
Abstract
Introduction:
Indigenous peoples in Canada continue to experience major health inequities and lower-quality care. Cultural safety provides a framework to address these disparities by transforming provider attitudes and practices and emphasizing the need for education and training to improve health care experiences and outcomes.
Methods:
This paper deepens the understanding of cultural safety within Indigenous health care by highlighting the ongoing impacts of colonialism, systemic racism, and historical trauma on Indigenous health outcomes, and explores the role of nurses in advancing health equity.
Results:
The paper highlights gaps in nursing practice, including limited tools to assess cultural safety from Indigenous perspectives, and underscores nurses’ responsibility to support systemic change aligned with Truth and Reconciliation Commission Calls to Action and United Nations Declaration on the Rights of Indigenous Peoples.
Discussion:
By identifying these issues and analyzing their impact on nursing practice, this paper underscores the urgent need for culturally safe approaches that are reflective, patient-defined, and embedded within both individual and institutional levels of care.
Introduction
Growing evidence indicates that Indigenous peoples of Canada face significant health disparities and receive lower-quality health care services compared with non-Indigenous populations (Chakanyuka et al., 2022). These disparities among Indigenous peoples in health and health care have grown larger over time (Katz et al., 2021). Health disparities are complex and rooted in various underlying issues, such as systemic injustice, racism, and the enduring legacy of colonialism, all of which affect every part of society, including health care (Chakanyuka et al., 2022; Katz et al., 2021). Indigenous peoples’ encounters with health care are commonly negative, due to negative stereotypes, racism, and past harms, leading to avoidance in seeking medical care, and there is concern that these experiences can contribute to further adverse health outcomes (Goodman et al., 2017; Hole et al., 2015; O’Sullivan, 2013).
Cultural safety is a framework used in health care to help reduce the health inequalities between Indigenous and non-Indigenous people. It aims to mitigate these factors by transforming the attitudes and behaviors of health care providers (HCPs), fostering a health care setting free from racism and stereotypes, and ensuring that Indigenous peoples are treated with “empathy, dignity, and respect” (O’Sullivan, 2013, p. E27). Cultural safety helps patients feel more respected, heard, and in control of their own health care decisions. When cultural safety is practiced, patients feel safe to speak up and share their concerns or preferences. In return, cultural safety helps patients feel more respected, heard, and in control of their own health care decisions. This then creates a trusting relationship, where the patient and provider work together as partners to find the best path for care. As a result, care becomes more effective because it is based on mutual respect, shared decision-making, and cultural understanding, not just what the provider thinks is best (Carlson & Redvers, 2023; McGough et al., 2022; Wylie et al., 2021).
Furthermore, the adoption of cultural safety practices can increase confidence in care delivery among HCPs. Importantly, cultural safety has been shown to reduce the avoidance or delay of medical care, promote treatment compliance, and encourage participation in preventive health care measures like screenings and immunizations among Indigenous populations (O’Sullivan, 2013). Therefore, HCPs have a responsibility to deliver care that is culturally safe to properly support Indigenous peoples in Canada (Yeung, 2016). Addressing the complex and historically rooted health needs of Indigenous peoples is especially important for nurses because they serve as the most consistent point of contact in health care settings, positioning them uniquely to support the health needs of Indigenous peoples through trust-building, advocacy, and continuity of care. (Barbo & Alam, 2024; Wilson et al., 2022). Moreover, their consistent presence allows them to coordinate care, advocate for patients’ needs, and mitigate challenges arising from fragmented health services (Karam et al., 2021; Kwame & Petrucka, 2021).
Method
In this paper, based on a broad review of the literature, we will use the framework of cultural safety to examine how historical and ongoing colonial practices have contributed to health disparities among Indigenous peoples in Canada. We define the concept of cultural safety and explore how it differs from related terms. Using the cultural safety framework, we begin to address the persistent gap in culturally safe nursing care by exploring how power imbalances, systemic racism, and lack of effective implementation continue to undermine equitable health care. By identifying these issues and analyzing their impact on nursing practice, this paper will underscore the urgent need for culturally safe approaches that are reflective, patient-defined, and embedded within both individual and institutional levels of care.
Results
Historical Factors That Influence Indigenous Peoples’ Health
Indigenous peoples of Canada have experienced a history of colonization and cultural genocide through residential schools and other governmental policies such as the Indian Act of 1876, leading to historical trauma and the loss of cultural structure (Dell et al., 2016; Katz et al., 2021; Yeung, 2016). The effects of colonization are evident in Indigenous peoples’ health and well-being, affecting not only their physical health but also their mental, emotional, and spiritual health (Loppie & Wien, 2022). These health disparities have been a result of assimilation leading to physical and emotional harm to children, lower educational achievement, loss of land, culture and language, and the breaking apart of Indigenous families and traditional ways of raising children (Katz et al., 2021; Wilk et al., 2017).
Many of the co-morbidities experienced by Canada’s Indigenous peoples include obesity, diabetes, and cardiovascular disease that are health effects directly linked to colonization (Wilk et al., 2017). For instance, diabetes was extremely rare among Indigenous peoples in Canada before the 1940s (Howard, 2014). It has become increasingly common among Indigenous peoples in Canada and is now considered an epidemic. Compared with the general Canadian population, Indigenous individuals are being diagnosed as having diabetes more frequently and at younger ages (Cheran et al., 2023; Howard, 2014). Studies have shown that type 2 diabetes and its complications occur at rates two to five times higher in Indigenous populations than in non-Indigenous peoples in Canada (Cheran et al., 2023). Furthermore, the negative impacts of the residential school system, which was designed to assimilate Indigenous children into European Canadian culture, are being passed down through multiple generations (Wilk et al., 2017). Research has shown that children of individuals who attended these schools tend to have worse health compared with children whose parents did not attend. In addition, families where more than one generation attended residential schools experience even greater health disparities, meaning that the negative effects of the system, such as trauma, poverty, and disconnection from culture, accumulate over time and affect the health of descendants, resulting in intergenerational trauma (Wilk et al., 2017).
The Truth and Reconciliation Commission (TRC) of Canada has emphasized the need for improved tracking and reporting of health differences between Indigenous and non-Indigenous peoples to reduce these health gaps. The TRC points out that these disparities, where Indigenous peoples generally experience worse health outcomes than non-Indigenous peoples, are directly tied to harmful policies created by past Canadian governments. They are not viewed as isolated issues but as ongoing consequences of colonization and policies that intentionally targeted Indigenous peoples (Katz et al., 2021; TRC, 2015). The TRC Calls to Action, particularly Call to Action #18, urge federal, provincial, territorial, and Indigenous governments to acknowledge that the current state of Indigenous health in Canada stems directly from historical government policies, including the residential school system. This call to action emphasizes the need to recognize and uphold Indigenous peoples’ inherent right to health care, as affirmed through international law, constitutional law, and Treaty obligations. Call to Action #18 highlights that the health disparities experienced by Indigenous peoples are a lasting legacy of colonial practices that sought to erase or diminish Indigenous cultures, rights, and well-being, which have effects that continue to shape the health of Indigenous communities today (TRC, 2015).
Enhancing health outcomes for all populations is a continuous global objective, with particular emphasis on Indigenous peoples worldwide. This aim is highlighted in the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) (Moloney et al., 2023; United Nations [UN], 2007). Established in 2007, UNDRIP is a declaration designed to support reconciliation between Indigenous and non-Indigenous peoples. This international human rights declaration protects individual and collective rights of Indigenous peoples around the world, including rights to culture, identity, language, employment, health, education, and self-determination (UN, 2007).
The implementation of UNDRIP in Canada aims to support Indigenous self-determination and improve access to culturally safe, community-driven health care. It also provides direction for governments and health systems to respect Indigenous knowledge and governance, ensuring future policies uphold both constitutional and international responsibilities. It is meant to support a long-term change toward reconciliation, justice, and equity (Government of Canada, 2021a). The UNDRIP is not yet fully upheld in this country, as acknowledged in the 2024 Government of Canada’s progress report, which points out that to make meaningful progress, the government must coordinate better, set fair and efficient timelines, track results clearly, ensure enough funding, and make sure responsibilities are well-defined (Government of Canada, 2024). However, Canada’s Government initially rejected this declaration, and it was not until 2016 that it revised its position. The initial refusal of this declaration from the Canadian Government has negatively affected health and health care for Indigenous peoples, resulting in the further exacerbation of intergenerational traumas and the ongoing colonization of health care delivery (Moloney et al., 2023).
Defining Cultural Safety
Cultural safety originated in the 1980s from the work of Māori nurse Ramsden as a political response to the poor health of Māori people and inadequate nursing care for Indigenous peoples in New Zealand (Guerra & Kurtz, 2016; Moloney et al., 2023). She developed this concept within nursing education in response to the negative health effects from colonization on the Indigenous peoples of New Zealand (Moloney et al., 2023; Yeung, 2016). Cultural safety and cultural humility are closely related yet distinct concepts that are important to compare when considering culturally appropriate care. Cultural safety aims to create health care environments where patients feel respected, free from racism and discrimination and grounded in the strengths of identity, culture, and community (Northern Health, 2025). Cultural humility means that nurses continuously reflect on their own values, beliefs, and biases, and recognize how these influence their interactions with patients. By approaching care this way, nurses build trust and create culturally safe environments where patients feel empowered to share their needs. Cultural humility then becomes the foundation for culturally safe nursing practice, and it is how nurses ensure that care is genuinely person-centered and free from assumptions or power imbalances (Northern Health, 2025).
The philosophical underpinnings of cultural safety are about sharing respect, knowledge and experience while learning with dignity and awareness. This calls for HCPs to think critically about their own identity, culture, and any unconscious biases or stereotypes they may hold, as these influence how they interact with patients. It emphasizes that building a respectful and effective patient-practitioner relationship starts with self-awareness. It also calls for HCPs to learn about the broader social factors like housing, education, income, and access to care that affect Indigenous people’s health today, especially as these issues are shaped by the lasting impacts of colonization (Yeung, 2016).
Nurses are encouraged to reflect on their culture, values, and beliefs to better understand and respect cultural differences. Cultural safety is achieved not only through this personal reflection but also by addressing systemic inequalities within health care. This approach helps create a more respectful and inclusive environment for Indigenous patients (McGough et al., 2022). Horrill (2020) argues that cultural safety is not knowing about specific cultural beliefs, and practices, or about being exclusively sensitive to diverse perspectives. Although these aspects have value, they often fail to address the influence of power dynamics within health care systems and often overlook the broader context of patients’ lives, including the social and structural factors that shape health outcomes and access to care (Horrill, 2020). Instead of assuming that understanding someone’s cultural context is enough, cultural safety means creating an environment where the patient feels respected, safe, and heard. Therefore, only they can decide if their care is culturally safe. It shifts the focus from provider knowledge to patient experience and empowerment (Wilson et al., 2022).
Cultural safety is rooted in critical theory and social justice principles (Kerrigan et al., 2020). Social justice in the health care system refers to providing equitable health care services for all individuals, regardless of their circumstances (Habibzadeh et al., 2021). According to Todic et al. (2022), health disparities, such as the unequal health outcomes that are seen in marginalized groups, are caused by social injustices, such as racism or inequality. Because of this, you cannot resolve these issues by overlooking power dynamics. Critical theory encourages us to look closely at the systems of power that create and maintain these health gaps. It is about understanding the root causes, not just the symptoms (Todic et al., 2022).
Todic et al. (2022) further explain that critical theory urges HCPs to shift away from viewing health disparities as merely the result of individual actions or behaviors and toward an understanding that considers historical, social, and structural factors. By doing so, HCPs can accurately identify the true causes of health inequalities and work toward addressing them. Furthermore, by exposing social problems through analyzing power relations, critical theory seeks to remove them through praxis, a thoughtful reflection with practical action in a way that is informed by a deep, critical understanding of the issues (Todic et al., 2022). Critical theory calls for HCPs and health organizations in positions of power to engage in self-reflection and critically examine the systems that sustain health inequities (Kerrigan et al., 2020). In nursing, critical theory serves as a tool to address structures of power, politics, and injustice within health care systems, supporting advocacy for system change (Zaben, 2024).
Addressing the Gaps in Cultural Safety
There is an urgent need to enhance HCP’s competencies through cultural safety education and training programs to promote culturally sensitive and safe care for Indigenous individuals (Wylie et al., 2021). Health care organizations have the ability to influence the health care environment in ways that reduce the likelihood of implicit and explicit biases among providers. Health care inequities do not arise because HCPs lack awareness of cultural diversity but rather from systemic issues such as unequal power dynamics, marginalization, bias, unacknowledged privilege, and institutional racism (Curtis et al., 2019).
For example, in September of 2020, Joyce Echaquan, a First Nations woman, broadcasted a live stream on Facebook revealing hospital staff directing racist insults at her while she was dying in a Quebec hospital (Wylie et al., 2021). Questions were raised about the quality of the care received by the patient and the inappropriate comments made about her resulting in a legal investigation (Kamel, 2020). The young mother’s death was partially caused by racism and prejudice that she encountered while trying to receive medical care. The report emphasizes that the systemic and personal biases faced by the woman played a significant role in the tragic outcome (Kamel, 2020; Stevenson & Tobias, 2023).
As a result of her death Joyce’s Principle was created. It is a framework that requires governments to guarantee Indigenous people equitable access to health and social services without discrimination and the right to the best possible physical, mental, emotional, and spiritual health. It also mandates the recognition and respect of Indigenous knowledge in all aspects of health and was developed to implement the principles of the UNDRIP (Council of the Atikamekw of Manawan & Council de la Nation Atikamekw, 2020; Government of Canada, 2021b). In addition, the Canadian Nurses Association (CNA) and the Canadian Indigenous Nurses Association (CINA) are dedicated to improving the health outcomes of Indigenous peoples in Canada by promoting culturally responsive care, combating racism and supporting Indigenous nurses. Both national organizations support policies like Joyce’s Principle to address systemic inequities in services for Indigenous peoples (CNA, 2025a, 2025b).
While the concept of cultural safety is well-established in academic and educational fields, especially in nursing, there is still room for improvement in its application and in evaluating the outcome in clinical settings. A 2024 scoping review by Clough et al. examined cultural safety initiatives in Australian hospitals and found that evaluations predominantly focused on HCP’S attitudes and knowledge, with minimal attention to patient experiences. Notably, only one out of nine studies assessed patient outcomes, despite cultural safety being defined by the recipients of care. The review also identified a lack of validated evaluation tools and theoretical frameworks guiding these initiatives, indicating a need for evidence-based and patient-centered approaches (Clough et al., 2024). Policies that guide cultural safety present significant challenges in evaluating and ensuring its proper implementation in health care settings due to the lack of measurable outcomes. There is a need for better tools, indicators, and commitment from health organizations to address this gap to implement best practices in providing culturally safe health care (McGough et al., 2022).
To begin to address this gap, Sehgal et al. (2024) offer a framework aimed to better capture the complex health needs of Indigenous peoples in Canada. The authors explain that existing patient complexity assessment tools are rooted in a biomedical model and fail to consider the social, cultural, historical, and structural factors that shape Indigenous health experiences. Using a multi-phase approach, including a scoping review, qualitative interviews with Indigenous patients, and a modified Delphi consensus process with experts, the researchers developed a nine-domain framework consisting of 27 concepts. These domains include biological, social, health literacy, psychological, functioning, health care access, adverse life experiences, resilience and culture, and health care violence. This framework shifts the understanding of patient complexity away from viewing individuals as “difficult” or “noncompliant” and toward recognizing the systemic impacts of colonization, racism, and social inequities. The authors emphasize that the tool aims to promote culturally safe care and align with the TRC’s Calls to Action by helping HCPs understand the broader context of Indigenous patients’ health (Sehgal et al., 2024).
The authors conclude that the Indigenous-centered patient complexity framework is an important step toward promoting health equity for Indigenous peoples in Canada. They suggest it can guide HCPs, systems, and policymakers in better understanding and addressing the complex factors influencing Indigenous health, ultimately improving outcomes and supporting reconciliation. The next phase involves developing and testing a practical assessment tool based on the framework to ensure its effectiveness in real-world health care settings (Sehgal et al., 2024). Thus, research on cultural safety and related training interventions requires greater clarity. The methods currently used to assess the effectiveness of cultural safety training and related interventions may not be rigorous enough. Therefore, research is needed to develop appropriate, more reliable ways to measure whether these programs are truly improving the delivery of culturally safe care in health care settings (MacLean et al., 2023; McGough et al., 2022). Stevenson and Tobias (2023) suggest that to assess whether these programs are effective, it is important to evaluate HCP’s behavioral outcomes, patient health outcomes, and patient satisfaction. Health care systems can then determine whether their cultural safety interventions are truly effective in improving patient care and experiences (Stevenson and Tobias, 2023).
Measuring cultural safety training strategies in health systems in collaboration with Indigenous peoples can help identify where the problems are to target quality improvement efforts (Canadian Institute for Health Information, 2019; McGough et al., 2022; Stevenson & Tobias, 2023). The true measure of cultural safety programs cannot come solely from HCPs, institutions, or external evaluators. Instead, it must be assessed based on the experiences and perspectives of Indigenous patients and communities who directly interact with the health care system. Their feedback will reveal whether these programs are effectively improving the quality of care, increasing cultural understanding, and ensuring that Indigenous people feel respected and safe within health care systems (Hardy et al., 2023; Kerrigan et al., 2020).
Discussion
Even though system-wide changes take time, nurses can still make a positive impact by practicing cultural safety (McGough et al., 2022). Given that cultural safety is about the balance of power between HCPs and people receiving care, nurses need to address their “biases, attitudes, assumptions, stereotypes, prejudices, structures, and characteristics that may affect the quality of care and engage in self-reflection” (Pirhofer et al., 2022, p. 2). This means that nurses need to think about how their background, life experiences, and advantages might shape the way they see and treat others (McGough et al., 2022). By understanding, nurses can work toward a culturally safe, respectful, and equitable health care space for this population (McGough et al., 2022).
When working with Indigenous clients, it is important to explore their understanding and experience of the situation. Using a framework such as the Four Cs model allows nurses to gain insight into what the client considers to be the problem, the cause of the issue, how they are coping, and what concerns they may have (Stuart et al., 2012) (Table 1). This approach helps build a shared understanding and supports culturally safe communication (Beaulieu et al., 2025). This is especially important for Indigenous peoples because the health care system has historically been a place where they faced racism, stereotyping, and mistreatment, often resulting in mistrust and poorer health outcomes (O’Sullivan, 2013).
The Four Cs of Culture.
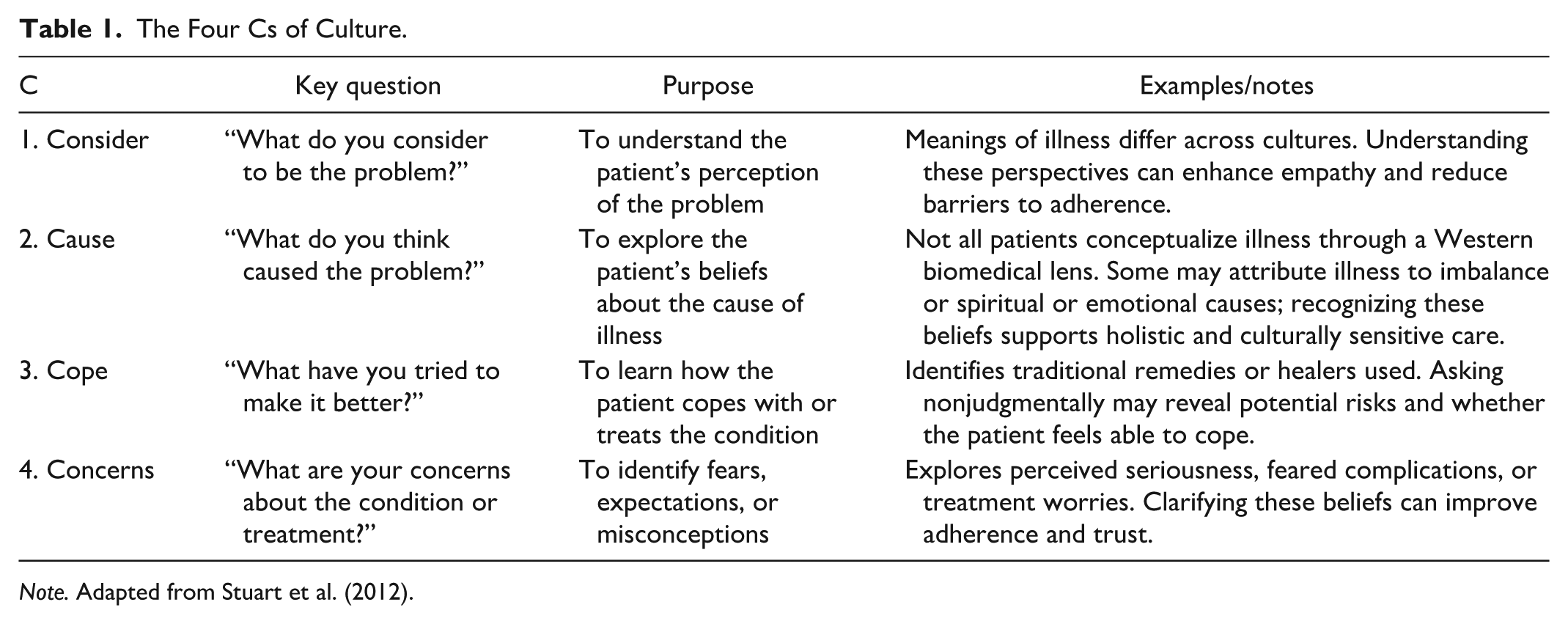
Note. Adapted from Stuart et al. (2012).
In addition, nurses can achieve culturally safe practice by demonstrating a commitment to building trust and engaging in activities that involve reciprocity or two-way learning between them and the Indigenous patient (McGough et al., 2022; Wilson et al., 2022). One way to achieve this is to incorporate Indigenous people’s “knowledge, beliefs, values, practices, medicines, and models of health and healing alongside those of Western medicine in delivering healthcare” (Wieman & Malhotra, 2023, p. 1) This is known as “two-eyed seeing,” where one view represents Indigenous knowledge, and the other represents Western knowledge. The idea is that by viewing health care through both perspectives, nurses can gain a deeper, more comprehensive understanding of how to care for Indigenous individuals (Wieman & Malhotra, 2023).
The “two-eyed seeing” model highlights the importance of integrating traditional Indigenous healing practices into health care. It includes activities such as harvesting, preparing, and using traditional medicine, along with talking circles. Talking circles may include storytelling, traditional songs, drumming, dancing, and ceremonies like smudging, sweat lodges, and cold-water baths, all of which foster spiritual, emotional, and communal healing. Land- and water-based practices such as fishing, hunting, harvesting, and eating traditional foods are also vital for well-being (Wieman & Malhotra, 2023).
Working with Indigenous patients means recognizing that effective care should align not only with clinical guidelines but also with what is personally and culturally important to the patient. Rather than imposing standardized care, the HCP collaborates with the patient to create goals that are both medically appropriate and culturally meaningful. For example, in diabetes management, instead of asking a patient to give up traditional foods entirely, the nurse might explore ways to prepare those foods in a healthier way or participate in community-based physical activities that align with their cultural norms. This approach ensures that care feels personal and attainable, and it helps build trust and engagement between the patient and the HCP (Murdoch-Flowers et al., 2019).
Incorporating these cultural practices into health care services and programs, and encouraging their use as part of self-care, has been shown to enhance health outcomes for Indigenous peoples by supporting holistic healing and strengthening cultural identity (Wieman & Malhotra, 2023). HCPs who understand and accept the “two
What This Paper Adds
This paper significantly contributes to nursing education and research by deepening the understanding of cultural safety within an Indigenous context. It highlights how colonialism, systemic racism, and historical trauma continue to shape Indigenous health outcomes, emphasizing the need for nurses to engage in critical reflection and advocate for social justice. By distinguishing cultural safety from cultural humility, the paper challenges nurses to address power imbalances and ensure care environments where Indigenous patients feel respected and safe. It also identifies important gaps in current practice, particularly the lack of effective tools to measure cultural safety based on Indigenous experiences rather than provider intentions. Furthermore, the paper positions nurses as key leaders in systemic change, encouraging the integration of Indigenous knowledge systems, such as the “two-eyed seeing” model, into clinical practice and health care structures. Through these insights, the paper advances nursing education and research by offering practical strategies to build trust, promote two-way learning, and hold systems accountable for delivering culturally safe care.
Conclusion
Indigenous peoples in Canada continue to face significant health disparities and receive lower-quality health care due to racism, negative stereotypes, and historical injustices. These ongoing challenges have led many Indigenous individuals to avoid seeking medical care. To help address these disparities, health care systems are increasingly adopting an approach to cultural safety. This concept focuses on creating health care environments that are respectful, inclusive, and empowering for Indigenous patients. Cultural safety requires HCPs to engage in cultural humility and critical self-reflection, examining their own biases and understanding how social and historical contexts, such as colonization and systemic racism, affect the health and well-being of Indigenous peoples. Providers must also be aware of the inherent power imbalances that exist in health care relationships, particularly between non-Indigenous providers and Indigenous patients. Evidence shows that cultural safety practices lead to better patient-provider relationships, increased access to health care services among Indigenous populations, and improved confidence in providing care among health care staff. To build cultural safety, institutions are encouraged to commit to trust-building, reciprocity, and two-way learning with Indigenous communities. Nurses, who make up the largest group in the health care workforce, are in a key position to lead the implementation of culturally safe practices. Their close relationships with patients allow them to play a crucial role in meeting the unique health needs of Indigenous peoples. Ultimately, the goal of cultural safety is for HCPs to develop the knowledge, skills, and attitudes necessary to deliver care that is not only clinically effective but also culturally respectful and safe for Indigenous individuals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.