
Abstract
Introduction:
As healthcare systems become diverse, tensions between Islamic modesty values and nursing guidelines remain underexplored. Requirements related to dress codes, cross-gender interaction, and physical contact may conflict with Islamic principles, while clear institutional guidance is often lacking.
Methods:
A scoping review was conducted to map empirical and nonempirical literature examining conflicts between Islamic modesty and clinical nursing practice. Descriptive and content analysis were used to identify areas of conflict, challenges, navigational responses, and proposed solutions.
Results:
Recurring conflicts involved professional dress requirements, cross-gender care, gender preference, physical contact, and limited gender-sensitive environments. Without clear guidance, Muslim healthcare providers and students relied on individual coping strategies rather than consistent organizational support.
Discussion:
Addressing these conflicts requires culturally responsive policies, flexible practice arrangements, and religious sensitivity training to support inclusive and ethically sustainable care across diverse healthcare settings.
Introduction
Al-ḥayā’ (modesty) is a core Islamic principle, embedded in the Qur’an and Hadith as both a moral and ethical guide. It promotes self-discipline, discourages undesirable behavior, and represents a spiritual and religious commitment rather than mere social discomfort (Sawai et al., 2020). Modesty applies to both men and women, though expressed differently across genders (Islam, 2023).
In health care, modesty shapes attire, interpersonal interactions, and workplace norms. Muslim nurses often cover their necks, forearms, and hair as part of religious practice, sometimes described as personal choice but grounded in theological obligation. These practices frequently clash with institutional dress codes, such as the “bare below the elbows” (BBE) rule designed for infection control (Alqufly et al., 2019; Saidun et al., 2018). Efforts to reconcile professional standards with religious requirements are increasing (Momeni & Asghari, 2020), particularly as attire also influences perceptions of professionalism and competence (Pawłowski et al., 2019). However, institutional regulations that fail to accommodate religious dress continue to create challenges (Momeni & Asghari, 2020; Saidun, 2020).
Modesty also extends to gender interactions. Muslim patients often prefer same-gender providers due to religious and cultural considerations, although shortages of male or female staff make this difficult (Odeh Yosef, 2008). Similarly, Muslim professionals may experience conflict when staff shortages require cross-gender care, placing professional duties in tension with religious principles (Kareem & Adeogun, 2020).
In conservative Islamic societies such as Saudi Arabia, gender segregation strongly shapes health care by influencing nurse recruitment, retention, and workplace dynamics (Miller-Rosser et al., 2006). Cultural and religious expectations often limit cross-gender care, creating challenges for both providers and patients (Cheraghi et al., 2019). Muslim male professionals in non-Muslim contexts also face difficulties, as Islamic law permits mixed-gender care only when medically necessary (Wojda, 2021). These examples demonstrate how modesty norms directly affect clinical practice and expose the tension between Islamic ethics and institutional healthcare standards.
Reconciling these religious values with professional responsibilities remains a complex challenge, particularly in multicultural and transnational contexts. Although Islamic modesty carries significant ethical and cultural importance for many patients and providers, its interaction with healthcare standards is rarely examined in depth. Current research is limited, conceptually fragmented, and often avoids addressing these value-based conflicts directly, both in Muslim-majority systems and in Western contexts, where Muslim minorities face additional complexities (Malik et al., 2019; Yaseen et al., 2021).
A preliminary review of the literature confirmed the absence of any systematic or scoping reviews dedicated to this issue. This gap underscored the need for a structured synthesis of available evidence to examine how modesty-related concerns have been described, categorized, and conceptualized across healthcare contexts. In response, a scoping review was selected as the most suitable methodological approach. Commonly used to explore conceptually diffuse and inconsistently defined topics, this method enables a comprehensive mapping of the literature by clarifying thematic patterns, identifying inconsistencies, and revealing gaps, rather than producing new theory.
Accordingly, this review aims to systematically examine how Islamic modesty, as a religiously grounded value, is represented within healthcare literature, to resolve key conceptual ambiguities, and to identify overlooked areas of inquiry. The resulting synthesis provides a foundation for developing culturally responsive clinical guidelines and policies that more effectively balance religious commitments with professional standards.
Specifically, this review seeks to clarify how Islamic modesty, understood as a religious value derived from Islamic teachings, is defined and expressed in healthcare settings; to examine its interaction with clinical guidelines; to identify points of conflict; to explore the resulting challenges, navigation strategies, and proposed or existing solutions; and to highlight gaps in the literature to guide future research and policy development.
Method
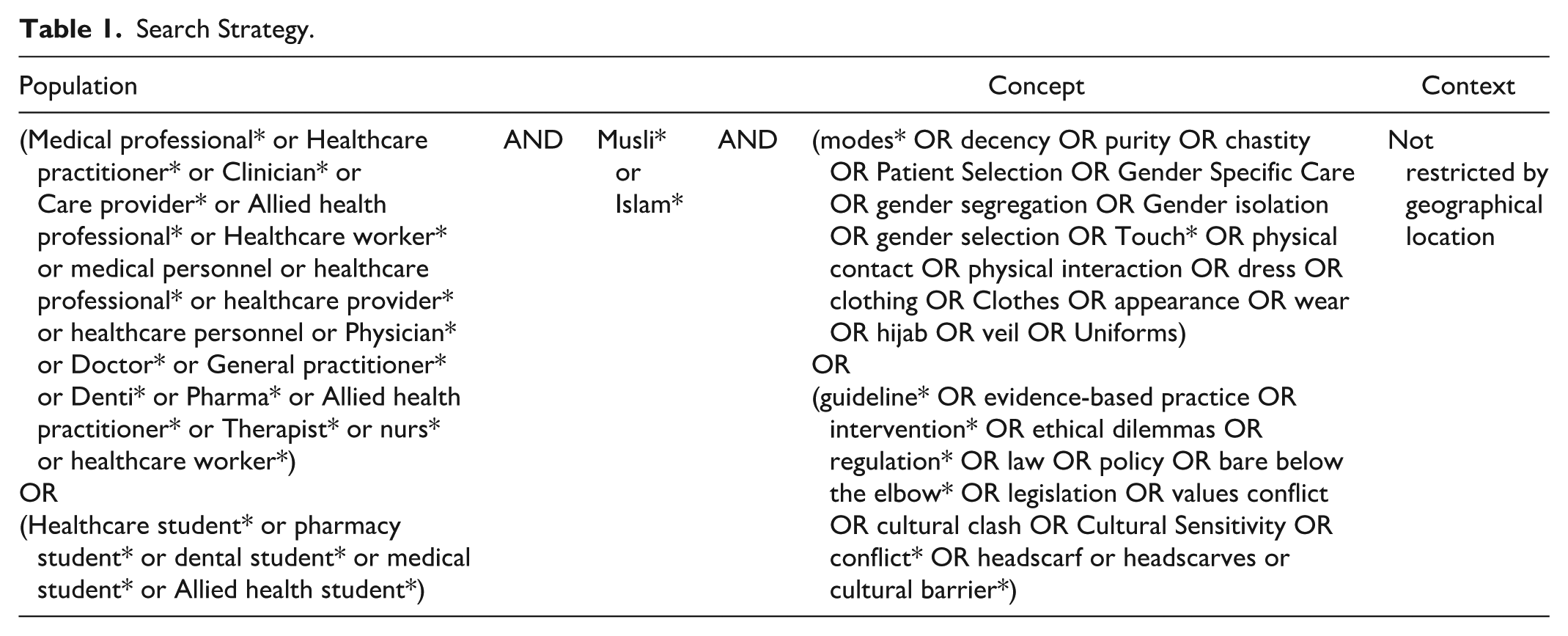
This review followed the JBI guidelines and the PRISMA-ScR framework (Peters et al., 2020) to ensure rigor and transparency. The PRISMA-ScR checklist (Tricco et al., 2018) guided the methodology and reporting. The PCC framework (Population, Concept, Context) was used to define the research question and inclusion criteria (see Table 1).
Search Strategy.
Eligibility Criteria
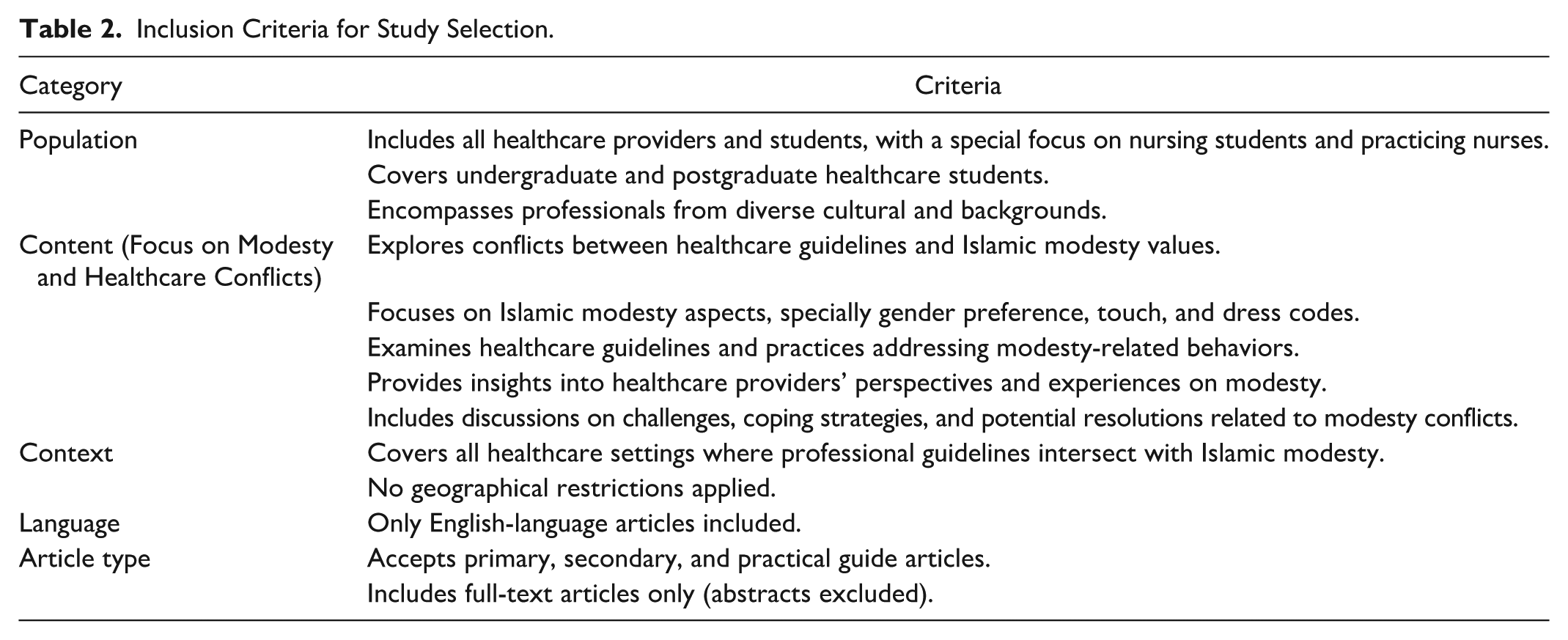
This review focused on studies involving healthcare providers affected by nursing guidelines related to Islamic modesty—specifically regarding touch, dress codes, gender preferences, value conflicts, and coping strategies. Only English-language studies were included. Detailed inclusion and exclusion criteria are provided in Table 2.
Inclusion Criteria for Study Selection.
Information Sources
Databases searched included Medline, CINAHL, PsycINFO, Scopus, and Embase. Gray literature was identified through targeted searches as outlined in Online Appendix 2. Citation tracking was also used to identify additional relevant sources.
Search Strategy
A three-step search strategy was used, in accordance with JBI methodology (Peters et al., 2020). The strategy was refined with input from an academic librarian, following recommendations by McGowan et al. (2016). To ensure transparency and reproducibility, Online Appendix 3 presents the full search strategy, including the search conducted in the CINAHL database.
Selection Process
All sources were imported into Zotero and screened using Covidence software through title, abstract, and full-text levels. A third reviewer was consulted to resolve disagreements during screening.
Types of Sources
Included sources were qualitative studies, literature reviews, practical guides, and quantitative studies addressing healthcare professional (HCP) experiences. Both peer-reviewed and gray literature (e.g., reports, policies, and dissertations) were considered.
Appraisal of Sources
Consistent with scoping review methodology (Munn et al., 2018), no formal quality appraisal of sources was conducted.
Data Extraction
The JBI data extraction template (Peters et al., 2020) was adapted to capture essential study characteristics, including citation details, population, concept, context, and key findings, as summarized in Table 3. One reviewer extracted data, while two independently verified consistency. Discrepancies were resolved through discussion and consensus to ensure transparency and accuracy.
Data Extraction Table.

Collating, Summarizing, and Reporting the Results
The results were reported following the PRISMA-ScR framework (Online Appendix 1) and presented through graphs, tables, and descriptive summaries to address the review questions. In line with JBI guidelines, a descriptive content analysis was conducted, applying basic data coding to summarize key findings without thematic synthesis (Peters et al., 2020). Unlike systematic reviews, which use in-depth thematic analysis, this approach provided a structured yet broad overview. Data were categorized by publication count, study type, Islamic modesty principles, nursing guidelines, touch, gender preference, and dress code.
Ethical Considerations
This scoping review used previously published literature and did not involve human participants or personal data; therefore, formal ethical approval was not required. Ethical clearance for the overall project was obtained from the Research Ethics Committee at Queen’s University Belfast.
Results
Search Results
A systematic search of five databases (CINAHL, Medline, Embase, PsycINFO, and Scopus) yielded 4,942 records; 1,980 duplicates and 2,086 titles/abstracts were excluded. Of 242 full texts screened, 204 were removed for irrelevance, duplication, unavailability, or language, leaving 38 articles for inclusion. Gray literature added two guideline-based websites. The selection process is shown in the PRISMA diagram (Figure 1).
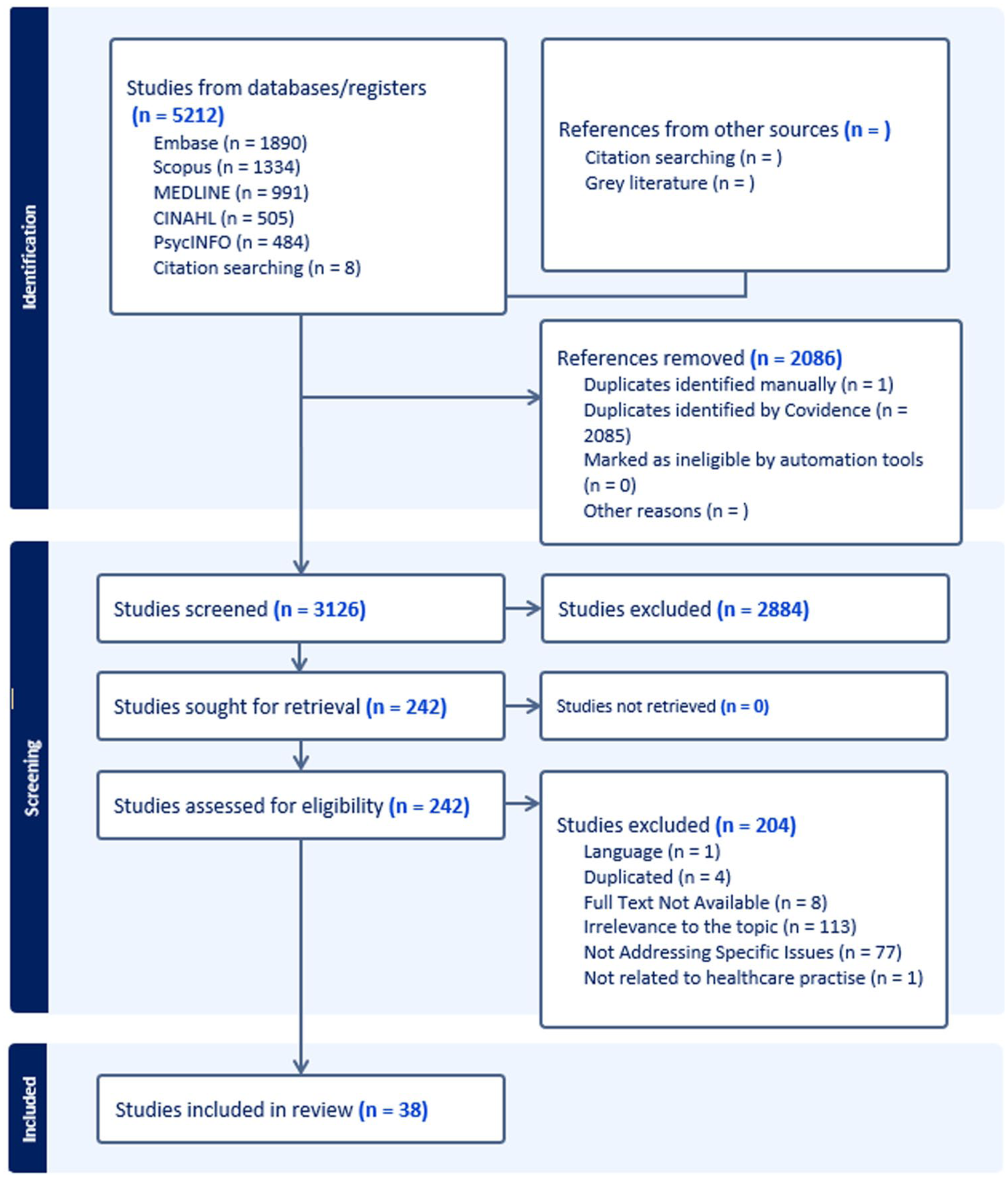
PRISMA-ScR Flow Diagram.
Studies’ Characteristics
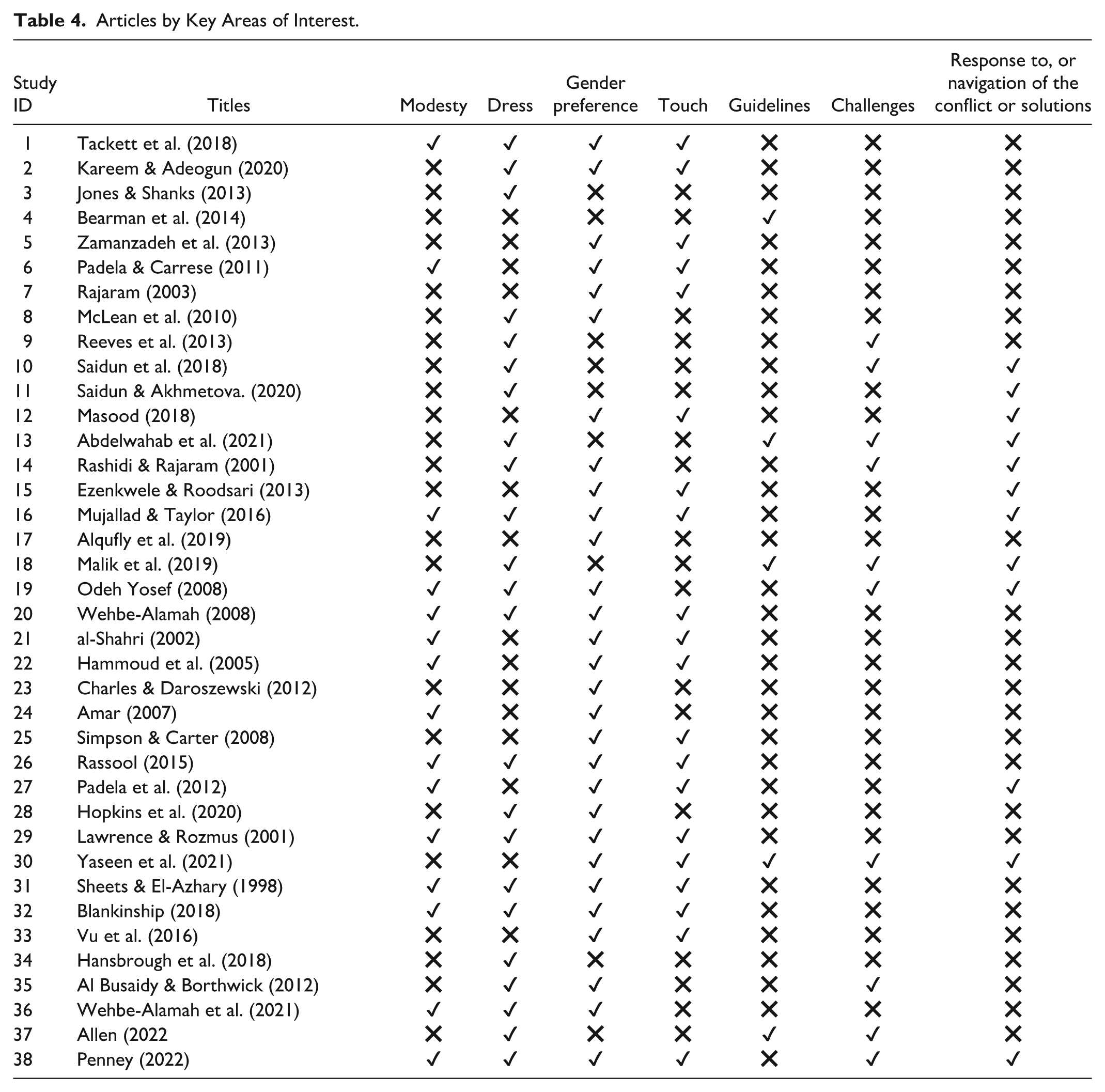
This review includes 38 studies published between 1998 and 2023, most after 2014. Geographically, 12 were from the United States (Muslim patients and cultural competence), six from the Middle East (regional challenges), four from the United Kingdom (policy and integration), and others from Pakistan, Nigeria, Malaysia, plus 12 global studies. Methodologies comprised qualitative (n = 11), reviews (n = 17), quantitative (n = 5), theoretical (n = 2), and policy/guideline papers (n = 3). Although 17 were primary studies, most addressed patients rather than healthcare providers, and modesty and conflict were often examined separately. Using descriptive content analysis, findings were organized into six domains: modesty, dress, gender preference, touch-related challenges, navigation strategies, and healthcare guidelines (see Table 4).
Articles by Key Areas of Interest.
Themes
Modesty-related expressions were classified under the main theme of modesty, with two subthemes: dress-related and gender interaction, reflecting appearance and interpersonal conduct. Developed iteratively through descriptive content analysis (Elo & Kyngäs, 2008) and refined with expert consultation, this framework resolves inconsistencies in terms such as hijab, touch, gaze, and gender preference, ensuring conceptual clarity and clinical relevance.
Theme 1: Modesty
Modesty is a core Islamic principle grounded in the Qur’an and Hadith, shaping dress, behavior, and social interactions as a religious obligation that reinforces faith and identity (Amar, 2007; Mujallad & Taylor, 2016; Padela & Del Pozo, 2011; Tackett et al., 2018). Some scholars, however, view modesty as culturally constructed, tied to gender roles, family honor, and social expectations, with HCPs at times adopting modest dress more for social or professional reasons than religious ones (al-Shahri, 2002; Penney, 2022). Wehbe-Alamah et al. (2021) argue that modesty lies at the intersection of religion and culture, shaping conduct in both personal and professional settings.
Despite its centrality, the literature reveals ambiguity in how modesty is defined, with no consensus on its forms or expressions. Studies variously frame it through dress, gender preference, physical touch, and disclosure of sensitive information. Tackett et al. (2018), for example, identified four dimensions relevant to health care—physical appearance, touch, sensitive disclosure, and provider gender preference—while emphasizing that cultural and religious factors shape how modesty is expressed and negotiated in clinical contexts.
Lawrence and Rozmus (2001), al-Shahri (2002), and Blankinship (2018) emphasize dress, gender preference, and physical touch as central elements of modesty, while Wehbe-Alamah et al. (2021) similarly identify these aspects. Padela and Del Pozo (2011) also stress modesty as a principle in cross-gender interactions, expressed through dress codes, seclusion, and physical contact.
By contrast, some scholars view dress and gender preference as distinct from modesty, framing them as expressions of religious identity (Odeh Yosef, 2008; Penney, 2022). Penney (2022) treats them as markers of identity, while Odeh Yosef (2008) highlights their cultural and religious significance.
Others expand modesty to include behaviors such as avoiding eye contact, limiting cross-gender interactions, and involving male relatives in communication with providers of the opposite gender, as a way to reduce seclusion and uphold religious values (Mujallad & Taylor, 2016; Saherwala et al., 2021). These practices reflect broader aspects of modesty rather than a distinct category.
Subtheme 1: Dress Code
Islamic teachings emphasize modesty through loose, nontransparent clothing covering the body except for the face and hands, yet styles vary across regions. Women may wear the jilbab in Jordan and Syria, the abaya or chador in Saudi Arabia and Iran, or the shalwar kameez in Pakistan (Mujallad & Taylor, 2016; Wehbe-Alamah, 2008). In West Africa, colorful garments and turbans are common, while in Southeast Asia, tunics with headscarves predominate (Mujallad & Taylor, 2016). In Western countries, Muslim women’s practices range from Western fashion to traditional modest dress (Lawrence & Rozmus, 2001; Sheets & El-Azhary, 1998). Men are required to cover from navel to knee, with attire also reflecting culture, such as the thobe and ghutra in Saudi Arabia (Mujallad & Taylor, 2016). These variations illustrate how cultural, legal, and personal factors shape the application of Islamic dress codes.
In health care, modesty requirements often conflict with institutional policies, particularly infection-control measures. The “bare below the elbows” (BBE) policy, mandating uncovered forearms, contradicts Islamic guidelines for women. Jones and Shanks (2013), in their analysis of 105 online commentaries, highlighted this conflict, while Malik et al. (2019), in a U.K. survey of 84 Muslim female professionals, identified BBE as a significant challenge. Our review found no studies culturing sleeves; BBE is presented here as a widely cited source of modesty-related conflict rather than as microbiological evidence.
A second area of conflict arises in sterile environments, such as operating theaters, where modesty-related dress (e.g., head coverings and long sleeves) is restricted by infection-control rules requiring bare forearms and uncovered heads outside sterile attire. Abdelwahab et al. (2021) at the Mayo Clinic provided guidance on accommodating religious staff during surgical scrubbing, while Saidun et al. (2018) proposed modesty-sensitive dress guidelines, and Allen (2022) also noted tensions between modesty and surgical attire.
A third challenge relates to security and identification, particularly for women wearing the niqab, who must reconcile modesty with workplace visibility (Abdelwahab et al., 2021; Saidun et al., 2018). Corporate image policies add further pressure, with some institutions encouraging fitted or short uniforms to appear approachable, creating direct conflicts with Islamic modesty standards (Saidun et al., 2018).
Such policies often leave Muslim staff feeling excluded or forced to compromise religious practice, especially when asked to alter head or forearm coverings. This can lead to experiences of discrimination, reduced career opportunities, and reluctance to pursue roles in surgery (Kareem & Adeogun, 2020; Malik et al., 2019; McLean et al., 2010; Penney, 2022; Reeves et al., 2013). The absence of consistent guidance exacerbates these tensions, fostering isolation and harming the mental well-being of providers who feel their beliefs are not respected (Jones & Shanks, 2013; Malik et al., 2019).
To manage dress code conflicts, Muslim healthcare staff and institutions have adopted various strategies. Some staff use disposable sleeves or bring their own clean headscarves to balance modesty with safety (Abdelwahab et al., 2021; Jones & Shanks, 2013). Organizations have introduced accommodations such as long-sleeved gowns in nonsterile areas and approved head coverings, while layered uniforms and surgical caps over hijabs are also practical solutions (Hopkins et al., 2020; Malik et al., 2019). Open communication between staff and employers has been effective in creating collaborative approaches that maintain sterility while respecting modest dress (Malik et al., 2019).
Despite these efforts, no clear national guidelines exist regarding Muslim dress codes in health care. In many Muslim-majority countries, policies remain absent or inaccessible, leaving institutions to create their own rules and causing inconsistency (Saidun et al., 2018). Malaysia has attempted to propose guidelines, but nationwide regulations are still lacking (Saidun et al., 2018).
In Muslim-minority contexts, policies are equally fragmented. In the United Kingdom, NHS Trusts provide some guidance on hijabs and forearm coverage, yet approaches vary. Some Trusts allow hijabs under specific conditions—plain, secure, washable at 60°C, and paired with surgical caps—and permit disposable sleeves for forearms, while others prohibit these practices (Jones & Shanks, 2013; Malik et al., 2019; NHS England and NHS Improvement, 2020). This inconsistency leaves Muslim staff facing differing expectations across workplaces. In the United States, the Equal Employment Opportunity Commission (EEOC) requires accommodation of religious dress unless it poses safety risks (EEOC, 2023). However, no standardized guidelines exist on how attire such as the hijab aligns with infection control and bare-below-the-elbows (BBE) policies, leaving practices unclear.
Subtheme 2: Intergender Interaction
Across the 38 articles reviewed, the literature on cross-gender interactions between Muslim HCPs and patients highlights several key concepts that shape gender dynamics in healthcare settings. These include gender preferences (Al Busaidy & Borthwick, 2012; Ezenkwele & Roodsari, 2013; Kareem & Adeogun, 2020; Sheets & El-Azhary, 1998; Simpson & Carter, 2008), touch or physical contact (al-Shahri, 2002; Blankinship, 2018; Charles & Daroszewski, 2011; Mujallad & Taylor, 2016; Padela et al., 2012; Rajaram & Rashidi, 2003; Simpson & Carter, 2008; Yaseen et al., 2021), gender-concordant care (al-Shahri, 2002; Alqufly et al., 2019; Ezenkwele & Roodsari, 2013; Hammoud et al., 2005; Hopkins et al., 2020; Kareem & Adeogun, 2020; Lawrence & Rozmus, 2001; Mujallad & Taylor, 2016; Odeh Yosef, 2008; Padela & Del Pozo, 2011; Padela et al., 2012; Penney, 2022; Rashidi & Rajaram, 2001; Rassool, 2015; Tackett et al., 2018; Vu et al., 2016; Wehbe-Alamah, 2008; Wehbe-Alamah et al., 2021), khalwa, or seclusion (Padela & Del Pozo, 2011; Wehbe-Alamah et al., 2021), and gender segregation or separation (al-Shahri, 2002; Amar, 2007; Lawrence & Rozmus, 2001; Masood, 2019; Mujallad & Taylor, 2016; Vu et al., 2016). Together, these concepts illustrate how Islamic principles of modesty influence gender interactions in health care, particularly in settings where cultural and religious values play a central role in the provision of care.
Islamic principles of modesty significantly influence gender interactions in health care, particularly in settings where cultural and religious values shape care provision. Gender preference reflects both providers’ and patients’ inclination for same-gender interactions, rooted in teachings on Awrah (bodily exposure), Lams (physical contact), Khalwa (seclusion), and eye contact (Rashidi & Rajaram, 2001; Padela & Del Pozo, 2011; Kareem & Adeogun, 2020; Mujallad & Taylor, 2016). These concerns are heightened in gynecological care, where exposure can cause emotional distress (Kareem & Adeogun, 2020; Mujallad & Taylor, 2016; Padela & Del Pozo, 2011).
Islamic teachings discourage unnecessary physical contact, reinforcing gender-concordant care, particularly in obstetrics and gynecology, where it is often viewed as essential (Kareem & Adeogun, 2020; McLean et al., 2010). Separation mandates extend to healthcare facility design, ensuring gender-segregated care (Mujallad & Taylor, 2016). Meanwhile, Khalwa (private seclusion of a non-mahram man and woman) is explicitly prohibited, posing challenges in consultations and physical examinations (Mujallad & Taylor, 2016; Padela & Del Pozo, 2011; Wehbe-Alamah et al., 2021).
In practice, translating these concepts into healthcare settings presents significant challenges. Muslim HCPs and students often experience difficulty with cross-gender interactions due to the tension between Islamic principles of modesty and the practical demands of clinical guidelines. These challenges are especially apparent in relation to gender preferences, physical contact, and the professional obligation to provide care to patients of the opposite sex. This tension is highlighted in a qualitative interview study conducted in Oman by Al Busaidy and Borthwick (2012), which explored how occupational therapists navigate modesty-related conflicts in cross-gender care (Al Busaidy & Borthwick, 2012). In healthcare settings, Islamic teachings prohibiting physical contact between unrelated men and women create substantial obstacles. For instance, female healthcare providers may experience psychological and emotional discomfort when performing intimate procedures or caring for male patients, as these actions conflict with their beliefs on modesty. Similarly, male HCPs and nursing students often struggle to gain clinical experience or practice essential skills, particularly in obstetrics and gynecology. Many Muslim women decline care from male students due to modesty-related values, restricting these students’ ability to complete vital training (McLean et al., 2010; Odeh Yosef, 2008; Yaseen et al., 2021).
Professional ethics require all HCPs to provide equal care to all patients (Kareem & Adeogun, 2020; Padela & Del Pozo, 2011; Yaseen et al., 2021); however, the lack of policies accommodating religious modesty—such as providing privacy during care or allowing flexibility for modesty requirements—exacerbates this conflict. This further challenges HCPs in balancing their religious beliefs with professional obligations (Yaseen et al., 2021).
Muslim HCPs draw on different strategies to manage modesty-related challenges in clinical practice. Some ask for a chaperone when working with patients of the opposite gender, especially during intimate procedures, as a way to maintain modesty and reduce personal discomfort (Mujallad & Taylor, 2016). Others take simple practical steps, such as wearing gloves to limit skin-to-skin contact (Ezenkwele & Roodsari, 2013; Penney, 2022), or requesting same-gender assignments through discussions with supervisors whenever possible (McLean et al., 2010). These approaches can be effective but are not always sufficient, particularly in emergencies or high-pressure settings where gender-concordant care is difficult to arrange. In these cases, professionals may rely on the Islamic principle of necessity, which allows exceptions to religious rules to meet urgent care needs without abandoning faith commitments (Padela & Del Pozo, 2011). Even with these adaptations, the absence of consistent institutional policies leaves many Muslim healthcare providers and students under emotional and psychological strain. This highlights the importance of developing inclusive policies that take religious obligations into account, promote diversity, and ensure staff can meet professional responsibilities without compromising their beliefs (Kareem & Adeogun, 2020; Yaseen et al., 2021). The included studies provided recommendations to address conflicts related to gender interactions for HCPs and students in healthcare settings. One suggestion is to prioritize Muslim HCPs for same-gender care during sensitive procedures, which can help minimize the discomfort caused by such situations (Kareem & Adeogun, 2020; McLean et al., 2010; Padela & Del Pozo, 2011; Yaseen et al., 2021). If same-gender care is not feasible, it is essential to use a same-gender chaperone during cross-gender interactions, especially when providing care for intimate areas or exposing them. This approach ensures that professionals can uphold their values while continuing to deliver care effectively (Padela & Del Pozo, 2011; Rashidi & Rajaram, 2001; Yaseen et al., 2021).
In addition, inclusive policies should be implemented to support Muslim students in completing their clinical training without conflicting with their modesty beliefs. This can be achieved by offering same-gender supervision or providing alternative educational solutions, such as simulation-based training, role-playing exercises, or case-based learning, when care or interactions with the opposite gender are required. (McLean et al., 2010; Odeh Yosef, 2008; Yaseen et al., 2021).
Discussion
The discussion highlights the complex relationship between Islamic modesty and nursing guidelines, shedding light on the underlying challenges within contemporary healthcare frameworks. At its core, this conflict arises from fundamental differences between Islamic teachings and nursing perspectives. Specifically, the tension between Islamic collectivism and liberal individualism lies at the heart of this issue. On one hand, collectivism emphasizes the prioritization of community and collective rights, alongside religious duties (Ansori & Fauzan, 2022; Álvarez de la Roche, 2017). On the contrary, nursing guidelines, rooted in the principles of human rights and liberalism, place a strong emphasis on individual rights and self-determination (Frick, 2010). This stark contrast underscores a key structural dilemma in current healthcare systems, which often struggle to balance the integration of diverse cultural and religious practices with the maintenance of professional standards and protocols.
Central to the Islamic collectivist perspective is the concept of modesty (al-haya), which encompasses modesty in dress, behavior, and speech (Zilio-Grandi, 2017). From an Islamic viewpoint, modesty serves as a safeguard against sexual misconduct, providing clear guidance on behaviors and dress codes aimed at protecting individuals from harassment, rape or insult (Rahman, 2022). However, these principles often clash with the liberal individualist foundations of nursing guidelines, which are based on the belief that universal principles apply equally to all individuals, irrespective of their cultural or social contexts (Schuck, 2024). This ideological divide further complicates efforts to reconcile religious practices with professional healthcare requirements. As a result, Muslim nurses, caught between their professional duties and religious commitments, face psychological challenges that extend far beyond surface-level discomfort (Elzamzamy & Keshavarzi, 2019).
Turning to Islamic teachings, cross-gender interactions between unrelated men and women are generally discouraged, particularly if they may lead to temptation or a breach of Islamic principles. However, Islamic scholars emphasized such interactions are permissible in contexts like health care, education, and the workplace, provided that Islamic rules and guidelines are followed. These principles include dressing modestly, refraining from soft or tempting speech, avoiding adornment, preventing seclusion (khalwa) with an unrelated member of the opposite sex, limiting interactions to what is necessary, and favoring nonmixed environments whenever possible (Islamweb, 2015).
Despite the clarity of these Islamic principles, the review found that modesty and gender dynamics, particularly in cross-gender interactions within health care and education, are not well defined in the literature. Although these themes are frequently discussed, they appear in fragmented ways, using varied terminology and perspectives that create inconsistencies. For instance, the perception of modesty varies widely, and the literature reflects significant ambiguity in its classification, with no clear consensus on its forms or expressions. Similarly, in discussions of gender interaction, terms such as “gender preference,” “religious commitment,” “religious or cultural challenges,” “gender-concordant care,” and “gender segregation” are often used interchangeably, creating confusion about their precise meanings. Furthermore, many studies focus on personal opinions without clarifying whether they stem from religious teachings, cultural practices, personal interpretation, or a combination of these factors. This lack of conceptual clarity, particularly regarding how modesty behaviors are defined, classified, or understood in health care, complicates efforts to develop a comprehensive understanding of these issues within an Islamic context.
Beyond conceptual ambiguities, these inconsistencies create challenges in healthcare settings, particularly regarding dress requirements. Therefore, it is essential that dress regulations prioritize religious modesty as the primary consideration rather than cultural norms. While certain cultural garments, such as the thawb, may pose challenges in healthcare settings due to their length, style, or color, modest dress can still be maintained by ensuring clothing is loose-fitting and fully covers the skin. In this context, garment style and color become secondary concerns, provided infection-control policies remain flexible and accommodate religious principles.
However, these ambiguities extend beyond dress and daily healthcare practices, exposing a broader gap in academic and professional discourse. Further research is needed to understand modesty and gender interaction in Islam within healthcare settings across various academic and professional fields, as well as to determine whether these differences stem from cultural, religious, or personal interpretations. Addressing these distinctions is crucial for resolving conflicts with nursing guidelines and developing professional standards that uphold Islamic values while recognizing cultural influences as secondary considerations.
This gap in policy and training is closely linked to the insufficient research and exploration of healthcare providers’ experiences, resulting in guidelines that lack clarity and consistency. In Western healthcare systems, policies tend to be inconsistent, with decisions left to the subjective discretion of individual managers or institutions (Malik et al., 2019). As a result, disparities in implementation arise, leading to perceptions of unfair treatment. Similarly, in Muslim-majority countries, the absence of standardized guidelines creates uncertainty, leaving healthcare providers without adequate support to navigate these challenges. This lack of clarity not only exacerbates conflicts and causes inefficiencies but also further alienates Muslim nurses.
While some studies have suggested potential solutions, they remain fragmented across diverse fields, including ethics, healthcare policy, and religious studies, without being consolidated into a comprehensive and unified framework. In addition, they lack the depth needed to fully address how Islamic modesty concerns interact with healthcare policies in practice. Therefore, a deeper understanding is essential to developing standardized policies that balance professional requirements with religious and cultural considerations, ultimately fostering a more inclusive and equitable healthcare environment.
To address these challenges, clear guidelines accommodating religious practices while maintaining high-quality care are essential. Implementing modesty-compliant dress codes and gender-sensitive care fosters inclusivity, as seen in Singapore’s flexible policies (Kuah et al., 2021; Lian, 2016; Ministry of Health Singapore, 2021). Standardized policies ensure equitable treatment while safeguarding professional and patient care rights. Mandatory cultural competency training, successfully used in the United States, can help healthcare providers navigate diversity, reduce misunderstandings, and strengthen teamwork (Martin et al., 2016; Govere & Govere, 2016). In addition, adopting gender-based staff assignments, particularly for intimate care, can enhance trust, equity, and care quality (Padela & Del Pozo, 2011; Penney, 2022). Together, these strategies promote equity, effectiveness, and workplace cohesion.
However, while such strategies can support inclusivity and strengthen patient care, they also bring potential challenges. In practice, they may interrupt workflow, create uneven task distribution, or leave Muslim healthcare providers viewed by colleagues as inflexible (Saidun et al., 2021). At times, these adjustments can raise questions of fairness and even divide teams. They may add extra responsibilities to other staff, cause frustration, and, if poorly managed, erode morale and weaken teamwork. Over time, these tensions can damage professional relationships and foster perceptions of inequity within the workforce. The difficulty is compounded by the fact that most healthcare systems, having been shaped by liberal and secular traditions, were never originally designed to accommodate religious practices—making such changes more difficult to integrate smoothly.
Tackling these challenges requires a balance between inclusivity and the realities of clinical practice, supported by open communication and well-structured training programs (Afridah & Lubis, 2024; Kiradoo, 2022). Just as importantly, education should underline that making space for religious practices is not a favor or special treatment but a legal and ethical duty (Saidun et al., 2021). Framing it this way reinforces fairness and helps to build a workplace culture where inclusion is genuinely valued.
Gender-based staff allocation, particularly in intimate care, can strengthen trust, equity, and care quality (Padela & Del Pozo, 2011; Penney, 2022). However, without careful implementation, it may also cause divisions and perceptions of unfairness, underscoring the need for clear, evidence-based, and culturally competent policies. Current research largely centers on women, overlooking men’s experiences, and little is known about providers’ awareness of modesty or its role in clinical conflict. Future studies should adopt a gender-inclusive focus, especially on nurses’ experiences, to inform consistent, sensitive policies that support both staff and patient care.
Limitations
Several limitations were acknowledged in this review. Despite a comprehensive search, certain relevant studies, particularly non-English or nonindexed ones, may have been missed. Including both primary and secondary sources introduced variation in quality. Although the focus was on healthcare providers, many studies reflected patient or community perspectives due to limited research on providers. The conceptual ambiguity of modesty also posed challenges in interpretation. As a scoping review, the aim was to map the literature rather than evaluate evidence quality or produce generalisable conclusions.
Conclusion
This scoping review examined how Islamic modesty has been addressed in healthcare research. The findings show that modesty is discussed in fragmented and inconsistent ways, often without clear definition or explicit grounding in its religious and ethical foundations. As a result, modesty is usually mentioned briefly rather than examined as a distinct source of value-based conflict, which limits the literature’s ability to inform clinical practice, professional education, and policy development. By synthesizing this scattered evidence, the review highlights the need for more focused and analytically robust research on Islamic modesty in healthcare settings. Future studies should move beyond surface-level accounts to examine how modesty-related values are understood, experienced, and managed in everyday clinical practice, thereby supporting the development of guidance that respects religious values while remaining aligned with professional healthcare standard.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596261427431 – Supplemental material for Exploring Values Conflict Between Islamic Modesty and Healthcare Guidelines Among Healthcare Providers and Students: A Scoping Review
Supplemental material, sj-docx-1-tcn-10.1177_10436596261427431 for Exploring Values Conflict Between Islamic Modesty and Healthcare Guidelines Among Healthcare Providers and Students: A Scoping Review by Hamza Albawaizeh, Aideen Gildea and Iseult M. Wilson in Journal of Transcultural Nursing
Footnotes
Acknowledgements
The authors acknowledge the support of Queen’s University Belfast and Mutah University for providing research resources and academic support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a scholarship from Mutah University, Jordan, for doctoral studies at Queen’s University Belfast (QUB), United Kingdom.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.