
Abstract
First Nations people living with the human immunodeficiency virus (HIV) in Canada face a range of complex barriers during a time when infection rates are increasing. The Northern HIV Journey Mapping Project explored this issue from the perspectives of both First Nations people living with HIV and the health care service providers who support them. Drawing from an Indigenous-led, decolonizing methodology, this study adopted the philosophies of Two-Eyed Seeing and Ethical Research Space. A total of 18 First Nations people living with HIV and 11 health care providers from throughout the province of Manitoba participated in semi-structured interviews that explored the barriers and facilitators present at each of the six milestones of the HIV care cascade. Three interrelated themes emerged across all milestones and from both participant groups: (1) Intersectional stigmas operate throughout the entire HIV journey, both within the health care systems and in the lives of community members; (2) Privacy and confidentiality related to HIV status and other health care information is difficult to maintain in rural, remote, and northern care contexts; and (3) Knowledge gaps related to HIV and sexual health are common. Results were interpreted by both First Nations and non-First Nations team members, including the project Elder, showing that each theme reflects legacies of colonization. Recommendations include developing an Indigenous-led strategy that included peer-based education and support programs that address each theme simultaneously to improve the well-being of First Nations people living with HIV in Manitoba.
Introduction
Despite advances in the treatment of human immunodeficiency virus (HIV), First Nations persons (who along with the Inuit and Métis comprise Canada’s Indigenous peoples) with lived experience of the virus in the Canadian province of Manitoba remain vulnerable and disproportionately marginalized by social and structural factors that impact their overall wellness (Nguyen et al., 2020; Richmond & Cook, 2016; Wylie & McConkey, 2019). Not only does this call into question the efficacy of advancements toward eliminating HIV, but it also points to the broader issue of health inequities across non-majority sociocultural groups (Jackson & Huston, 2016).
The Northern HIV Journey Mapping Project was initiated in 2019 as a qualitative study grounded in First Nations and decolonizing methodologies, with the aim of understanding the journey of First Nation people living with HIV through the HIV care cascade (Figure 1), which comprised the typical steps from the initial HIV diagnosis to receiving treatment and achieving a suppressed viral load (L. McClarty, Blanchard et al., 2021; L. M. McClarty, Kasper, et al., 2021). The purpose of the study was to generate insight into ways to improve the overall well-being of First Nations people living with HIV through research grounded in decolonizing principles (Marshall & Bartlett, 2015), ensuring that the voices and experiences of First Nations people are centered in the research findings and subsequent recommendations. HIV Care Cascade.
Throughout the study, a number of data points, insights, and theoretical constructs emerged that reveal a pathway for the development of community-informed program and policy interventions. Initial published results from the study focused on the use of First Nations research methodologies (Larcombe et al., 2020), as well as the impact of COVID-19 on First Nations people living with HIV (Larcombe et al., 2023). In this paper, we return to the data to examine themes emerging from interviews with participants that appeared consistently across all milestones of the HIV care cascade, and that were interrelated and/or connected to each other in terms of their effect on living with HIV. Moreover, we chose to apply our decolonizing methodology in a new way by inviting the project Elder into the interpretation of findings to reflect both Two-Eyed Seeing and Ethical Research Space approaches in action. What follows are findings that illuminate a path forward for the development of policies and programs as interpreted by both Indigenous and Western members of our research team, contextualized by the teachings and wisdom of Dr. Albert McLeod, and the potential impact of study results on HIV policies and programs in Manitoba is discussed.
Background
HIV and First Nations Health in Manitoba
The province of Manitoba is situated in western Canada, with a total population of 1,342,153 (Government of Canada: Statistics Canada, 2022), 12.24% of whom self-identify as First Nations (Canada, 2021). Manitoba continues to experience increases in the incidence of HIV infection, with a significant rise of 130% between 2021 and 2023 resulting in the highest ever recorded incidence rate of 26.4 HIV diagnoses per 100,000 people (Rueda et al., 2025). Among all newly diagnosed in 2023, 85.1% of females and 68.6 of males self-identified as Indigenous (Manitoba HIV Program, 2024). These statistics reflect the trend of steady increases in new HIV diagnoses in the province since 2020, with a disproportionate number of infections affecting First Nations individuals.
HIV infection, like many other health conditions, reflects the health inequities faced by First Nations people and communities in Manitoba, driven by the social determinants of health (King et al., 2009; Marmot & Wilkinson, 2005; Reading & Wien, 2009). Poverty, racism, risk of incarceration, a lack of access to employment, and secure/stable housing are among key social determinants that affect their health (Kim, 2019). These social determinants are framed within the context of structural issues, rooted in policy driven by colonial agendas within the contemporary context that implicitly and explicitly govern aspects of First Nations peoples’ lives. First Nations people are at greater risk for acquiring HIV due to a range of structural determinants (Greenwood et al., 2018). Furthermore, despite advances in health care specific to HIV, there remains a great disparity between Indigenous and non-Indigenous Canadians (Public Health Agency of Canada, 2006; Keynan et al., 2023; L. McClarty, Blanchard, et al., 2021, L. M. McClarty, Kasper, et al., 2021).
The practice of academic scholars partnering with Indigenous communities to conduct research is growing within the Canadian context and serves as a tangible act of reconciliation in response to the harms caused by research on Indigenous people (Allen et al., 2020; Wilson, 2020). It is within Indigenous-driven research that opportunities for reclaiming culturally grounded solutions to colonial problems emerge (Larcombe et al., 2020; Marshall & Bartlett, 2015). The principle of shared responsibility and leadership is relevant to the field of HIV research to identify and understand HIV-related concerns through Indigenous cultural and worldview approaches (Flicker et al., 2015; Nowgesic, 2013; Peltier et al., 2020). Through an Indigenous lens, physical displacement resulting from land theft, dispossession and relocation of Indigenous communities, the breaking of treaties, forced attendance at residential schools, lack of access to traditional foods, medicine, and ceremony, and the effects of broken family ties are among a long list of factors contributing to cultural stress (Bartlett, 2003; De Leeuw, 2015; Richmond & Ross, 2009; Smylie, 2016). In turn, these histories are related to both the drivers of HIV infections and disparities in the quality of life outcomes for this population when compared to non-Indigenous Canadians.
Methodology
This overarching research project is situated within a long-term collaboration and partnership between University of Manitoba researchers and First Nations communities. First Nations research partners initially identified a gap in knowledge about the experiences of First Nations people undergoing HIV testing, getting linked to care, and living with HIV in northern Manitoba (Larcombe et al., 2019). In response to these concerns, the current study was launched in 2019 to address gaps in knowledge about the experiences of First Nations people in HIV diagnosis and care in northern Manitoba. The research team consisted of both Indigenous and non-Indigenous researchers, community members, students, people with lived experience of HIV, and health care providers engaged in sexual health programs and services. The first author of this work, who led the conceptualization, data analysis, and writing of this article, is a non-Indigenous person with no experience of living with HIV; however, they have engaged in sexual health service delivery and community-based research within the Manitoban and Canadian context for over 18 years.
Given the mix of Indigenous and non-Indigenous research team members, we actively engaged in reflexivity throughout the research process to situate and locate our perspectives and biases. Reflexive strategies included ongoing discussions within our team, with some guided by an Elder to engage critically with the power dynamics at play and to understand how our assumptions and social locations influence the research process (Hesse-Biber, 2011). Through the analysis process, decisions related to coding, categorizing, and theming were regularly attended to within our reflexive discussions. All results were shared with First Nations people with lived experience and our Elder prior to drafting this report, all of whom are listed as co-authors.
Decolonizing Research Through Ethical Space and Two-Eyed Seeing Approaches
The study commenced with a series of workshops for team members led by Two-Spirit First Nation Elder Dr. Albert McLeod, whose ancestry derives from Nisichawayasihk Cree Nation and the Métis communities of Cross Lake and Norway House in northern Manitoba. The sessions focused on First Nations research methodologies, including Two-Eyed Seeing (Hovey et al., 2017; Larcombe et al., 2020; Marshall & Bartlett, 2015). Two-Eyed Seeing incorporates data collection, analysis, and interpretation that invites both Western and Indigenous perspectives in the interpretation of results. Researchers and research participants, from different cultures and ways of knowing, meet within an “Ethical Space” (Ermine, 2007) which is defined as a research engagement, between those who may have differing ways of being and worldviews, that prioritizes respect, reciprocity, and responsibility. The outcome of this approach, rooted in the teachings of our Elder, was a rich, nuanced approach to qualitative inquiry and data analysis that aligned with decolonizing research principles, fostering a deeper understanding of First Nations people’s lived experiences and perspectives while challenging and disrupting colonial research paradigms.
Methods
Data were gathered by way of semi-structured interviews within two participant groups: First Nations people living with HIV and health care providers involved in HIV care throughout Manitoba. Inclusion criteria for First Nations people living with HIV included self-identification as a First Nation person, living in Manitoba, and being at least 18 years old. Health care providers were eligible if they had experience with First Nations people living with HIV in Manitoba, either with direct health care or through HIV programs that directly serve First Nations people living with HIV. Participants were recruited into the study by a variety of means (posters, word of mouth, and recruitment at local HIV program sites).
Interviews were conducted between July 2020 to February 2022 by two research associates with lived experience of HIV, one who identified as First Nations and another as Métis. The interviews were held remotely using Zoom during the initial phase of the study, due to COVID-19 restrictions, and in person after COVID-19 restrictions were lifted. Two unique semi-structured interview guides were developed with insight from the project Elder and the community research associates with lived HIV experience (guides are included as Supplemental material). Both guides asked questions related to each milestone along the HIV care cascade (see Figure 1); however, questions were tailored to each participant group. First Nations people living with HIV were invited to share about their personal experiences related to each milestone while health care service providers were asked to talk about both their reflections and the processes involved with supporting clients to progress successfully throughout the HIV cascade of care. Both guides supported interviews through a mix of open- and close-ended questions that aimed to characterize the overall HIV care cascade journey from two important perspectives, highlighting where participant experiences aligned with an expected or standardized process (e.g., during linkage to care) or where experiences diverged. All participants provided written and verbal informed consent. The study was approved by the University of Manitoba Research Ethics Board (HS231123). Participants received a $50 honorarium in recognition of their time.
Analysis of interview transcripts was conducted by the first author using MAXQDA, a computer-assisted data analysis software program (VERBI Software, 2024). Within the software, a combination of open, inductive coding was combined with closed, deductive coding to capture unanticipated insights alongside responses to specific questions from the interview guide. The coding process was reviewed with members of the research team to ensure consistency with the overall study and to discuss code definitions and categorizing processes. Overlapping codes were organized into a range of categories that best reflected the holistic experiences of participants, which were then organized into broad themes capturing quotes from both participant groups relating to each milestone of the HIV care cascade (see Star et al., 2025 for a detailed case study of the use of MAXQDA within this project).
The choice to integrate findings through presenting quotes and organizing themes from both participant groups reflects our intention to highlight where data converge into actionable findings that are relevant to both the client and provider’s perspectives. While there were areas of difference, these were few and far between; the majority of data points that reflected opposing views were due to the timepoints referred to by the participant (e.g., participants linking to care in the early 2000s vs. health care providers speaking to their current understanding of the linkage to care process), or differences in the ways the questions were interpreted. As such, the findings below reflect insights about the HIV care cascade that are mutually validated and thus more broadly applicable to the current context.
The results of this work, and all themes, were presented and discussed at a data interpretation workshop in December of 2023 to a group of 44 people that included First Nations and non-First Nations health policymakers, health care providers, researchers, and people with lived experience of HIV from both northern and southern Manitoba. We chose to host this event in lieu of member-checking for several reasons: (1) true member-checking proved very difficult given the transient and disparate nature of reaching participants and (2) due to the interruptions and challenges presented through data collection during COVID-19. While some participants from both groups were present in the workshop, we used our time together to confirm that the thematic categories reflected their experiences and remained true despite several years passing between initial data collection and the analysis process. The participants, including those living with HIV, also added insights into recommendations for change, further deepening our collective understanding of the data and increasing the credibility and trustworthiness of the results.
Results
Participants
There was a total of 29 people enrolled in this study. Eighteen First Nations people living with HIV were enrolled, five of whom identified as being from Northern Manitoba, with the remaining based in Winnipeg with one individual identifying as Métis with First Nations ancestry. Some participants currently in Winnipeg have experience living in the north and/or had migrated to Winnipeg from a rural or remote community. The study also enrolled a total of 11 First Nations and non-First Nations health care providers located throughout Manitoba, one of whom identified as Métis, from northern and southern urban, rural and remote hospital and clinic facilities and public health offices.
The ages of First Nations people living with HIV ranged between 25 and 59 years while the health care providers’ ages ranged between 30 and 60 years. The median length of time since receiving an HIV diagnosis was 16.5 years (minimum 2 years, maximum 34 years). Among all 29 participants, 18 participants living with HIV and four health care providers self-identified as First Nation (including Cree, Ojibwa, Dene, Oji-Cree, and other). The remaining seven health care providers identified as non-Indigenous. Participants reported their genders as man, woman, and/or non-binary, and sexual orientation as heterosexual, gay, lesbian, and two-spirit.
Theme 1: Intersectional Stigma
Intersectional stigmas related to HIV, other sexually transmitted and blood-borne infections (STBBIs), and general issues of sexuality were mentioned by both participant groups across each of the six milestones. Stories shared by participants highlighted that HIV stigma operates at multiple levels (in the community and in the health care system) and at every milestone along the HIV care cascade, resulting in a sustained and pronounced burden on their health and wellness. Stigma was also noted as the main reason for delaying or avoiding getting tested. When participants did eventually test positive for HIV, fear of experiencing stigma was a reason for delaying linking to care. The following quote reflects an example of the fear that participants felt when considering the reactions of friends, family members, and other community members if they found out: I was scared to go in [the community-based HIV clinic in Winnipeg] because I was scared people would see me walking into a place that was involved with people, with living with HIV or having AIDS or whatever, and they'd look down on me and everything and they'd know … (First Nation person living with HIV, P24)
When linked to care, participants living with HIV reported experiencing stigma within the health care system related to being First Nations and shared examples of health care providers judging and shaming First Nations people living with HIV. For example, participants highlighted stories of navigating challenging health care encounters where their HIV status led to being treated differently, which compounded with other experiences of stigma already present in their health care encounters: Yeah, so you know, I have to go to the hospital to get my gallbladder out. And they’re like, “you have any health concerns?” And then, you know, I have to disclose that I’m HIV [positive], right? And it’s like the shocked looks that I get! And I mean, this is at the hospital … (First Nation person living with HIV, P25)
Health care providers also shared their perspectives regarding the effect that the fear of stigma can have in their interactions with clients: … in my experiences, like some people have nobody and will not tell a single soul for fear of repercussions or stigma or … losing their job or … family. (Health care provider, P04)
First Nations people living with HIV in rural and remote regions reported that they often were required to travel to Winnipeg where specialized services are available. Arrangements for travel, either by car, bus, or plane are coordinated by health system managers, leading to expressed fear regarding potential breaches of confidentiality. Both participants living with HIV and their health care providers noted this as a key barrier and source of stress, particularly early in the care cascade at a challenging time of adjustment to their diagnosis.
Participants also reported experiences of stigma throughout the care cascade, affecting personal and intimate relationships, the seeking and retaining of employment, and emotional life, illustrated by the following quote: Well, everybody is scared to say I have HIV because, once they know you have HIV, that’s when you get treated different because when people knew I had, they started treating me different. It’s like they treat me like a plague so I withdrew from [others in my community]. I keep my distance. (First Nation person living with HIV, P36)
Health care providers reflected a very similar understanding of the connection between individual experiences of stigma and broader societal structures that support racism and discrimination toward First Nations people: I think just attitudes in general is of generalized stereotypes that many persons, care providers, have of First Nations people are barriers. So, [negative] stereotypes … are the kind of things that I believe that the health care providers in the north have around Indigenous peoples. (Health care provider, P04) It must be very difficult to ask if you have to advocate for yourself and ask for a test, which would take a lot of, I think, bravery, given the small community. (Health care provider, P07)
Participants living with HIV suggested that education about sexual health for youth that addresses myths, stereotypes, and teachings that promote healthy behaviors/practices is key to reducing stigma in their communities. Health care providers noted the need for methods to reduce the requirement for extensive travel, including increasing access to virtual options and in-person care in their home communities.
Theme 2: Privacy and Confidentiality Challenges and Their Impact on HIV Care
Nearly all participants in this study provided examples of how a lack of privacy and confidentiality, with ensuing experiences of stigma, affect the quality of life of First Nations people living with HIV. The expansive geography of northern Manitoba, where First Nations people reside in small remote communities, and the scarcity of human and technical resources in those communities, create challenges for confidential care. For example, the following quotes illustrate a heightened awareness of the need for confidentiality on the part of health care providers and the commensurate increase in vigilance on the part of community members when accessing health care appointments at HIV care sites: … I’ve seen lots of people be very, very afraid of anybody in their community finding out because it would spread like wildfire, and they would be ostracized. So, my general impression would be that there is not a whole lot of motivation to be tested for HIV because the repercussions of having that label in a small community would be catastrophic for some people. (Health care provider, P07) And, you know by virtue of the doctor, people know what kind of meeting you’re going to. (First Nation person living with HIV, P27)
Participants reported specific examples of challenging situations for First Nations people living with HIV, including with respect to arrangements for medical transport, either by plane or by car, to Winnipeg in groups that prevent privacy, as well as family members having access to medical records in their home communities: … you know, … the aunt and or the cousin or the second cousin is working at the nursing station. And you’re concerned about where this information will go, because definitely there’s been a number of cases where, you know, horrible [Personal Health Information Act Violations]. (Health care provider, P07)
The emotional effect of stress regarding confidentiality concerns is illustrated in the following statement: And if you could protect yourself and keep it very confidential, you know it would probably make things a lot easier for you. But if you lived in a community of 45 or 50 people and, you know, would you be able to? Probably not. And what would that mean for how much you cared about looking after yourself and wanting to live with HIV, being engaged [in care] and wanting to live with HIV? I think that would be the challenge. (Health care provider, P02) Well, back home, everybody knows everybody, and I have to be cautious about telling. Who do you trust? Who do you feel comfortable with? (First Nation person living with HIV, P036)
What is prominent in this thematic area is that health care providers were aware of the need for methods and strategies that protected the confidentiality, and ultimately privacy, of their clients’ personal lives. Without assurance of confidentiality, First Nations people living with HIV are demotivated to engage in care and to trust the health care system and those who work within it.
Theme 3: Bridging HIV Knowledge and Awareness Gaps
The third theme that emerged across all milestones of the HIV care cascade from both participant groups is the need for more HIV knowledge and awareness throughout First Nations communities and among staff in the health care services that support them. Health care providers demonstrated the dire consequence of a lack of general awareness of HIV among the communities they support: … Like, what if you lived in … [A small Indigenous community in Northern Manitoba] and everyone told me that, you know, you were positive, you’d get driven out of the community and you might as well commit suicide. (Health care provider, P06)
Conversely, participants living with HIV also expressed doubts about the skill level of health care providers in rural and remote communities: But the nurses up north, they didn’t know what to do, like, … they sent me down south to get healed for pneumonia. They didn’t have the pills maybe. I don’t know. Like, they didn’t know what to prescribe. They didn’t know what to do. (First Nation person living with HIV, P037)
Participants from both groups recognized the need for youth education in schools and in the community to address the gaps in awareness regarding how HIV is transmitted, how to prevent infection, and how to eradicate stigma. The following quote reflects a sentiment that emerged across both groups of study participants related to the need for more visibility and awareness: I think there should be more parades. Activism. Let them know it is OK. You should not have to live in the dark, under a rock. Because of these medicines [you can] live a normal life. (First Nation person living with HIV, P29)
Participants in both groups viewed the role of peers with lived experience as beneficial for providing education and offering one-on-one and group-based support for those who are newly diagnosed. The following quote illustrates the perspective of one person living with HIV that mirrored those of health care providers: I don’t know if they have this because I haven’t seen it yet, but I really wish there was a peer navigator [at the public health office]. That somebody that was diagnosed already [would be] there to support me. And another positive person that I could talk to because … there wasn’t a workshop where I can meet [others like me]. There wasn’t any workshops for me to go to. (First Nation person living with HIV, P21)
In this quote, the lived experience of a peer in care settings was identified as potentially offering a level of authenticity, humanity, and relatability to a newly diagnosed person with HIV, as well as reducing the power imbalances between health care providers and clients through the provision of services developed by and for First Nations people living with HIV.
Thematic Interrelatedness
The three themes that emerged across our data (stigma, confidentiality, and knowledge/awareness gaps) are closely interrelated (Figure 2). The following two quotes illustrate how their interconnection creates complex challenges for both participant groups: I think we’re back to the stigma and fear and privacy issues there. We have a large number of people that struggle with taking their medications because they have to keep them hidden away. (Health care provider, P07) I was dating him and somebody told him I was HIV positive and the family immediately had stigma against me and they were telling him, don’t date her, you’re going to catch HIV and die because they had stigma to the same stigma I had, because I know where they’re coming from, because that’s the exact same stigma I had when I was a kid. (First Nation person living with HIV, P27) Thematic Interrelatedness.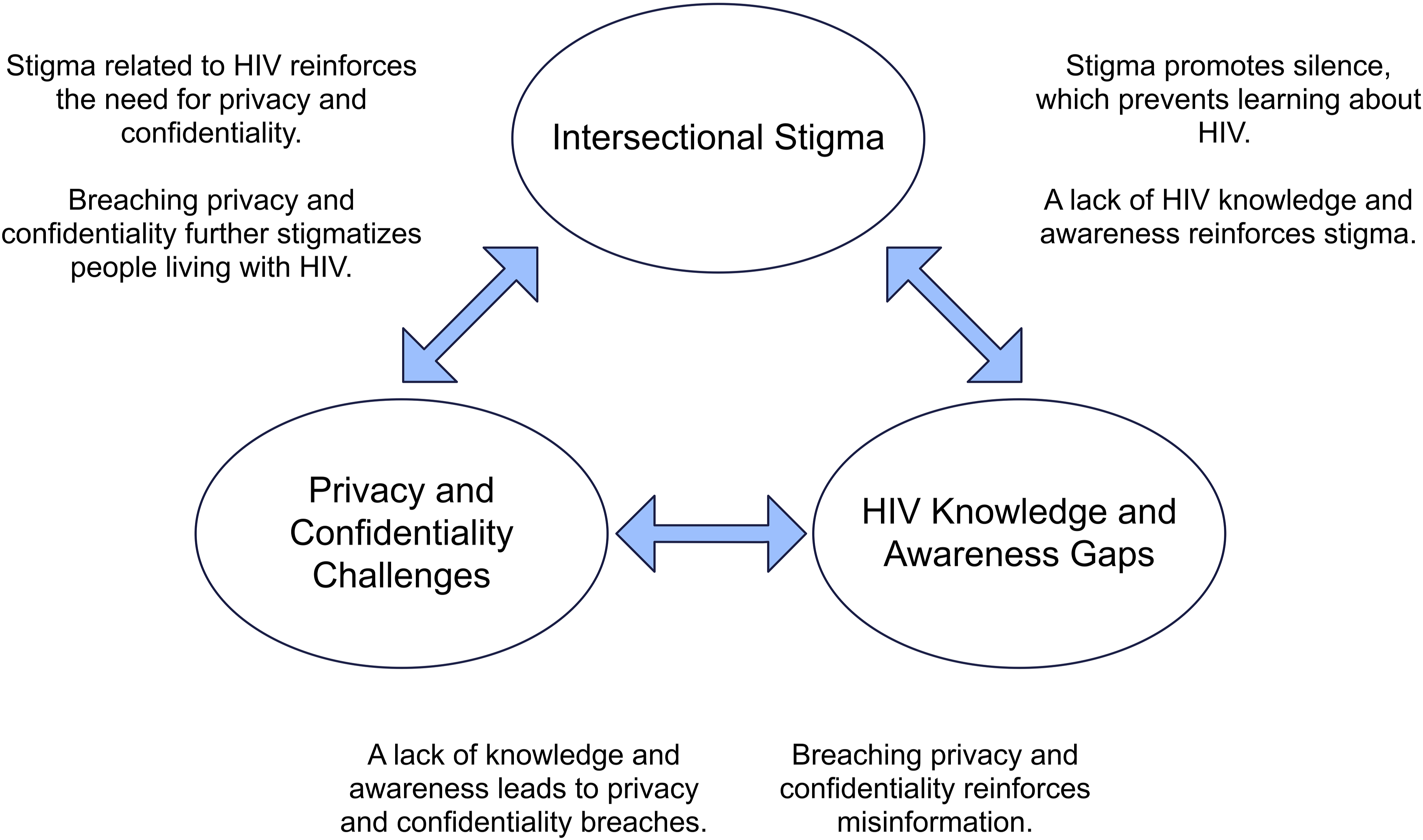
The responses provided by both participant groups shed light on how stigma was driven, in part, by a lack of awareness and understanding of HIV in the community, leading to stereotypes and myths that impacted peoples’ behavior. Furthermore, responses indicated that a lack of awareness existed regarding the importance of patient confidentiality related to a person’s HIV status, specifically within smaller communities, leading to privacy breaches with a range of negative impacts.
All three themes interact to make accessing health care in a small remote center challenging for First Nations people living with HIV: So, again, like, even nursing station care, there’s, you know. Might be your Auntie, your cousins working, you know. And depending on how sensitive you perceive the tests that you want to be in, that the stigma attached to what you’re getting health care for, you may or may not want that. (Health care provider, P02)
A lack of confidentiality in health care spaces is further challenged by the stigma associated with living with HIV, which, according to the participant quoted below, could be addressed by increasing awareness and knowledge about HIV: I think it just maybe a lack of education of knowing that, like, HIV is not a death sentence. It doesn’t make you dirty. It doesn’t make you that …. like that’s kind of like the statements that we get ... As people who end up getting diagnosed with HIV. To feel like they lose their friends. So, all of that before the test even happens comes up in conversation. And if it’s positive. What’s the community going to think? What are the family going to think? What are their friends going to think? (Health care provider, P09)
Discussion
As it relates to the purpose of improving the overall wellness of First Nations people living with HIV, results from this study confirm and reiterate other findings that demonstrate how stigma, driven in part by a lack of knowledge or awareness, increases the burden of negative outcomes associated with HIV for groups marginalized based on their social and cultural identities (Deering et al., 2021; Donnelly et al., 2016; Katz et al., 2013; Young & Bendavid, 2010). We also found that health care providers recognized room for improvement with respect to safeguarding confidentiality and privacy related to HIV status, which is complicated by the role that geography plays in reducing choice in health care services available to First Nations people living with HIV in northern Manitoba. Not only are there limited human resources to draw from to staff remote clinics, the vast distance between health care sites and clinics poses a barrier for those who would otherwise choose to travel to a site away from their home community to protect their privacy. The issue of privacy in HIV care has been explored, including findings noting that a lack of privacy is a key barrier to retention within the HIV care cascade (Marellapudi et al., 2022).
With respect to improving the overall journey through the HIV care cascade, participants recommended increasing access to education and resources that include people living with HIV as peers. This would address both the drivers of HIV-related stigma and support ethical practice among health care providers related to protecting privacy and confidentiality in health care settings. Stigma-reducing education de-mystifies HIV by combatting stereotypes and misinformation while also increasing empathy and awareness of the impacts of the virus. Increasing access to such education for both community members and health care providers would require a greater investment from both the health and education systems, both of which would need to act in concert to dismantle the structural barriers to health and health equity faced by First Nations people in Canada. The call for greater investment in peer-based education and support models is not new; other published studies see them as a direct intervention to the power dynamics that reinforce negative experiences of HIV care, broadly speaking (He et al., 2020). Given the emphasis here on First Nations experiences, we echo our colleagues who have called for such investments to be Indigenous-led and to explicitly link effort to achieving systemic change (Hillier et al., 2021).
Co-Interpretation and Contextualization of Findings With Elder Dr. Albert McLeod
First Nations research calls for the placement and interpretation of findings and observations within the context and workings of a spiritual, emotional, mental, and physically interconnected world (Wilson, 2020). To this end, tobacco was ceremonially offered to Dr. McLeod and in an ethical space the first author sought to engage in a reflective iterative dialogue of understanding and respect about the results noted above. The discussion and teachings took place in one meeting prior to drafting these results, and the entirety of this work was shared back with the Elder to ensure accuracy and clarity and to strengthen key points. The outcome of this discussion is presented below.
Placing participants’ responses within larger historical and current societal and political structures, Dr. McLeod reflected that infectious diseases are tools of colonialism that governments and other systems have used to advance assimilationist agendas, which privilege a certain segment of society. Recalling past experiences with tuberculosis where Indigenous people in Canada received segregated health care (Lux, 2016), and more recently with the COVID-19 pandemic, he shared the following thoughts and reflections: The HIV/AIDS stigma is an issue of systems supported by the federal, provincial, municipal, and Indigenous governments. They all quickly dealt with the COVID-19 pandemic, however they have avoided championing interventions related to HIV transmission, testing, treatment, and support for the past 20 years.
Dr. McLeod highlighted long-held societal attitudes and beliefs that stigmatize groups disproportionately affected by certain infectious diseases and which justify segregationist ideologies that separate Indigenous people and “their problems” from non-Indigenous communities. These separations are reinforced by racism, which was institutionalized in the reserve system, whereby First Nations people in Canada (and other colonized areas of the globe) were sequestered on small, dispersed tracts of land, as well as doctrines and ideologies espoused by the Christian church, which denigrated Indigenous teachings and promoted sin-based attitudes toward sexuality. The result shrouded Indigenous sexualities in a cloak of repression, shame, and silence that contributed to the colonial project of cultural genocide. As such, disproportionate inequities between Indigenous and non-Indigenous people living with HIV are a product of the continued legacy of colonization, requiring broad and systems-based solutions that may take generations to undo.
With respect to a way forward, Dr. McLeod pointed out that in his opinion, the provincial and federal governments are responsible for addressing the public health of the population in Manitoba yet have not renewed or developed a strategic framework for addressing the increasing burden of HIV and other STBBIs. In his words, “no strategy is a strategy,” leading to maintaining the status quo at the expense of communities marginalized by factors outside of their immediate control. In this situation, he noted that the sense of powerlessness among Indigenous communities is reinforced by complicated governance systems that obfuscate the locus of power in hierarchical systems that contravene collectivist approaches to community leadership, which were common prior to colonial contact. The outcome of this, when combined with the legacy of the residential school system and generations of harm, is a population made vulnerable by the very systems designed to keep them safe.
While the data in this research point to a potential solution that addresses each of the three themes simultaneously to interrupt their mutually reinforcing effect on each other, Dr. McLeod reflected that this occurs within the context of the colonial nation-state. Without a strategic approach led by Indigenous knowledge and cultures, any public health intervention risks repeating the failures of the past and failing to adequately improve the lives of First Nations people living with HIV.
Limitations
This research encountered a number of limitations throughout the process that are worth noting here. First, the onset of COVID-19 at the start of recruitment posed significant barriers to facilitating semi-structured interviews with participants in northern, remote, and rural First Nation communities. Internet stability, timing, and public space shutdowns led to the need to develop creative solutions to reaching First Nations people living with HIV. We recognize that this led to a lower number of participants than anticipated. However, the richness of data and consistency in findings across both participant groups alleviate our concerns with the relevance of these results. Second, the study results pertain to the specific First Nations and health care providers from whom recruitment occurred in Manitoba.
Conclusion
Using decolonizing research methods, this Canadian qualitative study of interviews with First Nations people living with HIV and HIV health care providers identified three dominant interrelated themes throughout the stages of the health care cascade: HIV Stigma, HIV Knowledge and Awareness, and Confidentiality. The knowledge shared within the Ethical Space of this encounter, and through both Western and Indigenous ways of knowing, reveals a nuanced and contextualized path forward. The recommendation that emerges from this research is for public health systems to engage First Nations people who have lived experience with HIV in developing a strategy that addresses HIV stigma and awareness, as well as the need for confidentiality in health care spaces, in ways that actively resist the effects of colonial systems. This strategy requires creating ethical spaces that support Two-Eyed Seeing to move us forward together in pursuit of better health outcomes for all. Elder Dr. Albert McLeod aided in situating these findings within the broader historical and current context of colonization, and cultural genocide. The results support previously voiced recommendations (Hillier et al., 2021; Pyett et al., 2009) that public health systems engage First Nations people with lived experience in developing solutions that address HIV stigma, awareness, and confidentiality simultaneously to promote a sustained impact across all domains. This must be done within an Indigenous-led strategic framework that actively resists the effects of prolonged colonial state violence.
Supplemental Material
Supplemental Material - First Nations People Living With HIV: Results From a Qualitative Study Through a Two-Eyed Seeing Approach
Supplemental Material for First Nations People Living With HIV: Results From a Qualitative Study Through a Two-Eyed Seeing Approach by Jared Star, Albert McLeod, Pamela Orr, Laurie Ringaert, Gayle Restall, Elizabeth Hydesmith, Ann Favel, Melissa Morris, Michael Payne, Rusty Souleymanov, Yoav Keynan, Kelly MacDonald, Matthew Singer, and Linda Larcombe in Qualitative Health Research
Footnotes
Acknowledgments
We gratefully thank the study participants for sharing their insights and First Nations members of the research team with lived experience of HIV for guiding this work.
Author Contributions
Jared Star: conceptualization, data curation, formal analysis, methodology, validation, visualization, writing—original draft, and writing—review and editing. Albert McLeod: conceptualization, formal analysis, funding acquisition, investigation, methodology, validation, writing—original draft, and writing—review and editing. Pamela Orr: conceptualization, funding acquisition, investigation, methodology, writing—original draft, and writing—review and editing. Laurie Ringaert: conceptualization, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualization, and writing—review and editing. Gayle Restall: funding acquisition, investigation, methodology, project administration, supervision, validation, visualization, and writing—review and editing. Elizabeth Hydesmith: investigation, methodology, supervision, and validation. Ann Favel: formal analysis, investigation, and validation. Melissa Morris: formal analysis, investigation, and validation. Michael Payne: funding acquisition and project administration. Rusty Souleymanov: methodology and resources. Yoav Keynan: funding acquisition and methodology. Kelly MacDonald: funding acquisition and investigation. Matthew Singer: methodology, project administration, supervision, and validation. Linda Larcombe: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualization, writing—original draft, and writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institute for Health Research (CIHR)—Operating Grant Number CBA-164022.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.