
Abstract
Objectives
This study aimed to evaluate the effectiveness of the digital and gamified WellWe intervention on parental self-efficacy for healthy behaviours and mindfulness in parenting at the comprehensive health checks of 4-year-old children.
Methods
Two-arm cluster, randomised, controlled trial with a 4-month follow-up.The data were collected from parents of 4-year-old children. Cluster randomisation was done at the municipality level. Fifteen child health clinics within 4 municipalities located in Southwest Finland were randomly allocated to either an intervention (WellWe intervention) or a control group (usual care). The outcome measures included the Parental Self-Efficacy for Healthy Behaviours (PDAP) and Mindfulness in Parenting (MIPQ) questionnaires. Data were collected at baseline, after the intervention and at the 4-month follow-up.
Results
Initially a total of 110 parents (50 in the intervention and 60 in the control group) participated in the study. At the end of the study, there were 33 parents involved, with 12 in the intervention group and 21 in the control group. Parental self-efficacy and mindfulness in parenting showed no statistically significant difference between the groups or within the groups at the different time points.
Conclusions
The results of the study showed no difference between the intervention and the usual care. The commitment of the subjects was lower than expected. The intervention could be improved by placing a greater focus on engaging and motivating both families and public health nurses (PHNs). Therefore, when refining the intervention further, it's important to involve the target group more actively in the design of both content and delivery.
Background
The basis for health and healthy habits starts to form in early childhood (ref). The creation of basic physical and psychological abilities occurs at that time. (Pillas et al., 2014.) Self-efficacy is a person’s experience of their own ability to cope with certain situations that affect their life (Bandura 1994). High parental self-efficacy is associated with factors promoting the child’s well-being and several positive outcomes in parenthood (Albanese et al., 2019; Wittkowski et al., 2016). Mindful parenting may promote child-parent interaction and decrease stress in parenting (Burgdorf et al., 2019; McCaffrey et al., 2017). Public health nurses (PHNs) working in child health clinics have a central role and contact with almost all families in Finnish healthcare. Over 99% of Finnish families with children use public child health clinic services. (Finnish Institute for Health and Welfare, 2022.) Hence, PHNs have an excellent opportunity to inform and guide families and implement interventions in matters related to improving children’s well-being and health.
The family-centred approach has been shown to be beneficial for families, and it could also advantage healthcare providers (Park et al., 2018). Family-centered care recognizes the family as the central unit. (Coyne et al., 2016). Using a family-centred approach in childhood obesity interventions can lead to better outcomes in the family and promote family satisfaction with healthcare services (Simione et al., 2020). Interventions for families with pre-school-aged children can be an effective method to address child overweight and obesity. Intervention should be versatile and include dietary, physical activity and/or behavioural components (ref). Mindfulness interventions for parents can reduce parental stress if that is the primary aim of the intervention (Burgdorf et al., 2019). However, there is still a gap in evidence-based studies within these fields (Burgdorf et al., 2019; Colquitt et al., 2016).
Response to the COVID-19 pandemic created a need for remote digital interventions in healthcare (Badawy & Radovic, 2020; Tullio et al., 2020). The pandemic increased the demand for digital interventions to promote the health of families with children (Gurwitch et al., 2020; Mörelius et al., 2021; Tang et al., 2021). When incorporating digital methods into interventions, it's crucial to consider relevant aspects that are already known. For instance, when providing a digital intervention for families, factors like choosing online video over phone calls and enhancing user acceptability through technical support and information should be taken into account. (Tang et al., 2021). Digital interventions can also potentially increase the health knowledge of parents of young children (Mörelius et al., 2021).
In addition, game-based interventions can be effective in decreasing BMI levels in overweight and obese school-aged children (Ameryoun et al., 2018). Health-promoting game-based interventions that utilise gamification can guide children to eat healthily and increase the use of vegetables and fruits (Chow et al., 2020). Within health and healthy habit-promoting applications, the most commonly used gamification elements include rewards, narrative, feedback, levels or progress, scoring, challenge, personalisation and customisation. These elements can motivate and engage participants in the implementation of the intervention. (Cheng et al., 2019; Chow et al., 2020; Kubota et al., 2022.)
Methods
This cluster randomised trial aimed to evaluate the effectiveness of the digital and gamified WellWe intervention on parental self-efficacy for healthy behaviours and mindfulness in parenting at the comprehensive health checks of 4-year-old children. The study was designed as a two-arm cluster, randomised, controlled trial with a 4-month follow-up. A detailed research study protocol was previously published (Pakarinen et al., 2018).
Settings
The study was carried out in 15 child health clinics in four municipalities in Southwest Finland. Eight of the clinics were allocated to an intervention group and seven to a control group.
In Finland, child health clinics are public services for families with children preschool age (1 week to 6 years). Families can attend 15 regular health checks before their child reaches school age. These include three comprehensive health checks, which examine the health and well-being of the child, the parents and the family as a whole, and an overall assessment. (Government Decree, 338/2011.)
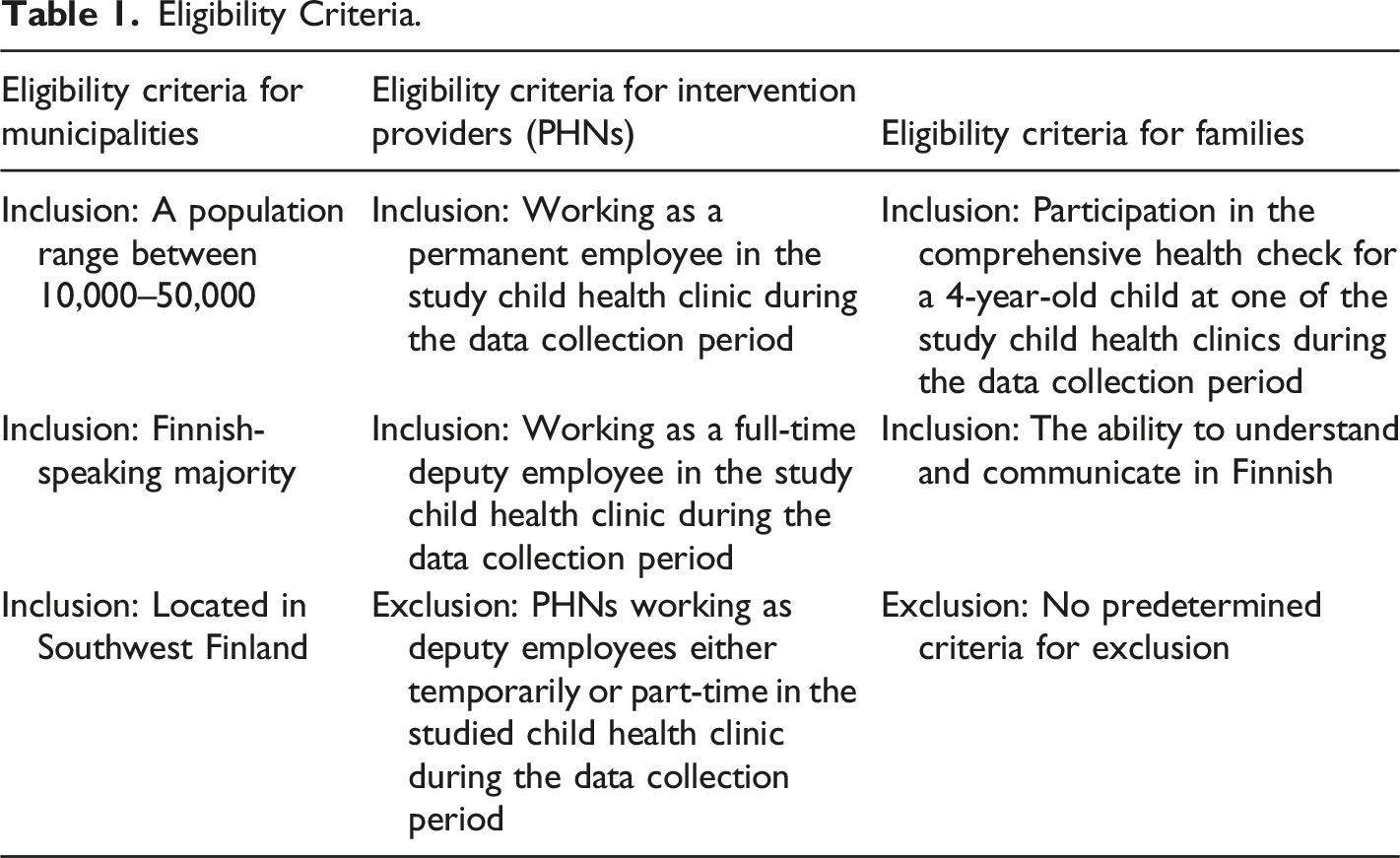
Participants and Eligibility Criteria
Eligibility Criteria.
Intervention
In this study, the WellWe intervention followed the mediating variable model (Baranowski et al., 1997). The detailed description of the mediating variable model and the development process of the WellWe intervention (Pakarinen et al., 2018) and usability testing of the intervention (Pakarinen et al., 2017a) have been reported in previous publications.
The intervention included two parts: a health discussion with a PHN and the use of the WellWe application, which was developed by a multidisciplinary team (Pakarinen et al., 2018). First, families used the WellWe application for approximately 30-40 minutes at home before entering the child health clinic for a comprehensive health check. Second, the WellWe application was used during the health check by the PHNs to facilitate health guidance and conversation with the family. The conversation lasted approximately 15–20 min, depending on the family and their situation.
The PHNs in the intervention group (n=9) received a two-hour training session on the study protocol. They also received a practical manual for WellWe intervention and full access to the WellWe application. The PHNs in the control group (n=13) were also trained in the study protocol from their point of view. They provided health guidance in the comprehensive health checks following the usual procedures, which meant that they used the pre-information questionnaires filled in by the families as the basis for the health conversation.
The WellWe application is an Internet-based application with four sections: physical activity, nutrition, family resources and daily rhythm (Figure 1). Because it is web-based, the app can be easily accessed from personal computers and mobile devices. It has two different user interfaces, a family view and a more statistical professional view. (Pakarinen et al., 2018.) The user interface of the WellWe application including the four sections.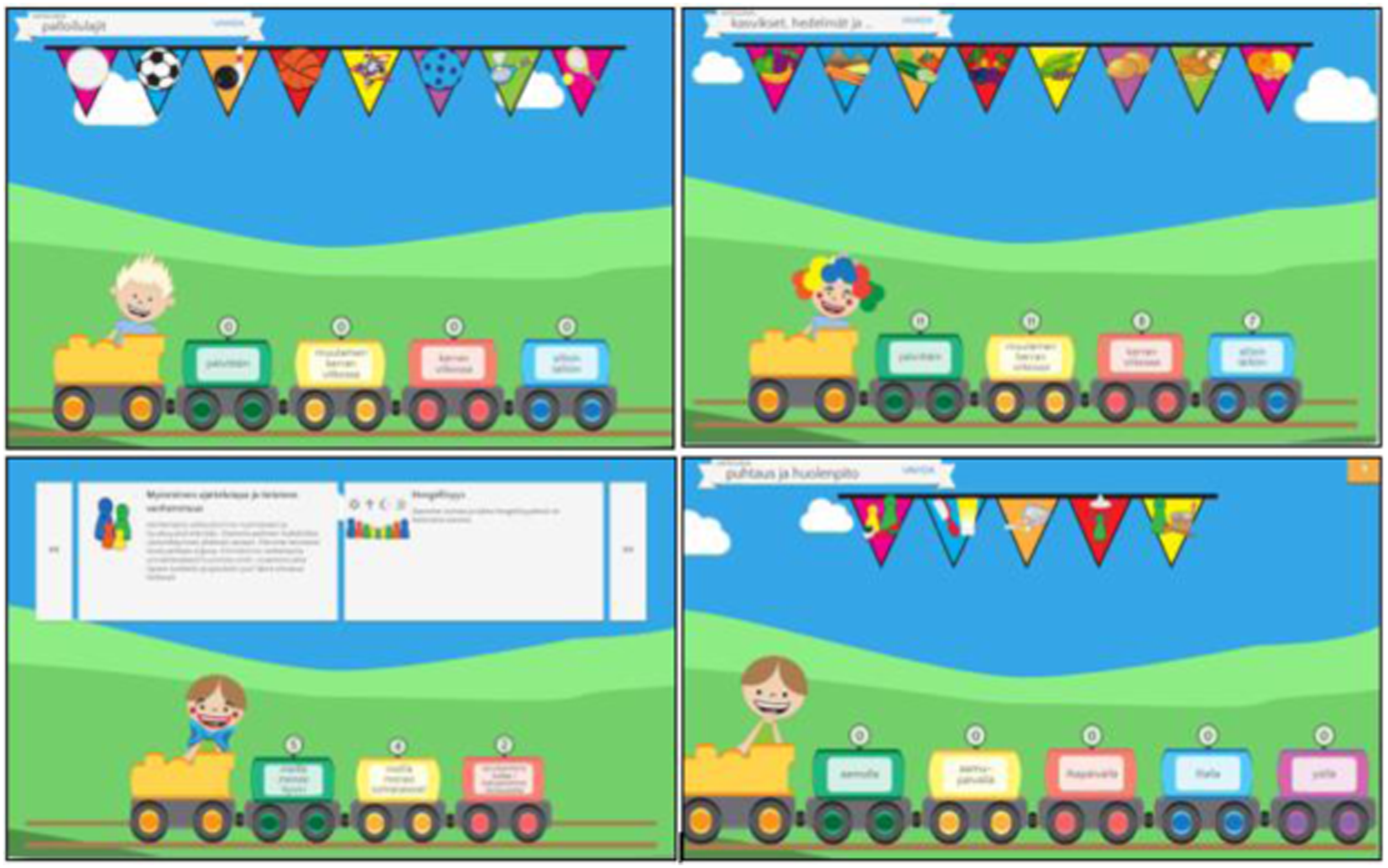
The first section is the physical activity section in which the families filled in a three-item questionnaire on their physical activity level. In this section, the families were to evaluate their weekly physical activity levels according to the directions that they were given. The second section is the nutrition section, in which the family was instructed to evaluate their weekly nutrition habits, such as the different foods and drinks that the family consumed during the week. The third section is the family resources section, which was based on mindfulness in parenting. In this section, the family was instructed to evaluate their resources, which are displayed as twelve resource cards. These cards show topics like parenting and child care, relationships, mental health and coping, positive thinking and mindful parenting. The fourth section is the daily rhythm section, considering that daily rhythm mirrors the complexity of everyday family life. Family members continually shape this multidimensional process through their individual and collective actions and emotions within the context of time and space. During the health check visit, the PHNs could discuss and provide feedback to the family about their physical activity and nutritional habits, daily rhythm, and situation regarding family resources. A detailed description of the WellWe application can be found in a previous publication (Pakarinen et al., 2018).
Randomisation and Recruitment
The randomisation of families into the intervention and control groups was based on cluster sampling (Figure 2) at the municipality level. The randomisation, with a 1:1 allocation, was done in two phases: first, municipalities were randomly selected from the list of eligible municipalities; after that, the chosen municipalities (n=4) were randomly allocated to the intervention (n=2) and control groups (n=2). PHNs were recruited by the directors of the child health clinics and were provided with materials on the research. Information sessions were held for all eligible PHNs and were conducted by the same researchers. Following the study briefings, informed consent was obtained from all eligible PHNs. Participants’ Flow Diagram.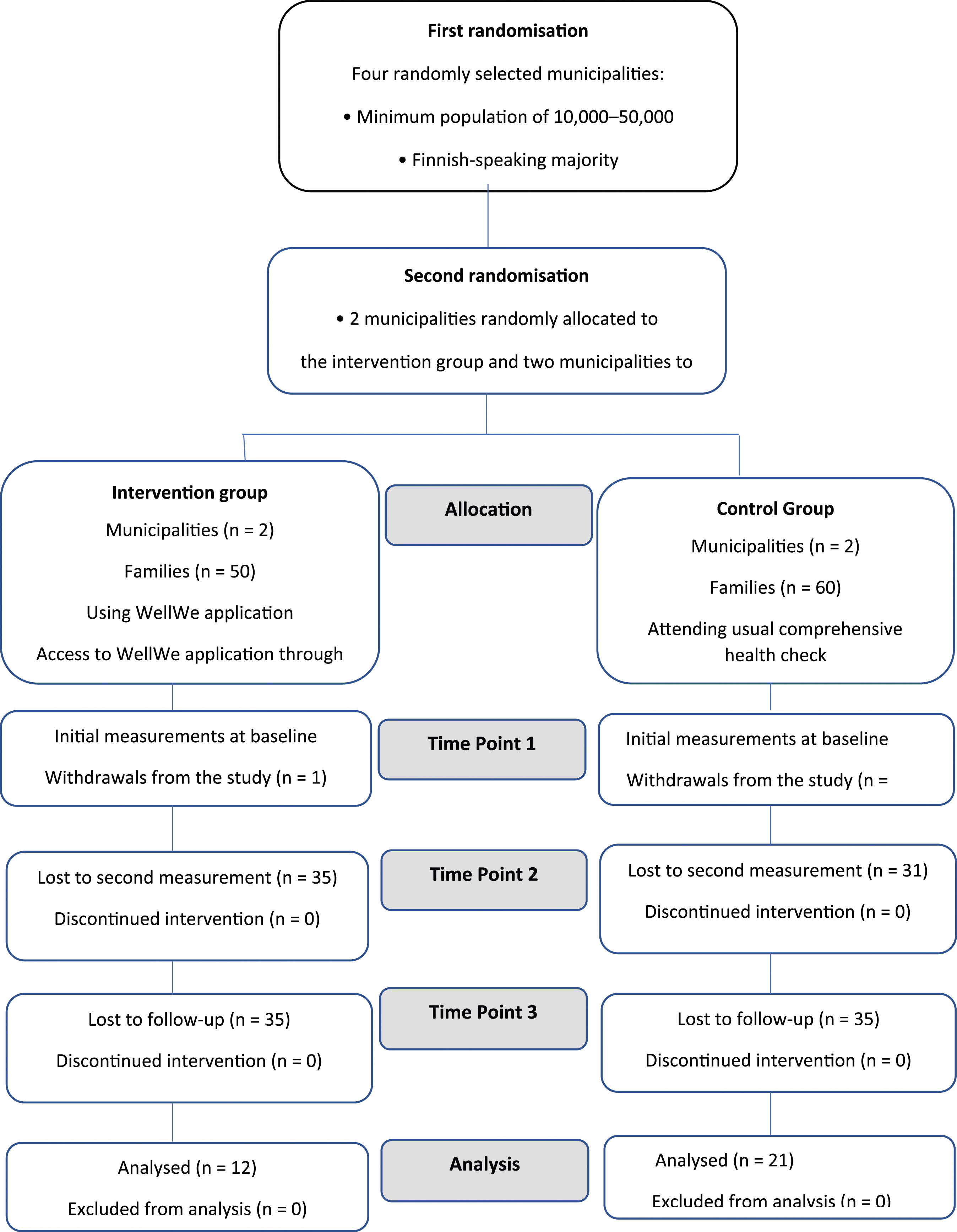
The families of the intervention group received the background information and questionnaires as electronic questionnaires, which they accessed via a link in the research bulletin. After answering the electronic forms, the families received a link to the WellWe application. The families of the control group were sent the informed consent document and the questionnaires in paper form, which they returned to the nurse in a sealed envelope at the clinic visit.
Data Collection and Outcomes
The primary outcomes were parental self-efficacy for healthy dietary and physical activity. The secondary outcomes were mindfulness in parenting at the comprehensive health check. Measurements were made before the intervention, immediately after the intervention, and four months after the intervention. The first measurement was performed 1-2 weeks before the child health clinic visit, between September 2017 and March 2018. Data were collected from participants using validated instruments. Parental self-efficacy for health behaviours was measured using the 21-item version of the Parental Self-Efficacy for Healthy Dietary and Physical Activity Behaviours in Preschoolers Scale (PDAP) (Bohman et al., 2016). Mindfulness in parenting was measured using the 28-item version of the Mindfulness in Parenting Questionnaire (MIPQ) (McCaffrey et al., 2017).
Data Analysis
The data were statistically analysed using R version 4.0.2. Descriptive statistics were calculated to describe the two groups. The similarity of the groups’ background variables was tested using the Mann-Whitney U-test for continuous variables and Fisher’s Exact test for categorical variables. Linear mixed models were used to test the difference in groups for the change between the time points. Within-group change was tested using paired t-tests for the MIPQ and the linear mixed model for the PDAP.
Validity and Reliability
The study design, procedures and reporting followed the CONSORT statement recommendations on randomised controlled trials (Consolidated Standards of Reporting Trials of Electronic and Mobile HEalth Applications and onLine TeleHealth) (Eysenbach et al., 2011). The trial was registered with Clinical Trials Registry ID Clinicaltrials.gov: NCT03278288. All questionnaires and instruments used for data collection have been demonstrated to have psychometric adequacy. The data analysis, including all statistical analysis, was performed by a study statistician who was also blinded to the allocation.
Ethical Considerations
The study was conducted in accordance with the ethical principles conforming to the Declaration of Helsinki (2013) and the responsible conduct of research guidelines (Finnish National Board on Research Integrity TENK, 2012). The autonomy, dignity and integrity of the study subjects were respected. The study was approved by the Ethics Committee of the University of Turku (64/2016) before the study was carried out.
Permission was obtained from the chief nurses of the different municipalities in May 2017. Information about the study and its implementation was provided in writing and verbally before obtaining informed consent forms from the PHNs and families. Data were stored and analysed using codes without any identifying information for participants. This prevented the identification of the child health clinic, the municipality or the individual participant.
Results
Background Information of the Participants
Background information and sense of coherence values of participants in the study.
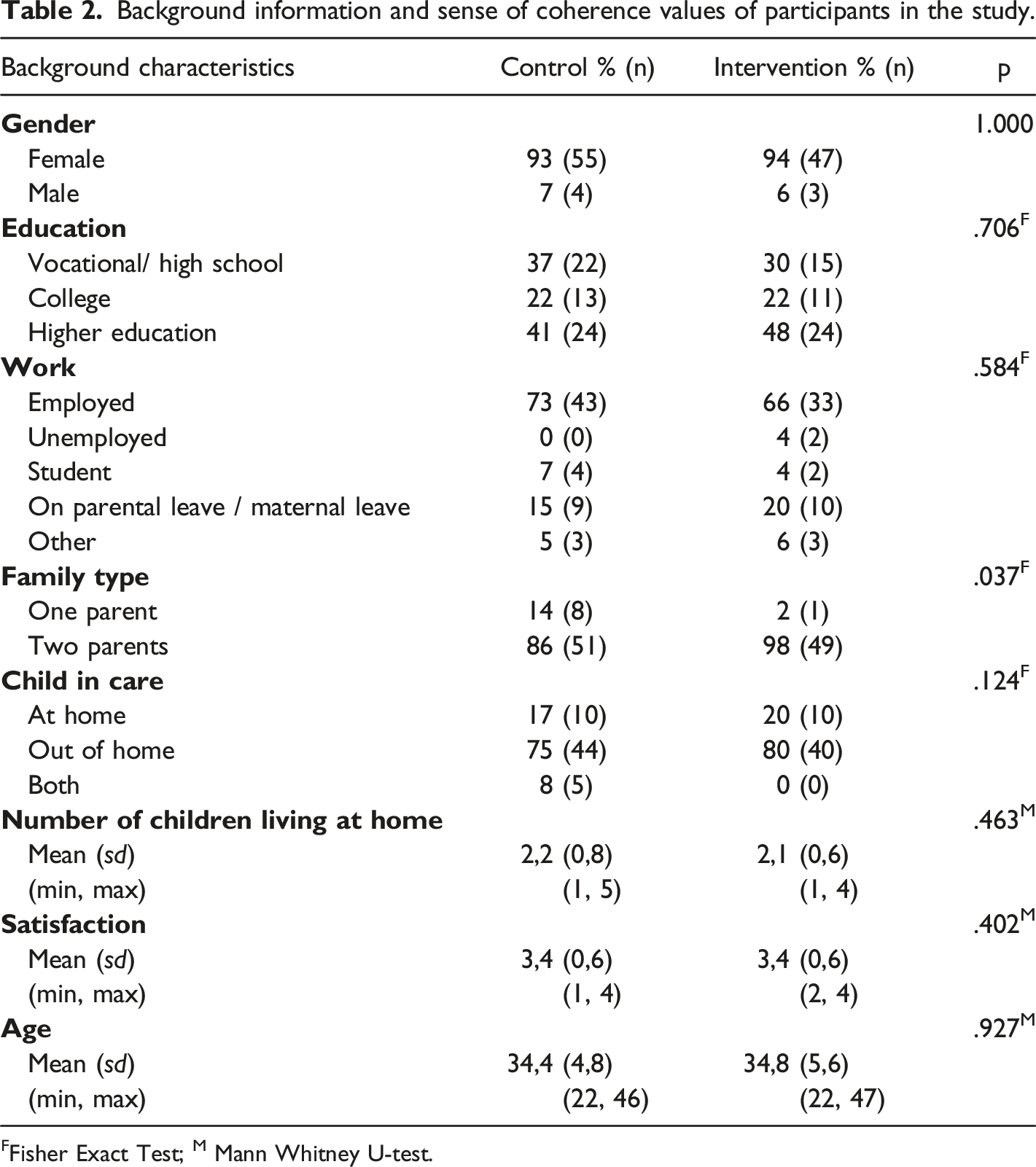
FFisher Exact Test; M Mann Whitney U-test.
Parental Self-Efficacy and Mindfulness in Parenting
At the first measurement point of the study, one participant in the intervention and two participants in the control group did not respond to the MIPQ questionnaire, and one participant in the control group did not respond to the PDAP questionnaire. At measurement point two, 31 participants from the control group and 35 participants from the intervention group did not answer the questionnaires and withdrew from the study for different reasons. After completing the intervention, ten more participants withdrew from the study. At the four-month measurements, the final number of participants was 33 (30%).
Participants’ self-efficacy scores for healthy dietary and physical activity behaviours before and after the intervention.
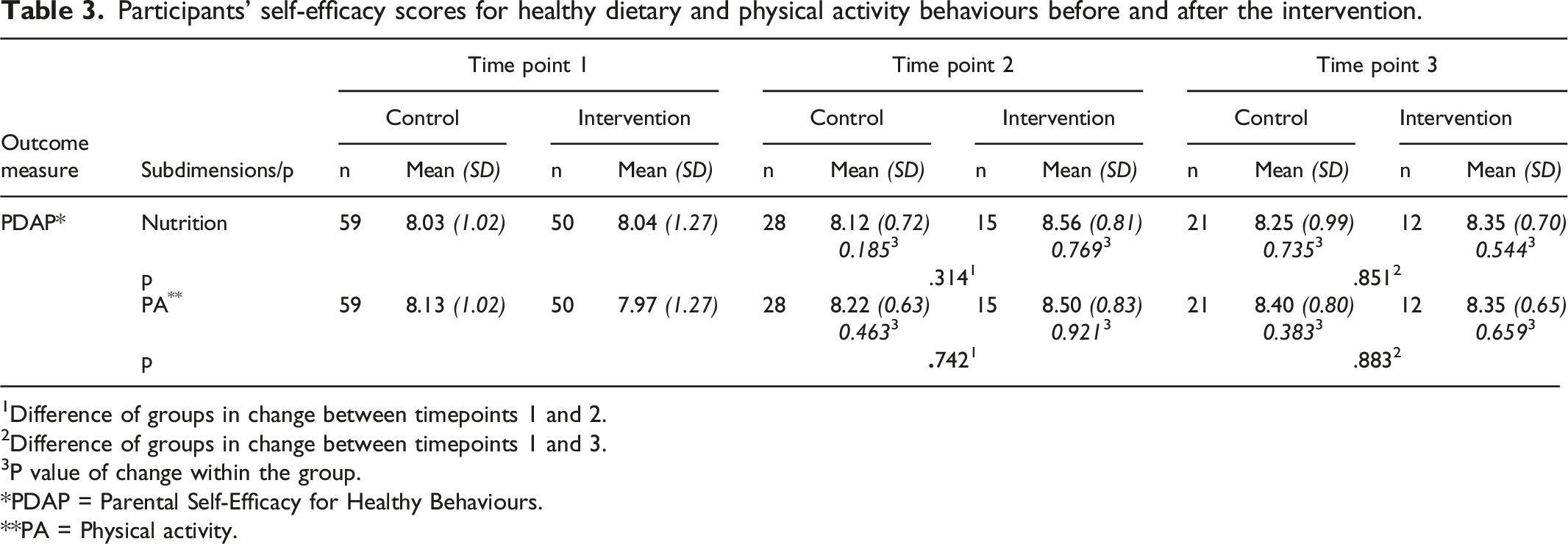
1Difference of groups in change between timepoints 1 and 2.
2Difference of groups in change between timepoints 1 and 3.
3P value of change within the group.
PDAP = Parental Self-Efficacy for Healthy Behaviours.
PA = Physical activity.
Participants’ mindfulness in parenting scores before and after the intervention.
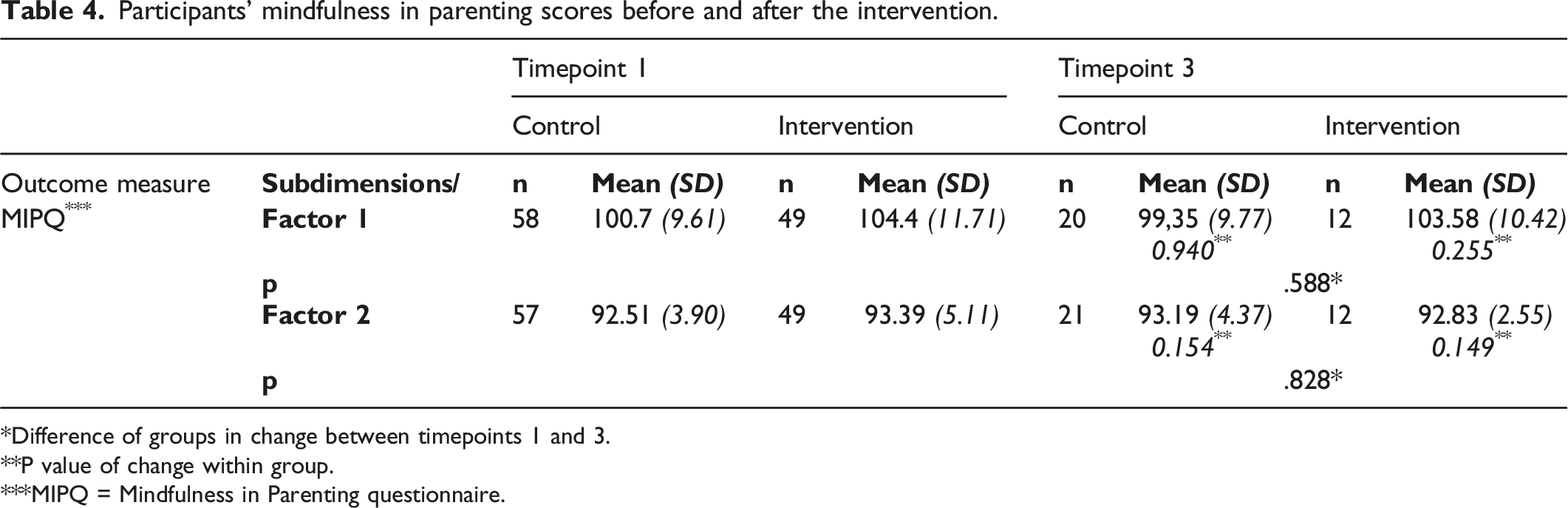
Difference of groups in change between timepoints 1 and 3.
P value of change within group.
MIPQ = Mindfulness in Parenting questionnaire.
Discussion
The WellWe intervention aimed to support the participation of families with young children in promoting their own health via a family-centred approach, including healthy behaviours and mindful parenting. To our knowledge, mindfulness and self-efficacy were being used as mediators based on a family-centred approach for the first time. The two hypotheses determined at the beginning of the study were tested; unfortunately, the desired positive results were not achieved. Statistical analysis showed no meaningful difference between the intervention and the usual care. Withdrawal of the participants could also affect the results. A total of 70% of the participants had withdrawn by the last time point of the study. Also, there was a statistical difference in family structure between the groups in regard to one-parent or two parent households, which may introduce a confounding variable, as family type can influence various aspects of parenting, self-efficacy and mindfulness.
Employing digital methods in health interventions within family contexts is a relatively recent development, and the available evidence presents conflicting findings. The effective use of digital methods that target both parents and children in particular is not well known (Breitenstein et al., 2014; Pakarinen et al., 2018). Although this study did not find positive results, the results provide valuable information and clues for future researchers planning to use digital methods in parent and child health services. At its best, using a family-centred approach as a basis of family interventions can increase the quality of healthcare and positively affect families and healthcare providers (Park et al., 2018). The Finnish Government programme also includes the goal of family-centredness and aims to increase it in family services, working life and support for families with children (Finnish Government, 2022).
This study did not find a significant difference between the intervention and control groups concerning parental self-efficacy for healthy behaviours and mindfulness in parenting at the comprehensive health check. However, an interesting observation was made at time point 2, where the intervention group exhibited a higher post-intervention score compared to the control group. This result is similar to what was found in a previous mHealth obesity prevention study among preschool-aged children, which also reported no significant group differences but noted a considerably higher post-intervention result in the intervention group (Nyström et al., 2017). This study showed that if researchers want to increase self-efficacy and mindfulness for parents, longer planning of the intervention process can make it easier to achieve positive results. For some users and different contexts, it may require more time to ensure commitment to the digital interventions (Michie et al., 2013; Michie et al., 2017). One opportunity could be to concentrate more on improving and supporting parents’ self-efficacy and mindful parenting perspective via participant education and the development of the application.
To ensure commitment developing new interventions, it is important to consider the motivation factors for both the intervention providers and participants. According to previous studies, parents are willing to use digital tools because they find them easy to use (Breitenstein et al., 2014). However, in this study, the commitment of the subjects was worse than expected. Therefore, the intervention should be further developed, noting this aspect and focusing on encouraging families to commit to the intervention. In addition, Baumel and Faber (2018) defined the weakest point of the digital parent training program they developed as the lack of monitoring and adaptation of parents. One opportunity could be finding ways to support and increase the adaptation of parents to using digital tools. Breitenstein et al. (2017) showed that parents’ engagement, commitment, and adherence are crucial for achieving positive outcomes. They also pointed out that the evaluation of parents’ engagement in the study can be useful. In the current study, the family used the WellWe application at home before they entered the comprehensive health check at the child health clinic. However, the evaluation of parents’ engagement with the application was not assessed periodically. If parents’ engagement had been evaluated, the researcher would have had an opportunity to identify possible problems beforehand, and these could have provided insight into the course of the intervention.
From the perspective of behaviour change theories, monitoring digital parent training programmes, feedback, and adaptivity can ideally allow the program to support parents’ self-management of their behaviours and respond to areas of difficulty they may encounter during the behaviour change process (Baumel & Faber, 2018). A systematic review of digital parenting training interventions found that using reminders such as phone calls and text messages can boost parents' commitment to the program (Breitenstein et al., 2014). Additionally, WellWe intervention incorporated gamification elements, which have been shown to have positive effects, such as enhancing participants' motivation and engagement in the program (Cheng et al., 2019; Chow et al., 2020).The other notable issue was the commitment to the intervention of PHNs working in the child health clinics. Despite the PHNs being trained by the same researcher before the intervention, their workloads or other reasons could have affected the implementation of the intervention. (Coyne et al., 2016; O’Toole et al., 2019). There was no possibility to control how the PHNs implemented the health conversations with the families in the real situation. Communication during the implementation of the intervention, such as organizing meetings between the researchers and PHNs, could provide an opportunity to gather more information about PHNs attitudes towards the intervention and its fidelity. .
The WellWe application provided an opportunity to collect data from individual families to be used during the comprehensive health check, and the WellWe database allowed the collection of metadata. The data collected in the WellWe database could empower organizations to make informed decisions. It can be utilized to evaluate the effectiveness of comprehensive health checks, assess the well-being of families with children, gauge the success of care interventions, and prompt organizations to take appropriate actions related to previous issues if necessary.The WellWe app offers the advantage of enhanced data accessibility due to its digital data collection method, in contrast to the conventional paper-based approach used in usual care for assessing family well-being during comprehensive health checks. The health-related database is also valuable when organisations want to provide services centrally to those who need them most. The data could also be used for resource management purposes.
The changes in health services caused by the COVID-19 pandemic can also be considered when implementing interventions. Using the digital application within the intervention would make it easier to make health checks remotely if needed. Both families and PHNs can see the application view on their own devices, and the health discussion could be held, for example, via a video meeting or phone.
Due to the nature of the intervention, the intervention providers (PHNs) could not be blinded to the allocation. Therefore, PHNs in the intervention group knew that they were using a new kind of method in their work with families, and this information could affect, for example, their behaviour. Their opinions on the intervention may also have emerged when they were working or recruiting families. In addition, some of the PHNs in the control group could have felt disappointed when they did not have the chance to use the new method, even if they did not know what it was.
Limitations
This study has some limitations. The attrition rate was an important limitation of the current study. Only 30% of the participants who enrolled in the study were still taking part at the end of the study. The other limitation was that there were not enough participants initially, which compounded the situation when some participants withdrew from the study.The research group also faced an issue when implementing the study because an unanticipated national-level study in child health clinics started at the same time. Because of that, child health clinics were not able to participate in two studies simultaneously.
Digital interventions are entering healthcare at a rapid pace and the results of this study showed the importance of paying particular attention to the public health nurses, as their perception and skills influence the successful implementation of the intervention. Although the results of this study were not positive, the findings provide valuable information for future researchers when planning and developing digital methods in parent and child health services. This study showcased one digital platform to collect health data and in future, combining the use of AI with interventions will increase the potential to use health data also for policy-making, in order to promote family health more effectively.
Conclusion
The WellWe intervention aimed to promote family health through a family-centered approach, targeting healthy behaviors and mindful parenting. While novel in its use of mindfulness and self-efficacy as mediators within a family-centered framework, the study did not achieve the anticipated positive outcomes. Factors such as participant withdrawal (70% by the study's end) and the relative novelty of digital methods in this field contributed to these challenges. The results shed light on critical considerations for future researchers in the realm of digital interventions for family health services. Specifically, the study emphasizes the need for longer planning phases to foster positive outcomes, as well as the importance of motivation factors for both intervention providers and participants. Monitoring and adapting the program, incorporating reminders and gamification elements, and evaluating participant engagement are crucial aspects to consider.
Furthermore, the commitment of public health nurses (PHNs) in child health clinics emerged as a noteworthy issue. Addressing workload and other factors affecting intervention implementation is essential. Collaboration between researchers and PHNs during implementation may provide valuable insights into improving intervention effectiveness. Moreover, the WellWe application's ability to collect and process data offers significant potential for decision-making, reviewing health check effectiveness, assessing family well-being, and optimizing care delivery. Finally, while the WellWe intervention did not yield the desired results, it serves as a valuable source of insights for researchers aiming to develop digital interventions in family health services. In the future, integrating AI with digital interventions has the potential to enhance family health promotion.
Footnotes
Acknowledgements
We would like to express our sincerest gratitude to all the children, their parents and personnel in the child health clinics in Southwest Finland for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.