
Abstract
Special educational needs (SENs) refer to learning difficulties or disabilities that impede children’s educational progress and holistic development (UNESCO, 2017). Due to the multifaceted nature of their sensory, cognitive, social, emotional, and behavioral needs, children with SEN are likely to need more support compared to their typically developing peers of similar age (Education, 1996). These unique characteristics exacerbate the childcare challenges and parenting stress (Maridal et al., 2021; Olson et al., 2022). Parents of children with SEN often articulate managing their children’s emotions and behaviors as the most demanding aspect of their caregiving experience (Baker et al., 2002; Ki & Joanne, 2014). Furthermore, factors such as limited social support networks, the severity of disabilities, coordination of school activities, as well as the financial outlays and logistical arrangements associated with therapeutic interventions, impose extra pressures and responsibilities upon parental roles (Plant & Sanders, 2007; Siracusano et al., 2021). Therefore, nurturing children with SEN could be extremely challenging and stressful for parents.
An extensive body of research has extensively documented the pronounced challenges faced by parents of children with SEN, as compared to those with typically developing children. These challenges include significant parental stress, poor mental well-being, financial stress, social stigma, career disruptions, diminished leisure opportunities, and marital dissatisfaction (Baxter et al., 2000; Chiang, 2014; Goudie et al., 2014; Ki & Joanne, 2014; Mak & Kwok, 2010; Silva & Schalock, 2012; Siracusano et al., 2021). Moreover, the literature highlights the essential role of parenting in shaping children’s developmental trajectories (Jennings & Dietz, 2007; Plant & Sanders, 2007). For instance, adverse parenting practices such as punitive disciplinary measures, inconsistent parenting styles, inadequate supervision, and dysfunctional parent-child interactions serve as precipitants for the emergence of externalizing (e.g., aggression, delinquency) and internalizing symptoms (e.g., anxiety, depression, low self-esteem) (Keleynikov et al., 2023). These behavioral manifestations create additional stress for caregivers. Empirical evidence suggests that for parents of children with SEN who engage in higher frequencies of negative parenting practices, their children tend to exhibit more behavioral and emotional problems (Keleynikov et al., 2023). Undesirable parenting practices not only hinder children’s interpersonal competencies but also discourage the cultivation of adaptive social skills. The parenting challenges and distress exert adverse effects on various facets of parental functioning, including parenting efficacy, psychological well-being, positive parental behaviors, parent-child relationships, family functioning, and child development (Giovagnoli et al., 2015; Jennings & Dietz, 2007; Mugno et al., 2007; Vahedparast et al., 2022). Moreover, empirical findings indicate a robust association between dysfunctional parenting behaviors, elevated parental stress, and diminished parenting competence (Bloomfield & Kendall, 2012; Sanders & Woolley, 2005). Parenting sense of competence, referring to parents’ confidence in their capacity to fulfill the responsibilities of parenthood effectively, is reported to be remarkably attenuated among parents of children with SEN (Bloomfield & Kendall, 2012; Jandrić & Kurtović, 2021). Indeed, strategies can effectively bolster parental efficacy and enhance the holistic well-being and development of children (Bloomfield & Kendall, 2012). Therefore, parenting interventions designed to furnish parents with effective parenting strategies, foster positive parent-child interactions, and cultivate emotion regulation skills emerge as particularly salient avenues of support for parents of children with SEN.
Existing Parental Education Programs and In vivo Practice
Parenting education programs tailored to the needs of parents of children with SENs are essential in equipping them with the necessary skills and strategies to navigate the complexities of caregiving. The parental education program is characterized by providing knowledge and skills to parents (Brookman-Frazee & Koegel, 2004), which is effective in enhancing parental competence and alleviating parental stress among parents of children with SEN (Dempsey et al., 2009; McConachie & Diggle, 2007). Many well-established research-supported parenting programs, like the Incredible Years (Lee McIntyre, 2008), the Stepping Stones Triple P Parenting (Sanders et al., 2004; Whittingham et al., 2009), and the Early Head Start (Berlin et al., 2018), were shown to be effective for parents of children with SEN. These group-based parenting programs not only create a space for developing a parenting sense of competence through peer learning, verbal persuasion and emotional arousal but also demonstrate significant improvements in maternal psycho-social health outcomes (Barlow & Coren, 2004; Bloomfield & Kendall, 2012). While existing programs such as Stones Triple P Parenting and Early Head Start have demonstrated effectiveness in enhancing parental competence and improving maternal psycho-social health outcomes, there remains a need for targeted interventions that address the specific challenges faced by parents of children with SEN. Systematic reviews commented that most of the studies focused on children’s outcomes, while less attention is paid to parents’ needs and their parenting capacities in the therapeutic group setting (Kuravackel et al., 2018; Whittingham et al., 2009). This suggests the need for parenting education programs aimed at equipping parents of children with SEN with positive parenting strategies, positive child-child interaction, and emotion management skills.
In vivo practice, a prevalent treatment approach for behavioral and emotional problems, has demonstrated efficacy in improving parenting-child interaction and attachment (Baghaei et al., 2021; Carl et al., 2019; Shanley & Niec, 2010). This intervention method involves simulated real-world scenarios designed for experimentation or study, providing parents with valuable feedback to enhance their parenting skills (VandenBos, 2007). Existing literature underscores the salutary impact of high-quality in vivo feedback on enhancing both parenting-child interaction and attachment outcomes (Caron et al., 2018). Recognized as an essential mechanism for change, the provision of in vivo feedback significantly contributes to the enhancement of parental skills (Shanley & Niec, 2010). Although empirical studies delineated how in vivo feedback mechanisms increase parent engagement and facilitate skill acquisition, little attention has been paid to understanding the nuanced effects of in vivo practices on parenting competence, parental distress, and dysfunctional parenting behaviors (Barnett et al., 2017; Shanley & Niec, 2010). To address this knowledge gap, the present study introduced the Strategies and Skills Learning and Development (SSLD) Parent Capacity-Building Program and evaluated its efficacy in improving the parenting capacity of Chinese parents of children with SEN. An integral feature of this program is the incorporation of in vivo practice sessions as a foundational component, providing parents with a practical avenue to apply acquired knowledge and skills within authentic parenting scenarios. This unique feature empowers parents to translate theoretical concepts into practical strategies, thereby fostering a deeper understanding of their children’s needs and enhancing their competence in addressing these needs effectively.
The SSLD Parent Capacity Building Program
The Strategies and Skills Learning and Development (SSLD) System, developed by A. Ka Tat Tsang, represents an action-oriented approach geared towards effecting transformative change across various dimensions of human life, encompassing cognition, action, motivation, emotion, and environmental contexts (Tsang, 2013). This innovative model empowers clients within diverse professional domains, including social work, health, mental health, and human services, to navigate their needs and aspirations effectively. The SSLD system focuses on helping people develop attainable learning objectives to meet their desired outcomes through systematically learning and developing strategies and skills that are effective, applicable, and relevant to the specific circumstances of their lives. Emphasizing the importance of adopting a multiple contingency mindset, the SSLD system acknowledges the intricate interplay of N3C—current needs, personal characteristics, circumstances, and capacity, positing that the relationship between cognition and emotion is inherently nuanced and cannot be distilled into a simplistic, linear framework (Tsang, 2013). This perspective underscores the need for an open and flexible mindset that considers diverse contingencies related to personal variables, cultural factors, and social determinants, empowering individuals to respond adeptly to their unique needs and circumstances.
Although the SSLD system has garnered considerable success across various human services domains, such as senior services (Liu et al., 2018; Tsang & Ip, 2017; Tsang & Li, 2017), immigrants and refugees (Tsang & Li, 2017), racial minorities (Tsang et al., 2022), and sexuality and intimacy (Chu et al., 2015); its efficacy within children's rehabilitation services remains relatively unexplored.
Parents of children with SEN often struggle with feelings of helplessness, distress, and frustration stemming from challenges in managing their child’s behavior and understanding their needs (Howe, 2006). Children with developmental disorders may find difficulties in recognizing others’ emotional and mental states from facial expressions, vocal intonation, body language, and context (Golan et al., 2010; Grossman et al., 2000). These children resort to behavioral strategies, such as auto-stimulation, object manipulation, and adherence to rigid patterns, to satisfy their needs or avoid negative emotional experiences. However, parents describe these behavioral strategies employed by children with SEN as sources of parenting stress, escalating parental pressure and disrupting parent-child relationships (Hastings, 2002). From the SSLD perspective, these parents—like other individuals—present problems that reflect their underlying needs, and they employ different behavioral strategies to fulfill the unmet needs. The SSLD Parent Capacity Building Program aims to assist parents in mastering this fundamental technique of ‘problem translation' to analyze their children's behaviors and discern their unmet needs of the presenting problems.
Within the SSLD framework, the SSLD Parent Capacity Building Program emerges as an action-oriented intervention specifically designed to assist parents of children with SEN in increasing parenting capacity to effectively address both their own and their children's needs. The goals of this parenting program are to help parents (1) comprehend their children's behaviors; (2) develop tailored parenting strategies to meet their children's needs; (3) improve parental competence and refine parenting styles; and (4) reduce parenting stress. The SSLD Parent Capacity Building Program is unique in incorporating in vivo practice sessions in its program design, especially emphasizing the application of individualized strategies based on the client's N3C in real-life scenarios rather than having a pre-standardized program. This innovative feature anticipates that parents will acquire the ability to translate presenting problems into specific learning objectives, formulate relevant strategies to fulfill unmet needs, and adeptly apply these acquired skills and strategies in real-life parenting situations.
Purpose of Study
The SSLD Parent Capacity Building Program is a parental education program with two in vivo practice sessions for enhancing parents of children with SEN in Hong Kong. This randomized controlled trial aimed to investigate the efficacy of the SSLD Parent Capacity Building Program on improving parental stress and parenting capacities in caring for children with SEN.
Method
Trial Registration and Participants
The study protocol and all procedures were approved by the Hong Kong Polytechnic University Institutional Review Board (IRB) (Reference number: HSEARS20171023003) This trial was also registered on the International Standard Randomized Controlled Trial Number (ISRCTN36895493) registry, which is a registry recognized by the World Health Organization (WHO). This study was conducted in seven child rehabilitation service units in Hong Kong, which provide professional rehabilitation services to children with SEN and their families.
Recruitment
Power analysis indicated that a minimum sample size of 26 in each group was required to study a large effect size. From December 2017 to February 2018, social workers in each training center recruited potential participants through the distribution of flyers at the training centers, referrals by healthcare professionals, and word of mouth. Parents were eligible to participate if (i) they had a child aged six years old or below; (ii) that child was diagnosed with SEN (such as Global Delay, Language Delay, Autism Spectrum Disorder, Attention-Deficit/Hyperactivity Disorder and learning disabilities); (iii) that child received rehabilitation services at one of the study sites; and (iv) they were available to join both intervention group sessions. Additional exclusion criteria were severe mental health problems with urgent needs for intensive treatments from the hospital and unavailability to attend the group sessions. A total of 115 parents were finally recruited for this study, and three participants were excluded based on the exclusion criteria. Figure 1 presents the sample size throughout the stages of the study, including ineligibility, randomization, and dropouts. A total of 112 parents were screened as eligible for the study. Among the participants, 56 parents were randomly allocated to the intervention group while 56 parents were to the control group. The final analytic sample comprised 109 parents, with 107 (98.2%) completing the baseline assessment; 102 (93.6%) completing the post-treatment/ post-waitlist assessment; and 98 (90.0%) completing the last time point (follow-up for the intervention group and post-treatment for the control group). As shown in Tables 1 and 2, the demographic characteristics were not significantly different between the intervention and control groups. Most of the participants were mothers (n = 90, 82.6%), and their ages ranged from 24 to 60 years old (M = 38.60; SD = 5.35). Their children ranged from 2 to 6 years old (M = 4.44, SD = 0.80).
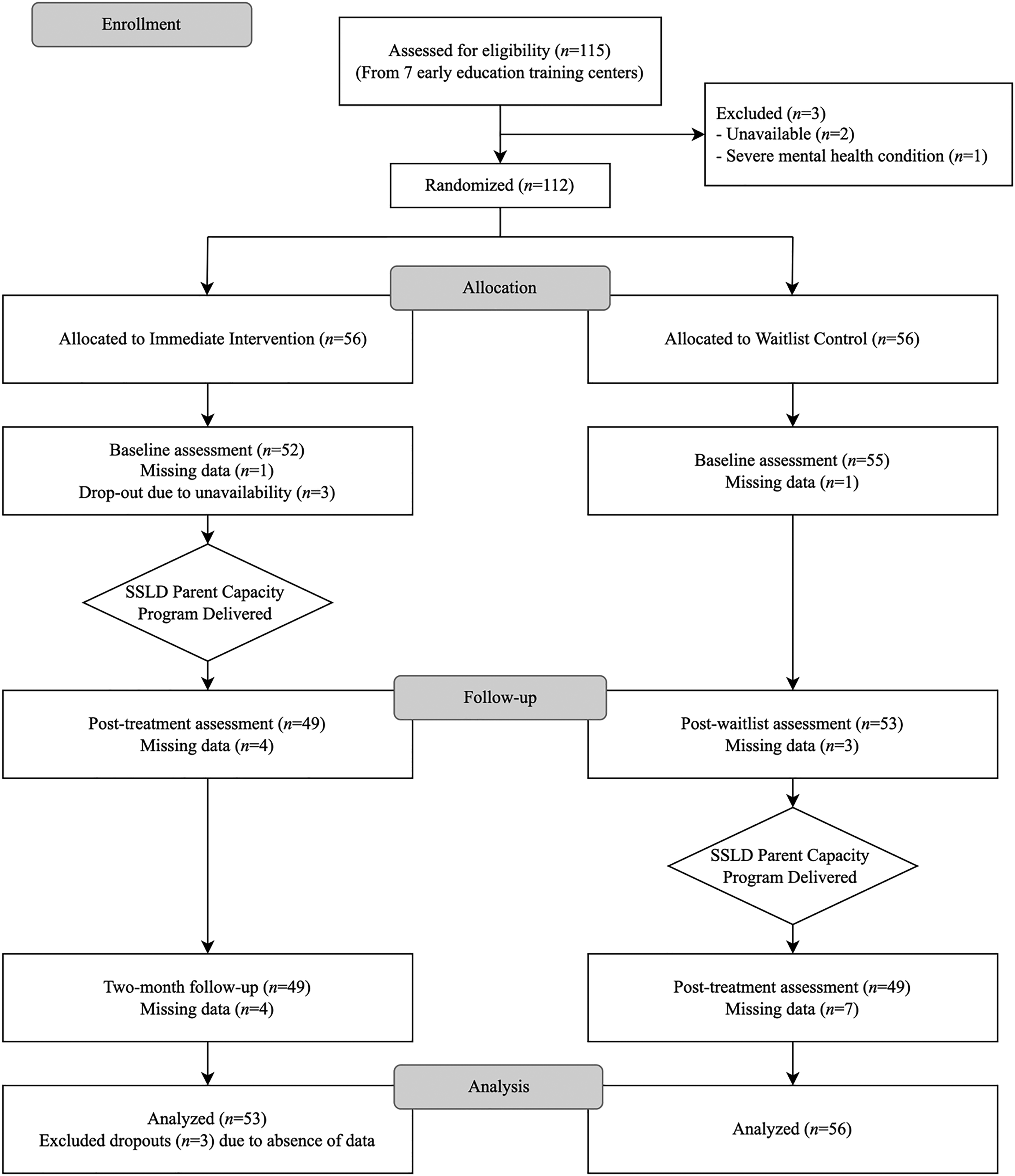
CONSORT flow diagram: The flow of participants through the study.
Demographic Characteristics of Parent Participants (n = 109).
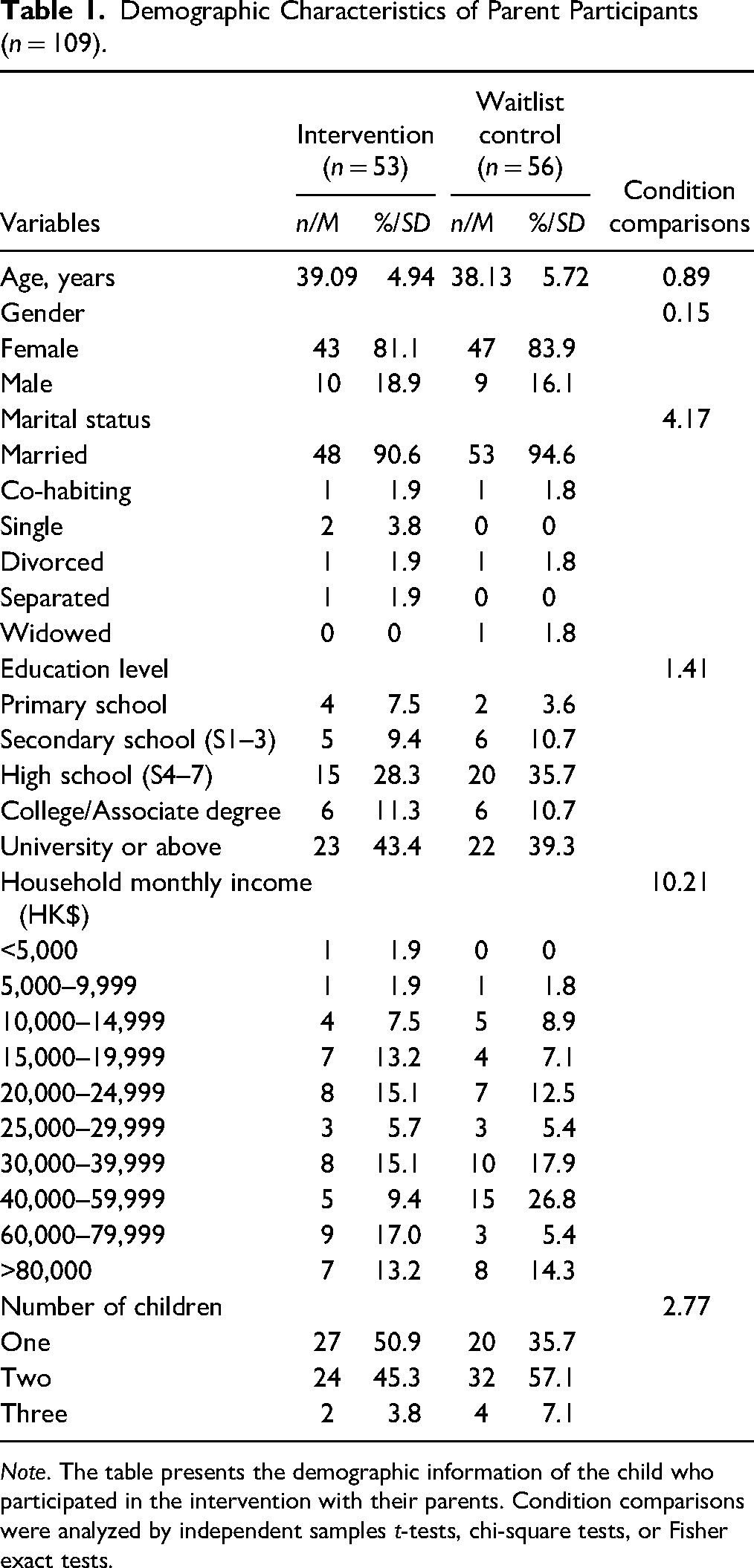
Note. The table presents the demographic information of the child who participated in the intervention with their parents. Condition comparisons were analyzed by independent samples t-tests, chi-square tests, or Fisher exact tests.
Demographic Characteristics of Participants' Children (n = 109).
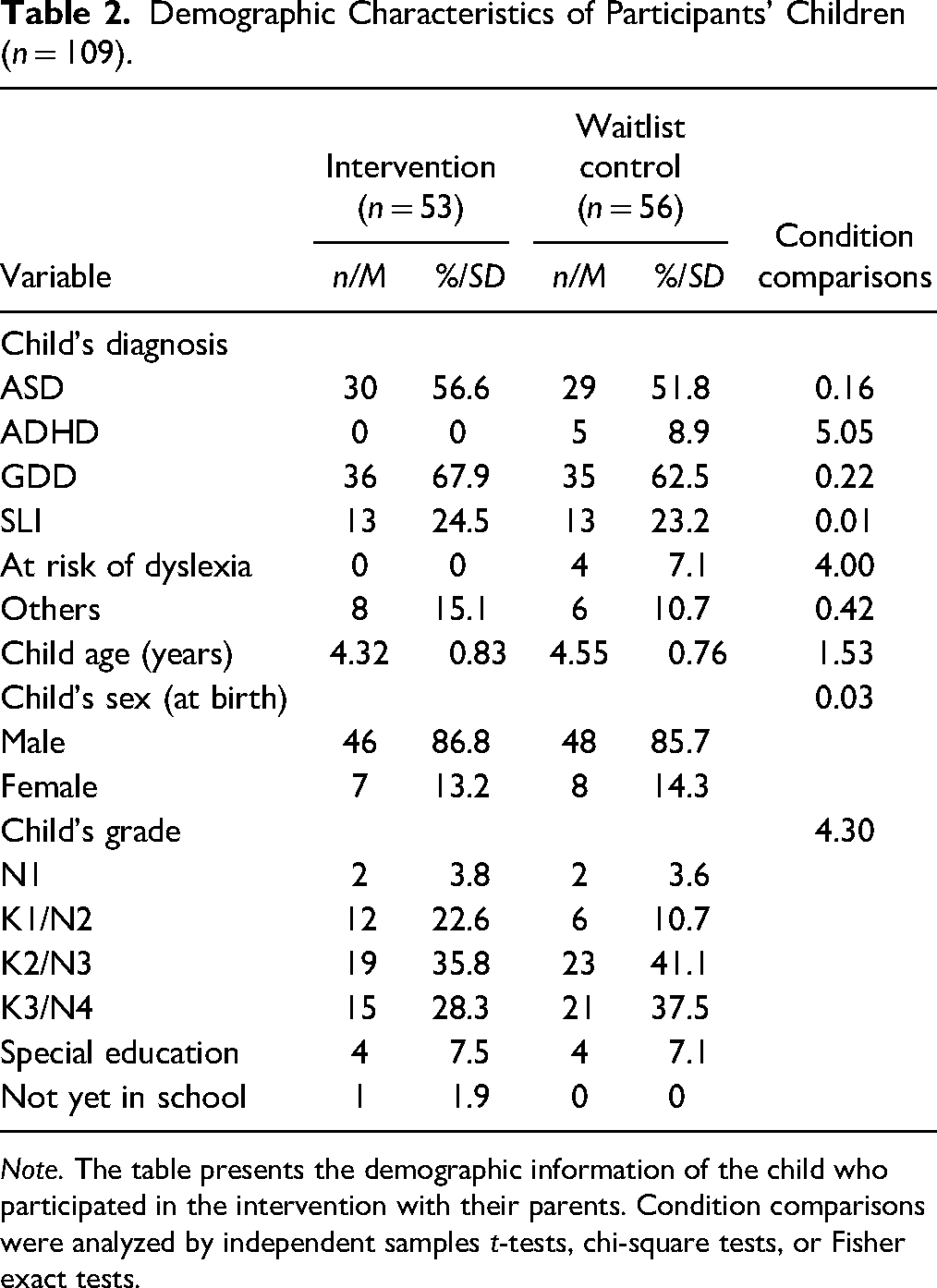
Note. The table presents the demographic information of the child who participated in the intervention with their parents. Condition comparisons were analyzed by independent samples t-tests, chi-square tests, or Fisher exact tests.
Procedure
Screening
Following the recruitment phase, social workers stationed at each training center contacted individuals expressing interest in participation, coordinating a screening interview either in person or via telephone. The screening interview served the dual purpose of assessing eligibility criteria and providing comprehensive explanations of the research study and associated intervention protocols, ensuring that participants were fully informed before consenting to involvement. After the randomization process, all randomized participants received notification regarding their group assignment and were promptly scheduled for individual pre-group sessions facilitated by the research team.
SSLD Parent Capacity Building Program
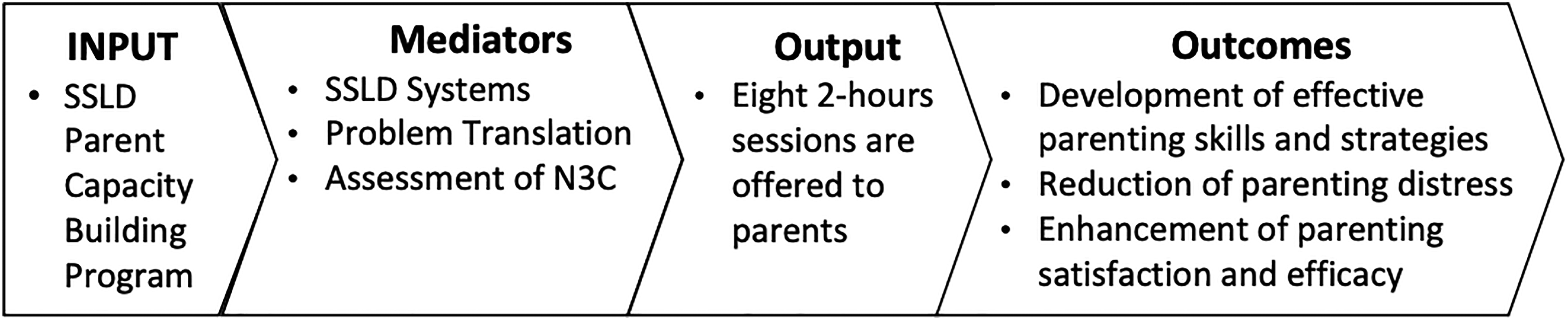
The intervention protocol comprises a series of eight weekly sessions, each spanning approximately two hours. A comprehensive breakdown of the agenda for each session is provided in Table 4. These sessions are designed with specific learning objectives aimed at guiding participants through a structured process conducive to enhancing their parenting competencies and overall well-being. The learning objectives include (1) facilitating parents’ comprehension of the underlying needs associated with presenting problems from an SSLD framework; (2) assisting parents in the translation of presenting issues into actionable learning objectives through a thorough N3C assessment; (3) enhancing parents’ capacity for acquiring and sharpening effective parenting techniques and strategies tailored to meet the identified unmet needs of their children; (4) fostering parental awareness regarding personal development and self-care practices essential for maintaining optimal caregiving efficacy and personal well-being; and (5) encouraging the application of acquired knowledge and skills to real-life parenting scenarios, supported by a multiple-contingency mindset. This methodological framework is visually represented in Figure 2, explicating the logical progression of the intervention components and their interrelationships.
Strategies and Skills Learning and Development (SSLD) parent capacity building program logic.
Condition and Time Comparisons for Key Outcome Variables.
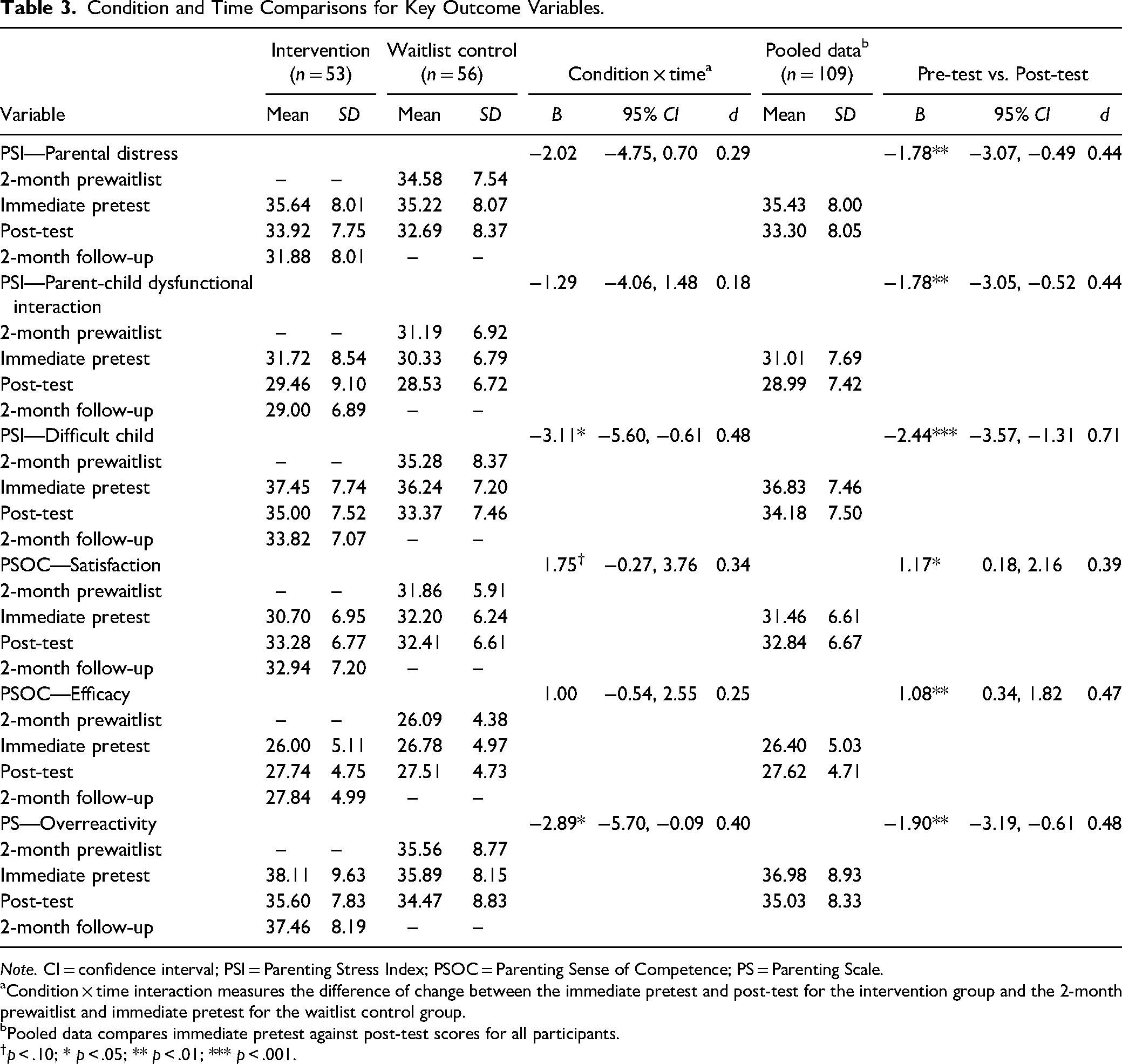
Note. CI = confidence interval; PSI = Parenting Stress Index; PSOC = Parenting Sense of Competence; PS = Parenting Scale.
Condition × time interaction measures the difference of change between the immediate pretest and post-test for the intervention group and the 2-month prewaitlist and immediate pretest for the waitlist control group.
Pooled data compares immediate pretest against post-test scores for all participants.
p < .10; * p < .05; ** p < .01; *** p < .001.
SSLD Parent Capacity Building Program Outline.
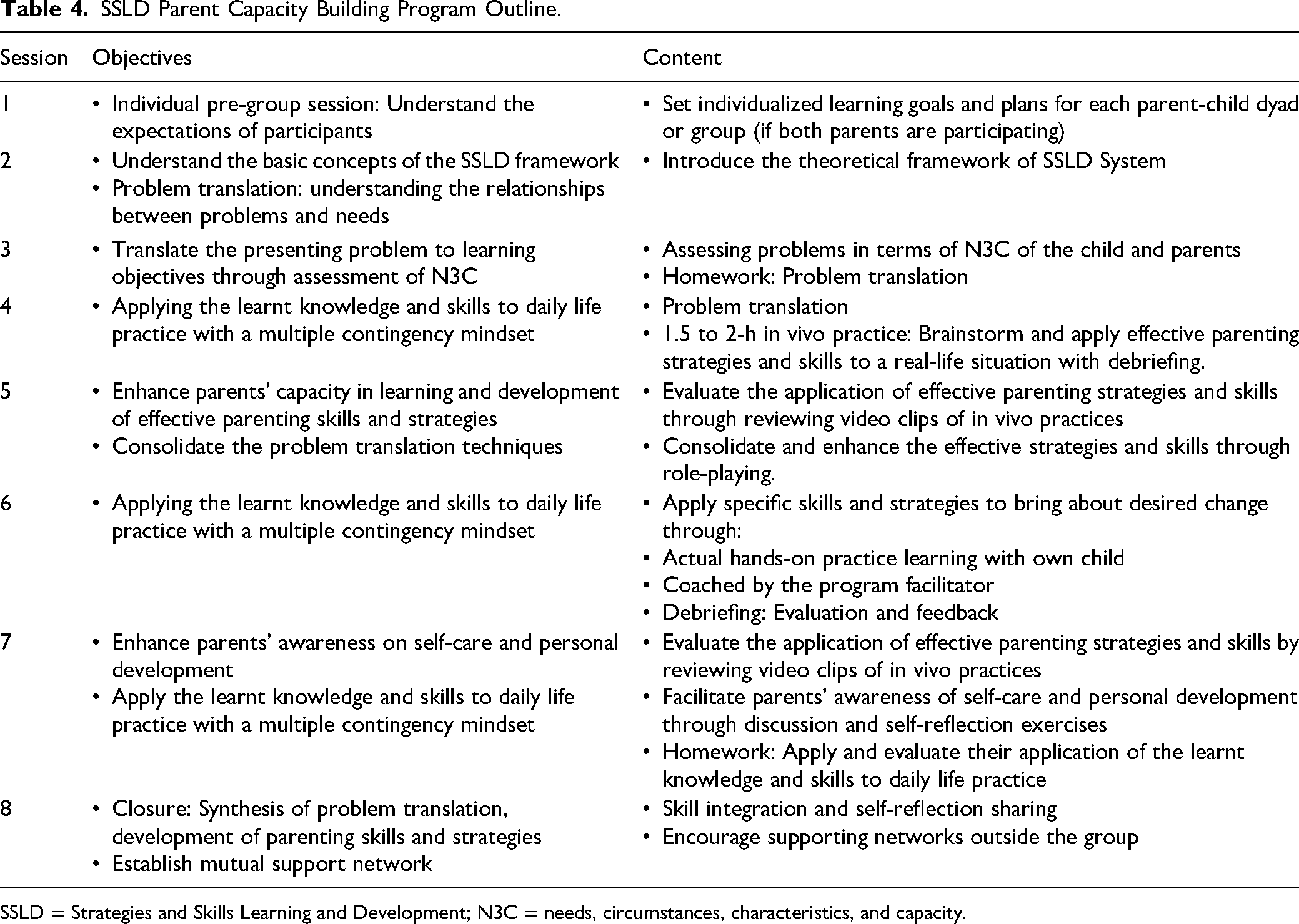
SSLD = Strategies and Skills Learning and Development; N3C = needs, circumstances, characteristics, and capacity.
Facilitator Training and Supervision
The SSLD Parent Capacity Building Program was led by two facilitators with social work training backgrounds. Prior to leading the program, all facilitators underwent a rigorous three-day training conducted by accredited SSLD trainers, wherein they received foundational instruction on the SSLD framework and were briefed on the course structure and objectives. To uphold program quality and fidelity, facilitators were furnished with a comprehensive facilitation manual detailing the SSLD Parent Capacity Building Program protocols, which served as a guiding framework throughout the program delivery process. Additionally, facilitators benefitted from a minimum of four sessions of onsite supervision conducted by accredited SSLD trainers, during which each session was recorded for supervisory purposes. Post-session debriefings were systematically organized to assess the efficacy of the group process and the attainment of session objectives. To accommodate absent participants and ensure continuity in learning, facilitators were mandated to allocate additional time to review session content with individuals who had missed sessions. This multifaceted approach was implemented to safeguard program integrity and optimize participant engagement and learning outcomes.
Attendance
Out of the 109 participants, 46 individuals (42.2%) completed all eight sessions of the intervention. A total of 98 participants (89.9%) attended more than half of the intervention (four sessions or above). It is imperative to emphasize that this study adopted an intent-to-treat approach, thereby encompassing all randomized participants (n = 109) in the analyses, irrespective of their level of engagement with the intervention protocol.
Outcome Measures
Analytic Plan
An intent-to-treat approach was used, including all randomized cases in the analyses (n = 109), with no missing data observed across all outcome measures (i.e., PSI-SF, PSOC, and PS). Prior to the main analyses, t-tests, chi-square tests, and Fisher exact tests were conducted to determine if there was any significant difference between participants in the intervention and control groups. Since no significant differences were found, the main analyses were conducted without including demographic covariates. The efficacy of the intervention was examined using a similar three-step approach described by Pachankis et al. (2015): (a) Comparisons of the effects between intervention and control conditions, (b) pooled analyses to examine changes between immediate pretest and post-test for all participants and (c) evaluation of the maintenance of intervention effects during the 2-month follow-up period for the intervention group.
First, linear mixed models with maximum likelihood estimation were used to estimate the effects of condition, time, and interaction term condition × time for all outcome variables. Changes after receiving the SSLD Parent Capacity Building Program for the intervention group were compared against a 2-month waiting period for the control group. Conditions were coded as intervention group = 1 and control group = 0, with the baseline measure coded as 0 and the second time point (post-test for the intervention group and immediate pretest for the control group) coded as 1. The interaction term condition × time was utilized to assess whether changes throughout this period varied between the two conditions. Second, the pooled analyses combined immediate pretest and post-test data from all participants to gain an overall understanding of intervention effects for the entire sample, considering that all participants eventually received the intervention by the study’s conclusion. Finally, changes between the post-test (coded as 0) and the 2-month follow-up assessment (coded as 1) for the intervention group were examined to determine whether effects were sustained two months after program completion and whether any additional changes to outcome variables occurred as participants continued to apply learned skills to real-life scenarios.
Linear mixed modeling was used for all three steps of analysis, and the therapy grouping was included as a cluster in the analyses to account for the possible interdependence of participants within each therapy group. For all analyses, effect sizes were calculated by Cohen’s d formula [d = 2t/√(df)], using the t value of the interaction term or the time factor (Howell, 1992).
Qualitative Focus Groups
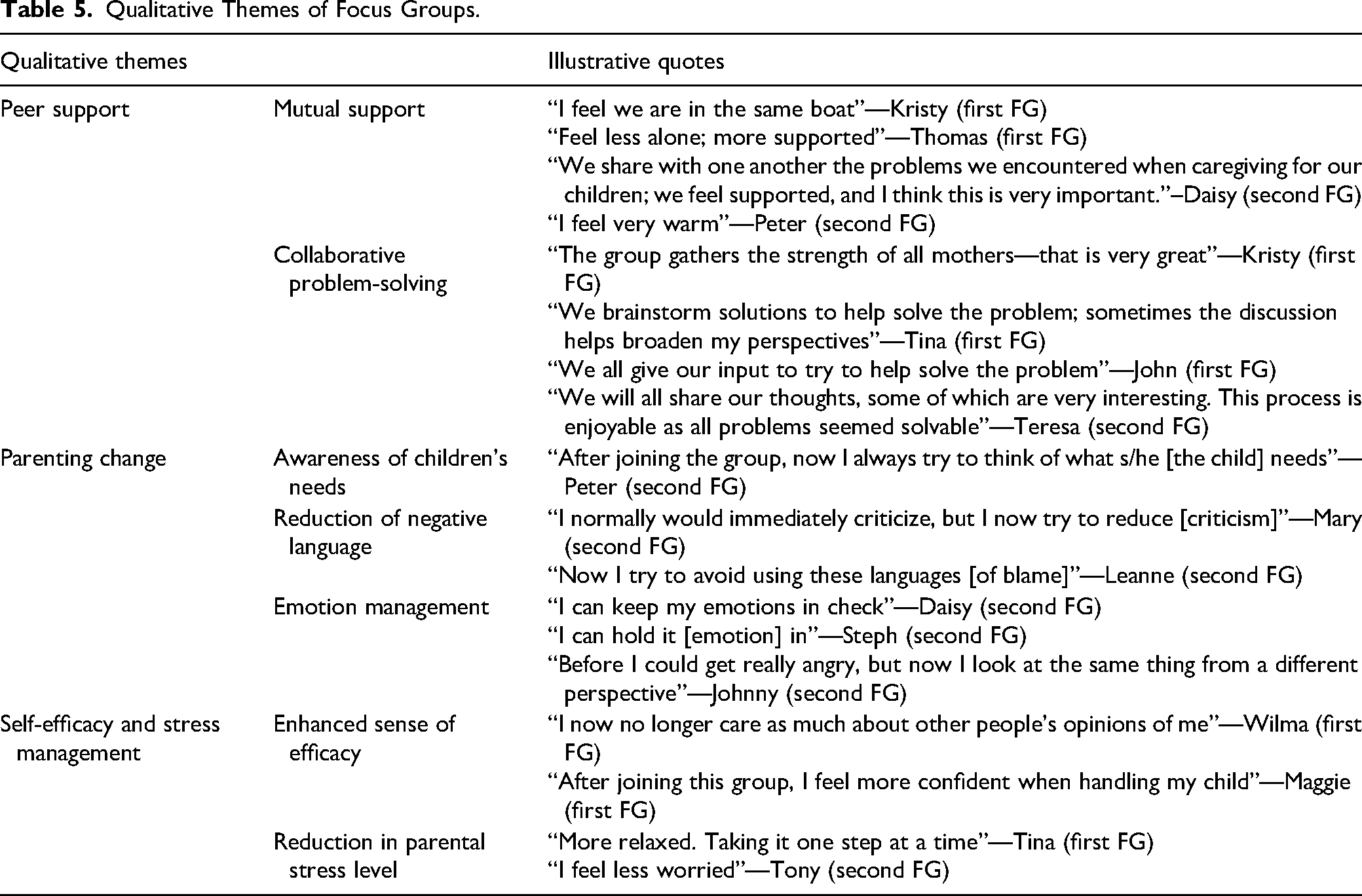
To explore the impact of the intervention from the participants’ perspectives, social workers from each training center reached out to participants from the randomized controlled trial study via telephone, inviting them to participate in this qualitative research component. Parents who expressed interest were subsequently invited to join focus groups. A total of 18 parents indicated their interest and were recruited for this qualitative study. Eight (n = 8) parents joined the focus group in August 2018 and ten (n = 10) were recruited to participate in a subsequent follow-up focus group in October 2020. The focus groups were conducted in Cantonese and facilitated by two researchers following a semi-structured facilitation guide with open-ended questions while keeping the prompts to a minimum to encourage original responses from participants about their overall experience with the intervention, the impacts of the intervention on the participants’ parenting practices and their feedback on the program. Following the focus group sessions, interviews were transcribed by a bilingual translator, initially transcribed into the source language (Chinese) and then translated into English. Back translation was independently conducted by another bilingual translator to ensure translation accuracy and validity. To mitigate the risk of translation discrepancies, the two translators then collaboratively reviewed the translated transcripts to ensure consistency and fidelity to the original content. Thematic analysis, following the approach outlined by Braun and Clarke (2012), was used to analyze the transcribed data. The research team followed an open coding approach to annotate anything significant and noted any repetitions, patterns, and differences. The initial set of codes was derived after the first round of open coding. Preliminary findings were reviewed and discussed among the research team to refine and categorize similar codes. Any discrepancies in themes were discussed, re-assessed, and negotiated at multiple rounds of research meetings until the research team reached agreements. The iterative process was repeated until the key themes below emerged. Illustrative quotes were included to support the themes. When selecting the quotes, the research team reviewed similar responses and selected those that were more semantically and conceptually reflective of the themes as illustrative quotes. To ensure anonymity, pseudonyms were used when presenting the illustrative quotes in Table 5.
Qualitative Themes of Focus Groups.
Results
Condition Comparisons
Table 3 presents the descriptive statistics of primary outcome measures and the main results. The changes in outcome scores during the first two time points were compared between the two conditions. The interaction term condition × time was significant for two outcome variables: PSI—Difficult Child (B = −3.11, p = .015, d = 0.48) and PS—Overreactivity (B = −2.89, p = .043, d = 0.40). Additionally, the interaction term was marginally significant for PSOC—Satisfaction (B = 1.75, p = .088, d = 0.34). These interaction effects had medium effect sizes. Participants in the intervention condition demonstrated significantly different changes between the immediate pre-test and post-test compared to changes between the pre-waitlist and immediate pretest for participants in the control.
For PSI—Difficult Child, the intervention group reported a significant reduction in scores after the intervention (B = −2.18, p = .018), while there was no significant change for the control (0.92, p = .292). Similarly, the intervention group participants had significantly decreased scores for PS—Overreactivity (B = −2.57, p = .013), while there was no change for the control participants (B = 0.32, p = .743). Furthermore, intervention group participants reported a significant increase in PSOC—Satisfaction after the intervention (B = 2.02, p = .007), while there was no significant change for waitlist control participants (B = 0.27, p = .699).
Pooled Analyses
Immediate pretest and post-test data from both conditions were combined for pooled analysis to examine changes in scores for all participants after the intervention. As shown in Table 3, participants experienced significant improvement in all primary outcomes from the immediate pretest to the post-test. Specifically, participants reported significant reductions in parental distress (B = −1.78, p = .007, d = 0.44), parenting-child dysfunctional interaction (B = −1.78, p = .006, d = 0.44), and reported their child to be less difficult (B = −2.44, p < .001, d = 0.71) after the intervention. Participants also had significantly higher parental satisfaction (B = 1.17, p = .021, d = 0.39) and efficacy (B = 1.08, p = .005, d = 0.47) at the post-test. Finally, there was a decrease in overreactivity scores after the intervention (B = −1.90, p = .004, d = 0.48). The effect sizes of the changes ranged from 0.39 to 0.71, indicating medium to large effects.
Maintenance in 2-Month Follow up
Outcome scores of the post-test and 2-month follow-up were compared for intervention group participants. Participants did not show significant differences between these two-time points for almost all outcome variables, including parent-child dysfunctional interaction (B = −0.72, p = .394), difficult child (B = −1.37, p = .192), satisfaction (B = −0.24, p = .777), efficacy (B = 0.13, p = .808), and overreactivity (B = 1.49, p = .143). The only exception was parental distress, which showed a significant decrease over the follow-up period (B = −2.41, p = .012, d = 0.76). These results demonstrate that the effects of the intervention were maintained throughout the 2-month follow-up period, with participants even showing continued decreases in parental distress after the intervention.
Qualitative Results
The qualitative thematic analysis allows for a holistic examination of participants’ experiences of the program. The themes derived from the analysis also extrapolate program components that were conducive to the cultivation of parenting capacity. Participants stated that they felt supported by their peers who shared similar experiences and that the group allowed for collaborative problem-solving to address challenges that they encountered. After the intervention, participants reported changes in their parenting, including an enhanced awareness of their children’s needs, a reduction in their use of negative language in parent-child interactions, and better emotion management. Additionally, participants also reported an enhanced sense of self-efficacy as well as a reduction in parental stress levels as a result of attending the program. These findings underscore the effectiveness of the SSLD Parent Capacity Building Program in fostering positive parental outcomes.
Discussion
Program Efficacy
The SSLD Parent Capacity Building Program stands out from other parent education programs for families with children having SEN due to its integration of in vivo practice sessions within its design. This unique feature offers parents invaluable opportunities to apply acquired knowledge directly into daily parenting practices, thereby strengthening their parenting capacities. Similar to other well-established research-supported parenting programs, this Parent Capacity Building Program has demonstrated efficacy in reducing parental stress, improving parenting behaviors, and enhancing the parent-child relationship (Bloomfield & Kendall, 2012; Brian et al., 2021; Karjalainen et al., 2019). Results from the randomized controlled trial indicated significant improvements in two key areas of parenting measures for the intervention group compared to the control group—intervention group participants were less likely to perceive their children as difficult to manage and were less likely to overreact after the intervention, while no changes were reported by the control group. The results support the efficacy of the program with promising results on key outcomes of parental stress and parenting-child dysfunctional interaction.
However, the intervention group did not exhibit significant changes in their sense of parental competence compared to the waitlist control group, aligning with findings from previous studies (Nicholson et al., 2008; Williams et al., 2012). This outcome may indicate that an increase in parental sense of competence requires a longer duration to manifest alongside the acquisition and application of new parenting skills. Parents may not gain an instant sense of competence after the intervention because developing self-efficacy necessitates ongoing practice and application of learned strategies (Whittingham et al., 2009). This randomized controlled trial did not extend to assessing long-term effects, as ethical considerations prompted the agency to offer the program to the waitlist control group subsequently. Consequently, the relatively short interval between the pretest and post-test limited the study’s ability to capture the program’s enduring benefits. Nevertheless, it is anticipated that with continued practice, parents will progressively experience increased competence over time. Encouragingly, qualitative study findings validate this assumption, with participants indicating feeling more competent and less stressed in managing their children’s behaviors after practicing the program’s approach for over two years.
Given the constraints of the randomized controlled trial and the sample size, pooled analyses were conducted to complement the findings and offer additional insights into the program’s efficacy. Comparing baseline data to immediate post-test results revealed significant improvements in all outcome measures. Specifically, participants reported significant reductions in parental distress, parent-child dysfunction, and perceptions of their child as difficult to manage. This suggests that parents experienced diminished distress in parenting their children, exhibited fewer dysfunctional interactions with their children, and were less likely to perceive their children as challenging to handle following the intervention. Moreover, postintervention assessments indicated that parents displayed decreased tendencies to overreact to their children’s behaviors and reported improved satisfaction and efficacy in their parenting roles. These effects were maintained two months after the intervention, with further reductions observed in parental distress during the follow-up period. Although lacking a control group for comparison, the promising findings provide preliminary support for the program’s efficacy in improving parental stress, parental sense of competence, and dysfunctional parenting styles. These results emphasize the potential benefits of the program in fostering positive parental outcomes, despite the study’s limitations. Further research with larger sample sizes and rigorous study designs is warranted to support these findings and provide deeper insights into the program’s effectiveness.
The qualitative data provided further depth and context to the quantitative results, explaining the mechanisms behind the observed changes. Parents highlighted that the program equipped them with an effective strategy to understand the underlying needs of behavioral challenges through the N3C assessment framework. By mastering this problem translation technique, parents found it less daunting to address their children’s behavioral issues as they could view the challenges from a different perspective. This enhanced parental sensitivity not only facilitated meeting the needs of their children but also improved parent-child interaction, which plays a crucial role in fostering positive parenting and parent-child relationships (Krauthamer Ewing et al., 2019). Parents reported having an enhanced awareness of their children’s needs, a reduction in the use of negative language in parent-child interactions, and better emotional regulation after participating in this program. Research suggests that parents who perceive themselves as more competent and satisfied experience lower stress levels when raising children with SEN (Arellano et al., 2019), further supporting the program’s efficacy.
Additionally, this innovative program design featuring in vivo practice sessions provided invaluable opportunities for applying acquired knowledge and skills to real-life scenarios. This practical experience enabled parents to expand their repertoire of parenting strategies and skills through a collaborative problem-solving process, aligning with previous studies emphasizing the effectiveness of such experiential learning approaches in promoting positive parenting practices and reducing punitive parenting methods (Chung et al., 2022; Sanders, 1999). Furthermore, participants stated feeling supported by peers with similar experiences, fostering a supportive group dynamic conducive to collaborative problem-solving (Rojas et al., 2022). Overall, these qualitative findings underscore the importance of incorporating experiential learning and peer support mechanisms into parent capacity-building interventions for children with SEN.
Limitations and Future Directions
Some limitations should be acknowledged in interpreting the findings of this study. Firstly, the power of the analyses was limited by the sample size. Due to its cluster design, the sample size of each cluster was relatively small (around 50), and it is less efficient, particularly with outcome measures that typically have lower intra-cluster correlations (Hemming & Taljaard, 2016). Additionally, the predominantly Chinese, maternal sample limits the generalizability of the findings. Future research should strive for greater diversity in participant demographics, including single parents and culturally diverse families, and ensure adequate representation of fathers and parents of children with different disabilities. Exploring factors influencing fathers’ participation in such programs and investigating impacts on broader family dynamics, including parent-child and couple relationships, would also enrich our understanding of program outcomes (Rankin et al., 2019; Sharabi & Marom-Golan, 2018).
Another limitation is the absence of fidelity checks, which could have influenced the consistency and quality of program delivery across facilitators, particularly those with varying levels of experience. While efforts were made to ensure protocol adherence through training and supervision, future research could employ consistent facilitators or consider facilitator experience as a covariate in analysis to mitigate this limitation. Further investigation into program fidelity and its impact on outcomes is warranted.
Given the evolving landscape of service delivery, future research could explore the feasibility and effectiveness of delivering the program virtually. Transitioning to an online format may offer immediate support to parents in their home environments, particularly in dynamic circumstances such as those precipitated by global events. Investigating the adaptability and outcomes of the SSLD parenting program in a virtual setting would be an important avenue for future inquiry.
Conclusion
This randomized controlled trial provides preliminary evidence supporting the effectiveness of the SSLD Parent Capacity Building Program for parents of children with SEN. The program facilitates a shift in parental perspective, encouraging parents to perceive presenting problems from alternative viewpoints and enhancing their parenting strategies and skills through collaborative problem-solving. The incorporation of in vivo practice sessions empowers parents to apply learned knowledge and skills directly to their real-life parenting scenarios. After participating in the program, parents reported a reduction in the use of harsh or punitive parenting methods and negative language in parent-child interactions. They also reported better emotional regulation and increased motivation and competence in their parenting role. The SSLD Parent Capacity Building Program offers a valuable resource for parents of children with SEN, providing both practical guidance and emotional support to help alleviate stress and enhance parenting competence. These findings hold significant implications for social work practice, suggesting that the intervention has the potential to positively impact parental well-being and child development outcomes within families of children with SEN. Future research should explore the applicability of the program across diverse populations, investigate additional outcome measures beyond those examined in this study, and provide comprehensive training and supervision to program facilitators. Additionally, given the increasingly digital nature of service delivery, further examination of the program’s efficacy in a virtual format could offer valuable insights for expanding access to supportive interventions for parents in need.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol and all procedures were approved by the Hong Kong Polytechnic University Institutional Review Board (IRB) (Reference number: HSEARS20171023003) This trial was also registered on the International Standard Randomized Controlled Trial Number (ISRCTN36895493) registry, which is a registry recognized by the World Health Organization (WHO).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.