
Abstract
Emergency Medical Service (EMS) responders deliver patient care in high-risk, high-stress, and highly variable scenarios. This unpredictable work environment exposes EMS responders to many risks, one of which is violence. The primary goals of this systematic literature review were to (1) define the issue of violence experienced by EMS responders and (2) identify the risk factors of violence associated with the EMS profession. An innovative inclusion of industrial literature with traditional peer-reviewed literature was performed. Of 387 articles retrieved, 104 articles were assessed and reviewed. Career exposure for EMS responders to at least one instance of verbal and/or physical violence was between 57 and 93 percent. There is a great need for rigorously designed, nationally representative examinations of occupational exposures in order to better understand the temporal associations of violence, cumulative occupational stressors, and the outcomes of physical and psychosocial injuries that are occurring as a result of exposures to violence.
Introduction
The Centers for Disease Control and Prevention and National Institute for Occupational Safety and Health (NIOSH) define workplace violence (WPV) as “violent acts, including physical assaults and threats of assaults, directed toward persons at work or on duty.” 1 The often unrecognized psychosocial component of violence is further refined in the World Health Organization’s definition of WPV as “incidents where staff are abused, threatened or assaulted in circumstances related to their work, including commuting to and from work, involving an explicit or implicit challenge to their safety, well-being or health.” 2 Health-related industries, particularly those involving patient care, experience the highest rates of WPV compared to all other industries—with patients described as the most significant contributor to provider injuries resultant from violence. 3
In the United States, the Emergency Medical Services (EMS) profession is comprised of approximately nine hundred thousand paid and unpaid (volunteer) EMS providers, responsible for an estimated annual patient volume of twenty-two million. 4 Due to the lack of a centralized licensing body, capturing a true estimate of the total number of EMS agencies and providers on a national level is difficult. 5 Increasingly, 911 emergency response systems are experiencing a departure from fire-related calls, toward a greater number of calls for EMS. 6 Of the 34.7 million calls to 911 in 2017, the average majority (64%) were for medical assistance 7 with some fire departments experiencing upward of 80 to 90 percent of their call volume dedicated to the EMS side of their work. 8 In 2015, there were twenty-nine million calls for EMS services, a 23 percent increase from 2014. 9 This increase represents a continually growing trend in the United States. Subsequently, the 911 response system is strained and increasingly calling upon EMS responders to deliver services 6 contributing to their feelings of being “banged-up and burned out.” 10 Feelings of burnout coupled with exposures to violent incidents can have lasting impacts upon EMS providers. 11
Increased community demand for services necessitates increased patient interactions, thereby increasing the injury potential to EMS responders. In 2016, approximately three thousand five hundred EMS responders were treated in the emergency department (ED) due to injuries sustained from violence. 12 A retrospective cohort study of nationally registered Emergency Medical Technicians (EMTs) found that assault was the cause for 8 percent of fatal injuries. 4 While these numbers may seem small in comparison to the nature and cause of other leading occupational injuries and fatalities in the fire and rescue service, there is evidence to believe injuries related to violence are vastly underreported due to the nonexistence of policies, procedures, and practices to support reporting of such incidents.6,11 Yet, work-related injuries among EMS responders were three times higher than the national average for all other occupations in 2013. 4 The rate of occupational fatalities among paramedics is more than twice the national average for all occupations and comparable to the rates of police and firefighters at 12.7 per one hundred thousand workers per year. 13 The rate of nonfatal injuries among paramedics is more than five times higher than the national average for all workers at 34.6 per 100 full-time workers per year. 14 Fatal assault (i.e., homicide) was found to be the third leading cause of death for EMS workers upon review of three fatality databases. 13
Serving as a crucial public health safety net, EMS is in a constant state of response to the persistent and emerging health needs of the community. 15 As a result, EMS responders are expected to provide patient care in unpredictable and ever-changing environments, and while some occupational hazards are “clear and imposing,” others, like violence, can be “insidious and silent.” 16 While legally, no EMS responder must unreasonably place their own life in jeopardy as maintained in the Occupational Safety and Health Act’s (OSHA) General Duty Clause, Section 5(a)(1) of 1970, 17 the expectations of the community coupled with the internalized belief among responders that they exist to serve frequently place the safety of the responder as secondary to the safety and well-being of the patient. 18
Less than a decade after the formal recognition of the EMS system in 1973, 19 industry publications mentioning violent patient encounters began to surface. 20 The year 1978 marks the beginning of a decades-long conversation by the EMS industry about violence experienced in the workplace when the phenomenon “aggression begets aggression” was first noted. 20 Similar sentiments continue to be voiced by emergency medical providers four decades later. 11 By contrast, the first academic study was published in 1993. 21 Research on violence against EMS responders categorized violence as verbal abuse, physical abuse, property damage or theft, sexual harassment, sexual assault, and intimidation.22–27 Acts of violence against EMS responders have been reported as “struck by patient,” “punched in the face by a drunkard,” “tackled by a large man,” and “assaulted by a combative patient.” 11 Formal recognition of this issue is increasing; however, compared to other healthcare settings, WPV in the prehospital setting is inadequately described and requires further consideration.21,24,27–31
The primary objective of this literature review was to describe what is known about the phenomena of violence against EMS responders by patients and bystanders. An innovative approach was taken to include academic and industrial publications. The second objective of this literature review was to identify risk factors and outcomes of violence in EMS.
Methods
Literature Search Strategy
This systematic review was conducted in accordance with the preferred reporting items for systematic reviews from the PRISMA-P checklist. 32 Review of industrial literature has been excluded from prior academic research on this topic. We chose to include the voices and perspectives of the industry to provide a more complete and comprehensive representation of the violence experienced by EMS responders. Three academic databases (PubMed, CINHAL, and Web of Science) were utilized systematically and iteratively to collect manuscripts from peer-reviewed and industrial trade journals, using EMS-specific terminology (Table 1). Medical Subject Headings (MeSH) operationalized the search by providing delineated sets of terms allowing various levels of specificity and contributing to the collection of relevant literature. As such, the term “Emergency Responder” when used with the MeSH subject heading automatically included the terms Emergency Medical Technician, Firefighter, and Police in the search results. MeSH subject headings were only used if the MeSH hierarchical terms were relevant to the field of EMS (e.g., “emergency responder” was used with MeSH headings because it returned results pertaining to EMTs and firefighters). In each database, operands and operators (e.g., “AND,” “OR,” and “NOT”) increased the number of relevant manuscripts as they permitted emphasis on desired search terms (e.g., assault OR violence) and excluded any unwanted subjects or terms (e.g., police). Additionally, the asterisk indicated in Table 1 denotes searching for a derivate of the search term.
Literature search terms used to retrieve academic peer-reviewed literature and industry publications through PubMed, CINHAL and Web of Science.
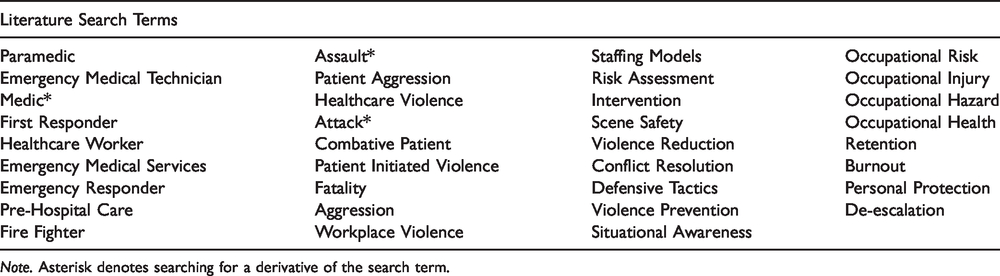
Note. Asterisk denotes searching for a derivative of the search term.
Selection of Articles for Review
The literature review was conducted in three phases: Phase 1 involved evaluating each article based on its title, abstract, and keywords; Phase 2 involved reviewing, assessing, and documenting titles and abstracts in chronological order; Phase 3 involved reviewing, assessing, and documenting the full articles of those deemed relevant based on the first two phases. In Phase 3, literature was coded per an iterative process in which major themes were recognized and cataloged. Phase 3 also included manual searches of the retrieved articles for additional references. A total of 104 full-text articles were reviewed for in-depth analysis based upon prioritization and relevance to our research question (Figure 1).
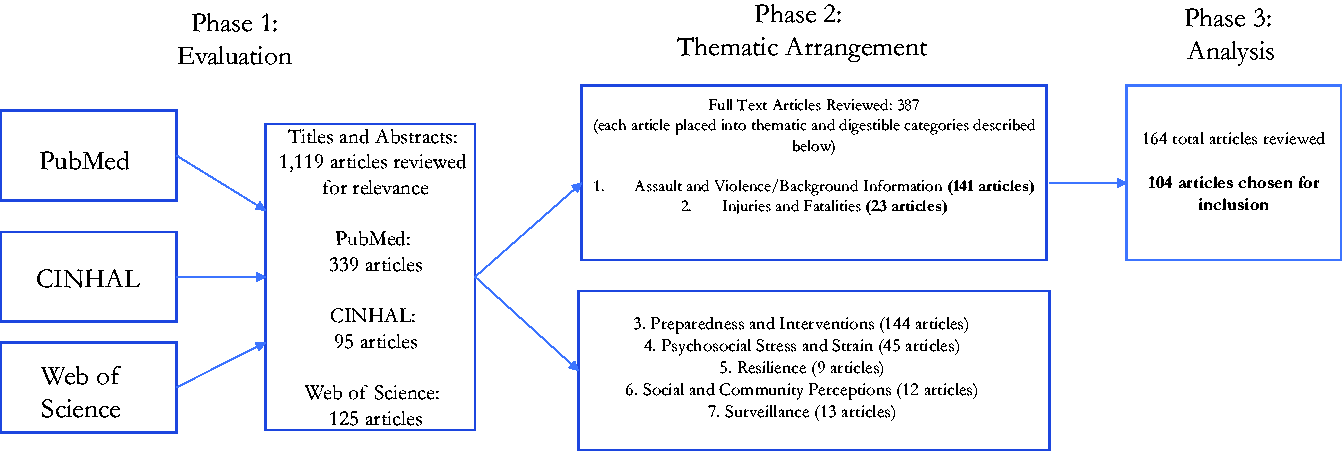
Flow diagram of literature search and retrieved results.
Criteria for Inclusion and Exclusion
The researchers decided the inclusion or exclusion of specific articles based on the process described here, which is consistent with current literature review convention. 33 Articles were excluded if (1) they did not discuss violence to EMS providers, (2) were published in a non-English language, (3) full-text versions were unavailable, and (4) were not in a prehospital environment or ED. All literature relating to the issue of violence in EMS published prior to 31 December 2016 was considered. Endnote, a referencing software tool, was used to assist with deduplication, ease of access, and citation of manuscripts. Special effort was made to find evaluated studies that would give rise to an evidence base of effective violence prevention interventions. While academic literature allows for enumeration and quantification of violence, industry publications discuss specific knowledge neglected by the scientific literature and provide a rich contextual portal into the realities of EMS work. Therefore, it was determined early in the literature search that industry-specific publications, such as trade journals and magazines would be included in this review.
Results
Of the 104 articles we retained for analysis, thirty-six were from industrial trade journals and sixty-eight articles were from academic journals (see online supplements Tables 2 and 3). Of the sixty-eight peer-reviewed articles, twenty-seven articles provided some estimate of violence (see online supplement Table 4). Of the twenty-seven articles measuring the prevalence of violence, fifteen articles defined or described the types of violence being measured.
The articles retained for analysis revealed eight key themes: “evolution of the definition of workplace violence,” “estimates of violence,” “psychosocial impact (stress),” “EMS responder-level characteristics,” “characteristics of perpetrators of violence,” “reporting/underreporting,” “industry best practices, policies, and procedures,” and “intervention and policy opportunities.” The tables include a descriptive statement, summary of major findings, and weight of evidence assessment for each article.
Evolution of the Definition of WPV
Definitions of WPV in EMS have gradually evolved to encompass more comprehensive classifications as the EMS system has developed. For instance, one of the first industry definitions of WPV defined it as “violent client behavior destructive to self, others or property.” 34 As previously stated, evaluation of the definition became inclusive of psychological impacts including cumulative stress and burnout. 2
Often, the definitions used to measure violence in research are purposefully selected and operationalized by the researcher, thereby resulting in varying violence measures. 35 In EMS-focused research on WPV, many survey studies do not define violence for the participants. When no definition of violence is predetermined or defined, it may be concluded that the interpretation of violence may vary significantly from participant to participant. 35 Across selected studies, no standardized definition of violence was used. Of studies measuring frequency of violence, 37 percent (ten out of twenty-seven articles; see online supplement Table 3) did not define or differentiate between types of violence (i.e., verbal assault versus physical assault).4,21,26,27,36–41 In 15 percent of studies (four out of twenty-seven), violence was determined after using other proxy terms such as “homicide” or injury-related terms.11,13,14,42
The lack of a standardized definition of WPV is problematic when attempting to describe the prevalence of violence, risks of exposure, and types of violence experienced. The American College of Emergency Physicians has recognized this limitation and has emphasized the importance of categorizing violence against EMS responders.
43
In response, we found the work of Koritsas et al. to be comprehensive and more highly utilized than any other definitions in the EMS literature, defining types of WPV against EMS responders:
Verbal abuse: a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s) using offensive language, yelling, or screaming with the intent of offending or frightening you. It can include threats of abuse over the phone but excludes sexual harassment and sexual assault. Property damage or theft: a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s) causing damage to, or stealing property belonging to you, your family, or your workplace. It includes damage to or theft of a vehicle, personal effects, home contents, office equipment and supplies, or office furnishings. Attempted theft of the above items is also included. Intimidation: a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s) purposely threatening, following you, or using gestures to purposely offend or frighten you. Physical abuse: a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s) physically attacking you, or attempting to attack you. It includes behaviors such as punching, slapping, kicking, or using a weapon or other object with the intent of causing bodily harm. Sexual harassment: any form of sexual propositioning or unwelcome sexual attention from a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s). It includes behaviors such as humiliating or offensive jokes and remarks with sexual overtones; suggestive looks or physical gestures; inappropriate gifts or requests for inappropriate physical examinations; pressure for dates; and brushing, touching, or grabbing excluding sexual touching (e.g., the genital or breast area). Sexual assault: any forced sexual act, rape or indecent assault perpetrated by a patient/client, their friend(s), family member(s), other professional(s), or work colleague(s). It includes brushing, touching, or grabbing of the genitals or breast. It also includes attempted sexual assault.
29
Thus, where applicable, we describe the extant literature in the following terms: verbal abuse, property damage or theft, intimidation, physical abuse, sexual harassment, and sexual assault.
29
Estimates of Violence
The key methods used to quantify the problem of violence against EMS responders have been cross-sectional surveys, direct observations, and injury reports. These methodological variations do not permit cross-comparisons between studies because they do not contain the same population denominator, and the intervals of violence measurement vary. While some studies assess career exposure, others compare rates of violence occurring over the last twelve months, three months, or one month. Thus, we can only describe the estimates and ranges of violence that exist compared to the population from which they were collected, and the appropriate time frame measured (see online supplement Table 4).
To date, there have been four studies conducted in the United States that may be considered nationally representative. These four studies utilized survey data from nationally certified EMS responders participating in the Longitudinal EMT Attributes and Demographics Study (LEADS) administered by the National Registry of EMTs.5,15,44,45 These data are the most comprehensive information on demographic characteristics and occupational injuries and exposures in EMS responders at the present time. Gormley et al. 44 note that while the National EMS Certification is required in forty-six states, nationally certified EMS responders are found in each state.
In studies measuring career prevalence, between 57 and 93 percent of EMS responders reported having experienced at least one act of verbal and/or physical violence during their career.21–24,26,27,46–48 A 2013 LEADS found that among the 1789 respondents of nationally registered EMTs in the United States, 69 percent experienced at least one form of physical and/or verbal violence in the last twelve months. 44 Furthermore, 44 percent experienced one or more forms of physical violence over the same study period. 44 Gormley et al. 44 defined violence in seven categories: cursing or making threats; punching, slapping, or scratching; spitting; biting; being struck with an object; stabbing or stabbing attempt; and shooting or shooting attempt. A New England study with a convenience sample of EMTs found the prevalence rate of violence to be 20.3/100 full-time employees/year. Thirty-eight percent of those surveyed reported multiple assaults within the last six months, and one EMT reported being assaulted nine times during that same six-month period. 38 Conversely, crude estimates from a study conducted in Southern California found a much lower frequency of 0.4 assaults per year per prehospital care provider. 27 Non-U.S. studies find comparable rates, with studies ranging from 67 to 88 percent of respondents whom reported some form of verbal and/or physical violence in the last twelve months.22,23,46 In a mixed methods study of violence on rural and urban EMS responders in Sweden, rates of verbal and physical violence in the last twelve months were 67 and 78 percent, respectively, showing similar rates to U.S. violence exposures. 46 In this same study, an additional 35 percent reported being victimized at least every three months. 46
Verbal abuse, physical assaults, and intimidation were the most frequently reported types of violence.22,23,25–27,49 Verbal violence was repeatedly described as the most prevalent form of occupational violence that EMS responders reported.22,23,25,26,44,46,48,50,51 The range of verbal violence ever experienced by EMS responders is estimated to be between 21 and 88 percent.23,25,28,46 The range of physical violence ever experienced by EMS responders is estimated between 23 and 90 percent.2,52 Sources of physical violence varied. The most frequent source of physical violence was “struck by” attempts, followed by “punching, slapping, or scratching,” “spitting,” and “biting.”22,26,39,44,53 The least frequent types of physical violence experienced by EMS personnel were “stabbing or stabbing attempts” and “shooting or shooting attempts.” 44 Minor injuries from these actions of violence include minor bruises and abrasions, whereas more serious injuries included contusions, hematomas, sprains and strains, eye injuries, facial injuries, bites, lacerations, dislocations, and fractures.27,47,53
Psychosocial Impact (Stress)
While we found robust evidence on the expected physical outcomes of violence against EMS responders, equally concerning information was discovered about the psychosocial impact of experiencing violence in this work. Some research found violence to be the leading cause of stress, 26 and stress found to be the most frequent injury reported by EMS survey respondents. 38 Violence exposure also has been associated with increased levels of stress, fear, and anxiety in EMS responders. 41 Oftentimes, stress is a result of exposure to traumatic incidents in the field. A systematic review of occupational risk factors in EMS found that between 82 and 100 percent of responders reported experiencing a traumatic event. 54 Numerous studies place prevalence rates of posttraumatic stress disorder in EMS responders to be greater than 20 percent.54–60
Stress has been categorized not only by exposure to traumatic incidents but also by exposure to the monotonous operational characteristics in EMS such as paperwork, lack of administrative support, low wages, long hours, irregular shifts, and cynical societal attitudes toward public safety officers.61,62 Attitudes about job performance, job stress, and lack of job satisfaction have been found to impact employee retention rates.63,64 Cumulative stress associated with the monotonous duties or low acuity calls and experiences with violence has led to EMS responders feeling decreased empathy toward their patients and desensitized from their job as a whole.6,11,65 Chronic organizational stressors in combination with cumulative exposure to critical incident stress, such as violence, can increase the risk for negative psychological outcomes like posttraumatic stress disorder. 54
Chronic organizational stress and cumulative critical incident stress from repeated traumatic exposures can also lead to organizational outcomes such as burnout. Burnout, defined as a “syndrome of emotional exhaustion and cynicism,” 66 is one of many organizational outcomes that may arise as a result of violence experienced by EMS responders. The question of whether or not violence would eventually lead to burnout was first raised by the industry in the early 1990s, 62 yet there is little known about the issue, and studies of burnout in EMS have been described as lacking.60,67,68 Despite this, burnout has been identified as a potential factor associated with decreased levels of quality patient care.65,69 Furthermore, mixed methods studies conducted in Sweden and the United States found that violent encounters alter the patient–provider relationship.11,46 Similar to findings in EDs,69,70 a 1998 study found that 7 percent of survey respondents within one urban fire department considered leaving EMS as a direct result of the violence they experienced on the job, and 42 percent stated that violence had an overall effect on their attitudes about their job, 26 suggesting that despite the lack of abundant evidence, there is a concerning relationship between burnout, violence, and quality of patient care.
EMS Responder-Level Characteristics
Age
Age was found to be a significant indicator for increased risk of violence in three selected studies.22,44,53 Conversely, one study of Canadian paramedics found age to be a protective factor and described that with each incremental increase in age, medics were less likely to be exposed to verbal violence. 22 In a nationally representative sample of EMTs in the United States, responders who experienced physical violence from a patient were 1.9 years younger than those who did not experience violence in the last twelve months. 44 In Mechem et al.’s 53 study detailing intentional and unintentional assault, the average age of victims was 37.0 ± 8.2 years and 33.8 ± 8.4 years, respectively, marking no difference in age. Therefore, we find the evidence supporting age to be inconclusive.
Gender
While some studies indicated with statistical significance that men were more likely to experience violence,25,28,38,53 others found women were more at risk.22,39 Not until Gormley et al. 44 and Oliver and Levine 45 utilized longitudinal cohort designs was this risk factor studied under more rigorous conditions. They found that among nationally registered EMTs, women had an increased risk for physical violence, 44 while men had an increased risk for verbal violence.44,45 Other research found the female gender to be a predictor only for cases of sexual assault and sexual harassment, 23 while another study found women at significant risk with regard to sexual assault, sexual harassment, and verbal violence. 29 In a review of three fatality databases, women were found to be the majority of EMS assault-related fatalities. 13 We found conflicting evidence of gender as a risk factor for EMS responders.
Years of experience
Some research shows that work experience is not a significant risk factor for encountering violence.22,47 Gormley et al. 44 found that personnel who had experienced violent patient encounters had more than double the median years of experience in a longitudinal cohort study of nationally registered EMTs. Likewise, Oliver and Levine 45 found that EMTs or their partners with more than ten years of work experience were more likely to experience violence in the form of being punched, slapped, or scratched compared to less experienced EMTs. These findings present inconclusive evidence supporting years of experience as a risk factor for EMS responders.
Occupational role
In Philadelphia, one study analyzed all injuries reported between January 1996 and December 1998. Of 1,100 injury reports related to violent incidents, 93.2 percent of documented assaults occurred during patient care activities, suggesting that EMS calls pose more risk compared to fire calls. 53 All other selected research yielded results showing provider level to be significantly associated with increased risk of violent interactions. Robust evidence points to paramedics being at increased risk for violence compared to firefighters.11,44,53 Responders who spent more time providing direct patient care were at increased risk for violence. 29 In one fire department, the odds of paramedics being assaulted compared to their firefighter counterparts were fourteen-fold higher. 11 Thus, these findings present robust evidence of occupational role as a strong characteristic associated with WPV.
Characteristics of Perpetrators of Violence
The literature identifies several patient characteristics associated with violent events including age, gender, mental status, substance abuse, and underlying health condition. No data exist describing which of these characteristics is the most frequent. We describe what is known from the extant literature included in this review.
Patient
A large body of evidence points to patients as the most common perpetrator of violence.5,13,22,25,26,28,34,38,42,44,46,47,50 It is worthwhile to consider the environment associated with providing prehospital care, as violent behaviors may be exacerbated by the confined space of an ambulance. Another consideration to note is the limited translation and transferability of policies, procedures, and practices that provide important institutional mechanisms to protect the safety and health of workers in the “bricks and mortar” fixed environment to that of the mobile EMS environment. These findings strongly suggest the patient as the primary contributor of violence against EMS providers.
Patient’s family, friend, or bystanders
Patients are not the only perpetrators of violence. Violence is also initiated by nonpatients such as family members of patients and bystanders.25,26,44,46,47,50,53,71 In a prospective, observational case-series study of 297 EMS runs conducted over 737 hours of observation, the violent person was not the patient in as many as one third (five out of sixteen) of violent calls. 25 A separate observational case-series found “others” to be the cause of violence in 10.3 percent (19 out of 184) of violent calls. 28 Studies were uniform in their findings that in addition to patient-initiated violence, family, friends, and bystanders also frequently engage in violence against EMS.
Mental status, substance abuse, and underlying health conditions
In a study of violent patients in the ED, those who demonstrated violent behaviors were more likely to be suffering from an altered mental capacity, compared to violent patients committing violence against EMS responders. 49 In the prehospital setting, Bernaldo-de-Quiros et al. 49 found that a majority (55.2%) of violent patients had no known altered mental capacity, and fewer than half of violent perpetrators had a psychiatric disorder or were under the influence of drugs and alcohol. Conversely, a prospective case-series study found that a suspected psychiatric disorder was significantly associated with violence against EMS responders. 28 Further, industry perspectives were uniform that three of the major patient characteristics associated with violence are intoxication, drugs, and altered mental status.16,72 Several academic studies support this claim.22,25,39,46,47 Additional research suggests that any medical condition that causes an altered mental status or consciousness, such as trauma and diabetes, may lead to patients committing violent acts.16,21,22,39,47,53,72–74 For instance, insulin-dependent diabetics experiencing hypoglycemic episodes were the cause of 9 percent of violent incidents in a retrospective review of ambulance call reports over a six-month study period. 21 In the larger healthcare context, altered mental status associated with dementia, delirium, and substance intoxication were the most common characteristics of violence perpetrators against healthcare workers. 75–80 These studies provide strong support that the patient’s medical status is a potential indicator for violent behavior.
Weapon possession
In studies measuring weapon possession, weapons were present on scene in less than 12 percent of violence-related patient cases.21,25,26 Although these studies suggest a relatively low incidence of weapons possessed by violent or combative patients, other research shows that many EMS responders may not be equipped or prepared to deal with the issue. As many as 42 percent of study participants comprised of EMS responders from the Boston and Los Angeles metropolitan areas indicated that they did not regularly search their patient for weapons, yet 62 percent had found a weapon on a patient in the course of their careers. 48 Another study showed that as many as 79 percent of respondents reported having “ever seen or found” a weapon on a patient. 27 More years of experience and those trained at the paramedic level were significantly associated with finding weapons on patients. 49 Likewise, EMS responders who had received weapons-specific training were more likely to report weapons found. 49 These studies suggest the need for more robust research to understand the role of a patient’s possession of a weapons.
Violent call type
Violent call type, a call that comes into dispatch as violence-related, is an understudied characteristic of the occupation that may be predictive of exposures to violence. One study found that while only 5 percent of calls (297 EMS runs over 737 hours of observation) involved a violent situation directed at EMS responders, an additional 14 percent of calls were flagged as locations where violence was mentioned to have occurred prior to the arrival of EMS responders (i.e., “postviolent” runs). 25 The 14 percent indicates a potentially hostile environment for responders upon arrival. Consequently, Mock et al. 25 suggest that 5 to 20 percent of sampled EMS calls in the urban EMS system were related to either physical or verbal violence. However, dispatch codes intended to alert responders to potentially violent scenes were not used in almost 40 percent of violent calls. 25 An analysis of responder narratives from the near-miss and injury events reported to the National Fire Fighter Near-Miss Reporting System revealed that violence may not be anticipated by responders in many cases, as violence can often erupt instantaneously. 42 Evidence supporting violent call type is inconclusive and future studies should continue to evaluate this variable in relation to WPV experienced in EMS.
Other factors
Other potential contributing factors for violent patient behaviors include dissatisfaction with response time 49 ; lack of understanding of treatment and care needs 49 ; feelings of helplessness, frustration, and anger in the face of an emergency 47 ; wishes to refuse transport 25 ; culture clash 47 ; and communication or language inadequacies.47,49 Similar factors have been indicated in the larger healthcare context. 81 Unlike other fields which have found a history of violence to be a precursor to committing interpersonal violence,82,83 the relationship between history of violence and resulting violent acts against healthcare workers has not yet been found. 84 Additional research on factors that contribute to and presage violent patient behaviors in healthcare and EMS is needed.
Reporting/Underreporting
One of the limitations that is frequently mentioned in both academic and industrial publications is the perception that violence is inherent to the profession and reporting violent incidents implies an inability to provide patient care and perform job duties competently.27 Such attitudes might lead to significant underreporting of violence in the field. 26 A study of 1,500 medical providers in New Mexico found that 56 percent of EMS survey respondents stated that violence is “just a part of the job.” 85 And although a large percentage believe violence is a part of the job, 40 percent believed that if no one was injured during the incident then there was no need to report. 85 Reasons for not reporting violent encounters include the fear of punitive actions such as being fired. 85 Other studies show higher frequencies, with as many as 71 percent believing that violence is a part of their job, and 84 percent believing that their personal safety was at risk as a direct result of violence. 26 In a Canadian study, 62 percent of participants stated that no actions were taken by most paramedics in response to the violent events, 61 percent did not report the violence to a superior or authority, and 81 percent did not formally document the occurrence in the patient care report narratives. 22 Regarding proper documentation of violent encounters, one study found that only 31 percent of all violent encounters were properly mentioned in the paramedic narrative. 25 This indicates that while the rates of violence from the literature are concerning, there is reason to believe that violence is vastly underreported and ill-documented in EMS. Therefore, any retrospective reviews of ambulance calls or paramedic narratives are likely to be missing the true prevalence of violence experienced by responders. 25 These research studies provide strong evidence that the issue of WPV in EMS is vastly underreported.
Industry Best Practices, Policies, and Procedures
To date, there exist no evidence-based interventions in the academic literature that prepare EMS responders for violence. Therefore, EMS has relied heavily on industrial publications to disseminate best practices, policies, and procedures. Industrial literature primarily highlights the use of prevention strategies to keep EMS providers from entering a potentially violent situation, such as scene safety.86–96 If scene safety precautions indicate potential violence, or if there is a known history of violence for that patient or location, current recommendations largely suggest requesting police backup; however, it is also cautioned that police do not guarantee responder safety and are not always available to respond to EMS requests for backup.86–89,91,97–101 While dispatch is integral to EMS operations, patient information received by EMS from dispatch is often unclear, incorrect, or incomplete, thus contributing to EMS responders feeling unsupported and placed unnecessarily in dangerous situations. 11 The industrial literature recognizes these fractures within the EMS system and heavily emphasizes the need to build and maintain supportive relationships between EMS and other organizational entities such as police and dispatch86–89,91,97–100,102 and is supported in academia as well.71,103,104
The industrial literature also emphasized the need for significant improvements to the quantity and quality of trainings provided to EMS responders, inclusive of de-escalation trainings to confer professional command and control in the event of unexpectedly violent persons.97,105,106 The industrial literature is particularly helpful in identifying specific call types and situations most likely to be associated with violence, such as alcohol or drug use, gang violence, homicides, domestic violence, mental health and psychiatric calls, suspected suicides and suicidal ideation, active shootings, bombings, terrorist events, and other events that pose threats of mass casualties.16,102,107,108 It is a lack of training that leads individuals to use excessive force or “pick the wrong tool to solve the problem” in many of these scenarios.97,109
Discussions regarding self-defense have become highly controversial, due to some attempts or requests by EMS organizations or EMS responders to arm personnel with weapons such as guns, tasers, mace, and pepper spray as additional forms of protection.11,91 The industrial literature provides warning that protective measures designed to arm EMS responders should be considered only as a last resort, and others argue whether their implementation is needed at all.91,100,110 No standards or evaluations on effectiveness exist for departments considering this protective measure. Furthermore, it has been posited in the academic literature that protocols to increase the safety of communities, in addition to training to provide confidence and competency in the face of violence, might supplant the need for EMS personnel to carry weapons for personal protection. 27 While providing body armor is less controversial than providing armament to EMS responders, it remains heavily debated.87,100,111
Intervention and Policy Opportunities
Currently, violence prevention training that exists consists of generic programs that are not tailored to the prehospital patient care provider and unique EMS mobile environment. 112 Available trainings also tend to focus primarily on self-defense techniques rather than prevention. 112 Infantino 34 suggests the following considerations for an EMS violence intervention program: environmental considerations, self-assessment, prevention, verbal intervention (calming/defusing techniques), escape and release procedures, control and restraint procedures, staff anxiety decompression, and postincident follow-up. Additional considerations include increasing (1) communication skills with patients and/or relatives and bystanders, (2) the ability to identify high-risk situations, (3) the ability to effectively implement safety measures, (4) support for mental health, and (5) the availability of resources to professionals who have suffered from WPV. 51
In 1998, the United States Department of Transportation developed a new paramedic-training curriculum that included expanded topics of abuse, assault, and violence. The curriculum is noted to have included learning objectives concerning how to handle victims, diffuse violent situations, and ensure personal safety. 113 However, since authority over EMS initiatives is held by state jurisdictions, individual states can choose not to adopt certain training interventions or curriculums.71,113 There have been calls for development of protocols at the national level in response to violent incidents through initiatives such as the National Fallen Firefighters Foundation Firefighter Life Safety Initiative 12, which states the need for development and implementation of practices and policies to reduce the likelihood that EMS responders will encounter violence, to standardize response protocols, and to increase survivability for fire and EMS personnel when violent situations are unavoidable.92,114 Other entities that advocate for safety and health in EMS include labor organizations, such as the International Association of Fire Fighters, the International Association of EMTs and Paramedics, EMS Workers United/American Federation of State, County and Municipal Employees, and many others. These labor organizations are dedicated and committed advocates that lobby for increased safety and health protections for the EMS work force. In fact, in 2016, the United States Fire Administration subcontracted a study on violence against EMS responders to the International Association of Fire Fighters because of their strong advocacy and commitment to improving responder safety. 115 Labor unions in healthcare and related industries have long called for increased research and protective regulations on the issue. 84 Within fire departments, local labor unions are successful champions of safety and health and advocates of policy change, resource installation, and safe reporting environments. 116 At individual workplaces, union advocacy can bring about changes in policies and in the availability of protective equipment even between contract negotiations. Unions can have an impact on underreporting by advocating for the elimination of disincentives to reporting. All of these can be strengthened further by getting them written into collective bargaining agreements. The ability to build solutions from the bottom up workplace by workplace and demonstrate their feasibility produces immediate gains for the represented workplaces and can ultimately lead to the adoption of similar solutions as best practices, guidelines, and/or enforceable standards. No other kind of advocacy organization can have that kind of direct impact on individual workplaces.
Other active initiatives to address WPV in EMS include the Center for Leadership, Innovation, and Research in EMS (CLIR), which has launched the EMS Voluntary Event Notification Tool to assist in data collection of exposures to violence. 117 In 2010, CLIR partnered with the National EMS Management Association and the End Violence Against Paramedics initiative to include violence in their data collection processes, which can be used to inform the development of interventions. 118 One such intervention that exists is Defensive Tactics 4 Escaping Mitigating Surviving Violence. 119 While this intervention has been developed specifically for the EMS industry, it has not been evaluated to determine its reach and effectiveness. In response to the growing issue of violence, some departments have taken it upon themselves to investigate causes of violence and respond proactively.
While NIOSH has not developed an EMS-specific intervention, they have recommended several best practices for fire departments as a way to prevent and mitigate violence at both the organizational and employee level. 120 In 2004, NIOSH released recommendations on methods to best mitigate violence following the investigation into the death of a female firefighter who responded to the scene of a civilian shooting. 121 While the recommendations have been disseminated, no formal intervention program has been developed nor has a formal evaluation of the recommendations been conducted. NIOSH has also recommended that employers establish a zero-tolerance policy for all incidents of violence, train workers on recognizing and preventing WPV, investigate all reports of violence, and work with police to identify dangerous neighborhoods where special precautions need to be taken and provide that information to employees. From the employee’s standpoint, NIOSH recommends that employees should participate in violence prevention training and report all incidents of violence, no matter how minor. 122
Supplemental to NIOSH’s recommendations are the guidelines proffered by OSHA in their updated 2015 “Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers.” 75 These guidelines offer critical recommendations on effective approaches to eliminate violence in the workplace, including the essential components to an effective WPV prevention program. While the guidelines are not regulatory in nature, several states including New York and California have adopted these guidelines as policy.123,124 In fact, in 1993, Cal OSHA (the California state OSHA program) was the first entity to establish WPV guidelines, which was a result of the persistent pressuring done by a multiunion task force on WPV. 84 This union-led initiative ultimately informed the creation of the federal OSHA guidelines, 84 further demonstrating the union’s fortified commitment to health and safety, especially as it relates to influencing the local, state, and federal policy arena of WPV. Components of OSHA’s guidelines that are relevant to EMS include their identified risk factors, of which eight out of ten, apply to EMS. 75 In addition, the components to an effective violence prevention program are highly adaptable to the EMS work environment and include management commitment and employee participation, worksite analysis, hazard prevention and control, safety and health training, and record-keeping and program evaluation. 75
While the EMS literature notes that the guidelines developed for violence reduction specific to ED settings do not generalize well to the EMS industry, 27 there is great utility in evaluating educational initiatives in the hospital setting for goodness of fit in the prehospital setting. Interventions such as the “Workplace Violence Prevention for Nurses” online training program have been designed and evaluated as a method to help healthcare workers recognize violence in the workplace and may be useful to consider when developing EMS-specific interventions and policy initiatives that focus on primary prevention. 125
Discussion
WPV is a concerning and complex issue facing much of the healthcare industry, including EMS. Most of our knowledge on the issue of WPV in healthcare stems from EDs and psychiatric facilities. Indeed, many research findings on WPV in EMS are not unique and have been indicated in the larger healthcare context.81,84,126–131 However, research on the issue of WPV in EMS is still lacking, with little to offer in terms of prevention programs and policy. This literature review sought to compile what is currently known so that effective interventions and policies aimed at increasing the safety and health of emergency responders can develop.
To date, two systematic reviews have been conducted regarding violence against EMS responders.132,133 Each employed a systematic process: Pourshaikhian’s review included eighteen articles in their analysis, and Maguire’s included twenty-five articles. There are six total articles between the two literature reviews absent from our analysis. This is likely due to their scope and case inclusion criteria, in which Maguire included literature pertaining to military ambulance officers and air ambulances, and Pourshaikhian included articles published in English and Persian. We believe these differences to be insignificant due to the immense return of our literature search which led to a total of sixty-eight academic publications included in our analysis.
Moreover, our case inclusion criteria and review of the literature led to the inclusion of thirty-six industrial publications. The industrial literature provided the unique perspective of how the industry perceives the issue of violence, its ideas for training opportunities, and its attempts at interventions to best mitigate and reduce violence exposures. It is our opinion that academic researchers should source from these publications to the same degree they do the peer-reviewed literature. In particular, the industrial literature gives unique credence to practices already utilized in the fire and rescue service that could be further buttressed by the academic community in terms of intervention development and evaluation. For example, the industrial literature expounds on a variety of best practices used during the multiple phases of emergency response. Fields such as public health and organizational science could bring their considerable prevention acumen to this process. With an approximately 20 percent increase in call volume each year, it is imperative to begin thinking about interventions that focus not on the individual EMS responders by making them do more with less 11 but by shifting the onus of safety and health from the individual to the organization. By utilizing the counsel of the industrial literature, multiple training, policy, and environmental interventions could be developed to better protect the safety, health, and well-being of EMS responders from stress and violence. Such interventions have the potential to impact organizational and safety outcomes in this profession. 134
The academic literature focused on incidence and prevalence estimates. Research conducted through 2016 used cross-sectional designs with small convenience samples. As such, there are very few studies that employed strong scientific design. Other limitations identified include (1) the lack of a standardized definition of violence, (2) variation in study design, (3) depth of data available, (4) insufficient studies using nationally representative data, and (5) wide-ranging estimates. There is a great need for rigorously designed, nationally representative examinations of occupational exposures in order to better understand the temporal associations of violence, cumulative occupational stressors, and the outcomes of physical and psychosocial injuries that are occurring as a result of exposures to violence. Based on current studies, it is not possible to discuss causality among violence risk factors and reported outcomes. Noticeably absent from both industry and academic literature is intervention evaluation to assess the effectiveness of best practices, training programs, and policies mentioned in both literatures. Research in the larger healthcare sector also shows that studies are typically designed to quantify the problem, with little mention or focus on methods designed to prevent violence from occurring. 81 Issues reminiscent of our findings—especially WPV being poorly defined and underreported—complicate the design of evidence-based policy.81,84,128,129
In the United States, there have been no widely applicable, efficacious interventions to address WPV in healthcare. 81 Due to the high prevalence of occupational violence compared to other industries, healthcare is often the subject of WPV research and initiatives, yet EMS is often absent from these national efforts. While numerous states have enacted felony assault statutes that include first responders, these policies are tertiary in nature and do not offer much in terms of prevention. 135 In order to prevent WPV in EMS from happening, we must focus our policy efforts on primary prevention strategies. The first step in doing so is to have national support advocating for the inclusion of EMS in forums and policy discussions on WPV. We can look to OSHA’s Guidelines for Preventing Workplace Violence to develop strong and effective prevention programs and policies.75 In 2017, the Department of Labor and OSHA issued a “Request For Information” on the prevention of WPV in healthcare and social assistance (Docket No. OSHA-2016–0014). 136 In response, coauthors of this manuscript submitted an executive summary on WPV in EMS advocating for the inclusion of emergency medical responders in OSHA’s development of standards and policies to prevent violence in the workplace. 137 This level of inclusion is important to ensure that EMS providers are not left out of crucial legislation and prevention opportunities. However, policy at the national-level is not the only way to affect positive changes in the safety and health of EMS providers. By focusing policy efforts at the local-level, we may be able to affect more immediate change by creating EMS-specific solutions to violence. The SAVER Systems-level Checklist, part of a current research study exploring the efficacy of policy and training to prevent WPV in fire-based EMS, holds promise for primary prevention.138,139 It was created as a checklist for the system (department and union leadership teams), as opposed to an individual-level checklist that would put more burden on already overstretched EMS responders. The checklist contains training, policy, and environmental modification interventions organized by phases of EMS response. It has “pause points” which are feedback mechanisms for the individual responder. The pause points redistribute traditional hierarchical power by giving the individual EMS responder the authority to pause an EMS encounter based on perceived risks to their safety. The checklist creates organizational support that can positively impact burnout, morale, and work engagement while decreasing the number of assaults and injuries experienced by EMS personnel. While too early in its implementation to have evaluation results, the SAVER Systems-level Checklist is already inspiring policy and program development within fire departments such as the creation of standard operating procedures for supporting members assaulted on duty (Philadelphia)140,141 and the creation of resilience programs to reduce occupational burnout (Dallas). 142
We undertook this comprehensive literature review to more deeply understand the incidence and prevalence of violence against EMS responders, but in so doing, we uncovered additional stressors that emanate from the organizational culture. Such stressors may be duration of shift for busy EMS responders, the skill mix of personnel on EMS runs, the ability to rest and recover after traumatic or compelling events, and the busyness of responders visiting the community. Also important to consider is the sometimes sensitive nature of this research topic. Sharing sensitive and traumatic details associated with violent exposures can impact an individual’s willingness to report. Academic and industry publications equally posit the notion that violence is an expectation of the work, and the high frequency of violence occurring in the profession has caused it to be internalized as “part of the job.”26,27,85,98 This perception is validated by the almost nonexistent reporting by EMS responders Thus, it is imperative for leadership in EMS to support and champion consistent and mandatory reporting and follow-up with responders who have experienced violence during the course of their duty. The sharp rise in community demand is an increasing stressor for departments and agencies providing EMS. For example, the top five busiest medic units in the United States run between seventeen and twenty-four calls per day. 143 In a twenty-four-hour period, this gives little or no time to “eat, sleep, or pee.” These added occupational stressors can increase the level of job dissatisfaction that responders experience. 6 Exposures to WPV, especially cumulative exposures, in concert with these added stressors, may result in mental health outcomes such as anxiety, depression, and posttraumatic stress disorder. Poor work environments and deficient social networks, in combination with anxiety, depression, and posttraumatic stress disorder, have been known to lead to suicidal ideation and, in some cases, suicide completion. 59 Future research should systematically measure and understand the degree to which the stress of increasing community demand intersects with the stress of insufficient resources in fire and rescue organizations. Finally, the psychological impact of experiencing violence on the job can change the way EMS responders approach the occupation and has implications for quality of patient care and patient outcomes. 11
Conclusion
We found that from 1978 to 1992, the issue of WPV in EMS is only discussed within industrial trade journals which addressed the risks of the job long before the first peer-reviewed research was published in 1993. While prevalence estimates fluctuate slightly from 1993 to 2016, authors are discussing the same issues forty years later, highlighting the fact that little progress has been made to protect EMS responders against violence in the field. Today, literature on the issue of violence has been bolstered by intensified efforts of EMS organizations and officials to decrease the prevalence of violence in the industry, yet violence remains poorly defined and assessed. This systematic review warrants further rigorous scientific inquiry to better identify risk factors for violence, circumstances surrounding violence, and methods to best mitigate violence so that resources can be properly allocated to protect the health, safety, and well-being of EMS responders. As public health researchers, we are compelled to advocate for increased research and development of interventions and policies to reduce and prevent the occurrence of WPV in EMS. In order to ensure that EMS remains a vital community resource, we must protect the safety and well-being of responders against all harm, starting with the harm caused by the very people they are seeking to help. We have identified the following content areas for future inquiry for EMS-focused research and practice related to OSHA’s Guidelines for Preventing Workplace Violence. These content areas include (1) standardizing the definition of violence used in EMS research; (2) creating reliable and consistent epidemiological surveillance on violence against EMS responders through data system development and recurring surveys; (3) securing sufficient funding for scientific research on EMS violence that uses rigorous scientific designs; (4) identifying and quantifying risk factors of providers, patients, and communities inclusive of stress, trauma, and mental health outcomes; (5) understanding the roles of coping, resilience, and social support in EMS; (6) developing practices, procedures, and policies that support EMS responders; (7) training all responders to recognize and respond to violence on the job; (8) conducting evaluations of existing trainings to measure their effectiveness; (9) developing new trainings as needed and evaluating their effectiveness; (10) conducting economic analyses on the psychosocial impact of violence in EMS; and (11) assessing the impact of violence on patient care and quality.
Supplemental Material
NEW893388 Supplemental Material1 - Supplemental material for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders
Supplemental material, NEW893388 Supplemental Material1 for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders by Regan M. Murray, Andrea L. Davis, Lauren J. Shepler, Lori Moore-Merrell, William J. Troup, Joseph A. Allen and Jennifer A. Taylor in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Supplemental Material
NEW893388 Supplemental Material2 - Supplemental material for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders
Supplemental material, NEW893388 Supplemental Material2 for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders by Regan M. Murray, Andrea L. Davis, Lauren J. Shepler, Lori Moore-Merrell, William J. Troup, Joseph A. Allen and Jennifer A. Taylor in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Supplemental Material
NEW893388 Supplemental Material3 - Supplemental material for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders
Supplemental material, NEW893388 Supplemental Material3 for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders by Regan M. Murray, Andrea L. Davis, Lauren J. Shepler, Lori Moore-Merrell, William J. Troup, Joseph A. Allen and Jennifer A. Taylor in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Supplemental Material
NEW893388 Supplemental Material4 - Supplemental material for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders
Supplemental material, NEW893388 Supplemental Material4 for A Systematic Review of Workplace Violence Against Emergency Medical Services Responders by Regan M. Murray, Andrea L. Davis, Lauren J. Shepler, Lori Moore-Merrell, William J. Troup, Joseph A. Allen and Jennifer A. Taylor in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Footnotes
Acknowledgments
The authors would like to thank the following colleagues for their contributions to this manuscript: Kathleen Turner, the Liaison Librarian for the Dornsife School of Public Health at Drexel University, and previous affiliates of the Center for Firefighter Injury Research and Safety Trends: Shannon Widman, Cydney McGuire, Shachi Mistry, and Cecelia Harrison. The authors also thank Dr. Darius Sivin for his contribution in deepening the explanation of how labor unions are uniquely positioned to advocate on the issue of workplace violence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a subcontract from the International Association of Fire Fighters under their contract with the Department of Homeland Security/Federal Emergency Management Agency/United States Fire Administration contract number: HSFE20-15-Q-0053 and the Federal Emergency Management Agency (FEMA) FY 2016 Assistance to Firefighters Grant Program, Fire Prevention and Safety Grants (Research & Development) Grant number: EMW-2016-FP-00277.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.