
Abstract
In Kyrgyzstan, registered HIV cases doubled from 2013 to 2019, with women constituting 39% of cases in 2021. Women living with HIV (WLHIV) encounter heightened intimate partner violence, stigma, and discrimination. This study explores the experiences and vulnerabilities of WLHIV in Kyrgyzstan from the perspective of professionals engaged in HIV care and advocacy. Data from in-depth, semi-structured interviews with 10 professionals engaged in HIV prevention were analyzed using grounded theory methods. The analysis revealed two primary categories related to the experiences of WLHIV as observed by professionals in the field: (a) Challenges faced by WLHIV at the personal, interpersonal, community, and institutional levels, and (b) The way forward—providers’ ideas about addressing stigma and vulnerability. Urgent action is needed to address the needs of WLHIV, emphasizing confidentiality and support, recognizing discrimination as violence, and fostering financial independence.
Introduction
While HIV incidence and prevalence are declining globally (UNAIDS, 2024), HIV prevalence in Central Asia and Eastern Europe doubled from 2010 to 2019 (Nikoloski et al., 2023; UNAIDS, 2018, 2022, 2023). The populations in this region most likely to be affected are people who inject drugs, sex workers, men who have sex with men, prisoners, young people, and migrants (Ancker & Rechel, 2015). The number of overall registered HIV cases in Kyrgyzstan doubled from 2013 to 2019, and the number of women diagnosed during this time increased as well (UNDP, 2023). Women accounted for 39% of the total number of people living with HIV(PLHIV) in 2021 compared to 28.7% in 2010 in Kyrgyzstan (UNAIDS, 2023). Despite a relatively higher level of political commitment to addressing HIV/AIDS compared to neighboring countries, Kyrgyzstan faces challenges in translating this commitment into action due to limited state resources (Ancker et al., 2013). As a result, the country heavily relies on international donors for support (Ancker & Rechel, 2015).
The increase in HIV incidences in certain regions, such as Kyrgyzstan, can be partly attributed to migration patterns. Out-migration is common in Kyrgyzstan and about a third of the national GDP comes from remittances sent by migrants (Oakes et al., 2020; World Bank, 2022). Many individuals migrate to countries with higher HIV prevalence, such as Russia, for work opportunities, and upon returning, they may unknowingly bring back the virus to their home communities. An estimated population of 700,000 migrants or 15% of the Kyrgyz population work in Russia and send back remittances that keep the economy afloat (Ruget & Usmanalieva, 2021; UNDP, 2015), with men making up 69% of the migrants to Russia (Rocheva & Varshaver, 2017). The Russian Federation is the main destination for Kyrgyz migrant workers with 83% of all migrants going there (Denisenko & Chudinovskikh, 2012). Russia has one of the highest incidences of HIV in the world with nine million documented cases of HIV infection reported in 2015 (Nikoloski et al., 2023; Pokrovskiy et al., 2015). Labor migrants who contract HIV abroad can potentially expose their spouses to the disease upon their return (Hernández-Rosete et al., 2008). This migration-driven transmission poses a significant challenge in HIV prevention efforts, especially among vulnerable groups like labor migrants who often lack adequate HIV knowledge and perception of risks (UNAIDS, 2023).
HIV stigma, and specifically health care workers’ stigmatizing attitudes toward PLHIV, is recognized as a major barrier to efforts to end the HIV epidemic (Bayat et al., 2020; Katz et al., 2013; Kutner et al., 2023; Logie & Gadalla, 2009; Rueda et al., 2016; Sullivan et al., 2020). Research suggests HIV-related stigma in the community contributes to internalized stigma among PLHIV who then anticipate stigmatizing experiences, and this anticipation results in adverse health and psychosocial outcomes (Turan et al., 2017). Several meta-analyses and systematic reviews show the harmful impacts of stigma on PLHIV including increased symptoms of poor mental health, substance use, and decreased ART adherence (Bayat et al., 2020; Katz et al., 2013; Kutner et al., 2023; Logie & Gadalla, 2009; Rueda et al., 2016). Furthermore, a systematic review of the psychological and social impact of HIV on women living with HIV (WLHIV) and their families in low- and middle-income Asian countries demonstrated that HIV, among other factors, contributed to stress, fear, worry, anxiety, and depression (Fauk et al., 2022). Several studies from Eastern Europe show the deleterious impact of HIV stigma on treatment, but few have focused exclusively on the experiences of WLHIV (Calabrese et al., 2016; Hook et al., 2023; Owczarzak et al., 2023) and fewer have examined HIV stigma in Central Asia (Primbetova et al., 2023).
While our current analysis focuses on provider-level HIV stigma, WLHIV also experience elevated levels of gender-based violence (GBV) often rooted in HIV stigma (Campbell et al., 2008; Gielen et al., 2000; Leddy et al., 2019; Y. Li et al., 2014). UN Women (Hale & Vazquez, 2011) defined violence against WLHIV as “any act, structure, or process in which power is exerted in such a way as to cause physical, sexual, psychological, financial, or legal harm to WLHIV” (p. 13). This increased likelihood of violence may prevent WLHIV from seeking help and receiving necessary health care (Leddy et al., 2019; Lichtenstein, 2005). Thus, PLHIV may be subjected to community-level and provider-level discrimination.
WLHIV are also disproportionately affected by intimate partner violence (IPV; Shi et al., 2013). In a study by Orza et al. (2015), which examined 832 WLHIV from 94 countries, the prevalence of IPV emerged as a concerning issue, particularly escalating after the disclosure of HIV status. This finding aligns with prior research conducted in various regions, such as South Africa (Bernstein et al., 2016), Kenya (Colombini et al., 2016), and Ethiopia (Meskele et al., 2021), which also uncovered significant instances of psychological abuse experienced by WLHIV. Moreover, a study conducted in Iran (Oskouie et al., 2017) revealed that HIV-related stigma led to self-discrimination stemming from internalized shame, and a preference for seeking treatment in facilities away from home.
There is little research that explores the experiences of WLHIV in Kyrgyzstan and the vulnerabilities they face from the perspective of professionals engaged in HIV care and advocacy. This research helps to address this gap. An experienced service provider can be a storehouse of information related to HIV because they deal with such cases on a daily basis as part of their profession. Not only do they witness the multifaceted nature of HIV spread and stigma, but they also chronicle the cases through analytical lenses over the years. The professionals selected were from diverse backgrounds to ensure every major sector that works with WLHIV is represented in the study. The diversity of professionals and service providers covers a wider base of perceptions on challenges faced by WLHIV in Kyrgyzstan and helps identify potential areas for improvement in service delivery and advocacy efforts.
Using grounded theory qualitative research methods, we aim to uncover the unique challenges and vulnerabilities encountered by WLHIV. The study is informed by Heise’s (1998) ecological model of violence which provides a comprehensive framework for understanding violence, considering personal, situational, and sociocultural factors. This model allows us to gain insights into how society treats WLHIV due to their HIV-positive status.
Method
The method of this study is informed by grounded theory methods for their adaptability and accessibility in research application, as explained by McCall and Edwards (2021). The core tenet of grounded theory is the conceptualization of social phenomena through inductive, systematic, and comparative approaches grounded in participant experience (McCall & Edwards, 2021). Grounded theory lacks universally accepted definitions and guidelines, with theorists holding varied opinions on blending traditions and selectively adopting components (Apramian et al., 2017).
Researchers determine which type of grounded theory approach to implement based on their research process, the data collected, their role, and the overarching purpose of their work. Due to this heterogeneity of grounded theory traditions and components, it has been proposed to distinguish between grounded theory methodologies which reflect specific worldviews and traditions, sometimes denoted through capitalizations like Grounded Theory Methodology (or big GT), and grounded theory methods (little gt), which refers to data collection and analysis procedures which are chosen and implemented within a larger research design, and can be denoted as “little gt” (McCall & Edwards, 2021, p. 99).
Grounded theory methods can produce conceptualizations informed by existing theories, offering valuable descriptive and explanatory models without necessarily leading to novel theory development. This approach may be beneficial for fields like social work and public health by broadening inclusion and allowing for cultural nuances (such as changing demographics and evolving social norms), which deepen the scope of existing theories (Charmaz, 2014). This approach allows researchers to adapt grounded theory methods to their specific study goals, with multiple potential results: extending or modifying existing theories, generating new or context-specific theories, or arriving at nontheoretical descriptive outcomes. By clearly defining their use of grounded theory methods and articulating their research designs and outcomes, researchers can effectively contribute to their fields without either overextending or underestimating resulting claims of theory development. By focusing on research aims and allowing data to guide inquiry, researchers can uncover meaningful findings with a variety of theoretical implications.
Sample and Data Collection
The data are drawn from semi-structured interviews with a subsample of 10 professionals, who were part of a larger study that included 83 professionals in the education, social services, and health sectors (see Table 1). The selection of informants followed the principles of theoretical sampling (Glaser & Strauss, 1967). The initial criteria for selecting the purposive sample of the participants included (a) being at least 18 years of age, (b) having a minimum of one year of experience in their current paid role in advocacy, direct client service, or agency leadership, (c) being able to provide informed consent, and (d) being proficient in either Russian or Kyrgyz language.
Participant Characteristics (N = 83).
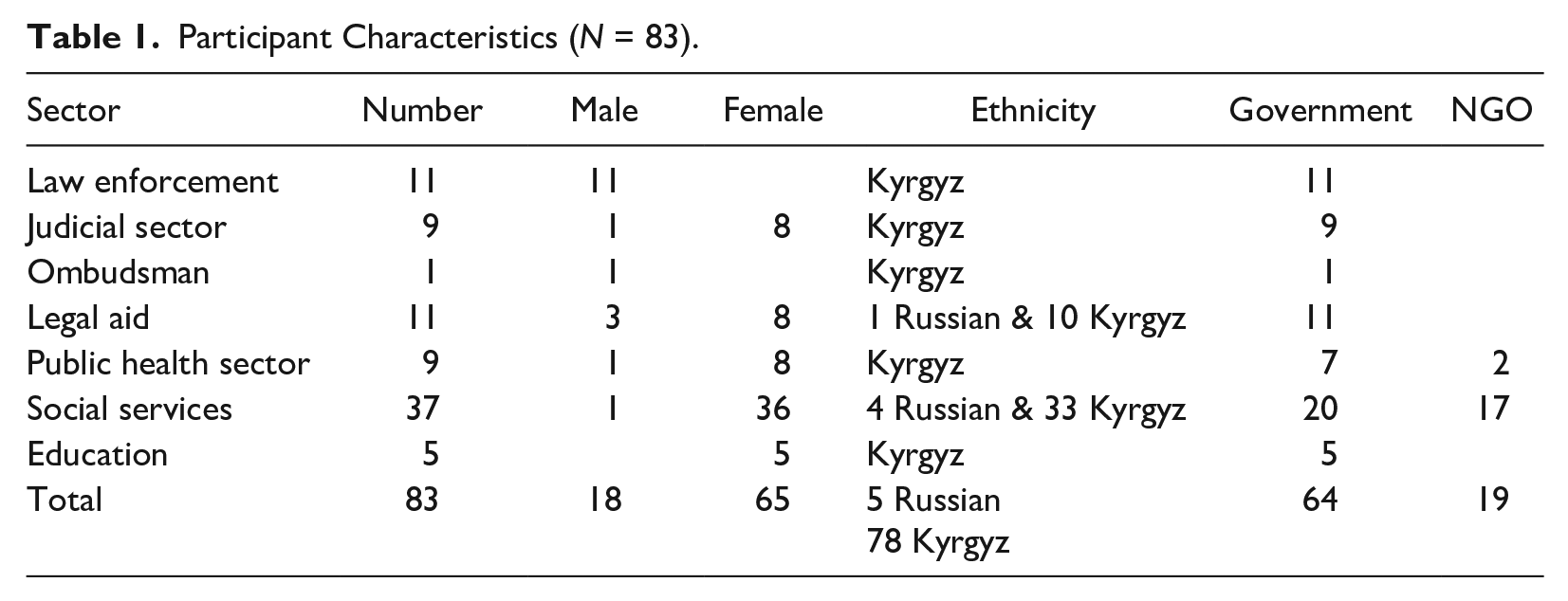
The initial selection of participants focused on professionals engaged in addressing GBV. Participants described their job tasks as including survivor advocacy, shelter services, legal and counseling services, prevention education, and agency leadership. Most participants identified as female, and the length of time in their professional role ranged from one to more than 20 years. As interviews progressed, professionals possessing expertise pertinent to the emerging research areas were identified through referrals and consultations with field experts. With partnerships from national GBV and HIV advocacy agencies, as well as their regional partners, participants were recruited to participate in semi-structured interviews to explore the intersection of HIV and GBV issues, including (a) risk factors and characteristics of violence after HIV-positive status revelation, (b) major challenges faced by WLHIV, (c) coping and help-seeking mechanisms, and (d) recommendations for best practices for addressing these challenges.
The interviewing process was informed by Kvale’s (2007) seven stages of an interview inquiry, including thematizing, designing, interviewing, transcribing, analyzing, verifying, and reporting. A total of 10 participants were interviewed, which is consistent with the qualitative research approach aimed at the depth of understanding rather than generalizability. Data saturation, the point at which “no new information emerges during coding” (Oktay, 2014, p. 81) and “no new properties of the pattern emerge” (Glaser, 2001 as cited in Charmaz, 2006, p. 113), or the point of reaching “diminished returns from the data collection efforts” (Maykut & Morehouse, 1994, p. 62), was determined through ongoing analysis and discussion among the research team, which acted as a system of checks and balances, providing diverse viewpoints, and opportunities for iterative analysis. “Theoretical sufficiency” (Dey, 1999, p. 257) or saturation was also informed by the “Cultural Consensus Model” developed in ethnographic work (Guest et al., 2006; Romney et al., 1986), coherence of the theoretical similarities accumulated within categories (Mason, 2010), and the quality and the depth of the information (Morse, 1995, 2008).
Procedure
The interviews were conducted face-to-face in private settings to facilitate rapport and ensure nonverbal cues were captured. Interviews lasted about an hour and were conducted one-on-one between the primary researcher and the participant to create a comfortable and confidential environment. The researcher did not have any pre-existing relationships with the participants prior to the interviews. The researcher established rapport and provided a clear explanation of the research objectives and the voluntary nature of participation during the recruitment process. All participants provided verbal consent and permission for audio recording prior to the beginning of data collection.
The primary researcher identifies as a cisgender female, has extensive experience in qualitative interviewing, and holds a PhD in social work with expertise in GBV prevention among former Soviet Union populations. She also brings significant experience as a development worker and social work researcher with vulnerable groups, particularly those with trauma, violence, and adverse childhood experiences in protracted conflict settings. This work builds on her prior experiences working on social development projects in Central Asia and on a network of collaboration and partnerships in the region. She remains thoughtful in navigating how her own insider (as a Central Asian woman) and outsider (as a North American academic) identities may be perceived and received by the people she engages with and how these might influence the research processes and results.
The interviews were conducted in Russian and Kyrgyz languages. A professional translator with a graduate degree in languages transcribed the recorded interviews verbatim and translated them into English. The study followed the protocol recommended by the World Health Organization (2001, 2013) for researching the challenges faced by WLHIV as narrated by people working at the grass-roots level with the affected women. To ensure the confidentiality of respondents, all identifying information was removed from transcripts and they have been given pseudonyms. The Institutional Review Board (IRB) approval was received from the first author’s University in the United States and the Ministry of Health of the Kyrgyz Republic.
No individuals declined to participate in the study. No follow-up interviews were conducted with the same participants, as the initial interviews yielded comprehensive data that adequately addressed the research topics. The interview guide was developed based on a thorough review of the literature and refined through consultation with experts in the field of GBV and social work. Prior to the study, the interview guide was piloted with two individuals to ensure clarity and relevance to the research objectives. During each interview, the primary researcher took notes to capture key points and observations. These field notes were used to supplement the audio recordings during data analysis.
Data Analysis
The coding team was composed of two researchers who were trained in grounded theory methods. Both coders independently conducted coding on all transcripts, ensuring comprehensive coverage and consistency in the coding process. Any discrepancies between coders’ interpretations were reconciled through discussions and consensus-building sessions. A detailed codebook was created using the Nvivo12 qualitative software program. Throughout the coding process, the researchers engaged in constant comparison, reflexivity, and memo writing to document their analytical decisions and insights.
These initial coding and analytic memoing techniques guided the sampling decisions and refinement of the interview guide. Open codes were generated through line-by-line coding to identify categories and patterns. Upon completing the open coding phase, the researchers used axial coding techniques (Oktay, 2014) to organize the codes into broader categories and subcategories. At the final selective coding stage, the researchers focused on refining and consolidating the core categories generated during the open and axial coding.
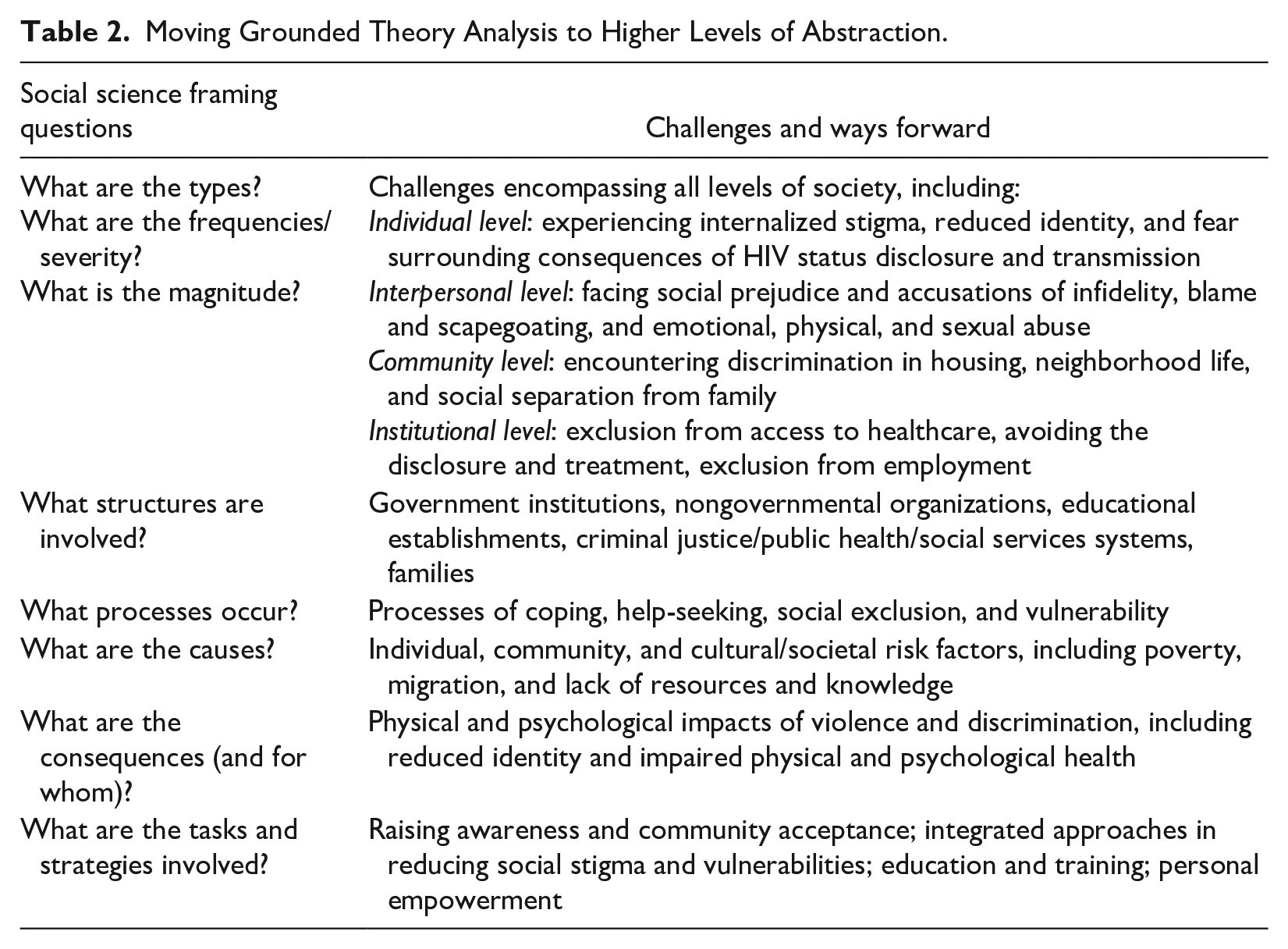
Following axial coding, the analysis progressed to meaning-making at a higher level of abstraction through a technique called “social science framing” (Lofland et al., 2006 as cited in Oktay, 2014, p. 79). This technique involves linking emerging categories to broader social science theory by continually asking eight basic questions (see Table 2). As a result of this iterative process, the researchers interrogated codes and categories and how they were related to theories of violence, specifically, the Integrated Ecological Framework of Violence Against Women (Heise, 1998). This process generated meaningful results at a higher level of abstraction which fit well with the theoretical conceptualizations of the ecological framework (see Figure 1).
Moving Grounded Theory Analysis to Higher Levels of Abstraction.
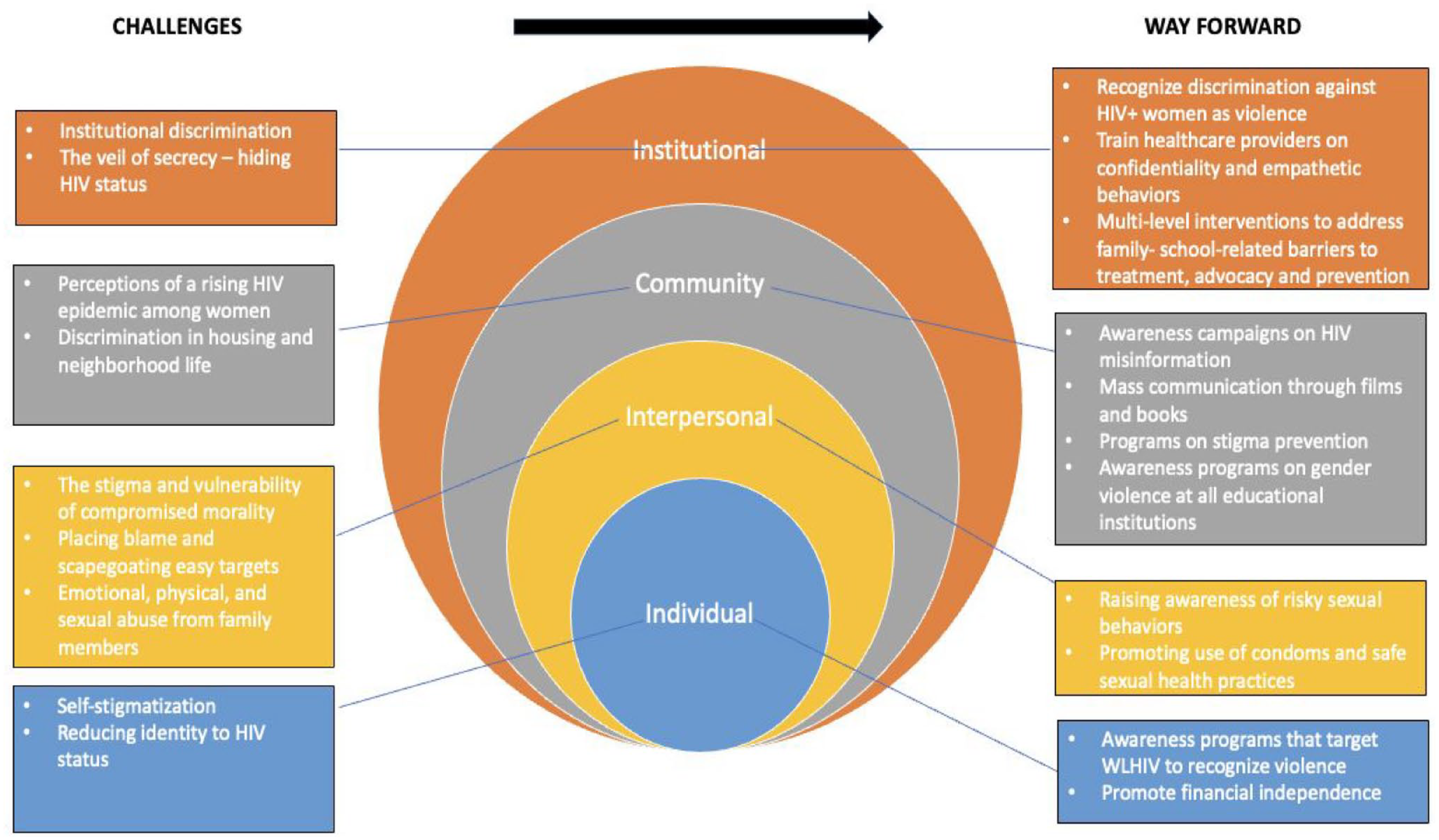
Socioecological Levels of HIV-Related Social Stigma and Vulnerability Among WLHIV.
To ensure the trustworthiness of the findings, investigator triangulation (using multiple coders; Denzin, 2017), prolonged engagement (spending multiple years in the research site building rapport and professional relationships; Lincoln & Guba, 1985), peer debriefing (Lincoln & Guba, 1985), audit-trail (Oktay, 2014), thick description (Geertz, 1973), and presentation of raw data were used to enhance the credibility steps. This study employed the “inquiry audit” technique, which stresses capturing the clarity of the process from data collection to interpretation and the warranty and internal coherence of the findings in relation to the data (Lincoln & Guba, 1985, p. 316). The computer-assisted analysis program provided a platform through which the raw data, the coding schemes, and the analysis memos were kept.
Findings
The data reflected two categories related to the experiences of WLHIV as observed by professionals in the field: (a) Challenges of stigma faced by WLHIV at the personal, interpersonal, community, and institutional level, and (b) The way forward—providers ’ ideas about addressing stigma and vulnerability. Within each category, a number of subcategories emerged illustrating the complexity of the challenges faced by WLHIV at different socioecological levels and providers’ recommendations about addressing them.
Category 1. The Challenges of Stigma Faced by WLHIV at the Personal, Interpersonal, Community, and Institutional Levels
WLHIV faced challenges and stigma from multiple sources that created immense psychological stress. The fear of being found out and being ostracized from every level of society, from neighbors to relatives to medical personnel, as well as the fear of character assassination and being labeled with the singular identity of “HIV infected,” generated a culture of secrecy and trauma among victims. The challenges faced by WLHIV violence can be organized using Heise’s (1998) ecological model examining vulnerabilities and stigma at individual, interpersonal, community, and institutional levels.
Subcategory 1.1. Individual-Level Challenges
Self-stigmatization
Interviewees reported that a WLHIV was vulnerable because of societal stigma, but they were also likely to engage in self-stigmatization and thus experienced both internal and enacted stigma. Jamal referenced this double stigma, noting that women with HIV “work on their self-stigmatization and additionally, on the enacted stigma coupled with different forms of violence.” Ulan, who is HIV-positive and is open about his status, also mentioned self-stigmatization when he discussed his work as an advocate for HIV-positive people. Ulan uses lessons learned in his earlier life as a drug user and prisoner to guide PLHIV on using available resources and advocacy. He described the self-stigmatization that emerged among men with HIV as they sought a romantic partner: I know many men who say, “Help me find an HIV-positive woman,” I say, “You are being treated. Find yourself a normal one. Why HIV positive?” “No, I am afraid.” He discriminates against himself. He puts a label on himself. Even [though] people did not put a label on him.
At the individual level, the label of HIV creates an internalized stigma.
Reducing Identity to HIV Status
Being diagnosed as HIV-positive meant that society tended to define a woman and her family solely through the lens of her health status, ignoring all other identity markers, such as education and profession. The stigma of an HIV-positive status was all-encompassing. In the eyes of society, the victim and her family had lost their honor. Jamal offered the following example: Even if a woman is educated, intelligent, a doctor or a teacher in the village, if her child is HIV-infected, everyone in the village will know about it, including her relatives. Then they start to ask, “Where, how, and why? It turns out that you are such and such.” It is definitely a vulnerable group.
Referring to his own experience, Ulan offered another example of PLHIV being identified based solely on their diagnosis. He disclosed, When they label and stigmatize you, it is useless to try to convince them. For them, there is no concept of HIV. You are AIDS. You are not a human. You are a second-class person. I experienced this for a very long time, especially when my wife was pregnant. Doctors forced her to have an abortion. They said, “A defective freak will be born.”
The HIV label is so stigmatizing in Kyrgyz society that individual identity is often subsumed by it.
Subcategory 1.2. Interpersonal-Level Challenges
The Stigma and Vulnerability of Compromised Morality
Jamal explained that when a woman is HIV positive, others question her character, especially if her husband is perceived to be negative. The woman is perceived as having loose morals or being involved in prostitution. She recounted how this stigmatization plays out: You can certainly encounter different types of violence; however, the bulk of the violence is undeniably psychological violence where [the victim] is stigmatized and discriminated [against], particularly if her husband is negative, but she and her child are positive [for HIV]. Everything may happen here right up to the accusations—when a husband tells his wife, “You may be a prostitute. Where did you get it if I am all clean? Perhaps you are with someone or offer your services, etc.”
Burul added that WLHIV are compelled to tolerate abuses because their partners threaten them with severe consequences. She explained, Blackmail . . . One of the types of blackmail is when he says that he will tell everything to his relatives or all his neighbors. This is the first. Second, sexual blackmail. In general, the action itself is to film [the couple having intercourse] and threaten to send it and file a complaint with law enforcement agencies that she infected him. Extortion and taking the children, manipulation of children. Rape, use, or sell as a means of profit. Sexual slavery.
The intense stigma and moral judgment around HIV status in Kyrgyz society makes women vulnerable to character disparagement and blackmail.
Placing Blame and Scapegoating Easy Targets
The stigma of compromised morality can lead to placing blame and scapegoating. Husbands may wrongly accuse their wives of adultery or prostitution, even if the husbands are the ones who were infected first and passed HIV to their wives. Many Kyrgyz men migrate to Russia for work, and some contract HIV during their time abroad. If they falsely claim to be HIV negative and their wife is HIV positive, it can result in accusations and psychological torment for the wife. While the claim may not be true, the husband’s words can be enough to cast doubt on the wife’s character. Jamal continued her explanation of the role of migration: Let’s say, if a husband just returned from Russia, he also faces stigma: “Instead of leading a normal life there, he brought infection here.” But when a husband says, “No, it is not me. I have had a [blood] test, it turns out that you are such and such.” Then right there, their stories begin.
Tazagul, who counsels individuals living with HIV, described a case in which a woman was blamed in this way: There was a case where a woman was expelled [from her family]. Her in-laws forbade her from seeing her children. However, it is not clear there who infected whom, because her husband was a migrant, and she was here [in Kyrgyzstan]. She lived with her husband’s relatives. He is a migrant. For some reason, she was accused.
Tazagul continued, noting that gender discrimination in Kyrgyzstan makes it convenient to blame women for everything that goes wrong, including HIV-positive status. She said, It is always easier to blame a woman for all these things. We are talking about gender factors. It is often assumed that the woman is to be blamed: if anything is wrong in the family—the woman is to blame; for issues with children—the woman is to blame. HIV is also a woman’s fault. They are a couple, but it is the woman who is to blame. Yes, the role of a woman is such that it is not the same as men. The opinion of our elders [old men] plays a big role in [rural] regions.
Lidia, who has worked in the field of HIV for over 30 years, concluded that women become scapegoats because they are easy targets. Lidia says that some men infect their wives even though they are aware of their HIV-positive status. She explained, In many cases, a man who returns home after migrating may become infected, often through casual sexual encounters or the use of sex workers. Upon returning, he unknowingly or knowingly transmits the virus to his wife. It is important to note that some men are aware of their HIV status when they infect their wives, while other are not. The revelation of the wife’s HIV status often occurs during pregnancy, and unfortunately, it tends to lead to blame being placed on the woman, even if her husband was already aware of his own HIV status. This tendency to assign blame disproportionately to women creates a situation where the family often ostracizes her, leading to her expulsion from the family unit.
Jamal attributed the changing nature of HIV transmission to migrant men, stating that their practices of maintaining multiple families and engaging in unsafe sex with prostitutes were the primary cause of the increasing HIV infections among Kyrgyz women. She described the role of migrant men as follows: Migrants are making their “contributions” as well. What are they doing?! They are leaving for Russia and getting married there; they have another family there. Before this period, they have been indulging [in unsafe sex]. They start to work and with the appearance of money, they start to use the services of the prostitutes. However, today they just look for other migrants, marry and live together there, while their families and children remain here [in Kyrgyzstan].
The widespread separation of couples due to migration and the cultural tendency to hold women responsible for family problems result in women being blamed and scapegoated for HIV transmission.
Emotional, Physical, and Sexual Abuse From Family Members
Interviewees discussed multiple ways that family members subject women with HIV to emotional abuse. Burul has a medical background and as the chairwoman of the public council of the Ministry of Health advocates for the rights of WLHIV. She explained that her job is to advise people on how to live with HIV and observed that infected women face psychological abuse because they are considered useless. She remarked, The biggest harm is probably emotional or psychological abuse. More [than] physical abuse. Because here goes, “You are now HIV positive. Who needs you now?” if we talk within the context of intimate, sexual partners. This is what concerns the family. They kick you out. If women are not kicked out, then they are beaten or raped. They have violent sex.
Burul continued, describing additional instances of emotional abuse and the consequences for women: And then, when [the mother-in-law] says, “Now we will tell everyone, you are no longer our daughter-in-law,” she obeys. Often so. The woman is forced to leave because it is impossible to live in such a hell. You just get kicked out and that is it. They beat her and drive her crazy. Every woman is dependent economically. It is economic violence that simply turns her into a slave.
The stigmatization is so strong that women become targets of emotional, physical, and sexual abuse and ostracization by their own families.
Subcategory 1.3. Community-Level Challenges
Perceptions of a Rising HIV Epidemic Among Women
In Kyrgyzstan more men than women report HIV-positive status; however, interviewees reported that this pattern is changing. For example, Jamal, a consultant at a university-based HIV treatment center, said that both the rate of infection among women and the nature of transmission have shifted: Currently, [the method of transmission] is 50/50. If previously [getting infected] via sexual intercourse made up 27-28% and via injection made up 72%, now it has become equal. What is interesting is that if 15 years ago women made up only a small percentage [of cases], today almost half of HIV infections are among women and are transmitted via sexual intercourse. In other words, a gradual generalization is taking place—HIV infection is becoming general among the population.
Tazagul’s observations highlight the role of women’s migration patterns in the propagation of the infection. She remarked, “In my opinion, migration plays a big role. It increases every year . . . Many young women are leaving. They start building relationships there. And there is a very high growth in the spread of HIV in Russia.”
Discrimination in Housing and Neighborhood Life
WLHIV feared disclosure of their health status because they were likely to face discrimination. Notably, interviewees stated that this discrimination occurred at both the individual level and the institutional level simultaneously.
Barchyn, the executive director of a nonprofit in the field of public health, offered an example of the discrimination and harassment victims experience from community members when they simply try to meet their basic needs, such as finding a place to live. She recounted that an HIV-positive person was considered a criminal for being infected, and neighbors pressured the apartment management through written complaints. Some women were forced to move several times because of the disclosure of their HIV-positive status. Barchyn recalled, During that time, we [our office] changed 5 or 6 apartments and houses because of stigma and discrimination. Neighbors begin to write a complaint: “We don’t want these people next to us; they are criminals; they are drug addicts; they are HIV infected.” And we had to move to another place again.
Ulan also referenced social discrimination, focusing on friends and family members. He commented, Due to the fact that relatives do not understand HIV and how it is transmitted, they begin to separate the dishes. There are families who are kicked out. They begin to worry about their children. Close friends begin to somehow move away or say, “He is HIV-infected. Be careful. Let us get rid of him.” On the part of relatives, there is judgment, discrimination, and stigma.
The stigma and vulnerability of HIV status led to discrimination, harassment, and social separation for WLHIV and their families.
Subcategory 1.4. Institutional-Level Challenges
Institutional Discrimination
Discrimination was not limited to neighbors and community members but also included institutional actors in health, law enforcement, employment, and public services. Barchyn talked about how discrimination against HIV-positive women extends to institutional actors, including doctors. She also described the intersectional nature of discrimination against drug addicts and those with HIV: Psychological violence is in the sense that if she goes to see a doctor, even a gynecologist, and if a doctor finds out that she is a drug addict, then he/she tries not to see her. Why would doctors see addicts? If she is infected with HIV?! [Doctors] will be afraid of getting infected. So, this [psychological violence] does have an adverse effect.
Burul also recounted discrimination and judgments from medical professionals, commenting, [The patient] comes to the doctor, and he/she says, “Ah, do you have this [HIV/AIDS]?” and that is it. The person becomes closed. Or a drug user. “Ah, you do not have veins to get tested” or “Ah, you sleep with anyone, right? You are so bad, a prostitute!” “Ah, if you had not cheated on your husband . . .”
Interviewees explained that WLHIV were considered criminals and treated as such. Alla, who is a consultant with a nonprofit social service center, described this treatment: It is evident that WLHIV face legal prosecution and are unjustly stigmatized. They are, in many cases, treated as criminals simply because of their HIV/AIDS status. This discrimination extends to a particularly vulnerable groups of women . . . those who have struggled with substance use and may have a criminal record. These women face a significant societal pressure- “It turns out that you have been a criminal for your whole life.” . . . It is the most difficult [vulnerable] group among those who are discriminated against by the society on the political, legal, and medical basis.
Ulan, an HIV-positive activist for PLHIV, described the negative impact of discrimination in the workplace: It hurts when the management [at the workplace] finds out that you have [HIV+] status . . . They [HIV+ employees] face such problems when management finds out that they may be asked to leave the job. Employees can judge at work.
Ulan also noted that government officials and decision-makers discriminate against HIV-positive individuals, although this discrimination may go unspoken: Especially decision-makers often do not understand anything and discriminate. They do not necessarily say, “He has HIV,” but they alienate by their behavior. For example, when a person with HIV comes to a reception on social issues at the Mayor’s office or Ayil Okmotu [village authorities], if someone knows that he has HIV, he starts saying, “Come tomorrow. I cannot accept you today. Turn to someone else.”
The stigma of HIV status makes WLHIV vulnerable to exclusion and discrimination in almost every institutional setting.
The Veil of Secrecy—Hiding HIV Status
The widespread stigma and discrimination against HIV-positive women led many to take extreme measures to conceal their HIV status. Due to the prevalence of misinformation and the fear that their doctors might not keep their information confidential, or that their health status might be revealed to neighbors and relatives, numerous WLHIV refrained from seeking treatment to safeguard their privacy. Regrettably, this led to even greater psychological trauma. Jamal explained the pattern of secrecy and avoidance of treatment: Some patients do not want to be treated by those doctors because they are afraid of the [lack of] confidentiality and are afraid that in a small society, someone will spill the beans and, as you know, stigma among the population is still relatively high because of the propaganda that implies that HIV is a plague of the 20th century. Due to this propaganda, in general, public opinion is that if you are HIV infected, you must have engaged in improper behavior, that is, you are either a prostitute or a drug addict, or homosexual, or something else.
The fear of being found out was so potent that some victims disposed of their medications when their husbands or parents-in-law were present. These women feared that family members would discover their HIV-positive status if they saw the medicine. To be on the safe side, they discarded their medications, even though doing so placed their health at risk. Jamal lamented, We have had patients, who out of fear that someone would discover their medicine, for example, if a husband or parents-in-law showed up, went and burned their medicine in a tandyr (a clay oven). Because “someone will see and ask,” she does not take her medicine while her relatives are staying in her house.
Women wanted to access mental health services, but they wanted help from an organization that ensured confidentiality. Living in a close-knit society meant that word traveled fast when information was leaked, and therefore women preferred visiting large, regional crisis centers rather than small, local centers. Jamal summarized the situation as follows: I have already pointed out that there are crisis centers and also a social bureau, where psychologists dig deep and find out the source of any problem. However, these crisis centers are not widely spread yet so one can go and obtain this help. First of all, not all patients give their consent because they are afraid of [the lack of] confidentiality, particularly in a small society. If you redirect them to the regional center, then they go there [without any problem]. They can come up with various reasons to go there and ask for help and open up there.
Lidia, who has been involved in the field of HIV since 1989 and has headed several projects related to HIV during that time, reported that because stigmatization was not limited to the infected person but affected the honor of the entire family, many HIV-positive women did not seek justice when they were harmed. She said, For example, a girl was kidnapped for marriage and she was infected with HIV. When she was diagnosed with HIV, she left her village for Bishkek. She was then told that she could sue the man who infected her. She said, “I have sisters. If all this becomes known, who will marry them?” She refused to persecute her offender. She just left her village and engaged in treatment.
The veil of secrecy behind which WLHIV hide to avoid disclosure of HIV status created additional vulnerability and stress.
Category 2. The Way Forward—Providers’ Ideas About Addressing Stigma and Vulnerability
Subcategory 2.1. Encouraging Support Groups
While WLHIV were hesitant to visit psychologists because of confidentiality concerns, they had faith in participant-run support groups with other WLHIV or people from the general population. Women could share their status in these groups because they felt accepted despite their health status, something they concealed even from people close to them, including their children. Tamara, a prevention specialist at a nonprofit public health organization, observed, Most importantly, our monitoring and conversations with clients reveal that generally, women come to us for self-support [participant-led support] groups. They tell us, “We are accepted here. We can talk openly about our HIV status because we conceal it from our close friends and family.”
Bakyt, the director of a nonprofit social service center, said the apprehension he felt about WLHIV interacting with women from the general population dissipated when the two groups bonded over common problems. He explained, Initially, we feared that WLHIV or sex workers would not get along with women from the general population. But it turns out that when they share the same problem—either it is violence or being homeless—it brings them together and they look after each other.
Peer support groups were seen by providers as a place in which disclosure was safe and not stigmatizing.
Subcategory 2.2. Recognizing Sex Work and Promoting Condom Use
The professionals working with PLHIV made several recommendations for the Kyrgyz government. They contended that to control the spread of HIV, the government must implement policies that promote protective measures such as the use of condoms, address prevalent social norms, raise awareness about HIV infection beginning at the school level, and dispel misinformation about HIV. These recommendations are discussed in detail below.
Several participants said the government should take a more proactive approach by focusing on preventive measures. Burul, who worked at the Ministry of Health, said the government should stop being apathetic and focus on preventive measures for people from every stratum of society. She remarked, “They [state representatives] need to open their eyes and say, ‘We may not accept their behavior, but we have to recognize these people [sex workers].’” She continued, They [government officials] are used to it being a disease of “bad people.” . . . The state, as always, does not have enough money for all this . . . The state does not understand that we need to focus on preventive measures, not only treatment.
Lidia noted that the entitlement men feel toward sex workers prevents them from using condoms and therefore puts the health of both the sex worker and the client at risk. She observed, They [clients] do not accept condoms. Condom is a curse [word] in our country. In fact, it is embarrassing to even say it out loud. That is why they do not use condoms. Often there is violence and unplanned sex, and there is an injury to the genital organs of both men and women. The risk increases . . . They [men] come for sex services and think, “Why use a condom if they came for sex services?,” so there is a high risk of HIV transmission from sex workers.
She continued, noting that “sex work itself is not a factor in HIV transmission” and citing press reports showing that “90% of sex workers in Africa were infected with HIV. In Europe, there were [only] isolated cases. Why? Because of the protection, culture, and health and hygiene of sex workers.”
Service providers focused on apathy, ignorance, and stigmatization on the part of officials in the public health sectors, and cultural attitudes toward condom use as factors that are allowing sexual transmission of HIV to go unchecked.
Subcategory 2.3. Raising Awareness About Gender and HIV
Several interviewees maintained that misinformation or a lack of information about HIV and gender issues impeded HIV prevention and treatment. Lidia suggested that misconceptions about gender have resulted in an apathetic approach to addressing HIV. She explained, Of course, school education should include issues of sexual violence, gender-based violence, and gender sensitivity. You know, most men think that gender is about women. . . Everyone thinks that gender is a swear word and is aimed at oppressing poor men in the interests of women.
Ulan believed that a lack of information among infected people limited their access to services, stating, “If you know the laws, then [you are] okay. If you do not know the laws, not only ours in Kyrgyzstan, but specifically the laws on HIV/AIDS, no one will tell you, act on your behalf, or help you.” He also said that if more people had correct information about HIV, they would support those who are infected. He explained, As for people living with HIV, work with families and people close to them. It is the most important [thing]—working with patients. When you disseminate more information and a person accepts it, his stereotypes change. He already understands that this is not so scary and that he can live with it. [The government should] conduct more training sessions.
Tazagul offered a similar assessment, concluding that self-stigmatization could be curtailed if the infected person received counseling with proper information: The level of violence depends on the woman’s own perception of herself
The lack of high-quality health information about HIV including its transmission, prevention, and treatment, and a lack of information about women’s health and vulnerabilities, are combining to perpetuate stigmatization of WLHIV in Kyrgyz society.
Subcategory 2.4. Focusing on Prevention
Finally, the interviewees suggested that the Kyrgyz government should concentrate on preventing HIV infections. Ulan wanted the government to raise awareness about prevention methods for HIV and drug use beginning at the school level, saying, “Pay more attention to people, and [it’s] better to spend money on prevention than treatment. Our prevention is lame.” Tazagul focused on “positive deviation”—shifting the accepted societal norms and turning her negative experience into positive—strengths and resilience. She observed, We need to work with women. The sooner prevention is implemented, the less HIV will be spread. A preventive program always shows effectiveness. In violence, too. The more we help a woman from the start, to change and look for resources, the more we protect her from radical [unwanted] relationships, physical beatings, sexual harassment, and more.
Tazagul noted that while most legal barriers have been addressed, interventions that would offer resources to help infected women obtain psychological support remain stuck in the proposal stage, and thus cannot be effective. She concluded, It seems to me that there is still a lack of psychosocial support. Treatment is provided. There are benefits. The ban on adoption was revised; now HIV-positive people are allowed to adopt kids. There are no such barriers at the legislative level; everything is fine on paper. But psychosocial support is not enough from government agencies and the non-governmental sector. There is, of course, a big drawback here.
Service providers called for a new policy focus on the prevention of HIV transmission and greater psychosocial support as priorities for improving the public health response to WLHIV.
Discussion
This study’s examination of in-depth interviews with professionals involved in HIV prevention, advocacy, and treatment programs in Kyrgyzstan contributes to a deeper understanding of the experiences of WLHIV and reveals the complicated nature of these women’s fears, as well as barriers to help-seeking within the sociocultural context of Kyrgyzstan. As HIV prevalence in the region rapidly rises in contrast with global trends, so too does the importance of documenting and addressing HIV stigma. The results from this study extend the HIV-related stigma literature and show the risks of violence following HIV status disclosure, and health and social service responses experienced by WLHIV in Kyrgyzstan.
The findings of the study show that women now comprise nearly half of the HIV-infected population in Kyrgyzstan, with a growing number contracting the virus through sexual intercourse, as noted in studies by Thorne et al. (2010), El-Bassel et al. (2011), and Scambler (2007). This trend in Kyrgyzstan aligns with a global pattern where two primary modes of transmission—sexual intercourse and needle sharing—have become equally responsible for the spread of HIV. The findings of this study are consistent with findings from previous systematic reviews and meta-analyses as well as studies among WLHIV from different populations and regions (Bayat et al., 2020; Katz et al., 2013; Logie & Gadalla, 2009; Rueda et al., 2016) that have found negative impacts of HIV stigma on a range of outcomes.
As described above, the ecological model (Heise, 1998) provides a framework for organizing our understanding of stigma and vulnerability and for improving responses to it (Figure 1). At the personal level, victims suffered self-stigmatization, which led them to indulge in risky behaviors to hide their HIV status. Victims experienced both internal and enacted stigma, which manifested in feelings of shame. The psychological pressure the victims faced had practical implications in that many women refused to visit care centers near their homes for fear of confidentiality breaches. WLHIV were perceived as having loose morals, engaging in infidelity, or working as prostitutes. Furthermore, an HIV diagnosis was likely to taint not only the victim’s character but also the honor of her family.
This finding is consistent with other countries’ experiences. In Botswana, qualitative studies have identified how testing policies contribute to a context where women bear the brunt of HIV stigma (Poku et al., 2023; Yang et al., 2021). A study among Black WLHIV in the United States found that greater anticipated stigma was correlated to poorer mental health, discrimination, and use of negative coping strategies (Travaglini et al., 2018). A study from Thailand (Mathew et al., 2020) found that WLHIV believed they would be denied job opportunities, and a study from Vietnam (Chi et al., 2010) found that WLHIV feared their children would be stigmatized and denied school admission if their HIV-positive status was known by others.
The WLHIV held self-stigmatizing beliefs because they were aware of negative attitudes, behaviors, and perceptions experienced by other PLHIV (Liamputtong et al., 2009; Mathew et al., 2020). WLHIV anticipated low social support and discrimination from society and feared a breach of confidentiality about HIV status due to changes in physical appearance. They saw themselves as being shameful to family, so they self-isolated from the community (Azhar, 2018; Liamputtong et al., 2009; Qin et al., 2019) and internalized the stigmatization. In Ukraine, intersectional internalized and enacted HIV and drug use stigma were significant predictors of HIV care engagement among WLHIV (Owczarzak et al., 2023).
At the relationship level, romantic relationships were difficult to engage in and maintain. The study shows that the women dreaded their condition being discovered by family members and the surrounding community. Providers described how many women went to great lengths to hide their HIV status—even risking their physical and mental health—to avoid being stigmatized. These findings are similar to results in India and Africa. In India, WLHIV were also likely to face stigma and discrimination not only from their husband and in-laws (Halli et al., 2017) but also from their parents and siblings (de Souza, 2010). WLHIV were labeled as sex workers, ostracized for their HIV-positive status, blamed by their in-laws for transmitting HIV to their husbands, and risked being expelled from their marital homes (de Souza, 2010; Halimatusa’diyah, 2019). A study in India (Halli et al., 2017) found that factors related to stigmatizing behaviors and attitudes from spouses included a wider age gap between WLHIV and the spouse, and financial dependence on the husband due to lack of WLHIV’s income-generating activities. A systematic review of mental health among PLHIV in Africa found that being female, receiving poor-quality health services, and lack of emotional support from family was associated with greater psychiatric morbidity (Brandt, 2009).
In many patriarchal societies, a woman’s behavior and life choices are associated with the entire family’s honor (Cihangir, 2013; Cooney, 2014). The family honor is heavily dependent on the woman’s behavior (Mosquera, 2013) and the woman’s negative reputation brings shame to both the woman and the family she is associated with (Cinthio, 2015). The negative social perceptions of HIV as a promiscuous infection and judgments of WLHIV as people with low moral values who peddled their chastity could be the reason for HIV-related stigma and discrimination observed across multiple studies (Fauk et al., 2021; Liamputtong et al., 2009). A WLHIV is perceived to have compromised the family honor and they are likely discriminated for this reason.
At the community level, the enacted stigma from relatives and neighbors prevented victims from reaching out for social support, which increased their likelihood of experiencing mental health issues. Similarly, findings from a study in India show gender was an important factor in how women were treated post-HIV status revelation compared to men (Jaiswal & Kumari, 2019) such that WLHIV had lower self-esteem and higher rumination because of family rejection, blame, shame, and guilt as compared to men living with HIV. Discrimination against WLHIV in India included social isolation through exclusion from social functions and public establishments, eviction from communities they were living in, and negative labeling (de Souza, 2010; Halli et al., 2017). The separation of eating utensils and refusal to share food and drinks touched by WLHIV for fear of contract HIV through social contacts was observed in India and Indonesia (Fauk et al., 2021). A recent systematic review found extensive psychological and social impacts associated with living with HIV for women and their families in Asian countries (Fauk et al., 2022).
A driving factor in stigma and discrimination against WLHIV is the lack of knowledge or proper information regarding HIV transmission and the fear of contracting HIV through social contact and interaction (Fauk et al., 2021; Liamputtong et al., 2009). The stigma toward PLHIV from noninfected people could be a psychological response toward the awareness about the existence of PLHIV in close proximity which could make them feel vulnerable (Earnshaw & Chaudoir, 2009; Fauk et al., 2021).
At the institutional level, victims faced discrimination from professionals such as doctors and policymakers—the very people who should have supported them. These findings are consistent with studies from India and parts of Africa. Institutional discrimination from other studies has included unnecessary referrals to other clinics (Azhar, 2018; Feyissa et al., 2012; Subramaniyan et al., 2013), coercion to terminate pregnancies, sterilization or loss of private health insurance after HIV diagnosis (Paxton et al., 2005), unofficial disclosure of HIV-positive status of clients (Feyissa et al., 2012), derogatory language and verbal harassment (Subramaniyan et al., 2013), and refusing to provide health care services and failing to enroll PLHIV in care and support activities (Azhar, 2018; Fauk et al., 2021; Feyissa et al., 2012).
Findings from a study among health care workers in Southwest Ethiopia (Feyissa et al., 2012) showed that institutional discrimination was more likely by health care workers who wanted to take extra precautions for fear of work-related HIV transmission. The study found that a lack of in-depth HIV knowledge, low HIV caseload, and lower perception of protocol-related institutional support, policy-related institutional support, and supply-related institutional support to be significant predictors of stigma and discrimination by health care workers against PLHIV (Feyissa et al., 2012). These factors led to feelings of lack of safety among health care workers. Discrimination was more likely from health care workers with lower education and lower training levels. The institutional discrimination against WLHIV in Kyrgyzstan could be a combination of the factors related to low knowledge of HIV transmission, poor understanding of protocol related to providing services for WLHIV, and inadequate supply of safety materials in health care settings, which led to perceptions of risk among health care workers while assisting WLHIV.
Despite facing challenges at the personal, interpersonal, community, and institutional levels, WLHIV persevered by seeking help at regional centers where they were assured of confidentiality. They sought comfort in self-support groups because they felt accepted in these settings and were comfortable talking openly about their HIV status. The results indicate that WLHIV will seek professional help when institutional support is strong enough to ensure confidentiality and security. Given this finding, institutional support should be strongly encouraged, particularly for peer support. The current findings align with the results of research on WLHIV in Iran (Oskouie et al., 2017), which found that women reported overcoming feelings of shame through face-to-face interactions with other WLHIV. Similarly, studies in Ethiopia and China (Feyissa et al., 2012; L. Li et al., 2007) suggest that higher levels of institutional support in the form of adequate materials and health supplies are correlated with less discrimination against PLHIV which could encourage women to reach out for help.
Implications for Practice, Policy, and Research
There are several implications for practice at all levels of ecology. The first important implication for practitioners (as described by the chairwoman of the public council of the Ministry of Health, for example) is that stigma and discrimination against WLHIV should be recognized as a form of violence. At the individual level, awareness programs that target WLHIV should be promoted so that these women can recognize the various forms of violence inflicted on them because of their status, identify violations of their rights, and find help to pursue remedies. A study of South African women (Pronyk et al., 2006) found that economically independent women were less likely to experience IPV despite their HIV-positive status. Given this, governments should offer economic incentives and promote the financial independence of women to reduce violence among WLHIV.
At the interpersonal level, both governmental and nongovernment agencies should focus on HIV prevention by creating awareness of risky sexual behaviors among men and advocating for laws prohibiting multiple and simultaneous sexual partners (Halperin & Epstein, 2007). In addition, these prevention efforts should promote the use of condoms. Prior research has shown that women’s fear of a partner’s potentially violent reaction to a request for condom use hinders safe sexual health practices (Champion et al., 2004; Davila, 2002).
At the community level, mass awareness campaigns organized and chaired by the Ministries of Health, Labor and Social Protection, and Education and Science of the Kyrgyz Republic aimed at the general population should be conducted to dispel inaccurate information about HIV and thus reduce discrimination against victims based on misinformation. A prior study in Kyrgyzstan (Imanbaev & Karabaeva, 2021) found that for young people, mass communication via feature films and books that depict people who use drugs, engage in prostitution, or have HIV/AIDS as characters may be more influential than training and lectures. In addition, programs and interventions should focus on stigma prevention so that infected women will be more likely to utilize resources and medical help.
At the institutional level, efforts should be made to ensure women feel safe in health care settings. A safe environment that accords the highest level of confidentiality is key to HIV-positive women seeking help for their physical and mental health. Health care practitioners should be trained to understand that their attitudes and words can push women to withdraw and avoid seeking help. The study from Southwest Ethiopia (Feyissa et al., 2012) showed that discrimination by health care workers was more likely when there was a lack of specific policies or guidelines related to the care of clients with HIV-positive status. Health care workers who had a deep knowledge of HIV and who had attended training on topics related to stigma and discrimination were less likely to discriminate; therefore, attention should be paid to regularly train health care workers on HIV-related issues. There are few existing interventions to address HIV stigma in the Central Asian region. One promising and innovative approach in development has used crowdsourcing methods to reduce stigma around HIV testing among adolescents and young adults in Kazakhstan; if shown to be successful, similar approaches could be adopted in Kyrgyzstan (Mergenova et al., 2022).
Another promising approach is effective prevention at a large scale with accessible entry points and generational time scales. Investigations addressing stigma through multilevel components that simultaneously address family- and school-related prevention and treatment, addressing poverty-impacted needs and barriers to help-seeking among PLHIV represent a valuable entry point and pathways for potential change (Andersson et al., 2020; McKay et al., 2014; Mutumba et al., 2022). Policymakers must implement measures that mitigate the violence that may follow an HIV diagnosis. In addition, more of the individuals at greatest risk for HIV should be included in policymaking processes—Ancker and Rechel (2015) found that at-risk populations were underrepresented in Kyrgyz nongovernmental organizations working in HIV/AIDS policy, even though these populations will likely feel the effects of resulting policies most strongly.
Limitations
The study has certain limitations. The study has a small subsample size, comprising only 10 informants, which may limit the generalizability of our findings to a broader population of service providers. Future research endeavors should strive to employ larger and more diverse samples. Further research could also be conducted among WLHIV to gather their perspectives and experiences of stigma and design programs that address these needs.
Despite the limitations, this study contributes in important ways to the growing literature on the violence experienced by WLHIV in Kyrgyzstan. Policymakers design policy revisions on raising awareness and information dissemination so that no WLHIV experiences institutional violence in health care settings, an issue that policymakers have the most control over. Institutional stigmatization should be recognized as a barrier to the effective treatment of physical and psychological violence and as a major barrier to HIV care. Future health care guidelines should incorporate strong policies regarding health practices and community engagement so that WLHIV do not repeatedly experience personal and institutional discrimination. To reduce the current upward trend in HIV incidence and prevalence, concentrated efforts are needed to address HIV stigma and vulnerability to improve care for WLHIV in Kyrgyzstan.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this article was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number K01HD106070. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This project was also supported by a Fulbright Program grant (grant no. PS00292785) sponsored by the Bureau of Educational and Cultural Affairs of the United States Department of State and administered by the Institute of International Education. Research for this article was supported in part by the Title VIII Research Scholar Program, which is funded by the U.S. State Department, Program for Research and Training on Eastern Europe and the Independent States of the Former Soviet Union (Title VIII) and administered by American Councils for International Education. The opinions, findings, and conclusions stated herein are those of the authors and do not necessarily reflect those of either the U.S. Department of State or the American Councils for International Education.