
Abstract
Purpose:
This study evaluated the video-feedback intervention Basic Trust in families with internationally adoptive children aged 2–12 years. The intervention aims to reduce child attachment insecurity and behavior problems by enhancing mothers’ and fathers’ sensitivity and mind-mindedness (parents’ capacity to hold in mind the mind of their child).
Method:
Fifty-three adoptive families participated in a pretest, posttest, and 6-month follow-up assessment. Questionnaires on parenting stress, child attachment insecurity, and behavior problems were administered. Parents’ sensitivity was assessed from free-play observations at home, and mind-mindedness was measured with a describe-your-child interview.
Results:
Parents reported less child behavior problems, insecure and disorganized attachment, and parenting stress at posttest and follow-up. Parents’ mind-mindedness increased from pre- to post-test but not from pretest to follow-up. Parents’ sensitivity showed an improvement at follow-up.
Conclusions:
Future studies should investigate whether the present study’s positive results can be replicated under conditions of strict experimental control.
Keywords
International adoption seems to be an intervention leading to long-term improvements for adopted children in all areas of development (van IJzendoorn & Juffer, 2006). The majority of internationally adopted children do not display severe or persistent medical, behavioral, or developmental problems (e.g., Bimmel, Juffer, van IJzendoorn, & Bakermans-Kranenburg, 2003). Still, a larger ratio of adopted children receives mental health counseling than do their nonadopted counterparts (Juffer & van IJzendoorn, 2005). The risk of developing mental health problems seems to stem from the fact that most internationally adopted children were exposed to severe environmental adversities before they were adopted (e.g., institutional rearing, poverty, social disorganization, abuse, malnutrition, poor pre- and postnatal care within the biological family; Colvert et al., 2008; van IJzendoorn & Juffer, 2006). Adopted children experienced the loss of at least one caregiver, and it is not uncommon that they went through multiple caregiver transitions in institutional care. Furthermore, the transition to a new culture and finding a connection with new caregivers constitute risks of successful adaptation (Havermans, Verheule, & Prinsen, 2016; Welsh, Viana, Petrill, & Mathias, 2007).
This list of unfavorable environmental conditions can especially be worrisome for the child’s developing attachment to their adoptive parents and other caregiving figures. Attachment, the newborn’s innate propensity to maintain proximity to an attachment figure in order to establish the experience of security, is hypothesized to affect children’s later social–emotional development (Bowlby, 1969/1982). Secure infants experience the primary caregiver as a secure base from which to explore the environment and as a haven of safety and a source of comfort (Ainsworth, Bell, & Stayton, 1974; Ainsworth, Blehar, Waters, & Wall, 1978; Benoit, 2004; Bowlby, 1969/1982). Attachment security thereby stimulates the development of healthy emotion regulation strategies in children as well as clear concepts of the self, others, and self–other relationships (Fonagy, Gergely, Jurist, & Target, 2002). In line with this reasoning, a large body of studies have demonstrated that attachment security during infancy predicts a wide variety of socio-emotional outcomes during childhood and adolescence, such as social competence and empathy (e.g., Cohn, 1990; Groh et al., 2014; Kestenbaum, Farber, Ellen, & Sroufe, 1989; Thompson & Raikes, 2003). Conversely, the likelihood that children with insecure attachment develop internalizing and externalizing problems has proven to be respectively 2.9 and 2.4 times greater compared with their secure counterparts (Madigan, Brumariu, Villani, Atkinson, & Lyons-Ruth, 2016). Enhancing the child’s sense of security may thus reduce (the risk of later) mental health and adjustment difficulties.
A meta-analysis on attachment in biological and adopted children showed that adopted children are at a substantial risk of becoming insecurely attached to their adoptive parents when they are adopted after the age of 12 months (i.e., after the sensitive phase of forming attachment relationships; van den Dries, Juffer, van IJzendoorn, & Bakermans-Kranenburg, 2009). During the past decade, changes in global health, international adoption attitudes, and regulation policies have led to children being older during the adoptive placement—currently 80% of the internationally adopted children is placed after they turned 1 year old (Ministerie van Veiligheid en Justitie, 2017; Selman, 2012). This percentage suggests that the vast majority of adopted children is indeed at risk of developing attachment insecurity. Moreover, although the differences seem to be small, a large body of studies suggest that (internationally) adopted children show elevated levels of behavioral problems as compared to nonadopted peers, for instance, externalizing behavior problems and high rates of inattentive/overactive behavior (e.g., Bimmel et al., 2003; Hoksbergen, ter Laak, van Dijkum, Rijk, Rijk, & Stoutjesdijk, 2003; Kreppner, O’Connor, Rutter, & English and Romanian Adoptees Study Team, 2001; McGuiness & Pallansch, 2000).
Prevention of maladaptive developmental pathways may be realized when adopted children are able to build a secure attachment relationship with an adoptive parent (Kerr & Cossar, 2014). Changing children’s attachment representation from insecure to secure may require from parents that they maximize behaviors that cultivate a sense of trust in their caregiver’s availability and comforting support in times of distress, by trying to accurately understand and respond sensitively to the child’s needs (Ainsworth et al., 1974; Polderman, 1998, 2017; Stovall & Dozier, 2000; Verhage et al., 2016; Zeegers, Colonnesi, Stams, & Meins, 2017).
Maximizing attachment-relevant caregiving behaviors poses challenges for all parents but possibly even more so for adoptive parents (Fishburn et al., 2017). Biological parents experience the development of their child from the very start (pregnancy), and their process of thinking about the child’s putative character starts to develop during pregnancy (Arnott & Meins, 2008). For parents of adopted children, the transition to parenthood often takes place in the context of complex losses that derive from infertility (Cudmore, 2005). Moreover, in the case of international adoption, parents typically come from different cultural backgrounds and know very little about their child’s pre-adoption caregiving history (Havermans et al., 2016). On the other hand, prior to the adoption (particularly in the case of late adoption), the adoptive child has developed cognitive models including expectations of the social world (Bowlby, 1969/1982), accompanied by certain behavioral patterns during social interaction. Not knowing the context from which a child’s patterns of behavior have developed seems to require a greater effort in caregivers’ mind-reading abilities and subsequently might affect whether caregivers are able to respond sensitively to their child’s cues (Fishburn et al., 2017; Zeegers et al., 2017).
For instance, when parents know that their daughter has been attacked by a dog in the past, it is easier for them to understand why their child cries and hides whenever a dog approaches and respond to this with understanding and comforting behavior. Disruptive or anxious behavior of insecurely attached adopted children may reflect, for a significant part, a history of (adverse) experiences unknown to the adoptive parents. This could cause more challenges for adoptive parents to understand the thoughts and feelings of their children.
Although there is little empirical evidence for the abovementioned notion, one study suggests that adoptive parents, compared to biological parents, are less likely to describe their children with reference to inner experiences and more likely to refer to behavior and physical aspects of their child (Fishburn et al., 2017). Moreover, another study showed that adoptive parents have shown to make fewer positive descriptions (e.g., “he is a very joyful boy”) and more negative descriptions (e.g., “he feels very tense about everything”; Harris-Waller, 2012) of their child. Thus, adoptive parents seem to have a higher tendency to think about their child’s behavior, rather than their thoughts and feelings, and are more likely to describe negative characteristics of their child.
The study of Fishburn et al. (2017) suggests that these outcomes could be explained partially by the higher prevalence of behavioral difficulties in adoptive children compared to nonadopted children (Bimmel et al., 2003; Harris-Waller, Granger, & Gurney-Smith, 2016; Juffer & van IJzendoorn, 2005). That is, their study demonstrated that the more adoptive parents perceive their child’s behavior as difficult, the less they focused on describing their child’s inner experiences. However, children’s behavioral difficulties could not fully account for the differences in mind reading between adoptive and biological parents. These outcomes point to a complex interplay between a noncontinuous parent–child relationship, parents’ caregiving abilities, and the child’s behavior problems. Hence, although the vulnerability of an adopted child makes it even more important for parents to have the mental tendencies that enable them to show sensitive responses to their child, adoptive parents probably face more challenges in doing so.
Attachment Interventions
Existing attachment interventions typically focus on providing psychoeducation, behavioral guidance, and/or changing the parent’s own mental representation of attachment (Howe, 2006). The existing behaviorally based attachment interventions target multiple domains of parenting behaviors that promote the development of a predictable and stable caregiving environment (Bakermans-Kranenburg, Van IJzendoorn, & Juffer, 2003; Welsh et al., 2007). The most established predictor of attachment security is parental sensitivity, referring to parents’ understanding of their child’s signals and their appropriate and prompt responding to these signals (Ainsworth et al., 1974; Verhage et al., 2016). So far, research indicates that attachment interventions that aim to improve parental sensitivity show more positive outcomes than attachment interventions that target multiple domains of parental functioning (Bakermans-Kranenburg et al., 2003). A comprehensive meta-analytic review including 70 studies and 88 interventions on parental sensitivity and infant attachment showed that interventions that focus exclusively on parental sensitivity are more successful in changing insensitive behavior and attachment insecurity, showing small to medium effect sizes (Bakermans-Kranenburg et al., 2003). Furthermore, this review highlighted that the most effective attachment interventions did not always include a large number of treatment sessions with the families and used video feedback to alter parenting behavior. So, there is some support for the potential success of short goal-directed attachment interventions that specifically target research-supported predictors of attachment.
However, the most recent meta-analytic reviews on effective elements in existing attachment interventions stem from 15 years ago (Bakermans-Kranenburg et al., 2003; Bakermans-Kranenburg, van IJzendoorn, & Juffer, 2005). Since then, research on predictors of attachment has expanded enormously, and other parenting behaviors and features of the parent-child relationship have shown to explain variation in attachment (e.g., Beebe & Steele, 2013; Bernier, Matte-Gagné, Bélanger, & Whipple, 2014; Davis et al., 2017; Feldman, 2015; Meins, Fernyhough, Fradley, & Tuckey, 2001) and therefore might be important to incorporate in the programs of existing attachment interventions. One parenting feature that gained much attention in attachment research in the past two decades is parental mind-mindedness, referring to parents’ tendency to represent and hold in mind the child’s putative mental states: thoughts, feelings, preferences, desires, and so on (Meins, 1997, 2013). Mind-mindedness is operationalized in terms of the parent’s use of appropriate or nonattuned mental state language during infant–parent interactions and the parent’s use of mind-related speech when describing their toddler or child (Meins, 1997; Meins et al., 2001; Meins, Fernyhough, Russell, & Clark-Carter, 1998). Mind-mindedness has shown to predict substantial variation in secure infant–parent attachment over and above parental sensitivity (e.g., Meins et al., 2001; Meins et al., 2012; see Zeegers, et al., 2017 for an overview). Furthermore, mind-mindedness has shown to predict individual differences in children’s socio-emotional development and behavior, for instance, theory of mind, social competence, behavior problems, and emotion regulation (e.g., Bernier, Carlson, & Whipple, 2010; Colonnesi, Zeegers, Majdandzic, van Steensel, & Bögels, 2019; Gagné, Bernier, & McMahon, 2018; Meins et al., 2001; Meins et al., 2002; Meins, Centifanti, Fernyhough, & Fishburn, 2013; Zeegers et al., 2018).
Given these outcomes, it seems interesting to investigate whether adoptive parents’ mind-mindedness could be improved and whether a mind-mindedness-oriented intervention leads to positive outcomes in children’s behavioral and emotional development. More specifically, focusing on parents’ mind-mindedness may be key in curative interventions that aim to change children’s attachment representations from insecure to secure. That is, insecurely attached children are hypothesized to lack the experience of frequent and/or appropriate (nonverbal) affect mirroring, which in turn disrupts the child’s developing concept of the self as being valuable and effective in interacting with others (Bowlby, 1969/1982; Fonagy et al., 2002). By appropriately referring to the child's internal states, parents may help their insecurely attached child to catch up with the experience of being reflected accurately and enable him or her to develop a clear and organized self-concept (Polderman, 2017). Further, parents’ mind-related speech stimulates the development of the child’s private speech which may in turn help the child to understand and tolerate arousal, rather than responding to arousal automatically (Fernyhough, 2008).
The Basic Trust Intervention
The Basic Trust intervention, on which we focus in the present study, aims to enhance the child’s sense of attachment security by improving parents’ sensitivity and mind-mindedness through the use of video feedback (Polderman, 1998, 2017). Although the Basic Trust intervention can also be applied in preventive settings, it is generally used as a component of curative intervention programs aimed at remediating attachment insecurity and disorganization in children (Polderman, 1998, 2017). Furthermore, in two-parent families (mother–father but also father–father and mother–mother), two separate child–caregiver attachment relationships are formed that are important to the child’s developmental health (Carone, Baiocco, Lingiardi, & Kern, 2020; Lamb, 2004; Lucassen et al., 2011). Therefore, mothers and fathers are asked to attend all sessions of the intervention.
The Basic Trust intervention on average consists of six to nine sessions. In the first session, parents visit the therapist alone to discuss the outcomes of the questionnaires and set therapy goals with the parents (Polderman, 2017). Parents also receive psychoeducation on insecure and disorganized attachment and on the mechanisms through which parents’ mind-mindedness and sensitive behavior stimulate the child’s sense of security. During the second, fourth, sixth, and eighth session, the therapist makes video recordings of parent–child interactions (e.g., playing together). During the third, fifth, seventh, and ninth session, parents visit the therapist alone to watch the video recordings. These sessions involve creating awareness and understanding of the child’s behavior and mind, as well as the parent’s own verbal and nonverbal responding to the child (Polderman, 2008, 2009). Parents and therapist first discuss how parents received and validated the child’s behavior and states nonverbally (e.g., seeking proximity, making eye contact, showing an attuned facial expression). After this, parents practice a stepwise method including a verbal response that they can use in each interaction with their child (Polderman, 2017). This method includes parents referring to their child’s behavior, thoughts, or feelings in a particular situation (Step 1) in an appropriate but affirmative way (i.e., without asking a question, e.g., “you grabbed a piece of the puzzle, you are wondering where to put it”). After this, parents make their own perspective clear to their child (Step 2; i.e., by mentioning their own thought or opinion, making a proposal, highlighting interpersonal contradictions, e.g., “I will help you look for a matching piece”). Parents, thus, learn to explicate their perspective on the child’s internal world as well as on their own. The verbalizing of the child’s and parent’s mental states is practiced in every video-feedback session. In order for parents to get used to verbalizing the child’s and their own perspective, they are stimulated to practice daily at home for 15 min.
The Basic Trust intervention has been examined previously in a pilot study including 20 adoptive families (Colonnesi et al., 2013). Decreases in children’s insecure attachments to their mothers and disorganized attachments to both their parents were found. Furthermore, mothers and fathers reported that their child’s conduct problems had decreased after the intervention. Colonnesi et al. (2013) did not find changes in parents’ sensitivity. Changes in parents’ mind-mindedness were not examined.
The Present Study
The aim of the present study was to perform a second, more comprehensive study on the effectiveness of the Basic Trust intervention in establishing a secure attachment relationship between internationally adopted children (aged 2–12 years) and their parents. We had expectations for eight different outcome measures: (1) parental mind-mindedness, (2) positive mind-related speech, (3) negative mind-related speech, (4) parental sensitivity, (5) child attachment insecurity, (6) child internalizing problems, (7) child externalizing problems, and (8) parenting stress. Since the intervention targets all primary caregivers, we expected that ratings of both mothers’ and fathers’ sensitivity as well as mind-mindedness would increase following the intervention. We also considered whether the emotional valence of parents’ mind-related speech changed, possibly as a result of changes in children’s behavior (problems). As mentioned above, adoptive parents may think about their child’s mind in a more negative way (Fishburn et al., 2017; Harris-Waller, 2012). Since parents may perceive motivational and behavioral changes in their child over the course of the intervention, the valence of mind-related comments may change. We, therefore, expected parents to display less negative and more positive descriptions of their child's mind after the intervention.
With regard to changes in children’s attachment, we expected decreases in avoidant, ambivalent, and disorganized attachment behaviors. We also expected the children’s internalizing and externalizing problems to decrease, as a result of the improved parent–child interactions and relationship. Because the training is assumed to enhance parents’ feelings of competence in managing the child’s emotions and behavior, we also expected a decrease of general parenting stress.
Method
Participants
A total of 53 Dutch adoptive families, including mothers and fathers, agreed to participate in this study. Figure 1 provides a flow diagram with the number of families at each assessment. Children (45.3% boys) were aged between 3 and 11 years old at pretest (M = 8.12 years, SD = 2.26). The mean age of placement in the adoptive home was 2.41 years (SD = 1.79 years, range = 0–6 years), and the majority (68.9%) of the children were placed after 12 months of age. At pretest, fathers had a mean age of 44.43 years (SD = 4.54; range = 32–51 years) and mothers 43.22 years (SD = 4.95; range = 29–53 years). On average, the socioeconomic status of the families was middle-to-high. The mean educational level of parents was fairly high (Mfathers = 3.80, SD = 0.81; Mmothers = 3.82, SD = 0.88, on a scale from 1 = primary education to 5 = university degree).
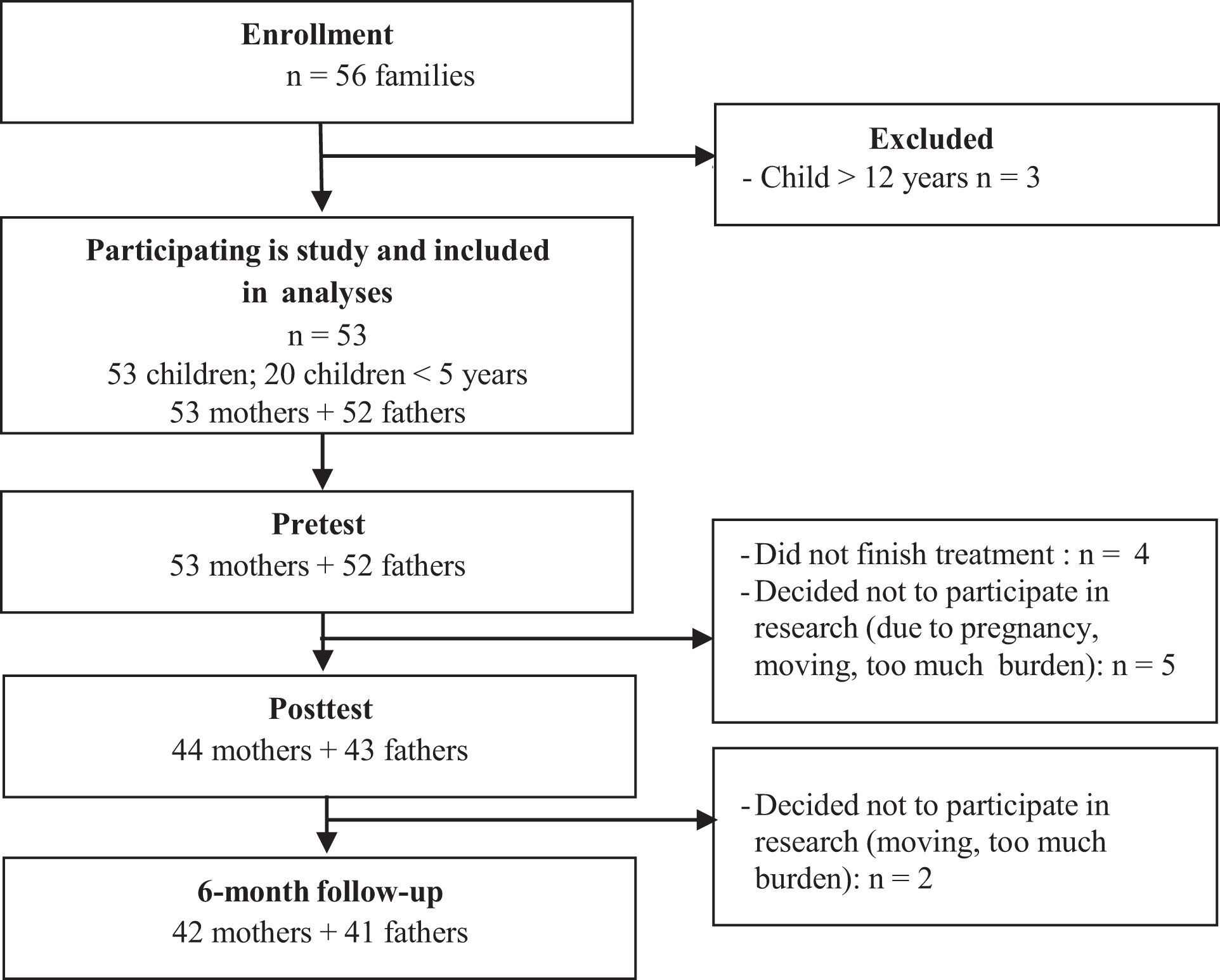
Flow diagram of the participants at each assessment.
Intervention and Research Procedure
The Basic Trust intervention is provided by Basic Trust, a Dutch national organization of qualified psychologists specialized in offering treatment for children with complex trauma or attachment problems. The psychologists follow an extensive 1- to 1.5-year training program in order to gain expertise in working with the Basic Trust treatment method, and they operate from their own treatment practice throughout different counties in the Netherlands. In the present study, eight therapists participated. Parents were typically referred to a Basic Trust therapist when their child had behavioral and/or emotional problems, and there was a presumption of attachment insecurity. Treatment started only when the Basic Trust therapist indicated that there was indeed a lack of secure attachment.
The Basic Trust intervention consists of on average eight sessions. In the present study, the average amount of sessions was 7 (range = 4–10 sessions). The intervention targets the involvement of all primary caregivers but can also be applied with secondary caregivers (e.g., school teachers). Involving both parents in the treatment process has shown to ameliorate the positive effects of parenting interventions in general and of attachment interventions specifically (e.g., Bakermans-Kranenburg et al., 2003; Lundahl, Tollefson, Risser, & Lovejoy, 2008). Both mothers and fathers took part in all sessions.
The present study involved a one-group pretest–posttest design including a pretest prior to the intervention, a posttest directly after the intervention, and a 6-month follow-up measurement. During each measurement time, parents filled in questionnaires, and a describe-your-child interview was conducted to assess parents’ mind-mindedness. Parents and children were videotaped for 10 minutes to assess parental sensitivity in a free-play interaction. Pretests were conducted at the treatment centers prior to the intake. Posttests and follow-up measurements were conducted at the family’s home because families appeared more willing to participate in the research if they did not have to travel to the treatment center for the purpose of the research only. The current study received permission from the ethical committee of the University of Amsterdam in February 2014 (Code: 2014-CDE-3395).
Instruments
Mind-mindedness
Mind-mindedness was assessed with the mind-mindedness interview (Meins et al., 1998). Parents were asked to describe their child, and answers were coded following the coding manual of Meins and Fernyhough (2015). Mind-mindedness is indexed by the proportion of mind-related attributes relative to the total amount of comments made by the parent. Mind-related descriptions were categorized by the type of internal state to which the parent referred: (a) mental descriptions (e.g., “she is a very curious girl”), (b) emotions (e.g., “he feels anxious in the presence of strangers”), (c) interests (e.g., she likes to read about historical events), and (d) the child’s preferences, needs, or desires (e.g., “he would like to have a little brother”). The emotional valence of each mind-related comment was classified as either positive, negative, or neutral based on the comments itself (see Demers, Bernier, Tarabulsy, & Provost, 2010). Finally, the other comments were not mind-related descriptions categorized in terms of behavioral (e.g., “he plays a lot of videogames”), physical (“she has green eyes”), and general descriptions.
Scores for both appropriateness and valence were computed as proportions of the total amount of comments parents made (Meins & Fernyhough, 2015). Trained coders (n = 4) independently rated the interviews, and 20% of the cases at each assessment (n = 56 in total) were randomly selected to calculate the interrater agreement among the coders. Interrater agreement on the proportion of mind-related comments per transcript was intraclass correlation (ICC) = .93, and for the coding of the valence of positive and negative comments, interrater agreement was ICC = .87 and ICC = .83 (Cicchetti, 1994).
Parental sensitivity
Parental sensitivity was measured with a 9-point sensitivity scale which was based on Ainsworth’s Original Sensitivity Scale (Ainsworth, 1969) and the Emotional Availability Scales (EAS-IV; Biringen, 2008). The EAS-IV are commonly used to assess parental sensitivity during free-play interactions between parents and children (Mesman & Emmen, 2013). The concept of parental sensitivity in the EAS-IV is broader than the original conception of Ainsworth, Bell, and Stayton’s (1974) sensitivity (which was constructed by observing infant–parent dyads). The EAS-IV highlight the positive, genuine, and creative communication between parent and child in addition to the appropriate responses. The addition of elements of the EAS-IV Scales was considered appropriate given the fact that we observed parent–child free-play interactions (and not natural home observations), and the EAS have previously been applied to assess sensitivity in parents of older children (Mesman & Emmen, 2013). The coding of the free-play interactions was performed by four independently trained observers who randomly coded recordings of the pre-, posttest, and follow-up. Twenty percent of the observations were coded twice to calculate interrater reliability. The reliability between the coders could be classified as excellent according to the guidelines of Cicchetti (1994), ICC = .86.
Attachment insecurity
The Attachment Insecurity Screening Inventory (AISI; Polderman & Kellaert-Knol, 2012; Spruit et al., 2018; Wissink et al., 2016) 2–5 years and 6–12 years were used to assess parents’ perspectives on the quality of the attachment relationship with their child aged between 2 and 5 years and 6 and 12 years. The questionnaire measures children’s insecure attachment behavior as reported by parents. Both versions of the questionnaire contain 20 6-point Likert-type items (never, sometimes, regularly, often, very often, and always) measuring total attachment insecurity by items belonging to three subscales: Avoidant, Ambivalent, and Disorganized Attachment Insecurity. A sum of these three subscales provides a total score for attachment insecurity.
Both questionnaires have been recently validated (Spruit et al., 2018; Wissink et al., 2016). Confirmatory factor analyses have demonstrated construct validity of the AISI, confirming the theoretically based factor solution, including the three subscales of attachment insecurity and one higher order total insecurity scale. It was furthermore reported that the AISI meets the demands of measurement invariance for the three-factor model across mothers and fathers (for the AISI 2–5 and 6–12) and across clinical and nonclinical groups (for the AISI 2–5). Further, for the AISI 2–5, convergent validity was supported by negative associations between the questionnaire scores and observed attachment security (Attachment Q–Sort (AQS); Waters & Deane,1985). Negative associations were found between observed parental sensitivity (Maternal Behavior Q-Sort, MBQS; Pederson, Moran, & Bento, 1999) and the AISI insecurity scores, while positive associations were found between psychopathology (Strengths and Difficulties Questionnaire; Goodman, 2001) and the AISI insecurity scores.
Reliability coefficients have previously been reported to range from sufficient to good for both questionnaires (Spruit et al., 2018; Wissink et al., 2016). For the AISI 2–5, Cronbach’s α was sufficient for the subscale Ambivalent Attachment (α = .67) and good for the subscales Avoidant Attachment (α = .80) and for Disorganized Attachment (α = .79). For the AISI 6–12, Cronbach’s α was sufficient for the subscale Ambivalent Attachment (α = .65) and good for the subscales Avoidant Attachment (α = .80) and Disorganized Attachment (α = .85). In the present study, similar internal consistency reliabilities at pre- and post-test were found for the AISI 2–5, α = .77 (avoidance), α = .64 (ambivalence), and α = .87 (disorganization), as well as for the AISI 6–12, α = .83 (avoidance), α = 70 (ambivalence), and α = .87 (disorganization).
Behavior and social–emotional problems
Parents completed the Child Behavior Checklist 1.5–5 or 6–18 (CBCL; Achenbach & Rescorla, 2000, 2001), which are standardized questionnaires on emotional and behavioral problems of children aged 1.5–5 years or 6–18 years. Parents rate the child’s behavior of the past 6 months using a 3-point scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). The CBCL 1.5–5 and 6–18 yield 99 and 120 items, respectively, and reflect Diagnostic and Statistical Manual of Mental Disorders-IV (American Psychiatric Association, 2000)-oriented subscales. Both questionnaires yield sum scores on internalizing behaviors and externalizing behaviors. A T score of 65 or below is considered to fall within the normal range, 65–70 within the borderline clinical range, and above 70 indicates parents’ clinically significant concerns.
Parenting stress
Parenting stress was assessed with the Dutch Questionnaire “Opvoedingsbelastingvragenlijst” (OBVL; Vermulst, Kroes, de Meyer, van Leeuwen, & Veerman, 2011). The OBVL is based on the Parenting Stress Index (Abidin, 1995), measuring parenting characteristics and the quality of the parent–child interactions. A total of 57 items measure five separate domains of parenting stress: (a) the caregiver–child relationship (10 items; the degree to which the caregiver experiences this relationship as problematic), (b) parenting competence (12 items; the degree to which the caregiver perceives to possess enough parenting skills), (c) depressive states (12 items; the degree to which a caregiver is content with him- or herself and life conditions), (d) role limitations (11 items; the degree to which a caregiver perceives the parental role as a containment on their own freedom), and (e) health complaints (12 items; the degree to which a caregiver feels physically unhealthy).
The questionnaire has shown high factor loadings and a satisfactory fit for the five subscales (Cronbach’s α ranging from .74 to .84) and the total parenting stress scale (Cronbach’s α = .89; Vermulst et al., 2011). In the present study, only the total scale was used, which showed an internal consistency reliability of α = .91.
Statistical Analyses
Multilevel analyses were performed to test the main hypotheses of the study using Statistical Package for the Social Sciences 22 (IBM, 2015) and the R 3.5.0 software environment to examine treatment effectiveness and factors that were important for predicting treatment effectiveness: gender of the parent, child age during placement, and number of treatment sessions. Multilevel analysis accounts for possible nesting of data, which means that data are organized at more than one level (e.g., individuals nested within certain contexts). In this study, measurement occasions (Level 1: pretests, posttest, and follow-up’s) were nested within individual respondents (Level 2: mothers and fathers), and respondents were nested within families (Level 3). ICCs were calculated to indicate how much of the variability in a particular variable was associated with differences between mothers and fathers (Level 2) and families (Level 3; Tabachnick & Fidell, 2013). Intraclass correlations at the second level ranged from low (ICC = .06) for the model including mind-mindedness to substantial (ICC = .39) for the model including attachment parenting stress. Intraclass correlations on the third level ranged from low (ICC = .09) for the model including mind-mindedness to high (ICC = .64) for the model including externalizing behavior problems. Besides accounting for nested data, an advantage of multilevel modeling is that missing data can be handled and imputation is not needed (Kreft & de Leeuw, 1998). Thus, this approach allows for the use of all available data including the data of the families with a pretest only. Analyses were thus ran with 53 families that completed at least the pretest measures.
All variables were normally distributed. The proportion of mind-related comments and ratings of avoidant attachment had extreme scores (z-score > 3.29, Tabachnick & Fidell, 2013). The variables with outlying scores were winsorized, and analyses were performed twice, once with the raw scores and once with the winsorized variables. The results were similar, suggesting that the extreme scores did not have a disproportionally large influence on the outcomes. We, therefore, decided to report the results on the analyses including the raw data in this article.
Results
Before running the main analyses, we checked whether the outcome variables were related to parent (educational level and age), child (age, age during placement, and gender), and therapist (gender, years of experience of working with the intervention) characteristics. Mothers with a higher educational level were classified as more sensitive during pretest, r(53) = .23, p = .011. Mothers’ educational level was, therefore, included as a covariate in the multilevel analyses on parental sensitivity. Child outcomes (behavior problems and attachment insecurity) were unrelated to child gender and age during placement, and the gender and experience of the therapists were unrelated to all outcome measures.
The means and standard deviations of the outcome variables on the three measurement occasions are presented in Table 1. Correlations between the outcome variables during pretest are presented in Table 2. Lastly, Table 3 shows the associations between mothers’ and fathers’ reports of attachment insecurity, behavior problems, and parenting stress as well as correlations between mothers’ and fathers’ mind-mindedness and sensitivity. Maternal and paternal reports of child internalizing and externalizing problems were highly correlated over all assessments (range rs from .52 to .78). Similar patterns were shown for parents’ reports on attachment insecurity, although reports on avoidant and ambivalent attachment behaviors were unrelated at the follow-up measurement. Mothers’ and fathers’ parenting stress scores were highly correlated at pretest, r(53) = .60 but were unrelated at both posttests. Couples’ sensitivity scores were associated at all measurement times (range rs from .40 to.60). Lastly, mothers’ and fathers’ levels of mind-mindedness were unrelated to each other at all assessment times.
Means and Standard Deviations of the Outcome Measures for Each Assessment Time.
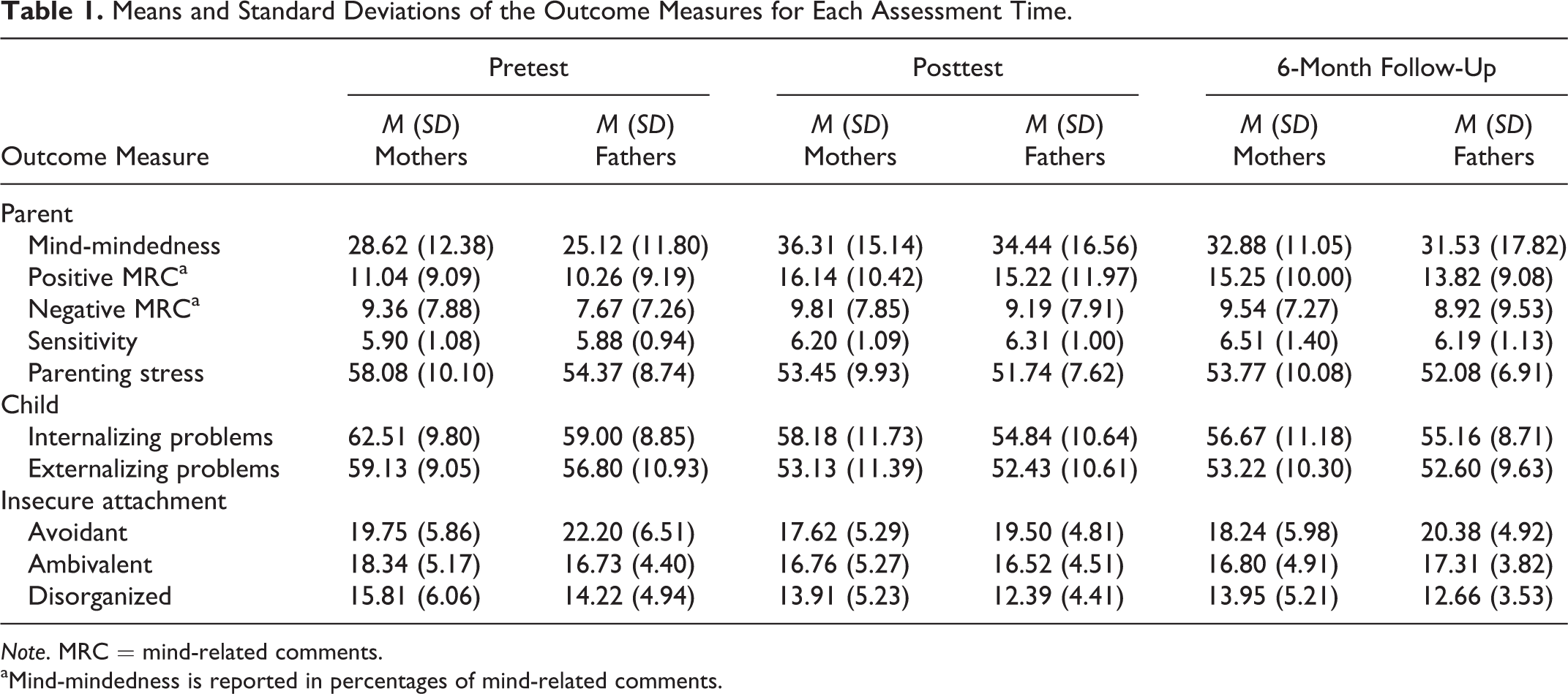
Note. MRC = mind-related comments.
aMind-mindedness is reported in percentages of mind-related comments.
Pearson’s Correlation Between the Outcome Measures at Pretest.
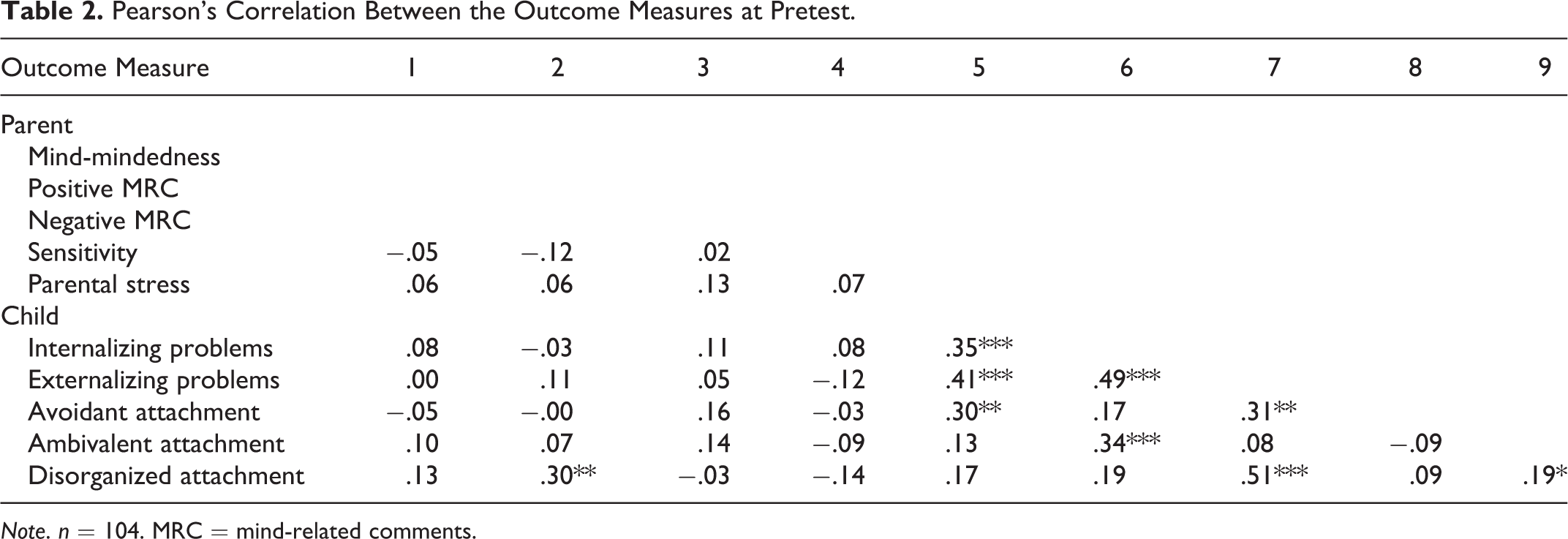
Note. n = 104. MRC = mind-related comments.
Pearson’s R Correlations Between Maternal and Paternal Measures at Pretest, Posttest, and Follow-Up.
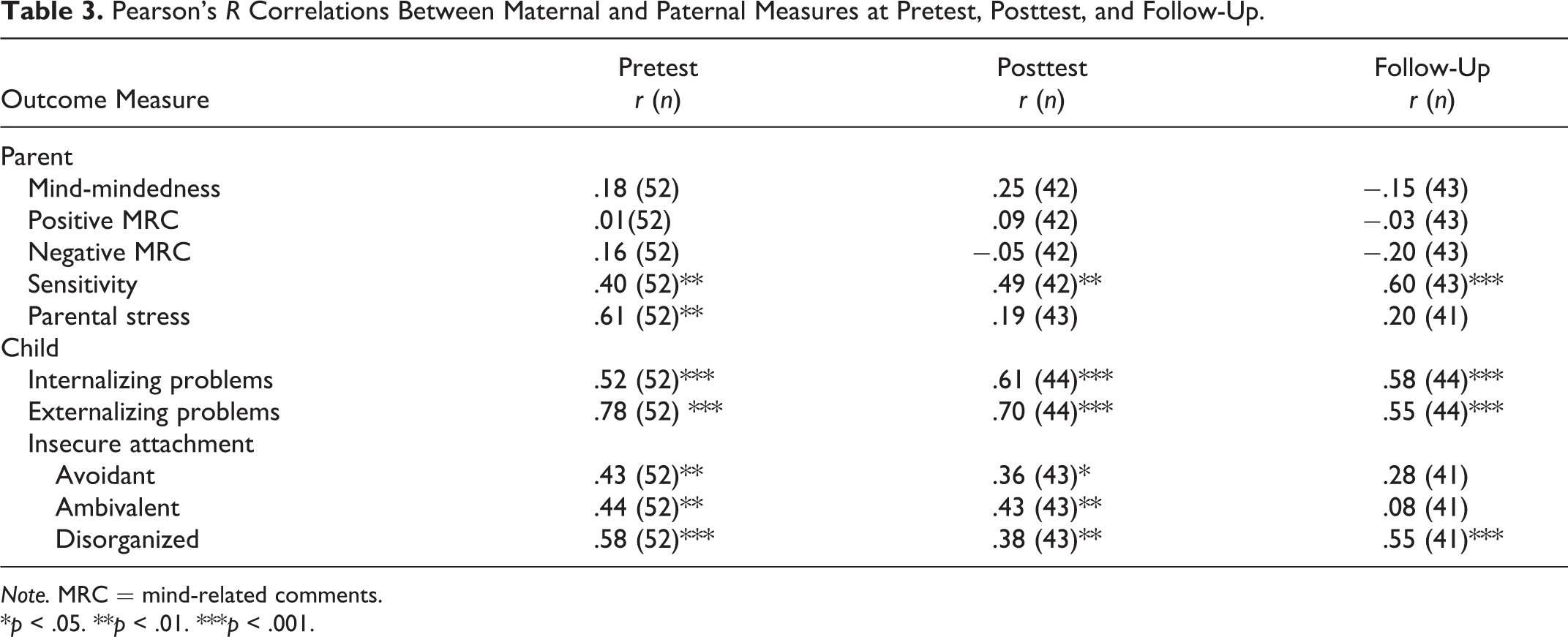
Note. MRC = mind-related comments.
*p < .05. **p < .01. ***p < .001.
Results of the multilevel analyses are presented in Table 4. This table displays the results of the overall intervention effects (mothers and fathers combined) on the parent and child outcome measures.
Main Effects of the Multilevel Analyses for Parents’ Mind-Mindedness, Sensitivity, and Stress, and Children’s Behavior Problems and Insecure Attachment.
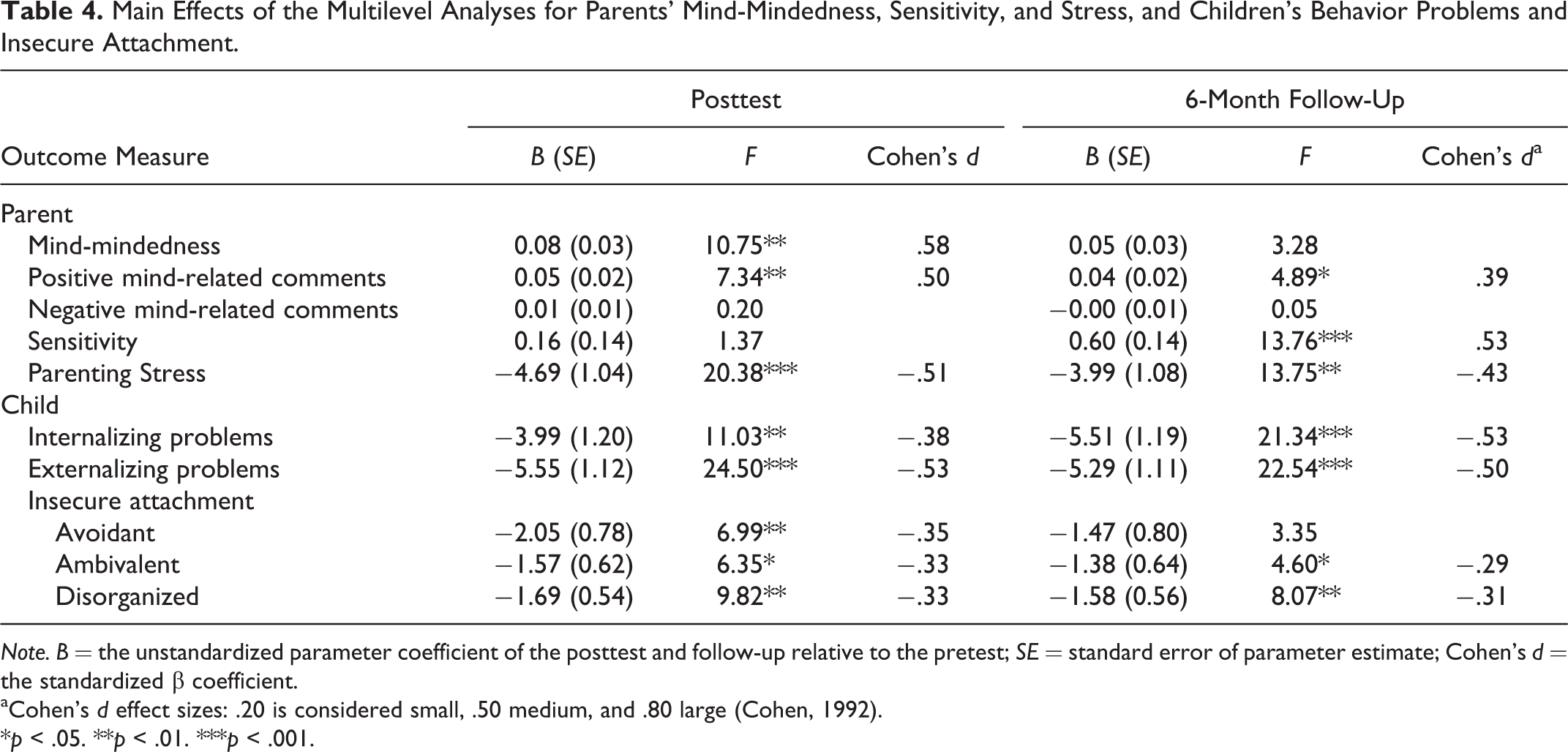
Note. B = the unstandardized parameter coefficient of the posttest and follow-up relative to the pretest; SE = standard error of parameter estimate; Cohen’s d = the standardized β coefficient.
aCohen’s d effect sizes: .20 is considered small, .50 medium, and .80 large (Cohen, 1992).
*p < .05. **p < .01. ***p < .001.
Mind-mindedness
Parents showed a significant increase (8%) in mind-related descriptions from pre- to post-test (medium-to-large effect size). From pretest to follow-up, the increase in mind-related descriptions was 5% but not significant.
Positive mind-related speech
Parents made significantly more positive mind-related descriptions at posttest (medium effect size) and follow-up (small effect size). From pre- to post-test, positive mind-related descriptions increased with 5% and from pre-test to follow-up with 4%.
Negative mind-related speech
Parents did not make less negative mind-related descriptions at both the posttest and follow-up.
Sensitivity
Parental sensitivity did not significantly increase from pre- to post-test but did from pretest to follow-up (medium effect size), showing a mean increase of 0.6 (on a scale from 1 to 9).
Internalizing problems
Parent reports on children’s internalizing problems showed a significant decrease from pre- to posttest (small-to-medium effect size) and follow-up (medium effect size). Compared to pretest, the mean T score was 4.3 lower at posttest and 5.8 lower at follow-up.
Externalizing problems
Parent reports on children’s externalizing problems showed a significant decrease from pre- to post-test (medium effect size) and follow-up (medium effect size). Compared to pretest, the mean T score was 5.2 lower at posttest and 5.1 lower at follow-up.
Insecure and disorganized attachment
Parent reported a significant decrease in children’s avoidant attachment behavior from pre- to posttest (small-to-medium effect size) but not from pretest to follow-up. Ambivalent and disorganized attachment behaviors were reported to be lower at both posttest (small-to-medium effect sizes) and follow-up assessments (small effect sizes) compared to pretest.
Parenting stress
Parents reported a significant decrease in parenting stress from pre- to posttest (medium effect size) and from pretest to 6-month follow-up (small-to-medium effect size). Compared to pretest, the mean T score was 4.6 lower at posttest and 4.3 lower at follow-up.
Mothers and fathers
We added interaction effects to test whether the intervention effects were different for mothers and fathers. The results of these analyses are presented in the Supplemental Material. Taken all assessments together, fathers reported less parenting stress, less avoidant and ambivalent attachment behaviors as well as less internalizing problems of their children. Mothers and fathers did not show differences in changes from pre- to post-test or pretest to follow-up.
Number of treatment sessions
We performed some additional analyses to check whether child treatment effects were dependent on children’s gender and age during placement and number of treatment sessions. Taken all measurement occasions together, children with higher levels of externalizing problems and avoidant and disorganized attachment had a higher number of treatment sessions. The number of treatment sessions was also related to parenting stress; families in which parents reported higher levels of stress over all assessments received more treatment sessions. The interaction effect between internalizing problems and number of treatment sessions was significant. This means that when children showed less decline in internalizing problems from pre- to posttest, the number of treatment sessions was larger.
Discussion and Applications to Practice
The present study examined whether the Basic Trust intervention led to an increase in parents’ mind-mindedness and sensitivity and to a decrease in attachment insecurity, disorganization, and behavior problems in a sample of 53 families with internationally adopted children. Overall, parents’ mind-mindedness increased from pre- to posttest but not from pretest to 6-month follow-up, whereas parents’ sensitivity showed improvement only at the follow-up. Children’s attachment insecurity and disorganization and behavior problems decreased from pretest to both posttest and follow-up. Parenting stress decreased from pre-test to posttest, and this effect sustained at the 6-month follow-up. Taken all measurement times together, fathers reported less parenting stress and lower rates of internalizing problems and attachment insecurity. Intervention effects, however, were not different for mothers and fathers. Thus, although fathers generally reported less stress and child emotional problems, they reported a similar decrease in problems compared to mothers.
First of all, behavior indicative of an ambivalent, avoidant, or disorganized attachment style diminished directly after the intervention, and children showed less internalizing and externalizing problems after the intervention. These effects sustained at the 6-month follow-up, with an exception of behavior indicative of an avoidant attachment style. In a prior study on the Basic Trust intervention, posttest measures were conducted 6 months after the intervention had ended. Children’s levels of avoidant and ambivalent attachment (to mothers only) were lower, but these decreases were not significant (Colonnesi et al., 2013). Children’s levels of disorganized attachment to both parents, however, were significantly reduced after 6 months (medium-to-large effect sizes).
It was argued that enhancing parents’ mind-related speech is especially helpful in improving children’s organization of their affects (Colonnesi et al., 2013; Sharp & Fonagy, 2008). The present study showed a slightly different picture: Both mothers and fathers reported less attachment insecurity at posttest and follow-up on the three subscales of the AISI, with small-to-medium effect sizes. At the follow-up assessment, the decrease in disorganized attachment behaviors remained strongest for this sample (d = 0.31).
The present study did not replicate the medium-to-large effect sizes for disorganized attachment of the previous study of Colonnesi and colleagues. The differences in outcomes could be due to sampling differences. However, methodological concerns may also underlie this outcome. In the study of Colonnesi et al., an observational measure of attachment security and organization was used (AQS; Waters & Deane, 1985), whereas the AISI, a questionnaire on children’s insecure and disorganized attachment behavior, was used in the present study. Wissink et al. (2016) reported only weak correlations between the parent-reported AISI scores and observed attachment security on the AQS. The AQS could have been more sensitive in detecting changes in disorganized attachment behavior. On the other hand, differences in the outcomes on attachment security (ambivalent and avoidant attachment) could also have been due to the small sample size of the previous study, which implies less statistical power to detect smaller pre- to post-test differences. The use of a multilevel approach to analyze the data contributed to maximizing the power in the present study. The multilevel approach also proved to be important in this study since we found associations between paternal and maternal reports of attachment and behavior problems as well as associations between mothers’ and fathers’ sensitivity at all measurement occasions. Taken the results from this and the previous study together, there seems to be some support that the Basic Trust intervention changes disorganized attachment behaviors.
An innovative aspect of the Basic Trust intervention is the explicit focus on parents’ use of mind-mindedness. Parents showed more mind-related speech after the intervention, suggesting that their level of mind-mindedness increased as a result of the treatment. Before the intervention, 28% of parents’ descriptions were related to mental aspects of the child. After the intervention, the percentage of mind-related descriptions was 36. Because the intervention is focused explicitly on retrieving and verbalizing appropriate explanations for the child’s behavior, rather than dismissing the behavior as being difficult or exhausting, parents may have been inclined to verbalize more mental characteristics during the describe-your-child interview. We hypothesized that parents would show more positive and less negative mind-related descriptions after the intervention (Fishburn et al., 2017; Harris-Waller, 2012). The percentage of negative mind-related comments at pretest was surprisingly low (9%) considering that all parents expressed major concerns about their child during intake sessions. At posttest, positive mind-related descriptions showed an increase of 5%, whereas percentages of negative comments were the same as at pretest. The intervention may thus have led to parents producing more positive, but not necessarily less negative, comments on their child’s mind.
At the follow-up assessment, the proportion of mind-related speech was still 5% higher than at pretest, but the difference was no longer significant. For some parents, it may be difficult to maintain a mind-minded stance when the child encounters new difficulties, particularly when the families face other stressors (e.g., work-related stress, medical or mental health problems of the parent, having multiple children with emotional or behavioral difficulties; van Aar, Leijten, Orobio de Castro, & Overbeek, 2016). Booster sessions may be helpful to prevent a fade-out effect, although there is little research to support the effectiveness of maintenance treatment in parenting interventions (e.g., Eyberg, Boggs, & Jaccard, 2014; Eyberg, Edwards, Boggs, & Foote, 1998; van Aar et al., 2016). During the follow-up assessments, we observed that some parents continued to actively use the Basic Trust method at home (i.e., verbalizing their child’s and their own thoughts and feelings), whereas other parents did not. This discrepancy in parents’ behavior might have been present already during the intervention period and could explain why the effect on parental mind-mindedness shows a slight fade-out 6 months postintervention. Future studies should therefore take into account a measure of treatment fidelity and motivation.
Interestingly, parents’ sensitivity was not enhanced directly after the intervention but did increase at the 6-month follow-up. This result indicates that parents show a change in their mind-mindedness before they show a change in parental sensitivity. Modification of maladaptive cognition is thought to be the process by which therapy is effective (Beck, 1970; DeRubeis, Tang, & Beck, 2001). The operationalization of mind-mindedness, as opposed to the operationalization of sensitivity, unites the mental or cognitive tendency of parents to form theories on their child’s mind (i.e., mentalizing) and parents’ behavioral tendency to translate these theories into words (Meins, 2013). The outcome that improvement in mind-mindedness preceded improvement in sensitivity suggests that the intervention first changes parents’ cognitions and perceptions of the child, after which changes in their behavior took place (i.e., sensitive responding). Prior to the intervention, one of the participating fathers held the belief that his son “is constantly seeking out a conflictual confrontation during dinner.” After the intervention, the father believed that his son “was angry because he was feeling rejected by my frequent commenting on his eating behavior.” In this example, the father initially gave an explanation of the child’s behavior. After the intervention, he was able to turn to the child’s motivation underlying the behavior. It may be that after the process of cognitive change, parents can (behaviorally) engage in more sensitive interactions with their child (e.g., responding to the anger with compassion instead of frustration). The outcomes may also be explained by the main focus of the Basic Trust intervention, which is the instruction on the content of parents’ verbal response. Verbalizing mental states was very new to most parents and required explicit attention and effort from the parents. Directly after the training, parents may, therefore, have been focused primarily on the verbal responses to their child and to a lesser extent on their nonverbal behavioral reactions.
The effect sizes on parent outcomes were medium, whereas the effect sizes for the child outcomes could be considered small to medium (Cohen, 1992). These results are in line with the effects of the Video-Feedback Intervention to Promote Positive Parenting and Sensitive Discipline (VIPP-SD), a widely used preventive attachment intervention (Juffer, Bakermans-Kranenburg, & van IJzendoorn, 2008). The VIPP-SD was designed for parents of children aged 0–6 years and has similar aims and methods as the Basic Trust intervention (i.e., promoting sensitive caregiving by means of video feedback; see Juffer, Struis, Werner, & Bakermans-Kranenburg, 2017 for an overview of the intervention elements). A recent meta-analysis on the effectiveness of the VIPP-SD included 12 randomized controlled trials (Juffer, Bakermans-Kranenburg, & van IJzendoorn, 2017). The meta-analysis showed that overall parents’ sensitivity increased after the intervention (pooled effect size of d = 0.47). Children’s behavior problems decreased (d = 0.26; k = 7). Only four studies investigated the intervention’s effect on attachment security, which pooled together showed an effect size of d = 0.36. The present study’s results are in line with the effects of the VIPP-SD, suggesting that short sensitivity-focused video-feedback interventions may be useful in preventing but also decreasing attachment problems.
It would be interesting to study whether an explicit focus on enhancing parents’ mind-related speech raises the effectiveness of attachment interventions. In other words, is it necessary to explicitly instruct parents to verbalize the child’s inner state? To examine this, it may be useful to compare the Basic Trust intervention to a similar intervention which puts less emphasis on promoting parents’ use of mental state language (e.g., VIPP-SD). Microtrials may also be useful tools to study what specific factors of a short intervention bring about the change in children’s sense of security (Klasnja et al., 2015).
The present study had limitations that should be addressed in future studies on the effectiveness of the Basic Trust intervention. First of all, conclusions about causality and placebo effects are limited by the lack of a (randomized) control group. Second, the sample size of the study was small, with 44 families completing the posttest assessment. Third, we used parent-report questionnaires to assess changes in child outcomes, and therefore, we cannot be sure that the effects were reflecting actual changes in behaviors of children and were not, for instance, demand effects. Moreover, we used the representational measure of mind-mindedness. It is recommended that the mind-mindedness of caregivers of older children (who are able to speak) is assessed with the mind-mindedness interview and not with the online observational measure of mind-mindedness (Meins & Fernyhough, 2015). That is, when children are able to speak, parents’ mind-related speech may be influenced greatly by what children say to their parents during interactions (Meins & Fernyhough, 2015). However, the representational operationalization of mind-mindedness may not have entirely captured the change in the core focus of the Basic Trust training, which is to verbalize children’s behavior, thoughts, and feelings during actual parent–child interactions. One study showed that the observational and representational (interview) measure of mind-mindedness are moderately correlated (r = .40; Meins et al., 2003), while another study reported no correlation between the observational and representational measure of mind-mindedness (Illingworth, MacLean, & Wiggs, 2016). The increase in mind-related speech during the interview implies that parents were more inclined to think about their children’s mind states than before the training. However, whether the intervention also led to changes in the interactional mind-related speech remains to be investigated. Lastly, a questionnaire on insecure attachment behaviors (AISI) was used with reliability coefficients ranging from sufficient to good. These reliability statistics may have been insufficient for the use of the questionnaire for individual diagnoses.
Altogether, these limitations imply that we should be careful about drawing strong causal conclusions from this study. A next step should be to (randomly) assign participants to a control group to study if the effects can be ascribed to the intervention with more certainty. Also, the Basic Trust intervention focuses primarily on changing parental behavior, which in turn may result in changes in children’s attachment security. We recommend that future studies investigate a model in which changes in caregiver behavior are modeled as a predictor of change in child attachment security, using a larger sample size. Lastly, future research should address whether the Basic Trust intervention is equally effective in biological and foster care families, as well as families with lower socioeconomic backgrounds, as the current sample primarily consisted of families from middle-to-high socioeconomic status.
Conclusion
The present study replicated the positive results of a previous study on the effectiveness of the Basic Trust intervention in a sample of families with internationally adopted children (Colonnesi et al., 2013). The results imply that the intervention reduces child attachment insecurity and disorganization as well as child behavior and emotional problems. Further, the outcomes suggest that the intervention enhances adoptive parents’ mind-mindedness and, in the longer term, sensitive caregiving behavior. Future studies should examine whether the results of the present study can be replicated under conditions of strict experimental control and in other types of families with children at risk of insecure attachment (e.g., foster or biological families).
Supplemental Material
Supplemental Material, Appendix_A - Remediating Child Attachment Insecurity: Evaluating the Basic Trust Intervention in Adoptive Families
Supplemental Material, Appendix_A for Remediating Child Attachment Insecurity: Evaluating the Basic Trust Intervention in Adoptive Families by Moniek A. J. Zeegers, Cristina Colonnesi, Marc J. Noom, Nelleke Polderman and Geert-Jan J. M. Stams in Research on Social Work Practice
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.