
Abstract
The way through first suspicion of developmental delays to the time a diagnosis of autism is confirmed can be a long and emotional road. Additional challenges are faced by families with an immigrant background who must learn to navigate an unfamiliar health and social service care system. The current study aims to document the variability of emotional experiences reported by parents with an immigrant background through the autism service trajectory, from the first suspicions of a developmental delay to school entry. Eighteen families participated in two semistructured interviews regarding their autism service trajectory. By using an inductive qualitative content analysis, findings revealed specific contexts in which strong emotional experiences were expressed and made it possible to identify targets for intervention at key moments to support parental psychological well-being.
Early childhood (i.e., 0–6 years) is a time of intense adaptation for all families, where parents are adapting to their new role as well as reorganizing the family system while dealing with emotional and health-related changes (Chatenoud et al., 2014; Keen et al., 2010; Mello et al., 2022; Rivard et al., 2021a). The intensity and extent of these adaptations may be exacerbated for parents who suspect their child has a developmental delay. They can quickly find themselves in a spiral of service and assessment requests within a complex and limitedly accessible health and social service care system. These additional challenges in early childhood are compounded by the intense emotions and high level of stress a parent may feel when they are left waiting for a diagnosis and appropriate supports, and this is especially true for parents whose children will be diagnosed with autism spectrum disorder (ASD; see Brewer, 2018). From the moment of initial concern, parents begin the process of navigating through a series of stages like the assessment and diagnostic processes, the search for services and wait lists for access to these services, early intervention (e.g., early intensive behavioral intervention [EIBI]), and the transition to school. This whole rollercoaster does not come without its share of intense emotions that have the potential to undermine the psychological well-being of parents.
Navigating through those many stages involved in supporting a child with ASD can be even more complex and requires a greater capacity for adaptation for families who have left their country of origin (Mandell et al., 2020; Stahmer et al., 2019). For instance, parents with an immigrant background who have a child with ASD must find their way through an unfamiliar health and social service system in a language that often differs from their native tongue in addition to having to reconcile differences in value systems and educational approaches. These challenges tend to be intensified by a lack of support from familial and social networks which parents would have otherwise been able to rely on in their country of origin (Rivard et al., 2021a; Mandell et al., 2020).
The parents’ experience following the confirmation of an ASD diagnosis for their child is well-documented (Boshoff et al., 2018; Corcoran et al., 2015; Makino et al., 2021; Potter, 2016). Few studies, however, capture the diversity and evolving nature of parents’ emotional experiences as they travel through the autism service trajectory, even less among families who face additional and highly specific immigrant-related challenges (Rivard et al., 2019, 2020). The subjective perception a person has of their experience (i.e., the narrative that one creates around their experience) and their emotional experiences evolve over time, and this has the potential to weaken or strengthen psychological well-being (Coyne et al., 2021). Investigating the variability of these emotional experiences across early childhood would allow for a better understanding of the realities of families with an immigrant background who face challenges associated with raising a child with ASD. As such, the present study aims to document the diversity and evolution of these emotional experiences reported by parents with an immigrant background through the different stages of the autism service trajectory, from the first suspicions of a developmental delay to school entry.
Emotional Experience of Parents of Young Children With ASD
Researchers have documented parent perspectives related to the diagnostic process, waiting periods, early intervention services, and the transition to school (Brewer, 2018; Ooi et al., 2016). Some of these studies reveal the emotions felt by parents following the diagnostic confirmation which include frustration, anger, guilt, fear, helplessness, discouragement, sadness, denial, or loss of hope (Brewer, 2018; Makino et al., 2021; Ooi et al., 2016). Studies have also revealed that parents may experience mental health issues, including significant depressive symptoms (Makino et al., 2021).
The waiting period between the time a diagnosis is received and the start of early intervention services like EIBI can be as long as 2 years, often leaving parents without interim support (Austin et al., 2016; Boshoff et al., 2019). This has the potential of increasing parental stress, exhaustion, and feelings of frustration and helplessness (Brewer, 2018; McKinsey, 2014; Ooi et al., 2016). Obtaining specialized services can be resource intensive for parents. Moreover, these services are typically child-centered (e.g., developmental needs, autism symptoms) and overlook the parents’ own psychological well-being in the process (Frantz et al., 2018; Grindle et al., 2009). While parents may be satisfied with specialized intervention services (e.g., EIBI; Lovaas et al., 1981) once received, they continue to report their own personal psychological difficulties (e.g., adjusting to their new reality) for which little support is provided (Quebec Ombudsman, 2012; Rivard et al., 2014).
The termination of early intervention services (i.e., prior to school entry in Quebec) and the transition to school is a challenge that can be a considerable source of anxiety and adjustment for families of children with ASD (Janus et al., 2008; Rivard et al., 2020). Specialized services within the education system can vary substantially across different areas based on the service model adopted by a given country, region, or even neighborhood (Chatenoud et al., 2019; Ouellette-Kuntz et al., 2009). Many parents feel that schools are not necessarily equipped to properly support children with ASD, both in terms of the availability of material and human resources and the school professionals’ lack of expertise (Ooi et al., 2016). Families report that early intervention professionals’ involvement eased the transition process at school entry and parents felt supported (Chatenoud et al., 2019).
Studies underscore the importance of documenting not only emotional challenges but also positive emotional experiences, family strengths, facilitating factors, and coping strategies which have the potential to alleviate stress levels (Hastings & Brown, 2021; Waizbard-Bartov et al., 2019). Families recognize their child’s unique qualities, intelligence, and displays of affection, and report being grateful for the experience regardless of diagnosis (Ooi et al., 2016). Some parents reported that having a child with ASD changed their perception of their child’s development and provided them with a sense of empowerment and greater insight, which in turn facilitated their capacity for adaptation (Waizbard-Bartov et al., 2019). Some families also demonstrate a great deal of resilience, allowing them to overcome adversity in various challenging contexts (Bayat, 2007). Commonly referred to as individual’s capacity for positive adaptation in face of adversity (Luthar & Cicchetti, 2000), resilience can act as an important protective factor helping one to overcome the emotional demands of a challenging situation (Bitsika et al., 2013).
The diversity and intensity of emotions experienced thus seems to fluctuate with the different transitions that families experience throughout the autism service trajectory, such as between diagnosis disclosure and the beginning of specialized early intervention like EIBI. However, no study to our knowledge documents this longitudinally. Also, a variety of emotions may coexist, and these emotions may have several adaptive functions depending on a given context. For example, a parent’s anger at having to wait for services may help them advocate in defense of their child’s rights (Camard et al., 2022). These emotions can also be influenced based on a parent’s internal representation or subjective perception of their specific situation (Coyne et al., 2021). Some families compare all of these varied emotional experiences, such as frustration, joy, or sadness, with a roller coaster (Makino et al., 2021). This complex emotional experience lived by parents highlights the importance of documenting their experience longitudinally and from a variable perspective to better target the supports needed to maintain parents’ psychological well-being in a context where little support is specifically dedicated to them.
Autism Service Trajectory for Families With Immigrant Backgrounds in Early Childhood
Studies of immigrant and ethnic/cultural minority families report various barriers to accessing formal supports such as specialized autism assessments and intervention services (Gupta & Parisi, 2020; Mandell et al., 2020). These include language barriers, challenges in navigating service systems, and differences in intervention priorities and approaches across cultures (King & Bearman, 2011; Pickard & Ingersoll, 2016; Stahmer et al., 2019). Studies also report that families with an immigrant background are at higher risks to receive poorer quality services, including longer wait times, interventions lacking culturally sensitive practices, or interventions that do not reflect research-based best practices (Cho et al., 2003; Rivard et al., 2021b). These challenges can have a significant impact on the emotional experience of families and can be detrimental to the psychological health of parents.
Access to informal support, such as family, friends, or the community, is beneficial for families’ adaptation and would improve resilience (Bekhet et al., 2012; Fong et al., 2021; Shivers et al., 2017; Zauszniewski et al., 2010). For a family with a child with ASD, having access to some type of informal support, such as parent groups on social networks, allows them to share the difficulties they may experience on a daily basis and sometimes gives them access to information that is difficult to find within the public service network (Stahmer et al., 2019). These informal exchanges can encourage parents to learn about the different services and supports available and to take the necessary steps to obtain the services to which their child and family are entitled (Chatenoud et al., 2019). Moreover, connecting with other families who are going through a similar experience promotes the search for services and solutions, and offers support that is sensitive to the parents’ realities (Des Rivières-Pigeons et al., 2012). Social support has been identified as a key factor in the quality of life and well-being of families with a child with ASD (Millau et al., 2019; Samadi & McConkey, 2014). Families with an immigrant background who are raising a child with ASD are at greater risk of experiencing isolation or feeling misunderstood by members of their own family (Ijalba, 2016). These families may also have difficulty creating a support network within their new communities because of cultural differences or language barriers, which can compromise psychological health and make their journey throughout the autism service trajectory even more difficult (Rivard et al., 2021b).
To provide a clearer picture of the experience of families with an immigrant background along the autism service trajectory, a larger longitudinal study was conducted allowing 18 families to share (a) the various barriers and facilitators encountered from the moment of parents’ initial suspicions of a developmental delay to the time of diagnosis (see Rivard et al., 2019), (b) the times at which they were able to benefit from the recommended early intervention services within the public sector (EIBI; see Rivard et al., 2021a), and (c) their experience with the transition to school (see Rivard et al., 2021a). Investigation of these exchanges revealed that many parents also spontaneously reported the importance of developing their advocacy skills to gain access to assessment and intervention services for their child (Camard et al., 2022). As part of this larger longitudinal project, the present study aims to specifically focus on parents’ emotional experiences as they navigate through the autism service trajectory starting from the moment of their first concerns regarding their child’s development to school entry.
Purpose of Study
To better understand the diversity and variability in the emotional experiences of parents throughout the autism service trajectory in early childhood, this longitudinal qualitative study sought to map out the specific context in which heightened emotionality was reported. Based on the emotional experiences shared by families throughout the course of their autism service trajectory, clinical recommendations can be given to health and social service providers such that time-sensitive supports are offered to parents.
Method
To meet the purpose of the study, two semistructured interviews were conducted regarding the autism service trajectory with families with an immigrant background, and inductive qualitative content analysis was chosen to extract the parents’ emotional experiences.
Research Tools
Sociodemographic Questionnaire
The sociodemographic questionnaire was based on the Rivard and colleagues (2015) questionnaire and sociodemographic information collected relating to several factors such as family type, siblings, diagnosis and co-occurring disorders, socioeconomic status, education level, occupation, place of birth, and language spoken.
First Interview: From the Initial Suspicions of Developmental Delays to Diagnostic Confirmation
Parents’ perceptions and experiences of barriers and facilitators encountered during their child’s diagnostic evaluation process were documented through a semistructured interview averaging 90 min in length. The overall interview covered three themes: (a) the perception of ASD, (b) ASD diagnostic trajectory, and (c) family immigration history. This interview guide was developed by two of the researchers and reviewed by a committee consisting of an expert in pediatric ASD intervention, an expert in qualitative research, and an expert in program evaluation. The guide was reviewed and adjusted based on the proposed recommendations and pretested with a single participant to ensure that the questions would be understood. During the pretest, the participant mother was asked to indicate if there was any ambiguity in the wording of sentences, if they caused discomfort, or if she observed any lack of clarity in the interview process. No changes to the interview model or methods were deemed necessary by this participant.
Second Interview: Postdiagnostic Service Trajectory, Early Intervention Services, and Transition to School
A year later, a second interview consisting of 39 questions averaging 90 min in length was conducted with the same families. These questions fell within four general themes: (a) waiting period for early intervention services, (b) early intervention services, (c) termination of early intervention services, and (d) transition to school. Families were asked what facilitated the termination of early intervention services and the transition to school, as well as what made this period of time more difficult. They were also asked about the quality of their relationship with service providing professionals as well as the quality of the partnerships between institutions (e.g., rehabilitation center–school). As with the first set of interviews, this interview was developed by two of the authors and reviewed by a committee consisting of an expert in pediatric ASD intervention, an expert in qualitative research, and an expert in program evaluation. This interview was also pretested with a participant mother. No modifications to the model or interview methods were deemed necessary by the participant.
Procedure
To participate, one parent had to be a first-generation immigrant who was able to speak either English or French and families had to have a child with a formal diagnosis of ASD in accordance with the College of Physicians and College of Psychologists practice standards (2012). Families whose children had been diagnosed with ASD by a multidisciplinary team were recruited for the longitudinal study from two public rehabilitation centers for intellectual disability (ID) and ASD in the Montreal, Quebec, area. The supervisors responsible for overseeing the delivery of specialized services shared the contact information of families meeting inclusion criteria who expressed interest in participating in the study and consented to being contacted by the research team. A research assistant got in touch with the families to provide a brief description of the project, and initial meetings were scheduled with families who still wished to participate. At this first meeting, the parents reviewed the study’s information and consent form which was signed before beginning the interview. Sociodemographic questionnaire was then filled. One year after the first interview, the parents were contacted for the second interview regarding services received, the termination of services, and the transition to school. Three doctoral research assistants in psychology conducted these interviews in French (n = 17) and English (mixed English and French; n = 1). The interviews were transcribed by two research assistants for qualitative analysis.
Analysis
Transcripts of all interviews were imported into NVivo software (QSR International, 2012) for content analysis. The content analysis model proposed by L’Écuyer (1990) was followed. Categories were induced from the material analyzed by successive grouping of statements based on their relatedness or similarity of meaning to others. An initial reading of the interview transcripts was conducted by the first author to identify any units of meaning that expressed parents’ emotional experiences. For example, sentences with terms such as “it was difficult,” “we felt exhausted,” or “I cried all the time” were extracted from the interview verbatims. These units of meaning were reviewed and approved by the second author. Because emotional experience is a subjective phenomenon that may be subject to coder bias (L’Écuyer, 1990) or may require inference, the units of meaning were grouped according to their similar context to create categories of emotional contexts, rather than by categories representing emotions. For example, rather than inferring that the unit of meaning “I cried all the time” expresses sadness, exhaustion, or severe depression, which would require inference as the emotion is not clearly expressed by the parent, the families’ emotional discourse was instead classified according to the context in which it was expressed (e.g., at the time of the diagnostic confirmation).
Following this step, an empty grid with the general contexts created was given to a research assistant trained in qualitative analysis who classified 10% of the units of meaning. An encoding comparison of the classifications of the first author and the research assistant was performed to check for discrepancies. If a sorting decision diverged or if disagreement emerged in relation to the defined contexts, this was discussed to arrive at a consensus and final broad contexts. Once the broad contexts were refined, the units of meaning contained in each context were reviewed to generate subcontexts (i.e., more specific contexts) in an inductive manner grouped according to their similarities. Following the same process as the broader contexts, subcontexts were discussed, specified, modified, or defined by the first author and the research assistant. The purpose of this encoding comparison step is to ensure that each subcategory is mutually exclusive, clear, and precise. Following this meeting, some of the subcontexts were refined to arrive at the final grid. Following review of the final grid, the first two authors opted to add a discriminative code, allowing the authors to determine whether the emotional experience expressed by the families reflected a difficult or positive experience for them, a demonstration of resilience, or a functional or adaptive response based on those contexts (see Table 1). To arrive at the final results, the contexts were reviewed for the final classification.
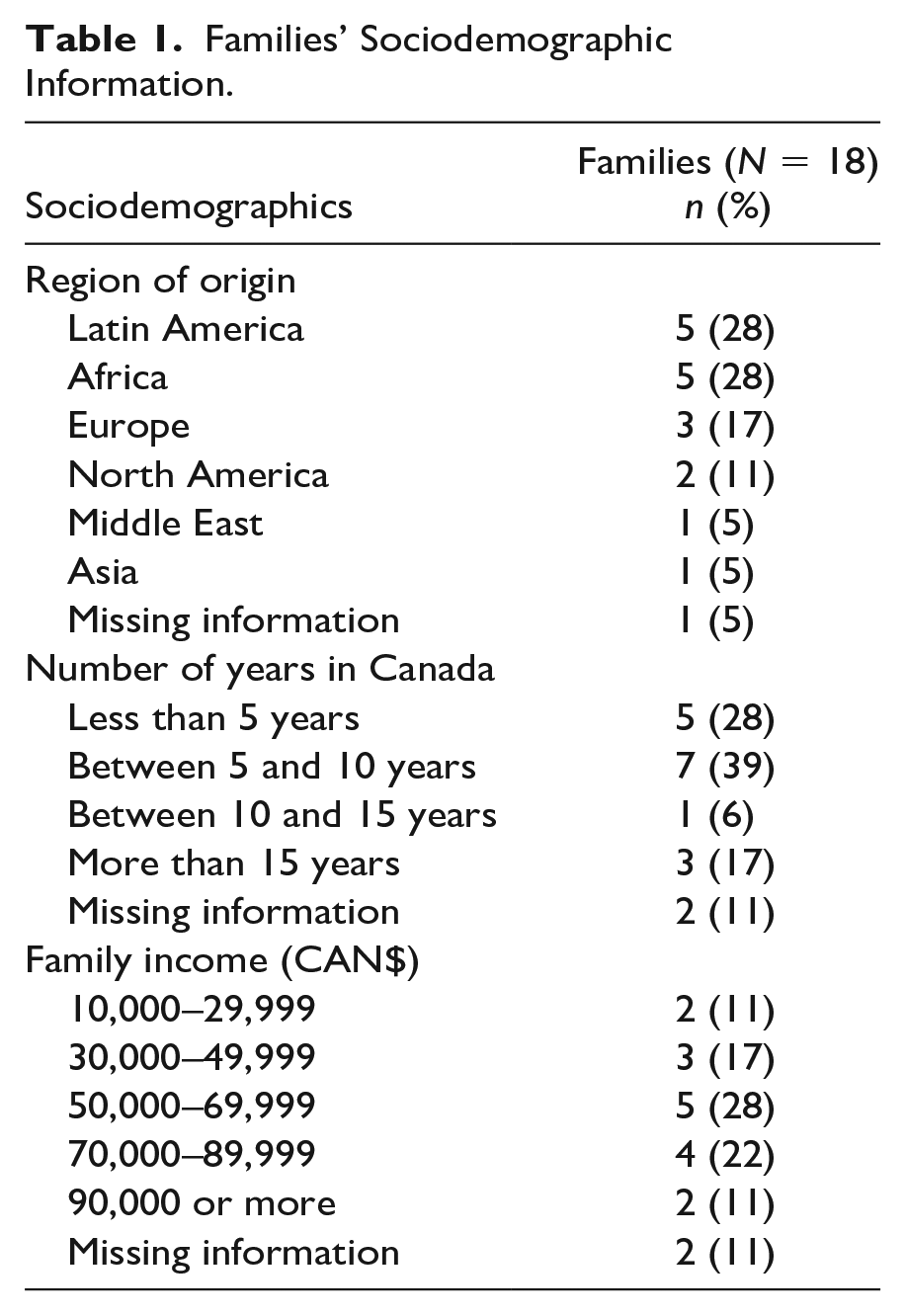
Families’ Sociodemographic Information.
Results
An inductive qualitative content analysis was used to extract data from two semistructured interviews conducted with families with an immigrant background. Participants’ sociodemographic data were gathered using a questionnaire at the first meeting.
Participants’ Data
Eighteen families participated in two semistructured interviews regarding their autism services trajectory. Most families were composed of the child’s biological father and mother (n = 16), while two families were single-parent families. More than half of the fathers (n = 7) and mothers (n = 13) had a university education. Information is missing for one family. For more information on sociodemographic information of participants, see Table 2.
Contexts Reflecting Emotional Experience in Families.
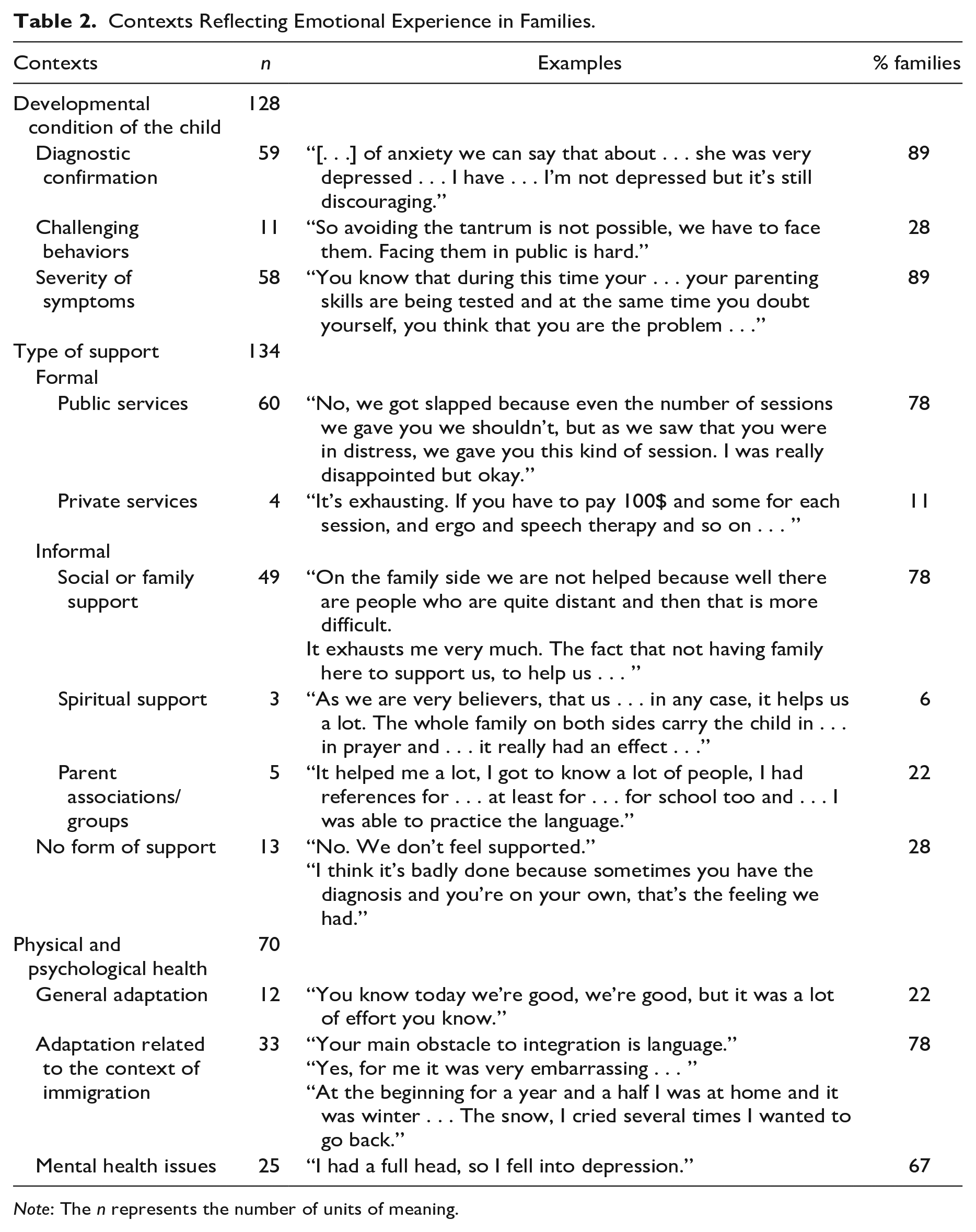
Note: The n represents the number of units of meaning.
Qualitative Data
An initial grouping of units of meaning was made according to the similar contexts in which emotional discourse was expressed by families. A total of 342 units of meaning reflecting an emotional experience were extracted from the 18 interview verbatims (see Table 3 for details). Three main contexts emerged: (a) the child’s developmental condition, (b) the availability of formal or informal supports, and (c) the parents’ general physical and psychological health. The results of each of these contexts are presented below.
Tone of Extracted Units of Meaning by Context.
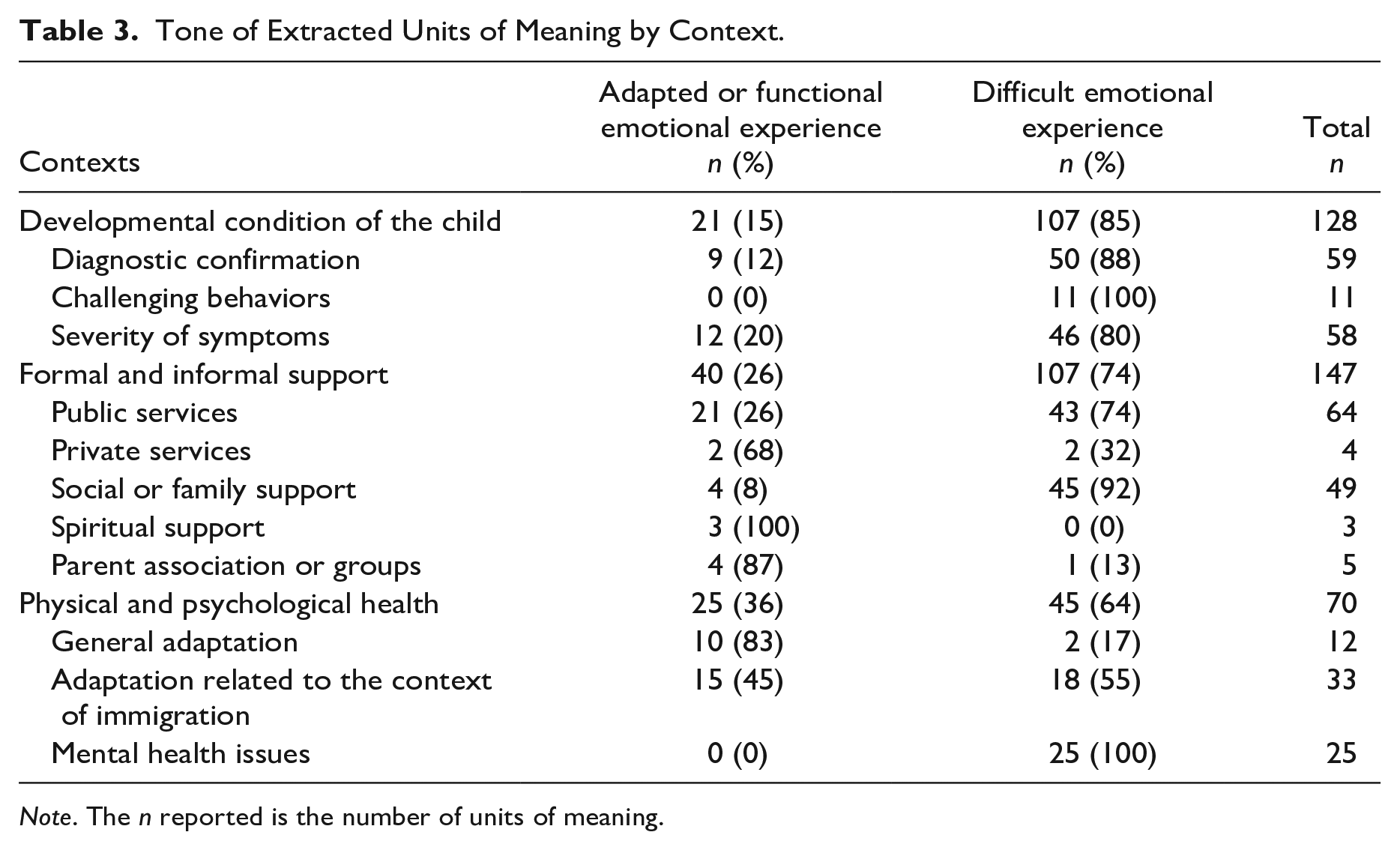
Note. The n reported is the number of units of meaning.
The Child’s Developmental Condition
A total of 128 units of meaning expressing an emotional experience related to the child’s developmental condition were extracted. The developmental condition context includes everything from the earliest suspicions of a developmental delay to the assessment and diagnostic period and the child’s day-to-day functioning. The assessment and diagnostic periods are included here to distinguish between the emotional experience directly related to the child’s development and the emotional experience expressed in relation to the professionals encountered or the services obtained (see formal and informal support). As such, the focus in this section is on the emotional experience of parents in relation to their child’s autism diagnosis or the behaviors exhibited by the child that may be associated with this diagnosis. Three subcontexts emerged from the parents’ emotional discourse: (a) the child’s diagnosis of autism, (b) the presence of challenging behaviors, and (c) the severity of their child’s symptoms.
When asked about the period of time revolving around their child’s diagnosis of autism, 16 families adopted a discourse reflecting a difficult emotional experience, such as sadness, anger, or denial: “I started to cry. You see it in black and white, it’s not easy.” Their child’s diagnostic confirmation is an upsetting and difficult reality for families to accept: “Plus, after I got the diagnosis, I told you, for me it wasn’t final. Why do I have to believe it, in two years it will go away?” Five of these families express relief or validation of their concerns that coexist with more difficult experiences: “We weren’t surprised. No, I would even say a little relieved.”
Sixteen families expressed an emotional discourse when they discussed the severity of their child’s ASD symptoms. For example, one parent mentioned that their child’s lack of communication skills is particularly difficult and makes them apprehensive about their child’s future independence: “My big fear is rather that his future development will not be satisfactory for him.” A total of nine families expressed concern about their child’s future: “The biggest fear is that he’ll be . . . also that he won’t be able to . . . integrate into society there like when we won’t be there anymore.” Finally, four families expressed guilt related to their child’s condition: “I try to stop feeling guilty too, because during the pregnancy I experienced a lot, a lot of stress.”
Families expressed emotions related to managing challenging behaviors such as sleeping and eating difficulties, aggressive behaviors toward self or others, and frequent tantrums. Five parents reported that their lives are affected on daily basis and that this has an impact on the well-being of the whole family: This is our life every day. It is a madness. . . . That’s not how life is. But we have to have respite and we can’t get respite. It’s not my son’s fault, but . . . we can’t breathe a little.
Families also reported that the lack of behavior management support led them to feel isolated. Some families declined invitations from other parents for fear that their child would have a meltdown, as they recall feeling judged: “Even outings, traveling, walking, because it was the crisis. . . . We stopped going out, we stopped everything, everything. And we started to lose a lot of friends.” The presence of challenging behaviors seems to lead some families to have a more negative experience with regard to their child’s difficulties: Because at night he didn’t sleep so we [don’t]. . . . Since he walks . . . my feet hurt so much. So down there, it’s open space. I walk back and forth in the kitchen, I’m tired.
However, among these difficult conversations, six families mention having accepted their child as they are, being able to appreciate and see the moments of joy, and not wanting to change their child: “I’m so happy with my daughter, that if someone had a magic wand and they told me they touched her and she became a child like everyone else, I’d rather she stayed the way she is.”
Formal and Informal Support
Families’ emotional experience in accessing formal and informal supports was spontaneously reported in the parents’ discourse, and several subcontexts associated to this broader theme emerged. Formal support includes public and private services: diagnostic assessment, specialized intervention (e.g., EIBI), family support (e.g., parent coaching or psychological support) or any consultation with a pediatrician, speech therapy, occupational therapy, and so on. Formal support is generally provided by facilities such as hospitals, local community service centers, rehabilitation centers, or private clinics. Informal support refers to any form of support that does not consist of services provided by health or education professionals such as support from family members or friends, a religious or spiritual community, and parent associations, social networks, or independent internet research.
Regarding formal support, a total of 64 units of meaning was extracted. Dissatisfaction was expressed about wait times and the lack of guidance as to where to access information or what steps to take: “So we had a lot of expectations concerning the [rehabilitation center] and we wanted to have access to it, so we were already very disappointed to be on waiting lists.” Some families also mentioned that they felt invalidated by their pediatrician: “Until then, everyone, even the pediatrician, was us. It was our fault. We were too demanding, we were exaggerating. . . . So, we were misunderstood I think.” Some families are also affected by the fact that public services are difficult to access: “I also find it revolting to be told to go to private services. I don’t think it’s right, on principle I don’t want to do that.”
On the contrary, other families reported feeling supported by their child’s therapist: “they were always open to answering my questions, and they offered me advice, little advice documents after I received the diagnosis, I was very happy.” Seven families noted positive experience with public services, leading them to report a sense of reassurance or support. When talking about a professional in a rehabilitation center, one family mentioned, “She calmed us down a lot, we felt understood, listened to, she accompanied us, supported us.”
A total of 54 units of meaning expressed emotional experience regarding informal support. More specifically, 14 families reported an emotion related to the presence or absence of family or social support. For half of them, a feeling of loneliness was expressed: “We are isolated, period.” These parents reported feeling isolated, judged, and misunderstood by other family members: “I can’t say they are able to support me. I don’t know, it’s hard.” Two families reported not talking to other family members about their child’s diagnosis because of their feeling of discomfort or their fear of being misunderstood: “We didn’t see any benefit in sharing this information, because we knew that they wouldn’t understand”; “We went through a lot of difficulties, so we didn’t talk because we didn’t want to worry people either.” Conversely, three families mentioned that frequent calls from their loved ones is an important source of support on a daily basis: All of our two families uh are aware, the reaction has been, uh . . . difficult precisely it’s a . . . it’s news that is not . . . pleasant so . . . . It’s the whole family that calls, that supports.
Regarding social support, nine families mention not having friends in the area in which they settled: “We’re alone”; “Yeah, here on the South Shore, I don’t know anybody. So, I could try a little bit to have contacts, but it’s hard, because I don’t go out, I don’t work.” Three families, however, reported that they were able to create a support network and felt surrounded.
The immigration context is salient in the parents’ discourse when they talk about social and family support, with one family mentioning, “It was difficult. I don’t think for anyone it was easy, it’s always hard to leave your parents and then find your place here.” Four families reported that seeking support from associations, parent groups, or through social networks was beneficial for them: [We heard] testimonies from parents that maybe it’s been a year, two years that have been in there [and] to tell us you know what . . . the world isn’t falling apart, your son [is] alive . . . there is hope.
Finally, one family mentioned turning to their religious community or spirituality to feel supported or for appeasement: “Since we are very religious it helps us . . . in any case it helps us a lot. The whole family . . . carries the child in prayer.”
Parents’ General Physical and Psychological Health
A total of 70 units of meaning expressed emotional experiences in the context of the parents’ general physical and psychological health. Four specific subcontexts not directly expressed in relation to their child’s condition or diagnosis emerged: (a) general adjustment, (b) adjustment related to the immigration context, and (c) mental health issues.
Eight families talked about their current level of adaptation, whether psychological or cultural. In fact, four families expressed the fact that they were doing better or that they were “trying to find solutions . . . to be able to function” or to put forward that “it was a lot of effort” to adapt. Some families reported that, overall, their psychological health had improved since their arrival in Canada and since their child’s diagnosis of autism: “today, we’re better”; “I’m happy now, yeah.”
Several emotional experiences were expressed when parents spoke of their immigrant reality. For example, one mother expressed that the language barrier was “embarrassing” for her and was an obstacle to her adaptation. Another parent said, “when I arrived, my ears couldn’t hear anything, I couldn’t understand anything. So, it was hard at first.” Two families mentioned the difficulties they had in adapting to the climate of their new country: “the snow, I cried several times I wanted to go back.”
Eleven families reported having experienced personal mental health issues following the diagnosis period. Three parents reported having received a formal diagnosis of depression, and six families reported experiencing significant general exhaustion. One mother recounted the impact her physical and psychological health had on her work: because I doze off, because I’m not focused. And I make careless mistakes at work and that creates tension with my superiors. I had problems with my superiors because I was tired at work and I . . . I got upset.
Discussion
Raising a child with ASD brings its share of challenges and joys for all family members (Chatenoud et al., 2014; Hastings & Brown, 2021; Keen et al., 2010). When parents first become concerned by their child’s developmental delays, they can quickly find themselves in a whirlwind of unknowns and fears, and they must initiate a process that has the potential to undermine their psychological well-being as it requires adaptation on many levels. They are required to become their child’s caregivers, while carrying out their responsibilities as new parents and coming to terms with their child’s developmental reality (Mandell et al., 2020; Stahmer et al., 2019). This could have a toll emotionally and physically and yet studies pinpoint the importance of direct services for parents, to support their psychological well-being, and enhance their parental availability to undergo through the navigation of services for their child (Frantz et al., 2018). However, few studies on families with an immigrant background having a child with ASD capture the complexity of their reality with an inductive qualitative method. With this goal in mind, the current study gave us a portrait of the variance in emotional experiences in a longitudinal perspective and identified delicate contexts where different types of support should be offered.
Implications for Practice
It is important for service providers to recognize the unique needs and experiences of families with an immigrant background who have a child with ASD and to take steps to provide culturally sensitive, accessible, and emotionally supportive services.
Supporting Parents’ Emotional Experience Related to the Child’s Needs and Diagnosis
Previous studies have found that a reciprocal relationship exists between mental health indicators, such as parental stress, and child behavior, underscoring the importance of supporting parental psychological well-being (Alostaz et al., 2022; Ooi et al., 2016; Smith et al., 2008). In the current study, three ASD-related difficulties cause parents to feel emotionally burdened: (a) their experience with the diagnosis itself, (b) the consequences of challenging behaviors, and (c) the effects of the severity of the symptoms and intensity of their child’s needs. The findings imply that to better support parents, it is important to concentrate on these different components that can be brought with the ASD construct at diagnosis disclosure by professionals.
Regarding the diagnosis itself, some studies show that acceptance of the diagnosis is a mediator of psychological well-being (Bayat, 2007; MacDonald & Hastings, 2010; Retzlaff, 2007). Nuancing what acceptance represents individually would be essential to better tailor the support needed by a parent. As health care professionals, it seems crucial to concentrate on what an ASD diagnosis means for each parent, to intervene and provide tailored assistance based on their comprehension of the diagnosis, what they know about it, but most importantly how they feel about receiving the diagnosis for their child. Path to acceptance, but mostly accepting having to face such adaptation, is not linear, and awareness of the variety of emotions that can be experienced by parents (and sometimes the feeling of ambivalence that emerges when different emotional states coexist), should be the first step in any process that aims to support this adaptation. It is also important to remember that acceptance does not preclude painful emotional experience (Hayes et al., 1999). Rather, in this context, acceptance refers to an openness to the emotional experiences associated with the challenges of raising a child with ASD while acknowledging the joys that come with it. Acceptance, as it is understood here, refers to the parent’s journey of recognizing their child’s condition, the challenges associated with it as well as the joys, but also and above all, the recognition and acceptance of their own emotions in their complexities and diversities. Each difficulty experienced is then viewed as a learning opportunity rather than a hindrance to the developmental potential of the child and the potential of the parent in supporting their child’s development (Whittingham & Coyne, 2019). With this in mind, the focus of psychological support offered to parents should perhaps not be on diagnostic acceptance per se, but rather on the acceptance of varied and dense emotions experienced by parents: “shutting down, isolating yourself, is not good. Him now . . . me now, I accept him as he is. I don’t care.”
A study by Greeff and Nolting (2013) revealed that a positive attitude when facing new experiences and potential challenges is correlated with better family adjustment. These positive attitudes can be leveraged for the development of psychological coping strategies. In turn, parents can rely on these coping strategies when painful emotions are experienced and to help them accept the presence of these emotions. Positive attitudes, as conceived by Greeff and Nolting (2013), could be the basis for the development of problem-focused strategies. The use of problem-focused strategies by parents of children with ASD is associated with lower levels of distress whereas strategies focused on negative emotions (such as guilt, rumination, avoidance, etc.) are associated with greater levels of psychological distress (Cappe et al., 2011; Corman, 2009; Mazurek & Smith, 2013). These studies help to highlight the importance of developing parent support programs very early in the specialized service trajectory to avoid the development of engrained symptoms of depression and anxiety. Furthermore, as Stahmer and colleagues (2019) have pointed out, families should have access to support groups for parents with related experiences (e.g., immigration history, raising a child with ASD). This would afford parents the opportunity to share their experiences, reduce stigma, exchange information, and develop advocacy skills to assert their rights and those of their child.
As the challenging behavior associated with ASD was also a frequent context for dense emotional experiences, the data of this study suggest that the support at early stages of autism services trajectory should include coaching strategies for the management of challenging behaviors as well as specific psychological support for the parent’s well-being in context of challenging behaviors. Indeed, according to the study’s findings, parents’ psychological and physical health may be negatively affected by their children’s problematic behaviors. Recognizing that parental well-being can be adversely affected by challenging behaviors and that it can affect service-seeking and strategy application, it is important to equip parents with a range of tools to manage these challenges, including psychological adaptation strategies and effective strategies for managing their child’s behaviors. By providing parents with these resources, we can break free from the cycle of challenges and create a positive and supportive environment for all family members to thrive (Rivard et al., 2021b).
Several studies highlight the importance of accessing early intervention for young children, both for parental well-being and for a better prognosis for the child (Guralnick, 2005). In addition to this scientific literature, the present parents’ discourse demonstrates that their personal well-being is inextricably related to this accessibility. Therefore, when giving families access to targeted interventions for a child’s developmental needs and educating them of the potential impacts of those interventions on the child’s prognosis, we are also promoting parental psychological adjustment and well-being (Rivard et al., 2016). The present data then reinforce crucial importance of accessing these evidence-based early intervention services that are tailored to their requirements in accordance with the severity of their symptoms to facilitate parental adaptation (Klintwall et al., 2015; Mello et al., 2022).
Enhancing Parental Emotional Support Through Formal Services
The autism service trajectory in early childhood, while filled with obstacles, presents an opportunity for parents to develop their adaptability skills as they navigate the evaluation process, early intervention, and passage to school (Brewer, 2018). Although parents may experience intense emotions when faced with barriers in accessing services, such emotions reflect their strength and resilience in advocating for their children’s needs (Brewer, 2018; Ooi et al., 2016). These emotionally charged contexts are also opportunities for growth and development, as highlighted in a meta-analysis by Ooi and colleagues (2016). Despite the challenges surrounding assessment and diagnostic confirmation, as well as difficulties accessing formal and informal supports, parents can tap into their inner resources to navigate these experiences (Chatenoud et al., 2019; Magaña et al., 2017). Rapid access to specialized services can serve as a protective factor for parents’ psychological well-being, allowing them to better meet their children’s needs and advocate for their right to receive high-quality services (Chatenoud et al., 2019; Magaña et al., 2017).
The results of the current study show that the added challenges associated with the particularities of the immigration context can exacerbate emotional difficulties in the face of barriers to access to formal services. Sensitivity to the unique experiences of families with an immigrant background is necessary to enhance the specific support needed for the whole family to thrive. An empathetic, sensitive, and humble approach as well as a posture of openness and listening are all essential elements that must be adopted by health professionals working with families with an immigrant background who has a child with ASD (Rivard et al., 2021b). Research shows that families feel isolated by having a child with a developmental disability (Samsell et al., 2022), and the families in this study expressed that much of this isolation was related to leaving their loved ones behind, the lack of understanding of their child’s condition, and the feeling of judgment by family or health care professionals. Access to formal supports such as assessment services or early intervention centers can be much more difficult, due to a number of barriers such as unfamiliarity with the health care system, language barriers, or the invalidation experienced by some health care professionals (Mandell et al., 2020). The implementation of a conceptual intervention model targeting cultural humility is essential. Families with an immigrant background are already facing important adaptive issues. Indeed, depending on the reasons and the context of immigration, they may have experienced a variety of stressful situations (e.g., administrative procedures, assisting other family members with immigration, sometimes life-threatening situations). Those situations requiring an investment in terms of time, energy, financial resources, and adaptation capacities leave little room for the management of other situations. It is therefore important to be sensitive to immigration-specific challenges when accompanying parents of a child with ASD (Rivard et al., 2021b).
Supporting Families’ Overall Mental Health: It Can Be Hard and a Relief at the Same Time
Families can discover happiness, express gratitude for the unique experience of raising a child with ASD, and gain some insight into their own personal development as a result of that experience (Millau et al., 2019; Waizbard-Bartov et al., 2019). Even still, most parents find this life experience challenging, and as shown in the present study, some additionally have serious personal mental health concerns on top of their challenging adapting. Courcy and Des Rivières-Pigeons (2021) found that a depressive episode may slow down a parent’s search for services, which highlights the importance of offering support to parents. Studies also pinpoint the risk in some of developing symptoms of posttraumatic stress disorder when the child exhibits challenging behaviors common to ASD (Stewart et al., 2020). Beyond the specialized services for ASD offered to the family, it is essential to identify the parents requiring individual psychological interventions and to have the possibility of providing them such a resource when necessary to prevent mental health difficulties in parents (Fulton et al., 2019).
Recognizing and Supporting Emotional Complexity and Variability
The findings of this study emphasize the importance of considering that parents’ emotional experiences, even at the same point in their service trajectory or family life cycle, can be charged with multiple emotions at once and that challenging emotions can coexist with positive or appeasing emotions (Millau et al., 2019). The way a specific stage of the autism service trajectory (e.g., diagnostic disclosure or waiting periods) will be experienced cannot be reduced to a single emotion, so it is important to consider the emotional experience of each parent in all its complexity. Moreover, coexisiting emotions can generate feelings of ambivalence and complicate their understanding of this experience (“I went out and I felt like the world was ending. I was relieved, but it was like a confirmation”). Similarly, a parent who feels sad as a result of being isolated from their family abroad may also feel gratitude toward their community for supporting them at a distance. It might be helpful to consider the complexity of this subjective experience and the parent’s acceptance of the emotions that underlie it in supports for families. The goal of contextualizing the emotional experience is to better understand its function and better focus the necessary support. An approach such as Acceptance and Commitment Therapy (ACT), which is a model derived from functional contextualism (Hayes, 1993), has the potential to fulfill this goal. According to studies, a kind disposition and an acceptance of one’s feelings appear to be protective factors against depression symptoms and would lessen family distress (Jones et al., 2014; Kim et al. 2018). Such a strategy might show promise in assisting families’ psychological adjustments and assisting them in meeting this significant adaptation need of being parents (Whittingham & Coyne, 2019).
Limitations of the Current Study
The study’s results should be considered in light of its methodological limitations, including a small sample size, data collection in a specific region, and recruitment from a single clinic with access to specialized services. Findings may not generalize to all immigrant families in Quebec or other countries. Other factors not analyzed, such as reasons for immigration or the number of children in the family, may also affect the emotional experiences expressed.
Conclusion
The results of this qualitative study highlight key moments when parents seem to have a rich emotional experience and when support needs can be put forward. The families’ discourse also reflects the diversity and coexistence of complex emotions that can resurface throughout the different stages of their child’s service trajectory. Access to early specialized services for the child and also individual psychological support for parents should both be prioritized as soon as the families have begun the evaluation process for developmental delays for their child. Taking the time to listen and hear parents, to validate their emotions in all its complexity, and to relieve them of guilt are all skills that must be at the heart of support programs. Furthermore, presenting a benevolent curiosity about their culture, specific challenges, and immigration history is essential to create an egalitarian, humble, and harmonious relationship.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Institut universitaire en Déficience intellectuelle, the Consortium national de recherche sur l’intégration sociale, and the Fonds de recherche du Québec—Société et culture—Santé.