowers through restoring their voice and ability to make choices” (Kelly & Westmarland, 2015, p.14). This scale was asked across Waves 1 and 2 to ascertain the extent to which victim-survivors experienced controlling behaviors. Due to the small sample size and non-normal distribution of the controlling behaviors scale at Waves 1 (n = 14) and 2 (n = 8), a Wilcoxon signed rank test was conducted. Results were statistically nonsignificant. However, a comparison of the mean scores shows a decrease in perceived controlling behaviors at Wave 2 (M = 1.60; SD = 0.45) when compared to Wave 1 (M = 2.40; SD = 0.87). In other words, victim-survivors reports suggest a decrease in men's controlling behaviors at the time the U-Turn program concluded.
Safety and Freedom From Violence and Abuse
The “Safety and Freedom from Violence and Abuse” scale contained 14 items, seven measuring nonphysical harassment and a further seven measuring experiences of physical and sexual harassment. Due to the small sample size and non-normal distribution of the nonphysical harassment scale at Waves 1 and 2, a Wilcoxon signed rank test was conducted to examine if there was a statistically significant difference between women's experiences of nonphysical harassment between Waves 1 and 2. Results of the test indicate that experiences of nonphysical harassment were statistically significantly lower at Wave 2 (Mdn = 1.00, n = 9) when compared to Wave 1 (Mdn = 2.43, n = 14), z = −2.68, p < .01, 95% confidence interval [0.38, 1.79], suggesting that men reduced the frequency of their nonphysical forms of harassment toward their victim-survivor. The medium effect size (r = 0.63) lends support to the role of the U-Turn program in curtailing harassing behaviors.
With regard to physical harassment at the hands of the U-Turn participant, women reported rarely experiencing each type of abuse at Wave 1 (M = 1.55; SD = 0.56; n = 14). At Wave 2, women reported that experiences of physical abuse had ceased altogether (M = 1.00; SD = 0.00; n = 8). A Wilcoxon signed rank test was conducted across each item at both waves but did not yield any statistically significant results. This is likely due to the small sample size that completed both waves of surveys.
Administrative Court Data
Administrative court data was utilized to identify whether participants had subsequent court contact after being referred to the U-Turn program. At the 12-month followup, nine U-Turn participants (30.0%) had criminal charges associated with their initial DVIO matter. Eight participants had at least one recorded DVIO breach on their court records since the DVIO came into effect. Breaches ranged from one to 11 breaches (27.6%; M = 3.9). Five participants with recorded DVIO breaches and four participants without recorded DVIO breaches also had other court matters heard since their first DVIO mention. Other court matters during the 12-month followup included alcohol-related offenses (n = 3), stealing offenses (n = 2), serious assault and criminal damage charges (n = 1), and a bond breach (n = 1).
While there are limitations to using court data to determine whether the U-Turn program was able to keep DVIO respondents out of the CJS (e.g., time lag between offenses occurring, charges being laid and matters being heard in court), the above findings suggest that the majority of U-Turn participants did not enter the CJS in the context of their DV offending behavior. None of the U-Turn participants reappeared in court for new DV matters (e.g., additional DVIOs and/or criminal charges involving a new partner) over the 12-month follow-up timeframe. Almost three-quarters (72.4%) of U-Turn participants did not appear in the court system for a DVIO breach during the follow-up timeframe. While some appeared for other criminal matters since their initial U-Turn referrals, some of these alleged offenses may have occurred prior to men's referral to U-Turn given the allowed timeframe of up to 12 months between charges being laid and a matter being mentioned in court for all non-DV matters, unless the matter involved a bail hearing.
Qualitative
Interview findings are presented according to three themes: men's AOD use, women's experiences of abuse, and the intersection of AOD use and DV. For the first two themes, interview data was coded into binary categories in order to provide descriptive insights into observed changes related to AOD and DV behaviors reported by victim-survivors (AOD and DV behaviors) and program participants (AOD behaviors only). The final theme draws on qualitative interview data to provide insights into victim-survivor and program participants’ understandings of the intersection of men's DV and AOD behaviors. These themes reflect the key outcomes assessed in the review of the pilot program and provide further insights into the quantitative assessment of change related to DV behaviors reported above.
Men's AOD Use
All victim-survivors and program participants who participated in a 6-month follow-up interview (n = 9, 64.3%; n = 16, 53.3%, respectively), were asked about men's AOD use. Eight victim-survivors were able to provide insights into men's AOD use at this timepoint (one was unable to comment on her ex-partner's current AOD use due to having no direct contact). This data is supplemented by self-report data from eight men where no corresponding victim-survivor data was available. Seven victim-survivors (87.5%) and seven program participants (87.5%) reported that changes to men's AOD use reported at program exit (Wave 2), had been maintained at the time of the 6-month follow-up interview (Wave 3). In the remaining two cases, one woman (14.3%) reported ongoing concerns about her ex-partner's problematic AOD use and one U-Turn participant (14.3%) whose ex-partner did not participate in the 6-month follow-up self-reported a deterioration in his drinking at the 6-month follow-up interview. While victim-survivor accounts are prioritized where available, notably, where both parties participated in Wave 3 interviews and were able to comment on men's AOD use (n = 7), men's self-reports related to AOD use aligned with that of their victim-survivor.
Women's Experiences of Abuse
All nine women who completed a 6-month follow-up interview were asked about potential ongoing abusive behaviors. Seven (77.8%) were in a relationship with the U-Turn participant at the time of the interview and confirmed that his reduced (or in some cases ceased) use of abusive behaviors reported at program exit had been maintained. The remaining two women (22.2%) were separated from the U-Turn participant and had reported limited or no improvement in abusive experiences at their ex-partner's program completion 6 months earlier. Of these two women, one experienced ongoing verbal and emotional abuse in the context of shared parenting contact and arrangements. The other woman had no ongoing direct contact with her ex-partner but reported being stalked and financial abuse connected to family law proceedings. Due to the limited sample size in this study, we are unable to draw conclusions on the influence of relationship status, however these findings lend support to the potential influence of relationship status on program participation and outcomes (see also, Gray et al., 2016).
Intersection of AOD Use and DV
The U-Turn program is designed to address men's comorbid use of DV and AOD. Moreover, there is a growing evidence base identifying the benefits of targeted interventions addressing this intersection. As such, this study aimed to understand how U-Turn participants and their victim-survivors made sense of their own experiences of this comorbidity. In order to understand men's reflections and insights on this intersection, we present men's and women’s qualitative accounts. Alcohol was the primary (and often sole) substance of concern for U-Turn participants. As reported above, changes to AOD behaviors were reported for most program participants (n = 14, 87.5%). They were reported as maintained at 6-month follow-up interviews by victim-survivors and program participants. These changes were reported to occur either after initial police or court contact or once they entered the U-Turn program. Alongside reduced AOD use, most U-Turn participants’ victim-survivors (n = 7, 77.8%) reported a reduction in DV and (where the relationship was ongoing) an overall improvement in their family relationships. These findings suggest that for many men in the U-Turn program, changes to their use of DV co-occurred with changes to problematic AOD use (primarily in the form of reduced alcohol intake). The below reflections by program participants illustrate recognition that addressing their problematic AOD used helped them address their use of DV:
I think I’ve just realized that all my problems—whenever my problems have occurred, they’ve been when I’ve been drinking as well. And I can’t think of a time when the police have been called or anything like that when both of us haven’t been drinking. Basically, I’ve realized that alcohol's probably the root of most of my problems. (Exit Interview, P11 Group 1)
I blamed her for everything. But now I can actually admit to it. If I wasn’t drinking—because I said to my wife, [name], “If I wasn’t drinking none of this would have happened.” I said that's what's made me change so I actually don’t drink anymore. (Exit Interview, P3 Group 1)
Program participants’ victim-survivors equally made sense of men's use of DV in the context of their problematic AOD consumption:
[At the time of the incident that led to police involvement] We’d had dinner together; we’d share one bottle of wine and then my husband continued to drink whisky. He consumed over half a bottle of whisky. (Exit Interview, Victim-Survivor12 Group 2)
[At the time of the incident that led to police involvement] He started hitting the alcohol a bit more harder [sic] than [usual] […] I think he just got a bit jealous, and he had a bit of a drink and then he showed up here and that's when it escalated. (Exit Interview, Victim-survivor6 Group 2)
While the above quotes illustrate the interconnectedness of men's drinking behaviors and their use of DV, they also highlight some noteworthy differences in women and men's accounts. While women partly understood men's use of violence or escalating aggression in the context of men's problematic AOD use and men tied their escalating anger and aggression closely to their level of intoxication, men also partly deflected their AOD use onto victim-survivors. Some men solely acknowledged their problematic AOD use in the context of describing excessive alcohol consumption by both parties. While they did not exclusively blame their victim-survivors’ AOD consumption for the occurrence or escalation of DV, there was an underlying connotation that both parties’ intoxication was associated with occurrences of DV. While these men recognized the intersection of their problematic AOD use and use of DV, immersed within these reflections are views that alcohol and other drugs are the cause of their use of DV and/or relationship problems generally. This is problematic when alcohol may be viewed as an excuse for behavior or used to minimize responsibility (Thomas et al., 2013; Radcliffe & Gilchrist, 2016) and suggests that some men in this study may benefit from longer-term accountability work to support lasting behavior change.
Limitations
While study findings overall highlight benefits of combined interventions, such as the U-Turn program, in (a) increasing family safety, (b) assisting men to maintain their achieved AOD and DV behavior change, and (c) keeping program participants out of the CJS, it must be noted that it is difficult to isolate this effect solely to men's participation in U-Turn in the absence of a control group design. Of the 25 men who participated in at least two waves of data collection, 22 were engaged with at least one other support service. Support services utilized by men parallel to and often beyond their participation in U-Turn included private psychologists and psychiatrists, one-on-one AOD counseling, and Alcoholics Anonymous. Further, most men reported conditions on their DVIOs that prohibited them from drinking at the family home or attending their victim-survivors’ residence while intoxicated. It is therefore likely that for at least some of the U-Turn participants, their reduction in problematic AOD use and use of DV may be attributable to factors beyond their U-Turn participation. The presence of these factors highlights the possible value of holistic engagement and monitoring for men with comorbid AOD and DV use. It is noteworthy, however, that some program participants reflected on what they had learnt in the U-Turn program and the impact of the program on their behavior related to both AOD use and DV.
Further, quantitative findings reported throughout the study were rarely statistically significant. This may be the result of the small sample size for U-Turn participants and victim-survivors who participated in the study. Future research should examine the effectiveness of combined interventions using larger sample sizes and, where possible, a control group design. Additionally, as discussed earlier in the measures section, the data presented in this paper excludes data collected at Wave 4 (14-month followup). Data for this project was collected across four U-Turn groups conducted as part of the pilot. However, due to COVID-19-related delays in the commencement of Groups 3 and 4, only Groups 1 and 2 had reached the 14-month follow-up timepoint when the study concluded. As a result, the participant sample for Wave 4 data collection was limited to two of the four pilot groups. Further, as reported earlier in the paper, the attrition rate by the Wave 4 data collection in Groups 1 and 2 was substantial, leaving only seven men (36.8%) who participated in Wave 4 data collection. These factors informed the exclusion of Wave 4 data. While high attrition rates in behavior change programs and related research are common (Jewell & Wormith, 2010; Rondeau et al., 2001), the lack of longer-term followup remains a significant limitation. In order to support more rigorous evidence building in this space, funding bodies need to ensure resources are able to facilitate the provision of multiple intervention groups, control group design and sufficient follow-up periods to capture long-term program impacts (see also Nicholas et al., 2020).
Discussion and Applications to Practice
Findings presented here support the potential value of combined interventions targeting men whose abusive behaviors are closely linked to problematic AOD use. For the vast majority of U-Turn participants, alcohol was the primary and, in most cases, sole substance of concern, which aligns with broader evidence that alcohol is the most common substance identified in the context of problematic AOD use in Australian and international prevalence studies (AIHW, 2020; Ting et al., 2009).
Findings indicate a reduction or cessation of problematic AOD use among the majority of male study participants over the course of their involvement in U-Turn, which appeared to be maintained throughout the 6-month follow-up period. Alongside the observed improvements in men's AOD behaviors, most victim-survivors who participated in the study across all three waves of data collection reported a reduction in DV over the course of men's participation in the 12-week U-Turn program. This appeared to be maintained over the 6-month follow-up period postprogram conclusion. These findings align with other research evidence that has identified a reduction in DV where men presenting with problematic AOD use address their AOD use through participation in combined interventions (Goldkamp et al., 1996; Easton & Sinha, 2002; Easton et al., 2007). Further, research has suggested more broadly that where men presenting with comorbid use of AOD and DV address their problematic AOD use, DV frequently decreases alongside a decrease in problematic AOD use (Klostermann et al., 2010; Lipsky et al., 2010; Stuart, 2005). However, while stand-alone AOD interventions, without specific emphasis on DV or intimate partner violence, have been shown to decrease violence, many program participants also continue to use violence, particularly where relapse occurs (Klostermann et al., 2010; Capezza et al., 2015). Therefore, while some improvements may be possible, social work practice must recognize its intersection and related increased risk of harm through holistic approach to behavior change in order “to achieve the best possible outcomes for both problems” (Capezza et al., 2015, p. 86; Karakurt et al., 2019; Meyer et al., 2020).
Qualitative data derived through 6-month follow-up interviews indicates that limitations to improved AOD and DV behaviors were primarily observed for separated couples. While limited to a small number of participants (as most U-Turn participants remained in or resumed a relationship with the victim-survivor), findings generated by the current study suggest that outcomes may be more promising for program participants who remained in a relationship with the victim-survivor or were working toward reconciliation. This observation aligns with other research, which notes that men using DV may be more responsive to behavior change interventions when the relationship is ongoing, or men are working toward reconciliation—as this has been identified as a motivator for change among abusive men (Gray et al., 2016; Chung & O’Leary, 2009).
As discussed earlier in this article, the U-Turn program specifically targets men who come to the attention of the local court for a DV matter involving AOD use and who do not have an extensive police or court record for DV or other offending behavior. As a result, few program participants presented with highly complex needs or substantial criminogenic risk factors. The small number of participants who presented with some level of complexity—including chronic illicit drug use, significant trauma and mental health problems, ongoing child protection involvement, and/or repeat or prolonged experiences of housing instability—disengaged from the study by the 6-month followup, with one already disengaging halfway through the 12-week intervention. Two men who presented with complex needs and completed the program but were uncontactable by Wave 3 data collection appeared to have achieved some level of change by Wave 2 data collection (program exit). However, the study was unable to capture whether this change was maintained postprogram completion among those presenting with more complex needs.
The “early intervention” referral pathway that forms part of the U-Turn program may therefore be a key contributing factor to the positive outcomes observed here and findings may not be as favorable for participants presenting with more complex needs. Future combined interventions in social work and justice settings should either operate as “early interventions” or—if aiming to address more complex needs—be integrated into a more holistic response to men presenting with comorbid AOD use and use of DV, involving for example housing, mental health, and child protection services as key program partners.
Finally, a key aim of the U-Turn program was to keep men presenting in court for a DV matter with identified problematic AOD use out of the CJS by jointly addressing problematic AOD use and their use of DV. It is not possible to attribute the absence of subsequent DV-related CJS contact among the majority of study participants solely to their participation in U-Turn due the absence of a control group study design. However, this observation is promising and aligns with research evidence from other studies that highlight the benefits of combined intervention approaches in increasing motivation to change and preventing repeat DV offending behavior (Easton & Sinha, 2002; Goldkamp et al., 1996). This has significant implications for social work practice, with social workers frequently providing clinical AOD and DV-related behavior change interventions. Recognizing the intersection of DV and problematic AOD use and the potential for combined interventions creates opportunities for men using violence to address AOD use related harm and take accountability for their abusive behaviors and its impact on women and children. As a result, social work and human services must ensure practitioners take a holistic approach to intersecting client needs to maximize opportunities for behavior change and family safety in the context of DV and AOD use (Meyer et al., 2020).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.