
Abstract
More than 15% of refugee families will experience pregnancy loss. Feelings of stigma, shame, and guilt may be common after experiencing such a loss. The presence or absence of supports may help to exacerbate or ameliorate these feelings. The research used a qualitative approach to explore experiences of pregnancy loss among Syrian refugee families who were displaced in Lebanon. The foundation of the research was 15 collaborative family interviews with mother-father dyads followed by one-on-one interviews with mothers and fathers and two peer group discussions. The viewpoints and experiences of practitioners were elicited through three one-on-one interviews and four peer group discussions. By focusing on both formal and informal supports, the research suggests ways that practice and policy may be improved to better meet the needs of displaced families who have experienced pregnancy loss.
Keywords
Introduction
War tears apart the social fabric of families and communities. In addition to high civilian death rates, surviving family members may be exposed to violence and lack access to basic needs such as food and shelter. If a family is able to flee the violence within their home community, they may find themselves living in unfamiliar and inhospitable surroundings devoid of the social support networks that they typically relied on in the past.
At the same time that families are struggling in the face of war and displacement, they continue to engage in life-affirming family practices such as childbearing and childrearing. Fifty percent of war-affected and displaced populations are women and girls (United Nations High Commissioner for Refugees [UNHCR], 2025), who often bear a heavy burden caring for families and communities (Global Affairs Canada, 2017; UNHCR, 2019). An estimated 20% of war-affected women and girls are considered to be of reproductive age (Hynes et al., 2002; Sachs, 1997), with one in five likely to become pregnant at any time during war and displacement (Bendavid et al., 2021). It is further estimated that about 15% of these families will experience some form of pregnancy loss, defined as miscarriage (loss of pregnancy before 20 weeks of gestation), stillbirth (death from 20 weeks of gestation), and neonatal death (death up to 28 days after birth) (Harakow et al., 2021; Khadra et al., 2022). However, miscarriages and stillbirths are not systematically recorded, suggesting that the percentage is likely higher (UN Inter-agency Group for Child Mortality Estimation [UN IGCME], 2020). While pregnancy loss is a common experience for women in both peaceful and wartime settings, there is little research on the experience of pregnancy loss among war-affected populations. This research aims to fill the gap by exploring the phenomenon of pregnancy loss among a population of war-affected Syrian refugee families displaced in Lebanon.
Context and Literature Review
Displaced Syrians in Lebanon
The conflict in Syria was considered to be one of the worst humanitarian crises in modern history. Since the start of the conflict in March 2011, over half of Syria’s population was displaced both inside Syria and in neighboring countries. Most Syrian families sought refuge in neighboring countries, including Lebanon, a small country of just 4,000 square miles (Dionigi, 2016). Lebanon hosted approximately 1.5 million Syrian refugees (European Commission, 2025), and there was no country in the world that had taken in as many refugees in proportion to its size (Kelley, 2017; van Teutem, 2025).
Lebanon is not economically prosperous, and it has been historically battered by religious divisions and political violence. The large number of Syrian refugees further strained Lebanon’s already stressed infrastructure, increasing social tensions, while deepening the country’s socioeconomic disparities (United Nations High Commissioner for Refugees, 2024). Within this context, high rates of poverty, burdensome governmental policies and regulations, a lack of affordable housing, food insecurity, decreased school attendance, and family violence all increased the vulnerability of Syrian families living in Lebanon. Exacerbated by the war and subsequent displacement, these vulnerabilities have a destabilizing effect on Syrian parents, as they struggle to meet their families’ needs in a low-resource and inhospitable environment (Akesson & Badawi, 2021).
The political landscape in Syria and Lebanon has shifted dramatically following the fall of Bashar al-Assad’s regime in late 2024. While the collapse of the regime initially sparked hope among displaced Syrians, the ensuing power vacuum and factional infighting have prolonged instability, dashing prospects for safe return. For refugee families in Lebanon, this transition has paradoxically worsened conditions: host-country restrictions remain stringent and the absence of a centralized Syrian authority has stalled repatriation agreements and international coordination (Baroud, 2025).
Syrian families living in Lebanon continue to face many hardships, which are exacerbated by the Lebanon government policy that does not officially recognize them as refugees under the 1951 Refugee Convention. Therefore, displaced Syrians who wish to legally live in Lebanon require an annual residency permit with a $200 annual fee and sponsorship by a Lebanese citizen. This requirement is unattainable for most Syrian families, as 90% of them live below the poverty line (Yasin, 2023) and 20-50% are food insecure (Integrated Food Security Phase Classification [IPC], 2023). With global attention diverted to Syria’s internal fragmentation, humanitarian aid to refugees in Lebanon has dwindled, exacerbating food insecurity, unemployment, and barriers to health care (Mishra, 2025). Amid these systemic failures, pregnancy loss—already a traumatic event—becomes another layer of grief compounded by existential uncertainty and fractured support systems.
Pregnancy and Pregnancy Loss in War and Displacement
Approximately 500 women in war-affected countries die each day from complications related to pregnancy and childbirth (Osotimehin, 2016; UN Women, 2024). While increased maternal mortality can be a direct consequence of armed conflict, research has found elevated levels up to three years post-conflict (Munyuzangabo et al., 2021). War-affected pregnant women also face increased risks of fetal mortality (The Lancet, 2016; McGready et al., 2018; World Health Organization [WHO], 2016), premature labor (Abu Hamad et al., 2007; Zahedroozegar et al., 2023), cesarean sections (Huster et al., 2014; Marsi, 2016), and low birthweight (Demirci et al., 2017; Zahedroozegar et al., 2023). Restricted movement of Syrian refugees in Lebanon contributes to increased health problems for pregnant refugees (Alnuaimi et al., 2017). Combined with precarious legal and economic status, pregnant women may face barriers accessing perinatal services (Mazhar, 2015; Nguyen & Le, 2022). War and displacement, which disrupts access to social support networks, along with restrictive gender role ideologies inherent in patriarchal family structures, may exacerbate mental health challenges among pregnant women (Bendavid et al., 2021; Falah-Hassani et al., 2015; Rahman & Creed, 2007). Furthermore, women who are subjected to family violence may not have an opportunity to access social services if their mobility is restricted (Samari, 2017).
Pregnancy loss is more prevalent among women in low-resource settings (The Lancet, 2016), particularly those affected by war and forced displacement. As is the case with Syrian refugees who are living in Lebanon, displaced populations often relocate to neighboring countries with strained systems, where limited access to medical care, malnutrition, and heightened stress contribute to adverse pregnancy outcomes (Reese Masterson et al., 2014). Trauma-related stress has been found to contribute to an increased number of pregnancy losses among Syrian refugees (Aswad, 2005; Khadra et al., 2022; Rowell, 2017). In Lebanon, pregnancy loss among Syrian mothers has also been linked to other environmental factors related to poor infrastructure and no access to services (Middle East Monitor, 2018; Rowell, 2017).
Despite a concerted effort and gains to address maternal morbidity and mortality through global initiatives such as the Millennium Development Goals, pregnancy loss remains “a neglected tragedy” (UN IGCME, 2020). The psychosocial impact of these losses is under-researched and under-discussed. What the research (especially from the Global North) has uncovered is that pregnancy loss—at any stage of pregnancy—is a major life event with the possibility of adverse psychosocial consequences for mothers, fathers, other members of the family, and the community (Gold et al., 2016). Mothers face a range of difficult emotions including distress, hopelessness, and a heightened risk of mental health conditions such as anxiety and depression (Bonanno et al., 2002; Meredith et al., 2017; Murphy et al., 2014; Turton et al., 2001). The loss can also have a destabilizing effect on the family, which is already in a precarious context of violence and uncertainty. For some, the loss will trigger adverse mental health outcomes ranging from depression, anxiety, and traumatic stress (Beutel et al., 1995; Cumming et al., 2007; Gold et al., 2015).
Theoretical Framework: The Triple Trauma Paradigm and Pregnancy Loss
The triple trauma paradigm provides a useful lens for understanding the compounded adversities faced by war-affected families, including Syrian refugees in Lebanon. This framework highlights how families endure cumulative stressors—such as poverty, trauma, and social isolation—with each layer exacerbating their vulnerability (Oduola & Dykxhoorn, 2022). For displaced Syrians, these stressors manifest as “layers of loss”: the loss of home, community, and country; separation from loved ones; and the erosion of stability in housing, livelihoods, health, and education. Pregnancy loss introduces an additional, deeply personal trauma, intersecting with these existing hardships to intensify psychosocial distress. Research suggests that such compounded losses can overwhelm coping mechanisms, leading to heightened risks of anxiety, depression, and familial strain (Hvidtfeldt et al., 2022; Schmidt, 2023)
Coping in the “Silent Environment” of Pregnancy Loss: The Importance of Social Supports for Mothers and Fathers
While mothers are often the focus of pregnancy loss research, fathers also experience profound grief, albeit expressed differently (Kersting & Wagner, 2012; Obst & Due, 2019). Studies note fathers may exhibit grief intensity similar to or exceeding mothers’ (Bonnette & Broom, 2012; Conway & Russell, 2000; Puddifoot & Johnson, 1997). Yet their needs remain overlooked, particularly in displacement contexts where compounded stressors—isolation, poverty, and trauma—further complicate mourning (Avelin et al., 2013). Our study directly addresses this gap by examining how social supports shape coping for both war-affected mothers and fathers, whose grief unfolds in a context of systemic deprivation.
Futhermore, pregnancy loss often occurs in a “silent environment” (Bansen & Stevens, 1992), where lack of recognition and limited avenues for open discussion exacerbate distress (Rowlands & Lee, 2010, p. 274). For displaced families, this silence is amplified by fractured support networks, making social connection not just beneficial but critical for mitigating trauma (Lasker & Toedter, 2000). Yet war disrupts the very relationships—kin, community, and cultural rituals—that traditionally buffer grief, leaving parents doubly vulnerable to the loss itself and to the absence of structures to process it.
Displacement severs access to origin-country networks that typically provide guidance and emotional support during reproductive transitions (Collins et al., 2011; Kingsbury et al., 2019). Research with Bhutanese refugees underscores how social ties directly improve maternal health by fostering practical advice and emotional resilience (Kingsbury et al., 2019), a finding especially relevant for pregnancy loss, where isolation heightens risks of depression (Dennis et al., 2017). However, no studies have examined whether these supports similarly protect displaced parents after pregnancy loss, nor how fathers engage with (or are excluded from) such networks.
Extending evidence linking social support to maternal wellbeing, we argue that targeted support mechanisms could mitigate pregnancy loss trauma for both genders in displacement. Our study is the first to explore how formal and informal supports—or their absence—interact with war-related adversities to shape parents’ coping strategies in displacement contexts.
Methodology
This paper reports findings from a research study that explored the pregnancy loss experiences of Syrian refugee families in Lebanon. The goals of the research included: (1) to describe the psychosocial impacts of pregnancy loss from mothers’ and fathers’ perspectives; and (2) to identify formal and informal supports that ameliorate or exacerbate the negative impacts of pregnancy loss.
The research took a qualitative approach, which allows for a rich exploration of the research participants’ lives (Chamberlain, 1999). Qualitative research is particularly effective for examining personally distressing issues that require greater sensitivity than is possible with just quantitative methods, which is especially important in the context of pregnancy loss (Rowlands & Lee, 2010). The research used interpretive phenomenological analysis (IPA), which produces data that will offer insight into the meanings that participants give to phenomenon, such as a major life event (Smith et al., 2009). IPA is especially useful for understanding under-examining phenomena or novel phenomena or that which is difficult to explain. It is therefore well-suited for research on pregnancy loss in the context of war. A phenomenological approach has been used in previous qualitative research on pregnancy loss in the Global North (see, for example, Adolfsson et al., 2004; Bansen & Stevens, 1992; Campbell-Jackson et al., 2014; O’Leary, 2005).
The research received human subjects’ approval from the Wilfrid Laurier University Research Ethics Board (REB #6390). Couples were first recruited to participate in the research by international and community-based organizations working with Syrian families who were living displaced in the Bekaa Valley. Some couples were beneficiaries of the international and community-based organizations, while others volunteered to participate through word-of-mouth. Regardless of their engagement with these organizations, couples were assured that their participation (or non-participation) would have no impact on the services that they received from these organizations.
The mothers who participated in the CFI were between 17 and 34 years old (M = 24.8 years old); fathers were between 21 and 42 years old (mean 29.9 years old). CFI-participating families had between zero and four living children at the time of the interview, with a mean of 2.28 living children. These families had experienced between one and seven losses at the time of the interview, with a mean of 2.21 losses. See Table 1 for the description of the sample. The mean number of losses (2.21) reflects cumulative experiences within a high-risk cohort (war-affected refugees facing compounded stressors), not incidence rates. External benchmarks for recurrent loss in similar contexts are scarce, as global data seldom disaggregate by displacement status or trauma exposure. Thus, while the sample’s frequency aligns with qualitative studies highlighting layered adversities in refugee populations, generalizability to broader norms is limited by design.
Family Description.
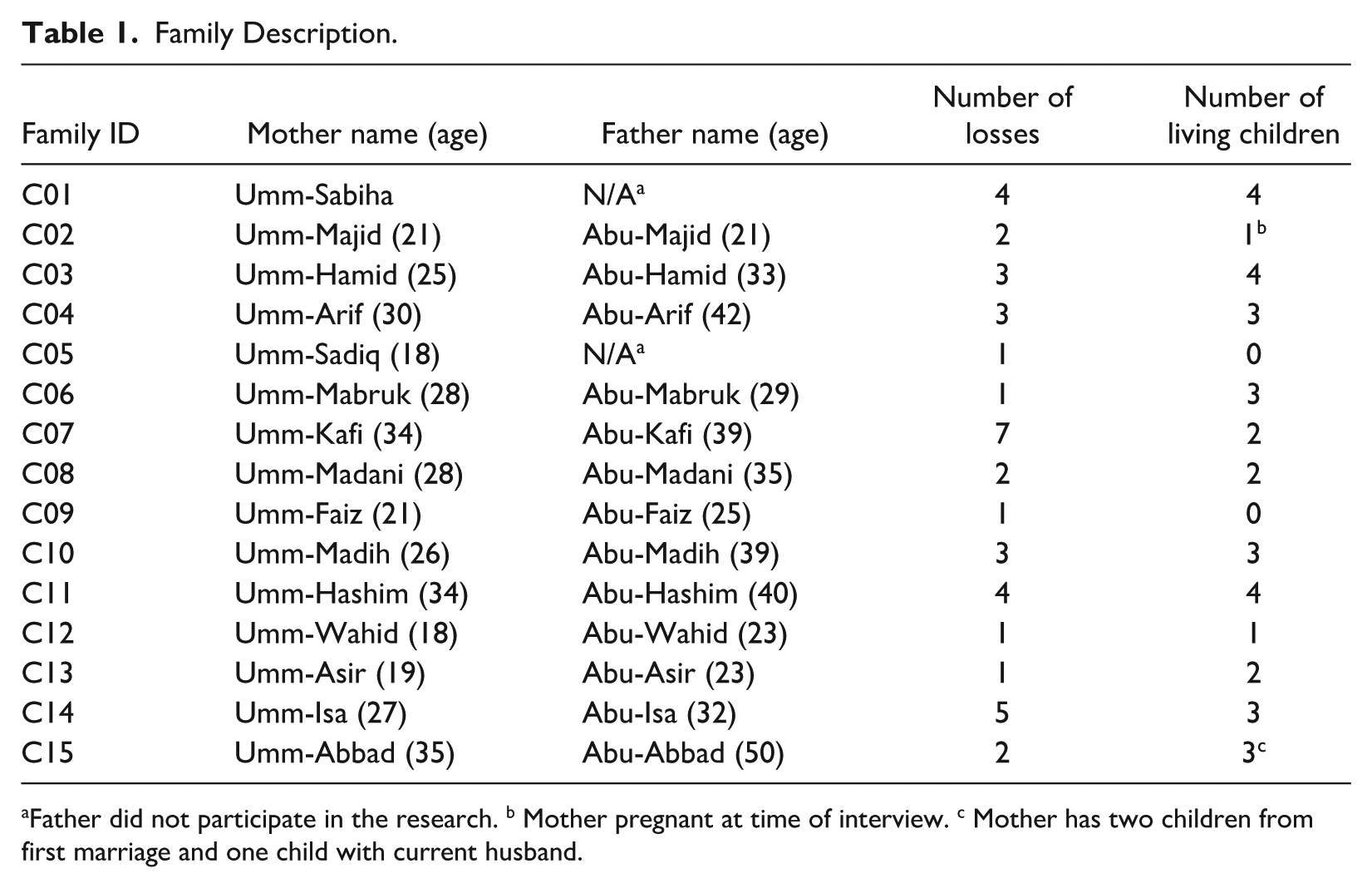
Father did not participate in the research. b Mother pregnant at time of interview. c Mother has two children from first marriage and one child with current husband.
The main data gathering method was the collaborative family interview (CFI) with mother-father dyads, which has previously been used successfully with war-affected and displaced families (Akesson & Frensch, 2024). Verbal and written consent was documented prior to beginning the CFI. At the beginning of each approximately 60-minute CFI, the research team gathered demographic data about the family (e.g., age, employment, education). CFIs were semi-structured in format, allowing time for the couple to co-construct their shared experience of loss, how they coped with loss, and what social supports were or were not available to them. The collaborative approach of the interview resulted in a reflexive and rich family narrative, with both mother and father ultimately adding a different element to their current experience living in Lebanon and collective memory of loss. CFIs were conducted with 15 families (15 mothers and 13 fathers). Two of the fathers declined to participate at the start of the CFI process; rather than canceling the CFI, the research team proceeded with the interview as the mothers both expressed a desire to share their story with the research team.
CFIs were followed by individual interviews with the mother and father participants. Aligned with cultural norms, participants were interviewed with a research assistant of the same gender. These 60-minute interviews provided the participants with an additional opportunity to expand upon what they had already shared in the CFI or share something new with the research team. In conjunction with the CFI, the individual interviews provided space for participants who may not have had the opportunity or were not comfortable sharing certain information during the CFI.
In addition to the CFIs and individual interviews, the research team conducted two peer group discussions (PGDs)—one for eight mothers and one for seven fathers—led by a research assistant of the same gender. All peer group discussion participants had experienced loss, which was a requirement to participate. See Table 2 for a sample of questions that guided the CFIs and PGDs.
.Sample of Open-Ended Interview Questions With Families and Health Practitioners.
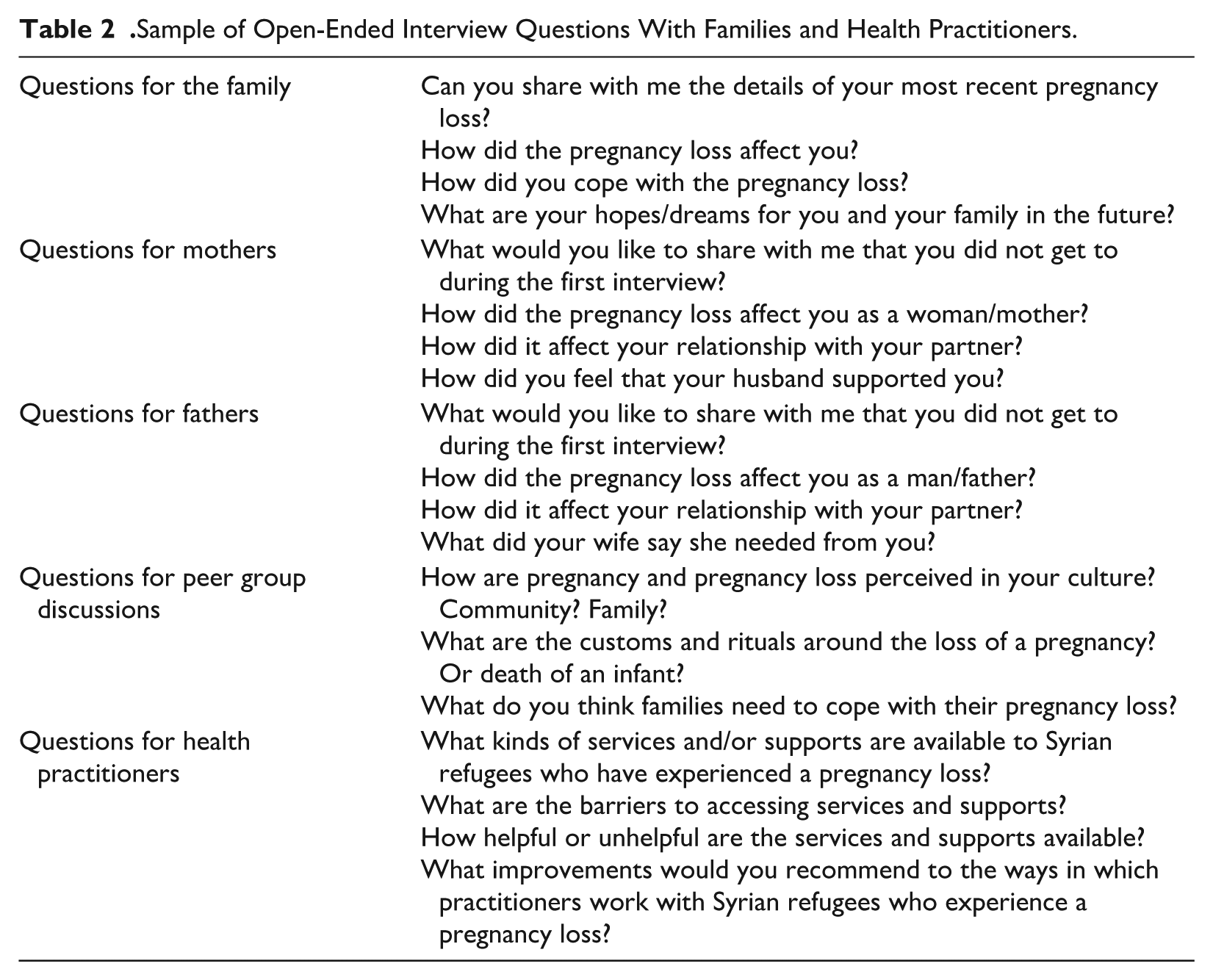
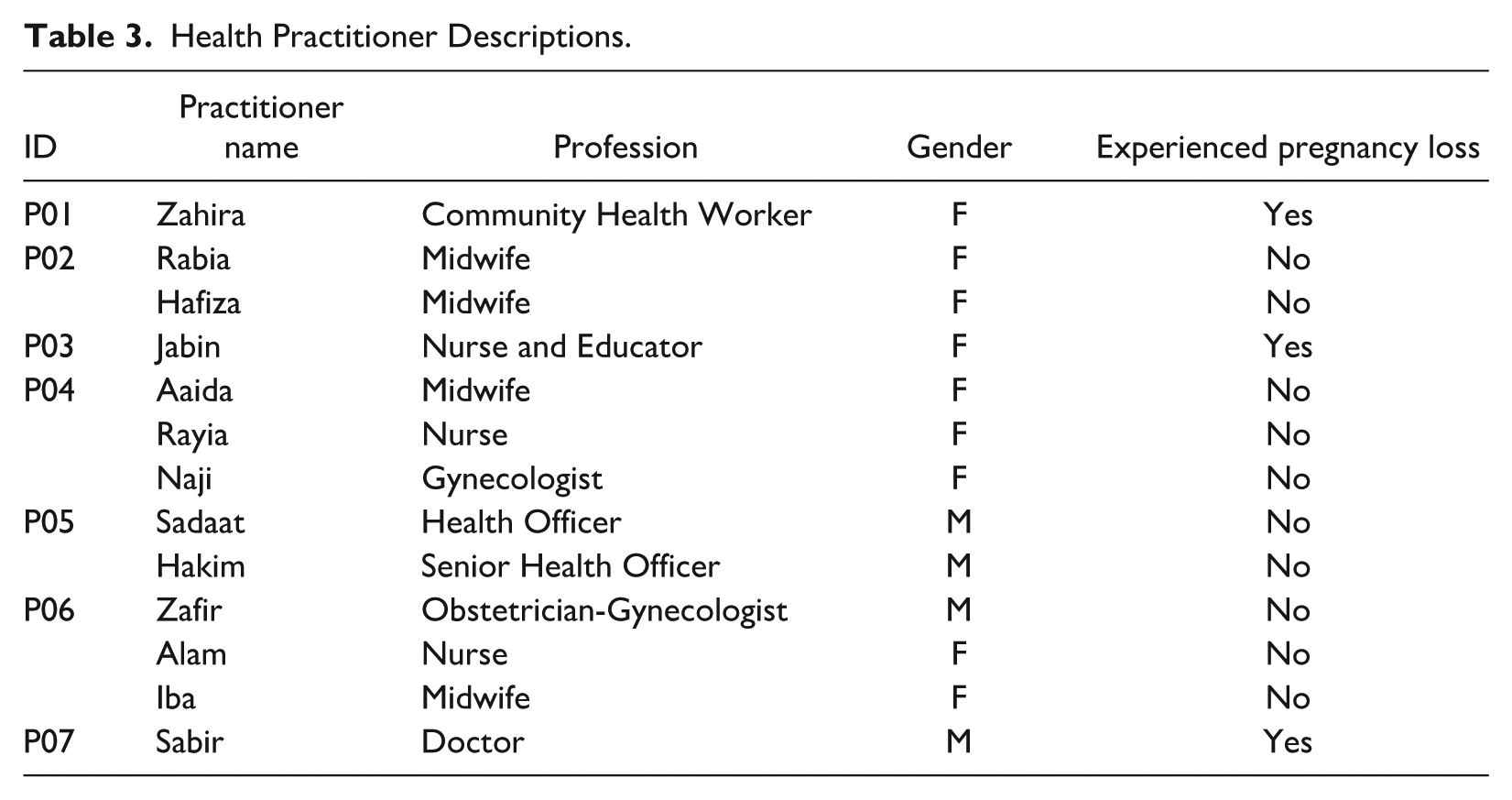
Finally, the research team interviewed 13 health practitioners (nine female and five male) including midwives, obstetricians, psychologists, nurses, social workers, and lactation specialists working directly with pregnant Syrian refugee women and their families in Lebanon. These health practitioners were invited to participate in either one-on-one interview or a joint interview with colleagues. Ultimately, three individual and four joint interviews (with 10 practitioners) with a total of 13 health practitioners were conducted. The addition of these voices helped to paint a more nuanced picture of the state of perinatal care for Syrian families in Lebanon. Furthermore, three of the health practitioner participants had reported their own pregnancy losses. Table 3 below provides more details about the health practitioners interviewed in this study. See Table 2 for a sample of the open-ended questions used in the health practitioner interviews.
Health Practitioner Descriptions.
All family and practitioner interviews (except for P3, which was conducted in English by the first author) were conducted in Arabic by Arabic-speaking research team members who had extensive experience working with the Syrian refugee community in Lebanon. With the permission of participants, interviews were recorded, transcribed, and translated into English. To ensure quality, the audio recordings and translated transcripts were checked by an Arabic speaker who did not conduct the interviews. All participants—parents and practitioners—were given pseudonyms for the sharing of research results.
The stories of the couples who participated in the CFI process were converted into family vignettes, or summaries of the family history and experience with loss. These vignettes ensured that the unique stories of the families were not lost in aggregate analysis. Furthermore, the vignette served to honor and respect what the couples went through and what they shared with the research team.
For data analysis, we conducted an interpretive phenomenological analysis (IPA) of the data to uncover insights into the meanings that participants gave to the specific phenomenon of pregnancy loss (Smith et al., 2009). To begin our data analysis, we held a series of discussion meetings with research team members, student research assistants, and key representatives from community-based organizations who helped with recruitment. These discussions were based on team members reading the three interviews (one CFI and two individual interviews) for a family and then sharing their observations of the content, including participants’ articulated thoughts, feelings, and reflections on their experience of pregnancy loss and the services and supports they did or did not receive.
Group notes taken during these discussions informed the thematic coding structure that emerged from the data and was used to subsequently code all the qualitative interview and peer group discussion data. Codes were organized thematically under the broad categories of supports (e.g., types of formal and informal support, barriers to support), attitudes (e.g., toward pregnancy loss, gender roles, seeking mental health services), psychological impacts (e.g., emotional impacts, coping, impacts on relationships), and recommendations (e.g., reflections on helpful and unhelpful practices).
We utilized Dedoose (www.dedoose.com), a qualitative research data software program, to apply codes to interview transcript content. Three graduate level research assistants (from psychology, social work, and international affairs) coded the data under the supervision of the first and second authors. The coded content was then analyzed in aggregate to highlight the most salient issues and experiences. This paper focuses on themes related to motivations and barriers to formal and informal supports.
Findings and Discussion
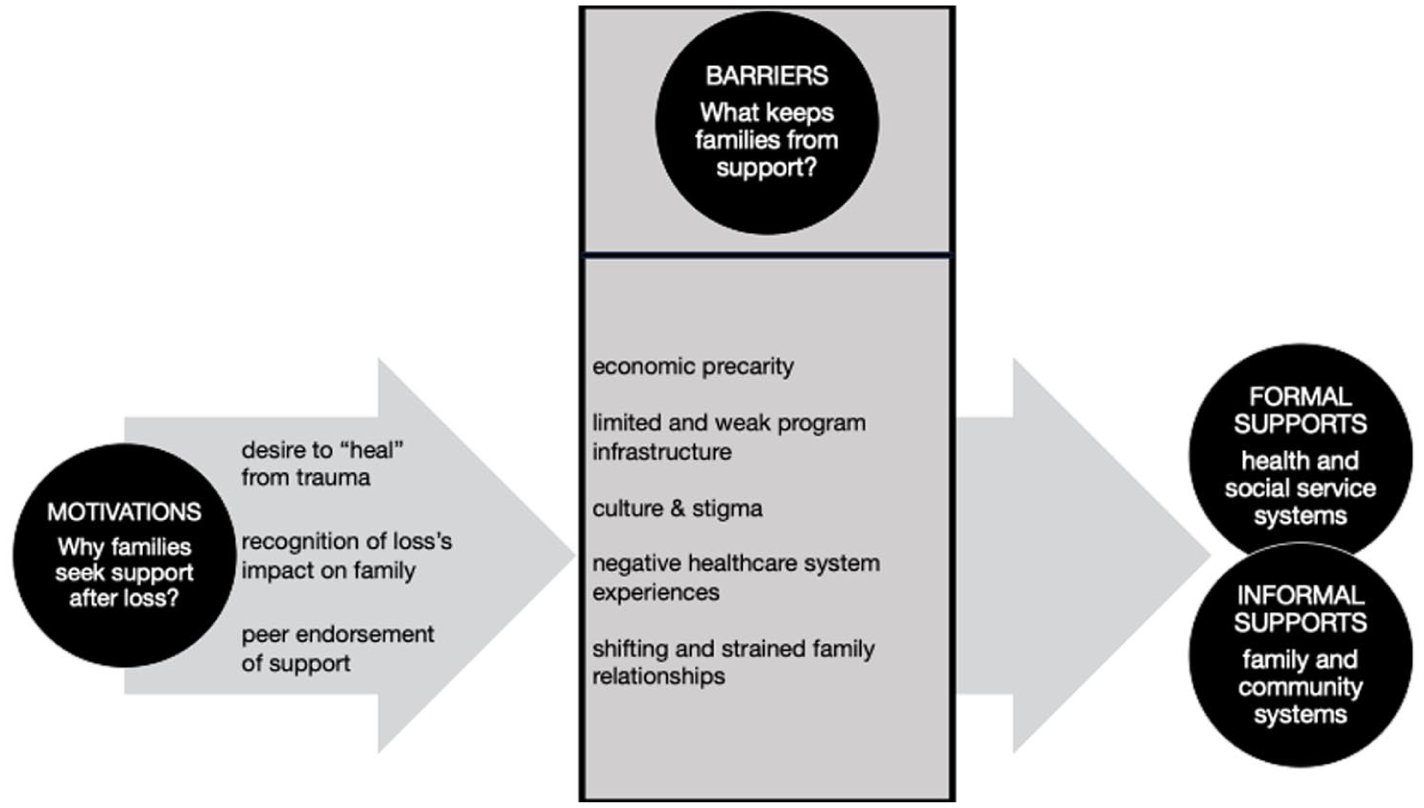
The findings were organized into two broad participant-driven categories: (a) motivations to seek support and (b) barriers to access support (see Figure 1). While families did not explicitly distinguish between formal and informal supports in their interviews, we introduced this distinction during analysis to bridge their experiences with actionable practice and policy recommendations. We present formal supports (e.g., clinician-led counseling, structured support groups) and informal supports (e.g., family/community networks) as complementary spheres in Figure 1, reflecting how both types of mechanisms emerged organically in families’ stories—even if not labeled as such.
Motivations and Barriers to Supports
Motivations to Seek Support
Before exploring barriers to support, we must understand families’ motivations to seek support. By understanding why couples seek support, research can tailor interventions, encourage increased engagement, and reduce the barriers that keep families from accessing support. The data indicate three main reasons that families seek support: (a) desire to “heal” from trauma, (b) recognition of impact of loss on family, and (c) peer endorsement of support.
Desire to “Heal” From Trauma
First, families may seek support out of a desire to “heal” from the trauma of pregnancy loss. The understanding that mental health is connected to physical health was first noted by Lebanese doctor Sabir who explained: “. . .the individual might pass through trauma. The woman’s body might not be able to get pregnant again because of fear. And if she got pregnant again, she will stay in fear until she gives birth.” Medical professionals interviewed in this study recognized the mind-body connection inherent in pregnancy loss and subsequent pregnancies, which has been noted in the literature (Qu et al., 2017), and saw this as a motivating factor for women to seek support.
Recognition of Loss’s Impact on Family
Second, parents recognized the impact of pregnancy loss on other family members. Notably, one mother from the peer group discussion said, I had severe depression. I had to take medication. I went to a doctor. And I improved a lot. I used to get upset from anything and slept all day. I suffered a lot. My kids lost a lot of weight. I didn’t cook and didn’t do anything. So, this psychiatrist helped me a lot.
One loss can have dramatic reverberations throughout the family. If a caregiver is struggling, this has direct implications on the care she provides to others. This aligns with research that emphasizes the importance of responsive caregiving for the wellbeing of other family members, specifically children (Sousa et al., 2024). Therefore, this remains a motivating factor for some parents in our study to seek support.
Peer Endorsement of Support
Third, the data point to the importance of peers in encouraging others to seek support. One participant from the women’s peer group discussion who had accessed mental health support after her pregnancy loss explained, “At the beginning, I didn’t tell anyone. But when I realized an improvement, I started advising others.” In addition to showing more trust in a system that supports the mental health of women, this word-of-mouth endorsement from someone who has also experienced her own loss also illustrates the potential of transforming pain into a source of support for others.
Barriers to Access Support
Even when participants were motivated to seek support, they still encountered significant barriers. We identified five barriers to both formal and informal supports: (a) economic precarity, (b) limited and weak program infrastructure, (c) culture and stigma (d) negative health care system experiences, and (e) shifting and strained family relationships.
Economic Precarity
For families in our study, the pregnancy loss was yet another loss layered upon multiple losses occurring in a context of extreme adversity. The most pressing adversity was economic precarity, exacerbated by lack of legal status in Lebanon, which restricted access to stable employment, health care, and social protections. Economic precarity was not merely a backdrop but an active agent of suffering, constricting choices, amplifying grief, and forcing families to prioritize survival over healing. Economic precarity casts a perpetual shadow on Syrian refugee families’ lives in Lebanon (Akesson & Badawi, 2021), with 90% living below the poverty line and 45% having less than acceptable access to food (World Bank, 2024).
40-year-old Abu-Hashim, a father of four who had experienced four pregnancy losses, described a situation that was common for all the families in our study: We live day by day. There is no work here. You work to live, that’s it, day by day. The rents are expensive. Everything is expensive. It is more expensive now. Oil is expensive. Gas is expensive. Food is expensive. Rice is expensive. The sugar. Everything is more expensive now . . . . Some people are barely able to eat. You work? You eat. You don’t work? You don’t eat.
Abu-Hashim’s account underscores how scarcity dominates every decision—from food to shelter—leaving parents with no bandwidth to attend to their grief around pregnancy loss.
Nearly all families in our study described the desperate circumstances that they navigated on a daily basis. Though pregnancy loss was devastating, the relentless grind of poverty and the everyday loss of dignity diverted attention from seeking mental health support. Abu-Arif and his 30-year-old wife Umm-Arif, who had experienced three losses described their economic situation:
We can’t. We can’t. [Abu-Arif] is not working. The situation is hard . . . Every week we need [money] for water . . . We have to pay rent. I wish it was a proper house. Who doesn’t wish to live in a proper house? This is all affecting. I swear I sometimes sit and cry. I cry alone.
How are you paying the rent?
Now?
We haven’t paid rent for three months. Why? Just because I don’t have.
For Umm-Arif and Abu-Arif, the impossibility of securing basic needs rendered pregnancy loss a luxury to grieve. Economic precarity permeated all aspects of life, compounding grief with shame and powerlessness. Yet even if families could overcome economic precarity, they still faced another barrier: limited and weak program infrastructure.
Limited and Weak Program Infrastructure
The data highlight a glaring lack of formal programs providing pregnancy loss support. This dearth of formal pregnancy loss support services is not just in Lebanon or even in the Global South, but throughout the world (WHO, n.d.). Jabin, a health educator who had herself experienced one pregnancy loss described the range of services available to pregnant women: “We give awareness sessions for women in their homes. . .about mental health, pregnancy. . .about depression before and after giving birth, as well as diabetes and chronic diseases and stuff like this. We give sessions about all diseases.” Neither Jabin nor any other practitioner interviewed in this research described programming that specifically addressed pregnancy loss. Once a woman experiences a loss, her engagement with pregnancy-support services stops. And there is a complete absence of supports for fathers during the perinatal period.
With the lack of loss-specific services, many families sought support through auxiliary services such as general mental health or food provision programs. But poor program infrastructure led to gaps in care, with families often reporting that organizations would say they would visit but never show up. Umm-Sabiha, a mother of four who had experienced four losses, said: “They told me they will come and to give the address. I gave them the address and they didn’t come.” Similarly, 30-year-old Umm-Arif explained how “Institutions take our names and all the information, and they say, ‘We will call you tomorrow,’ but the organization never visits again.”
Families also noted a disconnect between their needs and the services provided by organizations. Consider this example from Abu-Arif: Institutions take our names and all the information, and they say, “We will call you tomorrow.” During the lockdown, we sat [for] one month and a half at home. Don’t kids want to eat? Guess what [the organization] gave us? Wet wipes! I [asked] the organization, “[Should] I wrap sandwiches with it?” They said, “That is what we have.” The sheikh of the mosque received two food boxes. [The sheikh] gave me half. Honestly! [The sheikh] took the oil, sugar, and tea and gave me the rice and spaghetti. I told him, “Thank you.” I told him, “Ya, Sheikh, they gave us tissues” What do I do with tissues? I wipe my tears? Or wrap a sandwich for my child.”
These systemic failures—broken promises, mismatched aid, and abrupt withdrawal of services—compound the trauma of pregnancy loss. The jarring disconnect between families’ needs (e.g., food or psychosocial counseling) and organizations’ responses (e.g., unfulfilled visits and wet wipes) erodes trust not only in specific programs but in the humanitarian system as a whole. For war-affected families already navigating layers of instability, this solidifies their losses as invisible.
Culture and Stigma
Even if there were formalized pregnancy loss services that existed for the families in this study, culture and stigma still would have contributed to being significant barriers to accessing such services. The following exchange among mothers during the peer group discussion illustrates this barrier:
Honestly, people will say you’re crazy if you visit a psychiatrist.
But we have this mentality.
Even if we have it, [there is] no need to tell anyone.
Yes, we have it. When you feel that you will start a debate, you just do not go.
This hesitation to seek support extends beyond formal mental health services, as cultural norms and stigma also discourage families from pursuing informal support through relatives or community networks. These findings align with broader research demonstrating how culture and stigma systematically hinder health-seeking behaviors among Syrian refugees (Bawadi et al., 2022). And research in Germany revealed that mental health self-stigma is prevalent among Syrian refugees, which can impede their willingness to seek mental health care (Bär et al., 2021). Combined with the dearth of pregnancy loss support programs for Syrian families in Lebanon (Frensch et al., 2024), culture and stigma present a significant barrier, making accessing and utilizing pregnancy loss services extremely rare.
Negative Health Care System Experiences
Some participants described positive interactions with the health care system, which helped them after experiencing a pregnancy loss. For example, 21-year-old Umm-Majid who had experienced two losses, described what “good” formal support from a medical professional looked like: I was afraid. But [the psychiatrist] used to tell me it’s okay I will get another baby, they used to tell me the same thing; it’s good that I lost them in an early stage and not later. She used to tell me even though we lived a lot of painful experiences in Syria we should be strong to overcome it and be next to the people we love. She used to tell me I should be stronger than this for my husband, because I love him. And she really helped me with going to the United Nations.”
What is notable about Umm-Majid’s description of formal support is the inclusion of not just mental health care from the psychiatrist, but also the emphasis on support networks (e.g., “the people we love”) and other resources that can assist Syrian families in Lebanon (e.g., the United Nations).
However, positive descriptions of the health care system were rare among the research participants. In fact, the data suggested that negative experiences with the health care system served as a common barrier for parents seeking formal support for pregnancy loss. Participating families provided a multitude of examples of their interactions with the formal health care system during their pregnancy loss that impacted their desire to seek further support. One mother from the peer group discussion explained, In my last loss, I was in pain and bleeding. The doctor told [my husband], “She is fine, return her back home.” He said, “This medicine is good, it will help you.” It did not help me.
35-year-old Abu-Madani, a father of two who had experienced two pregnancy losses, described another example where he lost trust in the medical system, an experience which was repeated throughout the interviews and in the peer group discussions: The first time, the doctor told us that [my wife] should be pregnant to know what the problem is. The second time, there was a fetus, but they still do not know. If they did not know, who is supposed to know? Me?
Throughout the interviews, the families were not necessarily describing substandard medical care. In fact, the care they received may have been in line with the standard of care that is considered acceptable and appropriate by the medical profession in Lebanon. However, while these medical professionals may have been providing the correct health services, they may have done so without a level of compassion that is most helpful when responding to pregnancy loss. In other words, the medical professionals may have been providing the only services they could offer within the standard of care, but these services were deficient at adequately supporting pregnancy loss. Overall, these experiences posed a barrier for families to seek further formal support (for example, from mental health professionals) following pregnancy loss.
Shifting and Strained Family Relationships
A unique feature of this research was the active engagement of fathers who were open and willing to speak about their own experiences of pregnancy loss. While there were many father participants who spoke about ways they supported their wives and their wives corroborated this information in their own interviews, there were also fathers who were not supportive. When asked, “What did you need most from your husband when you were experiencing the pregnancy loss?” 21-year-old mother of three Umm-Madih who had experienced three losses replied, Everything. To stay with me and support me. But we barely saw each other. It is nice to have someone who would hear you and speak to you. My husband and I are not like this. He doesn’t speak to me at all.
Whether Umm-Madih and her husband’s lack of communication has always been present or was a result of losses is not relevant. But the result is emotional isolation where they each may feel isolated in their grief, intensifying feelings of loneliness and sadness during an already vulnerable time. Open dialogue can foster emotional intimacy, which is important in the wake of any loss (Neimeyer & Sands, 2011; Stroebe et al., 2017). Without it, the bond between the mother and father may weaken, making it harder to support one another effectively. This can also lead to increased conflict, which may further alienate them from one another. While there is research on the impact of pregnancy loss on the marital relationship in Western contexts (see, for example, Gold et al., 2010; Kiełek-Rataj et al., 2020), there are none that tackle this topic among war-affected and displaced populations.
Some research participants—specifically mothers—described especially tense relationships with their in-laws. Umm-Sabiha described how her husband’s parents treated her in the wake of her fourth pregnancy loss: My in-laws hated me the most. They hated me because I rawahet (lost the baby). [They said,] “She didn’t give birth to the boy. She lost the boy.” . . . My father-in-law used to tell me, “I hope you die every time you trawhe [lose a baby].” He used to tell me things that hurts me. I only cried. I cried and cried. I felt that I was going to die, then I slept.
Abusive in-laws can significantly compound the emotional, psychological, and social challenges faced by mothers and fathers who have experienced pregnancy loss. In Umm-Sabiha’s example, her in-laws clearly elevated her psychological distress, amplified her grief, and increased her feelings of guilt and shame (Nur, 2014; Raj et al., 2011). Abuse from in-laws can increase marital strain and impede coping mechanisms and support-seeking behavior between the mother and father (Raj et al., 2011). In-laws may discourage or prevent mothers from accessing formal support, leaving them with few avenues to seek help. Umm-Sabiha’s harrowing experience highlights the profound impact that abusive in-laws can have on women’s wellbeing following pregnancy loss, emphasizing the needs for targeted interventions and psychosocial supports.
Another factor that contributes to shifting and strained family relationships is the physical separation from one’s family, which was quite common among the mothers in our study. Women are likely to be separated from their parents and natal families due to cultural norms and patriarchal dynamics that direct women to live with her husband’s family. This is exacerbated in the context of war and displacement when families may be separated due to distance, economic precarity, and borders. Participants described their parents and other natal family members—who have the potential to serve as a wellspring of support for women following loss—as not being available because they often remained in Syria. A participant in the women’s peer group noted: “Passing through all these experiences is so hard, especially that we are alone. We are alone in this country and without our parents.” Similarly, Umm-Sabiha described how her parents remained in Syria and were therefore not available to support her after her pregnancy loss: “My parents were far. My mom was in Syria. . . . No one visited me and I was tired.” Umm-Sabiha’s experience underscores the impact of not having extended family members available for support during pregnancy loss, which can be experienced as another layer of loss.
With the absence of supportive natal family members, mothers often turned to their husbands for support. Forty-year-old Abu-Hashim who had experienced four losses explained how he could best support his wife after their pregnancy loss: She wants me to talk to her, to comfort her. To feel that I am with her. Her parents and siblings are not with her. Who is her family. I am her family. She only has me. I should always talk to her. So as not to feel alone. I am the one who comforts her [saying] “Thank God for your safety, you are still young, tomorrow you can get pregnant again.”
Abu-Hashim described his role is to provide emotional support to his wife during this time. By talking to her and comforting her, he fulfilled her need for connections and companionship during a vulnerable time. This quote highlights the centrality of close family members as informal supports contributing to emotional care after pregnancy loss. Abu-Hashem recognized that he must address the absence of his wife’s family through the enhancement of his own support of his wife.
Conclusion
This paper examines the motivations and barriers for Syrian refugee families in Lebanon to seek support following pregnancy loss. Key motivations include a desire to heal from the trauma of loss, recognition of its impact on family wellbeing, and encouragement from peers who have accessed support. However, families face significant barriers such as economic precarity, weak program infrastructure, cultural stigma, negative health care experiences, and strained family relationships. Economic challenges, compounded by displacement and lack of legal status, often deprioritize mental health support in favor of basic survival needs. Moreover, formal support services specific to pregnancy loss are notably absent, and interactions with health care systems often lack the compassion required for such sensitive issues.
This research also highlights the social dimensions of pregnancy loss, particularly the strained dynamics within families. Mothers can face judgment or abuse from in-laws, further exacerbating their grief and isolation. Physical separation from natal families, a consequence of the intersection of patriarchal norms and mobility restrictions due to the Syrian conflict, deprives women of traditional support networks that they need in the wake of pregnancy loss. In such circumstances, husbands play a pivotal role in providing emotional support, although strained marital relationships may hinder this support.
Limitations
We recognize several limitations in this study. First, the research did not use any objective measures to document formal pregnancy loss services. It is therefore possible that families were unaware that there were services available or were unsure about how to access them, potentially skewing the understanding of support availability. We attempted to address this by expanding our definition of supports to include both formal and informal mechanisms. Second, there may have been self-selection bias as the mothers and fathers who agreed to participate in the research were also comfortable sharing their experiences with pregnancy loss. This may have excluded families who may have been struggling more intensely in the aftermath of their loss. Third, while the study intentionally created space for fathers to share their emotional experiences of pregnancy loss, their narratives often centered on survival struggles (e.g., economic precarity) rather than explicit discussions of grief. This reflects both cultural constraints—where men’s vulnerability is stigmatized—and methodological challenges inherent in researching fathers’ bereavement in patriarchal contexts. Notably, our ability to engage fathers at all on this topic is significant given the near-absence of prior pregnancy loss research with refugee men. In fact, during the study design, we were uncertain whether fathers would participate at all. However, the relative scarcity of direct emotional disclosures underscores the need for future studies to employ targeted strategies to better access men’s inner experiences while respecting cultural norms.
Implications for Practice and Policy
The research findings point to areas of structural change that can be reinforced through effective practices and policies for war-affected families who have experienced pregnancy loss. First, practitioners and policymakers should consider that losses layer upon each other akin to the triple trauma paradigm. Families are not just struggling with trauma related to war and displacement or even the acute crisis of the pregnancy loss. Rather, there may be other challenges—such as poverty, food insecurity, lack of opportunities for education and livelihoods, etc.—representing layers of loss. These layers of loss often manifest as complex grief (Jones, 2020), where unresolved trauma from displacement compounds the psychosocial impacts of pregnancy loss. As Hall (2014) notes, bereavement in contexts of instability often defies linear recovery models, requiring interventions that address both immediate and systemic approaches. Practitioners and policymakers should look towards solutions that can minimize these layers of loss for families. For example, considering a family’s precarious legal status and strained financial situation should lead to formal mental health support that is logistically and financially accessible.
Second, normalizing pregnancy loss as part of perinatal discourse is critical to addressing the layered trauma of displacement, war, and grief outlined in the triple trauma paradigm. Given the silencing effects of stigma—which emerged as a key barrier to support in our study—integrating discussions of loss into routine family planning, perinatal services, and community awareness sessions can help reframe it as a shared, albeit painful, human experience. The “silent environment” surrounding pregnancy loss may prolong grief responses (Nickerson et al., 2014) particularly when cultural stigma prevents open mourning. Normalizing loss through community dialogue could mitigate this risk by creating spaces for shared meaning-making (Hall, 2014). Furthermore, training for medical professionals should emphasize compassionate, culturally-attuned communication to validate grief and counteract shame for both women and men. By dismantling the “silent environment” surrounding pregnancy loss, interventions can mitigate isolation and align with the broader need to address cumulative trauma in war-affected communities.
Third, practices and policies addressing pregnancy loss must actively include support for men, whose grief is often overlooked yet shapes family dynamics. For fathers, grief may compound preexisting stressors like unemployment or displacement while cultural norms of masculine stoicism simultaneously restrict their avenues for emotional expression of help-seeking. In patriarchal contexts where reproductive health is considered a feminine domain, men face structural barriers to involvement such as exclusion from clinical spaces and stigma for displaying vulnerability. While fathers in our study sometimes sought support to better assist their partners (e.g., Abu-Hashim’s efforts to comfort his wife, “so as not to feel alone”), others alluded to unmet emotional needs, reflecting a tension between cultural expectations of stoicism and their private distress. Gendered divisions of emotional labor and fear of stigmatization can paralyze men’s capacity to engage authentically. Yet as one health officer noted, “As long as you convince the man, things will work out,” a pragmatic acknowledgment of men’s gatekeeper role that also highlights how engaging men can facilitate family access to care. However, framing support for men solely as a means to benefit mothers risks perpetuating their invisibility in grief. Tailored interventions—such as peer groups for fathers or culturally-attuned counseling—should address men’s unique psychosocial needs while simultaneously reducing shame that has the potential to silence. Potential interventions could include reframing emotional support as a form of resilience against masculine ideals and collaborating with community and religious leaders to legitimize men’s participation in perinatal loss. By acknowledging men as both caregivers and grievers, practice and policy can disrupt the stigma surrounding pregnancy loss.
Fourth, the data pointed to the critical role that in-laws have in family life, especially impacting the mother. Practice and policy should broaden conceptualizations of family violence to include in-law abuse, thereby underscoring the profound impact that abusive in-laws can have on women’s wellbeing following pregnancy loss. This broader understanding of the circumstances of war-affected families following loss emphasizes a need for sensitive and supportive interventions and resources.
Finally, the families in this study demonstrated a level of generosity and openness by opening their homes to our research team to share their stories of pregnancy loss. Therefore, we believe that families in this situation would benefit from being involved in initiatives where they could share their stories through psychosocial support groups, community gatherings, or culturo-religious rituals. Shared storytelling in supportive environments may help reconstruct fractured narratives of loss (Hall, 2014) particularly for refugees whose grief is compounded by multiple traumatic separations (Jones, 2020). This is a way by which mothers, fathers, and families can feel heard and supported, or to again reiterate the words of Abu-Hashim, “so as not to feel alone.”
Implications for Future Research
This study is the first of its kind to explore the psychosocial implications of pregnancy loss among war-affected populations thereby opening the door to future threads of research on this topic including: the impact of pregnancy loss on parenting style with a focus on how parents engage with existing or subsequent children; the role of religion, religious leaders, and culturo-religious practices that can both ameliorate and/or hinder grief and recovery related to pregnancy loss; and host community experiences accessing pregnancy loss support services.
Footnotes
Disposition editor:
Cristina Mogro-Wilson
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by funding from the Social Sciences and Humanities Council of Canada (Grant No. 00812) and the Research Support Fund at Wilfrid Laurier University.