
Abstract
A systematic review was conducted to describe, and evaluate the effectiveness and cost-effectiveness of, intermediary services to support people with a disability to implement individualized funding plans. We included six records, including one subanalysis of randomized trial data, three qualitative studies, and two systematic reviews (reporting on 73 and 18 studies, respectively). No studies directly compared “consumer-directed plan plus intermediary services” to “consumer-directed plan with no/alternative intermediary,” so effectiveness of these interventions is uncertain. There is qualitative evidence from the perspective of disability planners and workers that intermediary interventions are important enablers of successful plan implementation. There is also qualitative evidence from consumer and family perspectives that external support is required to successfully navigate self-directed systems and that strong, trusting, and collaborative relationships with both paid and unpaid individuals in the person’s support network were facilitators of successful plan implementation. There was evidence of disabling practices and attitudes among some support agencies, resulting in coordinators being very risk averse in order to safeguard their clients. Suggestions for future research include carefully planned and ethically robust comparative trial designs, clear description and consistent delivery of interventions, and long-term evaluation of impact. The protocol was published on PROSPERO (CRD42020177607).
Services and supports for people with a disability have historically been delivered via institutionalized services or agencies, with a focus on medical needs (Benoot et al., 2021). In recent years, however, there has been a significant shift toward community-based health and social care services, including assistance with personal hygiene, dressing and feeding, or general life skills such as shopping, keeping active, working, and social participation with the service user placed at the center of decision-making and service delivery (Malley et al., 2012). This has led to a policy imperative that people with all disabilities should be autonomous and self-determined members of society (Fleming et al., 2019).
Individualized, or self-directed, service plans aim to facilitate empowerment, independence, and self-determination for people with disabilities. They enable the individual, and/or their family/caregiver, to plan, select, manage, distribute, and organize their own supports (Lakhani et al., 2018). They are now widely used in the United Kingdom, Ireland, Europe, Canada, and the United States. In the United States, they are known as Participant (or Consumer)-Directed Services (Sciegaj et al., 2016), and in the United Kingdom, Self-Directed Support (Harkes et al., 2014). These models have been consistently shown to positively affect participant satisfaction, and there is some evidence that they improve quality of life and sense of security (Fleming et al., 2019).
There are four main ways that people can self-direct their plan:
Open/user-led models, in which the budget holder is allocated cash payments which they can spend as they wish to support their needs or achieve their goals;
Planned/budgeted/managed models, in which the budget is paid to a host agency or provider who makes purchases on behalf of the budget holder for services or items included in an agreed plan;
Brokerage models: a third-party organization takes responsibility for overseeing administrative tasks and providing support, guidance or information to budget holders so that they can plan, arrange and manage their services and supports. This can include helping to develop an individual plan, establish a circle of support, negotiate costs with service providers, or commission bespoke services if none are available (Fleming et al., 2019).
Hybrid models, in which people can choose to use elements of open, planned and/or brokerage models.
All except Option 1 involve the use of an intermediary service, which some consumers need to assist them to understand and implement their individual plan, connect them to community or mainstream services, mitigate or manage crises, and build the person’s own capacity for self-direction and independence. In the United Kingdom, the National Audit Office has cautioned that if a personal budget is put in place without adequate support, information, or alignment with a user’s circumstance, it may not improve individual outcomes (Martinez & Pritchard, 2019).
For those who only require accurate and accessible information to support them to make informed choices, this may be provided by an advisory board (which can consist of family, friends, or other trusted individuals) or a dedicated officer (Harkes et al., 2014; Lombe et al., 2016). For those who need assistance with administration and financial management, a fiscal intermediary (Cook et al., 2004) may be engaged. Alternatively, a support broker (Timberlake et al., 2014) may be engaged to work with the person with a disability to negotiate with, coordinate, and hire professional support on their behalf, or research options within the local community to fulfill the goals of the plan. While these two services are sometimes conflated, it is considered important to maintain the independence of the brokerage/planning function from fiscal services to avoid conflicts of interest. This allows consumers (and their family or carers) to use “payroll” services without feeling obliged to use the same provider for planning and/or monitoring (Fleming et al., 2019).
These services are now a required element for any state in the United States wishing to set up a self-direction program option under Medicaid (U.S. Centers for Medicare and Medicaid Services, n.d.) which state “a supports broker/ consultant/ counsellor must be available to each individual who elects the self-direction option.” Guidelines in the Affordable Care Act (U.S. Government Publishing Office, 2014) further state that “If there is no support broker/agent required or chosen, the person must have training in acting as his/her own support broker” (Sebelius, 2014). A similar system applies in the Netherlands, where it is a program requirement for the user to have access to information and advice through an independent support broker, who can be a professional (such as a social worker) or a peer and the social insurance bank can manage employer responsibilities on behalf of consumers (Alakeson, 2016). In both countries, the consumer is not charged for the service, and advice and information must be independent of service providers as well as the initial assessment process. In Germany, however, it is an expectation that informal caregivers provide this, and in the UK legal and financial support is self-funded (Alakeson, 2016).
In Australia’s National Disability Insurance Scheme (NDIS) intermediary services are referred to as “Support Coordination,” which is organized into three different levels depending on the level of expertise and intensity of support the participant requires. These are Support connection; Coordination of supports; and Specialist Support Coordination (National Disability Insurance Agency, 2019). In the latter, the specialist may be an allied health professional or developmental educator; however, the first two levels may be delivered by NDIS staff/contractors (including specialist planners, Early Childhood Early Intervention services, community connectors in remote regions, Local Area Coordinators) or external providers (e.g., hospital discharge officers, recovery coaches for consumers with psychosocial disability, and justice liaison officers).
This rapid systematic review aimed to describe and, where possible, evaluate the effectiveness and cost-effectiveness of different interventions to implement individualized plans for people with disabilities. The specific review questions were as follows:
What are the key components of intermediary plan implementation models; and
What evidence exists regarding the effectiveness and cost-effectiveness of intermediary plan implementation services?
Method
This review used a “rapid review” approach, which allows an overview of evidence in a short time (Wright & Bragge, 2018). Whereas standard systematic reviews can take up to 2 years to complete, rapid reviews seek already synthesized research evidence and, where these are not available, high-quality or recent primary studies. Rapid review processes are similar to those used in systematic reviews, including establishing a search strategy, stating inclusion and exclusion criteria for literature screening and selection, data extraction, quality appraisal, and a synthesis of findings (Borg et al., 2019). The review protocol was registered with PROSPERO (CRD42020177607). The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) was used as a reporting framework.
Search Process
An initial limited search of PubMed, MEDLINE, and ASSIA (Applied Social Sciences Index and Abstracts) was undertaken to identify articles on the topic. The text contained in the titles and abstracts of relevant articles, and the index terms used to describe the articles were used to develop a full search strategy for report the name of the relevant database (see Appendix S2). The search strategy, including all identified keywords and index terms, was adapted for each included information source. The reference list of all studies selected for critical appraisal was screened for additional studies.
We searched The Cochrane Library, The Campbell Collaboration, Social Systems Evidence, ASSIA (Applied Social Sciences Index and Abstracts), EmBase, PubMed, PsycINFO, and Google Scholar. A search strategy with four strings was used to yield relevant sources. Below is the search strategy applied to the PubMed database, conducted on March 26, 2020, and repeated on April 12, 2021:
Disab* OR impair* OR disorder
Coordinat* OR “case manage*” OR “case work*” OR plann* OR broker* OR support* OR intermed* OR partner
Effect* OR cost-effect* OR evaluat*
“Quality of Life” OR Satisf* OR Independen* OR “daily living” OR particip*
Limits applied: Systematic Review or Randomized Controlled Trial or clinical trial, published from 2010 to 2020, in English.
All database searches were conducted between March 26 and April 2, 2020, and a repeat search was conducted using PubMed on April 12, 2021, to check if any relevant papers were published in the interim 12 months. In addition, we hand-searched references from all relevant papers and found 30 references dated on or after 2010. The full text of all 30 references was retrieved and considered; however, no additional studies were included in this systematic review.
Screening and Selection of Studies
One reviewer (I.R.) screened citations against the inclusion and exclusion criteria listed below. Potentially relevant studies were retrieved in full and assessed in detail against the inclusion criteria by two independent reviewers (I.R. and L.O.B.). Any disagreements that arose between the reviewers at each stage of the study selection process were resolved through discussion.
Inclusion criteria
Primary aim: Described or evaluated intermediary interventions designed to facilitate individual plan implementation for people with disabilities (any age). Outcomes of interest were quality of life, consumer satisfaction, and measures of independent living or participation. For cost-effectiveness, we planned to compare data that compared the specific model with any other model.
Publication type: For Question 1 (which aimed to collate descriptions of intermediary plan implementation/support models), we considered published case series or case studies as well as descriptions (e.g., reports and website text) of support models. For Question 2 (regarding the effectiveness and cost-effectiveness of these service models), we considered systematic reviews and both experimental and quasi-experimental study designs including randomized controlled trials, non-randomized controlled trials, before and after studies, and interrupted time-series studies. In addition, comparative observational studies including prospective and retrospective cohort studies were considered for inclusion.
Exclusion criteria
Studies published prior to 2010 (given the recent advances in self-direction policy and practices for people with a disability) and in a language other than English.
Conference or dissertation abstracts, book chapters, and discussion/conceptual/protocol papers without participant data.
Assessment of Methodological Quality
Eligible studies were critically appraised by one reviewer (L.O.B.) at the study level for methodological quality in the review using checklists available through CASP (Critical Appraisal Skills Programme, 2018). Although one paper was mixed method in design, the major methodology was qualitative; hence, it was rated against the qualitative checklist.
Data Extraction
Data were extracted from studies included in the review by both reviewers. We extracted specific details about the populations, study methods, interventions, funding sources, eligibility criteria for service, the provider of the service, and outcomes of significance to the review objective.
Analysis
The absence of comparative trials and heterogeneity of the review results precluded a quantitative meta-analysis. The output of the review is therefore a narrative summary of findings, focused on their contribution to each research question. We were unable to use the Grading of Recommendations Assessment, Development and Evaluation (GRADE) for quantitative data due to the diverse nature of the available studies, and data precluded the possibility of a meta-analysis.
Results
A total of 5,042 records were identified across all searches; 56 were duplicates and removed automatically using Covidence, an online systematic review tool (Veritas Health Innovation, n.d.). The abstracts of the remaining 4,986 records were screened by one reviewer (IR), with 4,959 excluded at this stage. The remaining 27 full texts were screened by two reviewers (L.O.B. and I.R.) and a further 21 were excluded as they did not describe or evaluate an intermediary plan support intervention. Figure 1 illustrates this process using a PRISMA flow diagram.
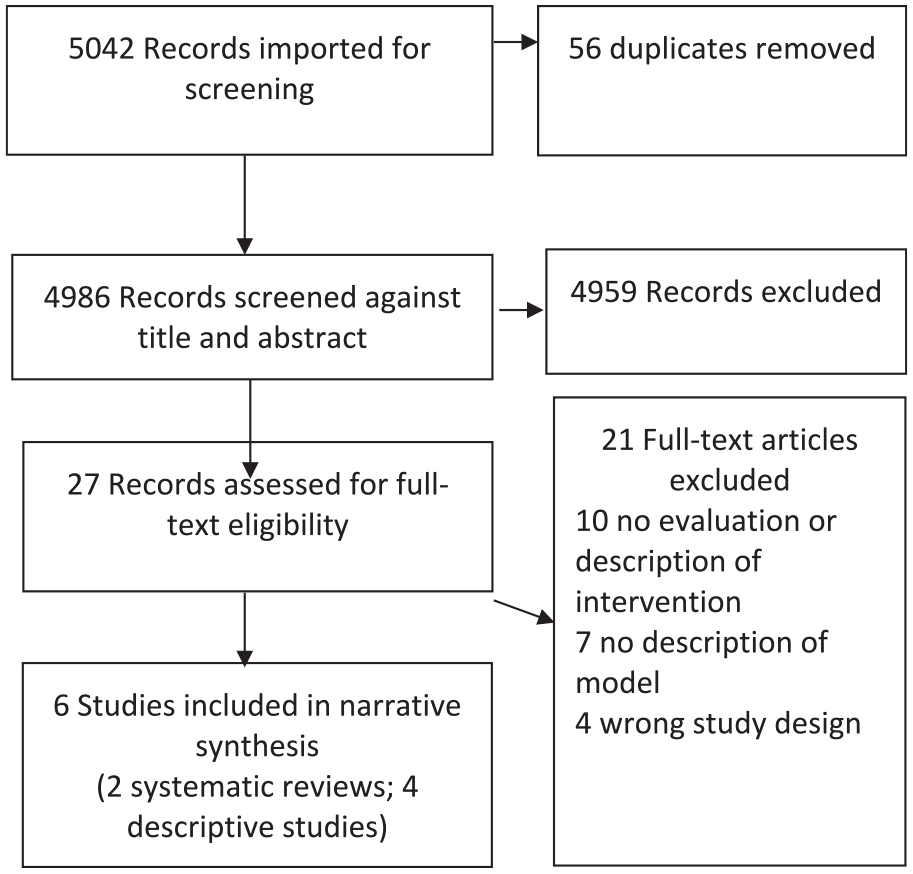
PRISMA flow diagram for rapid review.
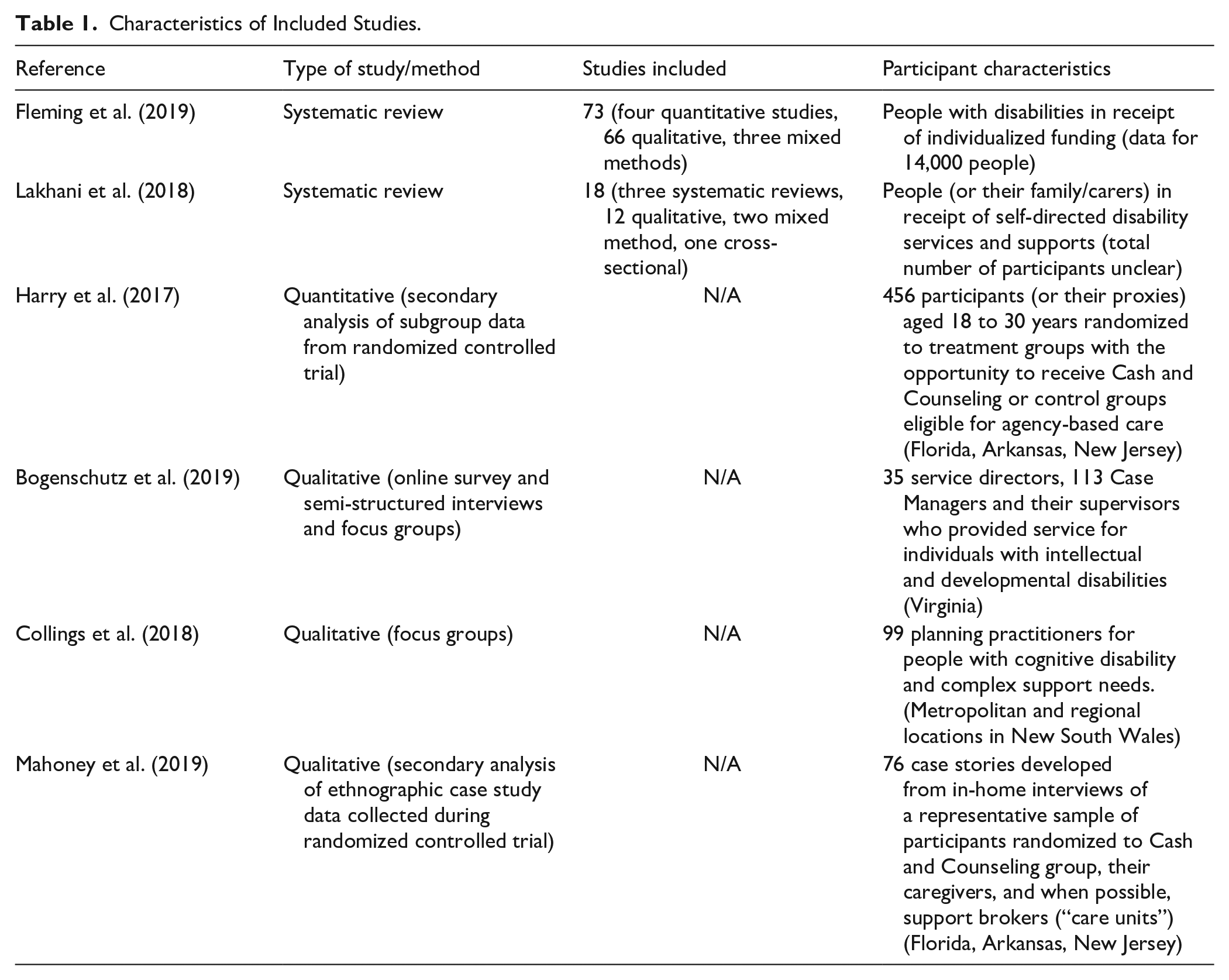
Of the six remaining, four peer-reviewed papers described either the structure of models or the key activities performed by intermediary services, which provided useful insights into how they had been implemented. Two systematic reviews, one focusing on facilitators of service users’ engagement and choice-making (Lakhani et al., 2018) and the other on the effectiveness of individualized funding interventions, but not specifically intermediary services (Fleming et al., 2019), were included as both provided syntheses of qualitative data relating to either consumer/family and/or staff perspectives of these services. None of the studies included in either review directly compared “consumer-directed plan plus intermediary services” with “consumer-directed plan with no/alternative intermediary,” and we found no comparative studies published after these reviews. Characteristics of included studies are summarized in Table 1.
Characteristics of Included Studies Related to Support for Implementing Individualized Funding Plans.
Quality Appraisal
One of the two systematic reviews (Fleming et al., 2019) was exceptionally rigorous and fulfilled all relevant criteria on the CASP Systematic review tool. The other (Lakhani et al., 2018) however had a weaker and narrower search strategy and unclear assessment of the quality of included articles. The one randomized controlled trial (Harry et al., 2017) presented secondary data analysis of data collected between 1999 and 2003 during the Cash and Counseling Demonstration and Evaluation (CCDE) randomized control trial in the United States which compared “Cash and Counseling” with “agency-based care as usual.” They specifically focused on a subgroup of participants age between 18 and 30 years; however, there were significant dropouts in the intervention group (25% in one state), which was not explained and no blinding of data collectors. The qualitative studies included were generally of good quality, although none provided clear statements regarding the relationship between researcher and participants. Results are summarized in Table 2 in the Supplemental Material.
What Are Key Components of Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans?
Of the four original research papers, two described the United States “Cash and Counselling” model (Harry et al., 2017; Mahoney et al., 2019), one described Case Management services for people with intellectual and developmental disabilities (Bogenschutz et al., 2019), and one explored planning supports for people with complex support needs across disability, mental health, alcohol and other drugs, housing, and criminal justice (Collings et al., 2018). Components are summarized in Table 3 (Supplemental Material).
Common to all models was the provision of information about how to manage the self-directed plan, and referral or direct linkage to services in the community. All highlighted the need for the intermediary to know about or find the right service, as people with complex needs may have had negative past experiences when attempting to access services. All except one (Collings et al., 2018) specifically included ongoing monitoring as part of the role. Assistance with financial management was not mentioned in two of the studies, but was explicit in the “Cash and Counselling” studies. This model includes services delivered by a Fiscal intermediary who helped manage the budget, wrote checks for hired support workers, and took responsibility for other payroll duties, such as withholding taxes.
The manner in which intermediary services were delivered was most important, with participants in one of the Cash and Counseling studies (Mahoney et al., 2019) valuing familiarity, proactivity, cultural friendliness, responsiveness, and supportive relationships with their broker. This was echoed from the provider’s perspective, with building rapport, avoiding shortcuts and rushed approaches to decision-making, and supporting the person to learn being key priorities (Collings et al., 2018).
What Do We Know About the Effectiveness of Intermediary Services?
We did not identify any comparative studies that experimentally compared an intermediary service intervention against an alternative (or no service) in terms of consumer outcomes or cost-effectiveness. Evaluation typically examined consumers’ and providers’ perceptions of benefit or facilitators of successful plan implementation.
From consumers’ perspectives, Fleming et al., 2019 systematic review mapped qualitative data from 66 qualitative and three mixed methods studies. They found qualitative evidence that strong, trusting, and collaborative relationships with both paid and unpaid individuals who formed the person’s network of support were facilitators of successful plan implementation. Consumers particularly valued assistance with information sourcing, recruitment of support workers, network building, and support with administrative and management tasks. The systematic review by Lakhani et al. (2018) included three review articles and 15 original studies (12 qualitative, two mixed methods, and one cross-sectional survey) and similarly concluded that independent third-party advisors supported informed decision-making among consumers and their families regarding budgeting or hiring of support workers. The authors concluded that service users and families need external support if they are to successfully navigate self-directed systems, plan and manage their budgets, and determine how they will allocate their funded resources among their choice of supports and services.
From the perspective of disability service workers, Fleming et al. (2019) concluded that “support and other human resources . . . such as intermediary services, community integration, and innovative/creative supporters” was a facilitator of successful plan implementation.
Adverse Effects
Fleming et al. (2019) found “extensive evidence of disabling practices and attitudes among some funding bodies and support agencies” which appeared related to fears regarding misuse of funds or other fraudulent activities by people with a disability or their network of support. This resulted in a tendency for planners or coordinators to be very risk averse in order to safeguard their clients. The qualitative data showed that fears were generally alleviated after successful plan implementation, and the establishment of strong networks of paid and/or unpaid support. No other harms associated with using an intermediary service were found in any other papers.
Discussion
This review is, to our knowledge, the first to describe and evaluate intermediary services to support people with a disability to implement individualized funding plans. We found no quantitative data comparing intermediary services with either “no service” or an alternative model, so their effectiveness (and cost-effectiveness) is uncertain.
We found consistent qualitative evidence from two systematic reviews that consumers and their families believe independent intermediary services supported them in informed decision-making, information sourcing, budget planning and management, hiring of support workers, network building, and administrative and management tasks. This is mostly consistent with consumer ratings from the only large-scale randomized controlled trial, the CCDE (Brown et al., 2007), which compared a new self-directed funding model (Cash and Counseling) to traditional agency-based service in three U.S. states. In this trial, which was conducted from 1998 to 2002, consumers randomized to the new model (N = 3047) were required to use counseling services (which covered how to set up their spending plans and how to recruit and train support workers); however, fiscal intermediary services were optional. Participant satisfaction with assistance to develop their spending plan was high (varying between 62.1% in the Florida participants age >60 years to 87.4% in Arkansas 18–64 years group) although lower ratings were achieved for recruiting and training workers (28.3%–57%). Interestingly, 93% chose to use fiscal intermediary service and were very satisfied with them. In all participating states and all age groups, 85%–95% of users of intermediary services found them to be helpful.
We also found evidence that some funding bodies and support agencies constrained consumers by being overly protective and risk averse, especially during early stages of plan implementation. This worrying finding was also evidenced in the Personal Outcomes Evaluation Tool (POET; Think Local Act Personal, 2017) results for 4,300 adults in receipt of personal budgets and personalized care and support in the United Kingdom, where only half (51%) of consumers said they could decide how the money in their personal budget was spent.
Our finding of that disability service workers regard intermediary services and community integration efforts as a key enabler of successful plan implementation is also supported by the literature. Fleming, 2016 research brief (Fleming, 2016) of four pilot individualized funding initiatives in Ireland found that “the availability of a ‘circle’ of natural supports provided significant benefits for consumers in terms of helping them learn to actively engage with the community, especially when learning new social, decision-making and independent living skills.” Where this was absent, intermediaries (e.g., organizational staff, broker, key worker, or mentor) identified and engaged with potential advocates. Those who performed this role best were described as
practical, amenable, friendly and encouraging in their approach. Other personal attributes that were important included having: vision; innovation; personal experience of disability; a willingness to challenge stakeholders and an active role in the community. Essential for all stakeholders was an appreciation of an individual’s abilities, passions and interests.
For populations who struggle to access online or written information, such as older people, those with mental health issues, or those with low literacy, these services are likely to be particularly important. A UK study exploring the experiences of using self-directed support and personal budgets for older people and those with mental health issues interviewed 69 scheme participants and carers, 40 practitioners and managers, and 12 support provider organizations, including five user-led organizations (Newbronner et al., 2011). They found that it was usually the time spent discussing their plan with their social worker, community psychiatric nurse, or support provider organization that was most helpful in its implementation. Community advocates have flagged that vulnerable populations, particularly those experiencing homelessness and/or mental health disability, are in many cases unable to appropriately engage with the supports identified in their plan without assistance (Kenyon, 2018).
Similarly, Australian parents of children with complex disabilities such as autism have highlighted the importance of this service when seeking supports
The only way to find quality services is via a good support coordinator, friends in the same situation or a lucky Google search. Now the NDIS has an up-to-date service provider list, but it still takes a lot of time and luck to find services that meet your needs. (Livanos, 2018)
and “I like that [broker] takes care of it, it is overwhelming to me . . . stressful situations get me upset, I could not do it [manage child’s plan] without help” (Timberlake et al., 2014). This preference was also noted in another Australian study (Valentine, 2010) which concluded that families want the “best” service or provider and prefer to rely on experts and professionals to decide what is “best.” A UK study of 111 young people with progressive disabling conditions, their parents, adults, and older people with fluctuating or sudden support needs (Rabiee & Glendinning, 2010) also found that many felt they did not have access to information that could enable them to make “informed” choices.
Limitations
Rapid reviews, by their nature, can lack the detail that traditional systematic reviews and a more detailed review might yield differing results. To mitigate this, the author of the most recent and comprehensive review (Dr Padraic Fleming) was contacted, and he concurred that no quantitative studies exist comparing “consumer-directed plan plus intermediary services” to “consumer-directed plan with no/alternative intermediary.”
We restricted our search to publications in English, which may mean we omitted relevant studies published in other languages. In addition, only one author conducted quality appraisals due to resourcing available to conduct the review.
Implications for Policy Development
Whilst some individuals may be “consummate consumers” (Alakeson, 2016), others will need greater assistance in implementing their plan due to isolation from their local community, lack of experience in navigating the funding system, or the ability to effectively procure and manage their own services. Ideally, policy should ensure that the level of support provided is flexible, informed by the consumer’s current needs and access to family or peer support, and should respect the individual’s choice and control. It may be helpful to conceptualize this as a two-tier system, as described by Carter Anand et al. (2012):
Professionally assisted: service users receive short-term assistance from case managers, coordinators, or brokers to access funding and implement their plan. The professional/agency/broker may also assist with decisions regarding management of support workers, purchasing of services or goods necessary to meet their needs and goals. Optional independent professional counseling and advice may be available, separately from the funding, to assist the service user. The “Cash and Counselling” model is an example of this type of service.
Professionally monitored: service users receive guidance over time from care managers or coordinators, who are also responsible for monitoring services according to the approved plan. Health professionals usually play a key role in the assessment and care planning processes. The “Direct Payments” (UK) program is an example of this, in which local councils (England and Wales) or Health and Social Care Trusts (Northern Ireland) make personal budgets available then provide a case manager (social worker or nurse) to develop and monitor the plan.
Finally, policy should guarantee that advice and information should remain independent of service providers as well as the initial assessment process. In the United States, the Centers for Medicare and Medicaid Services (Kako et al., 2013) have articulated the following core characteristics of conflict-free intermediary services (referred to as case management):
Responsibility for providing case management services is separated from responsibility for the provision of direct services and supports.
Case managers are not employed by an entity providing services.
Case managers are not responsible for determining individual funding levels.
Recommendations for Research
This review has highlighted the lack of robust effectiveness data on what is a complex social intervention. This is due to the inherent ethical and logistical challenges associated with collecting quantitative data via controlled comparative methods. We therefore suggest that future pilot trials include methodologically rigorous evaluation plans before rollout. Where it is unethical or unfeasible to randomize participants, observational study designs, often referred to as comparative effectiveness research (CER) (Sox & Goodman, 2012), may be used to directly compare the results of different interventions. While these designs lack the statistical purity of randomized controlled trials, results can be both scientifically rigorous and more relevant to consumers and decision makers as long as comparison groups are either matched at baseline or controlled for in analysis. The authors also suggest realist evaluation methods which allow for real-world evaluations of complex interventions within complex systems (HM Treasury, 2020).
Conclusion
Intermediary services are widely used internationally, but seldom described in detail or evaluated. Although they have not been tested experimentally, existing qualitative research suggests they are valued by consumers and are a major facilitator of successful plan implementation, providing support agencies avoid overly risk-averse attitudes. A clearer understanding of their effectiveness for different populations would require carefully planned and methodologically robust comparative trial designs, clear description and consistent delivery of interventions, and long-term evaluation of impact.
Supplemental Material
sj-docx-1-dps-10.1177_10442073221130529 – Supplemental material for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review
Supplemental material, sj-docx-1-dps-10.1177_10442073221130529 for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review by Lisa O’Brien and Ivana Randjelovic in Journal of Disability Policy Studies
Supplemental Material
sj-docx-2-dps-10.1177_10442073221130529 – Supplemental material for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review
Supplemental material, sj-docx-2-dps-10.1177_10442073221130529 for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review by Lisa O’Brien and Ivana Randjelovic in Journal of Disability Policy Studies
Supplemental Material
sj-docx-3-dps-10.1177_10442073221130529 – Supplemental material for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review
Supplemental material, sj-docx-3-dps-10.1177_10442073221130529 for Intermediary Services to Assist People With Disabilities to Implement Individualized Funding Plans: A Rapid Systematic Review by Lisa O’Brien and Ivana Randjelovic in Journal of Disability Policy Studies
Footnotes
Acknowledgements
The authors thank Assistant Prof. Claire Harris (Research and Evaluation, NDIS), Bridey Sanders and Deanne Williams (Provider and Markets, NDIS), and Hannah Simkin and Fiona Cromarty (Partner Program, NDIS) for input into the protocol for this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.