
Abstract
One third of U.S. adolescents experience anxiety. As adolescents spend more time outside the family, built environmental risk factors become salient. Although resilient family protects youth from various adversities, it is unclear how effective family resilience can buffer extrafamilial risks. This study examined the moderating role of family resilience in the association between neighborhood, school, and racial discrimination risk factors on adolescent anxiety. Using multiyear data (2016–2020) from the National Survey of Children’s Health (n = 81,809), the hierarchical logistic regression analysis suggests that neighborhood violence/safety, lack of neighborhood support, lack of school engagement, lack of school safety, and racial discrimination increased adolescent anxiety. Meanwhile, family resilience indicates both promotive and protective effects. Particularly, family resilience alleviated the positive association between lack of school engagement and adolescent anxiety. Among various built environment risk factors, family resilience was found to alleviate adolescent anxiety in the school context. Although family resilience was not found to be a panacea against all risks in neighborhood and school, adolescents experiencing anxiety due to lack of school engagement may take advantage of family resilience.
Introduction
Adolescent anxiety is a serious public health issue, entailing various psychosocial and developmental problems (Yang et al., 2023). The National Institute of Mental Health (NIMH, 2023) reports that 31.9% of adolescents between 13 and 18 years of age meet the criteria for anxiety disorders (e.g., panic disorder, generalized anxiety disorder); female adolescents (38.0%) show a higher rate of anxiety compared with male adolescents (26.1%). Although worrying and anxious feelings are typical emotional responses to stressful situations, excessive anxiety can impair adolescents’ ability to function (NIMH, 2023). As adolescents expand their social networks beyond family to explore social domains, such as school and neighborhood, the environment becomes increasingly influential to them. However, negative experiences within their school and neighborhood domains emerge as salient risks to adolescent anxiety (Buttazzoni et al., 2022). As family members, particularly parents, continue to have a significant impact on adolescents, those from resilient families are likely to overcome or outgrow difficult situations, indicating the important role of family members’ support for adolescents (Walsh, 2015). However, despite the significance of family resilience on adolescents, it is understudied to what extent family resilience can buffer the impact of risks experienced outside the family domain, such as the neighborhood and school. This study aims to understand the protective effect of family resilience on the impact of risk factors outside the family domain on adolescent anxiety. This study examines the impact of neighborhood risks (i.e., physical disorder, neighborhood violence and safety issues, and lack of neighborhood support), school risks (i.e., lack of school engagement and lack of school safety), and racial discrimination on adolescents’ anxiety and the promotive and protective effect of family resilience.
Theoretical Framework
Two integrated theoretical frameworks guide this study: the built environment theory (Evans, 2003) and the family resilience theory (Walsh, 2015). Evans (2003) posited that the built environment, which includes neighborhood quality, housing, and institutional settings may either directly or indirectly affect mental health. Meanwhile, supportive relationships and social cohesion count as critical factors for mental health. Consequently, built environment may alter the psychological process that affects mental health. Hence, adolescents’ adverse experiences within the negative built environment may increase the risk of anxiety.
Family resilience theory postulates that the family can buffer various adversities (Walsh, 2015). Family resilience comprises family strength and resources, and youth with higher family resilience are likely to overcome negative experiences. Family resilience has been documented to protect youth from various adverse experiences within the family. However, as adolescents spend more time outside their family domain compared with their younger counterparts, they are likely to experience more risk factors from their built environment, such as neighborhoods and schools. Hence, this study incorporates the two theoretical frameworks to examine the detrimental effects of built environment risks and the promotive and protective effects of family resilience on adolescents’ anxiety.
Neighborhood Risk Factors and Adolescent Anxiety
Neighborhoods have been recognized as both built environment determinants and social determinants of health (Kolak et al., 2020; Molina-García et al., 2017). In congruence with the built environment theory, the World Health Organization (WHO) specifically identified that neighborhood trust/safety, community-based participation, violence/crime rates, attributes of the natural and built environment, and the amount of neighborhood poverty are critical determinants of global mental health (WHO & Calouste Gulbenkian Foundation, 2014). Adolescents who witness or experience violence in their neighborhood are more prone to experience anxiety (Gaylord-Harden et al., 2011; Kennedy & Ceballo, 2016). The relationship’s mechanism might be rooted in the constant stress of feeling unsafe, leading to an increased hyperalertness. In one study, adolescents who indicated feeling unsafe in their neighborhood reported double the psychological distress of adolescents who felt safe (Goldman-Mellor et al., 2016).
Moreover, adolescents who live in high-poverty neighborhoods exhibit higher levels of anxiety compared with their peers who move out of high-poverty neighborhoods (King et al., 2022). Economic disadvantage at the neighborhood level exposes these adolescents to chronic stressors. Exposure to chronic stressors affects the brain and elevates the allostatic load, which gradually leads to increased mental distress (Gustafsson et al., 2014). In a quasi-experimental study, residents of an affordable housing development in a low-poverty neighborhood reported fewer anxiety symptoms than their counterparts who resided in a high-poverty neighborhood (Casciano & Massey, 2012). Lower property taxes in high-poverty neighborhoods mean less access to resourced schools for adolescents (Zhang et al., 2020). Aligning with the built environment theory (Evans, 2003), the built environmental aspects of the neighborhood often mean limited access to health care, mental health services, and green spaces, which are all associated with increased anxiety (Zhang et al., 2020). Furthermore, low neighborhood cohesion, or the level of support from neighbors that adolescents feel, also poses a risk for heightened anxiety (Cutrona et al., 2019). Neighborhood physical disorder, comprising social and built factors, such as residential instability, crime rates, and vandalism, is also associated with increased adolescent anxiety (Sampson et al., 2016).
School Risk Factors and Adolescent Anxiety
Research demonstrates the impact of the school environment on adolescent mental health, including anxiety. Several common school risk factors influence anxiety levels across ethnically and socioeconomically diverse groups of students. These school risk factors include school-related stress, school climate, school satisfaction, teacher turnover rate, school safety, and school connectedness (Brar et al., 2023; Davis et al., 2017; Zhu et al., 2019). School-related stress, which includes adolescent relationships with peers and teachers at school, is a risk factor for social anxiety. School-related stress also includes students’ academic achievement (Zhu et al., 2019). When the stress of these school factors is high, they predict higher levels of social anxiety in adolescents. In other words, as students struggle academically or struggle to have positive relationships with peers and teachers, they experience anxiety (Davis et al., 2017).
Another component of schools that affects adolescent anxiety is the school climate. The school’s climate describes the overall positivity or negativity of the relationships among students, staff, and teachers, which affect students’ ability to thrive (Rudasill et al., 2018). Accordingly, scholars argue that a positive school climate is an important factor in the overall mental well-being of adolescents (Cohen et al., 2009; Malone et al., 2022). Thus, adolescents who attend schools with a poor school climate are at higher risk of experiencing anxiety (Zhu et al., 2019). The school climate literature is similar to the concept of school satisfaction. Cohen and colleagues (2009) demonstrated that school satisfaction and anxiety have an inverse relationship; when students were highly satisfied with their school experience, anxiety decreased by 23%. School safety has emerged as a public health issue due to frequent safety-related incidents, such as exposure to gun-related and other types of violence, which increased the level of anxiety (Filindra et al., 2020; Shulman et al., 2021). Furthermore, school connectedness has been documented to be negatively associated with anxiety (Brar et al., 2023). School connectedness refers to students’ level of belonging and engagement in schools. Those adolescents with low levels of school connectedness have greater odds of experiencing anxiety (Brar et al., 2023).
Racial Discrimination and Anxiety
Since 2016, the United States has seen an increase in school violence and hate crimes (Edwards & Rushin, 2018). The driving force behind the majority of hate and bias incidents in schools seems to stem from racism, comprising 63% of incidents highlighted in news reports and 33% of incidents documented by educators (Southern Poverty Law Center, 2019). Because neighborhoods and schools often ignore or fail to respond to issues of racism, such as microaggressions, adolescents from socially marginalized groups may experience more of these incidents of hate or bias. Priest and colleagues (2013) found that 87% of Black youth experienced at least one discrimination incident within the previous year. Several studies show increased anxiety due to racial discrimination and microaggressions in schools (Davis et al., 2017; Priest et al., 2013; Seaton et al., 2008; Turner et al., 2016). A systematic review demonstrated a consistent and robust link between racial discrimination and anxiety and other mental health outcomes (Priest et al., 2013). Student anxiety was the highest in settings where students reported high levels of discrimination. Furthermore, their findings suggest that racial discrimination may predict psychological distress for racially marginalized groups more than other school or neighborhood stressors listed in the previous section.
A portion of the research on racial discrimination and anxiety expands upon school climate by distinguishing the school’s racial climate from the general school climate. Factors such as teacher racial/ethnic identity and student racial/ethnic identity are associated with positive and negative school racial climate (Malone et al., 2022). Ethnic/racial identity was positively associated with high anxiety levels for marginalized students. Adolescents were 22% more likely to experience anxiety if they had a strong racial identity but their school had a low enrollment of students with the same racial identity (Priest et al., 2013). Students’ discrimination experiences also accelerated the impact of several school risk factors previously mentioned, such as teacher turnover. At schools where the teacher turnover was high and racially marginalized adolescents experienced high levels of discrimination, these adolescents had an increased likelihood of anxiety (Priest et al., 2013). The racial composition of a school was also an important factor in determining anxiety levels, with the lowest levels of anxiety occurring when the majority of the students in a school matched an individual student’s racial/ethnic identity (Davis et al., 2017).
Racially marginalized youth even experience racism when seeking assistance for their mental health needs (Malone et al., 2022). For example, minority youth are less likely to be referred for community-based or school-based mental health than white students although the school is responsible for 70% to 80% of student mental health intervention (Malone et al., 2022). The impacts of racial discrimination, for male adolescents, have also been associated with increased anxiety even into adulthood, according to a longitudinal analysis of 681 Black youth followed for 12 waves of data collection, starting in 1994 and ending in 2012. Racial discrimination is a consistent and robust predictor of anxiety in racially marginalized adolescents (Davis et al., 2017).
Family Resilience and Anxiety
Family resilience primarily comprises family belief systems, organizational processes, and communication problem-solving processes (Walsh, 2015). Families with healthy communication skills that engage in positive activities with family members can build trust, cohesion, happiness, and togetherness, increasing the chance of overcoming crises and adversities (Gayatri & Irawaty, 2022). The role of family resilience is documented to have positive behavioral and mental health outcomes among adolescents (Song et al., 2021). In particular, adolescents with high levels of family resilience are likely to show lower levels of anxiety (Finklestein et al., 2022). Youth with the outlet to openly communicate with trusted and caring family members are likely to decrease the chance of bottling up negative emotions, which may lead to anxiety. Furthermore, adolescents who confront unexpected adversities outside the family can seek helpful and practical advice from their family members.
The Current Study
Adolescents are in a developmental stage of gradually searching for emotional separation from parents, identification with their peer group, and a sense of personal identity (Hazen et al., 2008). Consequently, as adolescents expand their social network outside the family, experiences in their neighborhood and school emerge as critical domains of both growth and challenges. Although adolescents are still bound and susceptible to their family members, it is unclear to what extent can family resilience buffer against risk factors experienced outside the family. To our knowledge, a paucity of research has explored the buffering effect of family resilience on adolescent anxiety in the context of risk factors experienced in the neighborhood and school. Hence, building upon prior studies, the focal research questions of our study are as follows:
Method
Data Source
This study is a secondary data analysis using the National Survey of Children’s Health (NSCH), a comprehensive survey endorsed on a national scale that compiles details regarding the physical and emotional health, health care availability, and familial and community factors of American children aged 0–17 years. Data were collected from the U.S. Department of Health and Human Services and the U.S. Census Bureau, between 2016 and 2021. The survey encompasses diverse data about child health and wellness, such as physical and mental health, health care accessibility, and social and emotional growth. Household addresses were randomly chosen from across the United States, and households participating in the survey received two reminder letters and postcards to prompt online survey completion. A paper questionnaire was sent if there was no response to the online survey. Households with eligible children were identified through a screening questionnaire. Further details regarding the survey can be found at the following link: https://www.childhealthdata.org/learn-about-the-nsch/NSCH (Table 1).
Descriptive Statistics for the Sample Population (age 11-17; aggregated NSCH data from 2016 to 2020).
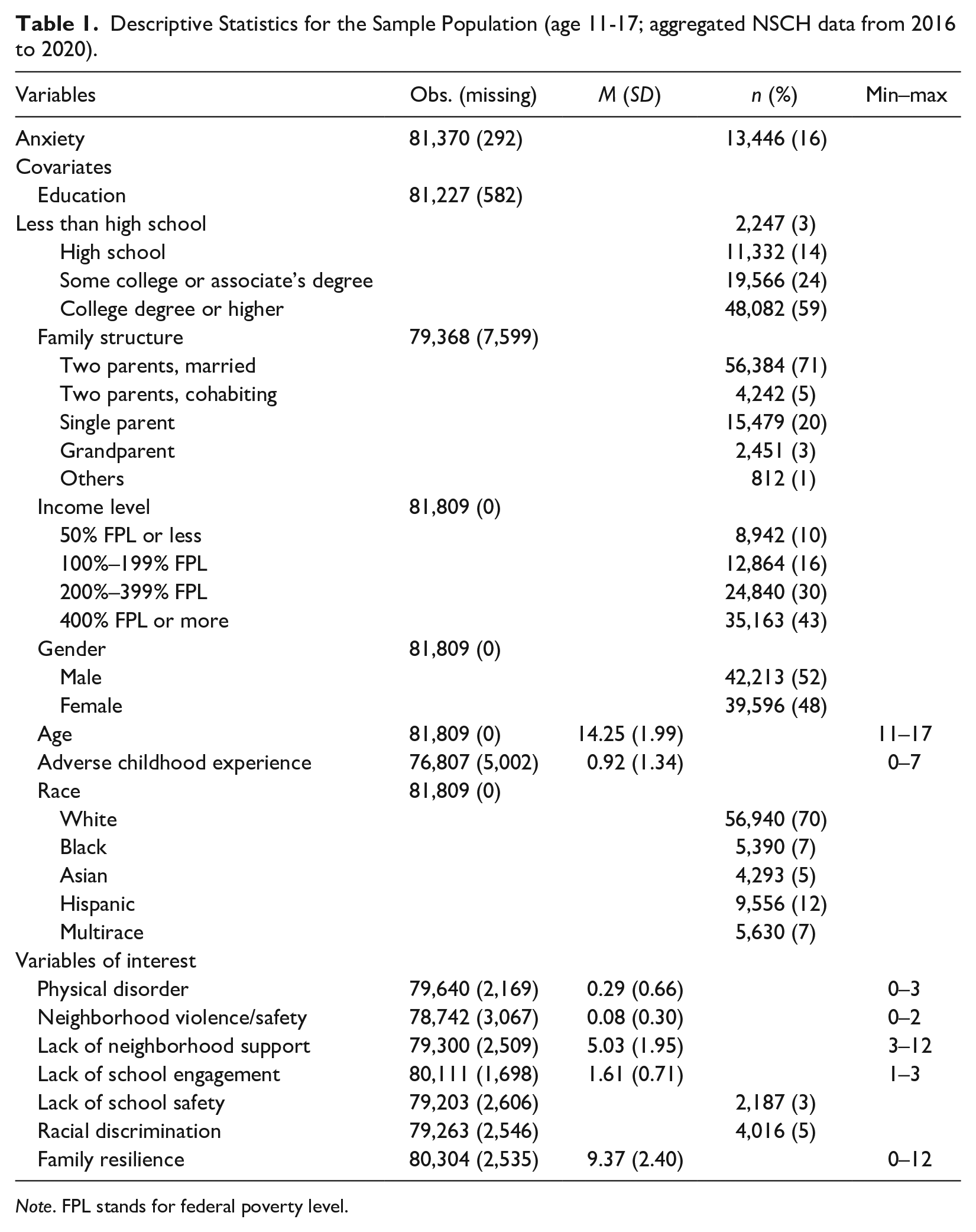
Note. FPL stands for federal poverty level.
Sample and Participants
This study’s analysis aggregated NSCH data from 2016 to 2020. NSCH provided a manual for collating multiyear data from 2016 to 2020, which was used to unify the data sets (U.S. Census Bureau, 2022). The data from 2021 were excluded from the analysis due to the possible influence of the COVID-19 pandemic on outdoor activities. Adolescents in middle and high school were the focus group of this analysis as they are susceptible to mental health problems due to physical changes and social interactions. From a total sample of 174,551 participants, we narrowed our focus to middle and high school adolescents aged 11–17 years as this period of growth is characterized by increased independence and a heightened desire for autonomy. Family involvement can significantly influence adolescents’ mental health, especially those at risk of anxiety (Blakemore, 2018). After filtering the respondents’ age, the final sample size from 2016 to 2020 was (n = 81,809).
Measures
Anxiety
Anxiety was measured using two items in the NSCH survey. The first item asked the parents, “Has a doctor or other health care provider EVER told you that this (adolescent) child has anxiety problems?” a follow-up item asked whether the child currently has anxiety problems. The response options for both items were (0 = no, 1 = yes). Based on the responses to these two questions, only children who were reported to currently have anxiety were classified as having anxiety (0 = does not currently have anxiety, 1 = currently has anxiety problems).
Physical Disorder
Neighborhood physical disorder was measured using three self-report items. These three items were used in a previous study to examine neighborhood physical disorder (Jackson et al., 2019). Item examples include the following: “In your neighborhood, is/are there vandalism such as broken windows or graffiti,” “poorly kept or rundown housing,” and “litter or garbage on the street or sidewalk?” Responses were 0 = no, 1 = yes. The three items were summed into a composite physical disorder score (ranging from 0 to 3).
Lack of Neighborhood Support
Neighborhood support was measured using three self-reported items. The items included, “People in this neighborhood help each other out,” “We watch out for each other’s children in this neighborhood,” and “When we encounter difficulties, we know where to go for help in our community.” Responses for each question were measured on a 4-point Likert-type scale (ranging from 1 = definitely agree to 4 = definitely disagree). The responses of the three items were summed into a composite lack of neighborhood support score that ranged from 3 to 12. The Cronbach’s alpha was .80.
Neighborhood Violence/Safety
Neighborhood violence/safety was measured using two self-reported items. Items include “(your adolescent child) was a victim of violence or witnessed violence in their neighborhood” and “this child is safe in our neighborhood.” The response for neighborhood violence was binary, with 0 = no, 1 = yes. For neighborhood safety, the responses were measured on a 4-point Likert-type scale, ranging from 1 (definitely disagree) to 4 (definitely agree), which were dichotomized into 0 = feeling safe, 1 = feeling unsafe. Referring to a previous study, the scores from the two items were summed (Jackson et al., 2019) into a composite neighborhood violence/safety score (ranging from 0 to 2).
Lack of School Engagement
Lack of school engagement was measured with two self-reported items, such as “how often does this child care about doing well in school?” and “how often does this child do all required homework?” Responses were categorized on a 4-point Likert-type scale ranging from 1 (always) to 4 (never). These items were recoded according to the NSCH codebook guidelines (CAHMI, 2022) into categories ranging from 1 to 3. If responses indicated that the adolescent “always” cares about doing well in school AND does required homework, they were categorized as 1 = always engaged in school. Adolescents were categorized as 2 = usually engaged in school, if responses were “usually” to both questions or “always” to one item and “usually” to the other. The remaining responses were categorized as 3 = sometimes or never engaged in school.
Lack of School Safety
The lack of school safety was measured with a single self-reported item asking, “(if) this child is safe at school.” Response options were 1 = definitely agree, 2 = somewhat agree, 3 = somewhat disagree, and 4 = definitely disagree. Referring to Ignacio and colleagues (2022), lack of school safety was dichotomized as 1 = unsafe: for “somewhat disagree” and “definitely disagree,” and the other responses were recoded as 0 = safe.
Racial Discrimination
Racial discrimination was measured with a single self-reported item, “(your child is) treated or judged unfairly because of their race or ethnic group”; the respondent answered 0 = no, 1 = yes.
Family Resilience
Family resilience was measured with four self-reported items beginning with the prompt, “when your family faces problems, how often are you likely to do each of the following?” Item examples included, “talk together about what to do,” “work together to solve our problems,” “know we have strengths to draw on,” and “stay hopeful even in difficult times.” Response options were measured on a 4-point Likert-type scale from 1 (all of the time) to 4 (none of the time), and then reverse recoded (ranging from 0 to 3) following the guidance in NSCH Codebook (CAHMI, 2022). Then, the four items were summed; the higher the score the more the resilience. The potential score for combined family resilience was from 0 to 12 (Heerman et al., 2022), with Cronbach’s alpha of .89.
Covariates
The study included a range of sociodemographic variables (gender, race, age, parents’ education, household income, and family structure) as covariates in the models. The covariates included gender (male vs. female), age (11–17 years of age), race (white, Black, Asian, Hispanic, and multirace), parental education level (less than high school, high school, some college or associate’s degree, and college degree or higher), family income level based on the federal poverty line (50% or below, 100%–199%, 200%–399%, and 400% or more), and the family structure (married, cohabiting, single parent, grandparent households, and others). Furthermore, this study controlled for the family risk factors from adverse childhood experiences (ACEs; Felitti et al., 1998). The 2016–2020 NSCH data set measured nine specific items from the original 10 ACEs questionnaire. Given the significance of family-related risk factors on adolescent anxiety, we intentionally controlled for the family-related risk factors from ACEs to examine the risk factors from school, neighborhood, and racial discrimination.
Data Analysis
We utilized Python for data cleaning and analysis, employing the statsmodels library (Seabold & Perktold, 2010) and scikit-learn (Pedregosa et al., 2011) for our analysis. Family structure exhibited the highest rate of missing data, at 9.3%, prompting us to apply imputation techniques to enhance model fitting accuracy by filling in missing values. Prior to imputation, we conducted Little’s Missing Completely at Random (MCAR) test to check whether the missing data were random. Finding that the data were missing at random, we proceeded to use Multiple Imputation by Chained Equations (MICE) for the imputation process.
The focal interest of our study is to explore the role of family resilience in buffering adolescents against the impact of the built environment risk factors such as those encountered in neighborhoods and schools. Our methodological approach involved hierarchical logistic regression analysis, conducted in three progressive steps to dissect the complexities of this relationship. In Model 1 (the covariate model), we adjusted for demographic and personal covariates to ensure that our findings were not confounded by these factors. In Model 2 (the main effect), we assessed the main effects of built environment risk factors, including physical disorder, violence/safety, support, lack of school engagement, lack of school safety, and racial discrimination along with the promotive effect of family resilience. In Model 3 (the interaction model), we examine the protective (moderating) effect of family resilience on the impact of the risk factors on adolescent anxiety.
Results
Table 2 shows the results of the hierarchical logistic regression models. In Model 1, compared with adolescents whose parents have less than a high school degree, those with parents holding a college or associate’s degree had 1.32 times (95% confidential interval [CI] = [1.14, 1.53]) higher odds of experiencing anxiety. Adolescents whose parents have a college degree or higher had 1.51 times (95% CI = [1.31, 1.75]) higher odds of experiencing anxiety compared with those whose parents have less than a high school degree. The household with 200%–399% of the federal poverty level (FPL) had 0.92 times (95% CI = [0.86, 0.99]) lower odds of experiencing anxiety compared with those from the 50% or less of the FPL. Adolescents with cohabiting parents had 0.88 times (95% CI = [0.81, 0.95]) lower odds of experiencing anxiety compared with those with married parents. Other types of family structures had 0.73 times (95% CI = [0.63, 0.85]) lower odds of experiencing anxiety. Female adolescents had 1.49 times (95% CI = [1.43, 1.55]) higher odds of experiencing anxiety compared with male adolescents. Every increase of 1 year in age was associated with 1.08 higher odds (95% CI = [1.07, 1.09]) of experiencing anxiety. An increase of one ACE was associated with 1.47 times (95% CI = [1.44, 1.49]) higher odds of experiencing anxiety. Black adolescents had 0.39 times (95% CI = [0.35, 0.43]) lower odds, Asian adolescents had 0.36 times (95% CI = [0.31, 0.41]) lower odds, Hispanic adolescents had 0.71 times (95% CI = [0.66, 0.76]) lower odds, and multiracial adolescents had 0.69 times (95% CI = [0.63, 0.75]) lower odds compared with their white counterparts’ odds of experiencing anxiety.
Results of Logistic Regression (Adolescent Anxiety as the Dependent Variable).
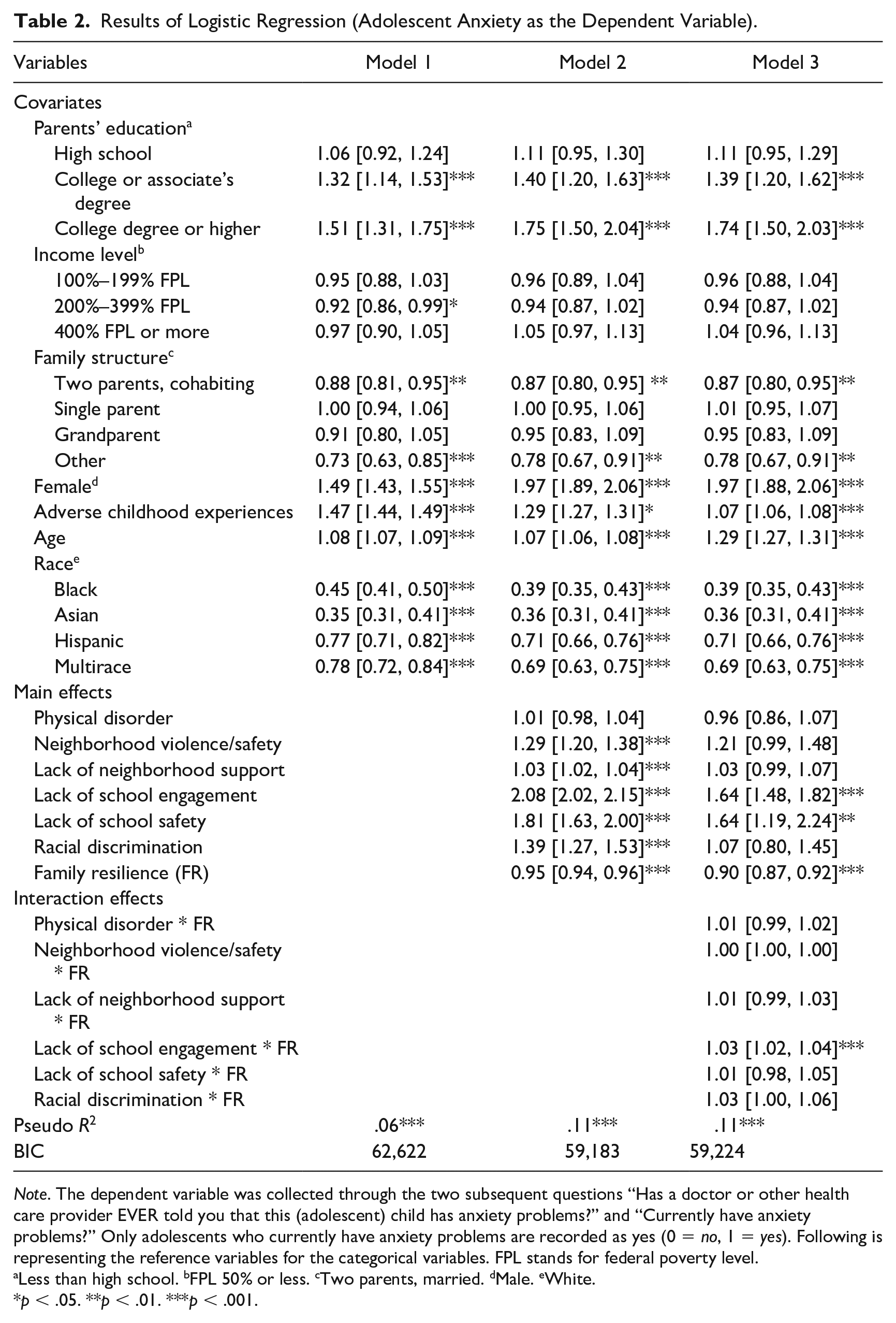
Note. The dependent variable was collected through the two subsequent questions “Has a doctor or other health care provider EVER told you that this (adolescent) child has anxiety problems?” and “Currently have anxiety problems?” Only adolescents who currently have anxiety problems are recorded as yes (0 = no, 1 = yes). Following is representing the reference variables for the categorical variables. FPL stands for federal poverty level.
Less than high school. bFPL 50% or less. cTwo parents, married. dMale. eWhite.
p < .05. **p < .01. ***p < .001.
In Model 2, a 1-point increase in the neighborhood violence/safety score was associated with 1.29 times (95% CI = [1.20, 1.38] higher odds of experiencing anxiety. Every 1-point increase in the lack of neighborhood support score was associated with 1.03 times (95% CI = [1.02, 1.04] higher odds of experiencing anxiety. Adolescents with a lack of school engagement had 2.08 times (95% CI = [2.02, 2.15] higher odds of experiencing anxiety. Adolescents with a lack of school safety had 1.81 times (95% CI = [1.63, 2.00] higher odds of experiencing anxiety. Adolescents who reported experiencing racial discrimination had 1.39 times (95% CI = [1.27, 1.53] higher odds of experiencing anxiety. Whereas, a 1-point increase in family resilience was associated with 0.95 times (95% CI = [0.94, 0.96] lower odds of experiencing anxiety.
In Model 3, regarding the main effects, the associations between parental education, income level, family structure, gender, ACEs, age, race, and the odds of experiencing anxiety remained significant. However, neighborhood violence/safety, lack of neighborhood support, and racial discrimination were no longer significant. Regarding interaction effects, the interaction between lack of school engagement and family resilience was statistically significant (ORR: 1.03, 95% CI = [1.02, 1.04], indicating that the effect of lack of school engagement on anxiety changed as the level of family resilience varies. Subsequent analysis aims to explore the buffering effect of family resilience in relation to the lack of school engagement.
Figure 1 shows the interaction effect between family resilience and school engagement on anxiety. To facilitate the interpretation of the interaction effect of family resilience, we plotted the predicted probability of adolescent anxiety across three distinct groups scoring 1 SD below the mean (–1 SD, low), at the mean (mid), and 1 SD above the mean (+1 SD, high). The upper graph presents the original values, whereas the lower graph displays standardized results to illustrate the variations in the slope (Δy/Δx) among the three groups. Irrespective of the degree of school engagement, adolescents in the group with low family resilience exhibited the highest probability of experiencing anxiety. This was followed by those in the mid-family resilience group, with the high-family resilience group showing the lowest anxiety probabilities. Moreover, to visualize the slope better, the y values of all three groups were shifted to the origin. After standardizing the y-axis, the findings revealed that the likelihood of anxiety escalates in conjunction with increases in the lack of school engagement, from 1 to 3. This escalation corresponds to an increase in the probability of anxiety as measured by logistic regression. Specifically, there is an increase of .213 of the predicted probability in the group with low family resilience, .196 of the predicted probability in the group with mid-family resilience, and .185 of the predicted probability in the group with high family resilience. This means that the low–family resilience group exhibited a 2.8% greater increase in the probability of anxiety compared with the high-family resilience group across the observed range of the lack of school engagement. Similarly, this group experienced a 1.7% greater increase in anxiety probability compared with the mid-family resilience group. The mid-family resilience group showed a 1.1% greater increase than the high-family resilience group.
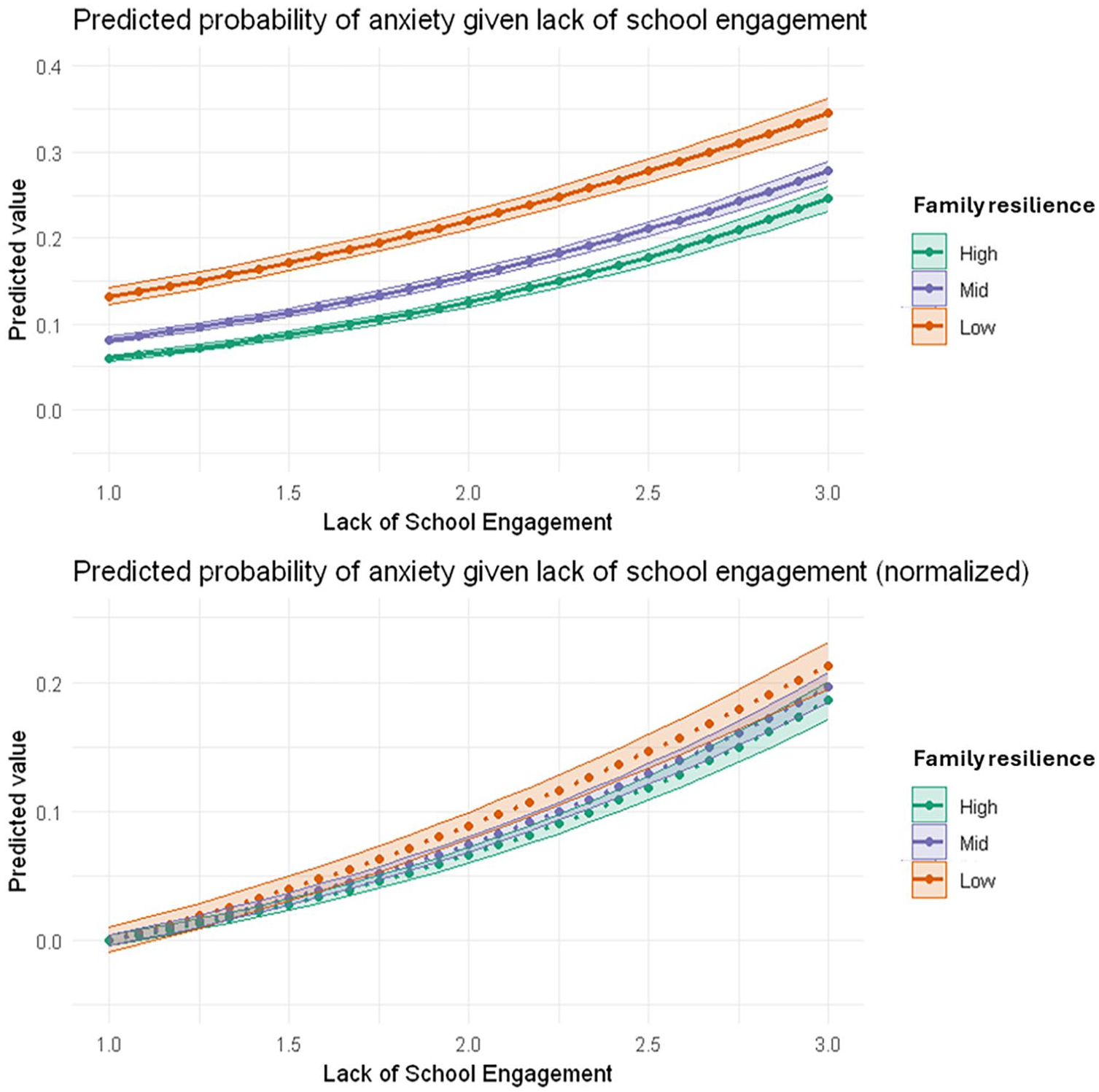
An Interaction Effect of Family Resilience and Lack of School Engagement on Probabilities of Anxiety: The Original Plot (Top) and the Normalized Plot to Compare the Slope.
Discussion
Risk Factors for Adolescent Anxiety
Guided by the built environment (Evans, 2003) and the family resilience theories (Walsh, 2015), this study used a nationally represented data set to examine risk across neighborhood, school, and racial discrimination and the buffering effect of family resilience on adolescent anxiety. Our findings suggest that roughly 16% of adolescents experienced anxiety, which was lower than the rate of 31.9% reported by NIMH (2023). The lower rate of anxiety in our study compared with the national rate may partially be explained by adolescents reluctant to discuss their mental health problems with their parents. Furthermore, because the data on adolescent anxiety were collected by being asked whether a doctor or health care professional told the parent that the adolescent child has anxiety, unless it was professionally recognized, the presence of adolescent anxiety could have been underreported, despite the presence. It should also be noted that because the source of adolescents came from parents’ response from a professional report, given the disparities in access to health care services and discrimination in the health care system, white youth might have turned out presenting higher rates of anxiety compared with their non-white counterparts, contradicting previous findings (Davis et al., 2017). Controlling for family-related ACEs, this study found that both neighborhood and school domains of risks were significant precursors of adolescent anxiety. Furthermore, family resilience had both promotive and protective effects on adolescent anxiety. More nuanced explanations are provided in the following.
Regarding our first research question, after controlling for demographic variables and family-related ACEs, neighborhood, school, and racial discrimination risks significantly increased adolescent anxiety. Within the neighborhood domain, neighborhood violence/safety issues and a lack of neighborhood support were found to be significant risk factors that increased anxiety among adolescents. A possible explanation may be that neighborhood violence and unsafe neighborhood environment are associated with high levels of increased hyperalertness, which may increase anxiety (Goldman-Mellor et al., 2016). Furthermore, consistent with Cutrona and colleagues (2019), adolescents who reported lower levels of neighborhood support experienced an elevated level of anxiety. Feeling unsupported by neighbors may lead to a lack of belongingness to the community, which may increase disconnected feelings. Particularly, adolescents are likely to expand their social network outside their homes, and the neighborhood is a critical domain for bonding. However, without appropriate support in the neighborhood, adolescents may be deprived of the opportunity to connect with others leading to an emotional state of feeling anxious. Meanwhile, inconsistent with Sampson et al. (2016), neighborhood physical disorder was not found to be a critical risk factor for adolescent anxiety. Overall, adolescents’ subjective experiences in their neighborhood, such as feeling unsupported and exposure to violence and unsafe environments, were salient risk factors for adolescent anxiety. Adolescents’ anxiety may be deeply associated with their perception of how closely they are connected with their neighbors and the safety they feel rather than the mere appearance of their neighborhood.
Furthermore, the school domain of risks was a critical precursor of adolescent anxiety. As many adolescents, except for homeschoolers, spend a large amount of time at school, lack of school engagement and lack of school safety were all significantly associated with adolescent anxiety. Adolescents’ lack of school engagement may lead to feelings of alienation at school and increase anxiety. Because adolescents gradually become emotionally independent from parents and build group identity with peers (Hazen et al., 2008), lacking school engagement may be a risk factor for increased anxiety. As adolescents may lose one of the most important grounds to build an identity with peers and achieve various academic and athletic goals, adolescents may feel they are lagging behind peers, resulting in an anxious state. Research supports that academic achievement has been found as a critical school-related stressor (Zhu et al., 2019), and feeling unengaged in school could predict greater social anxiety among adolescents. Furthermore, school violence and hate crimes have increased since 2016 (Edwards & Rushin, 2018). Due to various reasons (e.g., gang activities and gun violence), school safety has become a critical social issue. As appalling incidents of school safety issues are constantly broadcasted and shared on social media, adolescents’ awareness of school safety issues may increase concerns that keep them anxious at school. Despite the continuous effort to keep schools safe, schools are not necessarily safe although they should be. As a result, adolescents’ concern about safety at school elevated the risk of anxiety. When adolescents struggle academically or have challenges in building and maintaining healthy relationships with peers and teachers, they experience anxiety (Davis et al., 2017).
Finally, consistent with Priest and colleagues (2013), racial discrimination predicted anxiety among adolescents. As the United States has witnessed a rise in school violence and hate crimes since 2016 (Edwards & Rushin, 2018), racial discrimination has emerged as a systematic risk factor for anxiety. When the system fails to capture subtle acts, such as microaggressions, adolescents from socially marginalized groups may be exposed to higher risks of experiencing anxiety. Violence and microaggressions due to racial discrimination can leave adolescents powerless and hopeless leading to a state of anxiety.
Regarding the second research question, family resilience showed a promotive effect against adolescent anxiety. Consistent with prior studies (Finklestein et al., 2022; Song et al., 2021), adolescents in resilient families were less likely to experience mental health issues such as anxiety. As adolescents can have positive and functional interactions with their family members based on a sense of trust and care, they have a secure base in the family to decrease the risk of anxiety. As adolescents’ initial and enduring relationships begin within the family, a supportive and trustworthy family dynamic lays the essential groundwork for emotional stability. As Walsh (2015) explains, adolescents in resilient families are likely to have lower levels of emotional problems, such as anxiety.
Most importantly, regarding the third research question, the moderation analysis showed a more fine-grained narrative of to what extent family resilience can alleviate environmental risk factors in adolescents; family resilience was particularly protective against lack of school engagement. Although family resilience was not found to be a panacea against all the risks in the neighborhood or school, family resilience partially alleviated the negative impact of the lack of school engagement on adolescents’ anxiety. Considering that school engagement may stand out as an example of interactions with peers and teachers and getting involved in school activities, supportive and caring families may be an outlet for emotional distress regarding lack of engagement at school. Recognizing that effective family communication plays a crucial role in overcoming perceived challenges (Walsh, 2015), well-informed and affectionate parents can guide their adolescent child through difficult life situations. When parents show genuine interest and supportively interact in their adolescent child’s life, the family may become better equipped to address issues related to the adolescent’s disengagement from school. Given the multifaceted nature of reasons behind such disengagement, parents who remain vigilant about their child’s school experiences and stand ready to offer assistance can proactively explore alternative solutions. For example, parents who maintain a warm and caring connection with their adolescent child are more likely to discern the underlying causes of low school engagement. When parents interpret their child’s lack of school engagement as an initial indicator of potential negative developmental outcomes, they can collaborate with their child to explore alternative paths through open communication.
Despite the protective effect of family resilience, it was not found to moderate other risk factors that lead to adolescent anxiety. The negative effect of racial discrimination associated with anxiety may not be buffered by family resilience. The magnitude of racial discrimination remains highly alarming, particularly among adolescents. Adolescence is a period of self-awareness and identifying racial/ethnic identity becomes an important aspect in constructing self-identity. When adolescents, particularly those from minority groups, experience racial discrimination, family resilience is insufficient to resolve the stressors leading to anxiety.
Furthermore, family resilience did not buffer safety issues in both the neighborhood and school. Neighborhood risk factors may be an inveterate issue of adolescent anxiety. Neighborhood violence, safety issues, and lack of neighborhood support are prominent examples of a lack of social capital. Adolescents’ daily interaction and exposure within their neighborhood environment is a critical domain that may relate to their mental health. Violence, safety issues, and lack of neighborhood support may go beyond the capacity of family resilience. Particularly, school safety has long become a serious public issue. As family resilience was not found to protect adolescent anxiety against the aforementioned risk factors, a systematic endeavor should be necessary to deal with the structural issues that increase adolescent anxiety.
Limitations
Study limitations should be noted. First, although we aggregated 5 years of the data set in NSCH, we could not examine the longitudinal effect of the association among the variables. Hence, the causality among the variables cannot be inferred. Future research is recommended to examine the relationships among the variables using longitudinal data sets. Second, the responses were reported by the adolescent child’s primary caregiver. Therefore, the source of information may contain biased information. Diversifying the sources of responses, including adolescents, teachers, and peers is suggested. Third, teacher turnover rates have been discussed to be a critical risk factor for adolescent mental health. However, our data set did not include teachers’ turnover rates. As the interactions between teachers and adolescents are frequent and common, future studies should include variables considering the interactions. Fourth, the study sample was majority white (70%), which may not fully represent the experiences of minority adolescents. In addition, minority youth are likely to be exposed to racial discrimination more often than their white counterparts. Hence, group analysis based on race/ethnicity could further explain a more subtle narrative in adolescent anxiety. Fifth, qualitative data could further provide in-depth information about how family dynamics can help youth in preventing and alleviating anxiety caused by built environment risk factors. Finally, the adolescent’s anxiety variable was measured based on a single, parent-reported item asking whether “a doctor or other health care provider has told the parent their child has anxiety.” Given racial bias in diagnosing, racism in health care and historic mistrust of the medical system among racialized groups and racial disparities in access to mental health care, basing anxiety on it being recognized by a doctor or health care provider poses a limitation and could explain why non-white adolescents had lower levels of anxiety on this variable. Essentially, non-white adolescents might actually have higher anxiety, but due to these systemic factors, it may not have been recognized by a doctor or health care provider. Overall, assessing anxiety with a more formal instrument using various data sources would strengthen the quality of the data compared with the single parent–report item used in this study.
Implications for Practice
Controlling for family-related ACEs, our study found that family resilience has both promotive and protective factors. Practitioners should be aware that high level of family resilience itself may lead to a lower level of anxiety among adolescents. Although adolescence is a period of expanding social networks beyond family domain, family resilience still plays a significant promotive role in reducing adolescents’ anxiety. Furthermore, what is more promising is that family resilience may effectively reduce risk factors experienced outside the family domain such as lack of school engagement. Although the protective effect of family resilience was not dramatic as expected, high family resilience can reduce the risk of adolescent anxiety by 2.8% compared with those with low family resilience. It is worth noting that the emotional support and resources that families provide can reduce adolescent anxiety that is associated with lack of school engagement. When adolescents are having trouble engaging in school activities, family members may provide possible alternatives so that adolescents may be protected by experiencing anxiety. Particularly, it should be noted that families who have healthy communication skills and are willing to support their adolescent child may provide and search for alternative activities and provide information for their adolescent child. Although adolescents failing at school may experience anxiety (Zhu et al., 2019), adolescents with family members prepared to emotionally support them and provide external sources were likelier to feel less anxious. Lareau (2011) explains that families with resources and support can provide abundant chances to help children overcome various life challenges. A comprehensive approach to improve the family dynamics through family therapy or education may help to improve family resilience (Walsh, 2015). Adolescents with family support and resources are likely to find alternative options for lacking school engagement, such as tutoring and other extracurricular activities outside the school.
Conclusion
To our knowledge, this is one of the few studies that examined the buffering effect of family resilience in the context of the neighborhood and school domains among adolescents. As adolescents are in the developmental period of becoming independent and building identity by interacting with their peers and achieving various goals, underlying risk factors in neighborhoods and schools are likely to increase anxiety among adolescents. However, despite the inveterate risk factors in the neighborhood and schools, resilient families were likely to decrease adolescents’ anxiety (promotive effect). Furthermore, the risk of limited school engagement can be buffered by healthy and functional family interactions (protective effect). Considering that youth living in marginalized neighborhoods and attending under-resourced schools, which can hardly be improved within a short-term period, are exposed to elevated levels of risk, direct family-level interventions may provide support that buffers the immediate risk from the built environment. For example, structural family therapy has been extensively applied to marginalized populations. Minuchin and colleagues (2013) have extensively provided structural family therapy to families of the poor and found it effective in alleviating mental health problems. Training school and community social workers with family therapy or counseling can enhance intervention skills to improve family resilience. However, it should be noted that structural issues of lack of social capital and safety concerns within both neighborhoods and schools may call for a macro level of structural change to reduce adolescent anxiety.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.