
Abstract
Social work is one of the largest health and social service professions in Canada with approximately 52,823 social workers across the country, making it the third most prevalent health care profession after nurses and physicians (Canadian Institute for Health Information, 2020). Social workers have historically had a broad scope of micro and macro practice with roles in many areas including research, teaching, program evaluation, policy, leadership, and community organization. The Canadian Association of Social Work (CASW) defines social work as a “practice-based profession” that “responds to the needs of individuals, families, groups, and communities” with a focus on “improving health and social well-being,” and a “pursuit of social justice” (CASW, 2020, para. 1–2). Social work practice impacts diverse populations and is provided across different sectors including health care (Ashcroft et al., 2019; Craig et al., 2020), mental health and addictions, child welfare, private practice, and many other areas of specialization (Edwards et al., 2006; Ontario Association of Social Workers [OASW], 2018; Salsberg et al., 2017). There are a range of modalities in social work practice including case management, support services, individual, family, and group therapy or counseling, crisis services, supervision, community organization, policy development, and advocacy (CASW, 2020; IFSW, 2022).
While macro or indirect practice is a core part of social work education and training (CASWE-ACFTS, 2021a; 2021b), most social workers are employed in positions where they engage in direct or clinical social work practice (Edwards et al., 2006; Hare, 2004; Salsberg et al., 2020). There are limited Canadian statistics, but an American workforce survey of Master of Social Work (MSW) graduates (N = 3400) showed that only 7.5% of MSW graduates are doing macro practice (Salsberg et al., 2020). The Association of Social Work Boards (ASWB, 2018) defines clinical social work practice as “the application of specialized clinical knowledge and advanced clinical skills in the areas of assessment, diagnosis and treatment of mental, emotional, and behavioral disorders, conditions and addictions” (p. 6). The National Association of Social Workers (NASW) describes clinical social workers as the largest behavioral health practitioners in the United States (U.S.) with a “primary focus on the mental, emotional, and behavioral well-being of individuals, couples, families, and groups” (NASW, 2005, p.7). The CASW (2020) is a national federation that consists of 10 provincial and territorial associations and while it does not include a definition of clinical social work in its scope of practice statement, it describes “delivery of clinical services” using “culturally responsive practice that applies an anti-oppressive lens to all areas of practice” (para. 1–4). It also notes the importance of social worker competency through supervision, self-reflection, and ongoing professional development and training.
While the profession of social work in Canada has a history that spans more than 100 years (Jennissen & Lundy, 2011; Johnstone & Lee, 2020), a recent trend is the regulation of social work with the aim of increasing ethical practice and public protection (ASWB, 2021; Birnbaum & Silver, 2011). In Canada, professions are regulated provincially and most are self-regulating (Adams, 2016; Edwards et al., 2006). The Canadian Council on Social Work Regulators (CCSWR, 2012) which includes provincial and territorial social work regulators across the country, notes that professional regulation protects the public through oversight of qualifications, competence, and fitness to practice. Although the most common form of social work practice in Canada is direct or clinical practice, few Canadian provinces have a clinical social work designation, but all jurisdictions include clinical services in the scope of practice (CASW, 2020) with minimal and inconsistent standards for clinical practice across the country. A survey by the CCSWR (2012) found that entry level social workers do not have adequate clinical practice training and are also lacking in clinical knowledge and skills.
This article is a critical analysis of the regulation of clinical social work practice in Canada. The authors of this article hold a wide variety of roles (e.g., research, leadership, teaching, and practice) with diverse cultural identities from different parts of Canada. One unifying element is that all the authors are social workers with many years of clinical experience in Canada, U.S., and other parts of the world. Across the team of authors, there has been involvement in social work regulation, association, education, and accreditation. This article analyzes clinical social work practice in Canada by examining various forms of research literature with a specific focus on grey literature available through provincial regulatory bodies. The first section of the article will contextualize social work practice in Canada by providing an overview of the Canadian landscape and a brief historical account of the social work profession in Canada. The following section describes Canadian social work regulatory bodies, compares registration requirements and entrance exams across provinces and territories, as well as an examination of specific designations such as clinical social work practice and controlled acts such as psychotherapy and diagnosis. The subsequent sections focus on important aspects of clinical social work practice including supervision, continuing education, technology, and private practice. The next section examines how social work regulatory bodies are addressing diversity, equity, reconciliation, racism, and discrimination. The last section is the discussion and applications to practice section which synthesizes the state of regulation of clinical social work practice across Canada with recommendations to strengthen clinical social work practice.
Understanding the Canadian Context and Social Work Practice
Canada is a vast country that comprises 10 provinces and three territories. As of July 2021, the population of Canada is estimated to include over 38,000,000 people (Statistics Canada, 2021). The name Canada comes from the Huron-Iroquois word Kanata meaning village or settlement (Government of Canada, 2020; First Nations University of Canada, 2020). Indigenous peoples are the original inhabitants of the land and include First Nations, Inuit, and Métis people (Baskin & Sinclair, 2015). In 2016, Indigenous peoples comprised 4.9% of the population of Canada (Statistics Canada, 2017). White settler colonialism has caused atrocities, trauma, and cultural genocide for Indigenous peoples in Canada (Lee & Johnstone, 2021; Simpson, 2016). Approximately 150,000 Indigenous children were separated from their families and placed by force in residential schools (Rose et al., 2018; Sinclair, 2019). Scholars note that social workers were complicit with these harmful government policies and practices (Sinclair, 2019). Blackstock (2009) writes that little was done by social service or human rights groups to stop residential schools or to disrupt colonial policies. The role of early Canadian social work was described as emerging under dominant colonial policies in which Canada was fast changing with state-initiated recruitment (but active control) of racialized immigrants and the seclusion and cultural genocide of Indigenous peoples (Johnstone & Lee, 2020). To better understand how to reconcile the harm and improve clinical social work practice in Canada in the present day, it is important to understand how social work has perpetrated harms for many communities (Blackstock, 2009). Blackstock (2009) argues that there are inaccurate assumptions that professional practice standards, codes of ethics, and knowledge of anti-oppressive practice will prevent social workers from causing harm (Blackstock, 2009). Others have held hope that registration, professionalization, and professionalism create safer practice, increase accountability, and improve public perceptions of social work practice (Staniforth et al., 2022).
There have been criticisms about the lack of national standards and competencies for entry-level social workers in Canada (Bogo et al., 2011). Establishing social work competencies in Canada has been limited and divisive with concerns about this reinforcing managerialism, neoliberalism, power and control, and a reductionist approach (Brown et al., 2022). There are also concerns about professional suitability or competence among social workers and this is particularly salient when considering the minimal requirements for membership/licensure to many regulatory bodies which places social work programs in a gatekeeping role of determining that those minimum standards are met by graduates (Birnbaum & Lach, 2014).
Regulation and Clinical Social Work Practice in Canada
Regulation, Association, and Education
Social work in Canada is regulated by provincial or territorial law and regulatory bodies which establish title protection, admission requirements, ethical guidelines, standards of practice, continuing education, and supervision requirements, as well as a process and measures for complaints and discipline (ASWB, 2018; Birnbaum & Silver, 2011; CASW, n. d.). The ASWB (2017) is an overarching non-profit organization dedicated to social work regulation and a vision for all social workers to be licensed “to advance safe, competent, and ethical practices to strengthen public protection” (p.2). The ASWB is composed of members from all 10 Canadian provinces, all 50 states in the U.S., including the District of Columbia (DC), Guam, and the Northern Mariana Islands. Moreover, the ASWB owns, develops, and maintains social work licensing exams used in the U.S. and Canada.
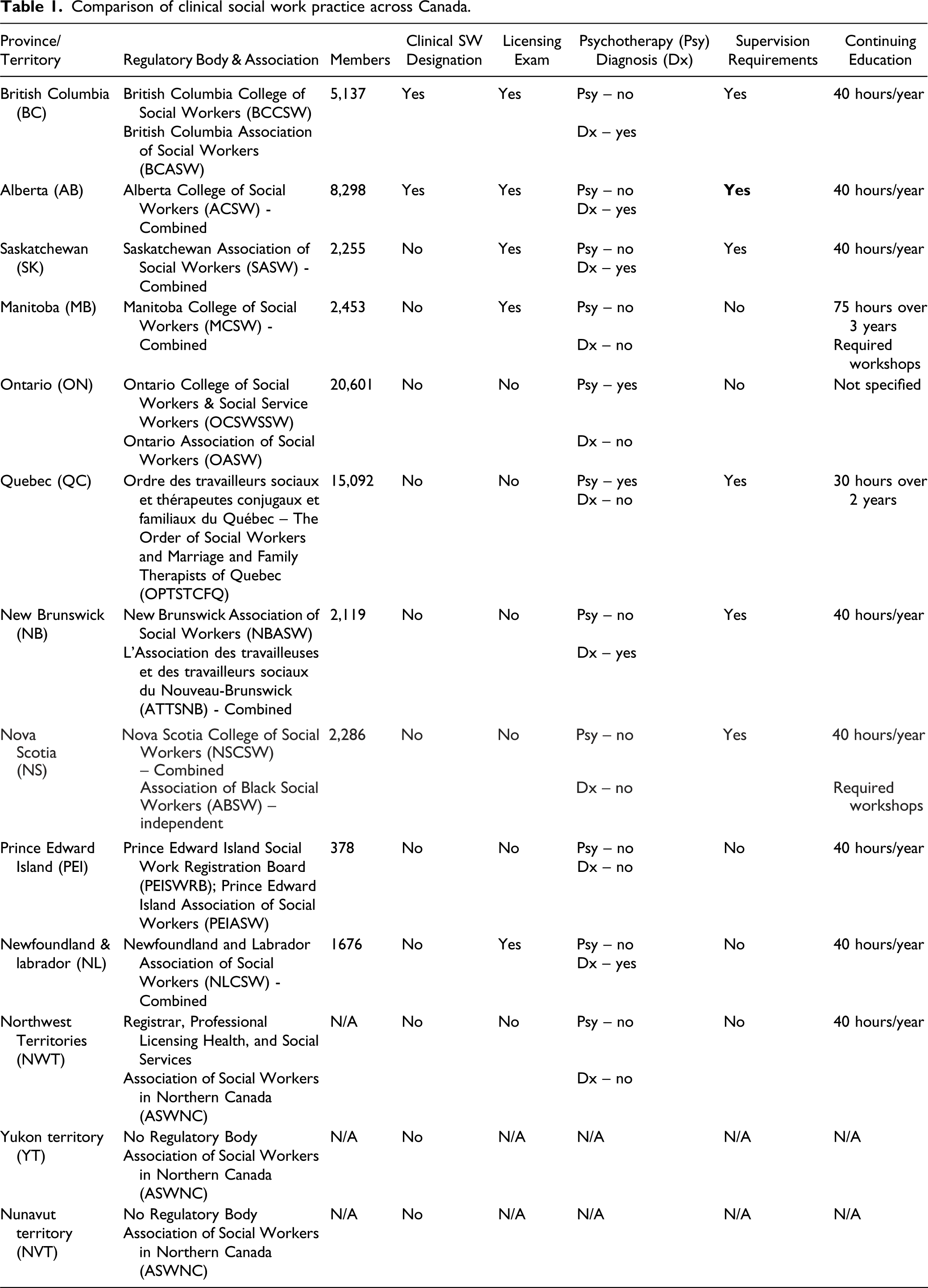
Comparison of clinical social work practice across Canada.
Nova Scotia also has an Association of Black Social Workers (ABSW) founded in 1979 by Maxene Prevost Sheppard, Frances Mills Clements, Althea Tolliver, and Senator Wanda Thomas Bernard. The ABSW is a support and professional development organization for Black social workers with a goal of contributing to the health and wellbeing of social workers of African descent in Nova Scotia (Bernard, 2015).
In Canada, regulation of social workers is recent even though the CASW made early efforts to develop legislation in 1938. The first social work law was enacted in 1966 by the Manitoba College of Social Workers (MCSW, 2022a), but most provinces did not pass their legislation until the 1990s and Ontario was the last jurisdiction to adopt legislation in 1998 (ASWB, 2021). Each self-regulating jurisdiction has legislation which guides the work of the provincial and territorial colleges and associations (CCSWR, 2012). Yukon and Nunavut do not have regulatory bodies, therefore, there is no governing legislation for either territory (ASWNC, 2011).
Another important body that influences social work education and ultimately social work practice is the Canadian Association for Social Work Education (CASWE). The CASWE (2021a) is responsible for the accreditation of academic social work programs. The CASWE (2021b) establishes educational standards and policies that must be adhered to by social work programs in Canada, which permit Bachelor of Social Work (BSW) and MSW graduates to register with the different colleges and associations. Research has shown social work education does not prepare students adequately for clinical practice and there have been calls to strengthen social work training and competence (Kourgiantakis et al., 2020; Lee et al., 2021).
Social Work Registration
In Canada, there are over forty post-secondary institutions offering accredited BSW or MSW programs (CASWE, 2021b). Seven of these schools offer Indigenous-centered social work programs and the curriculum is based on First Nations spirituality, knowledge, and approaches (First Nations University of Canada, 2020; Government of Canada, 2020). The key requirement of most regulatory bodies across Canada is a degree from an accredited social work program, therefore schools of social work have an important responsibility to prepare students for clinical social work practice (Birnbaum & Lach, 2014; Newberry-Koroluk, 2014). As a means of ensuring ethical and effective practice, there has been a movement towards competency-based education across many health and mental health professions wherein core knowledge, values, and skills are identified by the profession (Birnbaum & Silver, 2011; Bogo et al., 2011; CSWE, 2009, 2015). Competencies facilitate the conceptualization and definition of social work practice and guide the learning objectives and outcomes for students in social work programs (Bogo et al., 2011).
Across Canada, anyone using the title Social Worker, Registered Social Worker (RSW), or its French equivalent Travailleur(se) Social(e) must be registered with a provincial or territorial social work regulatory body. To use the protected title in Canada, individuals must apply for registration with a regulatory body in both the province or territory where they plan to practice and where their clients are located, as each jurisdiction has its own legislation (Birnbaum & Lach, 2014). However, registration is voluntary (Birnbaum & Lach, 2014) and while the social worker title is legally protected, it does not restrict who can provide clinical services (Newberry-Koroluk, 2014). The basis for registration in all provinces except Alberta is a BSW or MSW from an accredited social work program. The Alberta College of Social Workers (ACSW) accepts applications from applicants who have completed a BSW, MSW or social work diploma from an accredited program. Table 1 shows the number of social workers registered with regulatory bodies across Canada with the highest number of social workers (20,601) registered with the Ontario College of Social Workers and Social Service Workers (OCSWSSW) in the most populous province of the country (OCSWSSW, 2020) and the lowest number of social workers are in the least populated province of Prince Edward Island, known as PEI, with 378 registered members (PEISWRB, 2012).
Registration Requirements
Most Canadian regulatory bodies have a single-tier system of registration while most U.S. jurisdictions have multi-tiered licensures with different practice scopes for each category that correspond to education and experience levels (ASWB, 2021). Potential registrants are eligible with a BSW or MSW degree and apply for registration through their regulatory body. There is some confusion in the use of the term registration in Canada and licensure in the U.S. The ASWB states that for the purposes of regulation there is little difference between the terms and some Canadian regulatory bodies use registration and licensure interchangeably (ASWB, 2021). Historically, registration has referred to a voluntary system where individuals join a registry with qualification based on submission of completed educational requirements to use a protected title, while licensure has been associated with competency attainment such as passing a provincial or state specific ASWB competency exam (ASWB, 2021).
The ASWB has different exam categories including Associate, Bachelors, Masters, Advanced Generalist and Clinical Practice (ASWB, 2021). At present, five provinces including British Columbia, Alberta, Saskatchewan, Manitoba, and Newfoundland & Labrador, use one or more ASWB exams. British Columbia College of Social Workers (BCCSW, 2022a) requires all applicants to successfully complete the exam as part of the registration process, while the Alberta College (ACSW, 2022a) only requires applicants to take the exam if their recognized social work credential is over 3 years old at the time of application. ASWB’s Clinical Examination focuses on the delivery of direct social work practice, as well as other areas, such as community practice, research, and supervision (ASWB, 2018; 2022). For the Clinical Examination required by ACSW (2022a) and BCCSW (2022a), potential members with an MSW and more than 2 years of clinical experience are eligible to take ASWB’s Clinical Examination to advance to the designation of Registered Clinical Social Worker (RCSW). The Saskatchewan Association of Social Workers (SASW, n. d.) requires candidates to pass the ASWB Clinical Examination to qualify for Authorized Practice Endorsement which permits qualified social workers to diagnose mental health concerns. The ASWB has recently released demographic data on pass rates for the licensure exams which revealed racial disparities raising concerns about inequities, systemic racism, and the need for more transparency by regulatory bodies (Nienow et al., 2022). Table 1 shows which provinces have a licensing exam requirement for social workers.
Clinical Social Work Practice
An important guiding resource for best practices on social work regulation is the Model Social Work Practice Act and it was developed by an ASWB task force with input from social work regulatory bodies (ASWB, 2018). The Model Social Work Practice Act “establishes standards of minimal social work competence, methods of fairly and objectively addressing consumer complaints, and means of removing incompetent and/or unethical practitioners from practice” (ASWB, 2018, p.1). This Model Act promotes standardization and uniformity to increase understanding of social work, mobility for social workers across jurisdictions, and consistency with legislation and decision-making. There are six articles in the Model Social Work Practice Act including (1) title, purpose, and definition, (2) board of social work, (3) licensing, (4) enforcement, (5) confidentiality, and (6) mandatory reporting. The Model Social Work Practice Act is a guide that permits jurisdictions to know what laws governing social work practice should look like, but ultimately each jurisdiction can choose to adhere (or not) to these best practices (ASWB, 2018).
The Model Social Work Practice Act describes scopes of practice for three practice categories: Baccalaureate Social Workers, Master Social Workers, and Clinical Social Work with definitions and a description of appropriate interventions at the entry level for each category. It indicates that BSW and MSW social workers can practice independently after 2 years of full-time supervised practice (ASWB, 2018). ASWB describes clinical social work as a specialty practice under the category of Practice of Master’s Social Work which includes the “application of specialized knowledge and advanced practice skills in the areas of assessment, diagnosis, and treatment of mental, emotional, and behavioral disorders, conditions and addictions” (p. 6). Treatment methods used by clinical social workers include “individual, marital, couple, family and group counseling and psychotherapy” (p. 6). The Model Social Work Practice Act also states that the scope of clinical social work practice may include providing clinical supervision and working in private practice. Best practices outlined in the Model note that to be eligible for Clinical Social Worker designation, a candidate must have a Licensed Master’s Social Work (LMSW) and 3000 hours of clinical experience with 100 hours of direct supervision (ASWB, 2018).
As shown in Table 1, British Columbia and Alberta are the only provinces that offer the designation of Registered Clinical Social Worker (RCSW) through a licensure examination (ACSW, 2022a; BCCSW, 2022a). In British Columbia, members with an MSW are eligible to take the clinical social work (CSW) exam once they have completed 3000 supervised hours post MSW, as well as three courses on human behavior and development, assessment and diagnosis, and psychotherapy and clinical practice. The ACSW distinguishes clinical social work as a mental health profession “that utilizes social work methods to assess, diagnose and provide psychotherapeutic interventions across the lifespan with individuals, couples, families, and groups” (ACSW, 2020a, p.3). To qualify for the clinical social work registry in Alberta, applicants must be an RSW on the general registry, have completed 1600 hours of direct clinical practice (100 hours of clinical supervision with an identified Clinical Supervisor of Record), and three courses in the same areas required by British Columbia (ACSW, 2020a). The ACSW also refers to Restricted Psychosocial Interventions which are advanced areas of social work practice treating mental health disorders. Social workers performing Restricted Psychosocial Interventions require more training, education, and supervision. In the rest of the country, where there is not a specific clinical social work designation, there are standards of practice that set out minimal standards for professional practice and conduct (CCSWR, 2012).
Psychotherapy
While there is no clinical social work designation in Québec and Ontario, they are the only two jurisdictions that have the reserved title and controlled act of psychotherapy although there are discrepancies between the two provinces in the requirements needed to use this title and practice act. In Québec, a predominantly French speaking province, the regulatory body is the Ordre des Travailleurs Sociaux et des Thérapeutes Conjugaux et Familiaux du Québec (OTSTCFQ) also referred to as The Order. The Order has the following requirements for a psychotherapy permit: MSW degree at a minimum, 765 hours of training in psychotherapy, and 600 internship hours. Of these internship hours, 300 must be direct client contact and 100 hours must be individual supervision (OTSTCFQ, 2018). The Ontario College states that psychotherapy is not an entry to practice act and recommends supervision for members doing psychotherapy, but the College does not specify the number of required supervision hours. Moreover, all members of the Ontario College are eligible to use the title psychotherapist and perform the controlled act of psychotherapy including social workers with a BSW or MSW, as well as social service workers who hold a 2-year community college diploma (OCSWSSW, 2022a; 2009).
Diagnosis
The Model Social Work Practice Act states that only clinical social workers are qualified to diagnose using the Diagnostic and Statistical Manual of Mental Disorder (DSM), the International Classification of Diseases (ICD), and using other forms of assessment (ASWB, 2015). While social workers in most states can diagnose mental health disorders (Kourgiantakis et al., 2020), diagnosing has not been widespread across Canada. Increasingly, more Canadian jurisdictions have been including diagnosis of mental health concerns in the scope of practice of social workers. Presently, there are five jurisdictions where social workers with certain designations can diagnose mental disorders including British Columbia (BCCSW, 2022a), Alberta (ACSW, 2022a), Saskatchewan (SASW, 2020), New Brunswick (NBASW, 2017), and Newfoundland & Labrador (NLCSW, 2020a). In Saskatchewan, social workers are required to obtain the specialized classification of Authorized Practice Endorsement (APE) to diagnose mental health disorders (Austin, 2017; SASW, 2020). In Alberta, diagnosis is not a restricted activity and can be performed by all members, but Registered Clinical Social Workers are deemed to have this expertise due to their designation (Pearson, 2014). In British Columbia, diagnosis using the DSM is within the scope of practice for Registered Clinical Social Workers only (BCCSW, 2022a). In 2017, the New Brunswick Association of Social Workers (NBASW) announced that they were including diagnosis in the scope of social work practice as this would support the field in addressing mental distress and offer clients access to more efficient care (NBASW, 2017). In 2019, New Brunswick introduced the new clinical category of Advance Practice Registered Social Worker (APRSW), and it enables RSWs who meet specific advanced criteria to use the DSM-5 to diagnose and treat mental health and addiction concerns (NBASW, 2019a). The standards of the Newfoundland & Labrador College of Social Workers (NLCSW, 2020a) state that social workers using the DSM in their practice must have an MSW with a clinical focus, at least 5 years of experience in the field of mental health, and access to clinical supervision. A recent scoping review on diagnosis in clinical social work practice found that there is a need to strengthen social work education and training in diagnosis. At present, there is limited guidance on how to increase competence in social workers to be able to include diagnosis in social workers’ scope of practice (Sur et al., 2022). Table 1 shows which provinces include diagnosis in social workers’ scope of practice.
Supervision
Clinical supervision is defined as an interactive relationship between a social worker and an approved clinical supervisor in the Model Social Work Practice Act (ASWB, 2018). The Model Act focuses on the relationship between the approved clinical supervisor and supervisee and states that supervisors have legal and ethical accountability for the social worker’s practice. The goal of clinical supervision is professional growth and development and the focus is on practice skills, continuing education, professional identity, ethical practice, and cultural competence. Furthermore, the Act states that anyone providing supervision to a social worker with a BSW must have a BSW, MSW or Clinical Social Work designation. A social worker with an MSW can only receive supervision from a social worker with an MSW degree or clinical social worker. The Act also recommends that each regulatory body maintain a list of pre-approved supervisors who have at least 3 years of experience post-licensure and supervision training by an approved program (ASWB, 2018).
Table 1 shows that more than half of the Canadian provinces have specific supervision requirements although only two (Alberta and Nova Scotia) are entry to practice requirements. To become registered in Alberta, RSW applicants must have 1500 practice hours under the supervision of a qualified RSW (ACSW, 2022a). Nova Scotia requires an applicant who is qualified and has less than 2500 hours of post-degree supervised experience to register as a Registered Social Worker Candidate (RSWC) and complete the Candidacy Mentorship program (with at least 32 mentored hours). Candidacy mentors are experienced RSWs (NSCSW, 2022a). Six provinces have supervision requirements for clinical social work practice or advanced clinical social work practice including British Columbia, Alberta, Saskatchewan, Nova Scotia, Québec, and New Brunswick. In British Columbia, members applying to the clinical registry must have 3000 supervised clinical hours (BCCSW, 2022a). Alberta requires 1600 clinical hours and of those hours, 100 need to be supervised by a Clinical Supervisor of Record who must be a RCSW (ACSW, 2022a). Saskatchewan requires 3000 clinical supervision hours (with 100 supervised hours focused on diagnosis) to be eligible for the Authorized Practice Endorsement designation (SASW, 2020). Québec requires that 100 hours of clinical supervision are received for 300 direct clinical contact hours for those seeking to use the controlled act of psychotherapy (OTSTCFQ, 2018). The Ontario College underlines the importance of supervision for ongoing professional development and competence. It also notes that access to regular supervision is necessary for members in private practice, but in both examples, the Ontario College does not indicate the number of required hours. It is also important to note that as mentioned previously, the Ontario College regulates two professions, and the legislation permits social service workers to supervise BSW and MSW social workers (OCSWSSW, 2022a, 2008).
Continuing Education
In 1994, CASW released a policy statement on continuing education to address its significance as an ongoing process throughout one’s career. CASW delegated the primary responsibility for participating in continuing education to individual social workers, while also emphasizing the mutual responsibilities that fall on social work schools, employers, government, and professional associations to promote this constant learning (CASW, 1994). The Model Social Work Practice Act states that continuing education is one way of enhancing ongoing professional development and competence for social workers. The guidelines stipulate a minimum of 15 hours of continuing education through approved programs each year by a licensed social worker.
In Canada, continuing professional competence is required by all regulatory bodies across the country, however standards differ depending on the jurisdiction. All jurisdictions with a regulatory body require RSWs to complete a minimum number of hours of learning activities except Ontario. For example, colleges in British Columbia (BCCSW, 2022b), Alberta (ACSW, 2022b), Saskatchewan (SASW, n. d.), New Brunswick (NBASW, 2019a), Nova Scotia (NSCSW, 2022b), Newfoundland & Labrador (NLCSW, 2020b), Prince Edward Island (PEISWRB, 2012), and Northwest Territories (Health and Social Services [HSS], 2011) all require a minimum of 40 hours per year. Manitoba requires 75 hours over 3 years (MCSW, 2022b), and Québec requires 30 hours over 2 years (OTSTCFQ, 2022a). In addition, some Colleges make distinctions in the number of hours required depending on the member’s designation or type of membership (ACSW, 2022b; NBCSW, 2019a; 2019b; NSCSW, 2022b), and two require specific trainings for members (MCSW, 2022b; NSCSW, 2022b). For example, Nova Scotia has 6 hours of mandated professional development each year on five mandated topics (NSCSW, 2022b). Manitoba requires members to complete two workshops that are 8-hours in length every 3 years on ethics and social work practice with Indigenous peoples (MCSW, 2022b). Ontario has a mandatory continuing competence program that requires RSWs to complete a self-assessment and review the standards of practice annually, and then set learning goals and activities based on that self-assessment. However, there is not a specific number of hours required and this is not submitted for accountability (OCSWSSW, 2019). Continuing education requirements for each province are presented in Table 1.
Technology
The use of technology in social work practice became increasingly more prevalent with the onset of the COVID-19 pandemic (Mishna et al., 2021). Prior to the pandemic, the social work community was already exploring the impact of technology in clinical practice (NASW, 2017) and some jurisdictions had developed technology standards prior to the pandemic (BCCSW, 2016; NBASW, 2010). These technology standards support clinical social workers in how to incorporate technology in their services ethically and effectively, which can include video or telephone counselling, online or text chats, and interacting via social media (BCCSW, 2016; NBASW, 2010). In 2015, the ASWB published Model Regulatory Standards for Technology and Social Work Practice to serve as a guide for digital social work practice. It describes social work competence standards in the provision of electronic services and standards related to informed consent, privacy and confidentiality, boundaries, dual relationships and conflict of interest, records and documentation, collegial relationships, and electronic practice across jurisdictions (ASWB, 2015).
Four provinces have standards of practice specifically for electronic services: British Columbia (BCCSW, 2016), New Brunswick (NBASW, 2010), Québec (OTSTCFQ, 2017), and Newfoundland & Labrador (NLCSW, 2020b). Another four provinces including Alberta (ACSW, 2019a), Saskatchewan (SASW, 2020), Manitoba (MCSW, 2021a), and Nova Scotia (NSCSW, 2022c) identify technology standards within their broader standards of practice. Ontario has a practice note that serves as an educational tool to help clinical social workers offering electronic services (OCSWSSW, 2017). Across the different jurisdictions, there are similarities in technology best practice guidelines which include clinical competencies, electronic practice outside of one’s jurisdiction, informed consent, confidentiality and privacy, boundaries, dual roles, client records, and social media policies (BCCSW, 2016; NBASW, 2010; NLCSW, 2020c; OTSTCFQ, 2017).
Private Practice
Clinical social workers may provide services through private practice which is defined in the Model Social Work Practice Act as “the provision of clinical social work services by a licensed clinical social worker who assumes responsibility and accountability for the nature and quality of the services provided to the client in exchange for direct payment or third-party reimbursement” (ASWB, 2018, p.10). The information available to support ethical and effective clinical social work private practice is quite limited across most of the jurisdictions. Prince Edward Island (PEISWRB, 2016) and Newfoundland & Labrador (NLCSW, 2020c) are the only jurisdictions with a set of standards or policies that are specific for private practice, and both are the only jurisdictions that stipulate registration criteria for private practitioners. Both Colleges require an MSW degree, and both require registration and good standing as an RSW to practice privately. Prince Edward Island stipulates a minimum of 4 years of clinical experience, while Newfoundland & Labrador require 3 years of experience. Neither province has clear supervision guidelines for private practice social workers. Prince Edward Island requires previous supervision with someone in the member’s area of specialization and Newfoundland & Labrador requires access to registered professionals for consultation (NLCSW, 2020d; PEISWRB, 2016). Manitoba has a standard of practice that states: “social workers in private practice will maintain regular, consistent and structured supervision from a supervisor with relevant expertise, experience and knowledge of social work ethics and standards of practice” (MCSW, 2021a, p.15).
British Columbia, Alberta, Saskatchewan, Manitoba, Northwest Territories, and New Brunswick have one or more guidelines within their code of ethics or standards of practice that are specific to private practice. These private practice standards focus on professional liability insurance, availability for clients, coverage when unavailable (MCSW, 2021a; (Northwest Territories Standards of Practice for Social Workers, 2011), fees, cancelation policies, record keeping (ACSW, 2019a; MCSW, 2021a; NWT, 2011), not soliciting employers’ clients for private practice (ACSW, 2019a; BCCSW, 2009; MCSW, 2021b), conflict of interest, (MCSW, 2021b), ensuring offices do not obstruct mobility, and providing accommodations for clients (MCSW, 2021a; NWT, 2011). Ontario, Québec, and Nova Scotia provide some information about private practice on their websites which includes a private practice directory, guidelines for re-opening private practice following pandemic restrictions, recommended rates (NSCSW, 2022d), and additional resources to support clinical social workers in private practice (NSCSW, 2022d; OCSWSSW, 2022b; OTSTCF, 2022b).
Addressing Diversity, Equity, Reconciliation, Racism, and Discrimination
Most of the Canadian regulatory bodies have acknowledgements of racism, discrimination, historical trauma, and inequities as shown in their strategic priorities, public statements, committees, and practice guidelines. For example, the strategic priorities for the British Columbia College of Social Workers (BCCSW) for 2021–2025 include cultural safety, cultural humility, and anti-racism. Manitoba includes respect for diversity and equality, inclusion, and social justice as values of the College, and one of their strategic priorities is advancement of reconciliation with Indigenous peoples (MCSW, 2022a).
Northwest Territories and Manitoba have standards of practice that focus on cultural diversity, rural and northern social work practice, and advocacy and public policy (MCSW, 2021a; NWT, 2011). Alberta and Saskatchewan include cultural competence in their standards of practice (ACSW, 2019a; SASW, 2020), and Prince Edward Island (PEISWRB, 2010) and Québec (OPTSTCF, 2019) include social justice as values in their code of ethics or articles in their standards of practice. New Brunswick (NBASW, 2019b) and Alberta (ACSW, 2020b) have standards of practice that condemn reparative or conversion therapy which contradicts social work values and ethics.
Alberta has an Indigenous practice framework prepared by University nuhelot’jnethaiyots’jnistameyimakanak Blue Quills with the College titled Honouring Sacred Relationships: Wise Practices in Indigenous Social Work. This framework presents information about Indigenous worldviews and Indigenous social work with key themes that include (1) spirituality, ceremony, and culture, (2) relationships, (3) ethical space, (4) identity, lived experience, and knowing, (5) circles, (6) protocols and policies, (7) lifelong learning, and (8) becoming an ally (ACSW, 2019b).
New Brunswick has developed five cultural competence standards of practice for working with Indigenous peoples. Standard one states culturally competent social work practice shall be grounded in the ethics and values of the social work profession. Standard two focuses on awareness of one’s cultural identity and experiences in cross cultural practice. Standard three notes that social workers shall seek to understand the values, beliefs, traditions, and historical context of Indigenous clients and incorporate this knowledge into social work assessments and interventions. Standard four states that social workers demonstrate the use of effective intervention skills when working with clients from diverse cultural backgrounds, and standard five states that social workers engage in continuing professional development to foster knowledge, skills, and abilities in working with clients from diverse cultural backgrounds. This standard of practice document provides self-reflection questions that permit clinical social workers to reflect on their own values, approaches, and systems where they are practicing (NBASW, 2021).
British Columbia (BCSSW, 2022c), Alberta (ACSW, 2022c), and New Brunswick (NBASW, 2022) have Indigenous committees and councils that bring Indigenous knowledge, values, and approaches to culturally inform College policies and practices related to regulation and working with Indigenous communities. The Saskatchewan Association of Social Workers issued a statement on the first official National Day for Truth and Reconciliation on September 29, 2021, noting that they have formed a Truth and Reconciliation Working Group to influence the work towards reconciliation (SASW, 2021). Ontario has a diversity, equity, and inclusion task group and has put forward a recommendation to collect raced-based data from members on a voluntary basis at renewal (OCSWSSW, 2020). New Brunswick has a Social Action Committee engaged in social action and social change consistent with the code of ethics (NBASW, 2021).
Many regulatory bodies have published statements on anti-racism and anti-discrimination and due to space limitations, this article includes a few select examples. In June 2020, Alberta released a statement condemning all forms of racism against Black, Indigenous, and People of Colour, also acknowledging the harmful history of the social work profession and identifying ways to move forward (ACSW, 2020c). On May 31, 2021, the Ontario College released a statement honoring the 215 Indigenous children whose remains were found at a former residential school. The College recognized the ongoing impact of colonization and systemic racism and the shameful role of social workers underlining the importance of examining policies and practices that play a role in perpetuating systemic oppression (OCSWSSW, 2021). The Nova Scotia College of Social Workers published a statement on the first Emancipation Day on August 1, 2021, marking that day in 1834 when the Slavery Abolition Act came into effect in the British Empire (NSCSW, 2021). While there are initiatives by some regulatory bodies to address diversity, equity, and inclusion, the demographic data of licensure exams demonstrate that there are ongoing inequities, bias, and systemic racism in the regulatory system (Nienow et al., 2022). There is a need for a larger re-evaluation of policies and structural issues within regulation.
Discussion and Applications to Practice
This article provided an overview of regulation of clinical social work practice in Canada with a focus on key areas influencing clinical social work practice including entry to practice requirements, clinical social work designation, the controlled act of psychotherapy, diagnosis, supervision, continuing education, private practice, technology, and addressing diversity, equity, reconciliation, racism, and discrimination.
While clinical social work practice requires specialized clinical knowledge and advanced clinical skills (ASWB, 2018), examination of regulation in Canada shows only British Columbia and Alberta have a clinical social work designation. There are also significant differences between the provinces with some jurisdictions having more rigorous entry to practice requirements, as well as divergent requirements for supervision and continuing education.
This overview demonstrates a surprising lack of uniformity in regulatory standards and ethics across the country even though there was a survey conducted by the CCSWR in 2012 which had the aim of developing a competency framework that could be applied to all jurisdictions to harmonize the standards of social work practice (CCSWR, 2012). The current analysis of clinical social work practice and regulation shows that none of the provinces or territories adhere to all the standards outlined in the Model Social Work Practice Act, and there are some jurisdictions that comply with very few best practices. One of the Colleges with the lowest or minimal standards is the Ontario College of Social Workers and Social Service Workers which has the highest number of social workers in the country. The OCSWSSW has low entry to practice requirements (completion of SSW diploma or BSW or MSW degree) and no specific requirements for supervision, psychotherapy, continuing competence, and private practice. However, the OCSWSSW recently announced that an entry to practice exam will be implemented in 2027. It is unclear how the Ontario College will proceed with its plan for a licensing exam considering the recently revealed racial disparities in licensure exam pass rates. We are also unclear on how the other provinces that currently have licensing exams will respond to this important and pressing structural issue. We hope that provinces will re-evaluate the licensing exams and with transparency and community involvement will generate equitable ways of licensing competent social workers. Ontario and Alberta are the only regulatory bodies that regulate members with a community college diploma. In Ontario, there does not appear to be a distinction between the scope of practice of a social service worker and a social worker including standards of practice for psychotherapy, private practice, and supervision. The primary aim of regulation is public protection; therefore, it is important to examine how this protects the public if members register who do not have adequate training and competence for clinical practice. In its report, the CCSWR (2012) recommended a core set of competencies with performance standards at three levels, a communication plan to disseminate these standards, and training programs to develop the competencies for those who do not meet the standards.
Supervision was an important area highlighted in this analysis of clinical social work practice and research shows that it influences social work competence (CASW, 2020; Sewell et al., 2021). More than half of the regulatory bodies have requirements related to supervision, and research shows that there is minimal information and guidance on supervision for clinical social work practice (Sewell et al., 2021). The OASW conducted a survey on clinical supervision with members working in health care and found that a little more than half of the participants (52%) engaged in clinical supervision even though most spend over 50% of their time helping clients with complex needs (Sewell, et al., 2021). Vandette and Gosselin (2019) argue that clinical supervision is a professional competency and critical for interprofessional work. The authors recommend developing standards and guidelines to regulate its conceptualization and practice, as well as competencies and training for the supervisors. Most Colleges that have supervision requirements in Canada specify the level of degree, designation, and/or registration status of the supervisor (e.g., RSW or RCSW). However, most Colleges do not require the supervisor to have training or certification in supervision.
This article found that all Canadian Colleges engaged in some initiatives to address diversity, equity, reconciliation, racism, and discrimination. Some of the Colleges have integrated these areas in their values and strategic priorities, some have developed culturally responsive standards of practice, and some Colleges have committees consisting of community members who can inform College practices, events, and governance. Blackstock (2009) emphasizes the need for social work to acknowledge complicity and harms caused and engage in the reconciliation process. Gray et al. (2013) argue that decolonizing social work means not accepting hegemonic practices and imperialist frameworks. There have been criticisms that social work has abandoned its social justice mission with its increased focus on clinical practice (Specht & Courtney, 1994), but increasingly there is literature explaining the importance of combining critical and clinical approaches (Brown, 2021).
This article shows the importance of consistent standards and codes of ethics across the country to increase public protection, create more accountability, promote ethical, competent, culturally appropriate and anti-oppressive practice, and improve public perceptions and trust of the profession. Staniforth et al. (2022) argues there are public perceptions that professionalization through registration will produce higher standards in social work practice (Staniforth et al., 2022), but an examination of professional self-regulation in Canada has shown that in this neoliberal era there has been “less emphasis on qualifications as essential to service quality” and a growing tendency to see entry to practice qualifications as barriers to business rather than standards that protect the public (Adams, 2016, p.10).
To increase quality of clinical social work practice, there is a need for attention from all three pillars of the profession – regulation, association, and education (CASW, n. d.). CASWE is the education pillar in Canada and develops educational policies and accredits social work programs (CASWE, 2022). The CASW promotes the social work profession (CASW, n. d.) and many provinces and territories also have an association advocating to advance the profession, policies, social justice, and professional development. The third pillar is regulation which develops standards, ethical guidelines, and deals with professional misconduct (CCSWR, 2012).
Based on the analysis of regulation and clinical social work practice in Canada, the authors propose the following list of recommendations to strengthen clinical social work practice across the country: (1) concerted effort from regulation, education, and association to strengthen clinical social work practice; (2) make standards of practice and codes of ethics uniform across the country for increased mobility, improved public trust, and enhanced clinical competence; (3) create a clinical social work designation in every province; (4) create entry to practice supervision requirements for independent clinical practice and for private practice; (5) specify the qualifications of clinical supervisors and require supervisors to complete training in clinical supervision; (6) set a minimum number of hours for continuing education and make it mandatory for members to submit an annual report; (7) evaluate the need for additional training for advanced clinical social work practice; (8) develop standards for private practice in all provinces and territories and include minimum requirements for private practice; (9) Distinguish between educational levels (i.e., BSW, MSW) and/or designations (i.e., RCSW) to ensure members are adequately trained for practice; and (10) demonstrate a commitment to reconciliation, equity, diversity, anti-oppression anti-discrimination, and anti-racism through acknowledgement of harms and historical trauma, recognition of non-Western worldviews, partnerships with community members, transparency about decision making, and openness to make changes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.