
Abstract
Several states have invested in 1915(c) Home and Community Based Service (HCBS) Medicaid policies to improve outcomes and reduce costs for children and youth with significant behavioral health needs, or Severe Emotional Disturbance (SED). However, little is known about these programs and the children they serve. Through a retrospective cross-sectional analysis, this study aimed to understand if the program was successfully reaching its target population: children and youth with the highest clinical need, at the greatest risk for out-of-home care, and who may not otherwise be eligible for Medicaid through other avenues. Results describe the demographic, clinical, and service use characteristics of children and youth enrolled in one SED Waiver program, comparing them with those of similar, non-waiver enrolled children with behavioral health needs. Findings report that the waiver program examined rarely served children and families not otherwise eligible for Medicaid, but that waiver-enrolled children and youth had substantially more severe clinical need, were at higher risk for out-of-home placement and incurred greater public expenditures for service use. Findings suggest the program studied is serving children with more significant psychiatric needs, as the program intends, but points to the need for further research to understand the impacts of such programs on system and clinical outcomes.
Keywords
Home and Community Based Services (HCBS) Medicaid waivers are public health policies aimed at enhancing access to home and community-based support services for individuals with significant disabilities or complex medical needs who might otherwise have need for institutional levels of care (Harrington et al., 2012). Medicaid HCBS policies aim to reduce use of institutional levels of care for individuals and youth with complex health care needs in order to reduce associated public costs, improve the quality of life for participants, and comply with federal mandates under the Americans with Disabilities Act to serve individuals with disabilities in the least restrictive setting possible (Harrington et al., 2012).
The most widely used HCBS policies are those authorized under the 1915(c) section of the Social Security Act, which allows states to waive standard Medicaid mandates for statewide coverage, comparability of services, and income and resource rules (Watts & Musumeci, 2018). Under this law, states expand or omit income eligibility requirements for the state Medicaid program to extend Medicaid coverage for long-term supports provided in the home and community that would normally be unaffordable and are not covered under Medicaid, Medicare, or private insurance. Eligibility customarily rests on individuals’ demonstration of need for residential levels of care (Musumeci et al., 2020). In these programs, participants have access to all health care services covered under the regular Medicaid program—as well as additional, state-crafted, tailor-made home, and community-based health care services, specific to the needs of each target population.
In 48 states, over 250 HCBS Medicaid waiver programs deliver care to over 1.5 million individuals (Watts & Musumeci, 2018), including children and adults with developmental or intellectual disabilities, medically fragile or physically disabled children and adults, individuals with brain injuries, older adults, individuals living with HIV/AIDs (Musumeci et al., 2020), and children and adults with complex mental health needs (Graaf & Snowden, 2017). Though nearly 50,000 children are served in these programs, the majority of participants are adults with intellectual disabilities, older adults, or adults with physical disabilities (Musumeci et al., 2020). As a result, the bulk of research about these policies has focused on their use for older adults or for those with intellectual or developmental disabilities (ID/DD) (LaClair et al., 2019; Muramatsu et al., 2007; Sands et al., 2012; Velott et al., 2016). For older adults, these programs have been found to increase health care costs while also improving quality of life for participants and their caregivers (Grabowski, 2006) and enrollment is associated with reductions in hospitalizations, emergency department visits, and nursing home placements (Muramatsu et al., 2007; Sands et al., 2012). For families of children with autism, 1915(c) HCBS waivers have also been demonstrated to reduce rates of unmet health care need (Leslie, Iskandarani, Dick, et al., 2017), associated racial and ethnic disparities (LaClair et al., 2019), and reduce emergency department visits (Liu et al., 2022) and employment impacts of caregiving (Leslie, Iskandarani, Velott, et al., 2017).
1915(c) HCBS Waivers for Children With Complex Behavioral Health Needs
In the last 15 years, federal and state policy makers have invested in leveraging 1915(c) HCBS Medicaid policies to improve outcomes and reduce costs for children and youth with significant behavioral health needs, or Severe Emotional Disturbance (SED) (Graaf & Snowden, 2020). These youth demonstrate significant disturbance in role functioning due to a psychiatric disorder (Narrow et al., 1998). Children and youth with more severe SED, representing approximately 5% to 6% of the child population, may experience significant impairment (Williams et al., 2018). These children and youth most commonly experience mood disorders, attention-deficit disorders, and anxiety problems, and often carry a diagnosis for more than one disorder (Peiper et al., 2015). Impairments may manifest in aggressive or destructive behavior, substance use, self-harming, or disordered thinking, putting youth with SED at much greater risk of being placed in a psychiatric residential treatment facility (Rose & Lanier, 2017; Theall et al., 2022). As a result, mental disorders continue to be the most costly health condition among children, with Medicaid carrying almost 50% of this burden (Soni, 2015). Though less than 4% of Medicaid-covered children use residential care, this service accounts for nearly 20% of Medicaid spending for children with mental health conditions (Pires et al., 2013).
To address growing public costs for out-of-home behavioral health care for children, several states have adopted 1915(c) waivers for children and youth with SED. The number of participants served with mental health needs is growing rapidly, jumping over 350% from 2013 to 2014 (Watts & Musumeci, 2018). While participation in 1915(c) waiver programs decreased for children overall by almost 30% in this time, HCBS 1915(c) spending for those with mental health needs increased over 700%. Though HCBS waiver programs for children with SED have been formally promoted by the federal government for almost 10 years (Mann & Hyde, 2013) and are growing rapidly (Watts & Musumeci, 2018), little is known about these programs or the children and families they serve.
The Current Study
Examinations of participants in 1915(c) waiver programs for children and youth with SED are few. The clinical and sociodemographic characteristics and service use patterns of children served in these programs has been reported rarely. Furthermore, it is unknown how these characteristics compare to non-waiver enrolled children with SED or children with SED in non-waiver states. One previous study reported demographic and clinical characteristics of waiver-enrolled children with SED (Frimpong et al., 2018) and another provided minimal clinical or demographic descriptions of participants (Solhkhah et al., 2007). Neither study provided insight into waiver enrollment, Medicaid eligibility patterns, or clarified how waiver participants differ from other children and youth served in public mental health systems. Understanding the unique characteristics of populations served in SED waiver programs is a critical first step in designing research that can adequately evaluate these programs. Generating this knowledge can also provide insight for policy makers considering adoption of these policies—to help them understand the population that might targeted by waivers. Using a retrospective cross-sectional analytic design, this study aimed to describe the demographic, clinical, and service use characteristics of children and youth enrolled in one SED Waiver program. It compared these characteristics to those of diagnostically similar non-waiver enrolled children in the same public mental health system. Its primary objective was to understand how the program was utilized by families and if the program was successfully reaching its target population: children and youth with the highest clinical need, at the greatest risk for out-of-home care, and those who may not otherwise access Medicaid through other eligibility paths.
Methods
This study used a retrospective cross-sectional design, drawing on the Medicaid Analytic eXtract (MAX) data for one state. The state selected for this pilot adopted a 1915(c) waiver in 2009, and this study draws upon statewide MAX data from 2012. The state examined used the following criteria for program eligibility: the child must be (a) 3 to 18 years old; (b) have serious mental, emotional, and behavioral difficulties; (c) have a qualifying mental health diagnosis; (d) be at risk of being placed outside of their home due to their mental health needs; (e) meet the criteria to be in a psychiatric hospital; (f) be financially eligible for Medicaid based on the child’s income alone; and (g) currently live in a home setting with a legal guardian or on their own if they are legally emancipated. For eligible children, the program provides a wraparound case planning and care coordination approach and provides coverage for a wide range of highly specialized therapies and support services. Examples of specialized services include animal-assisted therapies, art therapies, parent and youth peer support services, and respite care.
Data Source
The MAX is the only national, person-level data source containing Medicaid enrollment and Medicaid-covered health care claims for all Medicaid beneficiaries each year. The files are prepared for research by the Centers for Medicare and Medicaid Services (CMS), derived from data submitted by all 50 states through the Medicaid Statistical Information System (MSIS), for the purpose of examining annual Medicaid enrollment, services, and expenditures. MAX transforms MSIS data into user-friendly calendar-year formats, based on date of service, and combines initial claims, voided claims, and claim adjustments into single final action claims. CMS’s transformation of MSIS data into the MAX data links eligibility and demographic information for each beneficiary to each claim and to a summary of utilization and expenditures for each beneficiary. It corrects coding inconsistencies in MSIS enrollment data, where possible, and identifies Section 1915(c) waiver participants by waiver target population.
Final MAX data sets include a person summary (PS) file and four claim files—inpatient (IP), institutional long-term care (LTC), prescription drug (RX), and other services (OT). The RX file was not used in this study. In the PS file, each beneficiary represents one observation, with demographic, expenditure, and utilization characteristics and summaries provided for each observation. In the four claims files, observations are both fee-for-service (FFS) and managed care (encounter) claims that include details regarding date of service, expenditures for services provided, diagnostic information (including principal diagnosis and 2nd through 9th diagnoses), and provider and procedure type. MAX-specific identification numbers for each beneficiary allow individuals to be examined across MAX files.
Variables
Individual beneficiaries were the unit of analysis for this study. A predictor variable, outcome variables, and all covariates were constructed from the PS file or from across multiple claims within the LTC, IP, and OT files for each beneficiary.
Predictor Variable
The predictor variable for this study was SED waiver enrollment, signified by an indicator variable (Waiver Type) within the PS MAX dataset. From this variable, a binary indicator of monthly SED waiver enrollment was created to identify beneficiaries enrolled in an HCBS 1915(c) waiver program targeting individuals with SED or Mental Illness.
Outcome Variables
Outcome variables for descriptive and multivariate analysis included annual inpatient and long-term care utilization. Binary variables indicated any annual use of inpatient or long-term care, total annual expenditures for inpatient or long-term care utilization, and total annual number of inpatient or long-term care stays. Total days of inpatient or long-term care stays was also described and compared across populations, using admission and discharge dates.
Inpatient Care
Inpatient variables were drawn from the IP MAX files in which each observation in the file represents an inpatient stay and includes an admission and discharge date. Using only inpatient stay observations with a principal behavioral health diagnosis (see Appendix A), a binary variable was created to indicate a beneficiary’s (a) use of any inpatient service use in the observation year, (b) total number of separate inpatient stays in the observation year, and (c) the total number of days of inpatient care received in the observation year. The total annual Medicaid-reimbursed expenditures for inpatient care represented the sum of expenditures for all inpatient claims with a principal behavioral health diagnosis in 2012 for each beneficiary. One of each outcome variable was created for each beneficiary.
Long-Term Care
Long-term care stays were drawn from the LTC file and included any long-term care claim for an inpatient psychiatric facility for individuals under the age of 21. As with the IP File, each observation in the LTC file represents a long-term care stay with a corresponding admission and discharge date. From these data, a binary variable was created to indicate a beneficiary’s (a) use of any long-term care service use in the observation year, (b) total number of separate long-term care stays in the observation year, and (c) and the total number of days of long-term care received in the observation year. The total annual Medicaid-reimbursed expenditures for long-term care represented the sum of long-term care expenditures provided in an inpatient psychiatric facility for individuals under the age of 21 in 2012 for each beneficiary.
Covariates
Covariates included both child-level and county-level characteristics. The PS files include the sex (male or female) and self-reported race/ethnicity (white, Black, Hispanic, Asian, American Indian/Alaska Native, Other, or Unknown) of beneficiaries. Ages were calculated on January 1, 2012, from beneficiaries’ dates of birth.
Medicaid Enrollment
Analysis both examined the patterns of non-waiver enrollment in Medicaid and controlled for non-waiver Medicaid enrollment in multivariable regression models. This variable was constructed from the Medicaid Eligibility variable in the PS file, which indicates the category under which the beneficiary is eligible for Medicaid. A binary variable indicating monthly Medicaid eligibility and a continuous variable representing the total months of Medicaid enrollment were constructed from this variable for each beneficiary.
Diagnostic Category
Each claim in the OT, IP, and LTC files includes up to 10 diagnoses associated with the service provided in the claim. Using the Agency for Health Care Research and Quality’s (AHRQ) Clinical Classification Software (CSS) based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), health care claim diagnostic and procedure codes were collapsed into a smaller number of clinically meaningful categories. Binary variables were created for each beneficiary for the most prevalent diagnostic categories: (a) anxiety disorders; (b) attention deficit, conduct, and disruptive behavior disorders; (c) developmental disorders; (d) mood disorders; and (e) schizophrenia and other psychotic disorders. A beneficiary was coded as having a disorder if it was included as a principal diagnosis on any health care claim in the IP or OT files.
Psychiatric Features
Analysis controlled for a set of psychiatric features that research has established to be associated with out-of-home behavioral health utilization: presence of psychosis, presence of suicidal or homicidal thoughts or behavior, developmental comorbidities, and psychiatric comorbidities (January et al., 2018; Lanier & Rose, 2017; Park et al., 2009; Rose & Lanier, 2017; Yampolskaya et al., 2014). These variables were derived from diagnostic codes associated with claims in the OT and IP files. The presence of psychosis was assessed through a binary variable created from diagnoses variables; if a beneficiary had a claim with an ICD-9 diagnostic code representing psychotic features as the primary diagnosis (see Appendix A), for any claim in 2012, they were coded as having the presence of psychotic features. The presence of suicidal or homicidal thought or behavior is indicated by a binary variable constructed to represent if the beneficiary had an ICD-9 V code for suicidal (V62.84) or homicidal ideation (V62.85) in any position in their diagnoses list for any claim in 2012. A child’s developmental comorbidity is indicated by a binary variable constructed from diagnoses across all claims for a beneficiary in 2012. If the child had both a developmental disorder as a principal diagnosis for any claim and a psychiatric disorder as a principal diagnosis for any other claim, they were coded as having developmental comorbidities. Psychiatric comorbidities are indicated by a binary variable that indicates two different psychiatric diagnostic categories associated with one beneficiary—either on the same claim or as the primary diagnosis across different claims in any of the files in 2012.
County Covariates
County-level covariates are drawn from the U.S. Census and Policy Map, including estimates of 2012 county median income levels and total mental health treatment facilities. Policy Map cites its data regarding total number of mental health facilities as drawn from the Substance Abuse and Mental Health Services Administration (SAMHSA).
Analytic Sample
This descriptive study drew on a randomly generated subsample of the 2012 MAX files for one state, combining the PS file, the OT file, the IP file, and the LT file. The subsample was randomly selected based on the following criteria: individuals under 21 years of age with a behavioral health diagnosis in any position on any claim in the 2012 MAX files. The study sample was constructed from this subsample. To allow for understanding of how waiver-enrolled children compared clinically and demographically with other children and youth served in the public mental health system, the study sample included all children enrolled in the SED waiver program as well as other “diagnostically similar” children in the state not enrolled in the waiver program. The comparison of these two groups of children assessed if the state’s waiver program was indeed serving children with more significant or complex mental health needs—as the program intends.
The state’s clinical criteria for waiver participation (described above) relies primarily on clinical features such as “serious mental, emotional, and behavioral difficulties,” meeting the criteria “to be in a psychiatric hospital,” and a “qualifying mental health diagnosis.” Because healthcare claims data provide little qualitative data to describe the clinical features of child’s mental health condition that might indicate “serious” difficulties or whether they meet criteria for psychiatric hospitals (which can vary depending on the hospital and the child’s insurance plan) (Funkenstein et al., 2016; Musumeci et al., 2019), we relied primarily on diagnosis to generate a subsample of “diagnostically similar” children for comparison with children enrolled in the SED waiver program. We limited this comparison sample to include only children with diagnoses observed in the waiver group of children: anxiety disorders, developmental disorders, mood disorders, and psychotic disorders. Thus, the comparison group carries similar diagnoses as the waiver-enrolled children—but they may vary from waiver-enrolled children in rates of comorbidities and other psychiatric features such as psychosis or suicidal ideation. It was hypothesized that such characteristics may be more prevalent among children who have “serious” difficulties or meet the criteria for psychiatric hospitalization, and therefore be more prevalent among waiver-enrolled children.
The comparison sample for this study included any Medicaid-enrolled child in the state in 2012, ages 4 to 18, who had at least one inpatient stay with a psychiatric diagnosis or two outpatient behavioral health services with anxiety disorders, developmental disorders, mood disorders, and psychotic disorders (N = 226,207). The diagnostic restrictions for this group are based on the most commonly observed diagnoses in the waiver-enrolled group, but these diagnoses have also been identified as predicting higher utilization and expenditures (Doupnik et al., 2020). Restricting inclusion to a subset of diagnoses also allowed regression models to omit diagnostic covariates, increasing the power of the models. This is particularly important given the small size of the waiver-enrolled sample: 81 children were enrolled in the SED waiver at some point in 2012. The state examined in this study adopted the waiver program in 2009 and piloted it in two counties initially. It was not expanded statewide until 2014. Thus, the small sample size reflects a waiver program in relatively early stages of program adoption.
Analysis
To understand patterns of enrollment in the waiver program over the course of the observation year, the SED Waiver-Enrolled subgroup was first examined alone, and five enrollment groups were identified and summarized: children and youth with full year enrollment, early year enrollment, midyear enrollment, late year enrollment, and intermittent enrollment. To report the total number of children and youth with Medicaid enrollment and eligibility outside of waiver enrollment, the Medicaid eligibility category most frequently reported for each child’s Medicaid coverage was summarized. Descriptive analyses were conducted to compare the demographic, clinical, and out-of-home behavioral health service utilization of the SED Waiver-Enrolled subgroup with other diagnostically similar children in the state’s public behavioral health system. Chi-square tests and t-tests were used to assess significance of differences in characteristics and utilization between the SED Waiver-Enrolled subgroup and other children in the state’s public mental health system.
To assess the association of waiver-enrollment with out-of-home behavioral health service use, multivariable regression models were constructed, comparing SED Waiver-Enrolled children with other children with similar diagnoses. Four separate Poisson models regressed waiver enrollment on any use of psychiatric inpatient care, total number of psychiatric inpatient stays, any use of psychiatric long-term care, and number of psychiatric long-term care stays. Two linear regression models assessed the association of waiver enrollment with total annual psychiatric inpatient expenditures and total annual long-term care psychiatric expenditures. Total expenditures were log-transformed to manage heteroskedasticity of the variables. Total sample size for regression analysis was 226,126.
To understand the pattern of out-of-home behavioral health care utilization in relation to waiver enrollment for waiver participants, new binary variables were created for descriptive analysis. Inpatient stays “Prior to Waiver Enrollment” represent the initiation of an inpatient stay in a month prior to when the beneficiary became enrolled in the waiver. Inpatient stays during waiver enrollment represent the initiation of an inpatient stay in a month when the beneficiary was enrolled in the waiver. If an inpatient claim stay ended in a month in which the beneficiary was not enrolled in the waiver, the stay was still considered “During Waiver Enrollment.” Inpatient stays “After Waiver Enrollment” represent the initiation of an inpatient stay in a month when the beneficiary was not enrolled in the waiver but had previously been enrolled in it. If an inpatient claim began after the beneficiary was enrolled in the waiver but occurred during a month in which they were not enrolled in the waiver, it was considered “After Waiver Enrollment” even if they subsequently re-enrolled in the waiver. An identical set of binary variables, using the same classification process, was created to represent long-term care use “Prior to,” “During,” or “After” waiver enrollment. These binary variables were analyzed descriptively to understand the number of inpatient and long-term care stays and mean number of inpatient and long-term care days of treatment prior to, during, or after waiver enrollment.
Results
Eighty-one children were enrolled in the SED waiver program in 2012. Table 1 reports waiver enrollment patterns and eligibility for Medicaid outside of waiver enrollment for waiver participants. Only three (3.7%) of these children were enrolled for the full year. Approximately 60% of this group were enrolled at the start of 2012 but exited the waiver program before the end of 2012; 5 participants were enrolled in the program mid-year, and 28% of participants enrolled in the program after January 1 and continued to be enrolled on December 31 of 2012. Only one participant enrolled in the waiver more than once in 2012. Among waiver participants not enrolled for the full year, over 90% had Medicaid coverage outside of waiver enrollment. Most of the youth covered under Medicaid outside of their waiver enrollment were eligible most frequently through disability status (71.2%), 11% were eligible through foster care involvement, and 11% were eligible through meeting poverty income standards. A small number of children or youth were eligible for their Medicaid coverage outside of waiver enrollment through other means, including through TANF or Transitional Medicaid Assistance, meeting adult poverty levels, or through the state’s Section 1115 waiver.
Most Frequent Non-Waiver Medicaid Eligibility Among Children Enrolled in the SED Waiver in 2012 (N = 81).
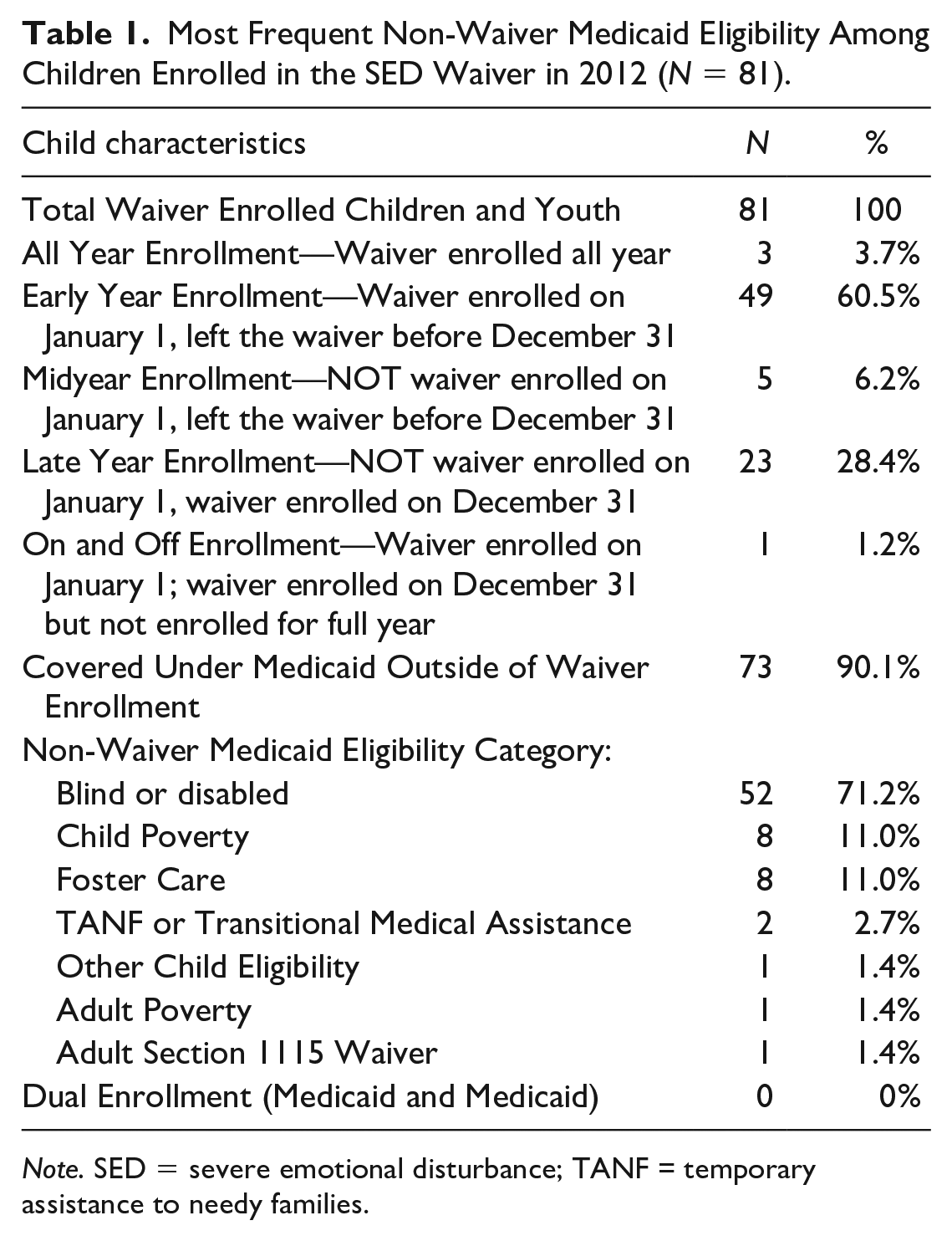
Note. SED = severe emotional disturbance; TANF = Temporary Assistance to Needy Families.
Table 2 provides a comparison of waiver participants with other children and youth with similar diagnoses served in the public behavioral health system in the state in 2012. It reports proportions and sample sizes for categorical variables and means and standard deviations for continuous variables. Females had higher representation (43.2% vs. 36%) and Hispanic children and youth had lower representation in the waiver group than among non-waiver enrolled children (25.9% vs. 46%). A significantly (p < .0001) larger proportion of the waiver group’s racial identity was “unknown” too (46.9% vs. 21%). The average age of waiver participants (12.4 years, standard deviation [SD] = 3.1) was significantly (p < .0001) higher than the other children and youth (9.750 SD = 3.96). The average months of Medicaid enrollment was similar across both groups, with waiver participants having an average of 5.3 months (SD = 2.80) of waiver participation.
Characteristics of Children With Significant Behavioral Health Needs in the Study State in 2012.
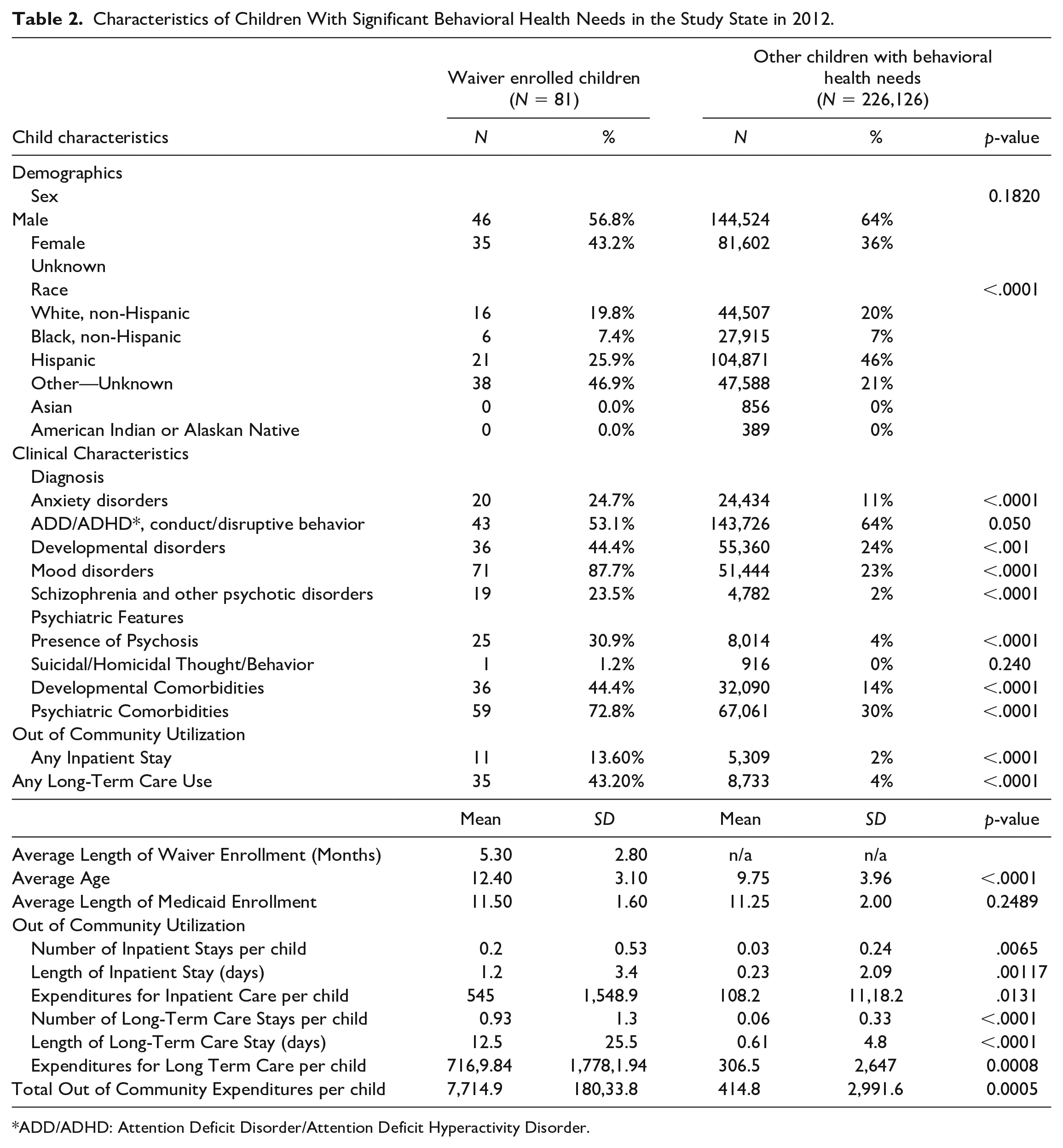
*ADD/ADHD: Attention Deficit Disorder/Attention Deficit Hyperactivity Disorder.
Significant (p < .0001) differences in clinical characteristics between groups included significantly higher rates of anxiety disorders (24.7% vs. 11%), developmental disorders (44.4% vs. 24%), mood disorders (87.7% vs. 23%), and schizophrenia or other psychotic disorders (23.5% vs. 2%) in the waiver group. Waiver enrollees had significantly (p < .0001) higher rates of psychosis (30.9% vs. 4%), developmental comorbidities (44.4% vs. 14%), and psychiatric comorbidities (72.8% vs. 30%).
Regarding use of out-of-home care, the waiver group had significantly (p < .0001) higher rates of having at least one inpatient stay (13.6% vs. 2%) and any long-term-care stay (43.2% vs. 4%). The average annual total of inpatient stays per child were significantly (p < .0001) higher for the waiver group (0.20 [0.53] vs. 0.03 [0.24]). Significant (p < .0001) differences also existed between the average length of the inpatient stays (1.2 days [0.53]) and Medicaid-reimbursed expenditures for inpatient care per child ($545 [$1,548.90]) for waiver youth compared with other diagnostically similar children (0.23 [2.09]; $108.20 [$1,118.20]).
The mean total annual number of long-term care stays per child were significantly (p < .0001) higher for the waiver group (0.93 [0.1.30] vs. 0.06 [0.33]). Significant (p < .0001) differences also existed between the average length of long-term care stays (12.5 days [25.50]) and Medicaid-reimbursed expenditures for long-term care per child ($7,169.84 [$17,781.94]) for waiver youth compared with other children in the sample (0.61 [4.80]; $306.50 [$2,647.00]). Total annual Medicaid reimbursed expenditures for out-of-home care of any type was also significantly (p < .0001) higher for the waiver-enrolled youth ($7,714.90 [$18,033.80] vs. $414.80 [2,991.60]).
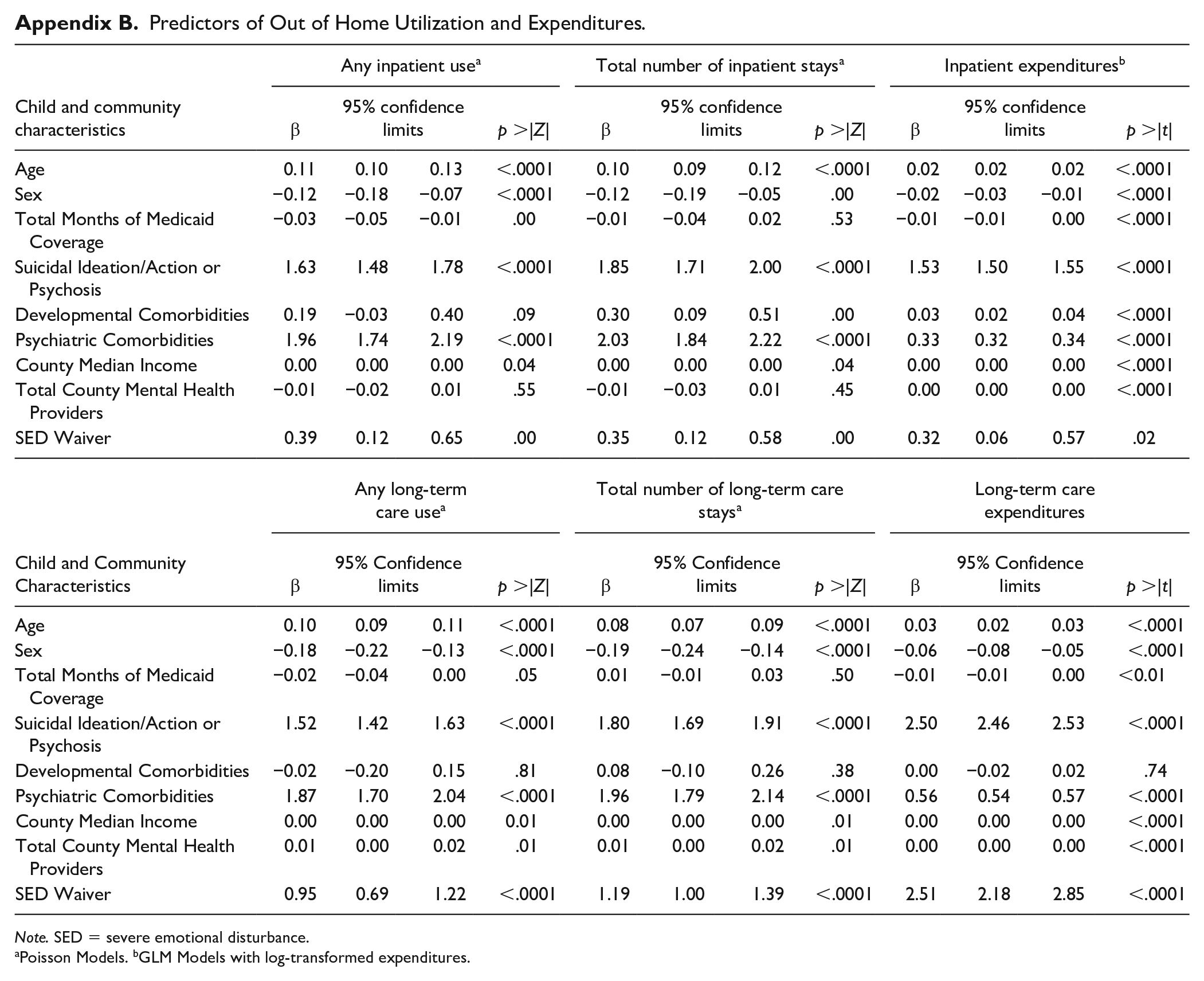
Table 3 reports the association of annual SED waiver enrollment with any use of inpatient or long-term care, the total number of inpatient and long-term care stays, and total annual Medicaid-reimbursed expenditures for inpatient or long-term care stays. Estimates adjust for the demographic and clinical characteristics of children and youth in the sample and differences in behavioral health system characteristics across counties, comparing waiver-enrolled youth with other children in the sample. (Full model outcomes are presented in Appendix B.) Annual enrollment in the SED waiver was significantly (p < .0001) and positively associated with any annual inpatient care use (b = 0.39, SE = 0.12), the total annual number of inpatient care stays (b = 0.35), and total inpatient care Medicaid-reimbursed expenditures (b = 0.32). SED waiver enrollment also significantly (p < .0001) predicted any use of long-term care stays in 2012 (b = 0.95), a greater number of long-term care stays in 1 year (b = 1.19), and higher total Medicaid reimbursed long-term care annual expenditures (b = 2.51).
SED Waiver Enrollment’s Association With Out of Home Psychiatric Service Utilization and Expenditures a .
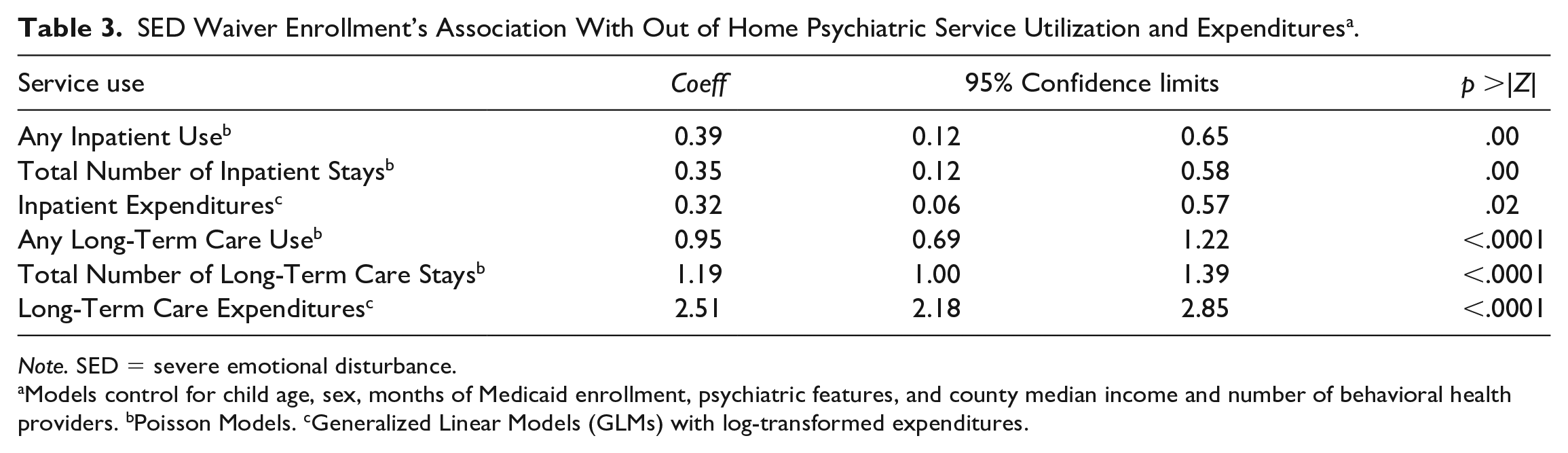
Note. SED = severe emotional disturbance.
Models control for child age, sex, months of Medicaid enrollment, psychiatric features, and county median income and number of behavioral health providers. bPoisson Models. cGeneralized Linear Models (GLMs) with log-transformed expenditures.
Table 4 provides some insight into patterns of inpatient and long-term care utilization in relation to waiver enrollment. In all, 13.6% of all waiver-enrolled youth experienced a psychiatric inpatient stay in 2012, with the group experiencing a total of 16 stays collectively, averaging 6.1 days each (SD = 1.5). In all, 31.25% of inpatient stays were prior to waiver enrollment, with an average length of stay of 6 days (SD = 1.2). A total of 37.5% of these stays were during participation in the waiver program, with an average length of stay of 5.8 days (SD = 1.3). A total of 33.3% of inpatient stays were after disenrollment from the waiver (mean length of stay = 6.6, SD = 2.0). In all, 43.2% of waiver participants experienced a psychiatric long-term care stay in 2012, with a total of 75 stays for the whole group collectively. A total of 32% of these stays were prior to waiver enrollment, with average length of stay of 15.1 days (SD = 26.3), and a median stay length of 6.5 days. Approximately 30.7% of these stays were during waiver enrollment, with an average length of stay of 12.6 days (SD = 21.0) and a median stay length of 6 days. Almost 40% of the LTC stays in this group were for waiver participants after ending waiver enrollment, with an average length of stay of 12.9 days (SD = 12.3) and a median length of stay of 7 days.
Out of Home Care Before, During, and After Waiver Enrollment.
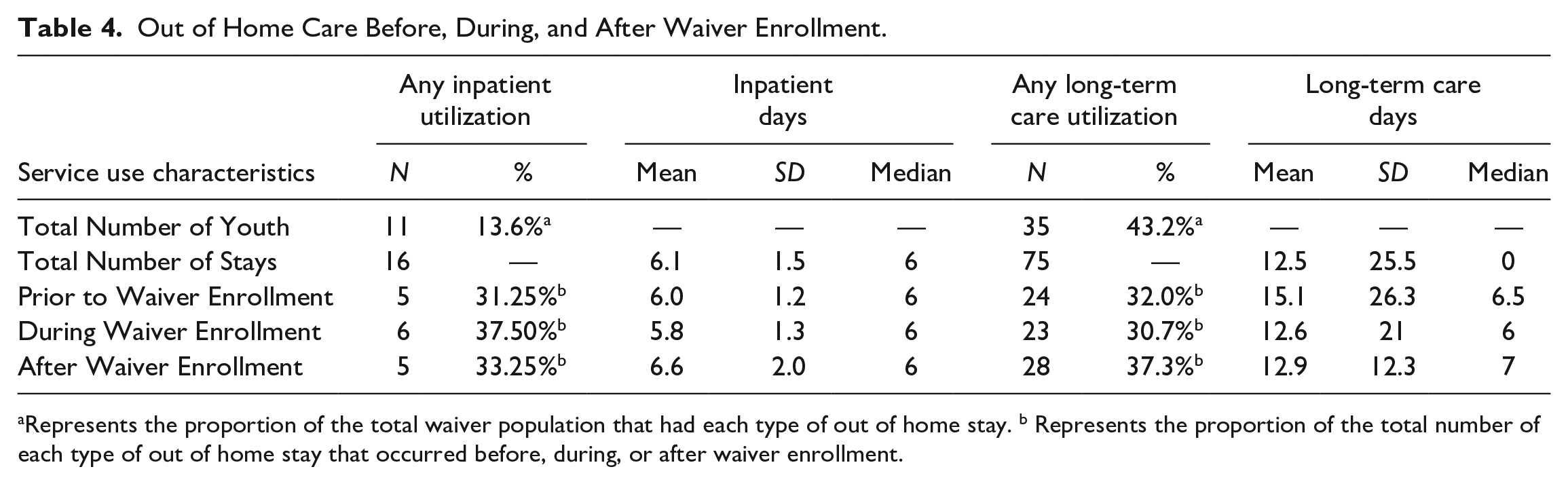
Represents the proportion of the total waiver population that had each type of out of home stay. b Represents the proportion of the total number of each type of out of home stay that occurred before, during, or after waiver enrollment.
Discussion
This is the first study of 1915(c) waiver participants that uses MAX data to examine and report SED waiver participants’ clinical and demographic characteristics and patterns of program and out-of-home service use. Its primary objective was to understand how the program was utilized by families and if the program was successfully reaching its target population: children and youth with the highest clinical need, at the greatest risk for out-of-home care, and those who may not otherwise be eligible for Medicaid through other avenues. Results indicate that the waiver program examined here rarely served children and families not otherwise eligible for Medicaid. However, waiver enrolled children and youth had substantially more severe clinical need, were at higher risk for out-of-home placement, and they incurred greater public expenditures for service use. These findings suggest that the program studied is successfully serving its target population. Additionally, comparisons of waiver-enrolled youth with non-waiver youth suggest several implications for policy and future directions for further investigations of SED Waiver programs. Results indicate that future research is needed to understand how SED Waivers compare and interact with Medicaid and other 1915(c) HCBS waiver programs for children in each state, and to understand their role in preventing or facilitating out-of-home service use.
Waiver Enrollment and Medicaid Eligibility
Among a total of 81 SED Waiver participants in one state, observed in the early stages of the states’ waiver program implementation, only three participants were enrolled in the program for the full year. This suggests relatively high churn rates for this program. This may be one reason why waitlists are shorter for SED waivers than for other types of waiver programs. Of the over 600,000 individuals or children on wait lists for waiver programs in 2016, older adults or those with intellectual disabilities/developmental disabilities (ID/DD) account for over 92% of this group. Those with mental health needs account for less than 1% (Musumeci et al., 2019). Furthermore, average wait times for waiver enrollment for are significantly less for mental health waivers—66 months for ID/DD waivers compared to 11 months for mental health waivers (Musumeci et al., 2019).
The high churn rate in this program also points to key question for future inquiry. Very little is known about the implementation of waiver programs for any population, and these processes may have a significant impact on the enrollment and service use patterns, engagement experiences, and outcomes of waiver participants. Implementation shapes who accesses the waiver, how long they are served in the program, and what services are provided to them while enrolled (Hupe & Hill, 2016). Qualitative and mixed methods studies are needed to unpack the complexities of how waiver policies are implemented, how implementation varies across and within states, and how these variations impact waiver target populations. Key questions might include understanding the specific assessments used to determine eligibility, the outreach and engagement processes used to educate families about the availability of the program, and how the intake, treatment planning, and discharge processes unfold for waiver participants.
This study also found that most waiver participants were eligible for Medicaid regardless of Waiver eligibility, most commonly through categorical eligibility for disability. This may be significant for two reasons. First, because 90% of waiver participants were insured by Medicaid outside of their waiver enrollment, their significant health services expenditures were born by the state’s public health and behavioral health system whether they were enrolled in the waiver or not. Thus, if waiver enrollment does indeed reduce overall costs for care for these children and youth—as 1915(c) waiver policies aim to do—targeting this population for waiver participation may be particularly economically efficient for a state. Second, because the waiver program disregards family income for Medicaid eligibility and provides coverage for a wider array of home and community-based behavioral health care, waiver participation may be critical for families whose children have significant behavioral health needs and who are not traditionally eligible for Medicaid. Opportunities to reach this vulnerable population through SED waiver enrollment were not being realized in the year this state’s waiver program was observed.
Developmental and Psychiatric Comorbidities
In the state examined, the SED Waiver program appears to have served children and youth with more complex behavioral health needs—as the program intends. Waiver recipients were, as expected, more distressed. Compared to other Medicaid-covered, diagnostically similar children who utilized behavioral health services in 2012 in the state, children and youth enrolled in the waiver program were significantly older, had substantially higher rates of anxiety, mood, and psychotic disorders, and higher rates of psychotic features and documented suicidal or homicidal thoughts or behavior. This group also had significantly higher rates of developmental disorders, psychiatric comorbidities, and developmental disorders co-occurring with psychiatric disorders.
Almost half of SED waiver participants carried a developmental disability diagnosis in addition to a psychiatric diagnosis. In addition to demonstrating the overlap between developmental disabilities and children with mental health conditions, consistent with much other research (Graaf & Gigli, 2021; Levy et al., 2010; Soke et al., 2018), this finding underscores that this type of comorbidity is observed in children who also have higher rates of out-of-home service use—and is common in children enrolled in SED waiver programs. While national estimates suggest that 10% of children with a developmental disability also have psychiatric diagnoses (Levy et al., 2010) and that 12% of children with complex health care needs carry both developmental and psychiatric diagnoses (Graaf & Gigli, 2021), over 40% of waiver participants carried diagnoses for both developmental and psychiatric conditions.
The high proportion of SED waiver participants with co-occurring developmental disabilities raises future research questions about how or why children or youth with developmental disabilities were referred to the SED waiver program rather than the state’s 1915(c) waiver programs for children with developmental disabilities. Over 40% of all 1915(c) waiver enrollees in the United States are youth and adults with ID or DD (Watts & Musumeci, 2018), and over 50 former or current waiver programs across 29 states explicitly target children or youth with autism spectrum disorder (ASD; Velott et al., 2016). However, these widely available waiver programs for those with ID or DD also have long waiting lists.
Currently, there are no studies—to these authors’ knowledge—that examine the implementation of waivers for children with either developmental disabilities or complex mental health needs that can provide additional insight into the eligibility paths used by children who may qualify for both programs. Future waiver implementation research should address such questions: Are children and youth accessing additional services through SED eligibility when they are unable to access supports through ID, DD, or ASD eligibility? How do states determine which eligibility door a child with developmental and psychiatric comorbidities can go through? How do waiver enrollment patterns for SED waivers differ from enrollment patterns for participants in 1915(c) HCBS programs targeting other populations? Is there greater capacity in SED waiver programs because of lower demand or greater churn in waiver enrollment?
Waiver Enrollment’s Association With Out-of-Home Care
As befits their greater clinical vulnerability, SED Waiver-enrolled youth had higher rates and more days of inpatient and long-term care utilization than other diagnostically similar children in the public mental health system in the state. Furthermore, annual waiver participation was associated with greater Medicaid-reimbursed expenditures for out-of-home care in 2012. This is consistent with recent research findings that demonstrate that expenditures are higher for waiver-enrolled children when compared to similar children receiving public community-based mental health care (Frimpong et al., 2018). However, this research establishes that costs decline more rapidly for waiver-enrolled children after discharge from the waiver than for other, clinically similar children.
The higher rates of psychiatric comorbidities, psychotic features, and documented suicidal or homicidal thoughts or behavior found among waiver-enrolled children in this study is consistent with their higher rates of out-of-home care—as these are often criteria used for establishing medical necessity for psychiatric hospitalization (Rabinowitz et al., 1995; Ziegenbein et al., 2006). It is also within expectations, given the state’s waiver program eligibility criteria that requires children have “serious” problems and meet criteria for psychiatric hospitalization. Understanding the clinical screening tools used in the eligibility determination process may provide additional information about how these children are identified and why they may systematically vary from the general population of child mental health users.
While these findings confirm that waivers are serving high cost and high need children and youth, they provide no clarity around the impact of SED waiver enrollment on out-of-home utilization and expenditures for waiver participants. To rigorously assess the impact of SED waiver enrollment on child and youth out-of-home service utilization and Medicaid-reimbursed expenditures, multiple years of Medicaid claims data from all 50 states must be used. A national and longitudinal analysis will allow for comparison of SED Waiver programs with other state approaches for funding HCBS for children with SED (Graaf & Snowden, 2019) and allow for comparison of outcomes in states before and after waiver adoption. Additionally—for children enrolled in Medicaid outside of waiver enrollment—longitudinal data will provide a clear understanding of service use prior to waiver enrollment and the impact waiver enrollment has on concurrent and subsequent behavioral health service use and service use trajectories (Frimpong et al., 2018; Liu et al., 2022). Future studies should examine patterns in both community-based and out-of-home care for waiver participants—as waivers theoretically divert participants from out-of-home care through increased provision of HCBS (Mandell et al., 2012; Sands et al., 2012).
Limitations
This study had several key limitations. The cross-sectional study design precludes any causal inferences regarding the impact of waiver enrollment on out-of-home service or expenditures. Furthermore, the small sample of waiver-enrolled children and youth, studied for a limited time and at an early phase of policy implementation, limits the generalizability of these findings to other state SED waiver programs. The waiver group’s small sample size, as noted above, also limited the number of potentially critical differences in clinical need that should be controlled for within multivariable regressions. Furthermore, at the time of the study, the waiver program was only operating in two counties; much variation can exist across county mental health systems, especially in states in which counties or local behavioral health boards play a key role in deciding and implementing mental health policy and programs (Graaf & Snowden, 2019). While the inclusion of only two counties in the state limits the generalizability of these findings to some degree, the state examined in this study—as is often the case in states that adopt waiver programs (Graaf & Snowden, 2020)—is one in which state mental health policy and programming decisions are primarily driven by state administrators and monitored through state oversight. Finally, though the waiver sample was small, the total sample in regression models was very large. This large total sample size contributes to adequate statistical power for generating estimates but increase the likelihood of revealing statistically significant results that are not very clinically significant. As such, caution is important in interpreting analytic results.
Conclusion
Despite these limitations, the study reported here provides preliminary descriptions of demographic and clinical characteristics of children served by an SED Waiver program, as well as their out of home service utilization patterns and how they relate to waiver enrollment. This research demonstrates that the program studied is successfully enrolling children that are targeted by the program, but that it may be underserving families who would not be eligible for Medicaid outside of waiver eligibility. Findings provide clear descriptions of the children being served in this program, laying the groundwork for additional research to understand the impact of these policies on children and their families, how these programs are implemented, how they interact with other waiver programs within the same state, and how implementation and policy interactions impact the experiences and outcomes of children and their families that are eligible for SED waiver programs.
Given the current policy environment, in which CMS promotes the use of HCBS policies and the Affordable Care Act (ACA) offers additional opportunities for states to expand HCBS for high needs populations (Harrington et al., 2012), understanding the impacts of such policies and their implementation on care utilization and associated public costs is urgent. Future research must identify policy mechanisms associated with more effective and efficient behavioral health services—and how their implementation impacts desired outcomes—to provide critical insights to national and state policy makers in organizing and funding behavioral health care for children with the most complex mental health needs.
Footnotes
Appendix
Predictors of Out of Home Utilization and Expenditures.
| Any inpatient use a | Total number of inpatient stays a | Inpatient expendituresb | ||||||||||
| Child and community characteristics | β | 95% confidence limits | p >|Z| | β | 95% confidence limits | p >|Z| | β | 95% confidence limits | p >|t| | |||
| Age | 0.11 | 0.10 | 0.13 | <.0001 | 0.10 | 0.09 | 0.12 | <.0001 | 0.02 | 0.02 | 0.02 | <.0001 |
| Sex | −0.12 | −0.18 | −0.07 | <.0001 | −0.12 | −0.19 | −0.05 | .00 | −0.02 | −0.03 | −0.01 | <.0001 |
| Total Months of Medicaid Coverage | −0.03 | −0.05 | −0.01 | .00 | −0.01 | −0.04 | 0.02 | .53 | −0.01 | −0.01 | 0.00 | <.0001 |
| Suicidal Ideation/Action or Psychosis | 1.63 | 1.48 | 1.78 | <.0001 | 1.85 | 1.71 | 2.00 | <.0001 | 1.53 | 1.50 | 1.55 | <.0001 |
| Developmental Comorbidities | 0.19 | −0.03 | 0.40 | .09 | 0.30 | 0.09 | 0.51 | .00 | 0.03 | 0.02 | 0.04 | <.0001 |
| Psychiatric Comorbidities | 1.96 | 1.74 | 2.19 | <.0001 | 2.03 | 1.84 | 2.22 | <.0001 | 0.33 | 0.32 | 0.34 | <.0001 |
| County Median Income | 0.00 | 0.00 | 0.00 | 0.04 | 0.00 | 0.00 | 0.00 | .04 | 0.00 | 0.00 | 0.00 | <.0001 |
| Total County Mental Health Providers | −0.01 | −0.02 | 0.01 | .55 | −0.01 | −0.03 | 0.01 | .45 | 0.00 | 0.00 | 0.00 | <.0001 |
| SED Waiver | 0.39 | 0.12 | 0.65 | .00 | 0.35 | 0.12 | 0.58 | .00 | 0.32 | 0.06 | 0.57 | .02 |
| Any long-term care use a | Total number of long-term care stays a | Long-term care expenditures | ||||||||||
| Child and community characteristics | β | 95% Confidence limits | p >|Z| | β | 95% Confidence limits | p >|Z| | β | 95% Confidence limits | p >|t| | |||
| Age | 0.10 | 0.09 | 0.11 | <.0001 | 0.08 | 0.07 | 0.09 | <.0001 | 0.03 | 0.02 | 0.03 | <.0001 |
| Sex | −0.18 | −0.22 | −0.13 | <.0001 | −0.19 | −0.24 | −0.14 | <.0001 | −0.06 | −0.08 | −0.05 | <.0001 |
| Total Months of Medicaid Coverage | −0.02 | −0.04 | 0.00 | .05 | 0.01 | −0.01 | 0.03 | .50 | −0.01 | −0.01 | 0.00 | <0.01 |
| Suicidal Ideation/Action or Psychosis | 1.52 | 1.42 | 1.63 | <.0001 | 1.80 | 1.69 | 1.91 | <.0001 | 2.50 | 2.46 | 2.53 | <.0001 |
| Developmental Comorbidities | −0.02 | −0.20 | 0.15 | .81 | 0.08 | −0.10 | 0.26 | .38 | 0.00 | −0.02 | 0.02 | .74 |
| Psychiatric Comorbidities | 1.87 | 1.70 | 2.04 | <.0001 | 1.96 | 1.79 | 2.14 | <.0001 | 0.56 | 0.54 | 0.57 | <.0001 |
| County Median Income | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 | 0.00 | 0.00 | .01 | 0.00 | 0.00 | 0.00 | <.0001 |
| Total County Mental Health Providers | 0.01 | 0.00 | 0.02 | .01 | 0.01 | 0.00 | 0.02 | .01 | 0.00 | 0.00 | 0.00 | <.0001 |
| SED Waiver | 0.95 | 0.69 | 1.22 | <.0001 | 1.19 | 1.00 | 1.39 | <.0001 | 2.51 | 2.18 | 2.85 | <.0001 |
Note. SED = severe emotional disturbance.
Poisson Models. bGLM Models with log-transformed expenditures.
Acknowledgements
We thank Dr. Roderick Rose for his methodological review of this study and manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research in this publication was supported in part by the University of Texas at Arlington’s Research Enhancement Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.