
Abstract
Introduction
The aim of the study was to evaluate undergraduate medical students’ knowledge and self-confidence to perform abscess incision after virtual reality-simulation or video lecture. Pre and post-knowledge assessment was conducted.
Materials and Methods
This was a multicentre randomised controlled trial from October 2021 to January 2022. The study was carried out at two universities providing medical education. Undergraduate medical students were randomized into either fully immersive head mounted display virtual reality-simulation (VR) or video lecture. Pre- and post-learning surveys probed self-confidence and student’s own assessment of competence. Participants were third-, fourth- and fifth-year medical students from the University of Eastern Finland and the University of Helsinki. All students were sent an email informing them of the opportunity to participate in this voluntary study. All willing students were included in the study.
Results
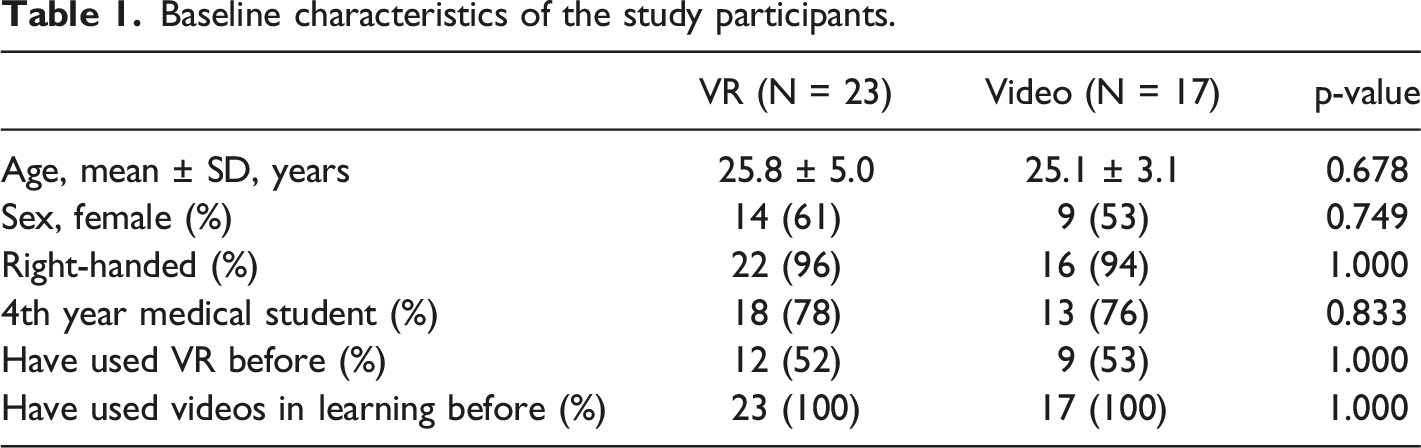
42 medical students participated in the study. Most were fourth year medical students, 52% of the participants had previously used VR in some context and the mean age of participants was around 25 years. Both methods increased knowledge and self-confidence equally. In VR subgroup, those with technical support available experienced greater learning than those without.
Conclusions
Interestingly, in the present study, both VR and video lecture increased knowledge and professional self-confidence equally.
Introduction
Virtual reality (VR) can potentially improve efficiency of medical education (Barteit et al., 2021). This technology offers a patient-safe way to train healthcare students and professionals, especially in surgical procedures. Virtual reality is not yet in routine use, despite the first medical education VR publications dating back to the 1990s (Satava, 1993; Noar, 1991). Currently, immersive VR includes vision, hearing, and haptics sensations, thus giving a real-life impression. Compared with more traditional learning /teaching methods, VR learning was effective with immersive VR compared to video (Lohre et al., 2020). Students experienced more joy of learning in VR, which can also explain the results (Lohre et al., 2020).
The differences between technologies in medical education have been studied limitely. According to Raleigh, different teaching methods should be compared (Raleigh et al., 2018). Integrating virtual reality to medical education also requires further research.
The aim of this study was to compare medical students’ knowledge and self-confidence after fully immersive head mounted display (HMD) VR-simulation compared to traditional video lectures. There is a paucity in the data regarding HMD VR in medical education (Barteit et al., 2021), (Lohre et al., 2020), Ojala et al., 2022, Barré et al., 2019, Tursø-Finnich et al., 2022. In this study, we focused on fully immersive HMD VR. To the best of our knowledge, there are no studies comparing the learning outcomes between HMD based VR-simulation and video teaching in undergraduate medical student education. We hypothesised based on previous publications, that highly interactive and fully immersive VR-simulation provides better learning outcomes than video lecture (Miller, 1990).
Materials and Methods
This study was a multicentre randomised controlled trial. The participants of this study consisted of third-, fourth- and fifth-year medical students from the University of Eastern Finland and the University of Helsinki. All students were sent an e-mail informing them of the opportunity to participate in this voluntary study. In the e-mail, students were told that the research topic was related to surgery and teaching technology. All willing students were included in the study; however, individuals with epilepsy were advised not to participate. The study was conducted from October 2021 to January 2022.
All students gave informed consent. The topic of the study was not given to the students in advance. They booked 60-minute slots in the booking calendar for the study. Upon arrival at the research site, the students took one envelope from the research box, which randomised the participants into either the VR-simulation group or the video group. After this, the students read the instructions for participating in the study from the research computer. At this point, students were informed that the study was about the incision of subcutaneous abscess in the knee area. The students completed the pre-questionnaire form, after which they completed the exercise one time (VR-simulation or Video), followed by the post-activity questionnaire.
The questionnaire was based on our previous study, where we explored the teacher's impact in VR-education (Raleigh et al., 2018). We developed a questionnaire measuring student’s self-confidence and a survey on the student’s own assessment of competence; these tasks were rated on a scale from 0 to 10 (0 = worst, 10 = best). In these queries, each numerical answer option included a sentence describing competence or self-confidence in the answer option. The students made assessments before and after the exercise; the same form also had multiple-choice task (in what order what is done, score 0-5) to map the knowledge before and after the exercise. So, the 3 categories of outcomes that was looked were; a) self-confidence in performing, b) self-assessment of competence and c) Test of knowledge of steps on incision and drainage.
The VR-simulation software was manufactured by VR4Healthcare Ltd. Oculus Rift S was used as the VR glasses. The software was in English, which is not the native language of Finns. The VR group had an initial introduction to the use of the device; it took 20 minutes to play the introduction in the virtual world. In the VR-simulation of the abcess incision, the students wore the VR glasses on their face, after which they were able to move freely in the virtual world. The students also heard the space sounds and received habitable feedback when they touched anything. In the VR-simulation, steps can be taken in the order participants want, but there is also the possibility of doing incorrect things. The software did not advise during the VR-simulation.
The video lecture of the abcess incision was created by the authors in Finnish and lasted for about two minutes. After the exercise, the students completed a questionnaire. Some of the students had technical support available. Technical support meant that the student knew the person to ask for technical assistance, if necessary, who was in the same room or apartment.
The collected data included whether the student learned something new, whether VR adds value to medical education, or whether VR was useful when incising an abscess. These tasks were rated on a scale from 0 to 10 (0 = worst, 10 = best). Statistical analysis was performed using IBM SPSS Statistics 25.0 software. We used Fisher’s exact test to compare nominal data and the Mann-Whitney U-test for nonparametric data. Mann-Whitney U-test was also used when comparing nonparametric data changes between the two groups. Results were considered statistically significant at p-values < 0.05.
According to the 488/1999 Finnish Medical Act (amendment 295/2004, 794/2010), research related to the development of teaching quality does not require permission from the research ethics committee.
Results
Baseline characteristics of the study participants.
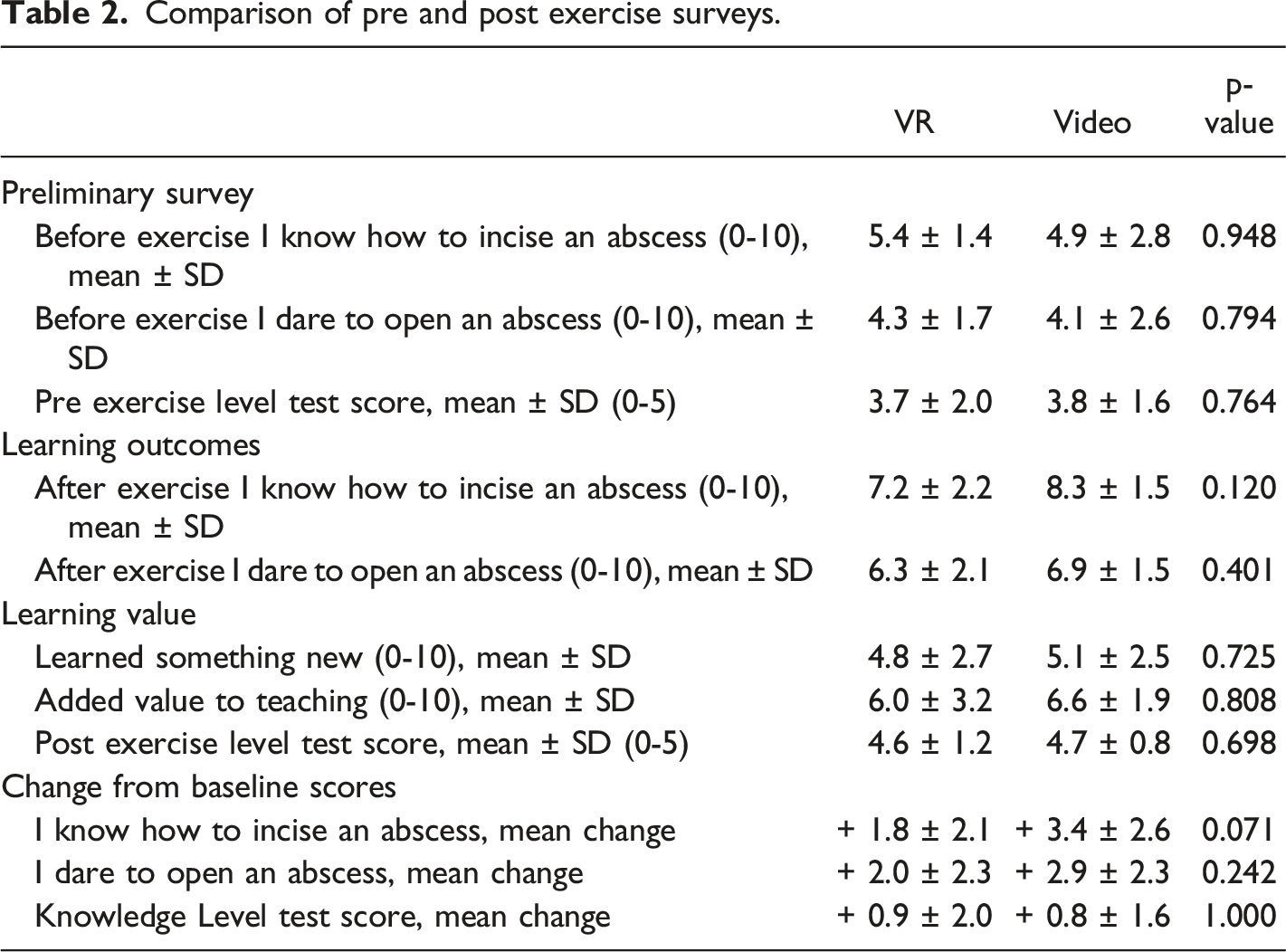
Comparison of pre and post exercise surveys.
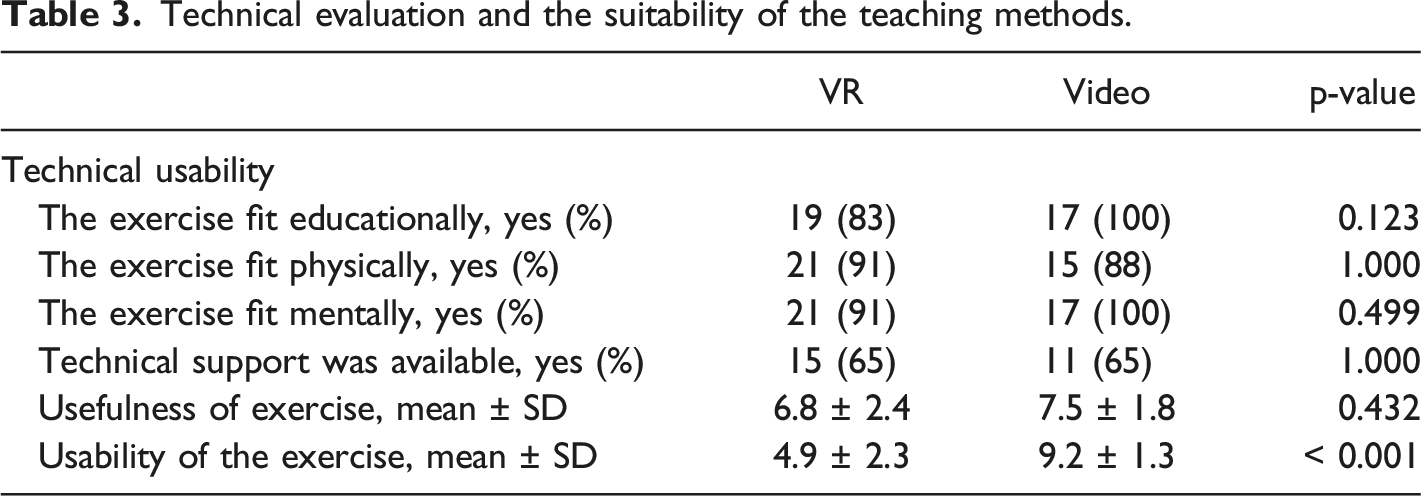
Technical evaluation and the suitability of the teaching methods.
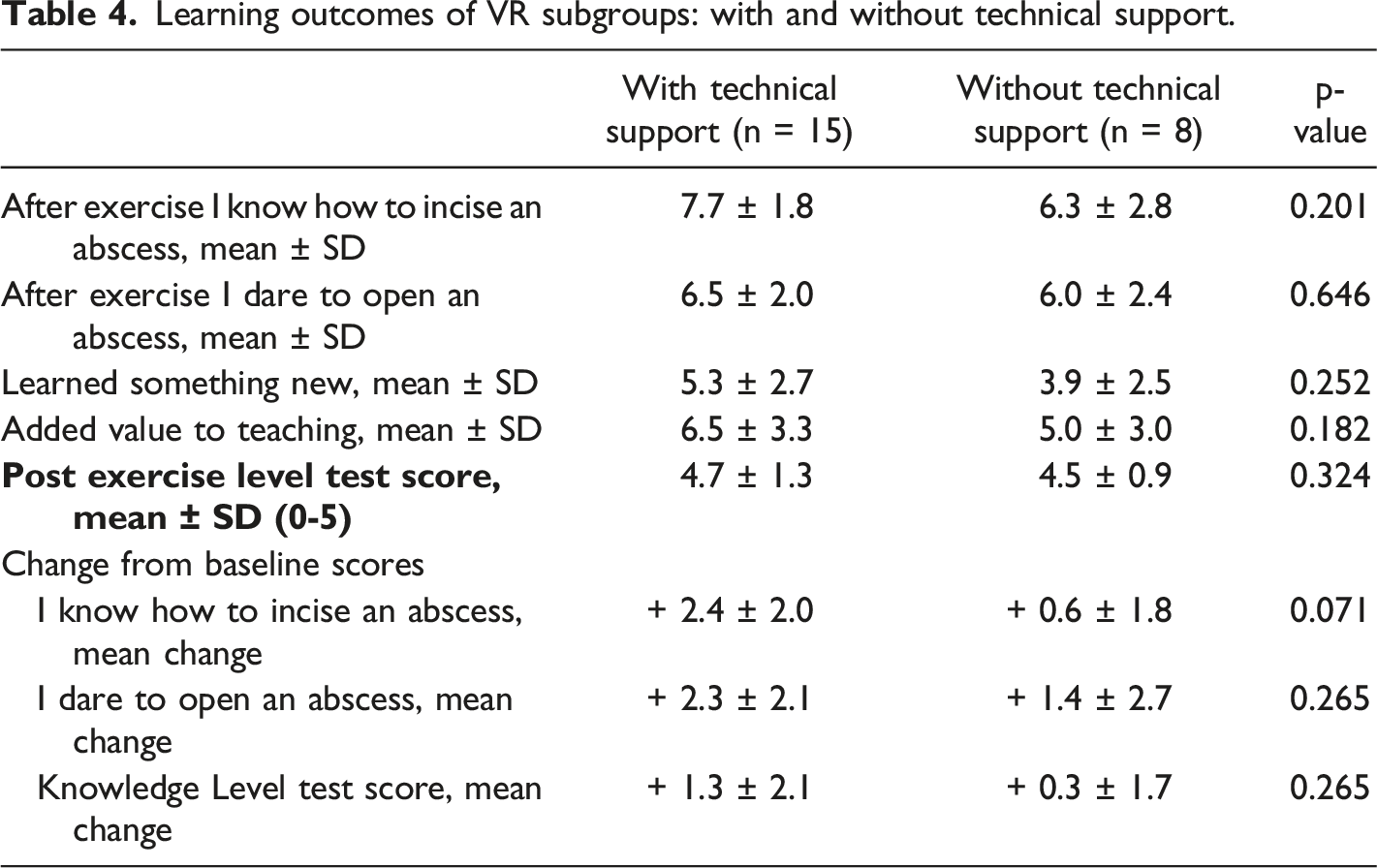
Learning outcomes of VR subgroups: with and without technical support.
Discussion
Herein, we compared video lecture to fully immersive HMD VR-simulations for abscess incision. We did not compare or evaluate improvements of surgical skills. We found that both methods increased undergraduate medical students’ knowledge and self-confidence in performance equally, contrary to previous publications (Kyaw et al., 2019; Yoganathan et al., 2018). Also according to Miller´s pyramid, more active VR-simulation should have been a more effective teaching method (Miller, 1990). The difference between the outcomes found in our study may be due to the lack of technical support in the VR group. Only a half of the participants had used VR before, this affected our results. It should be noted that when undergraduate student’s learning is evaluated using new technology, the student’s initial knowledge level may be too low, and thus the technology does not add value. Inexperienced students do not benefit from exercises that are too complex (Dankbaar et al., 2016). Our pre-level test showed that students had sufficient knowledge of the subject. Virtual reality education is not suitable for everyone, due to the side effects of dizziness/nausea that were recorded also in this current study (Taylor et al., 2022; Birrenbach et al., 2021).
The increase in knowledge in the VR group was slightly better, but only when technical support was available. Students requested also longer time for VR simulation, mainly to master the VR technological competence. The need for teacher or technical support is evident when VR technology is new, as only about half of the participants in both groups had previously used VR in either entertainment or teaching; this has also been stated in previous publications (Ojala et al., 2022). The teacher’s role is not merely a technical support, but with verbal guidance it is possible to provide additional information. The usability of the video was considered better, and students felt that the video lecture added more knowledge. Video teaching is routine for current medical students, and this was reflected in our results. The short duration of the video may lead to biased results, especially when participants only perform the exercise once. A short teaching session, such as the video in this study, can have a good immediate learning result.However, if the knowledge test were repeated a month later, the VR group may perform better since they have already practiced the procedure in VR. Based on the recent study, integrating virtual reality into medical education may require a technical advisor.
The haptics' weakness can affect the VR learning experience, especially in surgical procedures. The most important lesson in simple surgical HMD VR exercises is to learn the procedure. Simulators, on the other hand, primarily seek realistic haptics.
An abscess incision is one of the most common surgical procedures performed by a general practitioner. Pedagogically, training of abscess incision has been difficult, and traditionally, phantoms or cadavers have been used (Fitch et al., 2008). The drawback of phantoms is that the abscess drainage can only be done once or at least the cover must be replaced. Video is a good method for teaching abscess drainage (Fitch et al., 2008). However, the procedure itself cannot be done hands-on, which would allow for the information to be better retained. The advantages of VR include repetition of the procedure, so the learner knows how to act correctly in different situations.
Limitations and Suggestions for Further Future Research
The weakness of this study was the low number of participants. The initial email did not specify the topic, leading some students to skip the exercise. No validated survey was suitable for the study, which forced us to create our own. The limitation of the study is also the fact that practical learning (technical skills) learning in the VR had to be measured by the student’s experienced learning and knowledge, which does not correspond to the learning of technical skills. This can therefore affect the results of the study. It is possible that the students would have done the procedure in the real life before the study, but that was not asked in the survey. Objective structured assessment of technical skill (OSATS) did not fit because no surgical/technical skills were measured. In the future, a survey should be created that would be suitable for evaluating learning in simulations. Another drawback was the weak tactile feedback of technology, i.e., haptics. Madan showed that VR training without haptic feedback is not realistic; however, they did not have fully immersive HMD VR (Madan et al., 2005), the degree of fidelity or realism does not alter the effectiveness in training (Grober et al., 2004). The strengths of this study include multicentre RCT, which measured both pre and post scores and assessed teaching in a multidimensional way: self-confidence, knowledge, and usability.
Conclusions
In the present study, both VR and video education increased knowledge and professional self-confidence in abscess incision training. However, our hypothesis that VR is better as an active learning method was not confirmed. In the future, research into learning using new technologies should consider that the level of knowledge or skills has been measured or assessed in advance. In this way, studies are comparable when sources of error due to new technology and the student´s low knowledge level can be distinguished.
Supplemental Material
Supplemental Material - Virtual Reality simulation and Video Lecture are Equally Effective in Abscess Incision Training: A Multicentre Randomised Controlled Trial
Supplemental Material for Virtual Reality simulation and Video Lecture are Equally Effective in Abscess Incision Training: A Multicentre Randomised Controlled Trial by Henrik Nuutinen, Ville Bister, Virve Koljonen in Simulation & Gaming
Footnotes
Authors Contribution
All authors participated in the design and analysis of the study, all authors also wrote and revised the manuscript. All authors approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Henrik Nuutinen, is shareholder of VR4Healthcare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.