
Abstract
Guided by the principles of conversation analysis, we examined the communication practices used to negotiate levels of participation in cancer multidisciplinary team meetings and their implications for patient safety. Three cancer teams participated. Thirty-six weekly meetings were video recorded, encompassing 822 case reviews. A cross-section was transcribed using Jefferson notation. We found a low frequency of gaps between speakers (3%), high frequency of overlaps (24%), and no-gaps-no-overlaps (73%), suggesting fast turn transitions. Securing a turn to speak is challenging due to a systematic reduction in turn-taking opportunities. We contribute to group research with the development of a microlevel methodology for studying multidisciplinary teams.
Cancer multidisciplinary team meetings (MDMs or tumor boards), like other MDMs in health care, involve the coming together of a diverse group of professionals each possessing different levels of clinical expertise. Such MDMs typically include surgeons, oncologists, radiologists, histopathologists, cancer nurses, and in some cases allied health professionals. MDMs occur on a regular basis (e.g., weekly) to allow the members to regularly review cancer cases and formulate expert-informed treatment recommendations (Cancer Research UK, 2017; Department of Health, 2011; Raine et al., 2014).
The presence of the professional diversity in MDMs allows a holistic assessment of patients, which when combined with group history (i.e., transactive memory structure; Barnier et al., 2018; Poole & Hollingshead, 2005) enhances clinical decision-making and performance (Cancer Research UK, 2017; Department of Health, 2011; National Cancer Action Team, 2010). For this reason, multidisciplinary teams are regarded as the gold standard in cancer care. It has been frequently observed, however, that participation in MDM discussion is unequal, with underutilization of the available diversity in expertise, which results in suboptimal information sharing (Lamb et al., 2012, 2013; Soukup, Gandamihardja, et al., 2019). This effect has also been reported in nonclinical settings (Gardner, 2012; Valcea et al., 2019; Woolley et al., 2008) where information sharing has proved critical to team performance (Mesmer-Magnus & DeChurch, 2009). In MDMs, unequal participation is most frequently seen in nursing input, while deficiencies in information sharing and availability usually occur regarding patients’ comorbidities, their psychosocial circumstances and views on treatment options; both of which adversely affect the teams’ collective ability to formulate a recommendation (see Soukup, Gandamihardja, et al., 2019).
The reasons behind underutilization of expertise in meetings, and specifically cancer MDMs, are not fully understood (Valcea et al., 2019). Evidence points to poor communication (Woolley et al., 2008) and increased performance pressures (Gardner, 2012) as possible causes. In line with the principles of the functional perspective of group decision making, it is possible to reduce variability in performance and help teams to achieve better outcomes by using strategies that regulate group interactions (Forsyth, 2014; Kettner-Polley, 2016; Poole & Hollingshead, 2005). Building the relevant knowledge base is therefore critical for advancing small group research and, in the context of cancer MDMs, improving teamwork. This is particularly the case for settings where stakes are high and communication problems a leading cause of inadvertent patient harm (Leonard et al., 2004).
To date, the majority of literature on cancer MDMs (see Soukup, Lamb, et al., 2019) has focused on advancing the understanding of teamwork from a macrolevel perspective. The focus has been on information exchange and the input of individual disciplinary groups into the discussions of patients (or case discussions) and treatment planning. A recent systematic review on teamwork in health care (Dinh et al., 2020) has shown that studies of MDMs mainly rely on quantitative methods. This occurs at the expense of alternative methodologies, such as qualitative and mixed method approaches. Accordingly, there remains much to be explored at a microlevel; in particular, how individual professionals, or professional groups, communicate and interact, as well as the development of feasible methodologies to capture such interactions. Teams in general are considered complex adaptive systems (Ramos-Villagrasa et al., 2018) with professional meetings, such as cancer MDMs, a particularly intricate setting for studying groups (Halvorsen & Sarangi, 2015; Soukup, Lamb, et al., 2019). The lack of qualitative and hybrid methods (Dinh et al., 2020) may be partly driven by the immense time and resource investment required by existing tools and approaches for detailed microlevel observations and coding of team interactions (Jefferson, 2004; Kettner-Polley, 2016; Soukup et al., 2017). Developing feasible and valid methodologies to study team interaction and communication on microlevel is therefore needed (Keyton, 2016).
Turn Transitioning in Multidisciplinary Cancer Team Meetings
Examining the nature of turn-taking is one way of enhancing our understanding of interactional dynamics in MDMs at a microlevel. According to the turn-taking model proposed by Sacks et al. (1974), opportunities for speech exchange occur either by self-selection, current speaker selection of the next speaker, or by rules speakers orient to, to order speaker selection and turn taking. Such opportunities can shape the ongoing production of talk between members in a specific way, either by organizing talk to secure the turn to speak or delay the loss of a turn. Hence, turn-taking opportunities are valuable points of interaction, which have the potential to organise shared interaction within a group. The management of turn-taking by the chair of a meeting, for example, can be particularly useful (e.g., Modada, 2013; Svennevig, 2008).
Conversely, a reduction in turn-taking opportunities can lead to unequal participation. It has been argued that “speakers are intrinsically motivated to manipulate the internal structure of turn-constructional units” (Goodwin & Heritage, 1990, p. 22) to secure their turn to speak, or to delay arrival at a place where they risk losing it. Hence, turn transitioning between speakers can happen in one of the following three ways: overlaps, gaps, and no-gaps-no-overlaps (Heldner & Edlund, 2010; Sacks et al., 1974; Shriberg et al., 2001).
Overlap refers to speakers speaking simultaneously. A gap is a silence between turns that tends to be in the range of 0.2 to 0.6 s. No-gaps-no-overlap refers to overlap and gap-free turns, giving fluent and organized speech between speakers (Heldner & Edlund, 2010; Kurtić et al., 2013; Levinson, 2016). The placement and organization of these mechanisms of transition in a conversation can help build our understanding of how turn-taking and participation is managed. Gaps are considered the most frequent type, accounting for about 60% of turn transition in professional meetings, with overlaps occurring at a frequency of around 30%, and no-gap-no-overlap for the remainder (Heldner & Edlund, 2010; Kurtić et al., 2013; Shriberg et al., 2001).
Overlaps can take different forms depending on group dynamics and context (Adda-Decker et al., 2008; French & Local, 1983; Kurtić et al., 2013). Competitive overlaps are characterized as “wanting the floor to him/herself not when the current speaker has finished but now at this point in conversation” (French & Local, 1983, p. 30). Intrusion by the overlapper can disturb the primary speaker’s speech flow, resulting in increased level of interactivity, overlap, and disfluency, and ultimately a successful turn-stealing (Adda-Decker et al., 2008; French & Local, 1983; Kurtić et al., 2013). Noncompetitive overlaps have also been described. These include collaborative completions, support and acknowledgments of the primary speaker’s turn, and their right to continue. They consist of longer pauses and gaps, and more response tokens (Adda-Decker et al., 2008; French & Local, 1983; Kurtić et al., 2013).
In competitive overlaps, the incoming speaker does not wait until they detect the end of the primary speaker’s turn before they attempt to speak or take over the floor. The overlapper anticipates the moment in advance by monitoring for cues to turn-completion (e.g., phonetic, lexico-grammatical, and/or nonlinguistic, such as gaze). The incoming speaker also plans the content of the response as soon as their message can be understood (Barthel et al., 2016, 2017; Levinson, 2016). Equally, the primary speaker makes effective use of these same cues/practices to induce delays in turn-shift and signal turn-keeping (Ford & Stickle, 2012; Goodwin & Heritage, 1990). For instance, vocalizations, receipt tokens, and raised pitch precede the incoming/overlapper’s subsequent turn-taking (Kurtić et al., 2013). In anticipation of the turn the primary/overlapping speaker may use prolongations, pauses, and high pitch, so as to delay arrival at a place where they risk losing it (Goodwin & Heritage, 1990).
How overlaps, gaps, and no-gaps-no-overlaps are organized in cancer MDMs is not clearly understood. Building such understanding could provide a glimpse into the way interactions and participation in the meetings are managed. This might also inform the understanding of team interactions and complex organizational behavior in various other settings.
Methodologies for Studying Turn-Taking
Several approaches have been used to study turn-taking, such as speech science, interactional phonetics, and conversation analysis (CA). This study employs CA. In its broadest terms, CA focuses on the sequential organization of talk (Jefferson, 2004; Psathas, 1994; Ten Have, 2007). This approach will enable us to examine turn transitioning in cancer MDMs, while focusing on how language affects group interaction. This is important because the literature shows that the way language is used can affect inputs, processes, and outputs (Van Swol & Kane, 2019). Language can also determine the successful implementation of interventions and therapies for patients (Jordan et al., 2009). In the context of meetings, language structures role relationships and how roles provide ground for the authority of claims (Halvorsen & Sarangi, 2015).
While underutilized in the field of multidisciplinary teams (there are only two studies: Dew, 2016; Dew et al., 2014; Housley, 1999), CA has been used in organizational settings, including health care (e.g., Heritage & Maynard, 2006; Robinson, 2003; Stivers, 2001), law, corporations, education, and media to name but a few (e.g., Drew & Heritage, 1992; Gonzales, 1994). In such settings, it is understood that “talk is the central medium through which the daily working activities of many professionals and organizational representatives are conducted” (Drew & Heritage, 1992, p. 43). In the same vein, the in-depth analysis of talk and its organization between individuals can also help to build the understanding of processes within multidisciplinary teams.
Building on previous findings of the unequal participation in cancer MDMs, this study seeks to understand the interactional dynamics between team members in MDMs and identify the practices that members employ to shape levels of participation during individual case discussions. Guided by the principles of CA, we posit:
Method
Participants
Participants were members of one of the three enrolled cancer multidisciplinary teams. All teams had the same professional composition: surgeons, oncologists (clinical and/or medical), cancer nurses, radiologists, histopathologists, and coordinators who play an administrative role. The number of participants from each professional group differed across teams and meetings (Table 1). In terms of gender composition, breast and gynecological cancer teams had substantially more females (89%, 72%, respectively). The colorectal cancer team was mixed-gender with females comprising 47% of the team (Table 1). During the study period, all cases put forward for MDM were video recorded, including suspected or confirmed cancer, and in breast and gynecological cancer teams, also benign cases. Ethical approval for the study was given by the North West London Research Ethics Committee and also locally by the participating hospitals R&D departments. Oral and written consents were given by the team members.
Team Composition and Meeting Characteristics Across the Participating Cancer Multidisciplinary Teams.
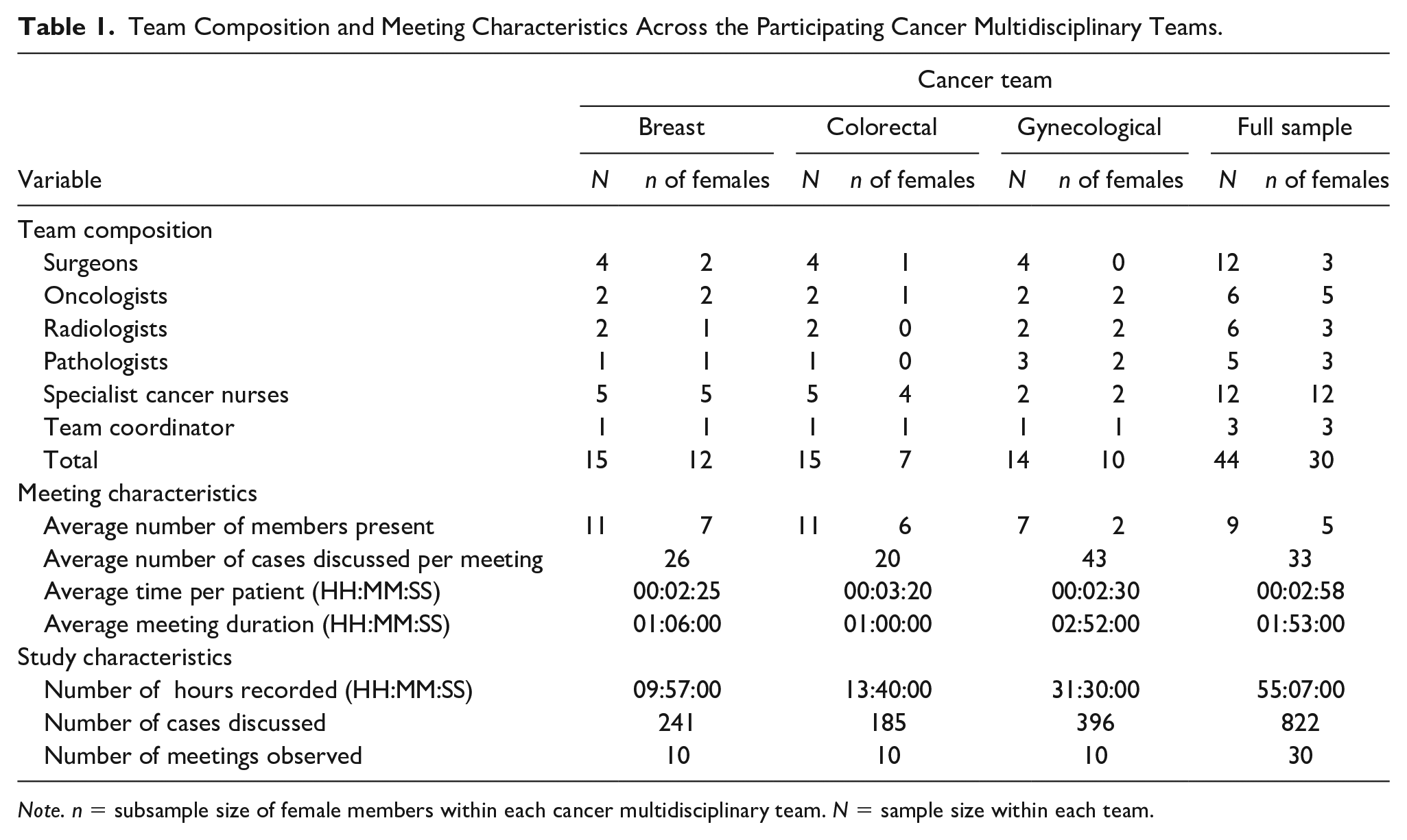
Note. n = subsample size of female members within each cancer multidisciplinary team. N = sample size within each team.
Our data are derived from 55 hr of uncut videotaped cancer meetings, comprising 30 weekly-meetings and 822 case discussions (Table 1). A selection of 24 malignant case discussions (eight from each team, respectively) is presented in this article, totaling 72 min of meeting footage. These selected case discussions were transcribed using Jefferson (2004) notation with all names changed to preserve confidentiality. The selection criteria for the 24 case discussions were as follows:
Audio quality and clarity for transcription using complex Jefferson (2004) notation, because analysis of overlapping talk in recordings of naturally occurring multiparty conversations can be difficult due to the problem of differentiating inputs from overlapping speakers (see Dew et al., 2014; Kurtić et al., 2013);
Feasibility, because (a) the transcription using Jefferson (2004) notation is complex and resource intense (especially for multiple speakers) and (b) the method of analyzing MDMs presented in this study is novel utilizing qualitative data extracts common in CA and quantitative frequency counts common in language sciences (see Materials), the subset was limited to 24 cases;
Malignancy, as benign cases are also discussed at some MDMs, and due to the nature and duration of these discussions, it was important to distinguish between malignant and nonmalignant cases (only malignant cases were included);
Duration of the case discussion, as this can vary from case to case and is important to consider when using frequencies (hence, the selected cases were similar duration, 00:02:25 to 00:03:25);
1st and 2nd half of the meeting ensuring equal distribution of case discussion across the meeting duration (four case discussions were selected from each half across teams);
Saturation on the basis of the case discussions that have met the above criteria.
Materials
Following the principles of CA, detailed data on the complex nature of interactions was generated using Jefferson notation within the transcripts (Jefferson, 2004; Psathas, 1994; Ten Have, 2007). While CA is traditionally a qualitative method, quantification with frequency counts has been used in previous research (e.g., Stivers, 2001, 2002), especially in the field of language sciences (e.g., Kurtić et al., 2013; Levinson & Torreira, 2015; Ten Bosch et al., 2004). A combination of qualitative data extracts and quantitative frequency counts was therefore used for analysis. This is a novel hybrid approach to studying MDMs, and to the best of our knowledge, this is the first study of its kind in the field of multidisciplinary teams. This approach was deemed necessary due to the complexity of the multiparty data that cancer MDMs present with. For quality control, the data have been discussed in multiple data sessions (N = 4) with leading international CA scholars who provided their critical input and insight into the analysis presented in this study. In a confidential manner, the scholars watched MDM videos and discussed the interactions, while formulating points of interest in the data, and how best to analyze such complex multiparty interactions. This is seen as a routine piece of scholarly teamwork and a vital part of CA (Ten Have, 2007).
The Jefferson (2004) transcription system was used to identify gaps, overlaps, and no-gaps-no-overlaps in each MDM case. Overlap was defined as simultaneous speech that can occur between speakers, while gap was defined as a silence between turns that tends to be in the range of 0.2 to 0.6 s. No-gap-no-overlap refers to fluent, organized, and overlap and gap-free turns (Heldner & Edlund, 2010; Kurtić et al., 2013; Levinson, 2016). Within the Jeffersonian transcript, overlap is commonly marked with square brackets [], while gaps are indicated in round brackets (0.2). Thus, all turn transitions between speakers in the data set were examined and instances of overlap, gaps, and no-gap-no-overlap counted and converted into percentages against a total number of turn shifts in a single case discussion. In line with previous research (Heritage & Maynard, 2006; Kurtić et al., 2013), we also examined turns in progress and how a turn may be secured with the focus on raised pitch (up-facing arrow, ↑), vocalizations (ah, eh, er, aw, hm, mm, um), receipt tokens (yeah, okay, yes), and prolongations (::).
The anonymized data set (Soukup, 2017) underpinning this article is on Zenodo, a secure data repository, at https://doi.org/10.5281/zenodo.582283 under Creative Commons Attribution 4.0.
Design and Procedure
This was a prospective observational study. It took place across three hospital sites in the Greater London and Derbyshire areas in the United Kingdom for 3 months during 2016. Twelve consecutive meetings were video recorded for each of the three cancer teams. The first two meetings from each team were excluded from the analysis. This enabled the teams to get used to the camera and being filmed, thus minimizing any Hawthorne effect.
All teams held their MDMs in a designated meeting room; hence, the layout and seating arrangement did not change from week to week. These rooms are fitted with two large wall screens (one displaying patient proforma that the coordinator fills in; the other displays the radiology images or histopathology specimens). The screens are connected to personal computers designated for the coordinator and radiologist, and the microscope for the histopathologist. The screens are also connected to a video conferencing system that allows remote dial-in with other hospital sites. Such set up allows all attendees to view in real time the radiology images, pathology specimens, and patient records. All attendees are seated in a U-shape facing the large screens. The behavior of all attendees can easily be captured by a single camera. The meetings were filmed discretely using a GoPro camera. The camera was positioned alongside the large screens, so that it blended in with the background equipment, and was therefore out of view of the team. Camera sounds and lights were switched off during recording. The camera was operated remotely from a smart phone application. The footage could be seen live on the smart phone and checked during filming without disrupting the meeting, or bringing team’s attention to the camera. Such discretion along with a prolonged period of filming helped to minimize any Hawthorne effect.
Results
Distribution and Temporal Aspects of Gaps, Overlaps, and No-Gaps-No-Overlaps (H1)
Frequency of gaps, overlaps, and no-gaps-no-overlaps
Table 2 contains frequency counts of gaps, overlaps, and no-gaps-no-overlaps, including also gender of the speakers. It is evident that, although the pattern was similar across the teams, there is some variation. For instance, the breast cancer team, which has the highest number of female members, allowed for more turn shifts between speakers compared to colorectal and gynecological teams. This indicates more diversity of speaker selection in the breast team compared to the other two teams where certain disciplines hold the floor for longer periods.
Frequency of Gaps, Overlaps, and No-Gap-No-Overlaps in the Breast, Colorectal, and Gynecological Cancer Team Meetings.
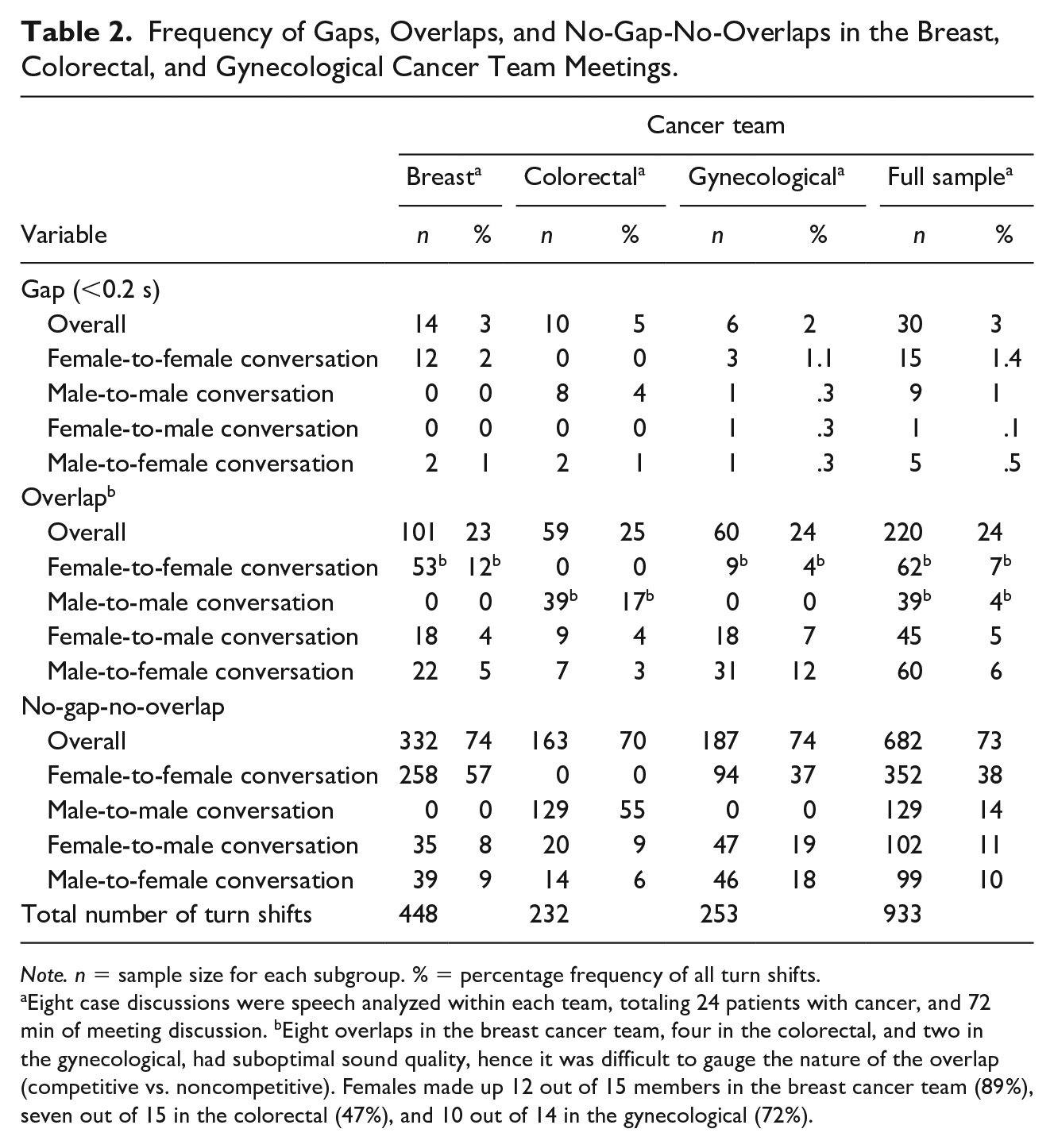
Note. n = sample size for each subgroup. % = percentage frequency of all turn shifts.
Eight case discussions were speech analyzed within each team, totaling 24 patients with cancer, and 72 min of meeting discussion. bEight overlaps in the breast cancer team, four in the colorectal, and two in the gynecological, had suboptimal sound quality, hence it was difficult to gauge the nature of the overlap (competitive vs. noncompetitive). Females made up 12 out of 15 members in the breast cancer team (89%), seven out of 15 in the colorectal (47%), and 10 out of 14 in the gynecological (72%).
H1 posited that overlaps will occur at a frequency of around 30% (H1a), gaps at 60% (H1b), and no-gap-no-overlaps at 10% (H2c; Heldner & Edlund, 2010; Kurtić et al., 2013; Shriberg et al., 2001). As can be seen in Table 2, these hypotheses were not supported. Gaps between speakers were minimal occurring in only 3% of total turn shifts, while overlaps accounted for 24%, and no-gaps-no-overlaps for 73% of transitions between speakers. This indicates that the level of interactivity in the studied teams was high, while turn transitioning was fast-paced (Heldner & Edlund, 2010; Kurtić et al., 2013; Shriberg et al., 2001).
This pattern was further evident in relation to gender composition (Table 2). Fast-paced turn transitioning with fewer gaps (0.6%) and no-gap-no-overlaps (21%) was evident in mixed-gender conversations with the frequency of overlaps increasing where a female was an incoming speaker (13%). In contrast, frequency of gaps (2.4%) and no-gap-no-overlaps (52%) was highest in the same gender pairs with overlaps least frequent in male only pairs (4%). This is in line with previous research indicating a higher rate of overlaps and turn-taking in male-to-female conversations, attributed to greater interpersonal sensitivity in females (Ghilzai & Baloch, 2016; Leaper & Robnett, 2011). However, it has also been argued that how soon the next speaker attempts to take the turn indicates a degree of interactional concern in the second speaker pertaining to relative social status and competitiveness in the tone of conversation (Wilson & Wilson, 2005).
Temporal aspects of gaps between speakers
Table 3 contains the duration of gaps between speakers against the duration of case discussions. It is evident that while gaps were the least frequent mode of turn transition across the teams, when they did occur they were longer than the commonly observed 0.2 s (Heldner & Edlund, 2010; Levinson, 2016; Levinson & Torreira, 2015). This contrasts with face-to-face interactions, which can generate longer gaps (Stivers, 2002). In the context of cancer MDMs, for instance, clinicians are often looking through patient’s notes to find relevant information, or they are requesting further information, or images from radiologists, histopathologists, or coordinators who themselves are searching for this information on the computer system. There are also logistical and technical issues (e.g., losing connection during a teleconference with a key clinician, or technical glitches; for a full list of logistical issues, see Soukup et al., in press). These situations can often produce longer gaps and periods of silence, hence 65% of gaps we recorded were longer than reported previously, that is, 0.2 s (Heldner & Edlund, 2010; Levinson, 2016; Levinson & Torreira, 2015).
Duration of Gaps Between Speakers Against the Duration of Case Discussions Across Cancer Teams.
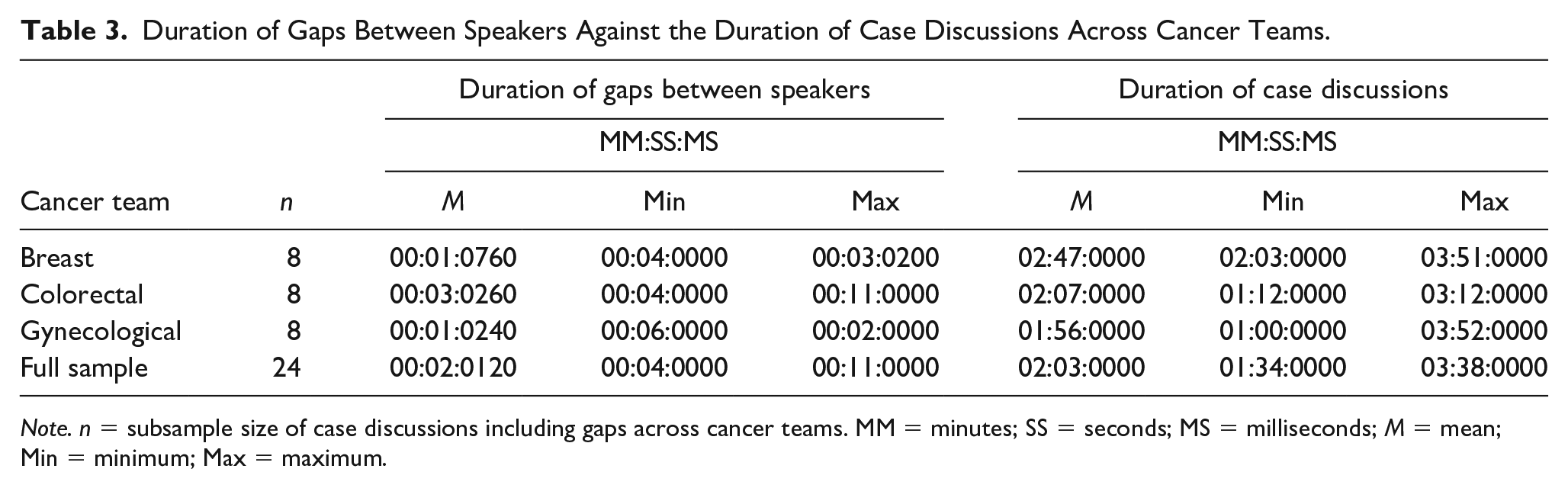
Note. n = subsample size of case discussions including gaps across cancer teams. MM = minutes; SS = seconds; MS = milliseconds; M = mean; Min = minimum; Max = maximum.
The following excerpt is an example of a longer gap and period of silence in the meetings. The female oncologist starts the sequence by asking the male radiologist to put x-ray images up on to the screen for the team to review. This is followed by a 2-s gap that allows the radiologist to find the x-ray and share it on the screen. Following the gap, the female surgeon immediately self-selects to speak by sharing their opinion of the x-ray.
89 female oncologist A: [ji:::m >↑can ] ↑we ↑just< ↑look at her x ray from
90 ↓
92 male radiologist A: [
93 female oncologist A: °↑thank you°
94 2.0 gap allowing the radiologist to share x-ray images on to the screen
95 female surgeon A: °u::::m° (.) °okay° (0.4) °that’s (the le::sion)° (0.8)
Competitive and noncompetitive overlaps
Table 4 shows frequency of competitive and noncompetitive overlaps, while Table 5 contains examples of the competitive and noncompetitive overlaps observed in the data. It is evident that more than half (57%) of all overlaps were competitive in nature. This pattern was consistently evident across all three teams. While the data show that 36% of these overlaps are in conversations where an incoming overlapping speaker is female, this seems to be the case for the breast and gynecological cancer teams only where females make up the majority. In contrast, in the colorectal cancer team where gender is more mixed (females are at 47%), the incoming overlapping speaker was predominantly a male member, accounting for 53% out of 63% of the total overlaps (and 14% out of 21% across all three teams). What is more, the colorectal cancer team showed the highest frequency of competitive (63%) and lowest frequency of noncompetitive overlaps (31%), in contrast to the remaining two teams with more females. These findings corroborate the literature on gender and turn-taking in groups, indicating that more mixed-gender conversations have a higher degree of competitiveness and interactional concern (Ghilzai & Baloch, 2016; Leaper & Robnett, 2011; Wilson & Wilson, 2005).
Frequency of Competitive and Noncompetitive Overlaps in the Breast, Colorectal, and Gynecological Cancer Team Meetings.
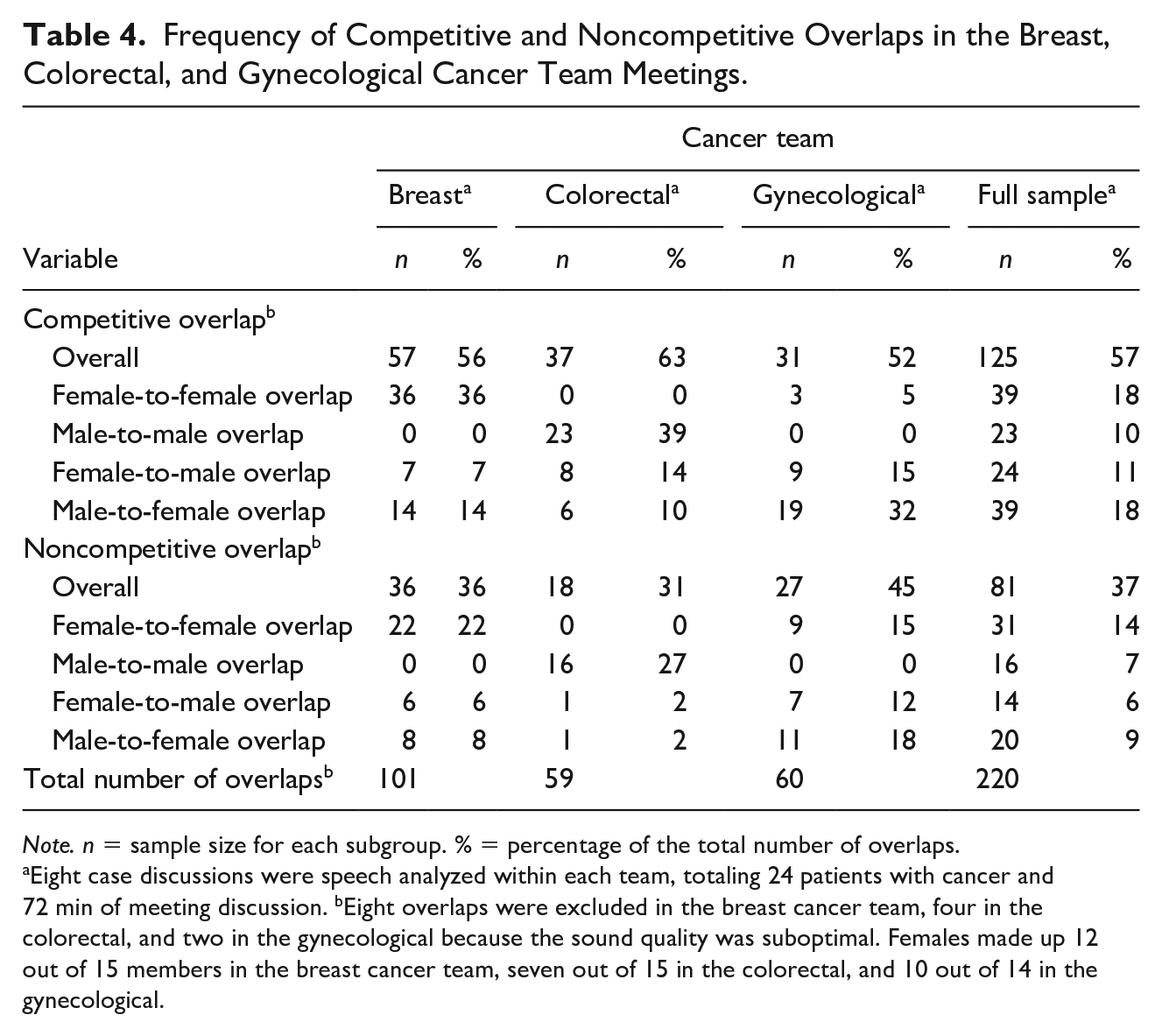
Note. n = sample size for each subgroup. % = percentage of the total number of overlaps.
Eight case discussions were speech analyzed within each team, totaling 24 patients with cancer and 72 min of meeting discussion. bEight overlaps were excluded in the breast cancer team, four in the colorectal, and two in the gynecological because the sound quality was suboptimal. Females made up 12 out of 15 members in the breast cancer team, seven out of 15 in the colorectal, and 10 out of 14 in the gynecological.
Definition and Examples of Competitive and Non-competitive Overlaps between Speakers.
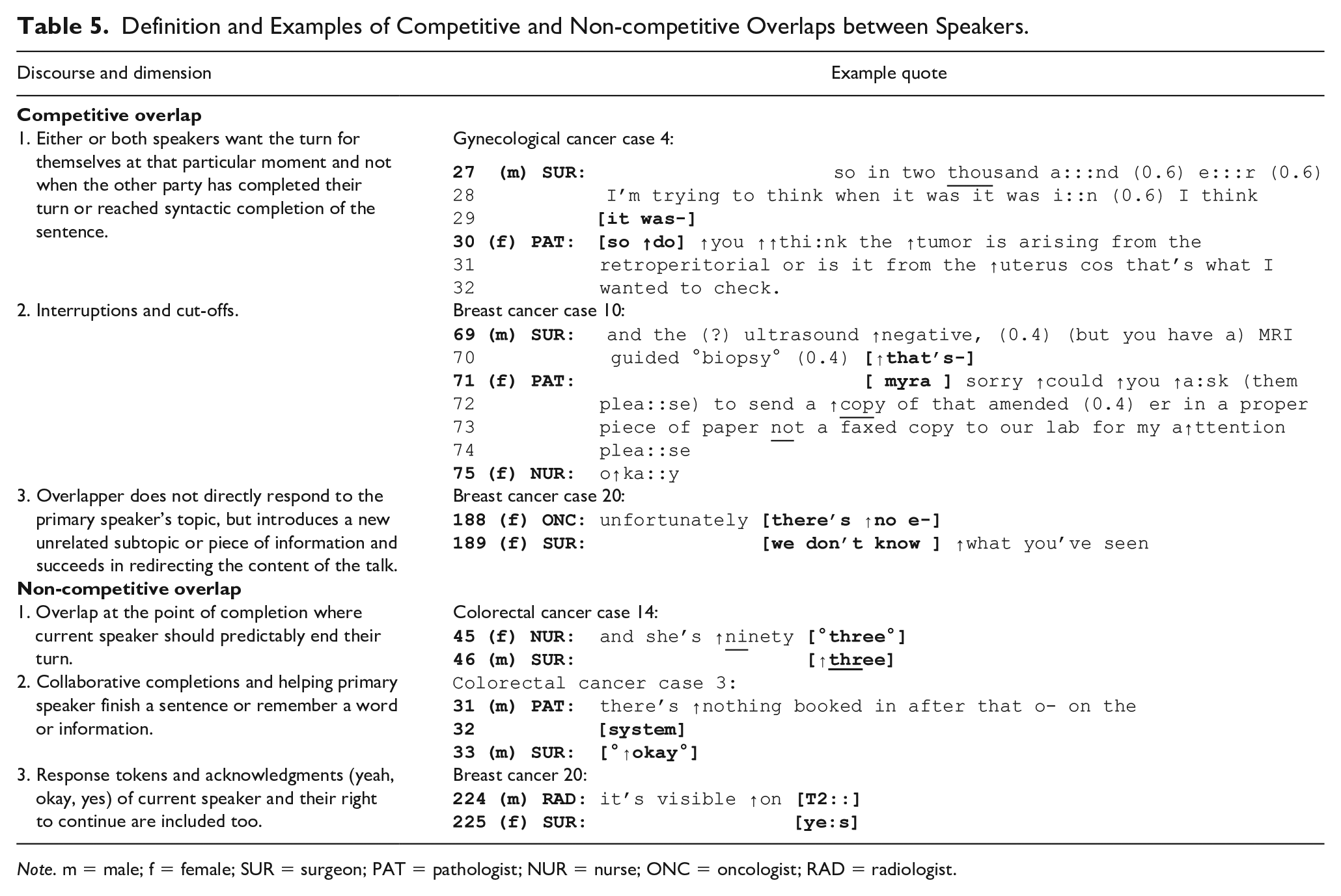
Note. m = male; f = female; SUR = surgeon; PAT = pathologist; NUR = nurse; ONC = oncologist; RAD = radiologist.
Nature of Turn Transitions
To further unpack how team members obtain and secure their turn to speak, we explored turns in progress in H2. The analysis focused on the raised pitch (up-facing arrow, ↑), pauses (.), vocalizations (ah, eh, er, aw, hm, mm, um), receipt tokens (yeah, okay, yes), and prolongations (:) (Heritage & Maynard, 2006; Kurtić et al., 2013).
H2 posited that vocalizations, receipt tokens, and raised pitch will precede overlapper’s turn-taking (H2a), while in the anticipation of turn the overlapping speaker will use prolongations, pauses, and high pitch (H2b). Both hypotheses were supported. Turn-taking was consistently preceded by raised pitch (↑), vocalizations and receipt tokens, and to a lesser extent prolongations (:), which supports H2a. These were used by the team members (male and female) to acknowledge the speaker and signal to them to continue (Sacks et al., 1974), as well as a form of pre-articulation to prepare the speaker and the team for the turn transition that follows (Levinson, 2016). Raised pitch, described in previous research as “turn competitive hitches” (Heritage & Maynard, 2006), appeared most frequently in overall 65% of all turn transitions. On the contrary, speakers appeared to use prolongations (::), pauses (.), and in some cases raised pitch (↑) in anticipation of turn stealing, “thus organizing their talk as to delay arrival at a place where they risk losing their turn” (Goodwin & Heritage, 1990). Thus, H2b was also supported.
While pitch, pauses, prolongations, vocalizations, and tokens were used in this manner by both male and female members, the incoming male speakers appeared to secure their turn within a fewer turn shifts than the females (see Table 2). Thus, there are greater turn-taking rates, especially overlaps, in male-to-female conversations, which has been attributed to interactional concerns, and in females, also interpersonal sensitivity (Ghilzai & Baloch, 2016; Leaper & Robnett, 2011; Wilson & Wilson, 2005).
We also found that team members, irrespective of gender, predominantly self-selected to speak. They were also selected by the preceding speaker, especially when information was being requested (e.g., imaging from radiologists, lab results from histopathologists). This pattern, in the context of MDMs, appears to be driven by the activity roles, in particular the level of information and responsibility the team member that self-selects to speak has, or perceives to have, over the patient’s case. Hence, both male and female members tend to self-select to speak in such circumstances. This is in line with previous research (Halvorsen & Sarangi, 2015; Housley, 1999) showing that the roles of the meeting participants cumulatively add to the joint production of decisions based on their organizational role responsibility and expertise.
The following are excerpts of turn shifts across the three participating cancer teams that demonstrate the aforementioned observations and the corresponding literature.
Breast cancer team
First is an example of an exchange between a female surgeon and a female oncologist in a meeting with 15 health professionals present, 12 of whom were females. Out of four surgeons (three females, one male), female surgeon A begins presenting a patient to the team. Female surgeon A uses frequent prolongations (::) in anticipation of the turn shift by female oncologist A. Out of two female oncologists, oncologist A self-selects to speak. Female oncologist A responds twice using vocalizations (mm, hmm) with raised pitch (↑), and repeated overlaps [], before taking over the floor in the final line. In contrast, the first speaker, female surgeon A, uses frequent prolongations (::; n = 10), high pitch (↑; n = 10), and pauses (n = 10) in anticipation of losing their turn to speak and opportunity to input into the case discussion.
1 female surgeon A: so ↑she is a lady who:: (0.4) ↑basically:: ha::s (0.4) u:::m
2 (0.4) a ↑symptomatic lump which has been there for (.) a
3 ↑few ↑yea::rs (0.4) ↑did a ↑biopsy turned out to be a
4 grade[one]
5 female oncologist A: [↑mm]
6 female surgeon A: >we started her< on letriz[o:l]
7 female oncologist A:
8 female surgeon A: u::::m (.) ↑which (0.6) after few months (0.6) got ↑bigger,
9 e:::r and it ↑did actually:: (0.4) you kno:w (0.4) become
10 slightly bi[gger]
11 female oncologist A: [why] did she sta:rt on letri↑zole?
Colorectal cancer team
This is an exchange between a female nurse and a male surgeon in a meeting with 15 health professionals present, seven of whom were female. Out of five nurses (four females, one male), female nurse A starts with a case presentation to the team. Female nurse A uses frequent pauses and prolongations (::). Out of three male surgeons, surgeon A self-selects to speak. Male surgeon A responds with a prolongation (::) and raised pitch (↑), embedded into the vocalization, “hm:::↑mm,” before securing their turn to speak. In the anticipation of this turn the first speaker, female nurse A, repeatedly uses frequent pauses (n = 9), high pitch (↑; n = 7) and prolongations (::; n = 6) within each turn. This is in the attempt to delay arriving at the point where they lose their turn to speak and opportunity to input into the case discussion.
1 female nurse A: this is the ↑lady that was um, (.) seen (.) ↑privately by:: mister
2 otsuka because um the GP found (?) (would be) (a↑rranged) (0.4)
3 and she had a change in ↑bowel habits and weight loss and loss of
4 appetite,(0.4) and she was ↑seen ↑here ↑by arthu::r (0.4) o::n
5 saturday (0.4)
6 male surgeon A: hm:::↑mm
7 female nurse A: and the::n, (0.6) .tch ↑si::nce (.) since she was seen by:: arthur (0.4)
8 (apparently) the ↑GP told her that she might have er bowel cancer
9 (0.6)
10
11 male surgeon A:
Gynecological cancer team
The exchange is between a female radiologist and female oncologist in a meeting with 14 health professionals present, 10 of whom are female. Of the three female radiologists, radiologist A self-selects to speak and makes a statement to the team. Out of the entire team and two other female oncologists, oncologist A self-selects to speak. Female oncologist A responds with a response token, “Yeah,” which includes prolongations (::) and raised pitch (↑) three times in succession prior to a successful turn switch in the final line. In the anticipation of this turn the female radiologist A uses frequent high pitch (n = 12), pauses (n = 7), and prolongations (n = 4) repeatedly within each turn in the attempt to delay arriving at the point where they lose their turn to speak and opportunity to input into the case discussion.
19 female radiologist A: we ↑picked ↑it ↑up originally with [°(?)° ] as a
20 malignant (0.4) retroperitonea:l=
21 female oncologist A:
22 female radiologist A: =fi↑brosis sort of
23 female oncologist A:
24 female radiologist A:
25 everything< >in the< (.) >in the< (↑posterior) aspect and
26 it’s< (0.4) it’s pro↑gessing (0.6) there’s ↑no fat planes in the
27 pelvis at ↑a:ll now
28 female oncologist A: ↑yea:h
29 female radiologist A: ↑I:’m, (0.4) >sort of< slightly surprised she hasn’t got a
30 ↑bowel obstruction.
31 female oncologist A: ↑we:ll (.) she does have occasional bleeding (0.4) (PR) but
32 (.) we: we had it ↑checked out (it was because of some)
33 (radiotherapy) (?) ↑she::’s, (.) ↑not ↑well lady (0.4) ↑a::nd,
34 (.) u::m, (0.6) ↑i::t’s she ↑would (.) she’s devastated she has
35 (children)
Discussion
This study aimed to explore, on a microlevel, the nature of turn-taking during discussions about the patients in cancer MDMs with the focus on two objectives. The first objective was to identify the distribution and temporal aspects of overlaps, gaps, and no-gaps-no-overlaps in line with the turn-taking model proposed by Sacks et al. (1974). The second objective was to examine turns in progress to identify how members obtain their turn to speak (Goodwin & Heritage, 1990).
For the first set of hypotheses, the frequency distribution of gaps, overlaps, and no-gaps-no-overlaps in this study contradicts previous research (Heldner & Edlund, 2010). Hence, H1a to H1c were not supported. Previous studies have shown that when measured against the number of speaker-turns, overlap has been documented at a frequency of 30% in multiparty meetings, with gap considered the most frequent type of turn transition accounting for 60%, whereas no-gap-no-overlap accounted for the remaining difference (Heldner & Edlund, 2010; Kurtić et al., 2013; Shriberg et al., 2001). In contrast, in MDMs we found that the overlap accounted for 24% of the total speaker-turns, with the gap being the least frequent type of turn transitioning accounting for only 3%, and no-gaps-no-overlaps for 73%. This finding points to fast turn-taking between members, and a highly interactive meeting environment. Mixed-gender conversations further intensified this pattern. Female incoming speakers allowed for more turn shifts, while male speakers secured their turn to speak more quickly, that is, within a fewer turn transitions. This is in line with previous research demonstrating greater turn-taking rates in mixed-gender conversations that have been attributed to interactional concerns, and in females, also interpersonal sensitivity (Ghilzai & Baloch, 2016; Leaper & Robnett, 2011; Wilson & Wilson, 2005).
For the second set of hypotheses, turn transitioning between team members appeared to be secured predominantly with raised pitch, which accounted for more than half of all turn transitions. Vocalizations and receipt tokens were also used, as well as prolongations, although less frequently. This is consistent with our H2a and H2b, and also with previous research on turns in progress. We have shown that vocalizations, receipt tokens, and raised pitch tend to precede overlapper’s turn-taking (Kurtić et al., 2013) with a novel finding of occasional prolongation with the receipt token (H2a). On the contrary, the primary speaker appeared to use prolongations and pauses frequently, and in some instances high pitch (H2b). This is arguably in anticipation of turn stealing, thus organizing their talk as to delay arrival at a place where they risk losing it (Ford & Stickle, 2012; Goodwin & Heritage, 1990). A team member may use a response token, for instance, not only to acknowledge the speaker, but also to secure their turn and prepare the group for the subsequent turn shift (Heritage & Maynard, 2006; Levinson, 2016).
Such interactive setting can contribute to systematic reduction in turn-taking opportunities and present with difficulties in securing one’s turn to speak (Goodwin & Heritage, 1990). Hence, the observed inequality of participation that has been observed from a macroperspective in previous studies (see Soukup, Lamb, et al., 2019). This speaking challenge may intensify or lessen depending on the team members’ seniority (see Cosby & Croskerry, 2004; Kohn et al., 2000; Vincent, 2010), which could drive the ability to secure one’s turn to speak successfully and effectively contribute to a case discussion. In turn, it is possible that team members orient to this norm for structuring meetings (Dew, 2016; Dew et al., 2014; Heritage & Maynard, 2006). However, the question arises of whether this is an optimal set-up that effectively utilizes its greatest asset necessary for managing complex care of patients with cancer (i.e., the diversity of expertise). It repeatedly has been found that seniority and authority gradients have a negative impact on communication between health care professionals and on patient safety (see Francis, 2015; Kohn et al., 2000; Vincent, 2010). As one team member reported in an interview concerning effectiveness of MDMs, “I am always amazed how very able staff can be so passive” (Raine et al., 2014).
Building our understanding of teamwork from a microlevel is therefore important. It can help unpack the interactional dynamics underpinning decision-making in cancer MDMs and help in developing strategies for better outcomes. The contribution of this study is fourfold. First, the findings directly contribute to the social science study of teams and groups by unraveling some of the reasons behind underutilization of expertise in workplace meeting (Valcea et al., 2019). In addition to poor communication (Woolley et al., 2008) and increased performance pressures (Gardner, 2012), the findings reveal another barrier; that is, reduced opportunities for turn-taking, especially in mixed-gender interactions. This is due to an increased rate of turn-taking and overlaps with hardly any gaps.
Second, the findings highlight the importance of effective turn-taking management in these meetings, as adequate information sharing is critical to team performance (Mesmer-Magnus & DeChurch, 2009). The chair of the meeting has a particularly important role in this respect (Modada, 2013; Svennevig, 2008). In MDMs, for instance, the chair can coordinate turn-taking ensuring that all core members have an opportunity to contribute clinically and share critical information about the patient (Soukup et al., 2018; Soukup, Lamb, et al., 2019). Indeed, the functional perspective of group decision-making suggests that interaction process in groups can be regulated with appropriate strategies for better outcomes (Forsyth, 2014; Poole & Hollingshead, 2005).
Third, this study identified and tested for feasibility a novel method for studying micro-aspects of group communication and behavior in groups. This has been called for (Keyton, 2016) and shown to be methodologically understudied because the focus has been primarily on macro-aspects of teamwork through quantitative approaches (Dinh et al., 2020). Finally, the findings have an applied clinical value. They contribute directly to building knowledge base to facilitate team quality improvements going forward. They also narrow the gap in the literature on health care teams that is to date largely focused on evaluating teamwork from a macrolevel perspective (Soukup et al., 2016).
Further Research
Further studies are needed to explore three different components of interaction in MDMs. The first is related to overlapped speakers and how they deal with competition and incoming speakers, that is, whether they slow down or resist (also known as the attack/resist ratio). An increase in dysfluencies as a result of intrusive incoming speakers and how they affect team processes raises several questions. Do they add to the cognitive load of the team? Do they add to the overall duration of the meeting? How do they affect team decision-making? Addressing these questions can help design appropriate strategies for such teams that could regulate interaction process and improve team outcomes (Forsyth, 2014; Poole & Hollingshead, 2005). The second is the role of team culture and individual differences in the interactional dynamics among members, and how this relates to unequal participation. The third is silence in the meetings, which can be difficult to interpret (see Lamb et al., 2012, 2013). Hence, future studies should look at nonverbal means of communication between team members (e.g., gestures, eye contact) using CA, because it is methodologically suited to examine this in detail.
Implications for Practice
In terms of the practical implications of our findings for cancer MDMs, it is important to consider that cognitively, gaps in social interactions are important for language processing. Having rapid turn-transitions for a prolonged period of time may not work to the cancer team’s advantage because it can exacerbate the cognitive fatigue that is associated with sequential tasks. For instance, the preliminary evidence from studies of cancer MDMs suggests that the prolonged reviewing of sequential cases has a negative impact on the quality of treatment recommendations for patients (see Lamb et al., 2013; Soukup, Gandamihardja, et al., 2019; Soukup, Lamb, et al., 2019). Better quality decisions were associated with discussing patients at the beginning of the MDM. While in our study meeting duration was between 45 and 160 min, duration of up to 5 hr has been reported for some teams (not necessarily including a break; Cancer Research UK, 2017).
Specifically, a minimum of 0.6 s is needed for the brain to execute production planning for a single word (i.e., conceptualize, retrieve, and encode). Thus, gaps of this duration are a common silence threshold in the end of utterance detectors (Heldner & Edlund, 2010). However, gaps of 0.2 s are commonly found between speakers (an average duration of a single syllable). This suggests that in the middle of the incoming turn, the next speaker predicts the turn-end of that speaker (i.e., the rest of the utterance), while planning a response (Barthel et al., 2017; Heldner & Edlund, 2010; Levinson, 2016). Hence, the comprehension of the incoming turn and production of speech as a response overlap in the brain’s language processing system. See Figure 1 for a graphical representation of this point.
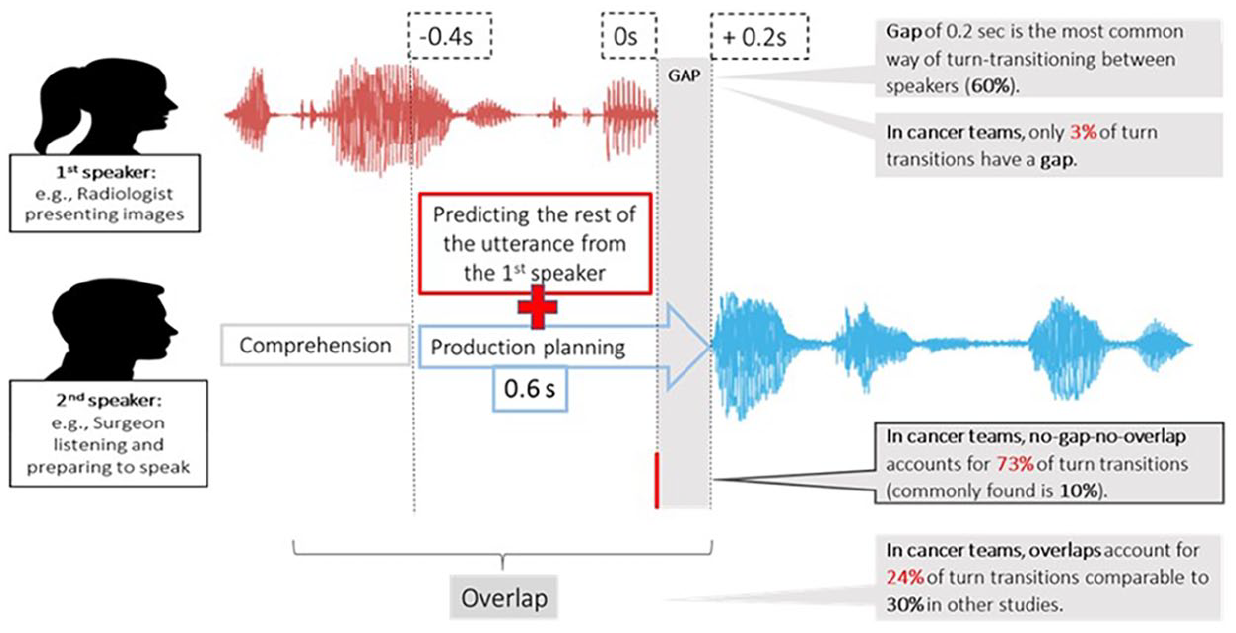
Cognitive challenge of turn transitioning in between two speakers during case discussions in cancer team meetings.
As the brain switches from comprehension to production, turn-taking is, therefore, a cognitively challenging task. This is particularly the case in the current data set where gaps occur in only 3% of turn shifts, which is substantially less than reported in previous research (e.g., 57%–59% across three different data sets; Heldner & Edlund, 2010). Likewise, it has been argued that in competitive environments, speakers may decide to start articulating speech before thoroughly understanding the remaining utterance from the first speaker. They may even overlap with them, which narrows down the gap necessary for adequate language processing (Barthel et al., 2016, 2017; Levinson & Torreira, 2015). This leaves room for error in comprehension that can have a knock-on effect on production planning, or, what is being said by the second speaker. See Figure 2 for an illustration of this point.
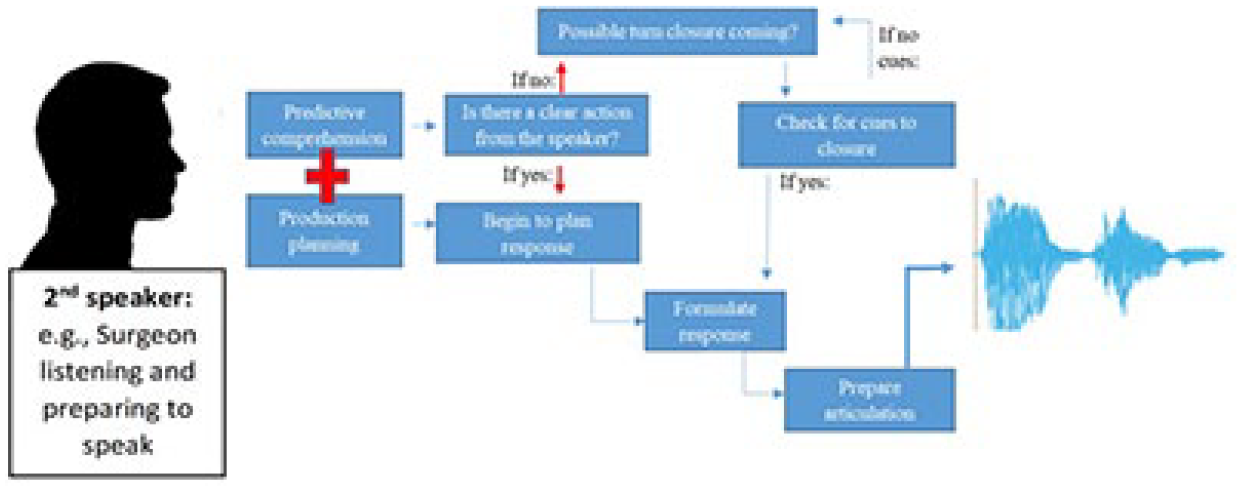
Cognitive challenge of turn transitioning in the second speaker during case discussions in cancer team meetings.
Taken collectively, it is reasonable to suggest that having rapid turn transitions for prolonged periods may hinder effective communication and open up the opportunity for misunderstanding and error. With the incidence of cancer and financial pressures on health care rising (World Health Organization, 2014), there are more patients to discuss, meetings are taking longer, and more than half of the patients are receiving less than 2 min of team input (Cancer Research UK, 2017). It is essential therefore to understand whether the current organization of cancer MDMs is sustainable and conducive to effective team processes and outcomes, as well as patient safety. This is especially important in the light of evidence showing communication issues as the leading cause of inadvertent patient harm (in over 70% of reported cases; Leonard et al., 2004). Designing strategies that regulate interaction processes in teams may be one way forward. A strategy to consider is to have a trained, clinically noncontributing chair to effectively coordinate turn-taking in MDMs (Dew et al., 2014; Modada, 2013; Svennevig, 2008); short breaks for food/fluid intake and respite (Soukup, Gandamihardja, et al., 2019; Soukup, Lamb, et al., 2019) are also recommended.
Limitations
Our study should be interpreted against certain limitations. The first is the Hawthorne effect, which we minimized by (a) adopting a long-term approach to filming (3 months for each team), (b) excluding the first two meetings in each team from the analysis, and (c) ensuring that filming is done discretely. Second, we did not look at nonverbal communication between team members, such as gesture and eye contact. Future studies should therefore further examine this aspect. Finally, while this study suggests a highly interactive meeting environment for cancer teams, there is currently no accepted standard for these matrices in the setting of cancer MDMs. As a result, the safety implications of this speech analysis remain exploratory and are not yet equated to clinical outcomes.
Our study also has strengths. As real-time observations of cancer teams, we captured the flow of behavior in its typical setting, thus achieving greater ecological validity. We generated new avenues of inquiry that can bring further insights for improvement of cancer teams and better understanding of teams in general. We demonstrated feasibility of the novel method of analyzing communication in teams, paving the way for future studies wishing to unpack complex interactional team dynamics (e.g., across different chronic conditions that use MDMs). Such studies could apply our method to a larger sample to help build knowledge and generalizability.
Conclusion
Theories of small groups point to the importance of understanding interactions between members for achieving better outcomes. Evidence from a macro-perspective points to unequal participation among members in cancer MDMs. From a micro-perspective, this study provides a window into the practices used to shape levels of participation. We found that the frequency of gaps was low, and the frequency of no-gaps-no-overlaps was high, pointing to fast turn-transitions, which with a high frequency of overlaps make for a highly interactive meeting environment. Securing one’s turn to speak can thus present with a challenge to team members, leading to unequal participation. Further research is needed to explore the role of authority gradients and the way members deal with incoming competing speakers. This in turn has implications for patient safety because rapid turn transitions for prolonged periods may hinder effective communication. We contribute directly to small group research by identifying a novel method for studying micro-aspects of group communication. We also contribute to health care research by narrowing the gap in the literature on teamwork, which to date has mainly focused on team evaluations from a macrolevel perspective.
Footnotes
Acknowledgements
The authors thank the participating cancer teams and their members for their time and commitment.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.S. is the Director of London Safety & Training Solutions Ltd, which provides team-working, patient safety, and improvement skills training and advice on a consultancy basis to hospitals and training programs in the United Kingdom and internationally. T.S. serves as a research consultant to F. Hoffmann-La Roche Ltd Diagnostics providing advisory research services in relation to innovations for multidisciplinary tumor boards in the United States. T.S. and B.W.L. also provide advisory research services and training in the assessment of cancer multidisciplinary teams in the United Kingdom through the Cancer Alliances Network. JSAG is a Director of Green Cross Medical Ltd that developed MDT FIT for use by National Health Service Cancer Teams in the UK. The other authors have no conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by the UK’s National Institute for Health Research (NIHR) via the Imperial Patient Safety Translational Research Centre. Sevdalis research is funded by the NIHR via the ‘Applied Research Collaboration South London’ at King’s College Hospital NHS Foundation Trust, London, UK. Sevdalis is also a member of King’s Improvement Science, which is part of the NIHR CLAHRC South London and comprises a specialist team of improvement scientists and senior researchers based at King’s College London. Its work is funded by King’s Health Partners (Guy’s and St Thomas’ NHS Foundation Trust, King’s College Hospital NHS Foundation Trust, King’s College London and South London and Maudsley NHS Foundation Trust), Guy’s and St Thomas’ Charity, the Maudsley Charity and the Health Foundation. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.