
Abstract
Comparative Efficacy of Online vs. Face-to-Face Group Interventions
The delivery of psychosocial interventions witnessed a transformation in recent years, largely due to the worldwide pandemic. Improved technologies and online platforms offered a new way for individuals to access remote psychosocial interventions. The advantages of online delivery include increased accessibility, reduced geographical barriers, and the flexibility to participate from the comfort of one's own home (Fitch, 2017; Lecomte et al., 2020; Schmidt Hanbidge et al., in press; Stoll et al., 2020). Yet, these conveniences come with challenges and potential limitations, such as concerns about the quality of therapeutic relationships, privacy, and the adaptability of interventions in the digital sphere (Banbury et al., 2018; Gerritzen et al., 2022; Washington et al., 2020; Weinberg, 2020). Additionally, few studies have examined if group work interventions delivered online are as efficacious as those delivered face-to-face (F2F). Practitioners would benefit from knowing which group work interventions may be effective online or in F2F format to guide their selection of interventions. Thus, a critical question is whether the online delivery of psychosocial interventions is as effective as traditional F2F methods.
Current Literature Gap
A search of the published literature (detailed in the methods section), which included the Campbell (https://www.campbellcollaboration.org/), Cochrane (https://www.cochrane.org/), and PROSPERO (https://www.crd.york.ac.uk/prospero/) sites, yielded relevant reviews. Several reviews have compared the efficacy of the two modalities in individually delivered interventions. For example, Carlbring et al. (2018) reviewed 20 studies that examined the comparative effectiveness of F2F Cognitive Behavioral Therapy (CBT) to the online format, finding equal overall effectiveness of the two modalities. Similarly, a systematic review of five studies found comparable effectiveness of online and F2F delivery of psychosocial interventions on anxiety disorder (Krzyzaniak et al., 2024). Another systematic review and meta-analysis of 12 randomized controlled trials (RCTs) that compared F2F and online delivery of psychotherapy for less common mental health conditions also found no significant difference in the studied outcomes between the two modalities (Greenwood et al., 2022).
Systematic reviews have documented that, overall, psychotherapeutic group interventions are effective for people with a range of psychosocial challenges (Burlingame & Jensen, 2017; Rosendahl et al., 2021). Systematic reviews have also examined the effectiveness of group therapy delivered remotely. Banbury et al. (2018) investigated the effectiveness of group therapy delivered through video conferencing (VC) to provide education and social support to clients in home settings in 17 studies. Although they did not compare VC to F2F within their review, Banbury et al. (2018) concluded VC offers comparable effectiveness to results reported for F2F groups. Similarly, in a systematic review of 40 studies, Gentry et al. (2019) concluded that VC delivered CBT groups offered comparable outcomes to the F2F modality. Another systematic review (n = 29) explored the effectiveness of group therapy to ameliorate clinical symptoms of grief and found that online peer support groups can provide emotional relief and increase the sense of control but do not mitigate symptoms such as grief and distress (Robinson & Pond, 2019). However, none of these reviews exclusively focused on including studies designed to compare the effectiveness of similar group interventions when provided online versus F2F.
The recent COVID-19 pandemic accelerated the adoption of online group work interventions and group work authors and organizations developed guides to help practitioners with the online format (Weinberg, 2020). For example, the International Association for Social Work with Groups (IASWG) updated its Standards for Social Work Practice with Groups (IASWG Standards) and included recommendations on adopting technology in providing group-based interventions (IASWG, 2022). Yet, the empirical question remains about how effective online group work is when compared with F2F. Specifically, up to the date of the search, none of the systematic reviews examined if online group work is as effective when compared with similar F2F group interventions. This systematic review aims to synthesize and critically analyze existing empirical evidence from RCTs that compared the efficacy of online versus F2F delivery of similar group-based psychosocial interventions.
Method
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: a) compared in the same study a group-based psychosocial intervention/model (e.g., CBT) delivered in both F2F and online formats, b) utilized an RCT research design, and c) published in English. There was no restriction on population and type of outcome measures. Unpublished studies, dissertations, and grey literature were included.
Studies were excluded if they a) utilized only one modality of intervention (either F2F or online) without a comparison, b) compared interventions with dissimilar models or content, c) involved interventions that were not delivered in a group format, d) were not published in English, e) did not employ an RCT research design and f) utilized a qualitative research design.
Literature Search
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021), a comprehensive literature search was conducted in August 2021 and was later updated in June 2023. The review protocol was registered and published in PROSPERO (Rafieifar et al., 2023).
The university-based databases searched included Medline, APA PsycNet, Web of Science, the Cochrane Library, the ProQuest Dissertations and Theses databases, Pubmed, PsycINFO, WorldCat, Google Scholar, Social Sciences Citation Index, and Open Grey. Keywords were chosen relevant to treatment modality (online vs. face-to-face), treatment type (group therapy), and intervention (to exclude non-intervention studies). The main keywords searched separately and in various combinations included online (Telemedicine* OR Internet* OR online* OR web* OR digital OR videoconferenc* OR video call OR virtual OR technology assisted OR telehealth* OR e-health* OR ehealth* OR tele-health*), Face to Face (Face-to-face OR face to face OR F2F OR in-person OR “in person”), and Group Work (“groupwork” OR “group work” OR “group counsel*” OR “group treatment*” OR “group therap*” OR “group intervention*” OR “group prevention*” OR “group psychotherap*” OR “group approach*” OR “small group” OR “group counseling”).
In alignment with the PRISMA 2020 guidelines (Page et al., 2021), the review process was designed to involve all authors. Initially, a collective agreement was reached on the search terms and the criteria for including and excluding studies. Following this, the lead author executed the search across the selected databases. The search results were then uploaded to Covidence online software program (2019) for screening. Three authors (MR, ASH, and SBL) independently reviewed the titles and abstracts. Subsequently, full-text versions of articles deemed potentially relevant were closely examined by two authors to check their suitability for inclusion. In instances of discrepancies, these were collaboratively discussed and resolved among the four team members, ensuring a unified final decision on the selection of articles for data extraction.
Analytic Strategy
Data Extraction
To facilitate data extraction, the authors developed an Excel master table following the Population, Intervention, Control, Outcome (PICO) framework (Schardt et al., 2007). Sample characteristics, intervention variables, methodological variables, and outcome variables were independently extracted from each article by two authors, with verification conducted by a third author.
Risk of Bias
The authors followed the Cochrane Risk of Bias Assessment Tool for randomized trials (Sterne et al., 2019), assigning “low,” “some concerns,” or “high” bias risk to each study. All four authors were involved in assessing each study's risk of bias. Two authors independently conducted the assessment, and then the complete author team discussed the results for each article to resolve discrepancies through discussion for a final decision by consensus.
Results
As indicated in Figure 1, the search yielded 3,742 articles with 1,685 excluded as duplications. In the title and abstract review stage, an additional 1,677 studies were excluded as not relevant. Out of the 380 articles that remained for closer, full-text screening, 354 studies were excluded for a number of reasons (Figure 1). As a final step, 18 articles were included for review and data extraction. As the data extraction process unfolded, it became evident that among these 18 articles, only 15 encompassed distinct studies and that there were instances where multiple articles reported findings from the same RCTs. For instance, Bulik et al. (2012), Watson et al. (2017), and Zerwas et al. (2017), were derived from a single study. From this group, Zerwas et al. (2017) was chosen because it provided complete data to analyze the outcomes. Similarly, when considering between Greene et al. (2010) and Morland et al. (2010), the latter was deemed the appropriate choice for closer review as it included more detailed data.
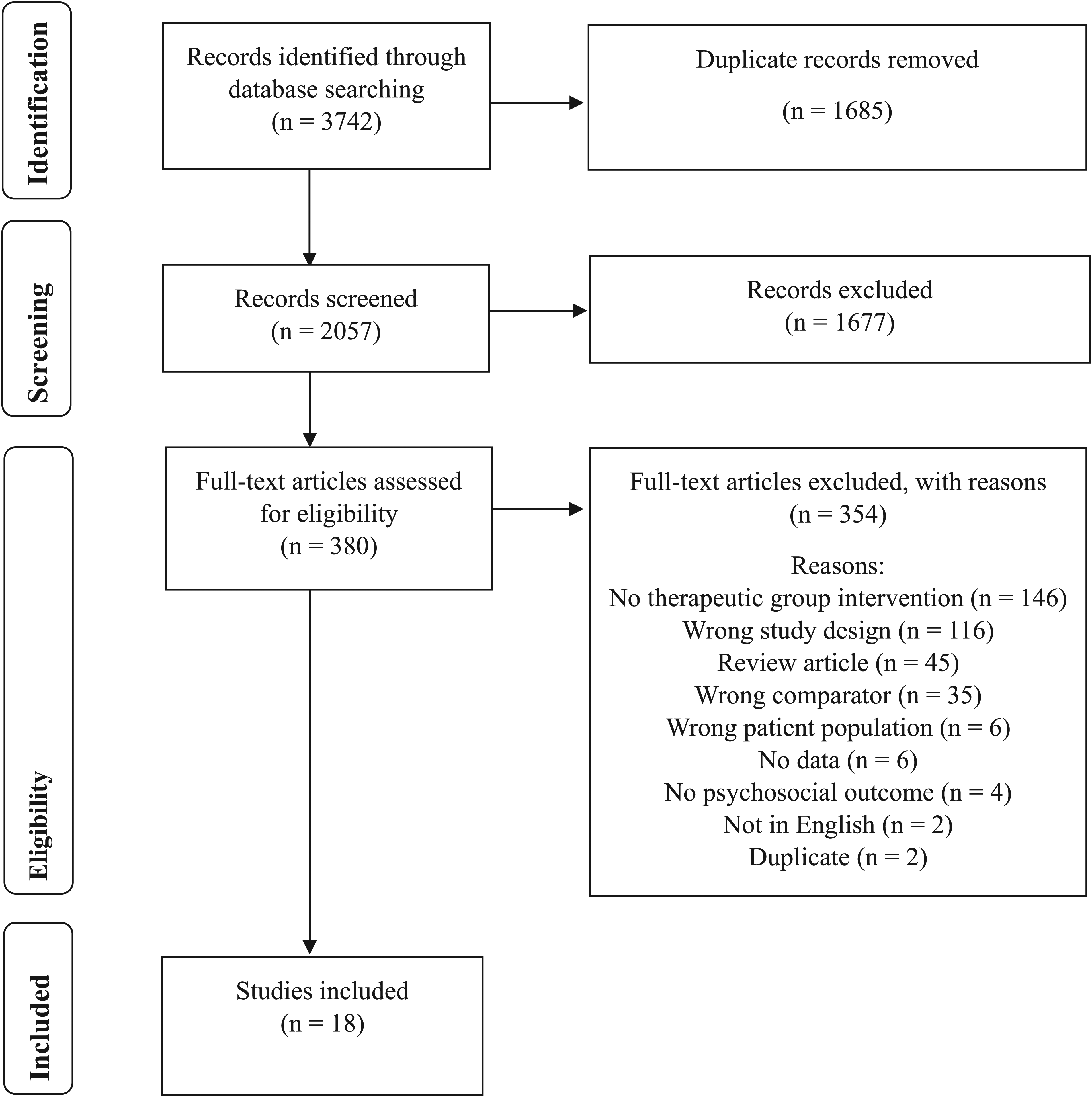
PRISMA flow chart of the study selection process.
Risk of Bias
The authors assessed the studies’ risk of bias using RoB 2, the revised tool for assessing risk of bias in randomized trials (Sterne et al., 2019) for RCTs. As seen in Table 1, only two studies have an overall “low” risk of bias (Morland et al., 2010, 2014). Conversely, seven studies (Andrews et al., 2011; Aspvall et al., 2021; Mayor-Silva et al., 2021; Morland et al., 2011; Rosal et al., 2014; Serdar et al., 2014; Zerwas et al., 2017) are categorized with an overall “some concerns” risk of bias. On the other hand, six studies (Clark et al., 2019; Gollings & Paxton, 2006; Hall et al., 2017; Lleras de Frutos et al., 2020; Morland et al., 2004; Paxton et al., 2007) are identified with a “high” overall risk of bias.
Risk of Bias for Randomized Controlled Trials.
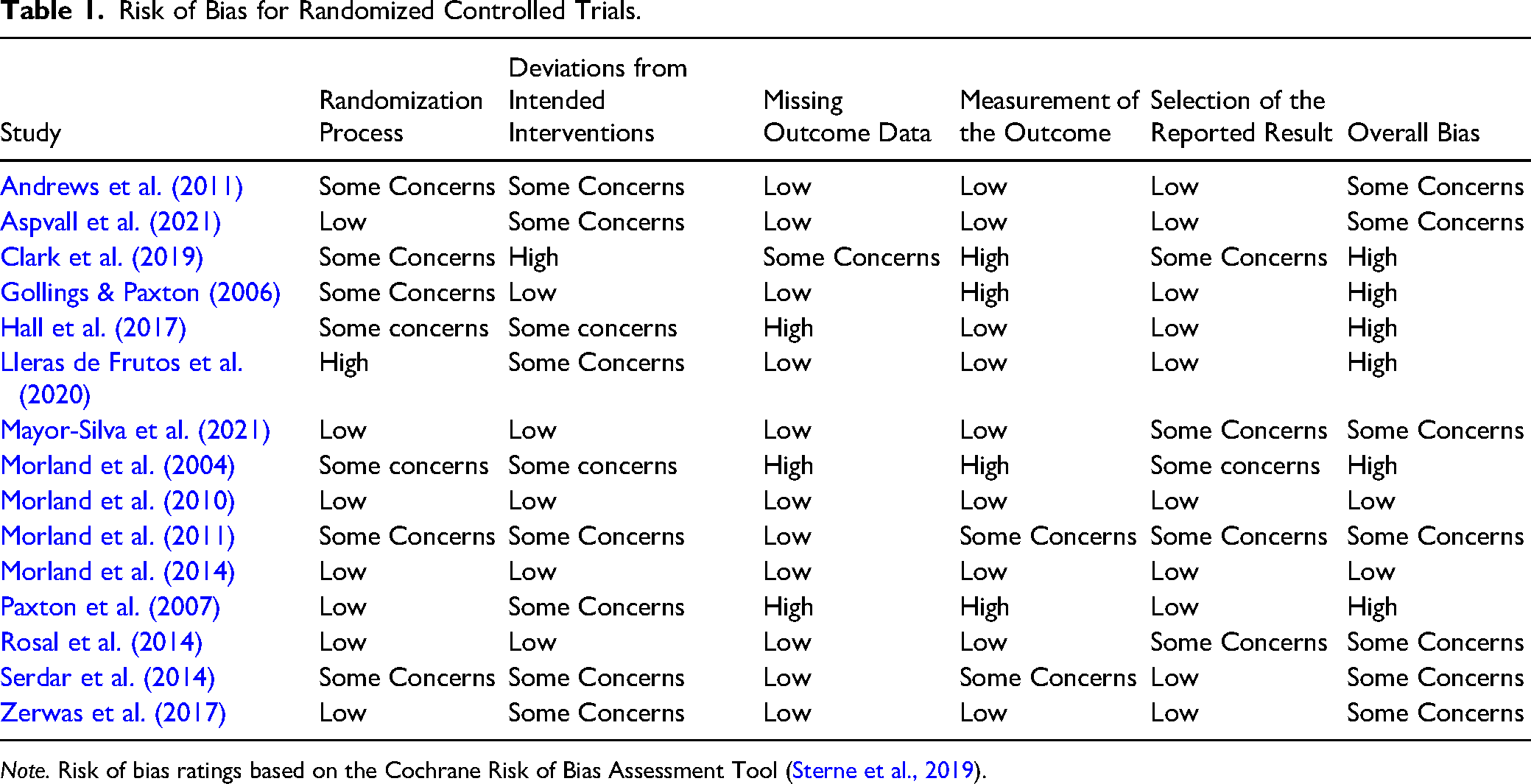
Note. Risk of bias ratings based on the Cochrane Risk of Bias Assessment Tool (Sterne et al., 2019).
Participant Characteristics
As shown in Table 2, the studies (n = 15) were published between 2004 and 2019 and included nine from the US, three from Australia, and two from Spain and Sweden. Over 90% of the studies included adult participants, one evaluated young adults with an average age of over 19 years (Mayor-Silva et al., 2021), and one included children and adolescents with a mean age of 13.4 years (Aspvall et al., 2021). Over one-third of the sample was at least 85% female (Gollings & Paxton, 2006; Hall et al., 2017; Lleras de Frutos et al., 2020; Paxton et al., 2007; Rosal et al., 2014; Serdar et al., 2014; Zerwas et al., 2017). Over two-thirds of the sample (n = 10) did not report data on race or ethnicity. The studies that reported race (n = 6) were all conducted in the US (Clark et al., 2019, Hall et al., 2017; Morland et al., 2010, 2011, 2014, and Zerwas et al., 2017).
Characteristics of the Samples Across Studies.
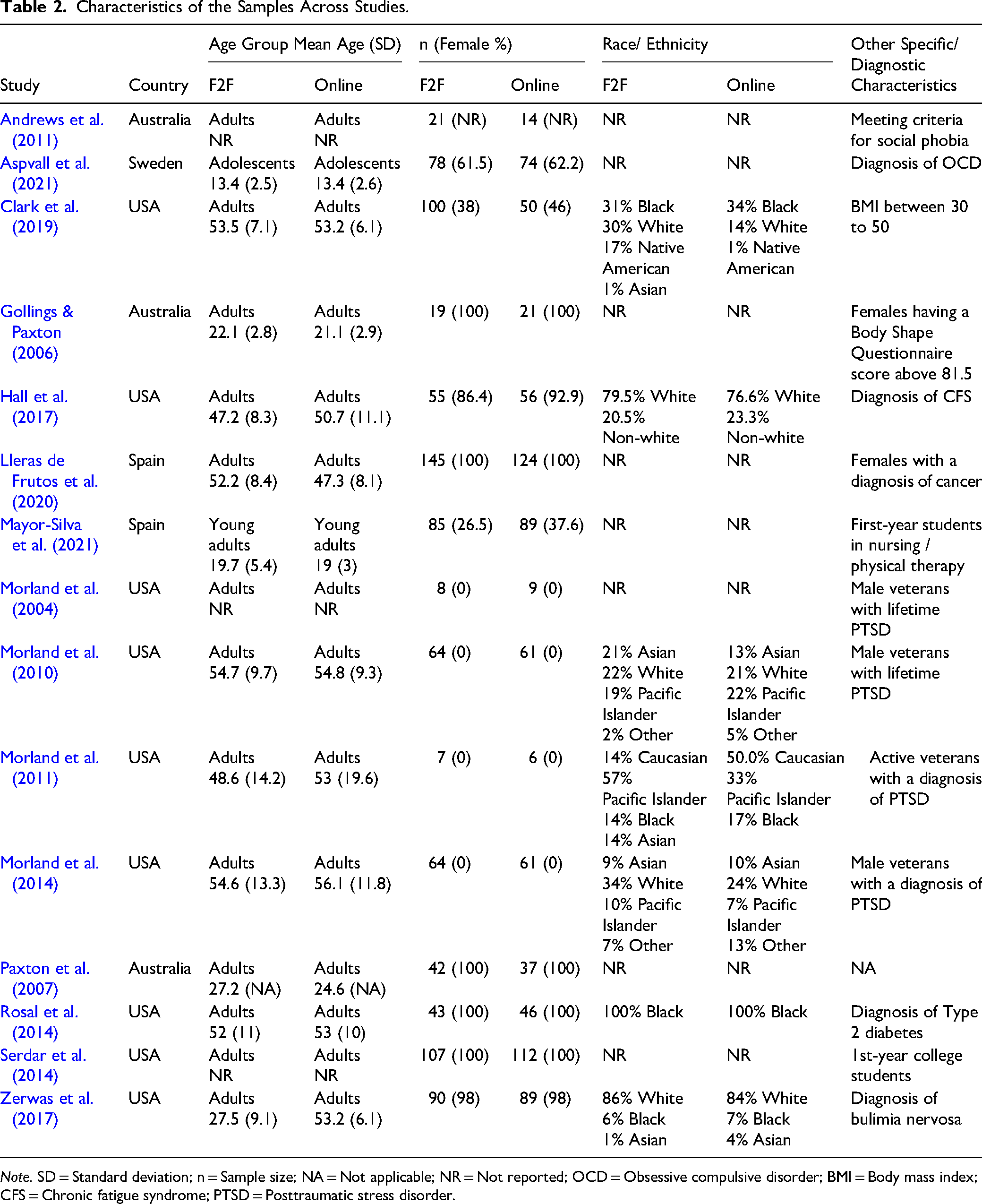
Note. SD = Standard deviation; n = Sample size; NA = Not applicable; NR = Not reported; OCD = Obsessive compulsive disorder; BMI = Body mass index; CFS = Chronic fatigue syndrome; PTSD = Posttraumatic stress disorder.
Intervention Characteristics
Based on the selection criteria, 15 group treatments were included that compared, in the same study, a group intervention delivered in two delivery formats, online and F2F (Table 3). CBT was the targeted intervention model for 11 studies (CBT, CPT, or CBT-based therapies), one intervention was nutrition and exercise focused (Clark et al., 2019), another utilized positive psychology model (Lleras de Frutos et al., 2020), one study identified coping skills psychoeducation (Morland et al., 2004) while a final study offered dissonance-based prevention (Serdar et al., 2014). In 11 studies, manualized interventions were utilized, with eight referencing the manuals, as demonstrated in Table 3. Notably, four studies (Andrews et al., 2011; Clark et al., 2019; Hall et al., 2017; Mayor-Silva et al., 2021) did not specify the use of a manualized intervention.
Intervention Characteristics.
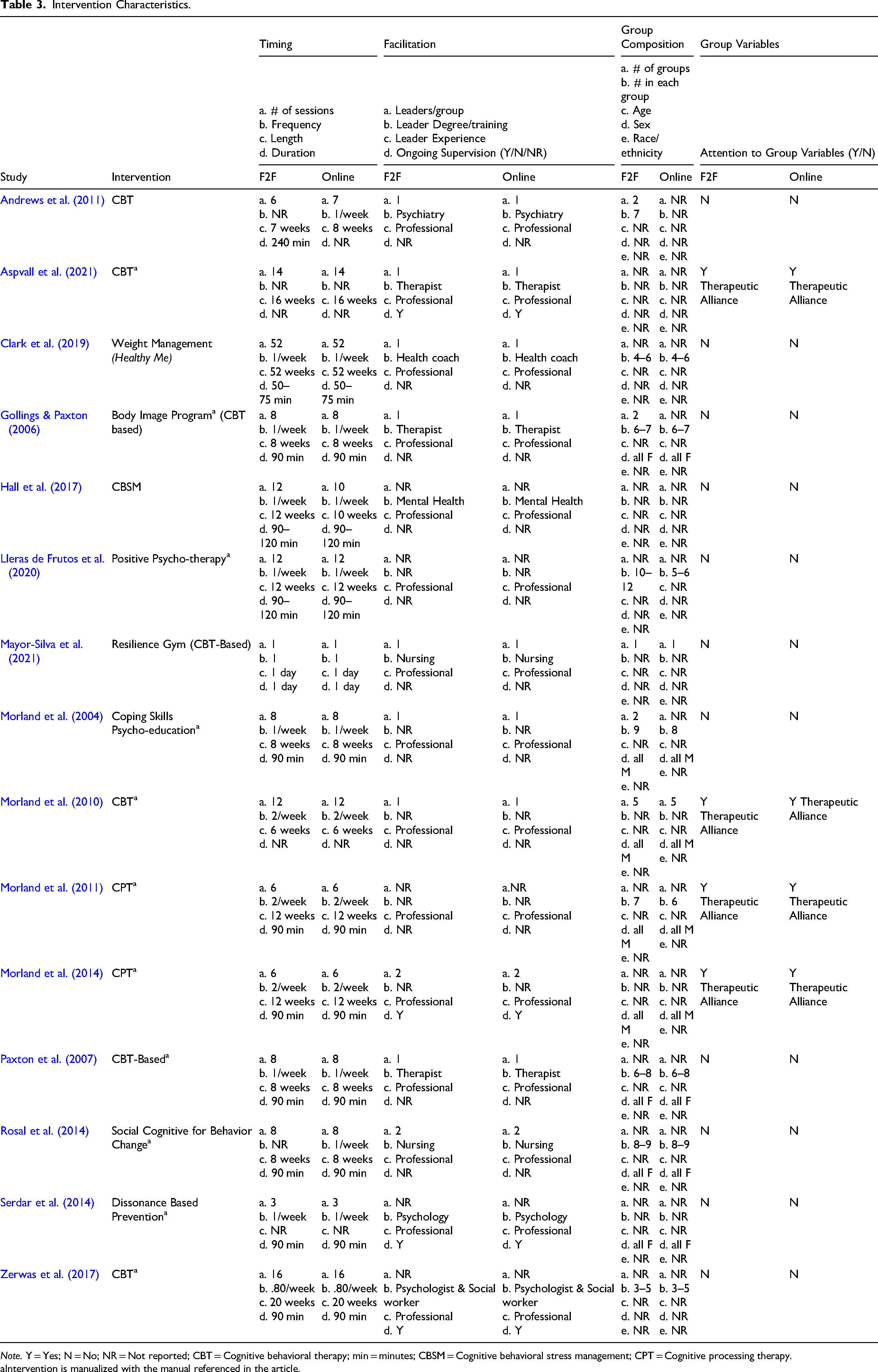
Note. Y = Yes; N = No; NR = Not reported; CBT = Cognitive behavioral therapy; min = minutes; CBSM = Cognitive behavioral stress management; CPT = Cognitive processing therapy.
Intervention is manualized with the manual referenced in the article.
Interventions described the frequency of sessions for both F2F and online, which included a wide range from a single session (Mayor-Silva et al., 2021) to as many as 52 sessions (Clark et al., 2019) (Table 2). While most interventions had the identical number of F2F and virtual sessions, two interventions varied in number where Andrews et al. (2011) offered 6 F2F to 7 online sessions, and Hall et al. (2017) offered 12 F2F compared to 10 online sessions.
All studies included closed group interventions (no new members after the first session). Group treatment sessions were offered F2F and virtually once weekly by eight of the studies, while three treatments were offered twice weekly (Morland et al., 2004, 2011, 2014). Three studies did not report on the frequency of F2F sessions (Andrews et al., 2011; Aspvall et al., 2021; Rosal et al., 2014), while one study (Mayor-Silva et al., 2021) offered a single session treatment for a full day. The length of both F2F and online sessions were mostly 90 min, while one study (Mayor-Silva et al., 2021) was a full day event, and another reported 50 −75-min sessions (Clark et al., 2019) and two studies were 90–120 minutes in length (Hall et al., 2017; Lleras de Frutos et al., 2020). Two studies (Aspvall et al., 2021; Morland et al., 2010) did not report on their session length.
Several studies offered insights into group characteristics and addressed factors relevant to the group, either through their intervention strategies or statistical approaches. As indicated in Table 3, some studies provided descriptive details regarding group sizes, composition, and leader characteristics. Group sizes varied, with the number of participants ranging from 3–12 individuals, whereas nine studies did not report on the number in each group. The number of individuals was comparable between the F2F and online groups except for the Lleras de Frutos et al. (2020) treatment, where the size of the F2F treatment had twice the number of members. The composition of each group was reported by 12 of the 15 studies.
All studies reviewed indicated the groups were facilitated by professionals rather than peer/lay workers. A range of health professionals provided group facilitation, including therapists (3), psychologists (2), mental health coaches (2), nurses (2), psychiatrists (1), and social workers (1). Five studies did not report on the profession of the group facilitators (Lleras de Frutos et al., 2020; Morland et al., 2004, 2010, 2011, 2014). Four studies reported that the group facilitators had ongoing supervision for both the online and F2F groups (Aspvall et al., 2021; Morland et al., 2014; Serdar et al., 2014; Zerwas et al., 2017), whereas 11 studies did not report on this.
Most studies (n = 11) provided no information about group variables (e.g., structures, processes). Of the group treatments delivered, only four of the fifteen studies (Aspvall et al., 2021; Morland et al., 2010, 2011, 2014) explored therapeutic alliance for both online and F2F groups. All four studies used CBT-based interventions and except for one (Morland et al., 2010), all found comparable levels of therapeutic alliance between the two modalities. Morland et al. (2010) found significantly higher group therapy alliance in F2F group.
All studies compared attendance and treatment adherence on both modalities except for two articles (Andrews et al., 2011; Clark et al., 2019). The majority of the studies (n = 11) reported no significant differences between conditions regarding treatment attrition. However, there were exceptions. In the study by Zerwas et al. (2017), which involved a CBT intervention, there were high dropout rates observed in both modalities, with the online format showing a higher attrition rate compared to F2F. Conversely, Morland et al. (2004), who utilized coping skills psychoeducation, found a significant level of attrition in the F2F format.
Only five studies compared participants’ satisfaction. Four (Morland et al., 2004, 2010, 2014; Rosal et al., 2014) found no significant difference between the two modalities, and one (Zerwas et al., 2017) found F2F participants more satisfied than those who attended online treatment. No study assessed and discussed technology usability in online groups. Only three studies discussed the comparative cost-effectiveness of the two modalities (Andrews et al., 2011; Aspvall et al., 2021; Rosal et al., 2014), with one finding online to be more costly (Rosal et al., 2014) and the other two finding it less costly (Andrews et al., 2011; Aspvall et al., 2021). It is worth noting that in the case where online therapy was deemed more expensive, the intervention involved the utilization of virtual reality technology, which necessitated a higher level of technological infrastructure.
Methodological Characteristics
As detailed in Table 4, all publications used a between group comparison including F2F to online conditions in RCTs. In four instances, the studies incorporated a third comparison condition alongside online and F2F group treatments. These conditions included enhanced usual care (Gollings & Paxton, 2006), a waitlist (Paxton et al., 2007), and two no-treatment control conditions (Mayor-Silva et al., 2021; Serdar et al., 2014). The online interventions were delivered with different timing parameters including synchronously or asynchronously. Additionally, the modalities of the online condition varied. For example, some studies included synchronous video conferencing (Clark et al., 2019; Lleras de Frutos et al., 2020; Morland et al., 2004, 2010, 2011 & 2014), while others provided text-based chat groups (Aspvall et al., 2021; Serdar et al., 2014), or the virtual world (Rosal et al., 2014). One study included asynchronous educational modules, with a group chat option through short messaging service (SMS) (Andrews et al., 2011).
Methodological Characteristics of the Studies.
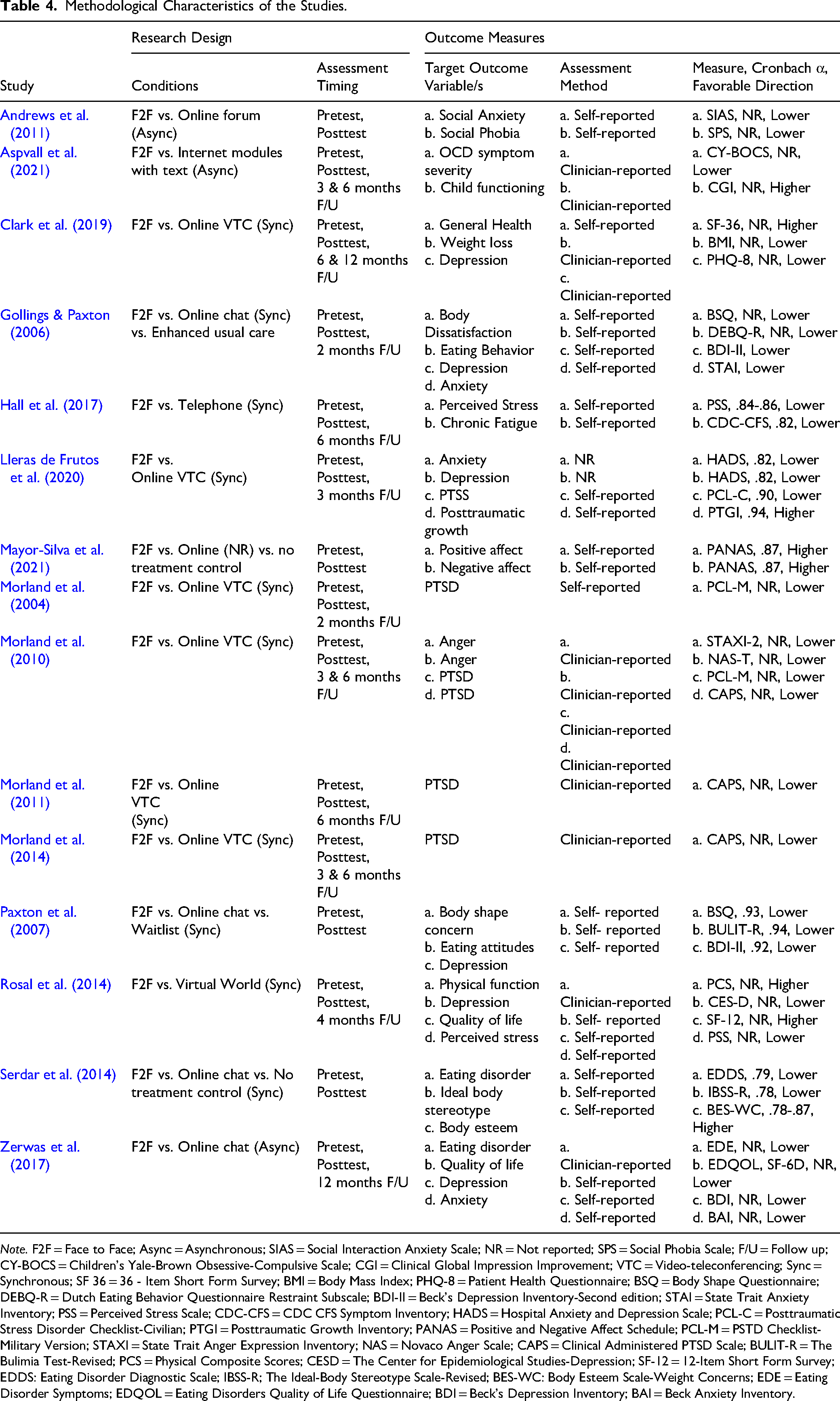
Note. F2F = Face to Face; Async = Asynchronous; SIAS = Social Interaction Anxiety Scale; NR = Not reported; SPS = Social Phobia Scale; F/U = Follow up; CY-BOCS = Children's Yale-Brown Obsessive-Compulsive Scale; CGI = Clinical Global Impression Improvement; VTC = Video-teleconferencing; Sync = Synchronous; SF 36 = 36 - Item Short Form Survey; BMI = Body Mass Index; PHQ-8 = Patient Health Questionnaire; BSQ = Body Shape Questionnaire; DEBQ-R = Dutch Eating Behavior Questionnaire Restraint Subscale; BDI-II = Beck's Depression Inventory-Second edition; STAI = State Trait Anxiety Inventory; PSS = Perceived Stress Scale; CDC-CFS = CDC CFS Symptom Inventory; HADS = Hospital Anxiety and Depression Scale; PCL-C = Posttraumatic Stress Disorder Checklist-Civilian; PTGI = Posttraumatic Growth Inventory; PANAS = Positive and Negative Affect Schedule; PCL-M = PSTD Checklist- Military Version; STAXI = State Trait Anger Expression Inventory; NAS = Novaco Anger Scale; CAPS = Clinical Administered PTSD Scale; BULIT-R = The Bulimia Test-Revised; PCS = Physical Composite Scores; CESD = The Center for Epidemiological Studies-Depression; SF-12 = 12-Item Short Form Survey; EDDS: Eating Disorder Diagnostic Scale; IBSS-R; The Ideal-Body Stereotype Scale-Revised; BES-WC: Body Esteem Scale-Weight Concerns; EDE = Eating Disorder Symptoms; EDQOL = Eating Disorders Quality of Life Questionnaire; BDI = Beck's Depression Inventory; BAI = Beck Anxiety Inventory.
The studies used self-report measurements at various times in the data collection process. Almost all publications included pretest/posttest measures; however, Mayor-Silva et al. (2021) uniquely assessed outcomes post treatment. For those studies that provided follow up assessment, the shortest follow up assessment period was at two months posttest (Gollings & Paxton, 2006) and the longest duration was 12 months (Clark et al., 2019; Zerwas et al., 2017).
Stress was the most frequently assessed psychosocial outcome, which was measured in eight studies (Hall et al., 2017; Lleras de Frutos et al., 2020; Mayor-Silva et al., 2021; Morland et al., 2004, 2010, 2011, 2014; Rosal et al., 2014). Among these, four studies focused on posttraumatic stress disorder (PTSD) (Morland et al., 2004, 2010, 2011, 2014). Depression was the second most frequently measured outcome which was assessed in four publications (Clark et al., 2019; Gollings & Paxton, 2006; Zerwas et al., 2017), and anxiety was the third most frequently measured (Andrews et al., 2011; Gollings & Paxton, 2006; Zerwas et al., 2017). Although some of the outcomes (stress, depression, and anxiety) measured across the studies were consistent, the tools used to assess the outcome differed (see Table 4 for the assessments used).
Within Condition Effect Sizes
Table 5 displays the effect sizes within each condition, calculated for individual outcomes in both F2F and online settings during the posttest and, when applicable, the last follow-up period. Several studies lacked sufficient data for the recalculation of effect sizes (Clark et al., 2019; Lleras de Frutos et al., 2020; Mayor-Silva et al., 2021; Morland et al., 2004, 2011; Zerwas et al., 2017). For these studies, the effectiveness of online and face-to-face interventions was reported, as the original article concluded.
Within Condition Effect Sizes.
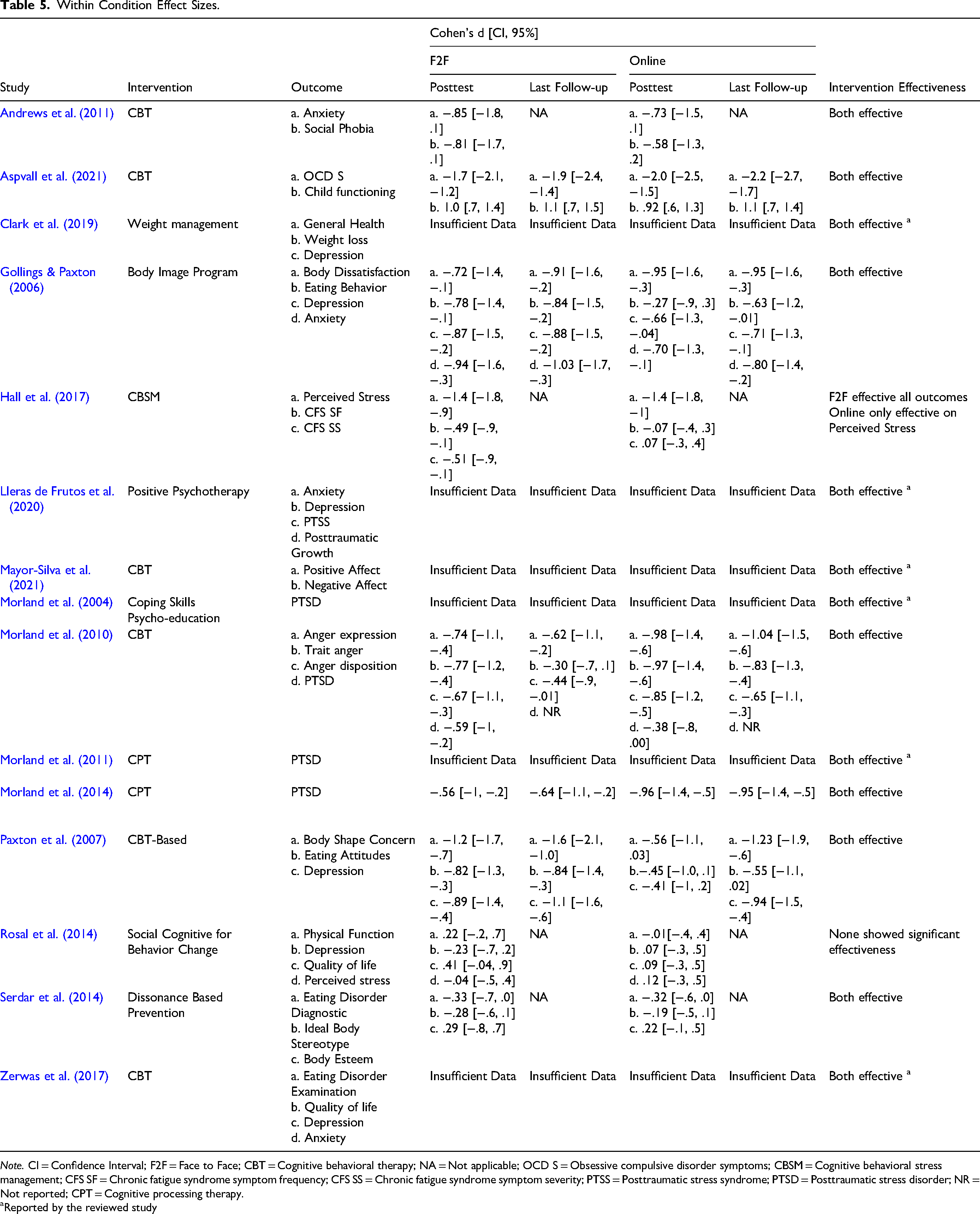
Note. CI = Confidence Interval; F2F = Face to Face; CBT = Cognitive behavioral therapy; NA = Not applicable; OCD S = Obsessive compulsive disorder symptoms; CBSM = Cognitive behavioral stress management; CFS SF = Chronic fatigue syndrome symptom frequency; CFS SS = Chronic fatigue syndrome symptom severity; PTSS = Posttraumatic stress syndrome; PTSD = Posttraumatic stress disorder; NR = Not reported; CPT = Cognitive processing therapy.
Reported by the reviewed study
Most studies demonstrated the effectiveness of both online and F2F interventions, with calculated effect sizes spanning from small to exceptionally large. One study, Rosal et al. (2014), which employed a cognitive behavioral stress management intervention, neither the F2F nor the online modality significantly improved the reported outcomes, including physical function, depression, quality of life, and perceived stress. Another study, Hall et al. (2017), which used a social cognitive framework for behavior change, reported that the online intervention was successful only in reducing perceived stress. However, it failed to improve chronic fatigue syndrome symptom severity and frequency.
Between Condition Effect Sizes
As displayed in Table 6, between condition effect sizes were recalculated for posttest and follow up, when applicable. Among the studies reviewed, a subset (Clark et al., 2019; Lleras de Frutos et al., 2020; Morland et al., 2011) lacked sufficient data to compute the between-condition effect sizes. In our calculations, a negative sign in effect size shows that F2F modality was more effective in improving outcome measures. Conversely, a positive sign indicates the online modality's greater efficacy. However, our assessment of the statistical significance of these differences hinged upon the reported results in the original studies. Most studies yielded nonsignificant differences in effectiveness between intervention modalities (online vs. F2F). Three studies (Hall et al., 2017; Paxton et al., 2007; Rosal et al., 2014) reported superior effectiveness in some outcomes associated with the F2F delivery of interventions compared to the online modality. Hall et al. (2017) found that while both F2F and online interventions were equally effective in reducing perceived stress, F2F was superior in lessening the severity and frequency of chronic fatigue syndrome symptoms. Paxton et al. (2007) found that F2F intervention was more effective than online at immediate posttest in addressing body shape concern, eating attitudes, and depression, but this advantage was not evident at follow-up. Lastly, Rosal et al. (2014) observed a greater effectiveness of F2F interventions in reducing depression but found no significant difference between F2F and online modalities in terms of improving physical function, quality of life, or perceived stress.
Between Group Effect Sizes.
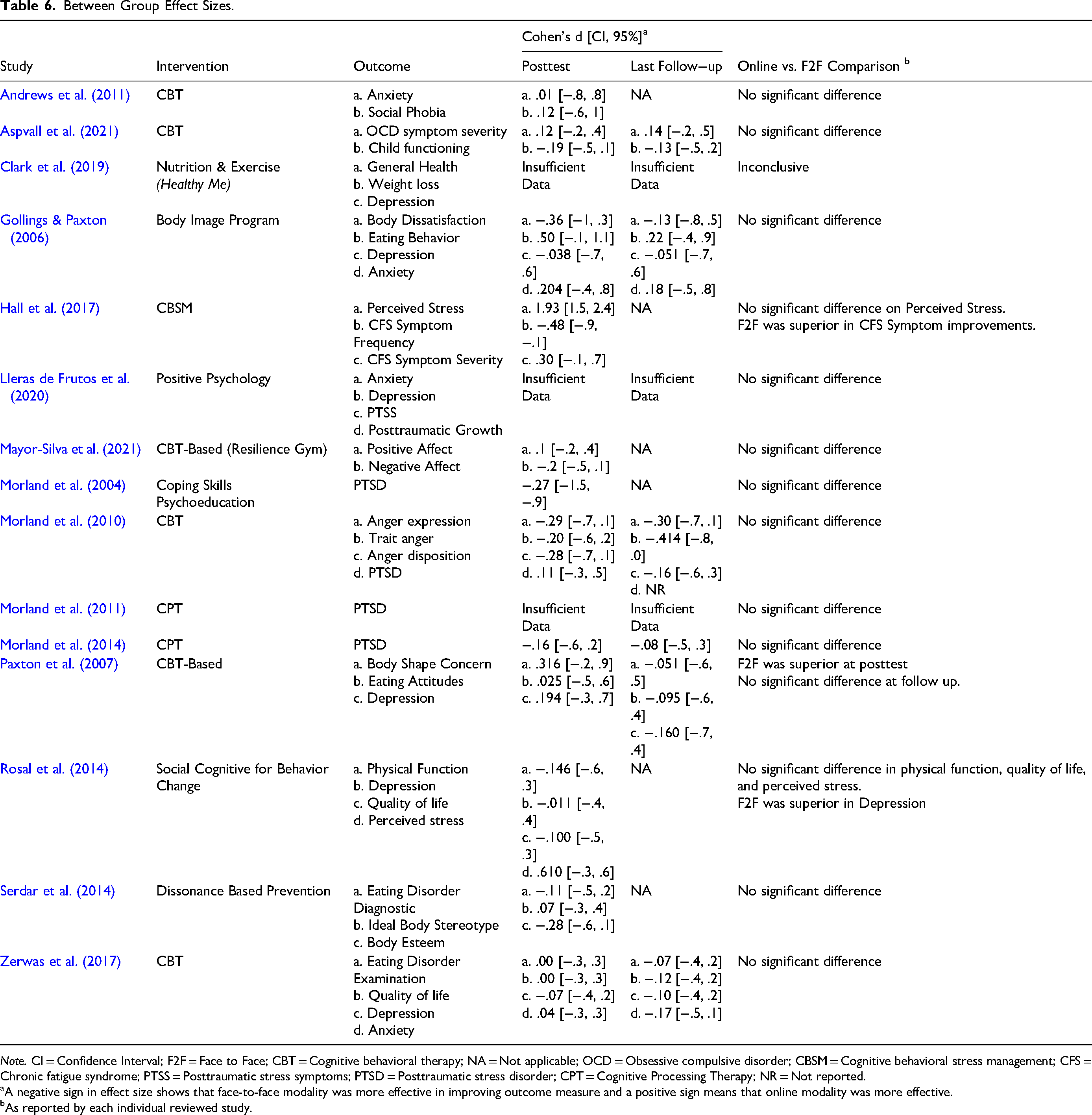
Note. CI = Confidence Interval; F2F = Face to Face; CBT = Cognitive behavioral therapy; NA = Not applicable; OCD = Obsessive compulsive disorder; CBSM = Cognitive behavioral stress management; CFS = Chronic fatigue syndrome; PTSS = Posttraumatic stress symptoms; PTSD = Posttraumatic stress disorder; CPT = Cognitive Processing Therapy; NR = Not reported.
A negative sign in effect size shows that face-to-face modality was more effective in improving outcome measure and a positive sign means that online modality was more effective.
As reported by each individual reviewed study.
Discussion and Application to Practice
This systematic review focused on research that examined the comparative effectiveness of F2F to online delivery of therapeutic group work interventions. Because of the diversity of outcomes, a meta-analysis to quantitatively synthesize the results was not possible. Through a systematic search, extraction, and analysis process that yielded 15 RCTs, interventions were examined that delivered a similar program in person and online. With the exception of Rosal et al. (2014), both F2F and online delivery of group interventions were effective in improving study outcomes, and most online interventions were at least comparable in outcomes to F2F approaches. The studies reported decreased symptoms for a range of presenting issues, including PTSD (Morland et al., 2004, 2010, 2011, 2014), bulimia (Zerwas et al., 2017), cancer (Lleras de Frutos et al., 2020), and social phobias (Andrews et al., 2011). In two studies, online interventions were less effective than F2F modalities for certain outcomes: Hall et al. (2017) found online interventions less effective for chronic fatigue syndrome symptoms’ severity and frequency, and Rosal et al. (2014) for depression. Additionally, Paxton et al. (2007) reported F2F superiority over online at posttest, but this advantage was not sustained at follow-up.
The findings are congruent with those of earlier studies of non-group interventions, which reported comparable effects between online and F2F (Carlbring et al., 2018; Esfandiari et al., 2021; Kambeitz-Ilankovic et al., 2022; Krzyzaniak et al., 2024). CBT was the common model across several studies with promising outcomes such as PTSD, stress, and depression. Most interventions were manualized, which may have helped the transition of F2F interventions to the online format. An implication for practice is that such manualized interventions for online delivery may facilitate a smoother transition for therapists.
Most studies revealed no significant differences between online and F2F modalities in terms of attendance and treatment attrition. This finding has important implications for practice, suggesting a level of flexibility in choosing the mode of delivery without compromising participant retention. It indicates that online interventions can be as effective as traditional F2F sessions in maintaining engagement, thus offering a viable alternative for individuals who may face barriers to in-person attendance. This could lead to broader accessibility of interventions, particularly for those in remote areas, with mobility issues, or with time constraints, ultimately expanding the reach and impact of various therapeutic and intervention programs.
Most studies had either some concerns (n = 7) or a high (n = 6) risk of bias, reducing confidence that the interventions were largely responsible for observed changes. Only two studies showed a low risk of bias (Morland et al., 2010, 2014). Incomplete reporting of methods and results was noted in several studies. More rigorously designed and implemented RCTs are needed. Future research should include at least two group variables, along with control conditions or treatment-as-usual (TAU) to assist interventionists in decision making for their specific group. RCTs that focus on core components with control conditions, especially those developed by social workers, are limited (Goddard-Eckrich et al., 2023). Another common design issue was limited follow-up times. Follow-ups of 6-months and one-year would deepen the evidence and help inform group work practice (Andersson et al., 2018).
Much of the data collected used self-reports, which raises concerns about validity, and the use of different measures of the same outcome across studies. Efforts for future research should include the use of similar, standardized, measurement tools to allow for comparisons between studies examined with the same outcomes.
Most studies evaluated intervention outcomes rather than the process and structures of the group interventions, which would help inform practice. Our findings resonate with the general concern around inadequate reporting of group-related variables and insufficient attention to examining how these variables impact the processes and results (Burlingame et al., 2004, 2013; Miles & Paquin, 2014; Rafieifar & Macgowan, 2022). This lack of adequate discussion on group structures and processes impacts the ability to deeply understand the group dynamics or guide the design and implementation of future group interventions, especially in an online format. For example, only four studies (three conducted by the same research team) measured group therapeutic alliance (Aspvall et al., 2021; Morland et al., 2010, 2011, 2014), which holds valuable data for interventions and clinicians (Baier et al., 2020; Fluckiger et al., 2018). Employing measures of group variables such as alliance, cohesion, or engagement (Burlingame et al., 2018; Macgowan & Newman, 2005) enables clinicians to better identify the group process elements for the most effective treatment response.
Most studies lacked information about group composition, group format, and group clinicians/therapists. Group composition information such as number of members, gender, race, and ethnicity helps practitioners determine an effective match to their groups (Northen & Kurland, 2001). Information on group format, such as if the groups are open (i.e., always adding new members) or closed to new members after the first session, is needed. Who delivered the groups is also important to note, including the use of single or co-leadership. Specific training, supervision, experience, and educational levels of group therapists should be included so practitioners can know if they are qualified or in need of additional training or staffing to deliver such interventions. There is also evidence that group members have been more accepting of online group therapy than therapists (Botta et al., 2021; Fogler et al., 2020; Gullo et al., 2022). A survey of 307 group therapists who transitioned to online work during COVID-19 showed less satisfaction with online therapy as compared to F2F (Gullo et al., 2022). Exploring the factors influencing therapist satisfaction in online therapy and ways to enhance their experience could provide valuable insights for practice.
Most studies employed CBT interventions. There is a need for further investigation into other common models used to gain a better understanding of a wider range of online interventions. Only a few studies examined the costs of interventions. Evaluations that measure and compare costs of interventions would be useful, as resources are often limited and typically finite in not-for-profit human service organizations. Cost effectiveness can be one motivator for organizations and clinicians for their selection of group-based interventions.
This systematic review has limitations. First, only RCTs were included, which excluded other quantitative designs and qualitative studies. Second, all studies were in English, undertaken in high-income countries, which limited the usefulness or transferability of findings to low- or middle-income countries with other languages or limited health care options.
In sum, the review aimed to answer the research question whether online delivery of psychosocial interventions is as effective as the traditional F2F methods. The evidence from the studies in this review suggested that both online and F2F modalities were beneficial, and most studies showed comparable outcomes across modalities. Given the proliferation of interventions into the online format, much more controlled research is needed, which attends to both processes and outcomes, to help guide practitioners.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.